

The above image of a physician performing a vaccination is courtesy of Google Images and The New York Times.
This post is the first of “Health Friday”, a new series of offerings related to Big Pharma, vaccines, general health, and related topics. It is an honor and privilege to contribute this series to the board. Since today’s post relates to COVID-19 and the COVID-19 “vaccines”, it is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023. However, the discussion will not be limited to what is presented today; it is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here. “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
The U Tree is for “argue it out” interactions: https://utree.home.blog
The “Rescue Thread” at the U Tree: https://utree.home.blog and click on the “Featured” article.
The “third site”, in case the above two are not accessible: https://theqtree579486807.wordpress.com/
Civil discussion is practiced here. The excellent and timely Rules of our late, good Wheatie prevail:
One: No food fights.
Two: No running with scissors.
Three: If you bring snacks, bring enough for everyone.
Please follow the added guidelines as expressed here: www.theqtree.com/2019/01/01/dear-maga-open-topic-20190101/. Please do not give the modern-day version of Cato the Elder the opportunity to show “enmity” to the board.
The extra items:
What Yours Truly writes in this series, as in her previous blog posts for this board, is not medical advice — they are opinions based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to please consult a healthcare practitioner regarding health concerns or conditions.
And now, to dive in. There is a lot to “unpack.”
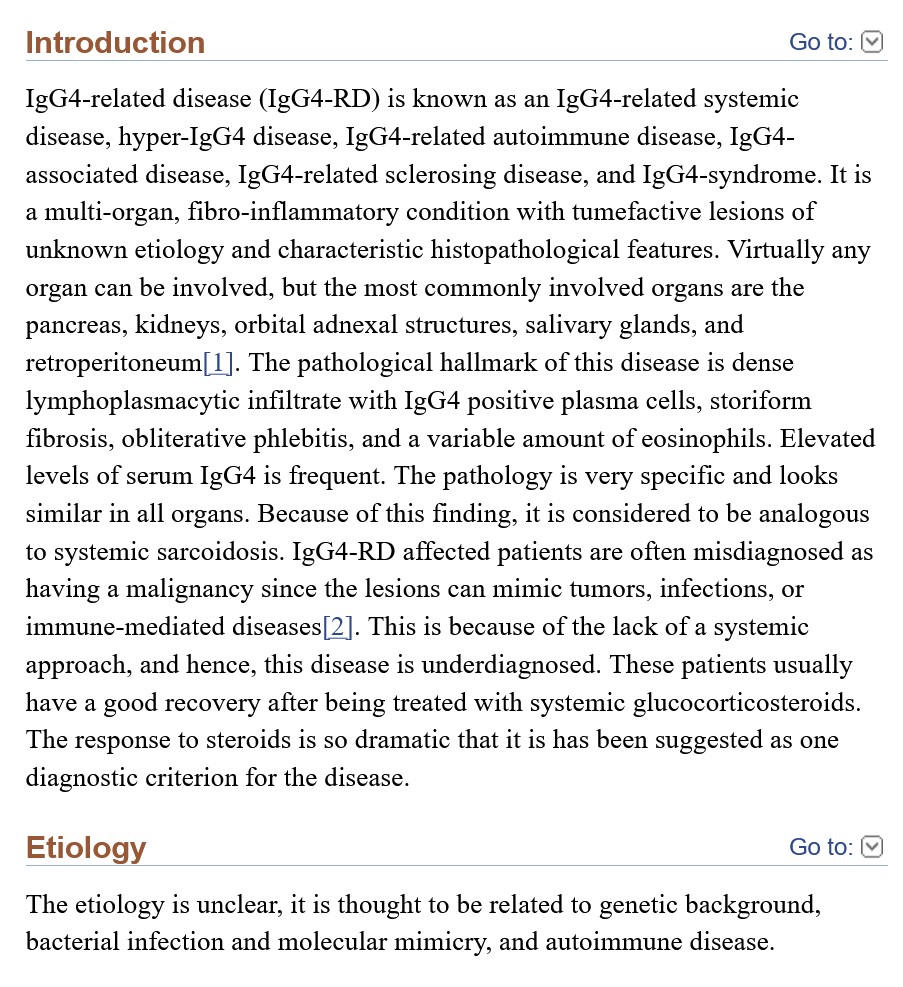
The modRNA COVID-19 “vaccines” induce IgG4-related disease (IgG4-RD.) IgG4-related disease (IgG4-RD) is a term that covers multiple medical conditions, ranging from neurological to ocular to cardiovascular to respiratory to gastrointestinal to urogenital. Since it is a chronic inflammatory condition, there can be more than one location of an IgG4-RD associated ailment within the patient’s body. Please see: https://en.wikipedia.org/wiki/IgG4-related_disease, “IgG4-related disease”, which has a list of symptoms in reported cases of IgG4-RD, and a list of body area sites that can be affected by IgG4-RD. The first instance of what is now called IgG4-RD was discovered in 1892 by Johann von Mikulicz, who diagnosed an “inflammatory disease of the salivary glands” in a patient (this condition was later called Mikulicz’ disease.) In 2021, Hamano et al. found elevated IgG4 levels in patients with Autoimmune Pancreatitis (AIP.) Please see: https://ojrd.biomedicalcentral.com/articles/10.1186/s13023-014-0110-z, “IgG4-related disease: an orphan disease with many faces”, Herwig Pieringer, et al., 16 July 2014. It appears that an issue with obtaining a true diagnosis of an IgG4-related disease is that many of the presenting elements can “mimic” other conditions, such as cancer or non-Hodgkin’s lymphoma. In addition, IgG4-RD can simply not present symptoms at all, until the patient concludes that “something is going on here.” In terms of the presenting symptoms of an IgG4-RD disease, there are, among others: storiform fibrosis (“spindle-shaped” cells that can, with collagen fibers, form a “flowing arrangement”); and, eosinophilia (high elevation of a type of white blood cell [eosinophils] that supports the natural immune system.) Please see: https://academic.oup.com/mr/article/31/3/529/6300281, “The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD”, Hisamori Umehara, et al., 4 May 2021. (Note: the entire article is restricted access.) Below is a portion from “IgG4-Related Disease” from StatPearls – NCBI Bookshelf, an article by Sudheer Nambiar and Tony I. Oliver (www.ncbi.nlm.nih.gov/books/NBK499825):
There are some IgG4-RD conditions that may be genetically-based; one example is Autoimmune Pancreatitis (AIP.) Please see: https://pubmed.ncbi.nlm.nih.gov/31104539/, “Genetic analysis of IgG4-related disease”, Yuki Ishikawa and Chikashi Terao, 7 June 2020. (Note: again, the entire article is restricted-access.) On the other hand, another IgG4-RD condition, Autoimmune Lymphoproliferative Syndrome (ALPS) appears to strike children. In addition, IgG4-RD conditions can be “immune-mediated” (meaning, the body’s immune system response is either inappropriate or excessive); and/or “autoimmune” (meaning, the body’s immune system attacks healthy tissues in the body.)
Yours Truly will examine the presence of eosinophilia as an indicator of IgG4-RD. This is an important “marker.” And it ties into the modRNA COVID-19 “vaccines” — the COVID-19 “vaccinated” person’s natural immune system being damaged and/or destroyed by the ingredients and mechanisms of these “vaccines”; and, with repeated injections of these “vaccines” compounding this damage and/or destruction.
The first item is a blog article by Dr. Jessica Rose, PhD: https://jessicar.substack.com/p/igg4-related-disease-and-igg4-means, “IgG4-related disease (IgG4RD) means FIBROSIS and organ destruction”, 28 December 2022. It is now known that the modRNA COVID-19 “vaccines” induce a “class switch” in the COVID-19 “vaccinated” person’s natural immune system; this “class switch” is the damage and/or destruction of IgG3 immune system cells (these cells help to fight off infections and other enemies that “invade” the natural immune system), replacing IgG3 cells with increased numbers of IgG4 cells (these cells help to allow the body to “tolerate” assaults to the natural immune system.) Repeated injections of modRNA COVID-19 “vaccines” exacerbate this process: please see https://doi.org/10.1126/sciimmunol.ade2798, “Class switch toward non inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination”, Irrgang P, et al., 22 December 2022. Notice the title: “non inflammatory”, “spike-specific”, “IgG4”, and “repeated SARS CoV-2 mRNA vaccination.” IgG4-RD conditions can present as non-inflammatory (the patient doesn’t notice anything wrong for some period of time, see above in today’s post); however, the IgG4 levels in the patient are high upon examination. Below is a portion of the Introduction of the above paper. Note: Comirnaty was the non-United States version of the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2. Comirnaty and BNT162b2 are the same product. Note 2: the 2023-2024 Comirnaty modRNA COVID-19 “vaccine” was given full FDA approval for use in the United States on 23 September 2023 for persons age 12 above: www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-receive-us-fda-approval-2023-2024-covid; the version that the FDA authorized (the “2023-2024 Formula COVID-19 Vaccine” by the same company) was for persons age 6 months through 11 years of age (www.fda.gov/media/167211/download.)
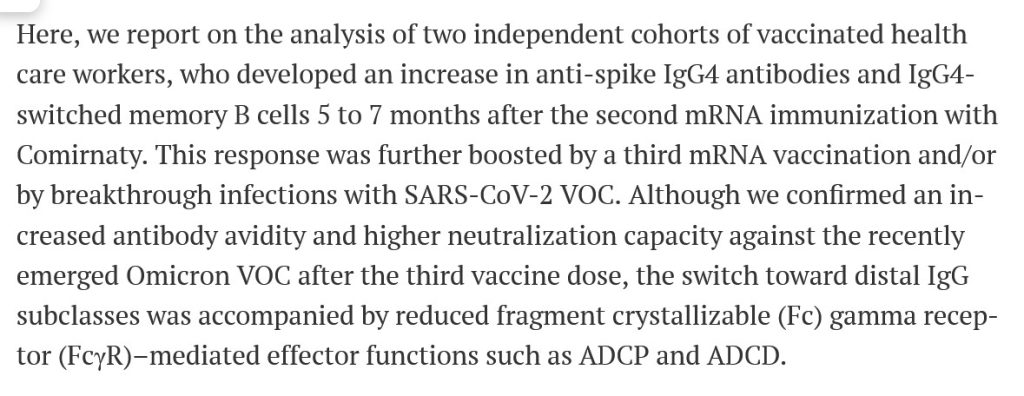
Note that the IgG4 cell increase extended for months after the second injection of Comirnaty and was further increased after the third injection. This correlates to the original “two-injection Primary Series” plus the original “booster shot” of Comirnaty that millions of persons took between December 2020 and early 2022. This would also include, since the formulations were the same, of the “Primary Series” and the original “booster shot” of BNT162b2 that were taken by millions of persons in the United States from December 2020, until Comirnaty was given full FDA approval in the United States on 8 July 2022 for persons age 12 and older (at which point, BNT162b2 was “replaced” by Comirnaty except for use in persons age 6 months to 11 years; the FDA authorized the “Pfizer-BioNTech COVID-19 Vaccine” for this age group.) This “product name situation” may seem a little confusing: at bottom, it had to with removal of liability for the “vaccine” manufacturer. This will be discussed at a later date.) Note also that “VOC” means Variants of Concern (in other words, the Delta, the Omicron, the XBB.1.5 variants of the SARS-CoV-2 [COVID-19] virus, and so on.)
The second item is here: www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021, given by Pfizer-BioNTech to the FDA on 30 April 2021. This report covers Adverse Event Reports that were submitted to the company between 11 December 2020 (the date on which the FDA in the United States granted the initial Emergency Use Authorization (EUA) for BNT162b2 to be used in the United States, 21 December 2020 (the date on which the EMA (European Medicines Agency) granted its initial EUA for BNT162b2 to be used in Europe / Scandinavia; and, 28 February 2021. The APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST, which begins on Page 30 of this report, lists over 1,200 different types of medical adverse events that were reported to Pfizer-BioNTech from the worldwide EUA start dates above. On Page 3 and Page 4 of the APPENDIX 1. (Page 32 and Page 33 of the report), there are the following Adverse Events of Special Interest listed: Eosinopenia; Eosinophilic fasciitis; Eosinophilic granulomatosis with polyangiitis; Eosinophilic oesophagitis. On Page 5 of the APPENDIX 1. (Page 34) of the report, there is listed: Immunoglobulin G4 related disease. On Page 8 of the APPENDIX 1. (Page 37 of the report) there is listed: Sjogren’s syndrome (another type of IgG4-RD.) These are a few of the IgG4-RD types of reports that are listed in the APPENDIX 1. section. Thus, the FDA knew, on 30 April 2021, that BNT162b2 “vaccination” induces IgG4-related disease conditions. Yet, the FDA did nothing to stop the continuing rollout of BNT162b2.
A third item is here: https://mole.substack.com/cp/147758416, a 15 August 2024 cross-post from Lioness of Judah Ministry, “German Study Links Covid Shots to Surge in VITAL ORGAN DAMAGE among Children”. The study found that there was a large increase of organ damage induced by BNT162b2 in children in Germany ages 5 to 11 years old. The study is here: https://journals.lww.com/pidj/fulltext/9900/delayed_induction_of_noninflammatory_sars_cov_2.959.aspx, “Delayed Induction of Noninflammatory SARS-CoV-2 Spike-Specific IgG4 Antibodies Detected 1 Year After BNT162b2 Vaccination in Children”. Kobbe, Robin MD, et al., 30 July 2024. The IgG4 antibodies were detected after the second dose of BNT162b2 (in other words, after the “Primary Series” of two BNT162b2 injections was completed.)
And, a fourth item is here, related to COVID-19, the COVID-19 “vaccines” and autoimmune conditions: https://wmcresearch.substack.com/p/long-covid-is-an-autoimmune-disease, “Long COVID is an Autoimmune Disease: Injecting Mice with IgG from Long COVID Patients Induces Symptomology”, by Walter M Chesnut, 4 June 2024. Mr. Chesnut has long posited that the spike protein of the COVID-19 virus itself contains elements that attack the natural immune system of the body of a person infected with this virus; and that the COVID-19 virus itself can induce what is now called “Long COVID.” Yours Truly will add the opinion that the difference between “Long COVID” in a person who is “unvaccinated” against COVID-19, and “Long COVID” in a COVID-19 “vaccinated” person, is this: the natural immune system of the “unvaccinated” person still has the potential to not only fight off a COVID-19 infection, but also to mitigate or eliminate the chance that “Long COVID” may result from the infection; whereas, the natural immune system of the COVID-19 “vaccinated” person has been damaged (or worse), resulting in a much larger potential for “Long COVID” (both in presentation and in duration.)
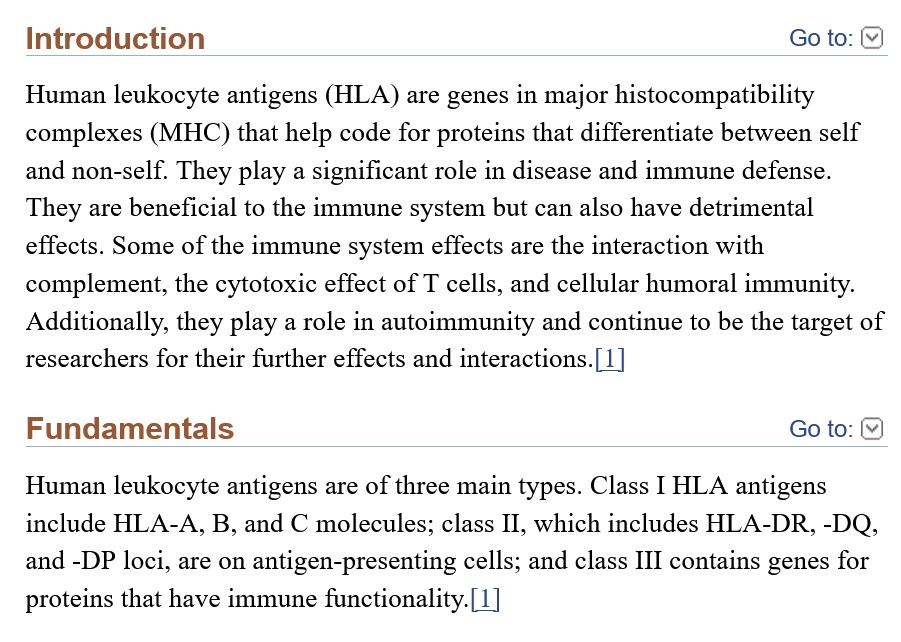
Yours Truly believes that the COVID-19 virus itself, and the ingredients and mechanisms of the modRNA COVID-19 “vaccines” (one of these ingredients being a “lab-modified” form of the RNA of said virus), both attack the natural immune system of the body. The COVID-19 “vaccines” have been shown to damage and/or destroy the IgG3 cells of the body’s natural immune system (these cells help to fight off viruses, etc.), replacing these with increased amounts of IgG4 cells (“toleration facilitator” cells.) In Yours Truly’s opinion, one of the important details here is the targeting of HLA cells (human leukocyte antigen cells, a type of white blood cells) by the COVID-19 virus itself, and, by extension, the COVID-19 “vaccines.”
In the book Biochemistry, HLA Antigens by Helen Nordquist and Radia T. Jamil, www.ncbi.nlm.nih.gov/books/NBK546662/, there is the following:
And, from this paper: www.ncbi.nlm.nih.gov/pmc/articles/PMC10864075, “HLA-DRB1 Is Associated with Therapeutic Responsiveness in IgG4-related disease”, Motohisa Yamamoto, et al., 23 May 2024:
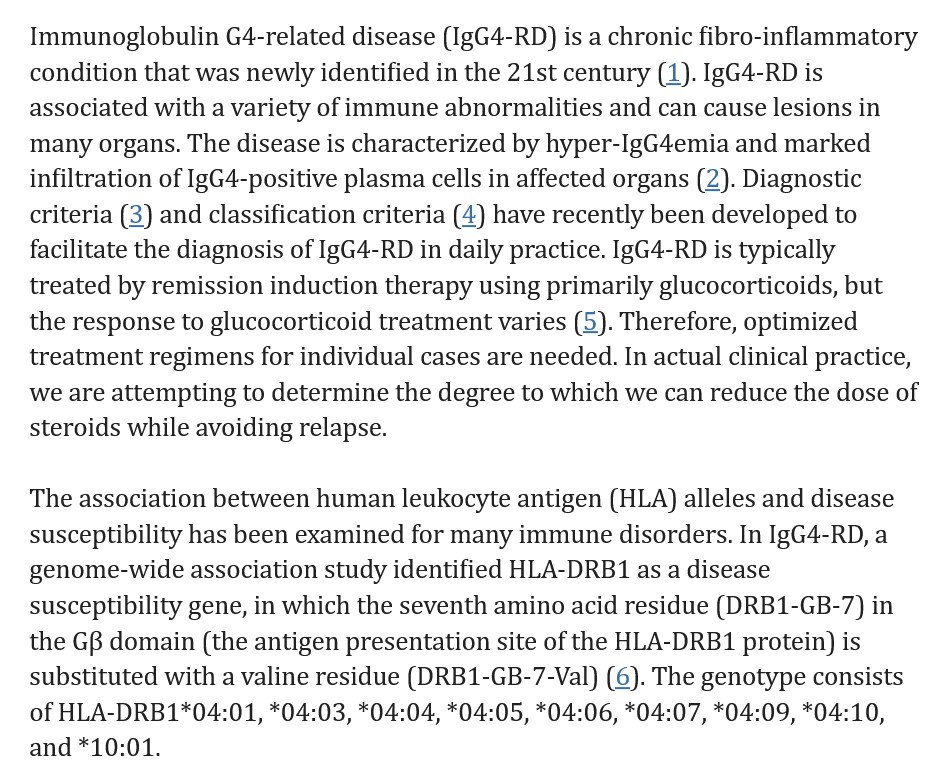
Note that one of the most-recommended and used treatments for IgG4-RD conditions is glucocorticoids (steroids); and that cessation of treatment likely results in relapse of the condition. But, long-term use of glucocorticoids have risks, including high blood pressure and Cushing’s Disease. Please see: www.webmd.com/multiple-sclerosis/what-are-glucocorticoids.
Yours Truly will posit that the lab-created SARS-CoV-2 (COVID-19) virus itself, with the lab enhancements made to the mRNA of this virus to create the modRNA of the COVID-19 “vaccines” (such as the SV40 African Green Monkey cancer promoter gene piece in BNT162b2), plus the addition of dangerous lipid nanoparticles (ALC-0159 and ALC-0315 in BNT162b2 and its “descendant” COVID-19 “vaccines”; and, SM-102 in the Moderna mRNA-1273 modRNA COVID-19 “vaccines” and its “descendant” COVID-19 “vaccines”) and other ingredients in these “vaccines” — have been, and continue to be, designed to wreak as much havoc and damage on the human race as possible. This havoc and damage includes that done to the body’s natural immune system, its elements, mechanisms, and responses. Recall that the “descendant” modRNA COVID-19 “vaccines” use the original (lab-enhanced) SARS-COV-2 (COVID-19) virus modRNA that was present in the earlier versions of these “vaccines”, but in smaller amounts. Therefore, in one’s opinion, the potential exists for immune system damage in persons who take these “descendant” modRNA COVID-19 “vaccines.”
Until fairly recently, it was not known HOW, or the DETAILS behind WHY, the COVID-19 virus itself and the COVID-19 “vaccines” have such potential for havoc and damage — all that was beginning to present were, and are, the ADVERSE EFFECTS of the virus and especially of the “vaccines”: turbo-cancers; miscarriages; Bell’s Palsy; deaths; the Adverse Events of Special Interest listings of negative effects induced by BNT162b2 in the APPENDIX 1. cited above. It is now starting to become more clear as to what SPECIFIC elements likely used in the creation of both the SARS-CoV-2 virus itself, and in the development of the modRNA COVID-19 “vaccines.” Yours Truly will posit that one of these SPECIFIC elements is something that attacks and compromises at least one important component of the human body’s immune system: the antigen site of the human leukocyte protein DRB1 (HLA-DRB1.) It took time, effort, and large amounts of funding to investigate these SPECIFIC elements; to experiment with them to ascertain the damage that could be caused; then, to “insert” these elements into the SARS-CoV-2 virus itself, and, by extension, into the modRNA COVID-19 “vaccines.” And, as the passage of time obscures or obliterates “fingerprints” of the damage done by the COVID-19 “vaccines” in the “vaccinated” individual, the involvement of these “vaccines” may well become harder and harder to trace (even though the damage is continuing in the “vaccinated” person, since one of the mechanisms of said “vaccines” is to change the DNA of the person who takes them.) Below is Slide 14 from the Palmer, MD and Sucharit, MD, article regarding what the COVID-19 “vaccines” do to the “vaccinated” person’s body. Slide 14 shows how the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2 changes the DNA of the “vaccinated” person:
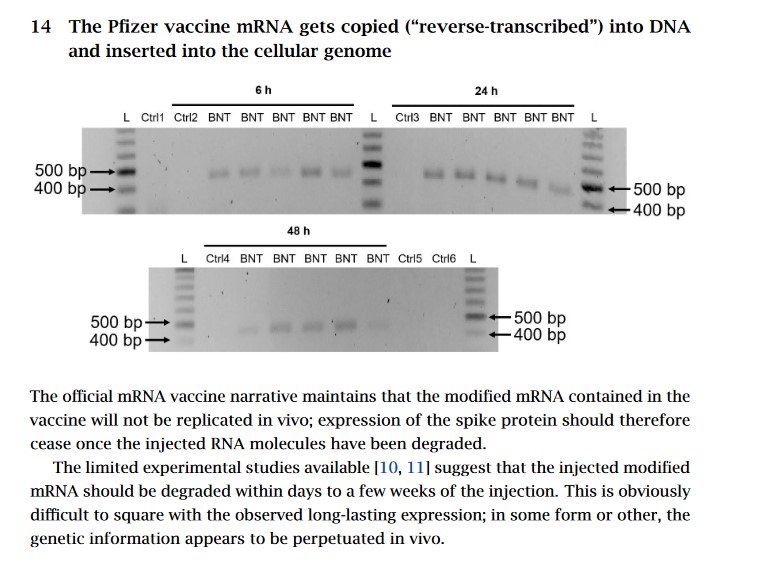
The article is found here: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, by Michael Palmer, MD and Sucharit Bhakdi, MD, 18 August 2022.
Yours Truly will emphasize that it is of the utmost importance that all persons, COVID-19 “vaccinated” or not, have and maintain the highest degree possible of natural immune system health. A healthy diet is one of many ways to support and maintain a healthy natural immune system. Here is an article on this topic: www.medicalnewstoday.com/articles/322412, “The best foods for boosting your immune system”, by Lana Burgess, 10 July 2018. Among other ways to help the natural immune system are lifestyle changes, regular exercise, taking supplements, and addressing stress, as discussed here: www.healthline.com/nutrition/how-to-boost-immune-health, “9 Ways to Boost Your Body’s Natural Defenses”, by SaVanna Shoemaker, RDN, 1 April 2020. Yours Truly will add the opinion that avoiding unnecessary antibiotics and “certain injectables” are additional items to consider.
Peace, Good Energy, Respect: PAVACA