“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
The header image of a vintage laboratory for today’s offering is courtesy of Adobe Stock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Yours Truly has checked today’s offering for AI-generated content. To the best of her knowledge and belief, there is none, except perhaps for AI-generated images embedded in certain links. If readers wish to post AI-generated content to the discussion thread of today’s offering, they must cite their source. Thank you.
Today’s offering contains more proof that, even though the United States government has “officially” paused Gain-of-Function experiments, these experiments are still continuing. Please see: https://www.theqtree.com/2025/08/29/health-friday-8-29-2025-open-thread-gain-of-function-research-is-still-going-on/. This time, there are two separate facilities in the United States that are performing the Gain-of-Function (GoF) work. The first is the new “bat experiments lab” at Colorado State University at Fort Collins, CO. The second is the laboratory at Georgia State University at Atlanta, GA. Bear with Yours Truly: the end of the post is the “punch line.” Yours Truly makes it clear at the start that there is no intent to “cast aspersions” on the research of any of the persons mentioned in today’s offering, or on the current Acting Director of the NIAID.
And, guess what? The “new bat research facility” in Fort Collins also has BSL-2 level labs: A screenshot from the Yellow Scene article is below:
The entire situation at CSU raises other questions: One, will professors ALSO “mix in” with students at this “bat breeding and research” facility? And, Two, why is CSU attempting to be the “United States version” of the Wuhan Institute of Virology, which is what the “new bat research facility” at CSU appears to be?
And, now, turning to the second issue, the continuing Gain-of-Function experiments with Avian Influenza viruses going on in the United States —- this time, at Georgia State University in Atlanta. Please see: https://jonfleetwood.substack.com/p/us-and-south-korean-scientists-lab, “U.S. and South Korean Scientists Lab-Engineer Frankenstein Bird Flu Viruses in Georgia: Journal ‘Virology'”. 14 September 2025. The GoF experiments at GSU, supported by an NIH grant, were performed by South Korean scientists who are ALSO be professors at Georgia State University, with a couple of said professors ALSO having ties to South Korean institutions. Yours Truly will also present **interesting information** regarding the scope of this research at GSU by one particular author of the paper just cited. Please see the screenshot below, from the Fleetwood article:
The paper cited in the Fleetwood article is here: https://doi.org/10.1016/j.virol.2025.110674, “Interferon-y receptor signaling is critical for balanced immune activation and protection against influenza after vaccination”, Sang-Moo Kang, et al., 6 September 2025. A screenshot of the list of the paper’s authors and their affiliations is below, from the paper itself:
Note that the TITLE of the paper does NOT mention what type of influenza was the study subject (in this case, it was Avian Influenza.) More on this aspect later on in today’s offering.
Following are screenshots from sections of the paper that are available online. Note: the entire paper is available only through institutional access, or through paid access.
Note the “clues”: “universal vaccination”; aged populations”; “multiple influenza proteins”; “translational science”; “cross protective efficacy.” However, the “multiple influenza proteins” that were experimented with in the paper cited above were not regular “seasonal flu viruses” — they were strains of H5N1, the Avian Influenza virus.
It appears that Dr. Kang has also used some of the AI154656 NIH grant on other research and papers, such as for this paper: https://doi.org/10.1016/j.vaccine.2025.127206, “Intranasal vaccination with multi-neuraminidase and M2e virus-like particle vaccine results in greater mucosal immunity and protection against influenza than intramuscular injection”, Sang-Moo Kang, et al., Version of Record 7 May 2025. Again, this is “Dr. Kang and his gang” at work; the exception here is that the researchers for this paper are all affiliated only with Georgia State University. And, again, the entire paper is available only through institutional access or through paid access. Keep in mind the emphasis of the paper on “intranasal vaccine delivery.”
This particular paper is the result of Dr. Kang’s, et al., research using another “mixture” of influenza viruses — H1N1 (“swine flu”, a subtype of Influenza A), plus H3N2 (a non-human influenza virus in pigs that can infect humans, https://oklahoma.gov/health/health-education/acute-disease-service/disease-information/influenza-a-h3n2-variant-.html), plus H5N1 Avian Influenza. Screenshots from the “snippets” of this paper that are available online are below: the Abstract; a portion of the Viruses section; and, a portion of the Acknowledgements section:
It appears that the paper purports to prove that the intranasal method of “vaccine delivery” is superior to the current intramuscular (injection) method. It is also clear that experiments that were performed were Gain-of-Function work — this time, combining various Influenza A subtypes (“swine flu” that infects humans; “swine flu” that can infect humans; and, Avian Influenza); plus, Influenza B. It is also clear that these experiments were designed to have maximum effect on the CD4 – CD8 cells and the IgG system. By the way, neuraminidase is an important component in the spread of influenza virus in human lungs. Interferon-y (IFN-y) is an element that is important in the regulation of immune and inflammatory responses, among other functions.
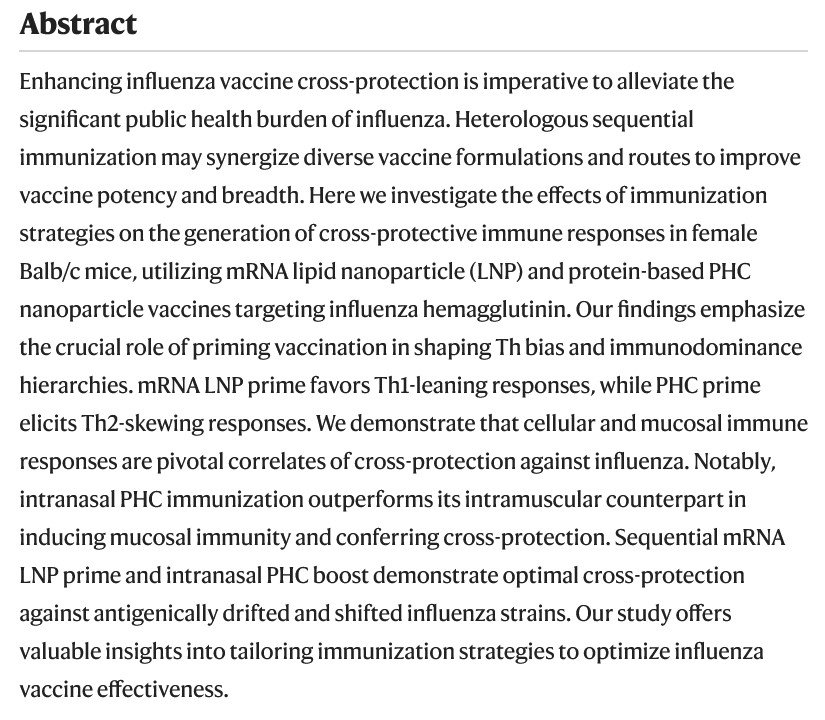
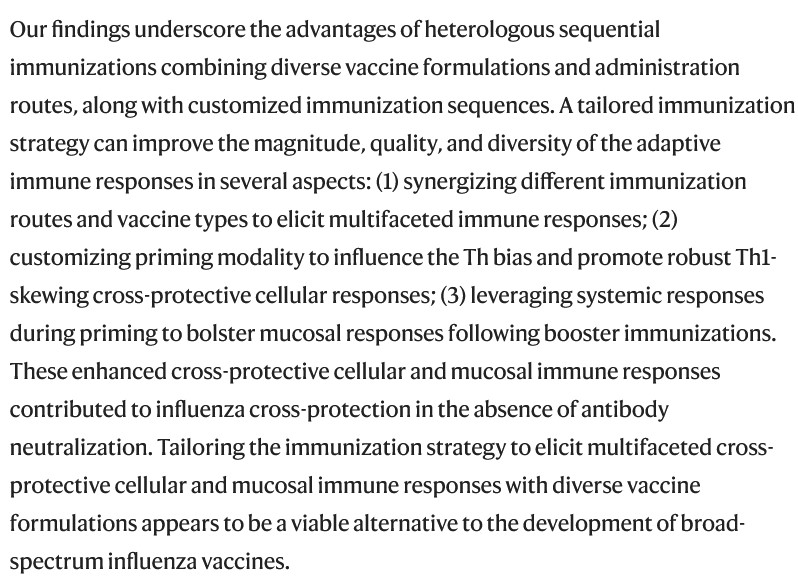
**** There is one more paper by “Dr. Kang and Gang” at GSU that bears scrutiny; this one, published in July 2024: https://doi.org/10.1038/s41467-024-50087-5, “Enhancing cross-protection against influenza by heterologous sequential immunization with mRNA LNP and protein nanoparticle vaccines”, Sang-Moo Kang, et al., 10 July 2024. This paper describes Gain-of-Function experiments not only with various influenza viruses (H3N2 and H7N9 [H7N9 is an Avian Influenza virus that is particularly lethal to humans who get infected with it]); it also describes what can only be Gain-of-Function experiments with “delivery methods” for the TWO different kinds of influenza “vaccines” that use EITHER lipid nanoparticles, OR use PHC (a protein-based nanoparticle.) Several screenshots from this paper are below, starting with the Abstract; then, Figure 1.; followed by a portion of the Discussion section:
The LNPs (lipid nanoparticles) used in the “mRNA initial series vaccine” in the experiments in the above paper are: DOTMA (cationic lipid, used in gene therapies, enhances gene transfection); DOPE (enhances intracellular “delivery” of the “vaccine” ingredients); and, DMG-PEG2000 (nanoparticle version of polyethylene glycol; one of the two LNPs in the Moderna modRNA COVID-19 “vaccines”, the other being SM-102.)
It appears that this paper describes how a “multi-delivery method” of a 2-injection series of a modRNA influenza “vaccine”, followed by a 1-dose “booster” of an intranasal modRNA influenza “vaccine”, is the “optimal” method for “cross-protection” against infection.
The “PUNCH LINE” section of today’s offering follows:
**** In fact, it appears that the above paper claims that modRNA influenza “vaccine” intramuscular injection (IM injection) is now to be considered as “priming the pump” for the subsequent use of modRNA intranasal delivery of the influenza “vaccine” in order to have “sufficient protection” against infection. In other words — TWO types of “delivery methods” need to used.
The above paper was funded by NIH grants R01AI101047 and R01AI143844 to “Dr. Kang and Gang” researcher Bao-Zhong Wang. Dr. Wang, by the way, seems to be from Communist China, having earned his PhD from the Chinese Academy of Sciences in 2003.
Which brings Yours Truly back to the “Broadly Protective Influenza Vaccine” Patent that is owned by Dr. Jeffery Taubenberger, a “career employee” of the NIH who is now the Acting Director of the NIAID. Yours Truly has written about this scientist in the Health Friday offering of 29 August 2025, cited above in today’s offering. This is the “Universal Influenza Vaccine” that Dr. Taubenberger developed at the NIH: https://www.techtransfer.nih.gov/tech/tab-3388, “Broadly Protective Influenza Vaccine Comprising a Cocktail of Inactivated Avian Influenza Viruses”, published 6 July 2020. A screenshot from this page is below:
Note the “intranasally or intramuscularly” in the above statement.
All of the foregoing appears to point in the direction of a “universal influenza vaccine” that includes various types of influenza viruses (“swine flu”; Avian influenza; Influenza B); that would require at least three doses of a “vaccine” to have “sufficient protection”; and, that the “delivery methods” of the three doses appears to be 2 intramuscular injections of a modRNA plus cationic lipid nanoparicles “vaccine” to “prime the pump”, plus 1 “booster dose” of an intranasal modRNA plus PHC-nanoparticle “vaccine” to “provide sufficient protection” from infection. And, that this situation is being “influenced”, so to speak, by the “new direction” of the NIAID, led by Acting Director Dr. Jeffery Taubenberger.
One must ask: Why is there so much emphasis on a “universal influenza vaccine” that combines elements of “swine flu” viruses, of various Avian Influenza viruses, and, of the Influenza B virus? Why is there an emphasis on “aged populations” in the Gain-of-Function experiments described above in today’s offering?
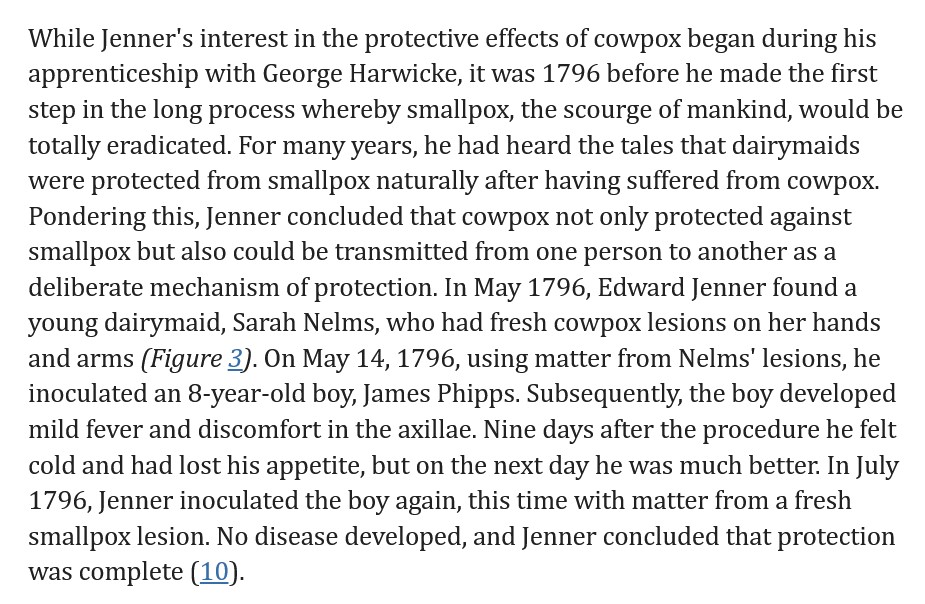
The above is a vintage image of Dr. Edward Jenner administering the first smallpox vaccination (inoculation) to James Phipps, 14 May 1796. Courtesy of www.sciencemuseum.org.uk/.
Today’s post, as it relates to the disaster of COVID-19 and the COVID-19 “vaccines”, is dedicated by Yours Truly in memory of her cousin Bill, who died “suddenly and unexpectedly” in September 2023. However, the discussion is not limited to what is presented here: it is an Open Thread.
There are two separate, although connected (Big Pharma), parts to today’s offering. Each part is of itself an expose’. This post is a long one, but important. Please, take a cup of coffee or tea; or, if it’s an appropriate time of the day, perhaps a “wee dram” of something like chilled D.O.M. Benedictine with a twist of lemon peel, and settle in for reading.
Readers already know the caveats regarding civil discussion on this board; of the alternate sites in case the main board is not accessible (here and here); and, that what Yours Truly presents on Health Friday is not medical advice, but opinions and/or hypotheses from ongoing research on COVID-19, Big Pharma, and other health topics.
“Quick, down-and-dirty summary” of today’s post:
One: Pfizer-BioNTech has begun a new enterprise, PfrizerForAllTM, which apparently seeks to completely circumvent / marginalize, in-person consumer contact with pharmacies; to “funnel” in-person consumer contact with healthcare practitioners to “Pfizer-affiliated” professionals; and, to “redirect” the dissemination of information about the COVID-19 “vaccines” to that provided by Pfizer-BioNTech.
Two: That the FDA approval of the very dangerous and deadly Smallpox “vaccine”, ACAM2000, for use also as a “prevention” for Mpox, is the result of a complex mixture of Big Pharma influence + FDA review of the Biologics License Applicaion for this use of ACAM2000 that is, in Yours Truly’s opinion, “a foregone conclusion despite serious reservations”, to say the least + Gain-of-Function experiments on the Mpox virus. There is also a potential tie-in to “an expanded biodefense role.”
Yours Truly has tried to avoid making today’s post read like a scientific paper; however, there is a lot of information that is relevant to each Expose’. Note: Mpox is now the “official” name for monkeypox.
Expose’ One: It appears that Pfizer-BioNTech is creating new ways to increase the company’s consumer operations (and, therefore, potential profit lines.) Pfizer-BioNTech has just launched PfizerForAllTM — a direct sell-to-consumer business that will provide online access to healthcare providers (online [virtual], or affiliated healthcare providers encounters [for example, to get a COVID-19 “vaccination”]); plus, “delivered to your door” prescription drugs and “easier access” to other company products, such as their COVID-19 “test kits.”
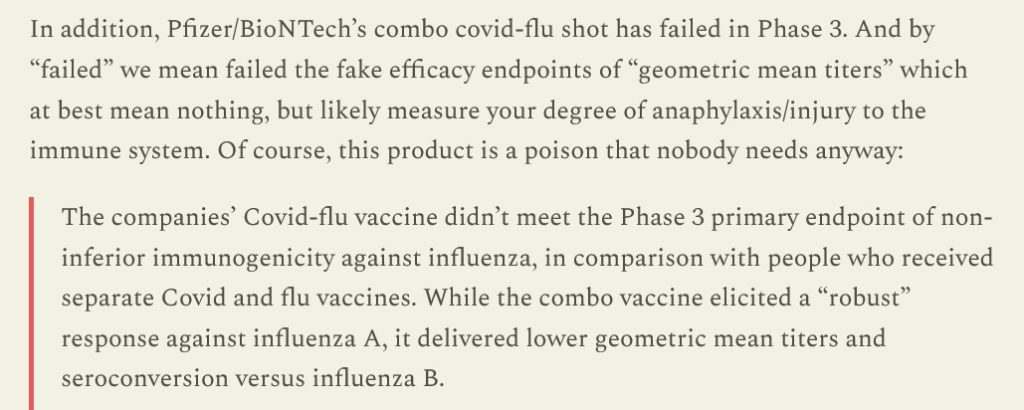
In other words, in Yours Truly’s opinion, Pfizer-BioNTech, not happy with the company’s portfolio loss due to falling consumer acceptance of the modRNA COVID-19 “vaccines” offered, and due to the failure of the company’s clinical trial of its “combo” modRNA COVID-19 “vaccine” + influenza “vaccine”, a corporate decision was made to find a way to go straight to the consumer and make it “so easy” to get access to the “vaccines”, plus other Pfizer products. Translation: banish “vaccine” hesitancy / “vaccine” refusal, by doing what may be called “straight to the consumer medical psy-op.” Again, from the Latypova article:
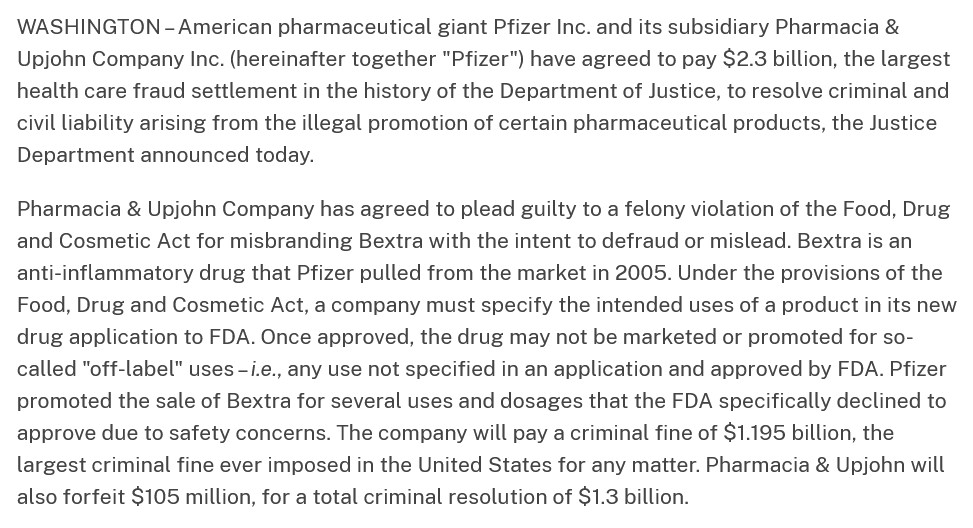
The lawsuit that Pfizer-BioNTech settled in 2009 was over the use of the company’s drug, Bextra, in “off-label” situations. The scope of the settlement is described here: www.justice.gov/, “Justice Department Announces Largest Health Care Fraud Settlement in Its History”, 1 November 2023. A portion of the announcement is below:
This lawsuit was the starting point for FDA changes to its “regulations” regarding the use of prescription drugs in “off-label” situations. The latest FDA changes are summarized here: www.sidley.com/en/insights/newsupdates/2023/11/fda-s-latest-off-label-guidance, 1 November 2023. It appears, in a nutshell, that drug manufacturers can be held responsible (liable) for “off-label” use of their products, even if they already comply with the “new” FDA “regulations.” (Think of this in light of the use of, for example, Ivermectin or Hydroxychloroquine to prevent or to treat COVID-19 — these uses, arguably, are “off-label” for these drugs.)
By the way, PfizerForAllTM is working with UpScript Health and Alto Pharmacy regarding access to healthcare services and filling prescriptions. Guess what? UpScript Health lists Pfizer as a “partner” on the company’s “About” page of their website: www.upscripthealth.com/about/. And, there’s more — Alto Pharmacy, the online prescription drug company, has a couple of interesting members on their Board of Advisors: Alex Azar (HHS head under then-President Trump); and, Dr. Ezekiel Emanuel (he who helped to write the “ObamaCare” bill; he who advocated for people to take their own lives at age 75 “to make room for the younger generation”, and more): www.alto.com/our-company. Dr. Emanuel is also involved with the Center for American Progress (Soros-connected: www.americanprogress.org/c3-our-supporters/); The Aspen Institute; and, he is Co-Director of the Healthcare Transformation Institute (HTI) at the University of Pennsylvania. Below is the Mission statement of HTI (https://hti.upenn.edu/mission/):
Note 1: the “objective” to transform the behavior of physicians and other healthcare providers. (Italics, mine.) Note 2: the “imagifashion” hyperlink, apparently, after getting past the “fake Latin language” on the main page, takes one to a clothing/accessories company in California: https://nilah.la-studioweb.com/contact-us/. (??)
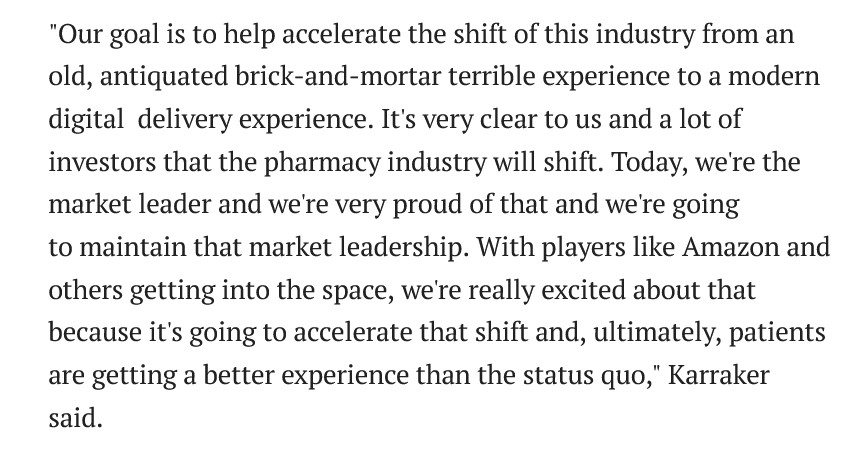
This statement really frosts Yours Truly. My late father was a Registered Pharmacist for 57 years, who: kept his pharmacy very clean and neat (one was part of the crew that swept the floors and cleaned the display shelves starting when she was 10 years old); made it a point to know about all of his patients and to TALK with with then they came to have prescriptions filled or refilled; worked out deals with his suppliers to get extra samples of OTC products to give to his patients who had lost their steel mill jobs when the mills left Pittsburgh in the late 1970s-early 1980s, and, who paid for their prescriptions with his own money at times, etc., — finds the language, “…brick-and-mortar terrible experience…” in the above statement not only to be personally insulting to the memory of her father: but, also, degrading to those “brick-and-mortar” pharmacists who do their job to keep their stores clean and organized.
Expose’ Two: This regards the FDA just “approving” the “expanded use” of the dangerousand deadly Smallpox “vaccine”, ACAM2000, for the “prevention” of Monkeypox (now called “Mpox.”) The FDA issued this “approval” on 29 August 2024. The trail on this begins here: https://mole.substack.com/p/acam2000-package-insert-warning-death, 14 September 2024.
To gain more understanding of Smallpox and inoculation / vaccination against Smallpox, please see: www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination. Both Smallpox (variola) and Mpox (mpox virus) are members of the genus Orthopoxvirus. Whereas, a disease condition that would equate to Smallpox goes at least as far back as to China around 3000BC, Mpox was first discovered in 1958 (all, per Wikipedia search.) Dr. Edward Jenner, an English physician, noticed that milkmaids were immune from Smallpox infection; he deduced that the Cowpox infections that they sustained had made them immune to the other type of infection. Dr. Jenner administered the first “inoculation” of Cowpox virus (to prevent Smallpox) to a child, James Phipps, on 14 May 1796. Another source of information is here: wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/smallpox-and-other-orthopoxvirus-associated-infections. Further details are found here, in the article, Edward Jenner and the history of smallpox and vaccination, January 2005. A screenshot of a portion of this article is below:
About ACAM2000: it is manufactured by Emergent BioSolutions, headquartered in Gaithersburg, MD. The FDA approved ACAM2000 for use for the prevention of Smallpox in August, 2007. It contains vaccinia, a live virus ingredient used in modern Smallpox vaccines. The vaccinia used in ACAM2000 is a replicating version. The vaccine is cultured in a mixture of African Green Monkey kidney cells (sound familiar? — as in, perhaps, SV40 African Green Monkey cancer promoter gene splice that was found in the Pfizer-BioNTech modRNA COVID-19 “vaccine” by Dr. Kevin McKernan?). ACAM2000 was originally only intended for use to prevent Smallpox — until its use was “suddenly expanded” on 29 August 2024 by the FDA to include prevention of Mpox (more on that later in the post.) Since then, articles such as this one have appeared (https://childrenshealthdefense.org/defender/fda-acam2000-mpox-vaccine-warning-death-unvaccinated/, 17 September 2024, by Suzanne Burdick, Ph.D.; and, social media has been posting items like this one: https://x.com/toastontheside/status/1835921932841062412. This tweet references the FDA-issued handout for patients and/or caregivers regarding ACAM2000. The FDA handout is found here: www.fda.gov/media/75800/download. FDA handout documents for patients and/or caregivers are likely to have, in Yours Truly’s opinion, “sanitized” information and “pablum-like” assurances regarding the “safety and efficacy” of the drug or injectable. The FDA handout for ACAM2000, however, is different: when one reads the handout, one gets a distinct impression that this “vaccine” is highly dangerous. Below is a screenshot portion of the FDA patient/caregiver handout for ACAM2000:
Note that there is NO MENTION of the other FDA-approved Mpox vaccine, JYNNEOS, which is arguably “safer” for the patient (see further down in the presentation regarding JYNNEOS.)
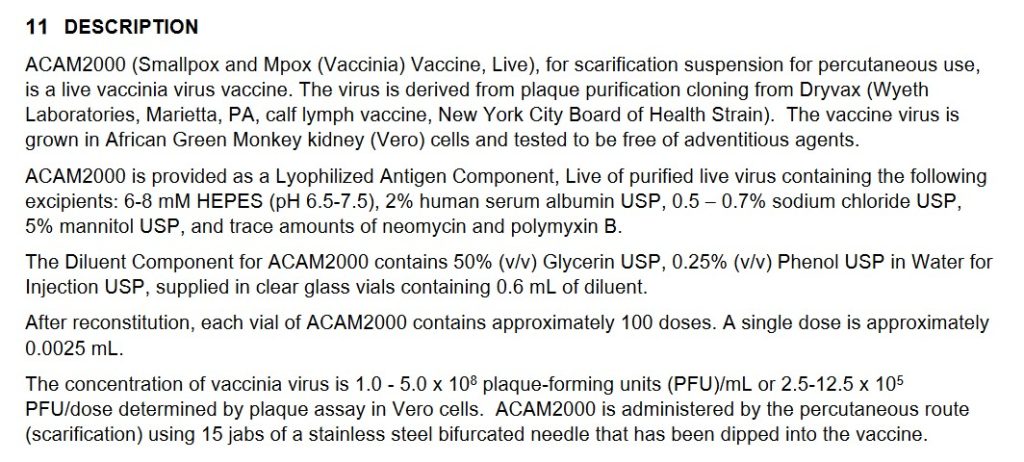
The Fact Sheet for Healthcare Providers for ACAM2000 is here: www.fda.gov/media/75792/download. The document gives a much more comprehensive picture of the dangers of this “vaccine.” Yours Truly will highlight a few of the items in this document which show how dangerous and deadly this vaccine is, beginning with two images from page 1 of the Fact Sheet: the Black Box Warning; and, the Warnings and Precautions:
Remember, this dangerous and deadly “vaccine” is now approved for persons “at risk for Mpox”, in addition to persons at risk for Smallpox (this disease was eradicated in 1980.)
And, from Section 6 Adverse Reactions portion of the Fact Sheet for ACAM2000:
Continuing with Section 11 Description from the Fact Sheet for ACAM2000:
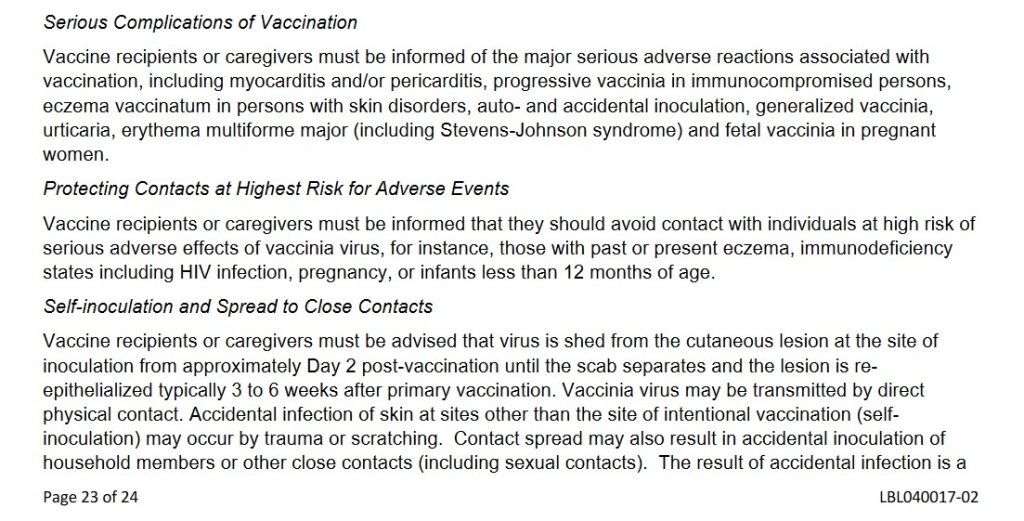
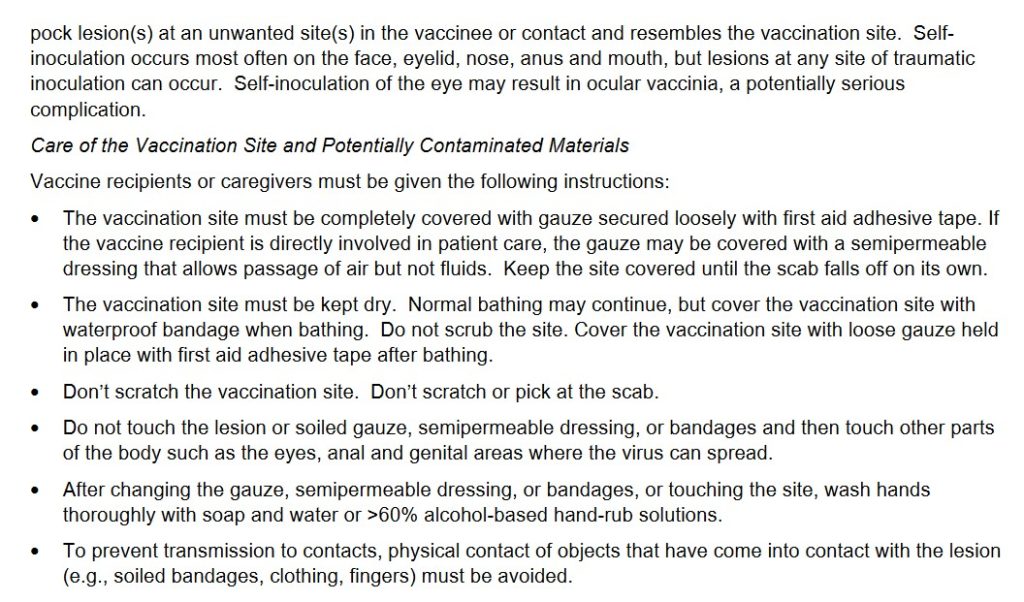
And, from Section 17 Patient Counseling Information of the Fact Sheet for ACAM2000, two portions:
Note several items from the above screenshots: One, that the “vaccine” must be given to the recipient via 15 separate jabs with a bifurcated needle; Two, there are MULTIPLE adverse reactions potential for persons taking this “vaccine”; Three, that persons who contract a Smallpox infection from a person “vaccinated” with ACAM2000 can die of the infection they contract; Four, that the ACAM2000-“vaccinated” person must stay away from pregnant women, household members, persons with eczema, etc., for a period of time after “vaccination”; among many other issues.
Yours Truly will again recall to the reader’s mind that ACAM2000 is now FDA-approved for PREVENTIVE USE among persons who are at risk for Mpox. From what Yours Truly has read about it, Mpox is, for all intents and purposes, likely to be a LESS-DANGEROUS form of Orthopoxvirus, compared to another form of the same Genus, variola (Smallpox virus.) [HOWEVER, see the presentation answering Question Two, further below in the post.] There is a vaccine that was previously FDA-APPROVED for the prevention of Mpox — JYNNEOS, manufactured by Bavarian-Nordic. This vaccine also uses the vaccinia virus as the foundation; but, JYNNEOS is cultured in a mixture of chicken embryo cells; and, although it also has live vaccinia, it is a NON-replicatingversion. JYNNEOS was also originally FDA-approved for the prevention of Smallpox. In Yours Truly’s opinion, even though JYNNEOS does indeed have potential for serious adverse reactions (for example, cardiac issues), this vaccine appears to be much less dangerous and deadly compared to ACAM2000. The FDA Fact Sheet for Healthcare Providers for JYNNEOS is here:www.fda.gov/131078/download.
Two questions arise immediately: First, what is about ACAM2000 that makes it so dangerous?; and, Second, why did the FDA suddenly approve the use of ACAM2000 for the prevention of Mpox in August 2024?
As to the first question: ACAM2000 is the “descendant Smallpox vaccine” from the older Dryvax Smallpox vaccine, which was manufactured by Wyeth. ACAM2000 replaced Dryvax in August 2007, after FDA approval. The Package Insert (archived version) for Dryvax is here: https://biotech.law.lsu.edu/blaw/bt/smallpox/dryvax_label.htm. Below are two screenshots from the Package Insert for Dryvax:
Note that the inoculation process for Dryvax consisted of 2 or 3 punctures for the initial (primary) vaccination; and that 15 punctures were used for revaccination. However, ACAM2000 requires 15 punctures for the initial vaccination. Why 15 punctures for the initial vaccination? It would appear, in Yours Truly’s opinion, that requiring 15 punctures for the initial vaccination with ACAM2000 exposes the patient to more of the ingredients of the vaccine (think the Moderna COVID-19 modRNA “vaccines”all having more than 3 times the “mcg payload” of lab-enhanced SARS-CoV-2 spike protein PER INJECTION, as compared to the “mcg payload” of the Pfizer-BioNTech modRNA COVID-19 “vaccines.” [Which is NOT to say that the Pfizer-BioNTech modRNA “vaccines” are somehow “safer” than those of Moderna. THEY ARE NOT.])
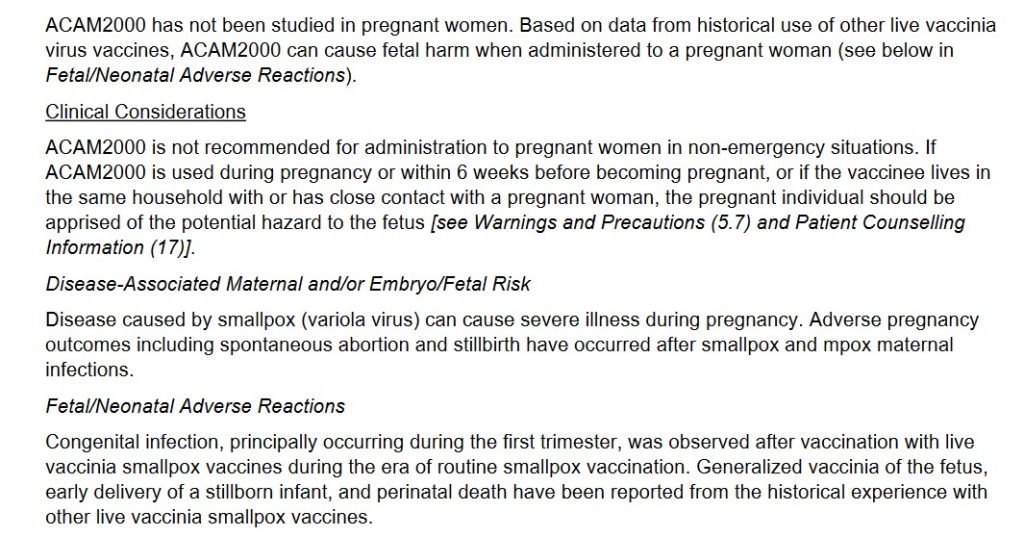
Yours Truly turns to section 8.1 of the FDA Fact Sheet for Healthcare Providers for ACAM2000 (link above.) This “vaccine” is particularly dangerous to pregnant women, to women who wish to become pregnant, and to a fetus carried by a pregnant woman (whether or not she is “vaccinated” with ACAM2000, since persons “vaccinated” with this product will “shed” ingredients [from the forming / formed pustule, or the scab from the pustule, etc.], onto other persons who come into contact with the “vaccinated” person.) Below is section 8.1:
It would also appear that there is inherent danger due to the fact that ACAM2000 uses a live, replicating vaccinia (another Orthopoxvirus that is “weaker” than variola [the Smallpox virus], and which is used to make modern-day Smallpox / Mpox vaccines), as compared to the live, NON-replicating vaccinia that is used the JYNNEOS Smallpox / Mpox vaccine. Once inoculated (vaccinated) with ACAM2000, the vaccinia produces a kind of “mini-infection” in the patient, affecting the area around the inoculation site, along with the lymph nodes in the same area. Vaccinia may also appear in the blood of the patient. There is also the issue of “self-inoculation” by the ACAM2000-“vaccinated” patient (from scratching or “picking at” the scab that forms after the “mini-infection” pustule forms on the skin, and also when this pustule begins to clear); and for other reasons — the FDA Fact Sheet section 17 Patient Counseling Information for ACAM2000 discusses this. In addition, there is the varying amount of vaccinia concentration that is produced in the patient after ACAM2000 inoculation; see below from section 11 Description of the FDA Fact Sheet for Healthcare Providers:
In other words, there are many areas about the ingredients and mechanisms of ACAM2000 that raise the risk of complications, including death, for the patient who takes this “vaccine”, for pregnant women and their fetuses, for women who wish to become pregnant, for persons who are immunocompromised, and for persons who are NOT “vaccinated” with ACAM2000, during the multiple “danger zone” weeks after ACAM2000 inoculation.
Turning to the second question, concerning the FDA approval in August 2024 for ACAM2000 to be used as an Mpox “vaccine”: this situation is complex. It involves Big Pharma, the WHO, and, what to Yours Truly “smells like” Gain-of-Function research, among other items.
Yours Truly will begin with Emergent BioSolutions, the company that produces ACAM2000. Emergent BioSolutions, a “global enterprise” with headquarters in Gaithersburg, MD, was established in 1998. Its first project was to partner with the United States Defense Department to supply the Anthrax vaccine that was administered to members of the military (www.emergentbiosolutions.com/about-us/.) The current CEO of the company is Joseph C. Papa. Mr. Papa’s most-recent position was CEO of Bausch + Lomb, another large Big Pharma company. Mr. Papa, apparently, is a “mover and shaker” in the pharmaceutical industry. However, it is also apparent that Baush + Lomb was in financial trouble when he left it to become CEO of Emergent BioSolutions. In fact, Bausch + Lomb is “exploring” selling off some of its pharmaceutical assets, due to “significant debt load” (https://finance.yahoo.com/news/bausch-lomb-explores-sale-amid-112230409.html.) Perhaps, the company’s Post-IPO debt funding was not enough: www.crunchbase.com/organization/bausch-lomb/company_financials; scroll down to “Investors.” Mr. Papa has Bachelor’s and Doctorate degrees in Pharmacy; his career includes working with many Big Pharma companies (Novartis, Cardinal Health, and Watson Pharmaceuticals, among others.) Please see his entry in Wikipedia; and, here: https://waterstreet.com/people/papa-joseph. Water Street (Water Street Healthcare Partners) is an investment company that has a portfolio worth approximately $6Billion spread across healthcare services companies, medical diagnostics companies, and pharmaceutical/life sciences companies (https://waterstreet.com/companies.)
Mr. Papa was hired on 21 February 2024 by Emergent BioSolutions to facilitate the financial turnaround of the company. Below is a screenshot of the company’s financials from September 2023 to September 2024, via Crunchbase. It appears that Mr. Papa, a “mover and shaker” in the Big Pharma world, is working hard:
Also, via Crunchbase, a snapshot of Emergent BioSolution’s funders:
It appears that now, Mpox is being “re-classified” as another, although serious, sexually-transmitted disease that can infect any sexually-active person; and, that Mpox has apparently “made the leap” from monkeys to other animals (rodents and even to domesticated dogs), and to between animals and humans. This leads to another aspect of the situation: Yours Truly’s suspicion that there have been / are ongoing, Gain-of-Function experiments on Mpox.
Here is the “fast and dirty” summary on Gain-of-Function experiments with Mpox:
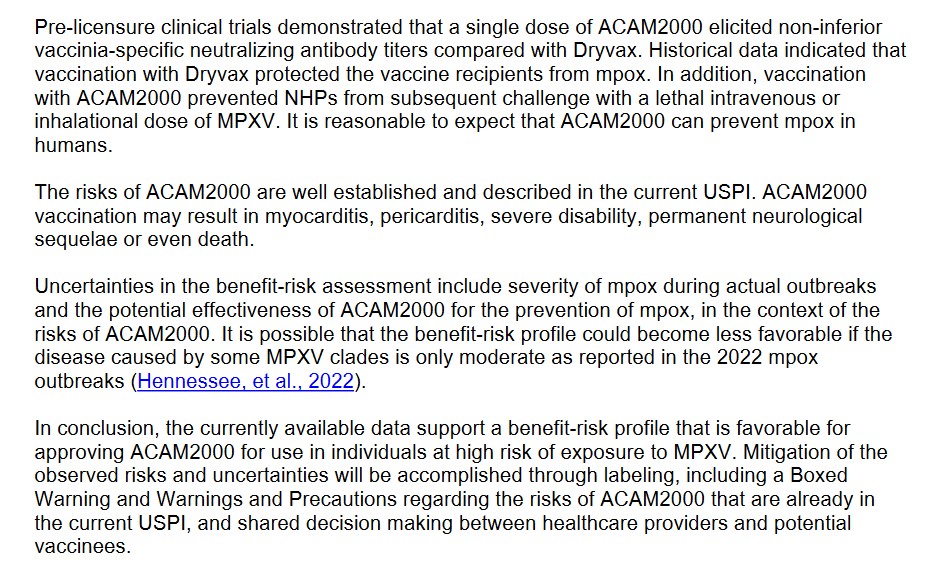
One: Up until 22 August 2024, the FDA had only ONE approved “vaccine” for Mpox: JYNNEOS. However, on that same day, the FDA conducted a “review” of the BLA Application (Biologics License Application) for ACAM2000 to have approval as a “vaccine” for Mpox. This application was approved on 29 August 2024 (www.fda.gov/news-events/press-announcements/fda-roundup-august-30-2024.) Please see: www.fda.gov/media/181552/download for the BLA review. The FDA reviewers, apparently, had some “reservations” about ACAM2000 — see the screenshot below:
Despite the multiple reviewer comments regarding the BLA for ACAM2000, the FDA approved it anyway for Mpox “prevention.” In fact, look at THIS, from section 11.2 of the ACAM2000 BLA document, below:
Two, the Gain-of-Function issue regarding Mpox: First, the CDC connection:
The CDC has an updated report on the incidence of Clade II infections of Mpox, an outbreak that originated in Central Africa (more on Clade II of Mpox further down in today’s post): www.cdc.gov/, “Clade II Mpox Outbreak Originating in Central Africa”, 13 September 2024. Per this article, there are no Clade I Mpox infections in the United States at this time; however, there are 2466 reported cases of Clade II Mpox infections, with 7 deaths. There are also, per the CDC report, cases of Clade II of Mpox literally all over the world at this time.
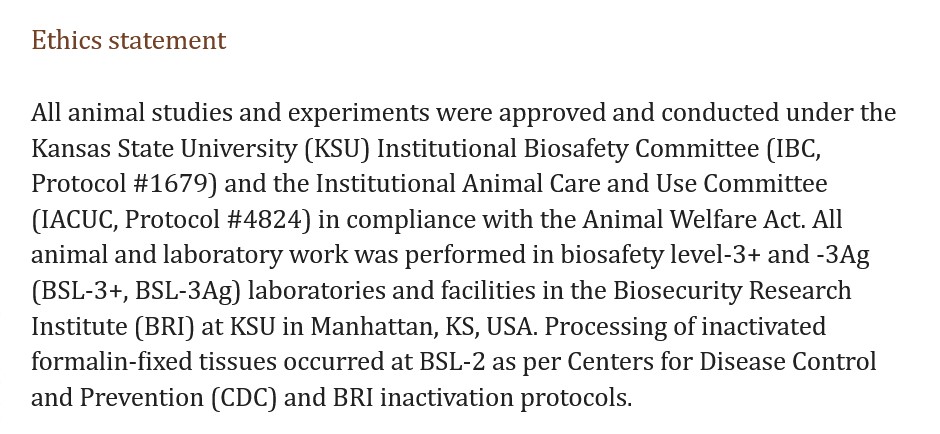
Here is an example of Gain-of-Function experiments with the Clade II of Mpox. This paper is about a study conducted at Kansas State University in which pigs were exposed to the Clade II of Mpox to see if they would get sick, and then take various blood and biological samples and test them. Sure enough, the pigs contracted Mpox. Please see: www.ncbi.nlm.nih.gov/pmc/articles/PMC11168330/, “Experimental inoculation of pigs with monkeypox virus results in productive infection and transmission to sentinels”, Emily Mantlo, et al., 7 May 2024. “Sentinels” were the pigs who were not injected with the Clade II Mpox, but were put in the same cages as those pigs who were. The “sentinel” pigs also came down with Mpox (in other words, animal-to-animal transmission of the virus.) Below are the Ethics Statement and the Funding Statement for this study:
Note that the study was conducted in BSL-3 labs at KSU; that tissue-processing was performed at CDC BSL-2 facilities; and, that, apparently, college students were working in the BSL-3 labs in the study. This indicates that Gain-of-Function experiments with the Clade II of Mpox were being performed; that lower-level biosafety labs were used; and, that college students were involved (how much close supervision was provided by KSU?)
So, Gain-of-Function experiments are being performed using the Mpox virus; experiments funded by the NIH. A very dangerous, deadly Smallpox “vaccine”, ACAM2000, was suddenly FDA-approved for the “prevention” of Mpox. The “definition” of who is “at risk” for an Mpox infection has been “expanded” to include all persons who are sexually active. The Clade II of Mpox (the one that is the subject of the Gain-of-Function experiments) is now infecting people all over the planet, including in the United States. And more. Cui bono? How many of the general public will line up for an injection of ACAM2000 because the CDC / FDA / AMA / Establishment Medicine, will issue a warning due to “increasing numbers of infections being reported of Mpox?” How many healthcare professionals will be “mandated” into taking ACAM2000 “to protect themselves and the patients they care for?” (Again, JYNNEOS was already approved for Mpox “vaccination”, and it is ** potentially ** a “safer” alternative “vaccine.”) How many more Gain-of-Function experiments will be conducted, not in facilities like the Wuhan Institute of Virology or the Baric Lab at UNC Chapel Hill — but at places like the BSL-3 Ag Lab at Kansas State University (a facility where, arguably, one would expect research on, say, equine viruses, not Clade II Mpox experiments on pigs)? How much more Gain-of-Function experimentation will be hidden and/or “obscured” from public knowledge, let alone from Congress?