“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
Author: PAVACA
BFA in Piano; BFA in Music Education; MA in Leadership. Retired professional musician and soprano, teacher, composer, accompanist/coach. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 - 2018), First Professor of the Darden School of the University of Virginia. Writes under the names of: M.E. Forbes; M.E.C. Forbes; PAVACA.
The image of Truth and Lies for the header of today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here.
>>>>>>>>>>>>>>>>>>>>
The COVID-19 bioweapon “vaccines” (in reality, dangerous and deadly gene-altering therapy injections) — which have now been proven to cause, to aggravate, or to re-establish a myriad of different types of medical conditions (physical and/or psychological conditions; including those which were under control or were in remission before the patient took any of these “vaccines”) — which have now been proven to cause or to aggravate these conditions as long as three and a half years post-injection — which render the “vaccinated” person to be a “ticking time bomb” of negative cardiac and lung issues — which interfere with and/or damage the p53 protein of the human body, the protein that detects cancer cells — which severely damage or even destroy the innate immune system of the human body, rendering it catastrophically vulnerable to all sorts of infections (including to COVID-19 infection) — which destroy up to 60% of the lifetime supply of eggs in the “vaccinated” female’s body — which induce myocarditis / pericarditis in children (and in adults) — are still being administered to millions of persons all over the world. These “vaccines” are still being pushed by the CDC and the FDA in the United States. These “vaccines” are still on the CDC’s Childhood and Adolescent Immunization Schedule. These “vaccines” are still on the CDC’s Adult Immunization Schedule. Those who are the main figures in the lab-creation of the COVID-19 bioweapon virus itself, and of the COVID-19 bioweapon “vaccines” (either in research, or in funding, or in suppression of the truth about these bioweapons) — Dr. Anthony Fauci; Dr. Francis Collins; Dr. Deborah Birx; Dr. Ralph Baric; Dr. Peter Daszak; Dr. Robert Redfield; Dr. Stephen Hahn; among others — have not been brought to justice. Please search the following sources for more information: https://jessicar.substack.com/; https://www.thefocalpoints.com/; https://www.theqtree.com/author/pavaca/; https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-age.html; https://www.cdc.gov/vaccines/hcp/imz-schedules/adult-age.html.
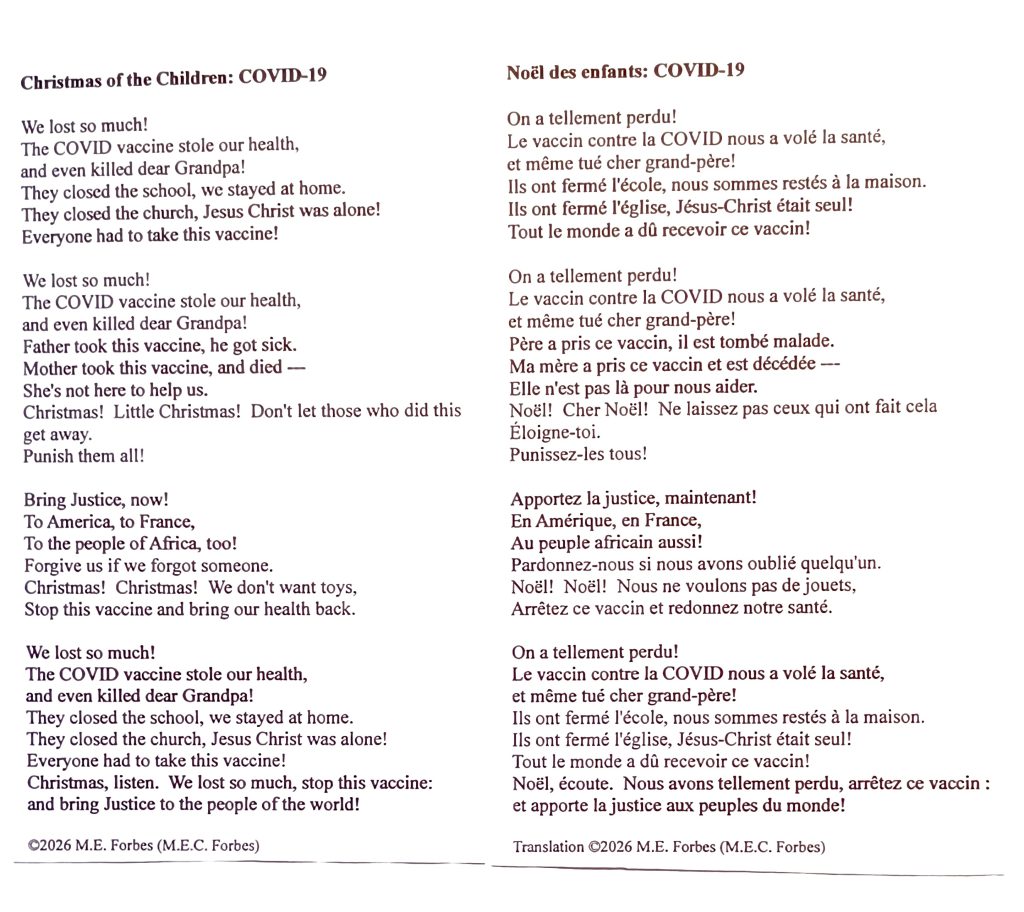
“Noel des Enfants qui N’ont Plus de Maisons” (“Christmas of the Children who No Longer Have a Home”) is an art song written in December 1915 (during World War I) by the French composer, Claude Debussy. The French lyrics are below, followed by the English translation:
Yours Truly is deeply appreciative of, and thanks, https://www.melodietreasury.com/ for the above image of the original French lyrics and of the English translation of this song.
In order to put into context how this song applies to today’s offering, please listen to baritone John Brancy perform it with pianist Peter Dugan. Yours Truly is deeply appreciative of the musical talents of the performers, and thanks https://www.youtube.com/ for the opportunity to share their efforts. The song is under three minutes long:
Years ago, Yours Truly had the honor to accompany her voice teacher, baritone Edmund Najera, when he performed this song as part of a voice recital. Even decades later, when I hear this song, it brings chills down the spine. The raw emotions of anger, sorrow, loss, and fear in the original lyrics leap out of the vocal line and of the piano accompaniment music.
>>>>>>>>>>>>>>>>>>>>
What the world has suffered since late 2019 — and what still continues today — is not a war of bombs and of bullets: It is a war waged with fear and gaslighting; with a lab-created “virus” cobbled together from pieces of various animal coronaviruses, and named SARS-CoV-2; with needles and syringes. It is waged in healthcare clinics, hospitals, and pharmacies. It is the war of COVID-19: the bioweapon virus itself, and the bioweapon “vaccines.” It is a war waged using unquestioning acceptance of government statements that the COVID-19 bioweapon “vaccines” are “safe and effective” — when it has been conclusively proven that they are not. It is a war waged using unquestioning compliance with “mandates” or “requirements” or “recommendations” by employers, by school systems, by healthcare providers, that people who wish to access these entities be COVID-19 “vaccinated.” It is waged in the laboratories of Pfizer-BioNTech, of Moderna, of Novovax, and of other entities, which lab-create and manufacture these “vaccines.” It is a war waged through the marginalizing, the silencing, the loss of jobs, the loss of Licenses to Practice Medicine, and the “de-platforming” of those who dare to question the official narratives; of those who dare to present solid evidence that these “vaccines” are dangerous and deadly to those who take them; of those who dare to treat COVID-19 infected persons — or to offer alternative (and safe) prophylactic COVID-19 protocols — using “off-label” drugs, and/or alternative therapeutic vitamins and supplements. It is waged through the enormous financial grants by government funders (NIH, NIAID), and by private funders (Gates Foundation, CEPI, GAVI) to those who lab-create these “vaccines.” A stunning, recent example of the “silencing” of those who dare to present evidence that the “vaccines” are NOT “safe and effective” is written about here: https://worldcouncilforhealth.substack.com/p/one-of-the-greatest-manipulations (the death by suicide of COVID-19 “vaccine” dangers statistician, Christine Cotton.) Meanwhile, the induced, aggravated, or re-established illnesses, injuries, and disabilities in “vaccinated” people, continues. The deaths that result from these “vaccines” being injected into human beings continues.
>>>>>>>>>>>>>>>>>>>>
Yours Truly presents a “modern-day” version that she wrote of the lyrics for “Noel des Enfants.” The English language version and the French language version are below:
As in the original lyrics by M. Debussy, the story is told through the experiences of children. However, in Yours Truly’s opinion, the lyrics can also be a story as told by adults — illness; death; loss of loved ones; a sense of helplessness. A sense — a realization — that, despite the assurances from government (World War I was supposed to be “the war to end all wars”; the COVID-19 bioweapon “vaccines” were supposed to “stop the spread” and be “safe and effective”) — these “assurances” were lies: and that people are paying the price for believing the lies.
(Notes: One: Apologies for the layout — one is not a professional editor; and, Two: while the original Claude Debussy lyrics and piano accompaniment are considered to be “In the public domain” in the United States (per Wikipedia search regarding Public Domain items in the United States), Yours Truly personally would not attempt to use the French translation of the new lyrics that I wrote to replace, or substitute for, the original lyrics of the song.)
>>>>>>>>>>>>>>>>>>>>
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA, A modRNA, AN saRNA, OR A taRNA PRODUCT OF ANY KIND. THIS INCLUDES THE COVID-19 BIOWEAPON “VACCINES.”
THERE MUST BE MUCH MORE RESEARCH INTO THESE PLATFORMS. THERE MUST BE COMPLETE AND DETAILED ANALYSES OF RESEARCH RESULTS DATA ON THESE PLATFORMS. THERE MUST BE COMPLETE AND RIGOROUS TESTING OF THESE PLATFORMS. THE RESULTS MUST CLEARLY INDICATE THAT THESE PLATFORMS ARE “SAFE AND EFFECTIVE” FOR USE IN HUMAN BEINGS. THE RESULTS MUST BE MADE PUBLIC. ONLY THEN, CAN PRODUCTS THAT USE THESE PLATFORMS BE ALLOWED TO APPLY FOR FDA AUTHORIZATION OR APPROVAL.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Disclaimer and Notice: Except for URL’s and other items available on the Internet, the ideas and/or opinions in today’s offering are by PAVACA (M.E. Forbes / M.E.C. Forbes.) Proper credit must be given to PAVACA if ideas and/or opinions in today’s offering are used by other blog writers; by podcasters; or in print or social media.)
BFA in Piano; BFA in Music Education; MA in Leadership. Retired professional musician and soprano, teacher, composer, accompanist/coach. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 – 2018), First Professor of the Darden School of the University of Virginia. Writes under the names of: M.E. Forbes; M.E.C. Forbes; PAVACA.
The vintage image of FDA items is courtesy of Hillerman Film and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications by our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated items in today’s offering will be cited as such. If readers, wish to post AI-generated items in today’s discussion thread, they must cite their source. Thank you.
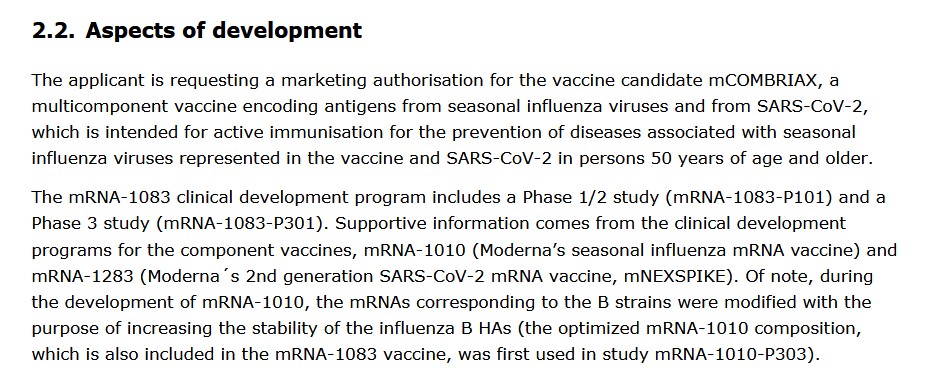
The “TD;LR” summary of the mRNA-1010 situation in the United States: Moderna is desperate to get FDA approval for this modRNA “influenza vaccine”, so the company can proceed to finish getting mCOMBRIAX also FDA-approved. The backstory on this situation is outlined here: https://www.patsnap.com/resources/blog/articles/pfizer-vs-moderna-mrna-patent-strategies-and-pipelines/, updated 2 April 2026. A screenshot from this article is below:
However, Moderna has ALREADY applied for a Patent for mRNA-1010: https://patents.google.com/patent/EP4274607A1/en; title: “Seasonal rna influenza virus vaccines.” The Patent application was submitted on 10 January 2022. The current Status of the application is “Pending.” By the way, the Patent claims state that as many as SEVEN different types of influenza virus strains can be used in the formulation of mRNA-1010. Also notice that the Patent application was filed back in January 2022: this means that the laboratory work to perform the experiments, aggregate data, analyze the data, and so on, was begun years before the application submission.
However, Moderna has ALREADY applied for a Trade Mark (TM) for mRNA-1010, under the brand name mFLUSIVA. The application was submitted on 27 February 2026: https://uspto.report/TM/99674080. **** It was on 26 February 2026 that the European Medicines Agency (cited above) recommended the use of mCOMBRIAX (mFLUSIVA + mNEXSPIKE combination “vaccine”) in the European Union.
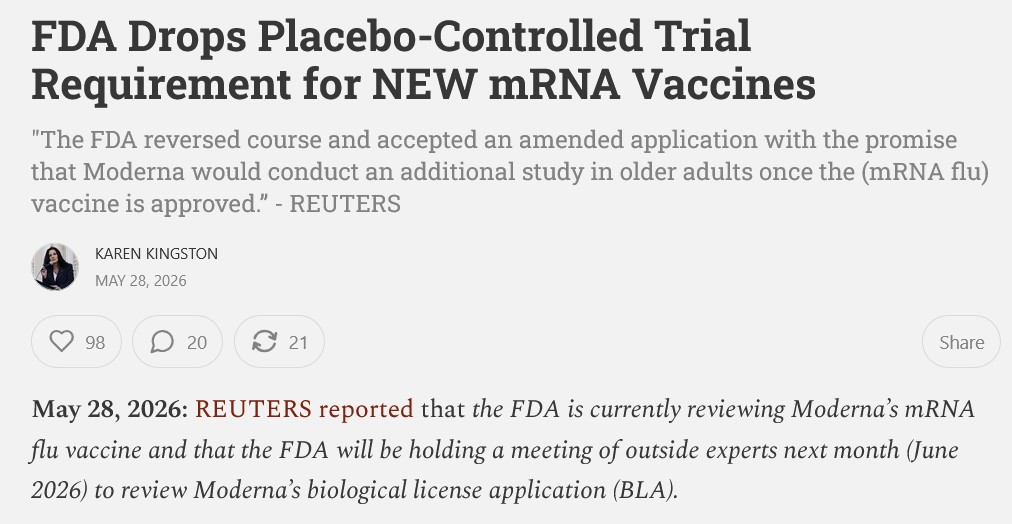
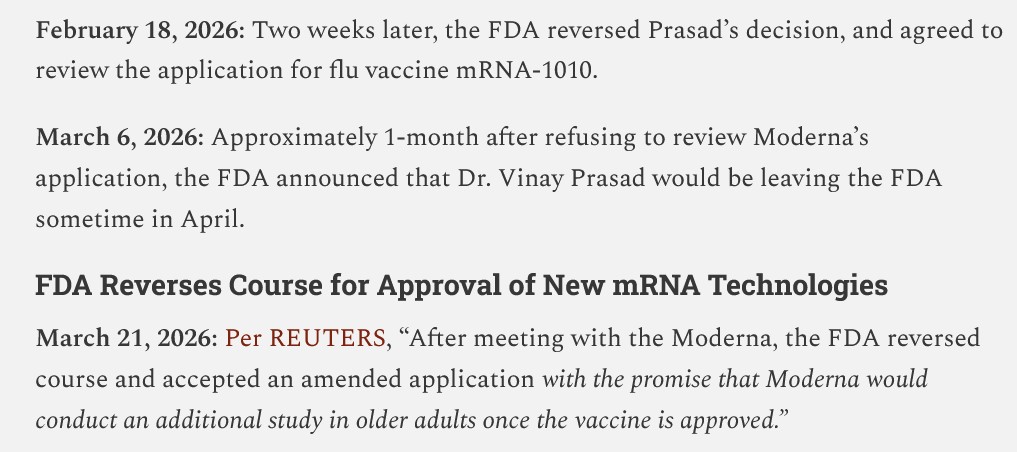
It appears that, in Yours Truly’s opinion, Moderna is performing “all the right moves” in order to ensure that mRNA-1010 (mFLUSIVA) is approved by the FDA for use in the United States as soon as possible. This includes, apparently, maneuvering to have Dr. Vinay Prasad (who refused the BLA application for mRNA-1010 in February 2026) removed from his position at the FDA. Per the Kingston Report, cited above:
This “FDA meeting with Moderna” was the “Type A” meeting that Yours Truly wrote about in the Health Friday posts cited above.
Does the reader see how the game is played by Big Pharma? It appears that Moderna will not allow anyone to interfere with the company’s goal of getting mRNA-1010 (mFLUSIVA) through the FDA approval process and have the injectable ready for the United States 2026-2027 “flu season market”; and, also, that Moderna will not allow anyone to interfere with the company’s goal of getting mRNA-1083 (mCOMBRIAX) through the FDA approval process and have the injectable ready for the United States market as soon as possible.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Disclaimer and Notice: Except for linked URLs and other items in today’s offering that are available on the Internet, the ideas and/or opinions of today’s offering are by PAVACA. Credit must be given to PAVACA if the ideas and/or opinions of today’s offering are used by other blog writers; by podcasters; or in print or social media.)
The header image for today’s offering is courtesy of Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: there is AI-generated material in The Focal Points and the 2nd Smartest Guy In The World articles in today’s offering. If readers wish to post AI-generated material in today’s discussion thread, they must cite their source. Thank you. Special thanks to our “sister blog”, https://www.marica1776.com/, for some of the items in today’s offering.
A personal note: On this date in 1947, a man named Samuel, and a woman named Catherine, were married at 10:30AM in a church ceremony in Pittsburgh, PA. It was a Thursday. They left right after the wedding breakfast for their two-and-a-half day honeymoon at Niagara Falls, NY. Samuel had to be back at work the following Monday as a pharmacist’s apprentice while finishing his studies at Pharmacy school; and, Catherine also had to be back at work the following Monday as a secretary. They set up housekeeping in their first home: a two-room apartment (with a shared bathroom) in a reconverted old house in the Shadyside section of Pittsburgh. Samuel and Catherine were Yours Truly’s parents. I believe they’re having a wonderful time together in the next world. Love you, Daddy and Mother. Miss you. Thank you — Thank you.
>>>>>>>>>>>>>>>>>>>>
Some Interesting Items from the plethora of news out there:
Ebola:
**** From The Focal Points: https://www.thefocalpoints.com/p/nih-ebola-expert-under-fbi-investigation, “NIH Ebola Expert Under FBI Investigation for Smuggling Pathogens Into America From the Congo”, Nicolas Hulscher, MPH, 20 May 2026. It appears that Dr. Vincent Munster, returning from a trip to the Democratic Republic of the Congo (and accompanied by another NIH employee), was detained at the airport when returning to the United States for attempting to bring undeclared dangerous pathogens back in his luggage. Dr. Munster’s lab at the NIH “specialized” in the study of, and experimentation with, the Ebola virus. He is also one of the co-authors of the rejected 2018 DEFUSE proposal — along with Dr. Peter Daszak AND Dr. Ralph Baric. Please see the article for more information. There is also an interview with Mr. Hulscher that is included. (Yours Truly: One wonders if the situation with Dr. Munster could be a “data point” in the “sudden resignation” of the now-former Acting Director of the NIAID — Dr. Jeffery Taubenberger, the Fauci acolyte and “inventor” of the “Universal Influenza Vaccine” in 2020 [while Dr. Taubenberger was working at the NIH]: https://www.usnews.com/news/health-news/articles/2026-05-22.acting-niaid-chief-steps-down-amid-ebola-hantavirus-concerns.)
**** Again, from The Focal Points: https://www.thefocalpoints.com/p/the-bedrock-of-containment-why-sanitation, “The Bedrock of Containment: Why Sanitation is the Key to Controlling Ebola”. Peter A. McCullough, MD, MPH, 25 May 2026. The scientific paper referred to in the article is here: https://doi.org/10.1186/s12889-020-8240-9. “Hygiene programming during outbreaks: a qualitative case study of the humanitarian response during the Ebola outbreak in Liberia”; Alexandra Czerniewska and Sian White. 2020.
**** And, last but not least, the involvement in Ebola virus experiments by the now-fired (“retired” for “no reason disclosed”) and disgraced “Eminence Grise” of the COVID-19 disaster: Dr. Ralph Baric, PhD; experiments that used Gain-of-Function techniques. Dr. Baric authored the following papers: the first, at approximately the same time that the 2014 Ebola outbreak was raging; the second, in 2024: https://pmc.ncbi.nlm.nih.gov/articles/PMC4241145/, “Host genetic diversity enables Ebola hemorrhagic fever pathogenesis and resistance”; Ralph Baric, PhD, et al. 30 October 2014; and, https://doi.org/1016/j.celrep.2024.114127, “Mapping of susceptibility loci for Ebola virus pathogenesis in mice”; Ralph Baric, PhD, et al. 28 May 2024.
>>>>>>>>>>>>>>>>>>>>
Ticks:
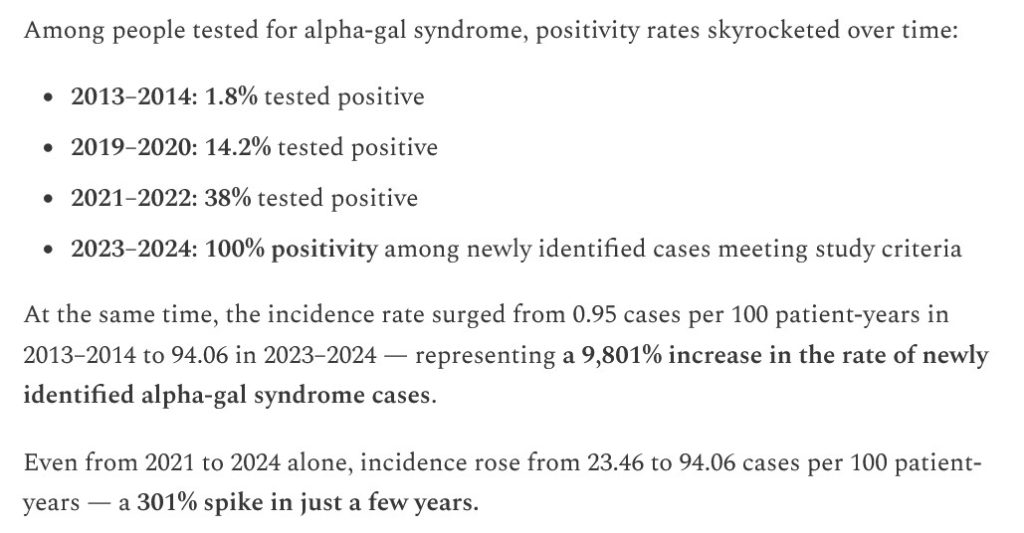
**** From The Focal Points: https://www.thefocalpoints.com/p/study-tick-borne-alpha-gal-syndrome, “STUDY: Tick-Borne Alpha-Gal Syndrome Incidence Skyrocketed 9,800% in the U.S. Since 2013”, Nicolas Hulscher, MPH, 22 May 2026. Please see the screenshot, below, from his article:
**** From 2nd Smartest Guy In The World: https://www.2ndsmartestguyintheworld.com/p/lyme-and-lone-star-bioweapon-diseases-33d, “LYME & LONE STAR BIOWEAPON DISEASES UPDATE: “This Tick Thing is Nuts” & Since 2013 Alpha-Gal Syndrome Incidence Skyrocketed 9,800%”, 24 May 2026. This article quotes the Hulscher post cited above, and also includes more information from other sources.
**** “And now, for something completely different”: the “contrarian view” from Sasha Latypova: https://sashalatypova.substack.com/p/trick-ticks-fear-porn-to-cover-up, “Weaponized Ticks!!!, a mini review”, 25 May 2026. Ms. Latypova argues that Alpha-Gal Syndrome is actually caused by immune system damage induced by vaccines.
Yours Truly will weigh in on the latter: One: there has been a huge increase in reported diagnoses of Alpha-Gal Syndrome since the rollout of the COVID-19 bioweapon “vaccines” in 2021. Two: the COVID-19 bioweapon “vaccines” induce or aggravate multiple types of immune and/or autoimmune disorders: see https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, regarding BNT162b2 (COMIRNATY), FDA date-stamped 30 April 2021; scroll down to the Appendix 1. List of Adverse Events of Special Interest section of this report. “Autoimmune disorder”; “Complement factor C1 decreased”; Complement factor C2 decreased”; Complement factor C3 decreased”; Complement factor C4 decreased” are among the listings. The Complement factors C1 to C4 are crucial proteins in the innate immune system. Decreases / deficiencies in any or all of these complement factors will create dysfunction / malfunction of the innate immune system, inducing conditions ranging from angioedema to recurrent infections to neurological conditions, and more. Three: Please see: https://www.annalallergy.org/article/S1081-1206(23)00002-9/fulltext, “Alpha-Gal Syndrome is an immunoparasitologic disease”, John C. Carlson, MD, PhD, April 2023. Four: there may well also be the involvement of other types of “vaccines” (in other words, non-COVID-19 bioweapon “vaccines”) in damage to the innate immune system.
>>>>>>>>>>>>>>>>>>>>
MAiD: It appears that the use of this “assisted suicide” protocol in Canada is “expanding”:
WHAT 🤯 A man in his 40s with inflammatory bowel disease, was assessed outside a Tim Hortons, offered MAID, AND driven by the DR to the assisted suicide facility, and killed by MAID 🤯
I honestly thought this headline was fake, but it’s real
Inflammatory bowel disease is treatable and manageable: https://www.cdc.gov/inflammatory-bowel-disease/living-with/index.html. By the way, “Inflammatory bowel disease” is ALSO LISTED in the Appendix 1. section of the BNT162b2 (COMIRNATY) report cited above: it can therefore be an adverse event of the COVID-19 bioweapon “vaccines.” Note: some media outlets (for example, https://www.vigilantfox.com/p/germany-and-canada-go-full-1984-daily), state that the man (in his 40s) suffered from Crohn’s Disease, mental health issues, and substance abuse issues — all of which are treatable and manageable: and is ALSO LISTED as an adverse event of the COVID-19 bioweapon “vaccines”, per the BNT162b2 (COMIRNATY) report cited above.
>>>>>>>>>>>>>>>>>>>>
And, last but not least, THIS insanity, in OREGON:
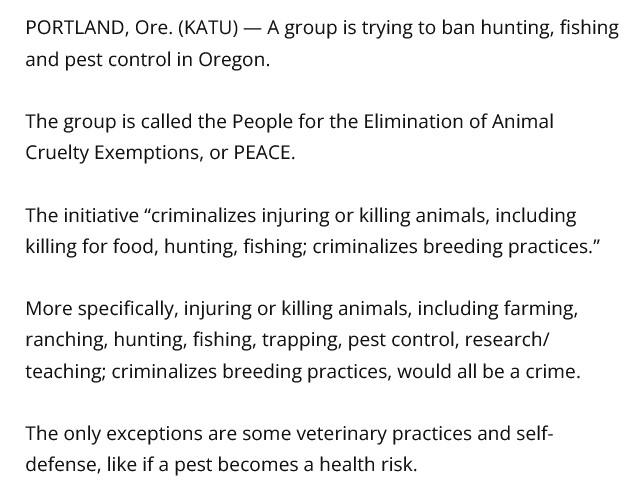
A petition is now the November ballot in Oregon that, if passed, would criminalize the killing of any animal (including fish and other marine life) for food; would ban pest and insect control; would criminalize and ban the teaching of these practices; and more. Enough signatures have been obtained to put this madness up for a vote:
An effort to criminalize the killing of animals for food in Oregon is a step closer to being on the November ballot.
IP-28 would make it illegal to injure or kill animals and would effectively ban hunting, fishing and the breeding of animals. https://t.co/Je1Z43xKAm
(Intellectual Disclaimer and Notice: Except for the linked URLs and other items in today’s offering that are found on the internet, the ideas and/or opinions in today’s offering are by PAVACA. Credit must be given to PAVACA if ideas and/or opinions in today’s offering are used by other blog writers; by podcasters; or in print or social media.)
The header image of Justice for today’s offering is courtesy of Mammoth Memory Art and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated items in today’s offering will be cited as such. If readers wish to post AI-generated items in today’s discussion thread, they must cite their source. Thank you.
It is time — in fact, is it past time — to bring Dr. Ralph Baric, PhD, to account. His activities must be be swept under the rug, now that the University of North Carolina, Chapel Hill, has forced him to retire in June of this year.
Yours Truly brings the following as “preliminaries”: https://merylnass.substack.com/p/today-ralph-baric-was-forcibly-retired, “Today, Ralph Baric was forcibly retired. Let’s examine his career and his central role in the COVID disaster”, Meryl Nass, MD, 12 May 2026. Dr. Nass, who lives in Maine, was suspended from her License to Practice Medicine in 2023 by the Maine Board of Licensure in Medicine — for prescribing Ivermectin to treat COVID-19. https://merylnass.substack.com/p/dr-meryl-nass-on-professional-cancellation, 20 December 2023. Her License to Practice Medicine was “License Suspension for Discipline”, with “Suspended Until: Open End Date.” This means that Dr. Nass (a physician with over 40 years’ experience) cannot practice medicine in Maine until she admits “wrongdoing” to the Licensure board; that she takes “re-education” courses; that she agrees to have her work monitored; and, that she “shows remorse” — all of which she refuses to do. Her case is a prime example of what Establishment Medicine will do to punish licensed physicians who dare to treat COVID-19 with repurposed drugs (such as, Ivermectin.)
Why are the above important? They illustrate the breadth and depth of Establishment Medicine and of media “cancellation” / censorship of those who dare to tell the truth about the COVID-19 bioweapon “vaccines”, and of those who dare to treat COVID-19 with prescription drugs / therapeutics that are not on the “FDA-approved” list.
Why are the above important? They illustrate one aspect of the myriad “ripple effects” of the results of the work of one scientist — Dr. Ralph Baric, PhD, (being forcibly retired in June 2026) of the University of North Carolina, Chapel Hill: the scientist who was the Master Designer of the SARS-CoV-2 virus. The scientist who invented the “No See’m” method for hiding insertions / changes in virus gene codes in order to lab-create “new virus gene codes” of spliced-in or deleted code pieces. The scientist who taught multiple other scientists how to lab-create coronaviruses via his “Synthetic Genomics” paper that was published in 2006. The scientist who obtained the Patent for his “invention” of the SARS-CoV-2 virus template — Patent Number US9884895B2 — in March 2015: which Patent was obtained months before Dr. Baric (with Dr. Zheng-li Shi) published the infamous “Circulating Bat Coronavirus” paper in November 2015. The scientist who was a prime “acolyte” of Dr. Anthony Fauci in working on lab-created coronaviruses — with NIH/NIAID grants money from Dr. Fauci that began in the mid-1980s. The scientist who had deep ties with the Wuhan Institute of Virology and Dr. Shi. The scientist who had deep ties with Dr. Peter Daszak and EcoHealth Alliance. Yours Truly’s Health Friday six part series, The Baric Files, discusses the above, and traces Dr. Baric’s research journey (https://www.theqtree.com/author/pavaca; search “The Baric Files.”) One of the recurring themes of The Baric Files is the repeated Gain-of-Function experiments that Dr. Baric performed, literally over decades (beginning in the mid-1980s), related to animal coronaviruses. The March 2020 Patent for his “invention” of the SARS-CoV-2 virus template, the November 2020 “Circulating Bat Coronaviruses” paper, and other items, reflect the Gain-of-Function approach in his research. Keep this mind when reading onward:
In Yours Truly’ opinion: It appears that Dr. Ralph Baric, PhD, was involved in continuing Gain-of-Function research on coronaviruses, even after the general pause on that type of research in the United States was implemented in 2014. It also appears that Dr. Ralph Baric, PhD, engaged in continuing Gain-of-Function research as described in the DEFUSE proposal made by Dr. Peter Daszak (with Dr. Baric as a co-contributer) in 2018 to the United States military, which proposal was turned down. And, in both circumstances, it appears that Dr. Baric misled officials regarding the nature of the work that he was continuing to perform (Gain-of-Function experiments.)
>>>>>>>>>>>>>>>>>>>>
On (or, perhaps, before) 6 May 2026, an HHS Action Referral Memorandum, Notice of Suspension and Proposed Debarment of Ralph Baric, PhD, was sent to Dr. Baric via email and by Certified Mail – Return Receipt Requested. There appears to be no actual “sent date” listed on the HHS document; it can be assumed that it was sent between 15 April 2026 (the date of the NIH ROI evidence items list in the document), and 6 May 2026; link is below. The Notice was signed by HHS employee Jennifer D. Johnson, Suspension and Debarment Official and Deputy Assistant Secretary of Acquisitions: https://www.science.org/cms/asset/8669-dc85-416d-bc3a-f4600-bd2cc70/hhssuspensionandproposeddebarmentofralphbaricphd_05.06.2026_r.pdf. Apparently, Dr. Baric furnished a copy of the Notice to the American Association for the Advancement of Science (AAAS.) Two screenshots from the final page of the Notice are below:
Dr. Baric stated that he would fight the HHS Notice: https://bioethics.com/archives/102651, “Virologist accused to starting COVID-19 will fight U.S. ban on funding”, 12 May 2026.
But, something else happened: Dr. Baric was apparently summarily “retired” from the Gillings School of Global Public Health of the University of North Carolina Chapel Hill on 12 May 2026. The action was done under the aegis of Dr. Nancy Messonnier, MD, (Dean of the Gillings School since 2022); and a message was emailed to Gillings School faculty and staff on 12 May. https://www.theassemblync.com/news/education/higher-education/unc-coronavirus-researcher-ralph-baric-retires/, Karie Dean, 12 May 2026. His “retirement” is official as of 1 June 2026. (Yes, it’s that Dr. Nancy Messonnier, MD: sister of Rod Rosenstein. She was the “chief architect” of the COVID-19 bioweapon “vaccine” rollout and imposition campaign. https://sph.unc.edu/adv_profile/nancy-messonnier-md/.)
So it’s official now. Ralph Baric, perhaps the world’s most famous coronavirologist (or infamous, depending on who you ask) has retired.
"Nancy Messonnier, dean of the Gillings School of Global Public Health, and Maria Gallo, chair of the school’s epidemiology department, made…
So, despite the accolades about Dr. Baric by Dr. Messonnier and Maria Gallo in the email above as reported in The Assembly, why does the full tweet above have the phrase, “Messonnier and Gallo’s message did not cite a reason for Baric’s retirement.”?
**** However, several other things also took place prior to the HHS Notice going to Dr. Baric on 6 May 2026:
**** Per the Carolina Journal article cited above, Lee H. Roberts, the Chancellor of the University of North Carolina Chapel Hill, is still refusing to fully cooperate with demands to release the withheld 5,205 remaining documents related to Dr. Baric’s activities in the origins of COVID-19. Why?
**** Why does it feel as if Dr. Nancy Messonnier, MD, Dean of the Gillings School of Global Public Health at the University of North Carolina Chapel Hill, “threw Dr. Ralph Baric, PhD, under the bus” and summarily “retired” him on 12 May 2026? It is almost impossible that Dr. Messonnier had not heard of Dr. Baric or of his Gain-of-Function experiments on coronaviruses prior to becoming Dean; or, if not before taking the job, then certainly, at some point after her becoming Dean. Why did she suddenly “retire” him?
**** What aboutDr. Boyd Yount, PhD, and Dr. Sudhakar Agnihothram, PhD, the CO-INVENTORS of the 2015 SARS-CoV-2 virus “template” Patent along with Dr. Ralph Baric, Patent Number US9884895B2? Dr. Yount is still employed by the Gillings School of Global Public Health at the University of North Carolina Chapel Hill (https://sph.unc.edu/adv_profile/boyd-yount-jr/.) Dr. Agnihothram left UNC and has been working at the FDA since at least 2021 — in the CBER division (Center for Biologics Evaluation and Research): https://www.linkedin.com/in/sudhakar-agnihothram-8195309. Why aren’t these two co-inventors being investigated for their activities alongside Dr. Baric? Why is Dr. Sudhakar Agnihothram, PhD, serving as a speaker at CBER conferences and meetings?: https://www.fda.gov/media/186566/download; scroll down the page to “FDA CBER PARTICIPANTS.” Surely, the FDA knows that Dr. Agnihothrom would likely be biased towards approving COVID-19 bioweapon “vaccines.”
Dr. Ralph Baric, PhD; and his co-inventors of the SARS-CoV-2 virus “template” Patent US9884895B2, must all be investigated. Thoroughly. And held to account. Their “invention” was undoubtedly used by Dr. Zheng-li Shi at the Wuhan Institute of Virology, starting in late November 2015, in her experiments to further develop the SARS-CoV-2 virus. This was the (potentially “unfinished”) virus that was “somehow leaked” from her lab at the WIV in the late fall of 2019, and which was subsequently named “COVID-19”: https://www.theqtree.com/2026/01/09/health-friday-1-9-2026-open-thread-the-baric-files-part-four-ecohealth-alliance-wuhan-institute-of-technology-dr-zheng-li-shi-the-template-virus/. Dr. Baric used the bat coronavirus SHC014, which Dr. Shi was working on at her lab at WIV, and samples of which virus she sent to him, in his SARS-CoV-2 virus “template” Patent, US9884895B2. Please see below, from the Detailed Description of the Invention section of the Patent (the SHC014 virus labelled “WiV1 S”):
>>>>>>>>>>>>>>>>>>>>
Why is Dr. Ralph Baric, PhD, in particular, still being “protected” for his activities in lab-creating the COVID-19 virus “template”? What is contained in the 5,205 pages of documents that the University of North Carolina still refuses to release? Does the University of North Carolina believe that, by apparently forcing Dr. Baric into retirement, the school has “shut the door” on further investigation into his activities?
DR. RALPH BARIC, PhD, MUST BE BROUGHT TO ACCOUNT, ALONG WITH HIS SARS-CoV-2 VIRUS “TEMPLATE” CO-INVENTORS.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Disclaimer and Notice: Except for linked URLs and other items available on the internet, the ideas and/or opinions of today’s offering are by PAVACA. Credit must be given to PAVACA for ideas and/or opinions of today’s offering that are used by other blog writers, by podcasters, or in print or social media.)
The free header image of the Andes Mountains for today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated items in today’s offering will be cited as such. If readers wish to post AI-generated items to today’s discussion thread, they must cite their source. Thank you.
Today’s offering is not an elegant, “gardens of Versailles”-type layout. There are many items to consider. This is an evolving situation: details, news items, and so on, multiply by the day. There are a few relevant screenshots / images below. Yours Truly’s opinion is:
Those who **planned** for the COVID-19 bioweapon virus itself, followed by the COVID-19 bioweapon “vaccines”, to perform the task of immediately/within a short amount of time, culling the population of the Earth down to a “manageable” number of approximately 500 million persons (per the late Ted Turner) — and, finding that this task was not performed “properly” — have resorted to a “Plan B”: using an outbreak of the Andes Hantavirus (ANDV) on the MV Hondius as the excuse to generate a new “plandemic”, complete with gaslighting/fear operations, calls for “masking”, “lockdowns”, “vaccination”, and more. There may be other new”plandemic” measures in the wings. This new “plandemic” takes advantage of the weakened / destroyed immune systems in persons who are “vaccinated” with COVID-19 bioweapon “vaccines.” Many of the same actors in the COVID-19 disaster are involved with this Andes Hantavirus (ANDV) new “plandemic” rollout: the WHO; the CDC; USAMRIID; Fort Detrick; Big Pharma; Big Donors (Gates Foundation) — among others.
If readers suspect that the above sounds like a “rerun” of the COVID-19 virus PPE (Personal Protection Equipment) CDC recommendations — that is correct.
WHY, if it is the case that the Hantavirus outbreak on the MV Hondius is so concerning, did the WHO (World Health Organization) facilitate the IMMEDIATE RELEASE of the passengers from the ship to be “assessed” when the vessel docked at the Canary Islands?https://armageddonprose.substack.com/p/who-inexplicably-immediately-releases, “WHO Inexplicably, Immediately Releases All Passengers on Hantavirus Cruise Ship Without Quarantine”, 8 May 2026. The video announcement about this situation by Dr. Tedros Ghebreyesus, Director General of the WHO, is below:
WHO announces plan to fly #hantavirus cruise passengers all around the globe in order to milk the terror for all its worth pic.twitter.com/TnDh6XCq6W
Especially since it can take as long as 42 days post-exposure to the Andes Hantavirus (ANDV)for symptoms to appear? If readers are “starting to smell a rat”, that would be correct. If readers’ “interior antennae” are starting to register, “This feels like the start of the COVID lockdowns and “mandates” again, but now it’s Hantavirus”, that also would be correct.
>>>>>>>>>>>>>>>>>>>>
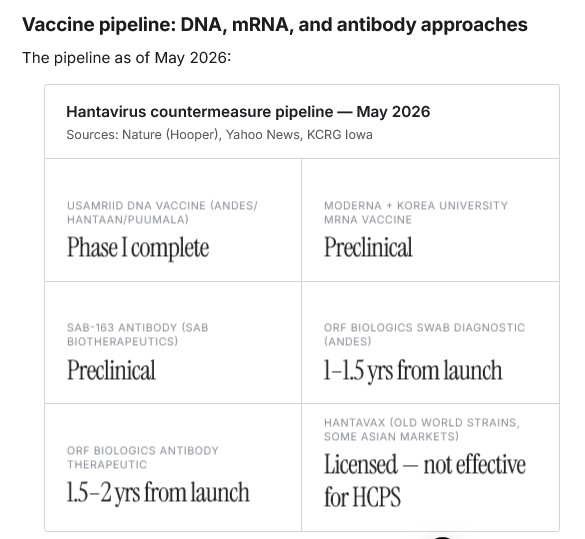
There is, currently, one vaccine against Hantavirus, an “inactivated” injectable called Hantavax (per Wikipedia.) It is only available for use in South Korea. Hantavax is not approved for use in other countries. There are, however, numerous “vaccines” against Hantavirus that are in development. Nicolas Hulscher, MPH, of The McCullough Foundation, notes that thirteen Hantavirus “vaccines” are currently under investigation: https://www.thefocalpoints.com/p/why-ivermectin-and-hydroxychloroquine, “Why Ivermectin and Hydroxychloroquine Could Work for Hantavirus”, 8 May 2026. Per Mr. Hulscher’s 6 May 2026 article on this situation, there are: 6 DNA-based “vaccines” (USAMRIID); 3 mRNA-based “vaccines” (Moderna; Communist China; Canada); 2 “viral vector vaccines” (UK; Canada); 1 “inactivated vaccine” (the Hantavax injectable, South Korea, in use there only); 1 “protein subunit vaccine” (Canada.) Note that the majority of the Hantavirus “vaccines” in development are under the aegis of the US Army (USAMRIID) — which indicates that the Department of War is involved. (https://www.thefocalpoints.com/p/the-vaccine-cartel-and-us-army-are, Nicolas Hulscher, MPH, 6 May 2026.)
The “situational briefing” from neodrop.ai on the current Hantavirus situation is here: https://neodrop.ai/feed/10x3geiL3Sz, “Hantavirus Global Situational Briefing — May 9, 2026.” Below, from the article, is the graphic regarding the “pipeline” of Hantavirus “vaccines” and antivirals in development:
Yours Truly found the USAMRIID Hantavirus “vaccine” clinical trial: https://clinicaltrials.gov/study/NCT04333459, “Safety and Immunogenicity of a Hantaan Virus DNA Vaccine and a Puumala Virus DNA Vaccine, For the Prevention of Hemorrhagic Fever With Renal Syndrome.” Per the Clinical Trials website, NCT04333459 is “Unknown status. Last known status: Recruiting.” The Study Start was 23 August 2021; the Study Completion (Estimated) was to be 31 December 2023. The Puumala virus (PUUV) is another form of Hantavirus; it infects persons in Scandinavia, Russia, and other countries.
BUT — the clinical study NCT03443459, which led this THIS paper: https://pmc.ncbi.nlm.nih.gov/articles/PMC11570633/, “Phase 1 clinical trial of Hantaan and Puumala virus DNA vaccines delivered by needle-free injection”, Jay W Hooper, et al.; 17 November 2024: which study and paper were funded by USAMRIID, and conducted by USAMRIID personnel (Hooper, et al., above): is ACTUALLY a paper about an EARLIER study, NCT02776761 (https://clinicaltrials.gov/study/NCT02776761, “A Single-blind Study to Evaluate the Safety, Tolerability, and Immunogenicity of a Hantaan Puumala Virus DNA Vaccine”), which ended on 27 September 2017. Digging into the details for NCT02776761, it appears that Jay W Hooper owns two Patents for Hantavirus and for Puumala “vaccines”: US8183358B2 and US7217812B2, both of which were assigned to USAMRIID. However, it appears that the Patent for US7217812B2 is “Status: Expired – Lifetime” as of 2 October 2021. If this is the case, why does it appear that this Patent “vaccine” formulation for the Puumala virus used in the clinical trial NCT04333459? This, however, did not stop Mr. Hooper from publishing yet another paper on the same topic: https://academic.oup.com/jid/article/229/1/30/7209758, “Safety and Immunogenicity of an Andes Virus DNA Vaccine by Needle-Free Injection: A Randomized, Controlled Phase I Study”; Jay W Hooper, et al. 28 June 2023. Except that, for this paper, there was also funding via HHS / NIH: Grant number HHS 272201300016I. Which indicates involvement with HHS grants funding and US military funding for biolab work at Fort Detrick.
HOWEVER — and this is a big HOWEVER — there IS a modRNA-based “Hantavirus vaccine” that has gone beyond “development”: a lab-created “vaccine” was PATENTED in 2025 by researchers at the University of Texas, Austin. A “vaccine” that’s ready to be “tested” and either granted an EUA from the FDA, or be “approved” by the FDA. The team of researchers at the University of Texas, Austin, was led by Dr. Jason McLellan, PhD (who may, in Yours Truly’s opinion, be considered as “The Successor to Ralph Baric” in terms of using Gain-of-Function experiments to lab-create viruses and “vaccine” templates.) Dr. McLellan’s Gain-of-Function based research on the COVID-19 virus spike protein was used by Pfizer-BioNTech, by Moderna, and by Novavax, in the development of these companies’ COVID-19 bioweapon “vaccines.” https://en.wikipedia.org/wiki/Jason_McLellan
Yours Truly dug into Dr. McLellan’s modRNA-based Hantavirus “vaccine” Patent. The Patent document is here: https://patents.google.com/patent/US20250127870A1/en, “mRNA Vaccines Against Hantavirus”, published 24 April 2025. The first application for this Patent was filed on 15 September 2022. Current status is “Pending.” The Patent may be summarized as the “invention” of a Gain-of-Function produced, modRNA-platform based “vaccine” that has an artificial “cleavage area” between the Gn and Gc proteins, which proteins are used as the “antigens” for the “vaccine.”
But it goes much deeper than just the above. The “meat” of the descriptions of the multiple ingredients and combinations for this “Hantavirus vaccine” are found along the left side of the Patent Description list (not the “Claims” list, which is on the right side of the document.) The Description list is numbered. Without going too far “into the weeds”, some of the more striking Description items on the list follow. If readers think that the Patent for BNT162b2 describes a “witches’ brew”, this “Hantavirus Vaccine” Patent, in Yours Truly’s’ opinion, goes far beyond (Bolding is mine):
#0019: Adenosine is replaced with N6-methyladenosine (also known as “m6a”) “to evade the host innate immunity and improve the translation.” [of the other ingredients of the “vaccine.”] Adenosine is one of the four “building blocks” of RNA. Please see: https://www.alidabio.com/blog-post/m6a_minor_modification_major_impact/, by Zachary Miles.)
#0033: Confirms the use of the Andes Hantavirus (ANDV) as the basis for the “vaccine.”
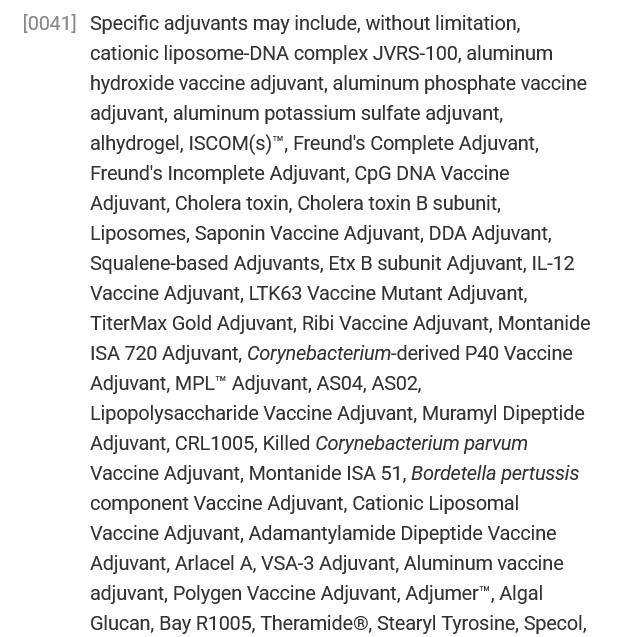
#0041: Formulation list of adjuvants: this list includes dozens of types of adjuvants that can be used in the “Hantavirus vaccine.” One such adjuvant, JVRS-100, is a cationic lipid DNA compound; another adjuvant is Cholera toxin. A screenshot of part of the adjuvants list is below:
#0046 and #0049: The “Hantavirus vaccine” can be used as a “primary” and as a “booster” injectable.
#0047: Routes of administration: can used as an injectable, an intranasal, etc.
#0048: The “Hantavirus vaccine” can contain AZT (zidovudine), used in treating HIV/AIDS.
#0057: This section of the Description is the “justification” for using Gain-of-Function.
#0092: IRES Sequences. This is important. IRES = internal ribosome entry site. Ribosomes are combinations of RNA and proteins. Ribosomes are where protein synthesis occurs in a cell. https://www.genome.gov/genetics-glossary/Ribosome. One of the main goals of the “Hantavirus vaccine” is to “hijack” and change / replace RNA in the body of the person who takes this “vaccine.” In this “Hantavirus vaccine”, some of the IRES Sequences that can be used come from: the Coxsackie virus (CVB3); the Polio virus (PV); Foot and Mouth Disease virus (FMDVD); Simian Immune Deficiency viruses (SIV.)
#00128: from the Pharmaceutical Compositions section: This “Hantavirus vaccine” can be administered to humans / non-human primates / mammals / birds and poultry.
#0143 – 0144: List of lipid nanoparticles (LNPs) that be used in the “vaccine.” Examples of the LNPs that can be used in this “Hantavirus vaccine” include: DODMA (https://www.medchemexpress.com/dodma.html); the description clearly states, “For research use only); and, DOXIL (a form of the anticancer drug, doxorubicin: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/doxil.) There are MULTIPLE other types of LNPs that are listed in sections #0143 – 0144. This also proves that this “Hantavirus vaccine” can contain at least ONE cancer treatment drug.
#0159: This “Hantavirus vaccine” can be used in “Multi-Dose & Repeat Dose Administration.”
>>>>>>>>>>>>>>>>>>>>
Yours Truly turns to the “lockstep, orchestrated gaslighting and fear COVID-19 virus campaign redone as Hantavirus” situation that is unfolding. Please see: https://maninamerica.substack.com/p/cp/197274890, “Hantavirus, Plandemics & Pre-Made Vaccines…Do You See It?”, 11 May 2026. The writer describes the various methods and actors being used to create a new “plandemic” of Hantavirus. Please also see: https://www.thefocalpoints.com/p/virus-in-the-dust-exposing-the-fabricated, “Virus in the Dust: Exposing the Fabricated Contagion of Andes Hantavirus”, Peter A. McCullough, MD, MPH, 10 May 2026.
HOWEVER — and this is another BIG HOWEVER — there is something ELSE in play here: the COVID-19 modRNA bioweapon “vaccines”, the damage / destruction these do to the immune system of the “vaccinated” person, and the documented THOUSANDS of serious adverse side effects and events (including death) from these “vaccines.”
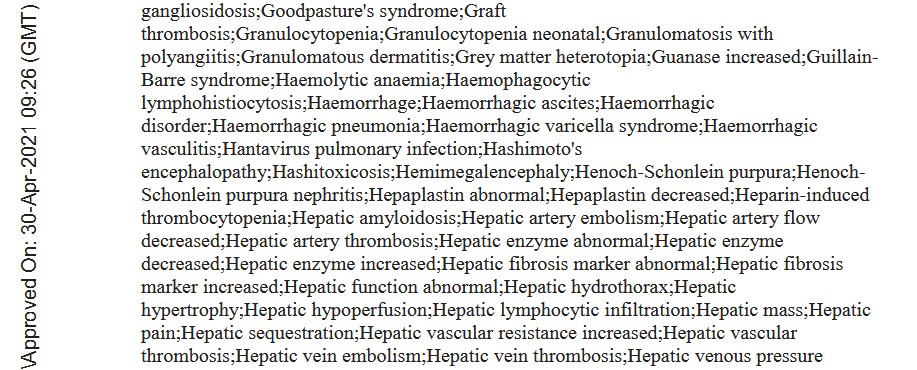
Look at Page 33 (Page 4 of the Appendix 1. List of Adverse Events of Special Interest section) of https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, “BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports“, given by Pfizer-BioNTech to the FDA on 30 April 2021. Please see the screenshot below, part of Page 33:
Does this mean that some BNT162b2 (approved by the FDA under the name COMIRNATY) “vaccinated” person(s) traveled to a place where the Andes Hantavirus (ANDV) is found, stayed there, had close / prolonged contact with infected rat droppings/saliva, or with a person there who was already infected with the Andes Hantavirus, THEN got positive test results for this virus?
OR — does it mean that BNT162b2 has elements of the Andes Hantavirus (ANDV) INCLUDED in the formulation?
OR — does it mean that the husband and wife who were bird-watching in Argentina, in a place where infected rats are prone to be, THEN the husband boards the MV Hondius, shows symptoms of ANDV infection and dies onboard, AND whose wife (who was NOT on board) ALSO becomes ill with ANDV infection and dies onshore, AND who were both COVID-19 “vaccinated” (therefore, their immune systems were badly damaged by said “vaccinations”) — had some kind of “activation” of ANDV infectious elements that were present in their COVID-19 “vaccinated” bodies: an “activation” which occurred while they were bird watching?
This is a non-transmissible organism. 98% synonymous mutations. 1 amino acid is not going to make it transmissible and cross species. The whole story is theatre.
Jikkyleaks thinks that USAMRIID “seeded” the virus on board the MV Hondius. A further discussion of the entire situation, including what Jikkyleaks tweeted, is on Dr. Jessica Rose’s blog: https://jessicar.substack.com/p/is-andv-hanta-natural-spillover-or, “Is ANDV hanta natural spillover or lab design?”, 13 May 2026.
And, WHY did the captain of the MV Hondius permit the body of the husband who DIED of an ANDV infection ON BOARD the vessel to REMAIN on board for TWO WEEKS, until it was offloaded, instead of performing a respectful, but IMMEDIATE, burial at sea? Why did the captain of the MV Hondius permit the body of the German woman who DIED of an ANDV infection CAUGHT ON BOARD to REMAIN on board for EIGHT DAYS? Again, WHY was there no respectful, but IMMEDIATE, burial at sea of this deceased woman’s body? No matter what “morgue-like” conditions these bodies were held in on board the MV Hondius, the corpses potentially exposing MULTIPLE persons on the ship to ANDV infection (think enclosed air-circulation system).
>>>>>>>>>>>>>>>>>>>>
The following articles are, in Yours Truly’s opinion, must-read items. The information in these articles point in the same general direction: there may be a new “plandemic” on the horizon (Andes Hantavirus [ANDV]); combined with “the usual suspects” rushing to, at the same time, implement some combination of COVID-19 disaster-style “lockdowns”, “masking”, “vaccines” development (and potential “mandated vaccination” schemes), plus control of information and coordination with compliant media to gaslight/frighten the general public:
From Dr. Peter A. McCullough, MD, MPH: https://www.thefocalpoints.com/p/source-of-contagion-hantavirus-andv, “Source of Contagion, Hantavirus ANDV, on MV Hondius: Rodent Excreta, Possibly Infected Corpses on Board for 22 Days”, 14 May 2026. There is a video interview with Dr. McCullough in the article.
USAMRIID is involved in the Andes Hantavirus / ANDV situation up to the eyeballs and beyond: https://jonfleetwood.substack.com/p/hantavirus-genome-was-built-from, “Hantavirus Genome Was Built From Human Blood at U.S. Military Biolab Fort Detrick Using Incomplete Computer Assembly and Reference Genome ‘Fill-Ins'”, 13 May 2026.
>>>>>>>>>>>>>>>>>>>>
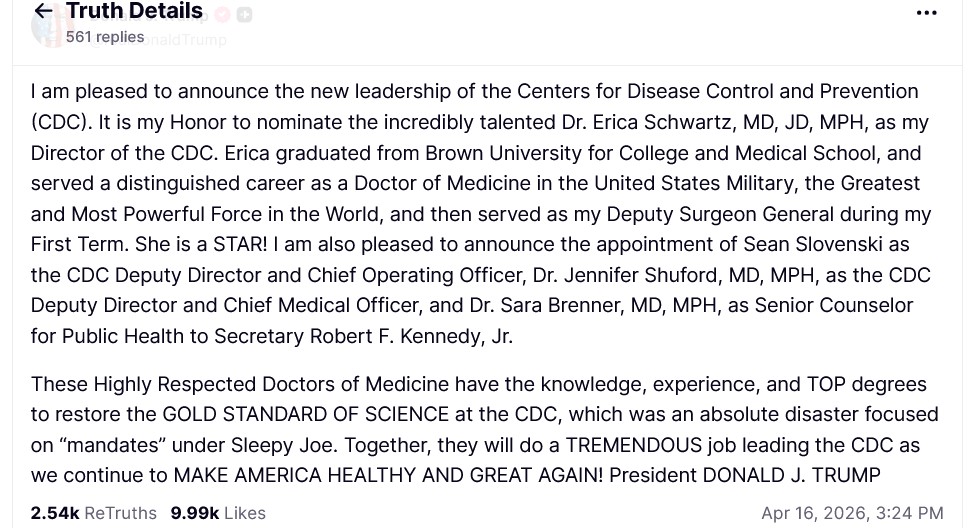
Which brings Yours Truly to one final item: the nomination of Dr. Erica Schwartz, MD, MPH, JD, as the next Director of the CDC. Dr. Schwartz, while serving in the U.S. Coast Guard as a physician, was also instrumental in the enforcement of the “military mandate” for all U.S. military personnel to be COVID-19 “vaccinated.” She is also called “the queen of vaccines.” If confirmed, Dr. Schwartz would be in a position to sign off on a CDC “recommendation” for an Andes Hantavirus (ANDV) and/or Puumala virus (PUUV) “vaccine” to be used on the general public in the United States. (https://www.theqtree.com/2026/05/08/health-friday-5-8-2026-open-thread-two-establishment-medicine-nominees-an-opinion-piece/)
Individual awareness and self-education, in Yours Truly’s opinion, are important aspects to the totality of the Andes Hantavirus (ANDV) / MV Hondius situation.
Peace, Good Energy, Respect: PAVACA
(Intellectual Disclaimer and Notice: With the exception of linked URLs and other items available on the Internet, the ideas and/or opinions in today’s offering are by PAVACA. Credit must be given to PAVACA if ideas and/or opinions in today’s offering are used by other blog writers, podcasters, or in print or social media.)
The header image of a physician consultation for today’s offering is courtesy of Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here: https://www.theqtree.com/2024/09/27/health-friday-open-thread-9-27-2024-another-scientific-paper-under-attack-for-telling-the-truth-about-the-covid-19-vaccines/. Note: AI-generated items in today’s offering will be cited as such. If readers wish to post AI-generated items in today’s discussion thread, they must cite their source. Thank you.
This nomination occurred after Dr. David Weldon withdrew from his nomination for the post; and, after Dr. Susan Monarez, PhD, was let go from her position as CDC director (fewer than six months after being confirmed by the Senate for the job) when it was discovered that she could have been working behind-the-scenes to obstruct the agenda for the agency that HHS Secretary Robert F. Kennedy, Jr., was attempting to implement.
Another take on the nomination of Dr. Schwartz is here: https://tdefender.substack.com/cp/194572403, ” ‘Cause for Real Concern: MAHA Activists Criticize Trump’s Pick to Lead CDC’ “, Michael Devradakis, PhD, 17 April 2026. It appears that there may be a combination of several factors involved in the nomination of Dr. Schwartz: among them, a further “reining in” of Sec. Kennedy, Jr.’s HHS agenda: also, a potential attempt to weaken and/or divide the groundswell of dissatisfaction with the COVID-19 bioweapon “vaccines”, along with the growing recognition of the documented dangers and deaths that these “vaccines” induce.
Yet other aspects regarding the nomination are presented by Dr. Peter A. McCullough, here: https://www.thefocalpoints.com/p/the-deep-states-medical-playbook, 27 April 2026. This post is a combination of video interview with Dr. McCullough by Emerald Robinson, and an AI-generated text summary. Dr. McCullough argues that if confirmed, Dr. Erica Schwartz could either be “the insider” who can lead the CDC into meaningful and positive change; or, she could be a “Trojan horse” of betrayal of Make American Healthy Again.
The questions arise: Why would HHS Sec. Kennedy, Jr., support “the queen of mandating vaccines” (Dr. Erica Schwartz, MD, MPH, JD) as the next Director of the CDC? Is this the same HHS Sec. Kennedy, Jr., who was sworn into the job last year?
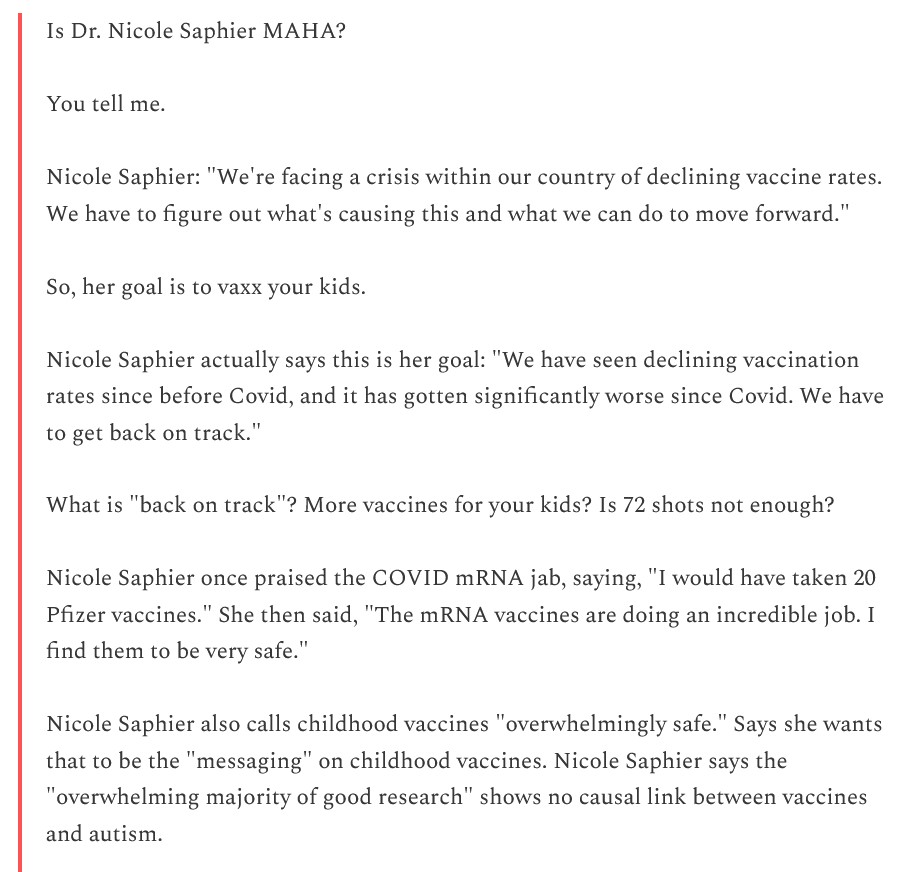
Dr. Saphier is another experienced physician, with credits at the Mayo Clinic and at the Memorial Sloan Kettering Cancer Center. Which sounds fine, except for the fact that Dr. Saphieris also a fierce proponent of the COVID-19 bioweapon “vaccines” — and of childhood “vaccination” in general:https://www.2ndsmartestguyintheworld.com/p/mixed-bag-maha-president-trump-nominates, 2 May 2026:
Jon Fleetwood weighs in on the nomination of Dr. Saphier: https://jonfleetwood.substack.com/p/trump-surgeon-general-pick-dr-saphier, “Trump Surgeon General Pick Repeatedly Instructed Americans to Take COVID-19 Shot”, 1 May 2026. In his article, Mr. Fleetwood traces Dr. Saphier’s advocacy of the COVID-19 bioweapon “vaccines.” A portion of his concluding remarks is below:
Yours Truly would point out the following required reading for Dr. Schwartz and Dr. Saphier: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, “BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports“, given by Pfizer-BioNTech to the FDA on 30 April 2021. The section Appendix 1. List of Adverse Events of Special Interest, which being on Page 30 of the report, lists the 1,291 types of conditions (including Death) that were induced by persons receiving BNT162b2 (now called COMIRNATY) between 11 December 2020 (the date that the FDA granted the initial EUA for use of BNT162b2 in the United States), and 28 February 2021 — a time frame of fewer than three months of market use of the “vaccine.”
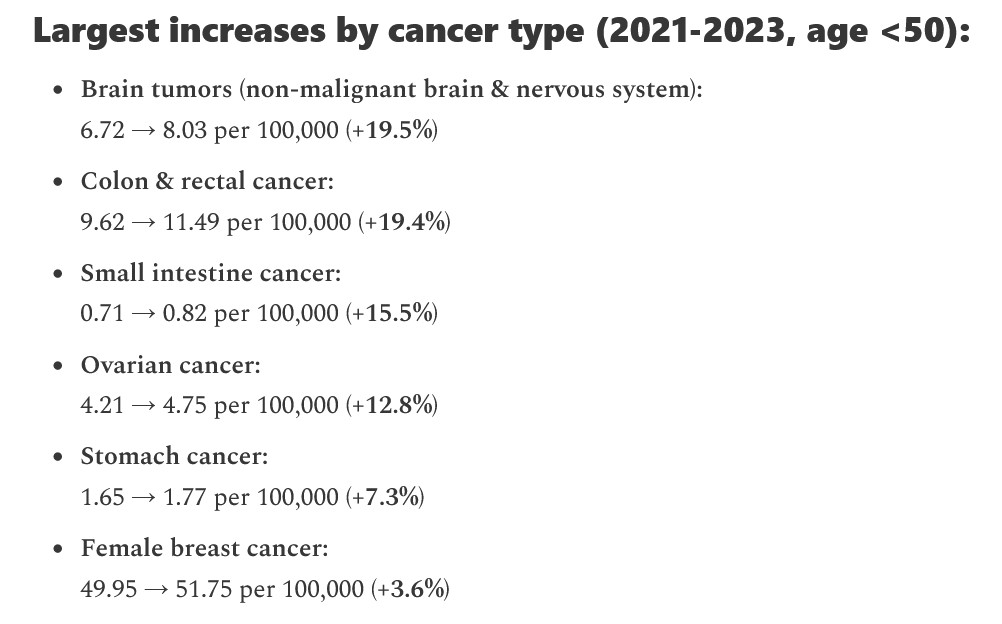
Another set of data points that needs to be required reading for Dr. Schwartz and Dr. Saphier: https://x.com/NicHulscher/status/2047483961354432956, 23 April 2026. Mr. Hulscher points out that cancers for persons under age 50 in the United States have risen, in the aggregate, 6.4% from 2021 (the year of the COVID-19 bioweapon “vaccines” rollout) and 2023. He discusses the situation in depth, here: https://www.thefocalpoints.com/p/breaking-us-government-cancer-data, 23 April 2026.
What is going on here regarding the nominations of two Establishment Medicine stalwarts, both of whom are strong proponents of “vaccination”, including COVID-19 bioweapon “vaccination”? Why is HHS Sec. Kennedy, Jr., supporting the nomination of Dr. Nicole Saphier? What “signals” are being given? Are these nominations another “outcome” of the “ruling” by Federal Judge Brian E. Murphy earlier this year, which reversed the new CDC childhood / adolescent immunization schedule (a new schedule that reduced the number and types of “vaccines” that would be “recommended”) — and re-instated the former CDC immunization schedule of 72 “vaccines” injections to be given to children from the day of birth, up to 18 years of age? Are these nominations to bring back “business as usual” / “the good old days” at the CDC and at the Surgeon General’s office?
The header image for today’s offering is courtesy of Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated content in today’s offering will be cited as such. If readers with to post AI-generated content in today’s discussion thread, they must cite their source. Thank you.
>>>>>>>>>>>>>>>>>>>>
Today is a “remembrance day” for Yours Truly. Twenty years ago today — 1 May 2006 — my late father suffered a massive stroke, the complications from which eventually took his life two months later. Yours Truly was the one who found him on the floor, hours after he had the stroke. Yours Truly spent the next two months at his side, going through Hell with him as he fought like a lion to regain some kind of health, ability to walk, to feed himself…while, at the same time, Yours Truly’s own husband was just starting to recuperate from the massive fall that he himself suffered a few months prior, in which he fractured his pelvis, broke numerous ribs, had a concussion, and, after days in the hospital, was being cared for 24/7 at home by rotations of private-duty CNAs and RNs. My father was 89 years old in May 2006; my husband was 96 years old.
My father was a Registered Pharmacist for 55 years at the time of his stroke: 45 years in practice; then, after his retirement, 10 more years in keeping his license current. He was working on Continuing Education credits for his upcoming license renewal when he was stricken. He was able to “dictate” answers to a few of the CE questions while at the rehab facility, until he lost the power of speech. When he died, he was still a Registered Pharmacist. His customers loved him. Hundreds of them came to his viewing at the funeral home in Pittsburgh — on the same street where he had kept his pharmacy for so many years.
My father hoped that Yours Truly would go into Pharmacy. Instead, I went into music. My father never said a word about any disappointment he may have felt. He would come home from work and sit on the living room sofa, listening to me practicing Beethoven and Chopin and Brahms. I think about my father when I research and write the Health Friday posts. Perhaps he is looking down from Heaven, where I believe he is with my mother, and saying, “You done good, Chick”, which was his humorous “stamp of approval.”
Some of the pain; some of the “what did I miss?”; some of the grief — still remain with Yours Truly, twenty years after my father’s death. The intensity has lessened, but grief never really leaves. Grief must, instead, be integrated into the life of the survivor. It is integrated as a combination of memory, acceptance, and resolve to move on in the healthiest way possible for the body, mind, and spirit. The integration is not quick or simple. It is a process. The “timeline” is different for each survivor. It is not a straight line. It is not “defined” in terms of weeks, months, or years. There are curves; there are twists and turns; there are times of feeling “stuck”; there are times of anger, intense regret, and deep, searing sorrow. Counseling can help; books on grieving can help; trusted friends and family can help; self-care can help; and more. But, ultimately, the integration process is carried on inside the survivor. It is organic. I feel that this inside, organic process is, at the deepest level, anchored in belief in a Higher Power — a Supreme Being — the Almighty God.
Samuel Regis Lewis, Sr., R.Ph. 1916-2006. Rest easy, Daddy. Stay with Mother. Be happy and at Peace in the next world. Love you. Miss you. Thank you — Thank you.
>>>>>>>>>>>>>>>>>>>>
Some Interesting Links:
Multiple types of cancer diagnoses have increased by over 6% since the COVID-19 modRNA bioweapon “vaccines” were rolled out in January 2021: https://www.thefocalpoints.com/p/breaking-us-government-cancer-data, “BREAKING: U.S. Government Cancer Data Shows Early-Onset Cancers Surged 6.4% From 2021 to 2023”, Nicolas Hulscher, MPH, 23 April 2026. The figures are from National Cancer Institute data. The aggregate increase for all cancers diagnosed in persons under age 50 is 6.4%. Below is an image of the various cancers increase breakdown:
>>>>>>>>>>>>>>>>>>>>
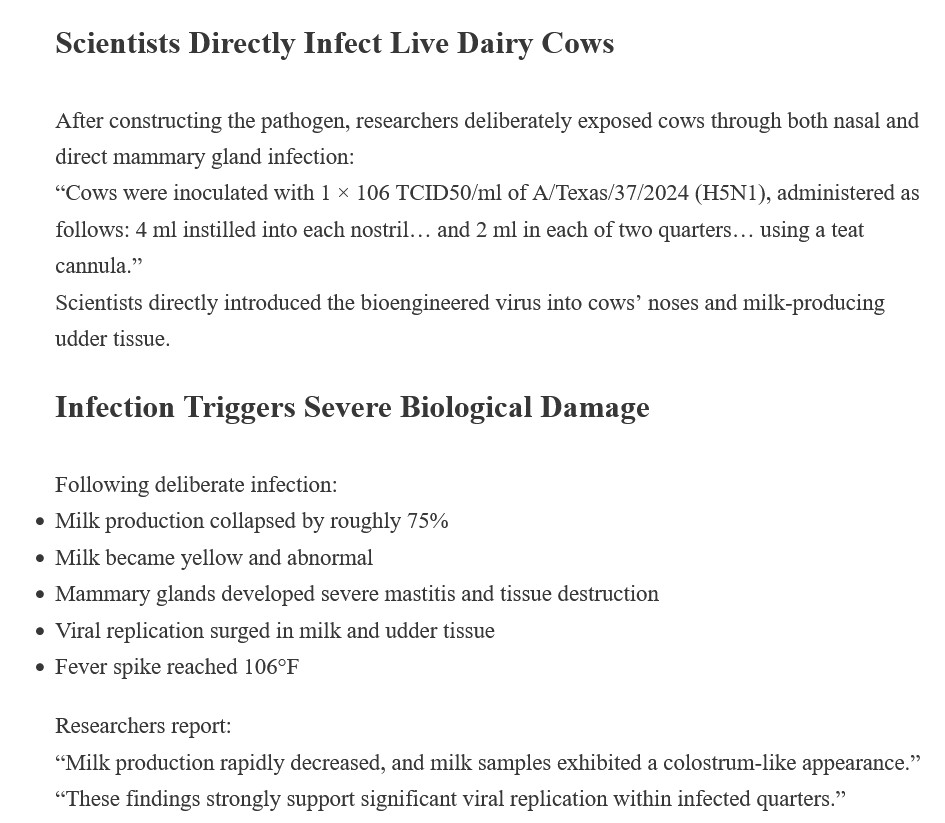
The United States government funded a recent Gain-of-Function experiment at the University of Georgia (Athens, GA) that created a dangerous, highly pathogenic H5N1 virus strain which was deliberately given to Jersey cows: https://jonfleetwood.substack.com/p/taxpayer-funded-scientists-create, “Taxpayer-Funded Scientists Create Human Bird Flu Virus in Georgia BSL-3 Lab That Successfully Crosses Species”, Jon Fleetwood, 26 April 2026. Please see the image from this article, below:
The paper published about this experiment is here: https://doi.org/10.1038/s44433-025-00002-5, “Experimental infection and viral pathogenesis of a human isolate of H5N1 highly pathogenic avian influenza strain in Jersey cows”, Flavio Cargnin Faccin, et al. 26 March 2026.
Note that this experiment was conducted in 2025, after President Donald Trump 47 assumed office.
>>>>>>>>>>>>>>>>>>>>
Dr. Peter A. McCullough weighs in on the nomination of Dr. Erica Schwartz as the new Director of the CDC, and more: https://www.thefocalpoints.com/p/the-deep-state-medical-playbook, 27 April 2026. This is a video interview by Emerald Robinson with Dr. McCullough and an AI-generated “text summary” of the interview in the above link. Two screenshots from the “summary” are below:
Note the use of “might grant here the necessary credibility…”, and “provided she shifts focus…” In Yours Truly’s opinion, if Dr. Schwartz is confirmed, it will represent a “watershed” situation for the CDC (and, indeed, for HHS) — either to face up to the truth regarding the need for real reform within the CDC (and the HHS), and to face up to the truth regarding the dangers and deadliness of the COVID-19 bioweapon “vaccines”; or, it will signal the return to “the good old days” at the CDC (and the HHS), with further consolidated control by Establishment Medicine and Big Pharma.
Note that Johns Hopkins is working on “advancing patents” for Ivermectin and for mebendazole.
What does this mean? Since a Patent cannot be granted for something found in nature, Johns Hopkins will have to “add” or “subtract” some element(s) from Ivermectin and from mebendazole, thus “inventing” a “newly isolated material.” https://law.stackexchange.com/questions/77228/can-you-patent-natural-things. It means that Johns Hopkins (and/or the entity that Johns Hopkins “assigns” the Patent to) will own the “newly isolated material.” It also means that the item can be used for making money for the Patent owners / assignee(s). It also means control of access, of availability, of manufacture, and of patient use. It also means that the use of the “newly isolated material” patented Ivermectin and mebendazole will be under the control of healthcare professionals who prescribe it for use in cancer treatment. It also means that the “newly isolated material” patented Ivermectin and mebendazole can be used as an ADJUNCT treatment for cancer, alongside conventional Establishment Medicine treatments such as radiation, surgery, and/or chemotherapy. It also means that the “newly isolated material” patented Ivermectin and mebendazole will become a “cancer treatment drug”, costing much more than the current Ivermectin and mebendazole which are non-patented. It also means that private insurance companies and/or Medicare and Medicaid can choose to either cover, or to not cover, treatment by the “newly isolated material” patented Ivermectin and mebendazole.
>>>>>>>>>>>>>>>>>>>>
The scientist who invented the “template” virus for COVID-19 — Dr. Ralph Baric, PhD, of the University of North Carolina, Chapel Hill, is finally being unmasked and brought to account:
EXCLUSIVE: NIH has removed virologist Ralph Baric from all his grants; UNC placed Baric on leave.
Senior HHS officials says UNC was complicit in starting the COVID pandemic.
“Baric designed the gun,” he said. “But the Chinese built it, and then they pulled the trigger.”… pic.twitter.com/CNvo3buLkw
This occurred immediately AFTER Dr. David Morens (a deputy of Dr. Anthony Fauci when Dr. Fauci was Director of NIAID) was indicted for his activities at NIAID in suppressing release of any information that would lead to the truth behind the real origins of the COVID-19 virus: https://www.2ndsmartestguyintheworld.com/p/psyop-19-justice-incoming-first-criminal, “PSYOP-19 JUSTICE INCOMING: First Criminal Indictment Against Senior COVID Official & Pressure Mounting on DOJ to Prosecute Dr. Fauci”, 30 April 2026. The five-year Statute of Limitations about lying to Congress runs out for Dr. Anthony Fauci on 11 May 2026. It is impossible that HHS Sec. Kennedy, Jr., does NOT know this. Is the United States government going to let the Statute of Limitations on Dr. Fauci run out on 11 May 2026? https://www.theburningplatform.com/2026/04/30/will-they-let-the-clock-run-out-on-charging-this-mass-murderer/. Yours Truly’s opinion — that possibility needs to be faced.
>>>>>>>>>>>>>>>>>>>>
The FDA deliberately “masked” (suppressed) 25 safety signals found in VAERS reports of COVID-19 bioweapon “vaccine”-induced health conditions AND deaths between March 2021 and July 2021: https://www.thefocalpoints.com/p/breaking-senate-investigation-finds-f15, “BREAKING: Senate Investigation Finds FDA Officials Covered-Up 25 COVID Shot Safety Signals”, Nicolas Hulscher, MPH, 29 April 2026. Dr. Ana Szarfman, an FDA employee, created a program that would basically sort out and identify COVID-19 “vaccine”-induced safety signals. Dr. Szarfman was eventually told by her superiors to “cease and desist” her work — the agency was afraid that the truth becoming known would “feed into vaccine misinformation.”Dr. Janet Woodcock was the Acting Director of the FDA in 2021. She must also be indicted and prosecuted.
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA, A modRNA, AN saRNA, OR A taRNA PRODUCT, OF ANY KIND.
THERE MUST BE MUCH MORE RESEARCH INTO THESE TECHNOLOGIES. THE RESULTS MUST BE FULLY ANALYZED. THE DATA MUST BE MADE AVAILABLE TO THE PUBLIC.
ALL COVID-19 BIOWEAPON “VACCINES” MUST BE REMOVED FROM THE MARKET AND FROM USE. NOW.
THOSE WHO LAB-CREATED THE COVID-19 BIOWEAPON VIRUS ITSELF, AND THE COVID-19 BIOWEAPON VACCINES, MUST NOW BE BROUGHT TO ACCOUNT.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Disclaimer and Notice: Except for linked URLs and other items that are available on the Internet, the ideas and/or opinions in today’s offering are by PAVACA. Credit must be given to PAVACA if the ideas and/or opinions in today’s offering are used by any other blog writer, by podcasters, or in print or social media.)
The vintage image of a vaccination record from 1867 for today’s offering header is courtesy of iStock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; theRules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated items in today’s offering will be cited as such. If readers wish to post AI-generated content in today’s discussion thread, they must cite their source. Thank you.
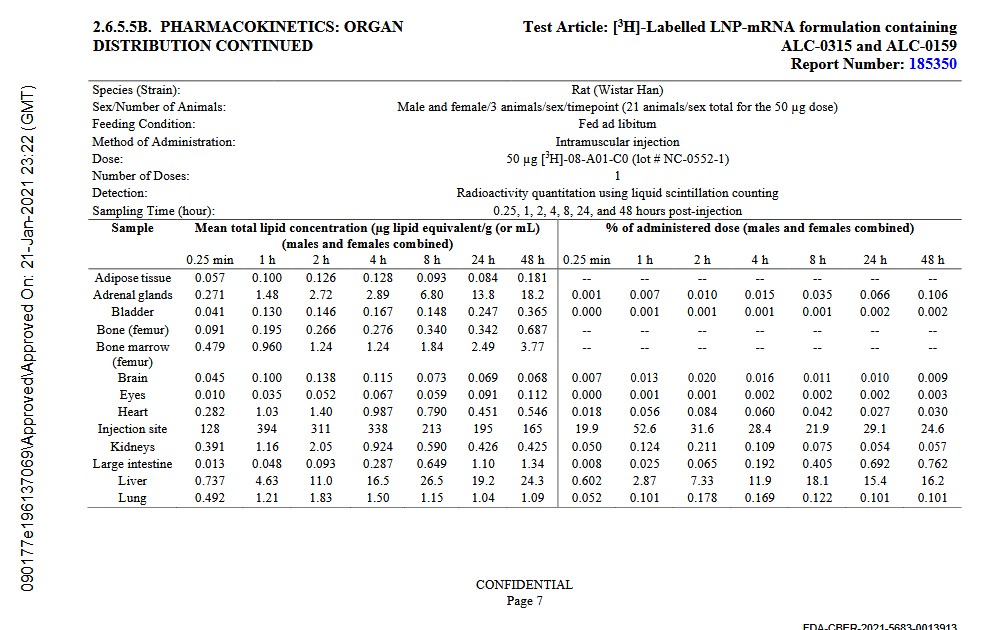
Today’s offering begins here: https://icandecide.org/wp-content/uploads/2022/03/125742_S1_M2_26_pharmkin-tabulated-summary.pdf, “MODULE 2.6.5 PHARMACOKINETICS TABULATED SUMMARY“, FDA Approved on 21 January 2021 at 23:22 GMT (Greenwich Mean Time.) This is the report regarding biodistribution data of the Pfizer-BioNTech modRNA COVID-19 bioweapon “vaccine”, BNT162b2, for which the FDA had granted the initial EUA (Emergency Use Authorization) for use in the United States on 11 December 2020. The experiments performed by Pfizer-BioNTech to produce the report, using BNT162b2 injections, were conducted on Wistar Han lab rats, Sprague Dawley lab rats, Cynomologus monkeys, and human liver microsomes and liver fractions. Data were extracted from in vivo and from in vitro results. The formulation of BNT162b2 used in the experiments was the same as that which was granted the FDA Emergency Use Authorization of 11 December 2020 for use on human beings in the United States.
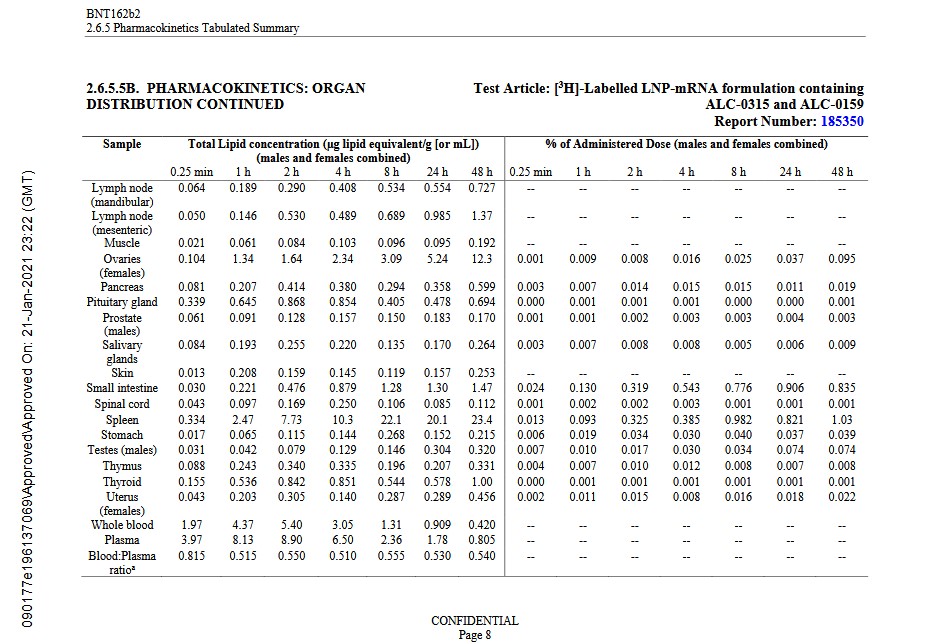
Yours Truly presents images of page 7 and page 8 of this report:
Note: the above data are the results from the injections given to the Wistar Han lab rats. Note also the accumulations of the lipid nanoparticles (LNPs), ALC-0159 and ALC-0315, used in the BNT162b2 formulation. Again, this is the same formulation that was granted the initial FDA Emergency Use Authorization on 11 December 2020, for BNT162b2 to be used on human beings in the United States. LNPs are the tiny fat molecules-based, lab-created “delivery system” that encases the “vaccine” ingredients to protect them from being detected and eliminated by the natural immune system of the body. Instead, the LNPs facilitate the entry of the “vaccine” into every cell of the body. Look at the highest accumulation amounts:
Adrenal Glands: 18.2. The adrenal glands release hormones, such as, adrenaline, directly into the bloodstream. These glands are crucial in the proper function of blood pressure and the body’s stress response. https://my.clevelandclinic.org/health/body/23005-adrenal-glands
Injection Site: 165. The injection of COMIRNATY into the arm of a human being results in the following: The body immediately sends “alarm signals” that there is an “enemy invader”, and starts the natural immune system process of fighting it / eliminating it. This is manifested in several ways, including: pain at the injection site, and/or a “rash” at the injection site. However, these immediate reactions can also indicate early-warning signals of anaphylactic shock — and must be closely monitored. Establishment Medicine explains this away by, first, stating that this reaction is “rare”, then proceeding to minimize the situation: https://ubiehealth.com/doctors-note/rash-after-covid-vaccine-causes-serious-warning-49121exp1, “Why do some people get a rash after the COVID vaccine and when is it serious?”, Yoshinori Abe, MD, 17 December 2025. This situation is called “COVID Arm.” In fact, Establishment Medicine minimizes “COVID Arm” reaction even if it occurs DAYS or a WEEK after “vaccination”: https://medlineplus.gov/ency/imagepages/19970.htm. “Arm Rash After COVID-19 Vaccination”, updated by Linda J. Vorvick MD, 1 January 2025.)
Ovaries: 12.3. The female ovaries make and release eggs for fertilization. They also produce hormones. At birth, a female has all the eggs that she will ever have. The ovaries constantly “communicate” with the brain. https://axiawh.com/resources/5-things-you-didnt-know-about-your-ovaries/
Spleen: 23.4. The spleen creates white blood cells and stores red blood cells. It helps to regulate blood platelets (which assists in proper blood clotting.) It filters out old or damaged blood cells. https://www.healthline.com/health/what-does-the-spleen-do
The above report, in Yours Truly’s opinion, needs to be required reading for any healthcare professional who is still “recommending”, let alone administering, COMIRNATY. And, in case a healthcare professional raises objections, such as, “The new COMIRNATY formula is different”, the facts that ALC-0159, ALC-0315, N1-Methylpseudouridine (all which were in the original BNT162b2 formulation), and the S1 spike protein (that can be traced back to the original Wuhan Hu1 SARS-CoV-2 strain) are ingredients in the “2025-2026 COMIRMATY” version of the injectable.
There is a reason behind why the accumulations of ALC-0159 and ALC-0315 are so high for the above body areas and organs: these lipid nanoparticles ensure that the ingredients and mechanisms of COMIRNATY enter these areas and organs: with the result that said areas and organs are interfered with, and/or damaged, and/or that the body’s ability to properly use them is destroyed. Example: over 60% of the lifetime supply of a female lab rat’s eggs are either damaged or destroyed due to it being “vaccinated” with COMIRNATY: https://www.thefocalpoints.com/p/breaking-covid-19-mrna-shots-destroy, “BREAKING: COVID-19 mRNA Shots Destroy Over 60% of Female Non-Renewable Egg Supply”, Nicolas Hulscher, 9 May 2025. If this is what happens with female Wistar lab rats being injected with these “vaccines”, the potential for damage to human female eggs is ALSO THERE: and, in fact, the Manniche, et al., study demonstrates this: https://www.preprints.org/manuscript/202504.2487/v1, “Rates of Successful Conceptions According to COVID-19 Vaccination Status: Data from the Czech Republic”, Vibeke Manniche, et al., 29 April 2025. Note: this paper is a preprint — therefore, it can be Removed, Retracted, or Withdrawn at any time. Yours Truly urges interested readers to download or otherwise archive this paper.
Before leaving the discussion of ALC-0159 and ALC-0315, please see the following images from the MSDS Safety Sheets for these lipid nanoparticles, below. First, from https://cdn.caymanchemical.com/cdn/msds/34336m.pdf, for ALC-0159:
Note that both compounds are for research only. In fact, both compounds rate as a carcinogen (ethanol content.) In particular, the Cayman Chemcial MSDS for ALC-0315 reads like a textbook example of a very dangerous compound.
**** Note from the images of Page 7 and Page 8 above, that BNT162b2 crosses the Blood-Brain Barrier, as seen in the accumulation data images above: the “vaccine” accumulates in the Brain and in the Pituitary Gland. In addition, there is BNT162b2 accumulation in the Skin and in the Kidneys — this indicates that the “vaccine” ingredients can be “shed” from the skin and/or excreted via the kidneys into urine.
The Appendix 1: List of Adverse Events of Special Interest section of this report about BNT162b2, also given to the FDA by Pfizer-BioNTech (April 2021) has the reports listings of over 1,200 serious / fatal side effects induced by this “vaccine.” The report is found here: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, “5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021“, FDA date-stamped 30 April 2021 at 09:26 GMT. This, in Yours Truly’s opinion, also needs to be required reading for any healthcare professional who is still “recommending”, let alone administering, COMIRNATY.
The COVID-19 bioweapon “vaccines” are actually gene-altering injectable therapies: they are not, strictly speaking, vaccines. Please see: https://academic,oup.com/intimm/article/33/10/521/6194108, “Development of COVID-19 vaccines utilizing gene therapy technology”, Hironori Nakagami, 27 March 2021. Every single person who has ever taken an injection of COMIRNATY has had a gene-altering therapy “cocktail” (under the guise of “it’s a vaccine”) injected into their body: something that “vaccinated” persons were never told about, nor for which they never explicitly granted permission to have put into their body.
>>>>>>>>>>>>>>>>>>>>>>>>
HHS Secretary Robert F. Kennedy, Jr., is not being allowed to do his job — and, in fact, to quote another blog writer, he is being “muzzled.” The COVID-19 bioweapon “vaccines” have been, via the American Academy of Pediatrics lawsuit and subsequent “ruling” by Federal Judge Brian E. Murphy, are now fully back into the CDC Childhood Immunization Schedule. The new nominee to head the CDC, Dr. Erica Schwartz, is an Establishment Medicine “vaccine” proponent: https://aaronsiri.substack.com/p/the-queen-of-mandating-vaccines, 18 April 2026. A screenshot from this article is below:
RFK Jr. drops the truth bomb on the COVID era: “They had to DESTROY ivermectin and hydroxychloroquine… because if they admitted it worked for ANYONE, the entire $200 BILLION vaccine enterprise would have COLLAPSED.”pic.twitter.com/rEEjSXrYPf
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA, A modRNA, AN saRNA, OR A taRNA PRODUCT OF ANY KIND.
THERE MUST BE MUCH MORE RESEARCH INTO THESE DELIVERY PLATFORMS, WITH EXTENSIVE TESTING AND DATA ANALYSES, AND WITH THE RESULTS BEING MADE PUBLIC.
THE COVID-19 BIOWEAPON “VACCINES” (GENE-THERAPY INJECTIONS) — ALL OF THEM — MUST BE REMOVED FROM THE MARKET AND FROM USE IN THE UNITED STATES. NOW.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Disclaimer and Notice: Except for URLs and other items that are available on the Internet, the ideas and/or opinions in today’s offering are by PAVACA. Proper credit must be given to PAVACA for ideas and/or opinions in today’s offering are used by other blog writers, by podcasters, or in print or social media.)
The vintage image of mass vaccination for today’s offering is courtesy of Google Images.
Health Friday is a series on information regarding Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated items in today’s offering, if any, will be cited as such. If readers wish to post AI-generated items in today’s discussion thread, they must cite their source. Thank you.
Yours Truly begins here: https://jonfleetwood.substack.com/p/hhs-funds-gain-of-function-influenzacovid, “HHS Funds Gain-of-Function Influenza — COVID ‘Frankenvirus’ Combining Influenza Entry With SARS-CoV-2 Human Cell – Binding Domain”, 10 April 2026. Two screenshots regarding this are below: the first, from the Fleetwood article; the second, from the paper itself (published December 2025). Thanks to Mr. Fleetwood for this information:
By the way, NIH grant P01-AI165075 (going to Rockefeller University, New York) has multiple “permutations” in the https://reporter.nih.gov/ listing. **** The “permutation” that helped to fund the paper below (cited in the Fleetwood article) is 3P01AI165075 – 01S1, Sub-Project ID: 6568, awarding entity NIAID, total funding: $983,100. (And this is only ONE “permutation” of P01-AI165075.)
**** What this lab-created “combo virus”, called X31 H3 S-RBD in the paper, contains:
The RBD (Receptor Binding Domain) from the Wuhan Hu1 SARS-CoV-2 virus (the original COVID-19 virus); plus
Seven other viral RNAs (vRNAs) from the H1N1 (Influenza A) Puerto Rico/1/1934 strain (PR8)
The Abstract of this paper is below. It is a clear statement that Gain-of-Function was used to lab-create this “combo virus” (lines 28 – 35):
Let’s take a look at the involvement with the Chinese Academy of Medical Sciences (CAMS) in the study that produced this paper. The paper states that Tiong Kit Tan, of the Chinese Academy of Sciences – Oxford Institute, Nuffield Department of Medicine, University of Oxford, is one of the researchers/co-authors. CAMS is a collaborator with the Chinese Communist People’s Liberation Army (PLA.) CAMS is one of the “Top 5” domestic (Chinese-based) collaborators with the PLA. Please see: https://www.nature.com/nature-index/institution-outputs/china/people-s-liberation-army-pla/555c2052140ba014648b456b; scroll down the page to the list of “Domestic Collaborators.”
Further down the page, there is the list of “International Collaborators” with the PLA. It is interesting to note that NUS (National University of Singapore) is ranked as Number One here. It is also interesting to note that NUS has a large medical school that is a “satellite” of Duke University (Chapel Hill, North Carolina;https://www.duke-nus.edu.sg.)
The question arises: How much research data, analyses, lab samples, and more, from these “international collaborators” with the Chinese Academy of Medical Sciences, wind up in laboratories run by the People’s Liberation Army in hospitals and universities throughout Communist China?
The NIH grant that helped to fund Dr. Kawaoka’s work for the above cited paper is 75N93021C00014. The grant contract information is found here: https://www.highergov.com/contract/759321C00014/. An image of the Government Description of this grant, from the website, is below:
Note that sentence about, “Includes international and domestic basic and clinical influenza research…” — in other words, covering “collaborators” like CAMS. Note that “studies of viral evolution, transmission, and immune responses in animal models and humans” covers Gain-of-Function work.
CEIRR stands for Centers of Excellence for Influenza Research and Response. The website description of this research division of NIAID is here: https://www.niaid.nih.gov/research/centers-excellence-influenza-research-response. Scroll down the page to “Main Areas of Focus” to this statement: “To support projects to determine how influenza viruses evolve, adapt and transmit between humans and at interspecies interfaces”. This is “code” for supporting Gain-of-Function research on influenza viruses. There are multiple “permutations” of NIH grant 75N93021C00014 listed at https://reporter.nih.gov/search/6vlkhZH5302zeKPiGnsO5g/projects, most of which were awarded to the Icahn School of Medicine at Mount Sinai, New York (one of the CEIRR main hubs of research.)
>>>>>>>>>>>>>>>>>>>>
Yours Truly turns to what might be, in her opinion, called a “permutation” of Gain-of-Function research: experiments on human beings to further a Patent invention.
The Patent in question is: US11369675B2, “Broadly protective inactivated influenza virus vaccine”, held by Dr. Jeffery Taubenberger, MD, Acting Director of NIAID. The Patent declaration is found here: https://patents.google.com/patent/US11369675B2/en. The application for the Patent was filed on 12 October 2020; the Patent was granted on 28 June 2022; the “Adjusted expiration” date of the Patent is 24 January 2039; and, the Patent was assigned to the Department of Health and Human Services (HHS.) Dr. Taubenberger, during this timeline, was an employee of HHS, before he became Acting Director of NIAID. He, in fact, is a career HHS (NIH) employee.
It appears that Dr. Taubenberger is working to further the Patent regarding the development of an intranasal “universal influenza vaccine.” His most recent published paper in this regard is here: https://pmc.ncbi.nlm.nih.gov/articles/PMC12375958/S#23, “Nasal and systemic immune responses correlate with viral shedding after influenza challenge in people with complex preexisting immunity”, Jeffery Taubenberger, et al., 6 August 2025. This paper describes a very small study of 74 persons (originally 80 persons) that was conducted in 2019 per the cited paper above (NCT01971255.) However, the ACTUAL study dates of NCT01971255, per https://clinicaltrials.gov/study/NCT01971255, indicate a timeframe between September 2013 and September 2015. In addition, the referenced paper number 11 in the cited paper above describes the same experimental study, but via a paper published about it in 2024 (https://pmc.ncbi.nlm.nih.gov/article/PMC10865821/, “Mucosal correlates of protection after influenza viral challenge of vaccinated and unvaccinated healthy volunteers”, Jeffery Taubenberger, et al., 9 January 2024.) This, to Yours Truly, raises questions regarding the timing of the publishing of these papers, since the actual study was conducted over 10 years ago. What goes on here?
The bottom lines of NCT10971255: there were 80 enrolled study subjects; half were vaccinated with a licensed influenza “vaccine”; half were unvaccinated; ALL subjects were then given an intranasal LIVE VIRUS H1N1 (swine flu), called Ca/04/2009/H1N1r Challenge Virus; ALL subjects were then tested numerous times via a middle turbinate nasal swab (this means that the swab samples were taken from well inside the upper nasal cavity each time); apparently, ALL subjects became ill with flu symptoms, some of which were severe; 6 study subjects withdrew for various reasons; all testing using the “intranasal challenge virus” was performed at the NIH Clinical Center in Bethesda, Maryland; the study subjects were brought there for the “challenge” (and likely had to stay there or in the immediate area, as they were assessed daily for a minimum of 9 days.)
Dr. Taubenberger is the recipient of NIAID research funding related to Avian Influenza viruses, his “universal influenza vaccine”, and to the SARS-CoV-2 virus — in the 2025 fiscal year, among other years. However, 2025 is the year in which Dr. Taubenberger became the Acting Director of NIAID. The “umbrella grant” prefix number is either 1ZIAAI00 or 1ZIAAI000, each followed with the suffix number: for example, 1ZIAAI001372-03, “Universal Influenza Vaccine Development”, for $2,153,677. This grant, as at least one other per https://reporter.nih.gov/ (search: Jeffery Taubenberger), lists NO contact data; NO Project Start Date; NO DUNS number; NO Budget End Date; among other lack of public information. What goes on here? Is Dr. Taubenberger perhaps granting NIAID research funds to himself?
>>>>>>>>>>>>>>>>>>>>
Finally, is appears that HHS Sec. Robert F. Kennedy, Jr., is going to start a podcast:
Sec. Kennedy, Jr., states that he will “…ask the questions and lift the taboos and expose the hypocrisy and the conflicts and the corruption…We’re going to follow the evidence wherever it leads, and we’re going to name the names of the forces that obstruct the paths to public health.”
All well and good. However — will Sec. Kennedy, Jr., “name the names”, such as: the person who invented the SARS-CoV-2 virus itself — Dr. Ralph Baric of the University of North Carolina, Chapel Hill? Such as, the person who could have stopped the entire COVID-19 “vaccine” disaster in the United States in December 2020, but who instead signed off on the CDC’s “recommendation” for the use of Pfizer-BioNTech’s modRNA COVID-19 bioweapon “vaccine”, BNT162b2, without any further investigation — Dr. Robert Redfield, then-Director of the CDC? Such as, the person who was responsible for the NIAID funding that produced the SARS-CoV-2 virus itself — Dr. Anthony Fauci, former NIAID Director? Such as, the USAMRIID personnel responsible for working with PfizerUSA (Pfizer-BioNTech) in the development of BNT162b2? Will Sec. Kennedy, Jr., “name the names” of the products that, by far, have obstructed, and continue to obstruct, “the paths to public health” — the COVID-19 bioweapon “vaccines”?
ALL GAIN-OF-FUNCTION WORK IN THE UNITED STATES, OF ANY TYPE, MUST BE STOPPED. NOW.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Disclosure and Notice: Except for the linked URLs and other items that can be found in the Internet, the ideas and/or opinions of today’s offering are by PAVACA. Credit must be given to PAVACA if the ideas and/or opinions of today’s offering are used by other blog writers, podcasters, or in social or print media.)
The header image of the word Interesting for today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics. There are Important Notifications form our host, Wolf Moon; the Rules of our late, good Wheatie; and certain caveats from Yours Truly, of which the reader should be aware. They are linked here. Note: AI-generated items in today’s offering are cited as such. if readers wish to post AI-generated items to today’s discussion thread, they must cite their source. Thank you.
Some Interesting Links:
Regarding the November 2025 exposure of an employee at the Rocky Mountain Lab (part of the NIH) to the Crimean-Congo Hemorrhagic Fever virus. The virus is being experimented on at this facility. Our good Aubergine posted a comment on this situation, which began a discussion: https://theqtree.com/2026/04/03/health-friday-4-3-2026-open-thread-where-the-focus-needs-to-be-now-an-opinion-piece/#comment-1595800. It has been proven that this virus does indeed shed; the shedding can be present in the body secretions and blood of the exposed / infected person. The published paper regarding shedding of Crimean-Congo Hemorrhagic Fever virus is here: https://pmc.ncbi.nlm.nih.gov/articles/PMC7078823/, “Monitoring Crimean-Congo haemorrhagic fever virus RNA shedding in a body secretions and serological status in hospitalized patients, Turkey, 2015.” Dilek Yagci-Caglayik, et al. 12 March 2020. (Yours Truly: While the paper is about the shedding of this virus in hospitalized patients, it, in my opinion, opens up the possibility that the virus can shed from non-hospitalized exposed or infected persons.)
>>>>>>>>>>>>>>>>>>>>>>>>
In Maryland, if a newly-proposed law there comes into effect, pharmacists will be able to order certain “vaccines” for patients; while, at the same time, placing the names of those persons into the Maryland state database for immunization tracking:https://jonfleetwood.substack.com/p/maryland-bill-lets-pharmacists-order, “Maryland Bill Lets Pharmacists Order Vaccines for You — Logging Your Name in State Tracking System Without Any Patient-Request Requirement”, 3 April 2026. A screenshot from this article is below:
Note that this bill regards pharmacists being granted permission to order vaccines — and to do so without the patient’s knowledge, consent, or request. The name of the patient is put into a state tracking database. The vaccines are paid for by private insurance (if the patient’s private insurance information is on file at the pharmacy), or are covered by Medicare/Medicaid. This opens up the potential for both the pharmacy and the state to “keep tabs” on the patient in order to get “vaccine compliance” from the patient.
>>>>>>>>>>>>>>>>>>>>>>>>
Why hasn’t James Lloyd Austin, III, Secretary of Defense under former “President” Joe Biden, been held to account for his “mandating” over 90% of United States military personnel being “vaccinated” with modRNA COVID-19 bioweapon “vaccines”? https://www.thefocalpoints.com/p/breaking-study-half-of-covid-19-vaccinated, “BREAKING STUDY: Half of COVID-19 Vaccinated Military Personnel Suffered Subclinical Heart Stress”, Nicolas Hulscher, MPH, 31 March 2026. The paper cited in the article is here: https://doi.org/10.1016/j.vaccine.2026.128535, “Transient elevation of NT-proBNP after mRNA COVID-19 vaccinations in healthy adults: A longitudinal biomarker analysis.” Pavel Dlouhy, et al. 30 April 2026.
Note that this paper studies heart issues that appeared in 50% of 83 healthy, adult military personnel after their being “vaccinated” with either BNT162b2 (Pfizer-BioNTech) or with mRNA-1273 (Moderna.) The military personnel were stationed at the Air Transportation Base Facility in Prague, Czech Republic. The troponin levels of their hearts were found to have gone up. Elevated troponin levels in the heart indicate stress on the heart muscle. Elevated troponin levels can indicate heart problems even if there are no overt symptoms. If that is what occurred in half of the “vaccinated” personnel tested at an air transportation base in the Czech Republic, how many thousands of United States military personnel potentially had the same effect after they were “mandated” to be “vaccinated” by former Defense Secretary Austin? (Austin was the former Secretary of what is now called the Department of War.)
Note also that the military personnel at the air transportation base in Prague were well over the age of 17 — in fact, the mean age of the 83 tested personnel was 39 years. This blows clean out of the water ALL of the claims of Big Pharma, Establishment Medicine, the CDC, the FDA, the AMA, and many other entities, that heart problems associated with COVID-19 “vaccination” are “rare” —and, are “confined mostly to persons between the age of 12 and 17 years.”
>>>>>>>>>>>>>>>>>>>>>>>>
Another example of how a physician who stood up against Big Pharma, the CDC / FDA, the AMA, and the AAP (American Academy of Pediatrics), was persecuted: his License to Practice Medicine in his home state (Oregon) was suspended in 2020; then, his License to Practice Medicine was revoked in the state where he had been credentialed (Washington State); then, his board credentials in the AAP were revoked; then, he had to surrender his License to Practice Medicine in Oregon in 2022 (https://omb.oregon.gov/Clients/ORMB/Public/VerificationDetails.aspx, effective 5 December 2022.) This was the journey of Dr. Paul Thomas, a highly-respected pediatrician: https://www.2ndsmartestguyintheworld.com/p/doctor-published-study-showing-vaccinated, “Doctor Published Study Showing Vaccinated Children Have 500% Increase In Chronic Diseases Only To Have License Suspended & Get Cancelled By BigPharma”, 8 April 2026. The study was Retracted by MDPI, the preprint publisher. It is available here: https://www.researchgate.net/publications/346088816_Relative_Incidence_of_Office_Visits_and_Cuulative_Rates_of_Billed_Diagnoses_Along_the_Axis_of_Vaccination. James Lyons-Weiler, Paul Thomas. 22 November 2020. (Yours Truly: Note that this paper was accepted and peer-reviewed before it was published.)
>>>>>>>>>>>>>>>>>>>>>>>>
Dr. Peter A. McCullough addresses the nexus among cancer patients who then get COVID-19 “vaccinated” and thereupon afterwards present with symptoms of Long COVID:https://www.thefocalpoints.com/p/the-hollow-promise-of-protection, 7 April 2026. A screenshot from this article is below (access to the entire particle is for subscribers only):
A related topic to the heart issues situation found in the military personnel at the air transportation base in Prague who had been COVID-19 “vaccinated”: This one regards subclinical myocarditis/pericarditis in COVID-19 “vaccinated” persons: https://www.thefocalpoints.com/p/breaking-peer-reviewed-paper-finds, “BREAKING: Peer-Reviewed Paper Finds mRNA “Vaccines” Convey Silent Heart Damage—Presents Approach to Diagnosis and Management”, Nicolas Hulscher, MPH, 31 December 2025. A screenshot from this paper is below:
The paper is found here: https://doi.org/10.1810/mra.v13i11.7078, “COVID-19 Vaccine-Induced Subclinical Myopericarditis: Pathophysiology, Diagnosis, and Clinical Management.” Peter A. McCullough, MD, MPH, M. Nathaniel Mead, MSc, PhD, Nicolas Hulscher, MPH. 30 November 2025.
Yours Truly: The above paper speaks to subclinical myocarditis/pericarditis in COVID-19 “vaccinated” persons — and makes it clear that, although many of the reported cases were found in “vaccinated” males under age 21, there were cases found in other “vaccinated” persons (male and female), and in other age groups. On the other hand, there is also the real phenomenon of “vaccine” shedding from “vaccinated” persons onto others, including onto non-COVID-19 “vaccinated” persons. Who knows how many non-COVID-19 “vaccinated” persons (including children) have been exposed to the ingredients and mechanisms of these “vaccines” that induce heart problems? At the same time, there are other factors that need to be considered when talking about what engenders or aggravates heart issues. Examples of other factors can include, but are not limited to: chronic stress; hypertension; family history of / predisposition to, heart disease; and, COPD (https://www.ummhealth.org/health-library/copd-and-heart-disease.)
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA, A modRNA, AN saRNA, OR A taRNA PRODUCT OF ANY KIND, IN ANY FORM.
ALL GAIN-OF-FUNCTION ACTIVITIES IN THE UNITED STATES MUST BE STOPPED, NOW.
ALL COVID-19 BIOWEAPON “VACCINES” MUST BE PULLED OFF THE MARKET AND REMOVED FROM USE IN THE UNITED STATES, NOW.