The free header image for today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As today’s offering is related, in part, to the disaster of the COVID-19 “vaccines”, Yours Truly dedicates it to all persons who have contracted injures, illnesses, or disabilities, induced or aggravated by the COVID-19 “vaccines” that were injected into their bodies; and, to the memory of all persons who have passed away from the negative effects of the COVID-19 “vaccines” that were injected into their bodies.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except for perhaps AI-generated images in any of the linked URLs below. If readers wish to post any AI-generated content in today’s discussion thread, they must cite their source. Thank you.
There are two sections to today’s Special Report offering: the first section, regarding the now-proven linkage of COVID-19 “vaccine boosters” to increases in cancer and in general mortality; the second section, regarding what appears to be the potential emergence of the “next plandemic” in Communist China. Please bear with Yours Truly: one does not want to “weary by recitals”, as the Duc de Saint-Simon once wrote — but there is a lot of information, multiple screenshots, and so on. The evolving knowledge regarding the disaster called COVID-19 (the virus itself, and the “vaccines”) is gaining speed with each passing day. This evolving knowledge base is important to understand in light of the developments regarding the new information about the “Chikungunya outbreak” currently in China, and which is apparently spreading to other countries (shades of the original COVID-19 virus itself outbreak in China.)
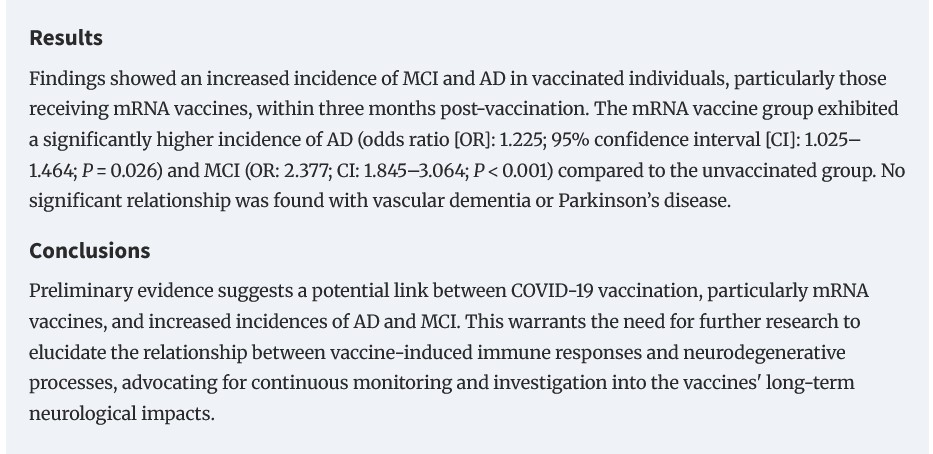
First section, the linkage between COVID-19 “booster vaccines” with increases in cancer and in general mortality. COVID-19 “vaccine boosters” means any injection of a “latest version” of a COVID-19 “vaccine.” This includes the FDA- approved 2025-2026 “new formula COVID-19 vaccine versions” of the Pfizer-BioNTech modRNA COVID-19 “vaccine”, COMIRNATY; of the Moderna modRNA COVID-19 “vaccine”, SPIKEVAX; and, of the Novavax COVID-19 “vaccine”, NUVAXOVID.
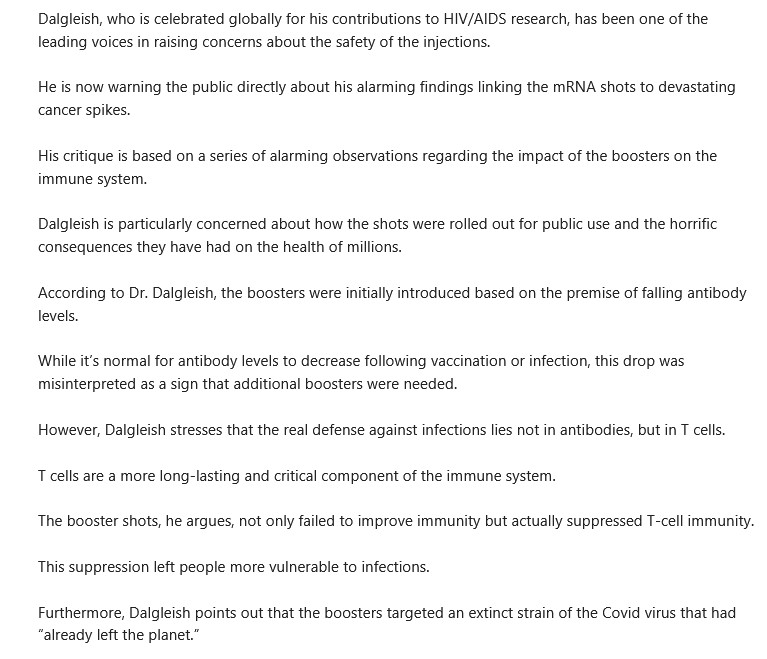
Yours Truly begins here: https://slaynews.com/news/renowned-oncologist-sounds-alarm-cancer-deaths-now-surging-among-covid-boosted/, “Renowned Oncologist Sounds Alarm: Cancer Deaths Are Now Surging Among Covid-Boosted”, by Frank Bergman, 6 August 2025. There is an embedded video statement by Prof. Dr. Angus Dalgleish (St. George’s, University of London.) Dr. Dalgleish warns, in no uncertain terms, that it is the suppression of T-cell immune cells in the body of the COVID-19 “vaccine boosted” that is causing the surge of cancer among these persons. Please see the screenshot from the Slay News article, below:
There is another study from Japan, which also confirms that repeated COVID-19 “vaccine boosters” cause increases in mortality. Please see: https://slaynews.com/news/official-japanese-data-confirms-covid-vaccines-caused-worsening-excess-death-surge/, by Frank Bergman, 1 August 2025 (the article title is the same as the URL.) Please see the screenshots from this article, below:


The paper referenced above is here: https://www.researchsquare.com/article/rs-6899448/v2, “Factors contributing to the sharp rise in excess mortality in Japan since 2021”, Atsushi Takahashi, 17 July 2025. This paper is a pre-print. Please see the screenshots from this paper, below. They are: portions of the Results section; Figure 4; and, Figure 9:
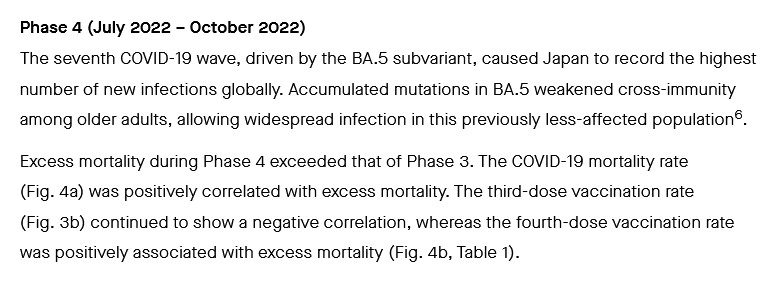
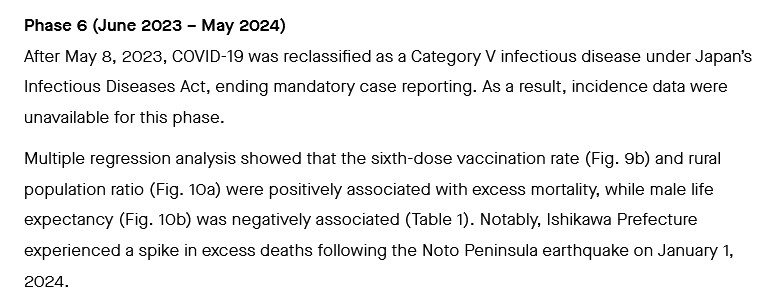
The identifier names are those of the Prefectures in Japan that were studied. Even with taking other factors into consideration (examples: the size and population of the various Prefectures; the number of adults in age brackets in the Prefectures; whether or not a Prefecture was “rural” in character and location, as compared to “urban”), it is clear that the increase in mortality is tied to an increased amount of COVID-19 “vaccine boosters” that were administered.
There is a Commentary to this paper, to be seen here: https://jxiv.jst.go.jp/index.php/jxiv/preprint/view/1398/, “Commentary: Immune imprinting and spike protein toxicity — rethinking COVID-19 vaccinesty: rethinking COVID-19 vaccines”, Yasuhiko Kamikubo; Takahashi, Atsushi, 2025. This Commentary is in a mixture of English and Japanese. The English translation (no figures included) is here: https://jxiv.jst.go.jp/index.php/jxiv/preprint/view/1398/3679.
The above items confirm this article, written in July 2025: https://justthenews.com/politics-policy/coronavirus/covid-boosters-correlate-worse-survival-rates-cancer-third-most-deaths, “COVID boosters correlate with worse survival rates for cancer with third-most deaths: study”, by Greg Piper, 9 July 2025. Please see the screenshots from this article, which relates to a study in Japan regarding survival rates among COVID-19 “vaccine boosted” pancreatic cancer patients, below:

The peer-reviewed paper on the Japan study is here: https://doi.org/10.3390/cancers17122006, “Repeated COVID-19 Vaccination as a Poor Prognostic Factor in Pancreatic Cancer: A Retrospective, Single-Center Cohort Study”, Makoto Abue, et al., 16 June 2025.
Yours Truly has written extensively for the board here regarding the damage / destruction of the natural immune system of the person who takes COVID-19 “vaccines.” These injectables were designed to attack, damage / destroy the CD4 – CD8 immune system cells. These injectables were designed to attack, damage / destroy the IgG3 immune system “fighter” cells, while at the same time, fostering the increase of IgG4 immune system “tolerate and never clear” cells. This damage / destruction increases with each injection of a modRNA COVID-19 “vaccine”, including injections of the “latest formula version” of said “vaccines”, which includes the “2025-2026 Formula versions” of said “vaccines” (COMIRNATY [Pfizer-BioNTech]; SPIKEVAX [Moderna]; and, NUVAXOVID [Novavax.])
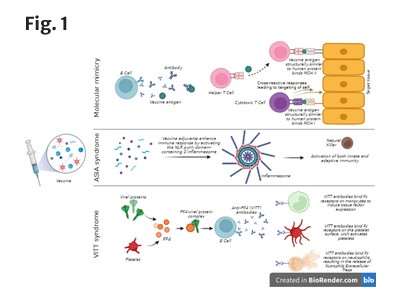
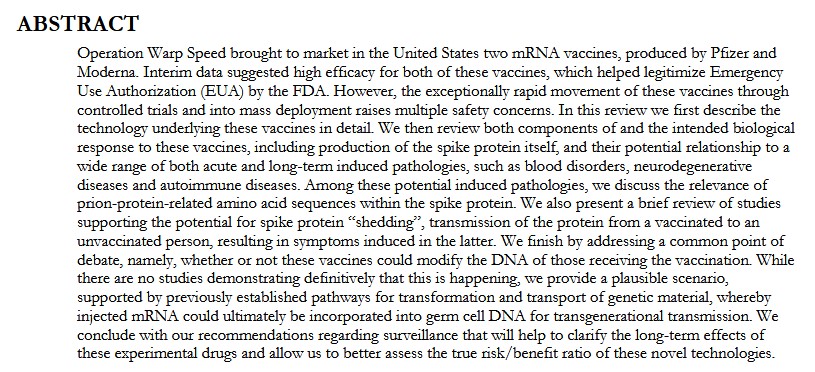
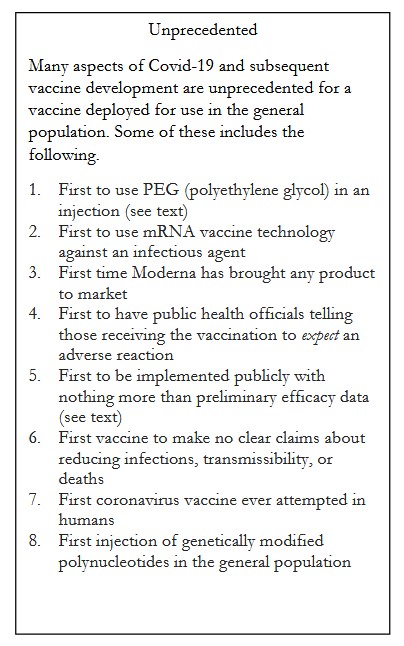
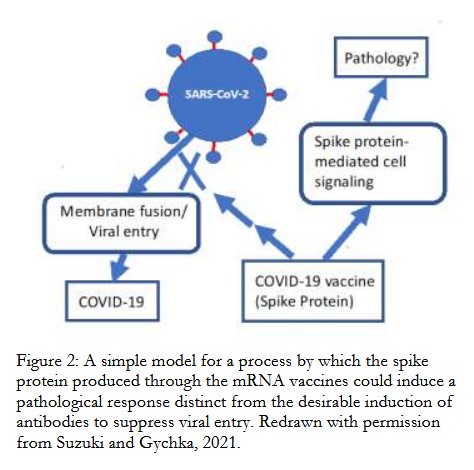
The “Seneff and Nigh” paper of 10 May 2021 discusses how “immune system imprinting” in the the body of persons who take the COVID-19 “vaccines” have the potential to result in what the authors call “unintended consequences.” The paper is available here: https://dpbh.nv.gov/uploadedFiles/dpbhnvgov/content/Boards/BOH/Meetings/2021/SENEFF-1.PDF, “Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19”, Stephanie Seneff and Greg Nigh; International Journal of Vaccine Theory, Practice, and Research 2(1), May 10, 2021, Page 38-79. Please see the screenshots from this article, below. They are: the Abstract; the “Unprecedented” box; and, Figure 2.
Further information regarding the “class switch” between IgG3 cells and IgG4 cells resulting from COVID-19 “vaccination” is here: https://jessicar.substack.com/p/the-immunological-mechanism-of-action, “The immunological mechanism of action for lost immunity, a shift to tolerance (and autoimmunity?) from the shots”, by Jessica Rose, PhD, 22 December 2022. Please also see: https://www.theqtree.com/2025/04/04/health-friday-4-4-2025-open-thread-the-covid-19-vaccines-decimate-the-igg-immune-system-cells/; and, https://www.theqtree.com/2024/12/06/health-friday-open-thread-12-6-2024-the-immune-system-after-covid-19-vaccination-and-a-note-on-the-virus-itself/.
Second section, regarding the potential for the “next plandemic” to come from Communist China. This has to do with the current emergence of mosquito-borne Chikungunya infections in several areas of China, which has resulted in various government-enforced measures. There is also an ** interesting connection ** to the United States involved in this situation.
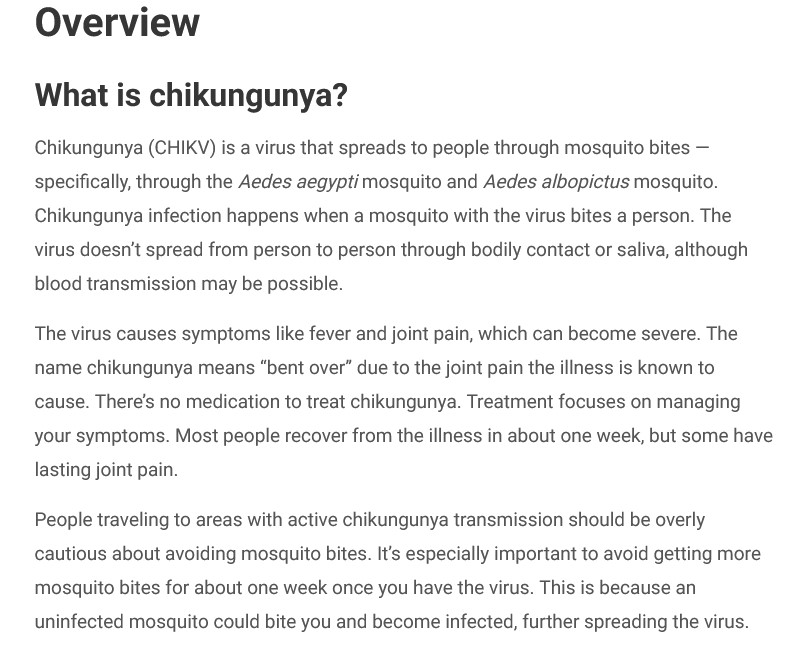
What is Chikungunya? It is a virus transmitted by the bite of an infected female mosquito of (usually) the Aedes aegypti or the Aedes albopictus species. (As an aside: female mosquitos of these species can also transmit Dengue fever via bites.) The virus that is transmitted causes joint pain and fever; these can progress to severe. Most people infected with Chikungunya, however, make a full recovery. The virus is an RNA alphavirus. Please see: https://my.clevelandclinic.org/health/diseases/25083-chikungunya; there is a screenshot from this article, below:
Another source of information regarding Chikungunya is here: https://www.who.int/news-room/fact-sheets/detail/chikungunya; please see the screenshot from this article, below:
Two recent articles regarding the Chikungunya outbreak in China: the first, here: https://jessicar.substack.com/p/the-new-pending-plandemic-is-it-scheduled, “The new pending “plandemic” — is it scheduled for November?”, by Jessica Rose, PhD, 12 August 2025. Dr. Rose makes it clear that the “alphavirus + saRNA-LNP platform” (self-amplifying RNA + lipid nanoparticles “vaccine” platform) is based on the VEEV alphavirus (Venezuelan Equine Encephalitis Virus.) Please see the screenshots from her article, below:


**** Note the mention of immune system issues that are induced in persons who are COVID-19 “vaccinated”, and how this can potentially severely complicate any infection by Chikungunya.
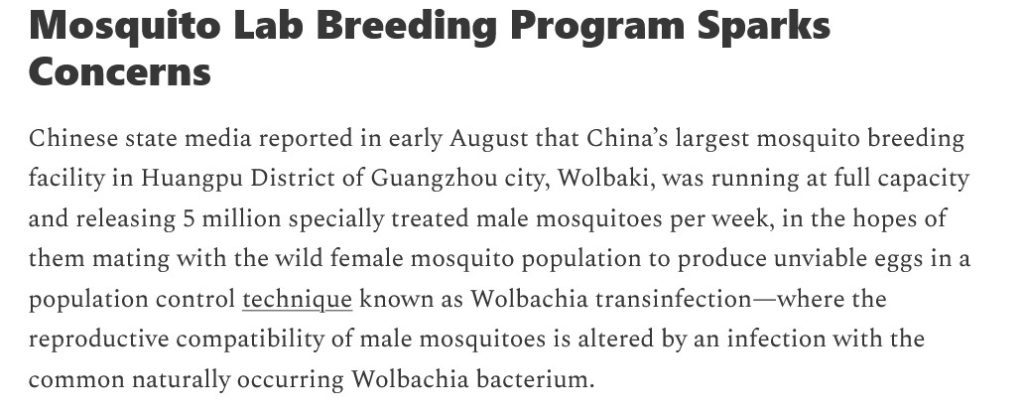
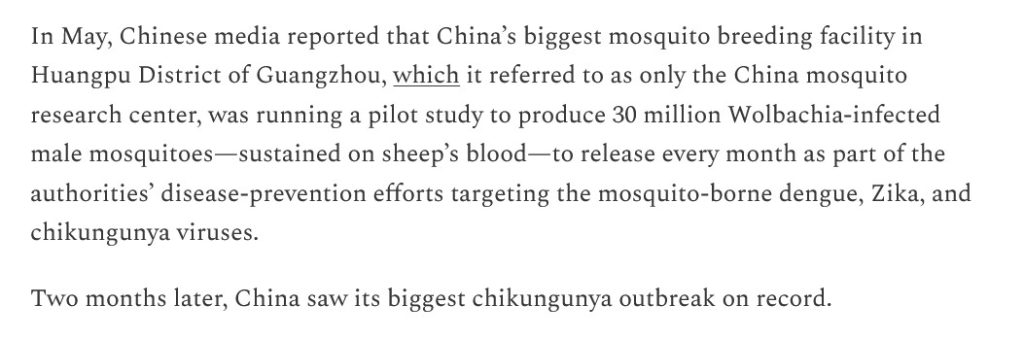
The second article is here: https://www.2ndsmartestguyintheworld.com/psyop-25-scamdemic-update-chinese, “PSYOP-25 SCAMDEMIC UPDATE: Chinese Authorities Mandating Blood Tests, Releasing Lab Mosquitoes to Fight Chikungunya Outbreak”, 13 August 2025. Please see the screenshots from this article, below:
The founder of the “mosquito lab” in Guangzhou is Dr. Zhiyong Xi. Please see the screenshot below from the above link:

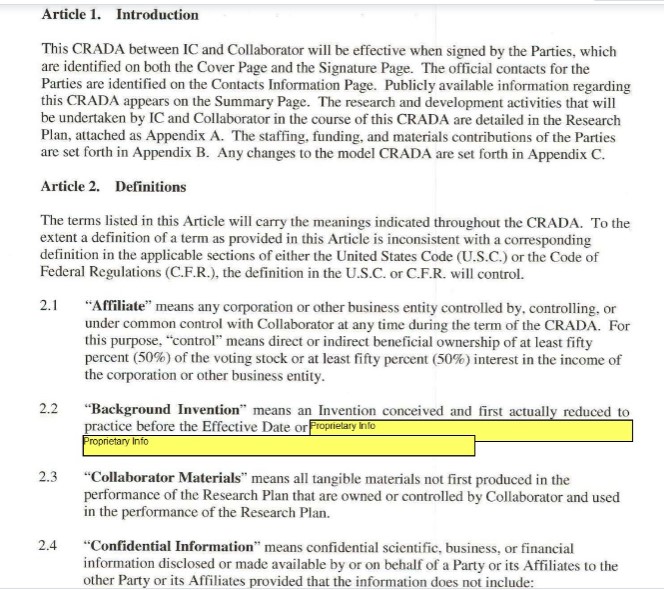
Let’s look at Dr. Zhiyong Xi. https://archive.md/b5xWD:
He is still a professor at Michigan State University in the United States: https://directory.natsci.msu.edu/Directory/Profiles/Person/101715, “Zhiyong Xi”:
And here is a portion of the work that Dr. Zhiyong Xi is doing at Michigan State University, via https://scholars.msu.edu/scholar/8639/ZHIYONG_XI:

Which work, at least in part, is being funded by NIAID (division of NIH — both divisions part of HHS.)
Which begs the following questions: WHY is Dr. Zhiyong XI still doing mosquito research in the United States if he founded a mosquito study lab in Communist China? WHY is Dr. Zhiyong Xi’s research at Michigan State University being funded, at least in part, by the NIH / NIAID?
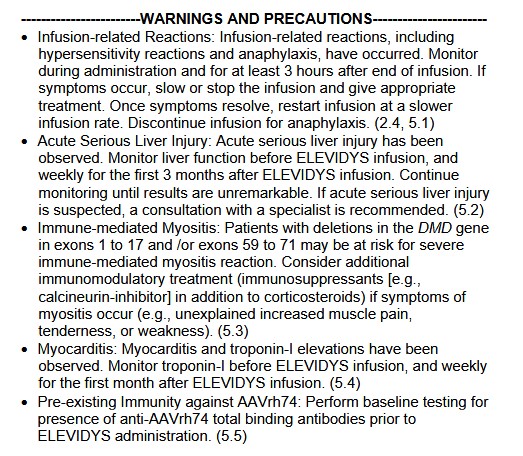
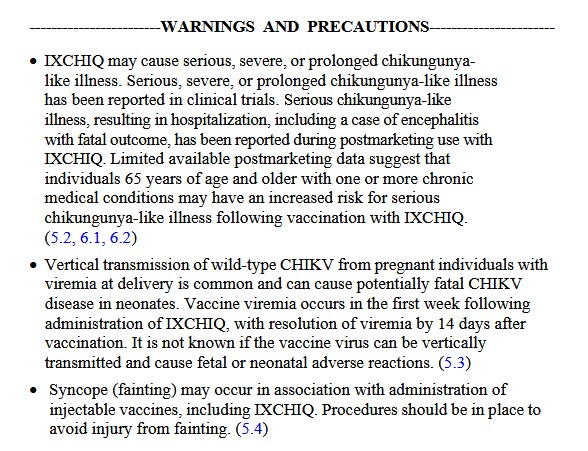
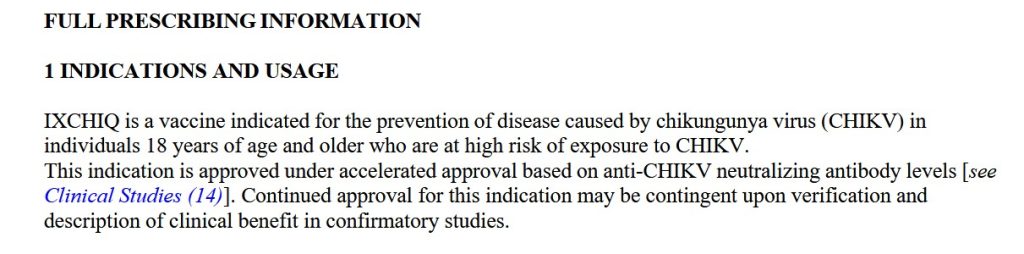
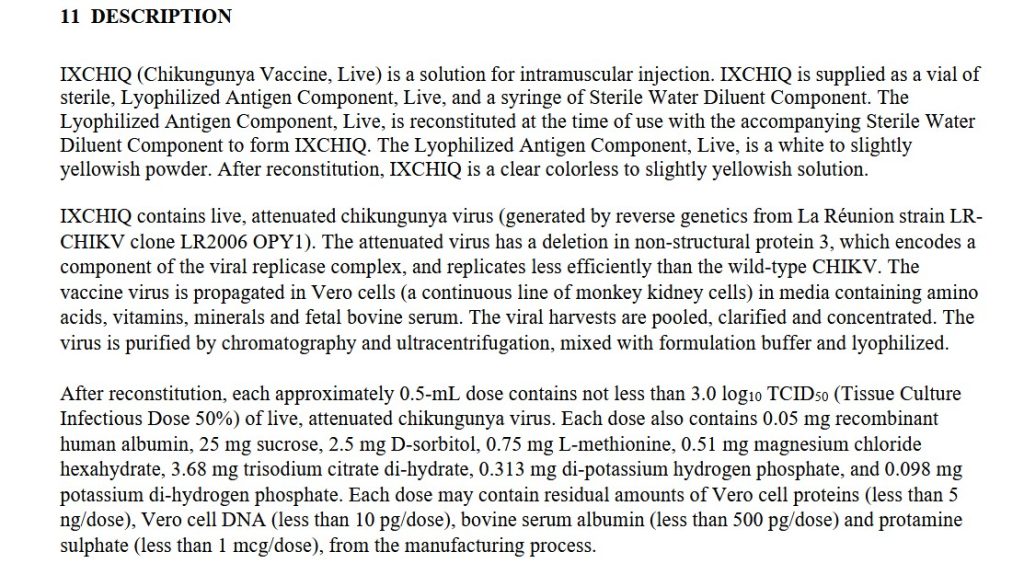
There are two “FDA-approved vaccines” against Chikungunya: IXCHIQ, and VIMKUNYA. BOTH of these “vaccines” were FDA-approved under “accelerated approval” methods. Please see the screenshots, below, from the Package Inserts for these injectables. First, from the Package Insert for IXCHIQ (https://ixchiqhcp.com/PI-new.pdf):

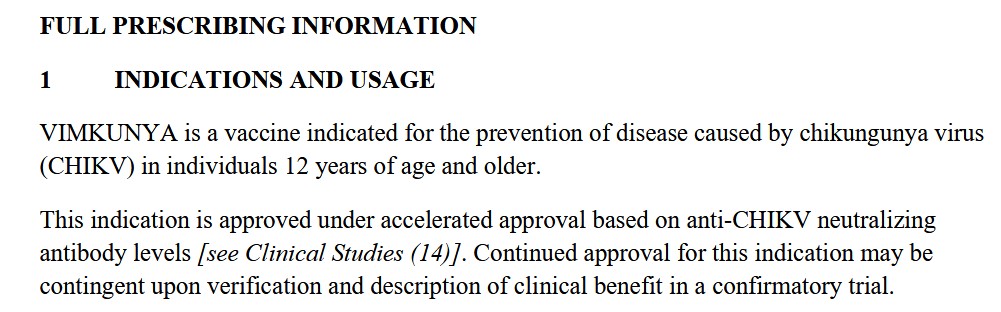
And, from the Package Insert for VIMKUNYA (https://bavariannordic.io/uploads/Vimkunya-pi.pdf):
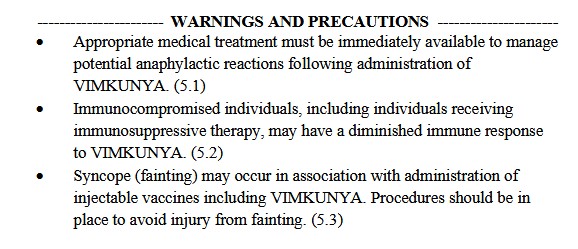
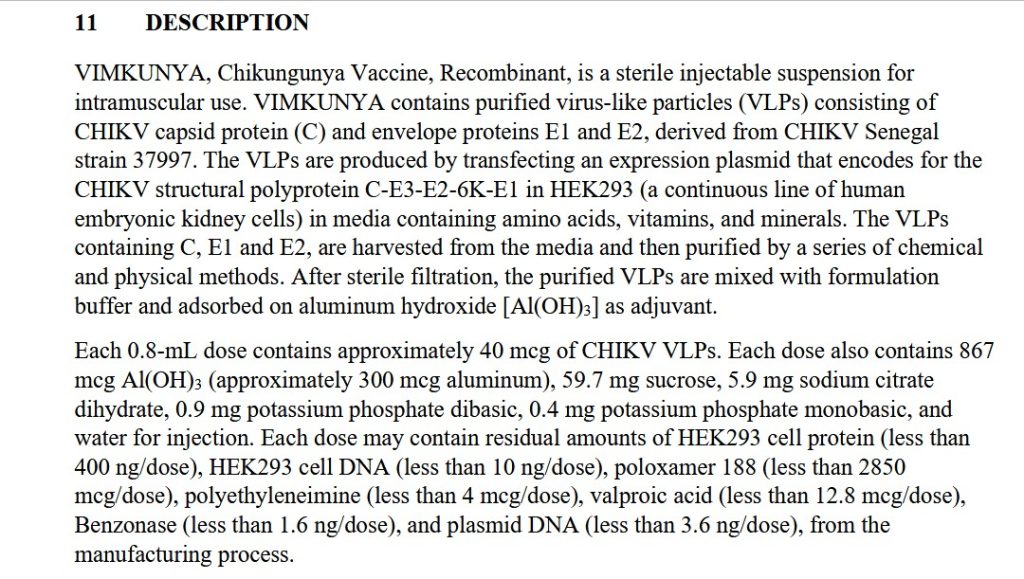
Note the presence of Aluminum Hydroxide as an adjuvant in VIMKUNYA.
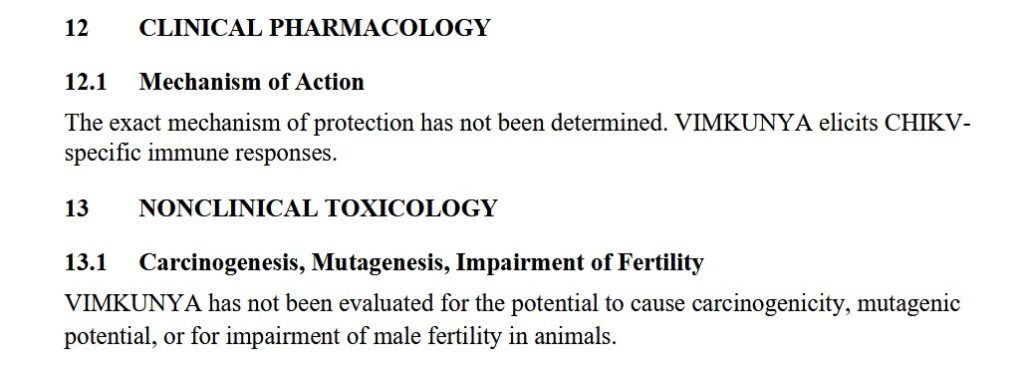
NOTE THAT THE “EXACT MECHANISM OF PROTECTION’ HAS NOT BEEN DETERMINED FOR EITHER IXCHIQ OR FOR VIMKUNYA. In other words, the United States government (via the FDA) is fine with injecting people with these “vaccines” WITHOUT THE FDA KNOWING THE EXACT MECHANISMS OF PROTECTION FOR EITHER OF THEM. What are the “CHIKV-specific immune responses” that these injectables supposedly elicit?
And, by the way, both IXCHIQ and VIMKUNYA can be “shed” onto newborn children if the expectant mother is sick with a virus (this is called viremia) at the time of delivery. A pregnant female who takes either one of the above “vaccines” runs the risk of contracting “viral viremia.” Neither IXCHIQ, nor VIMKUNYA have had proper testing for potential effects on pregnant females, their fetuses, or their newborns (section 8.1 Pregnancy in either Package Insert.)
All of the above begs the following questions: Does HHS Sec. Robert F. Kennedy, Jr., know about these Chikujgunya “vaccines”? Does he know that the FDA approved them under “accelerated approval” methods? Does he understand that the FDA does NOT know the “exact mechanism of protection” for either IXCHIQ or VIMKUNYA? Does Dr. Martin Makary (FDA Commissioner) know about this situation? Do either Sec. Kennedy, Jr., or Dr. Makary know that “career FDA types” in the CBER division signed the FDA Approval Letters for IXCHIQ (signed by R. Douglas Pratt, MD, 6 August 2025) and for VIMKUNYA (signed by David C. Kaslow, MD, 14 February 2025)?
Yours Truly will again emphasize that it is critically important for all persons, whether COVID-19 “vaccinated” or not, to follow some type of COVID-19 spike protein mitigation / prophylaxis protocol. It is also critically important that all persons, whether COVID-19 “vaccinated” or not, to do all they can to build and maintain their general health, and the health of their immune system, so as to be in the best shape possible.
THERE. MUST. BE. JUSTICE.
THERE. MUST. BE. TRUTH.
Peace, Good Energy, Respect: PAVACA