Our mission, as God-fearing and God-loving patriots, is to defend this Constitutional Republic and to increase its greatness, in all good things and ways, by using our voices in free but courteous speech, by discussing the happenings of the world and coming to a profound understanding of those things, and by sharing and promulgating these Truths on both this platform and others.
The header image for today’s offering is courtesy of Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: there is AI-generated material in The Focal Points and the 2nd Smartest Guy In The World articles in today’s offering. If readers wish to post AI-generated material in today’s discussion thread, they must cite their source. Thank you. Special thanks to our “sister blog”, https://www.marica1776.com/, for some of the items in today’s offering.
A personal note: On this date in 1947, a man named Samuel, and a woman named Catherine, were married at 10:30AM in a church ceremony in Pittsburgh, PA. It was a Thursday. They left right after the wedding breakfast for their two-and-a-half day honeymoon at Niagara Falls, NY. Samuel had to be back at work the following Monday as a pharmacist’s apprentice while finishing his studies at Pharmacy school; and, Catherine also had to be back at work the following Monday as a secretary. They set up housekeeping in their first home: a two-room apartment (with a shared bathroom) in a reconverted old house in the Shadyside section of Pittsburgh. Samuel and Catherine were Yours Truly’s parents. I believe they’re having a wonderful time together in the next world. Love you, Daddy and Mother. Miss you. Thank you — Thank you.
>>>>>>>>>>>>>>>>>>>>
Some Interesting Items from the plethora of news out there:
Ebola:
**** From The Focal Points: https://www.thefocalpoints.com/p/nih-ebola-expert-under-fbi-investigation, “NIH Ebola Expert Under FBI Investigation for Smuggling Pathogens Into America From the Congo”, Nicolas Hulscher, MPH, 20 May 2026. It appears that Dr. Vincent Munster, returning from a trip to the Democratic Republic of the Congo (and accompanied by another NIH employee), was detained at the airport when returning to the United States for attempting to bring undeclared dangerous pathogens back in his luggage. Dr. Munster’s lab at the NIH “specialized” in the study of, and experimentation with, the Ebola virus. He is also one of the co-authors of the rejected 2018 DEFUSE proposal — along with Dr. Peter Daszak AND Dr. Ralph Baric. Please see the article for more information. There is also an interview with Mr. Hulscher that is included. (Yours Truly: One wonders if the situation with Dr. Munster could be a “data point” in the “sudden resignation” of the now-former Acting Director of the NIAID — Dr. Jeffery Taubenberger, the Fauci acolyte and “inventor” of the “Universal Influenza Vaccine” in 2020 [while Dr. Taubenberger was working at the NIH]: https://www.usnews.com/news/health-news/articles/2026-05-22.acting-niaid-chief-steps-down-amid-ebola-hantavirus-concerns.)
**** Again, from The Focal Points: https://www.thefocalpoints.com/p/the-bedrock-of-containment-why-sanitation, “The Bedrock of Containment: Why Sanitation is the Key to Controlling Ebola”. Peter A. McCullough, MD, MPH, 25 May 2026. The scientific paper referred to in the article is here: https://doi.org/10.1186/s12889-020-8240-9. “Hygiene programming during outbreaks: a qualitative case study of the humanitarian response during the Ebola outbreak in Liberia”; Alexandra Czerniewska and Sian White. 2020.
**** And, last but not least, the involvement in Ebola virus experiments by the now-fired (“retired” for “no reason disclosed”) and disgraced “Eminence Grise” of the COVID-19 disaster: Dr. Ralph Baric, PhD; experiments that used Gain-of-Function techniques. Dr. Baric authored the following papers: the first, at approximately the same time that the 2014 Ebola outbreak was raging; the second, in 2024: https://pmc.ncbi.nlm.nih.gov/articles/PMC4241145/, “Host genetic diversity enables Ebola hemorrhagic fever pathogenesis and resistance”; Ralph Baric, PhD, et al. 30 October 2014; and, https://doi.org/1016/j.celrep.2024.114127, “Mapping of susceptibility loci for Ebola virus pathogenesis in mice”; Ralph Baric, PhD, et al. 28 May 2024.
>>>>>>>>>>>>>>>>>>>>
Ticks:
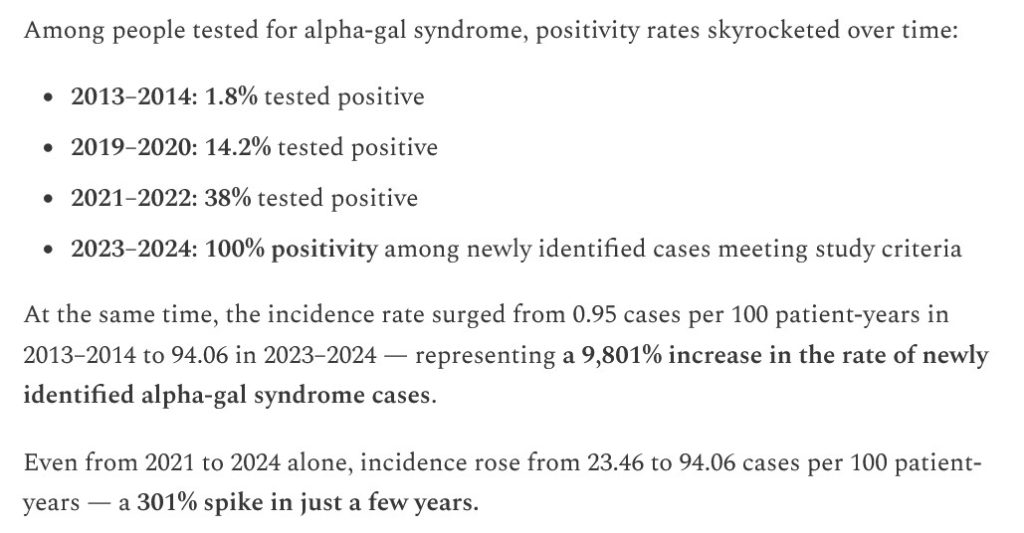
**** From The Focal Points: https://www.thefocalpoints.com/p/study-tick-borne-alpha-gal-syndrome, “STUDY: Tick-Borne Alpha-Gal Syndrome Incidence Skyrocketed 9,800% in the U.S. Since 2013”, Nicolas Hulscher, MPH, 22 May 2026. Please see the screenshot, below, from his article:
**** From 2nd Smartest Guy In The World: https://www.2ndsmartestguyintheworld.com/p/lyme-and-lone-star-bioweapon-diseases-33d, “LYME & LONE STAR BIOWEAPON DISEASES UPDATE: “This Tick Thing is Nuts” & Since 2013 Alpha-Gal Syndrome Incidence Skyrocketed 9,800%”, 24 May 2026. This article quotes the Hulscher post cited above, and also includes more information from other sources.
**** “And now, for something completely different”: the “contrarian view” from Sasha Latypova: https://sashalatypova.substack.com/p/trick-ticks-fear-porn-to-cover-up, “Weaponized Ticks!!!, a mini review”, 25 May 2026. Ms. Latypova argues that Alpha-Gal Syndrome is actually caused by immune system damage induced by vaccines.
Yours Truly will weigh in on the latter: One: there has been a huge increase in reported diagnoses of Alpha-Gal Syndrome since the rollout of the COVID-19 bioweapon “vaccines” in 2021. Two: the COVID-19 bioweapon “vaccines” induce or aggravate multiple types of immune and/or autoimmune disorders: see https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, regarding BNT162b2 (COMIRNATY), FDA date-stamped 30 April 2021; scroll down to the Appendix 1. List of Adverse Events of Special Interest section of this report. “Autoimmune disorder”; “Complement factor C1 decreased”; Complement factor C2 decreased”; Complement factor C3 decreased”; Complement factor C4 decreased” are among the listings. The Complement factors C1 to C4 are crucial proteins in the innate immune system. Decreases / deficiencies in any or all of these complement factors will create dysfunction / malfunction of the innate immune system, inducing conditions ranging from angioedema to recurrent infections to neurological conditions, and more. Three: Please see: https://www.annalallergy.org/article/S1081-1206(23)00002-9/fulltext, “Alpha-Gal Syndrome is an immunoparasitologic disease”, John C. Carlson, MD, PhD, April 2023. Four: there may well also be the involvement of other types of “vaccines” (in other words, non-COVID-19 bioweapon “vaccines”) in damage to the innate immune system.
>>>>>>>>>>>>>>>>>>>>
MAiD: It appears that the use of this “assisted suicide” protocol in Canada is “expanding”:
WHAT 🤯 A man in his 40s with inflammatory bowel disease, was assessed outside a Tim Hortons, offered MAID, AND driven by the DR to the assisted suicide facility, and killed by MAID 🤯
I honestly thought this headline was fake, but it’s real
Inflammatory bowel disease is treatable and manageable: https://www.cdc.gov/inflammatory-bowel-disease/living-with/index.html. By the way, “Inflammatory bowel disease” is ALSO LISTED in the Appendix 1. section of the BNT162b2 (COMIRNATY) report cited above: it can therefore be an adverse event of the COVID-19 bioweapon “vaccines.” Note: some media outlets (for example, https://www.vigilantfox.com/p/germany-and-canada-go-full-1984-daily), state that the man (in his 40s) suffered from Crohn’s Disease, mental health issues, and substance abuse issues — all of which are treatable and manageable: and is ALSO LISTED as an adverse event of the COVID-19 bioweapon “vaccines”, per the BNT162b2 (COMIRNATY) report cited above.
>>>>>>>>>>>>>>>>>>>>
And, last but not least, THIS insanity, in OREGON:
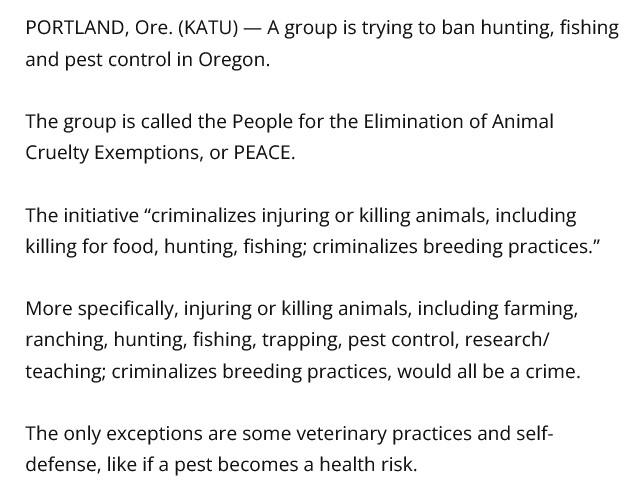
A petition is now the November ballot in Oregon that, if passed, would criminalize the killing of any animal (including fish and other marine life) for food; would ban pest and insect control; would criminalize and ban the teaching of these practices; and more. Enough signatures have been obtained to put this madness up for a vote:
An effort to criminalize the killing of animals for food in Oregon is a step closer to being on the November ballot.
IP-28 would make it illegal to injure or kill animals and would effectively ban hunting, fishing and the breeding of animals. https://t.co/Je1Z43xKAm
(Intellectual Disclaimer and Notice: Except for the linked URLs and other items in today’s offering that are found on the internet, the ideas and/or opinions in today’s offering are by PAVACA. Credit must be given to PAVACA if ideas and/or opinions in today’s offering are used by other blog writers; by podcasters; or in print or social media.)
The header image of the word Interesting for today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics. There are Important Notifications form our host, Wolf Moon; the Rules of our late, good Wheatie; and certain caveats from Yours Truly, of which the reader should be aware. They are linked here. Note: AI-generated items in today’s offering are cited as such. if readers wish to post AI-generated items to today’s discussion thread, they must cite their source. Thank you.
Some Interesting Links:
Regarding the November 2025 exposure of an employee at the Rocky Mountain Lab (part of the NIH) to the Crimean-Congo Hemorrhagic Fever virus. The virus is being experimented on at this facility. Our good Aubergine posted a comment on this situation, which began a discussion: https://theqtree.com/2026/04/03/health-friday-4-3-2026-open-thread-where-the-focus-needs-to-be-now-an-opinion-piece/#comment-1595800. It has been proven that this virus does indeed shed; the shedding can be present in the body secretions and blood of the exposed / infected person. The published paper regarding shedding of Crimean-Congo Hemorrhagic Fever virus is here: https://pmc.ncbi.nlm.nih.gov/articles/PMC7078823/, “Monitoring Crimean-Congo haemorrhagic fever virus RNA shedding in a body secretions and serological status in hospitalized patients, Turkey, 2015.” Dilek Yagci-Caglayik, et al. 12 March 2020. (Yours Truly: While the paper is about the shedding of this virus in hospitalized patients, it, in my opinion, opens up the possibility that the virus can shed from non-hospitalized exposed or infected persons.)
>>>>>>>>>>>>>>>>>>>>>>>>
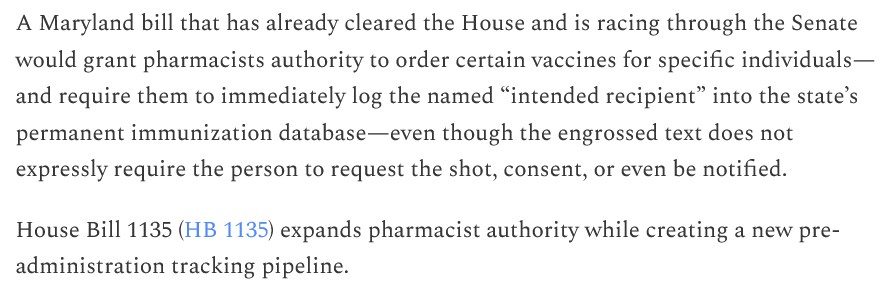
In Maryland, if a newly-proposed law there comes into effect, pharmacists will be able to order certain “vaccines” for patients; while, at the same time, placing the names of those persons into the Maryland state database for immunization tracking:https://jonfleetwood.substack.com/p/maryland-bill-lets-pharmacists-order, “Maryland Bill Lets Pharmacists Order Vaccines for You — Logging Your Name in State Tracking System Without Any Patient-Request Requirement”, 3 April 2026. A screenshot from this article is below:
Note that this bill regards pharmacists being granted permission to order vaccines — and to do so without the patient’s knowledge, consent, or request. The name of the patient is put into a state tracking database. The vaccines are paid for by private insurance (if the patient’s private insurance information is on file at the pharmacy), or are covered by Medicare/Medicaid. This opens up the potential for both the pharmacy and the state to “keep tabs” on the patient in order to get “vaccine compliance” from the patient.
>>>>>>>>>>>>>>>>>>>>>>>>
Why hasn’t James Lloyd Austin, III, Secretary of Defense under former “President” Joe Biden, been held to account for his “mandating” over 90% of United States military personnel being “vaccinated” with modRNA COVID-19 bioweapon “vaccines”? https://www.thefocalpoints.com/p/breaking-study-half-of-covid-19-vaccinated, “BREAKING STUDY: Half of COVID-19 Vaccinated Military Personnel Suffered Subclinical Heart Stress”, Nicolas Hulscher, MPH, 31 March 2026. The paper cited in the article is here: https://doi.org/10.1016/j.vaccine.2026.128535, “Transient elevation of NT-proBNP after mRNA COVID-19 vaccinations in healthy adults: A longitudinal biomarker analysis.” Pavel Dlouhy, et al. 30 April 2026.
Note that this paper studies heart issues that appeared in 50% of 83 healthy, adult military personnel after their being “vaccinated” with either BNT162b2 (Pfizer-BioNTech) or with mRNA-1273 (Moderna.) The military personnel were stationed at the Air Transportation Base Facility in Prague, Czech Republic. The troponin levels of their hearts were found to have gone up. Elevated troponin levels in the heart indicate stress on the heart muscle. Elevated troponin levels can indicate heart problems even if there are no overt symptoms. If that is what occurred in half of the “vaccinated” personnel tested at an air transportation base in the Czech Republic, how many thousands of United States military personnel potentially had the same effect after they were “mandated” to be “vaccinated” by former Defense Secretary Austin? (Austin was the former Secretary of what is now called the Department of War.)
Note also that the military personnel at the air transportation base in Prague were well over the age of 17 — in fact, the mean age of the 83 tested personnel was 39 years. This blows clean out of the water ALL of the claims of Big Pharma, Establishment Medicine, the CDC, the FDA, the AMA, and many other entities, that heart problems associated with COVID-19 “vaccination” are “rare” —and, are “confined mostly to persons between the age of 12 and 17 years.”
>>>>>>>>>>>>>>>>>>>>>>>>
Another example of how a physician who stood up against Big Pharma, the CDC / FDA, the AMA, and the AAP (American Academy of Pediatrics), was persecuted: his License to Practice Medicine in his home state (Oregon) was suspended in 2020; then, his License to Practice Medicine was revoked in the state where he had been credentialed (Washington State); then, his board credentials in the AAP were revoked; then, he had to surrender his License to Practice Medicine in Oregon in 2022 (https://omb.oregon.gov/Clients/ORMB/Public/VerificationDetails.aspx, effective 5 December 2022.) This was the journey of Dr. Paul Thomas, a highly-respected pediatrician: https://www.2ndsmartestguyintheworld.com/p/doctor-published-study-showing-vaccinated, “Doctor Published Study Showing Vaccinated Children Have 500% Increase In Chronic Diseases Only To Have License Suspended & Get Cancelled By BigPharma”, 8 April 2026. The study was Retracted by MDPI, the preprint publisher. It is available here: https://www.researchgate.net/publications/346088816_Relative_Incidence_of_Office_Visits_and_Cuulative_Rates_of_Billed_Diagnoses_Along_the_Axis_of_Vaccination. James Lyons-Weiler, Paul Thomas. 22 November 2020. (Yours Truly: Note that this paper was accepted and peer-reviewed before it was published.)
>>>>>>>>>>>>>>>>>>>>>>>>
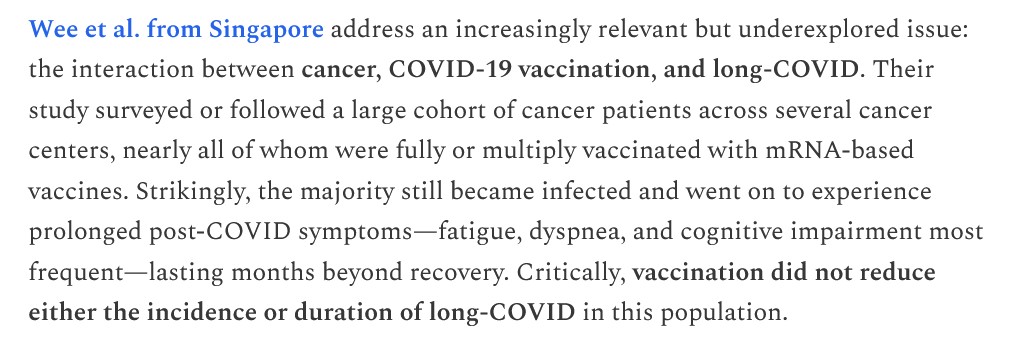
Dr. Peter A. McCullough addresses the nexus among cancer patients who then get COVID-19 “vaccinated” and thereupon afterwards present with symptoms of Long COVID:https://www.thefocalpoints.com/p/the-hollow-promise-of-protection, 7 April 2026. A screenshot from this article is below (access to the entire particle is for subscribers only):
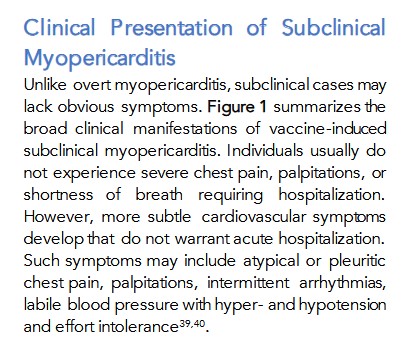
A related topic to the heart issues situation found in the military personnel at the air transportation base in Prague who had been COVID-19 “vaccinated”: This one regards subclinical myocarditis/pericarditis in COVID-19 “vaccinated” persons: https://www.thefocalpoints.com/p/breaking-peer-reviewed-paper-finds, “BREAKING: Peer-Reviewed Paper Finds mRNA “Vaccines” Convey Silent Heart Damage—Presents Approach to Diagnosis and Management”, Nicolas Hulscher, MPH, 31 December 2025. A screenshot from this paper is below:
The paper is found here: https://doi.org/10.1810/mra.v13i11.7078, “COVID-19 Vaccine-Induced Subclinical Myopericarditis: Pathophysiology, Diagnosis, and Clinical Management.” Peter A. McCullough, MD, MPH, M. Nathaniel Mead, MSc, PhD, Nicolas Hulscher, MPH. 30 November 2025.
Yours Truly: The above paper speaks to subclinical myocarditis/pericarditis in COVID-19 “vaccinated” persons — and makes it clear that, although many of the reported cases were found in “vaccinated” males under age 21, there were cases found in other “vaccinated” persons (male and female), and in other age groups. On the other hand, there is also the real phenomenon of “vaccine” shedding from “vaccinated” persons onto others, including onto non-COVID-19 “vaccinated” persons. Who knows how many non-COVID-19 “vaccinated” persons (including children) have been exposed to the ingredients and mechanisms of these “vaccines” that induce heart problems? At the same time, there are other factors that need to be considered when talking about what engenders or aggravates heart issues. Examples of other factors can include, but are not limited to: chronic stress; hypertension; family history of / predisposition to, heart disease; and, COPD (https://www.ummhealth.org/health-library/copd-and-heart-disease.)
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA, A modRNA, AN saRNA, OR A taRNA PRODUCT OF ANY KIND, IN ANY FORM.
ALL GAIN-OF-FUNCTION ACTIVITIES IN THE UNITED STATES MUST BE STOPPED, NOW.
ALL COVID-19 BIOWEAPON “VACCINES” MUST BE PULLED OFF THE MARKET AND REMOVED FROM USE IN THE UNITED STATES, NOW.
The free image of vintage Pfizer vaccine vials for the header in today’s offering is courtesy of Dreamstime and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As today’s offering speaks to the COVID-19 “vaccines”, Yours Truly dedicates it to all persons, of whatever age or location, who have passed away from the negative effects of the COVID-19 “vaccines” that they had in their body. May they rest in eternal Peace.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for AI-generated content. To the best of her knowledge and belief, there is none, except perhaps for AI-generated images within linked URLS. If readers wish to post AI-generated content to the discussion thread for today’s offering, they must cite their source. Thank you.
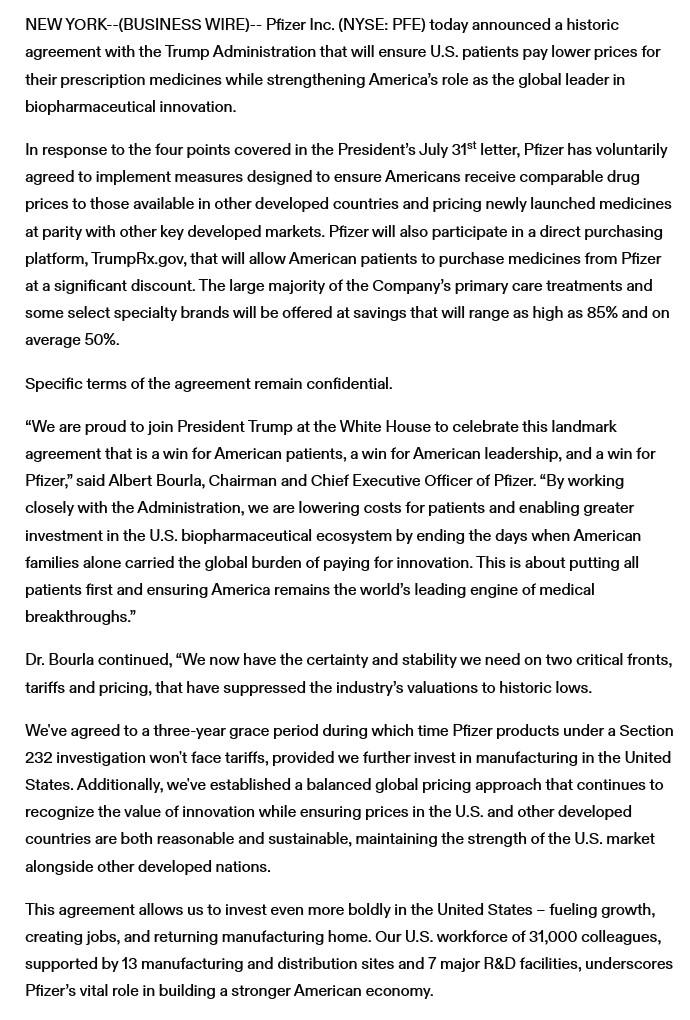
This Part One trail begins here, with two news reports regarding the September 2025 agreement reached between the United States government and Pfizer (PfizerUSA, the United States co-partner of Pfizer-BioNTech; BioNTech, the other co-partner, is headquartered in Mainz, Germany.). First, from Virginia Business (https://virginiabusiness.com/pfizer-agrees-to-lower-drug-costs-70b-us-investment/), “Pfizer agrees to lower drug costs, $70B US investment”, 30 September 2025. A screenshot from this article is below:
Note that the specific details of this agreement, which will affect millions of Americans, “remain confidential.”
The company called Pfizer-BioNTech is a formal co-partnership between Pfizer, also known as PfizerUSA (CEO, Dr. Albert Bourla, DVM); and, BIoNTech of Mainz, Germany (CEO, Dr. Ugur Sahin, MD.) Both PfizerUSA and BioNTech were involved / still are involved, in the development and manufacture of the modRNA COVID-19 “vaccine” line, COMIRNATY (this “vaccine” was previously known as BNT162b2, or “Pfizer-BioNTech COVID-19 Vaccine.“) Both PfizerUSA and BioNTech have agreements regarding their sharing royalty payments for COMIRNATY “vaccines” purchased and used throughout the world. PfizerUSA and BioNTech are also involved in the development and manufacture of other drugs and vaccines, either separately or in coordination with each other.
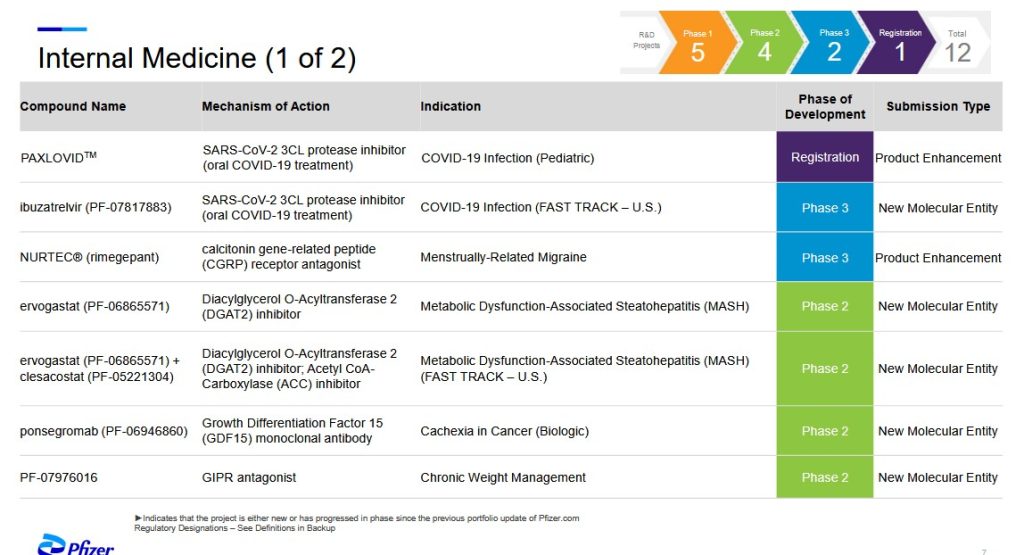
The most recent (as of 5 August 2025) PfizerUSA (and Pfizer-BioNTech) product “pipeline” website is here: https://www.pfizer.com/science/drug-product-pipeline. Click on “Downloadable PDF” to view the entire pipeline. Screenshots of two pipeline areas, Internal Medicine and Vaccines, follow. The first screenshot, Internal Medicine, with discussion by Yours Truly, is below:
****WHY is Paxlovid, a combo drug of nirmatrelvir (an antiviral) + ritonavir (an HIV/AIDS treatment drug that targets the immune system) going to be used on CHILDREN who become infected with COVID-19?
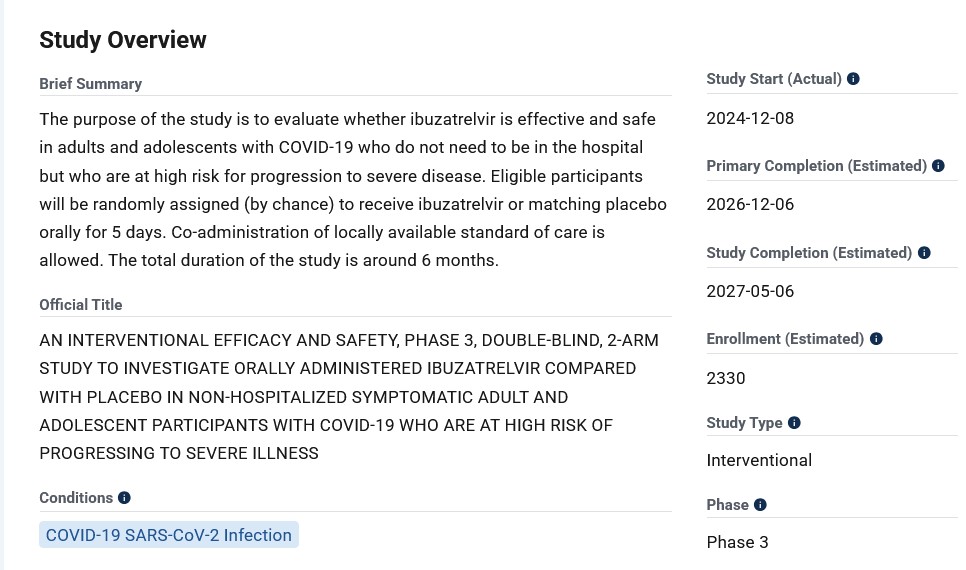
**** Ibuzatrelvir (PF-07817883), now in Phase 3 clinical trials, is an oral / enhanced “nirmatrelvir on steroids” treatment for COVID-19 infection that was granted “Fast Track” approval by the FDA The intended use of this drug appears to be as a “replacement” for Paxlovid.. Please see: https://pubs.acs.org/doi/10.1021/jacsau.4c00508, 30 July 2024. Pfizer has already patented this drug. Let’s take a look at the Overview of this Phase 3 clinical trial, as described here: https://clinicaltrials.gov/study/NCT06679140:
Does “Fast Track” approval by the FDA mean that the “Study Completion (Estimated)” of 6 May 2027 will be “bypassed”, and only the data from the “Primary Completion (Estimated)” of 12 December 2026 will be used to push this drug onto the market faster? In addition, WHY is the study subject pool so small (2330 persons) for a drug that would potentially be used on hundreds of thousands of persons?
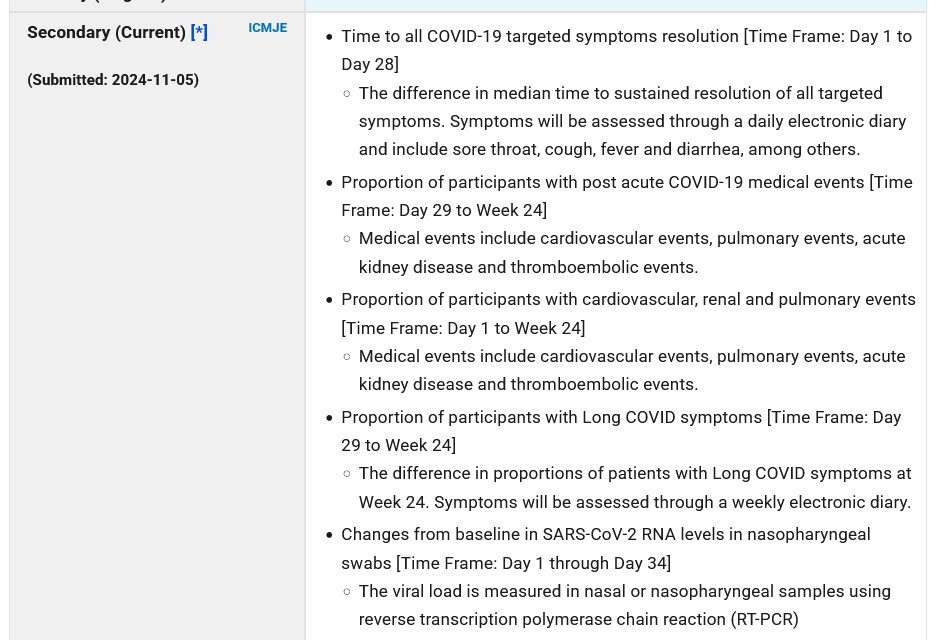
And, from the Researcher View of this clinical trial, part of the Secondary Outcomes descriptions:
Note that the “viral load” measurement will be performed via EITHER a nasal sample, OR via a nasopharyngeal sample. If a nasopharyngeal sample swab is used, this is the extremely long swab that reaches all the way to the VERY BACK of the nasal cavity and can touch the COVERING OF THE BRAIN. By the way, the correct administration of the nasopharyngeal swab is also to ROTATE the swab a couple of times after insertion.
In addition, in the information about NCT06679140, the “placebo tablet” that will be used is NOT described at all. Is the “placebo tablet” going to be Paxlovid? Is the “placebo tablet” going to be a completely drug-free “empty” tablet?
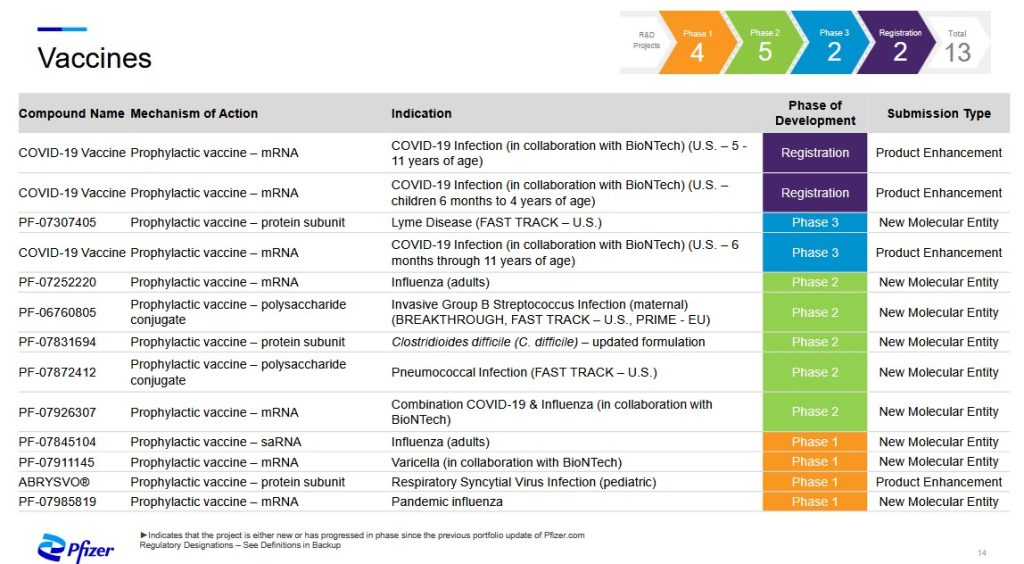
And now, the second screenshot from the “pipeline” PDF, Vaccines, is below. Yours Truly will discuss an interesting new “vaccine” from this list, under development by PfizerUSA (in conjunction with BioNTech) —PF-07926307, a combination modRNA-based COVID-19 plus influenza “vaccine“:
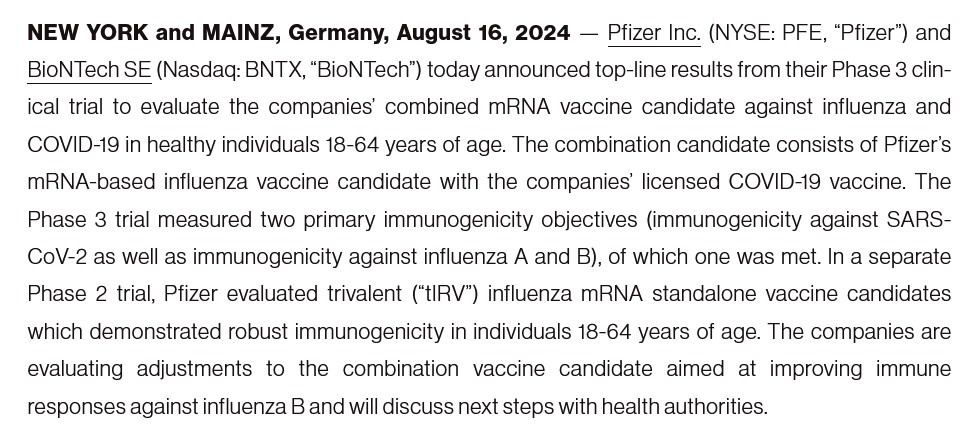
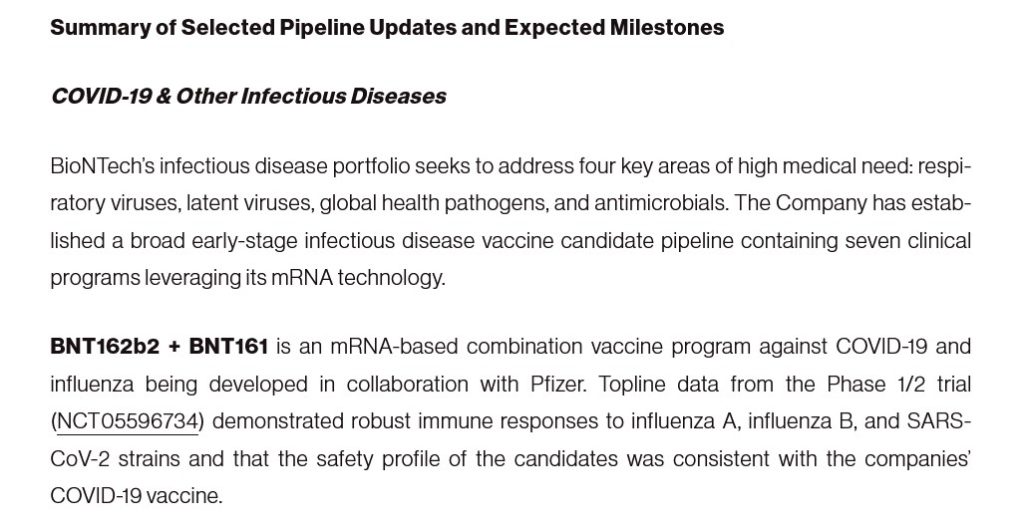
The available-to-the-public information regarding PF-07926307 is both confusing and concerning. Pfizer-BioNTech insists that this “combo vaccine” is only for “prophylactic” use against COVID-19 plus influenza: https://investors.biontech.de/news-releases/news-release-details/pfizer-and-biontech-provide-update-mrna-based-combination, “Pfizer and BioNTech Provide Update on mRNA-based Combination Vaccine Program Against Influenza and COVID-19 in Individuals 18-64 Years of Age”, 16 August 2024. Only ONE of of the two outcomes measurements of the Phase 3 clinical trial for this “vaccine” were met (NCT06178991.) A screenshot from the company’s press release is below:
Note that this press release emanates from Germany, not the United States;, and that the “combination candidate” is not identified as PF-07926307.
**** Note the clinical trial mentioned in the above screenshot: NCT05596734. The modRNA “combo vaccine” used in this clinical trial is none other than BNT162b2 (tozinameran, now marketed as COMIRNATY, but which was the ORIGINAL Pfizer-BioBNTech modRNA COVID-19 “vaccine” against the ORIGINAL Wuhan Hu1 SARS-CoV-2 [COVID-19] virus), plus BNT161 (famtozinameran, the ORIGINAL modRNA COVID-19 “vaccine” against the OMICRON variant BA.4/BA.5) Please see: https://covid-vaccine.canada.ca/comirnaty-original-omicron-ba4ba5/product-details, which also states, “Cancelled by sponsor May 3rd, 2024.”
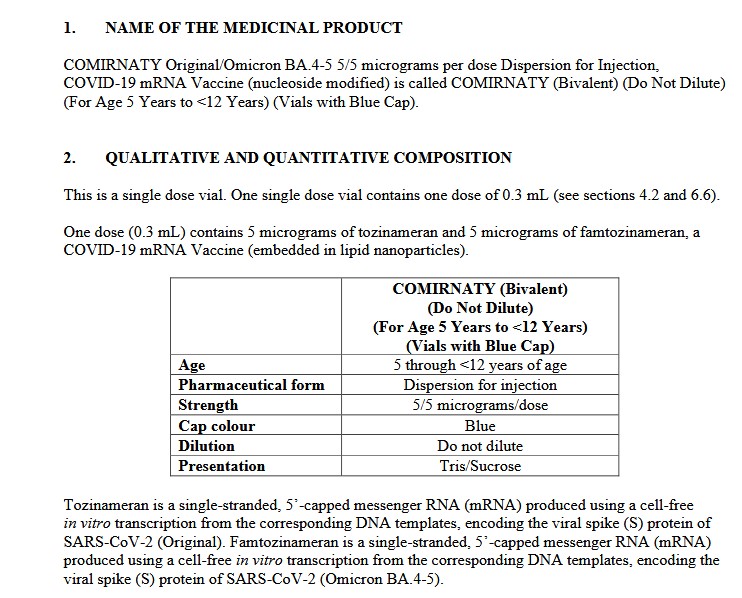
**** However, at the same time, it appears that this Pfizer-BioNTech modRNA COVID-19 “combo vaccine” of BNT162b2 plus BNT161 — also known as PF-07926307 — IS being used — in Singapore: https://labeling.pfizer.com/ShowLabeling.aspx?id=20959, “Date of last revision: July 2024.” Please see the screenshot from the package information for this product administered in Singapore, below:
And, screenshots from Page 65 (of 65), from the package information for the above injectable:
BNT161, one of the component modRNA “vaccines” in PF-07926307, is an influenza “vaccine”, meaning that it can be used against EITHER influenza OR COVID-19 (Omicron BA.4/BA.5.) The German partner of PfizerUSA — BioNTech — has been working on this injectable since at least 2022:https://biontechse.gcs-web.com/news-releases/press-release-details/biontech-announces-third-quarter-2022-financial-results-and, “BioNTech Announces Third Quarter 2022 Financial Results and Corporate Update”, 7 November 2022. A screenshot from this article is below:
Note that the press release is from BioNTech Sweden.
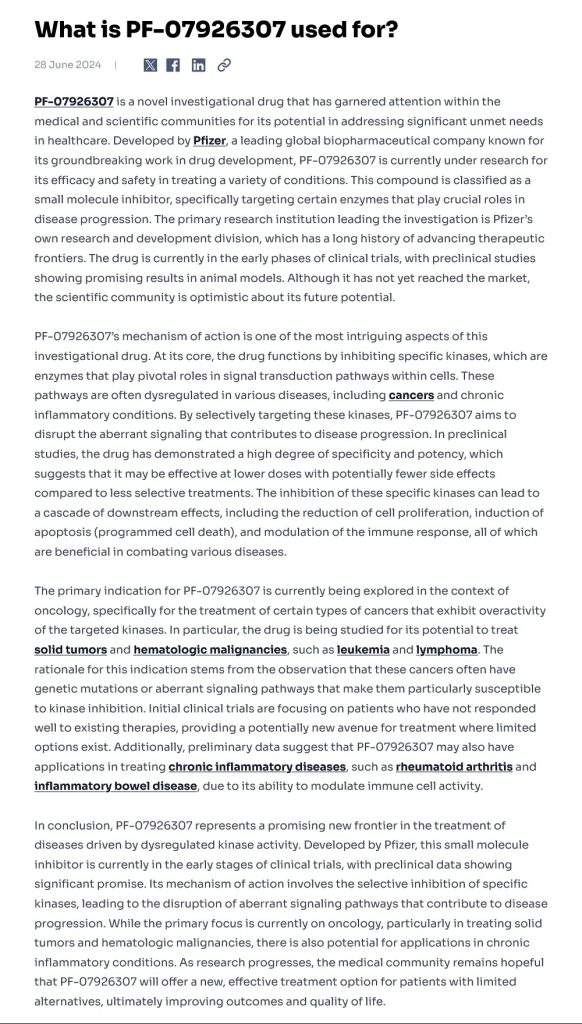
**** On the other hand, here is the article on PF-07926307 (BNT162b2 + BNT161) by the tech / AI / data collection and analysis platform, Patsnap: https://synapse.patsnap.com/article/what-is-pf-07926307-used-for?, 28 June 2024. A screenshot of the entire article is below; Yours Truly includes the entire article because it has a wealth of information and clues as to the possible real “agenda” behind this injectable:
****Note that, per the article above, the “primary indication” for the use of PF-07926307 is for the treatment of cancers caused by overactive kinases responses, such as are found in lymphomas; with what may be called a “secondary indication” for treatment of chronic inflammatory diseases. Lymphomas or chronic inflammatory diseases induced by, say, modRNA COVID-19 “vaccine” injections, such as BNT162b2 (COMIRNATY?) Is it remotely possible that PF-07926307 (BNT162b2 + BNT161) is being redesigned as a “backdoor oncology and/or chronic inflammatory diseases treatment” injectable?How does this square with what Pfizer-BioNTech claims that this “vaccine” is to be used for — against COVID-19 + influenza infection? What is the truth here?
**** In any case, WHY is Pfizer-BioNTech apparently using BNT162b2, the company’s original modRNA COVID-19 “vaccine”, as a foundational component in the development of a “New Molecular Entity” called PF-07926307, which is to used as a “prophylactic” against COVID-19 plus influenza? What happened regarding all those other modRNA COVID-19 “vaccines” made by this company, to be used against the LATEST MUTATIONS of the SARS-CoV-2 virus, such as the “2025-2026 version” of COMIRNATY? Why is Pfizer-BioNTech going all the way back to the ORIGINAL Wuhan Hu1 SARS-CoV-2 virus contained in BNT162b2 (COMIRNATY) to formulate PF-07926307?
What is going on at Pfizer-BioNTech? Does the United States government know about PF-07926307 (BNT162b2 + BNT161)? Did the “Specific terms of the agreement remain confidential” regarding the deal between the United States government and PfizerUSA reached in September 2025 include provisions that our government “looks the other way” about the activities of PfizerUSA’s co-partner, BioNTech? Does the HHS / FDA / CDC / BARDA have the complete details of the “Specific terms of the agreement remain confidential” provisions? Are the “specific details” being shared with only the “top brass” of the FDA / CDC / BARDA — and that HHS Sec. Kennedy, Jr., is being kept in the dark?
———————————————————————————
All current COVID-19 “vaccines” — ALL of them — MUST be pulled off the market and from use. Now.
All research and development of “new” COVID-19 “vaccines” that are in ANY form — injectable; oral; nasal; micro-needle — MUST be stopped. Now.
There MUST be complete analysis of the ingredients and mechanisms of the current COVID-19 “vaccines”, performed by impartial testing entities, and with complete results made public. Now.
THERE. MUST. BE. ACCOUNTABILITY.
THERE. MUST. BE. JUSTICE.
THERE. MUST. BE. TRUTH.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Notice: With the exception of links to published media reports and links to published scientific papers, the ideas and conclusions of today’s post are by PAVACA. Proper credit must be given to PAVACA if other blog writers, or persons on podcasts, social media, or print media, use the ideas and/or conclusions of today’s post. Thank you.)
The free vintage header image of writing a letter for today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post AI-generated content in today’s discussion thread, they must cite their source. Thank you.
Today’s offering is dedicated to all persons, of whatever age or location, who have suffered negative consequences from an infection of the COVID-19 virus itself after recovering from the infection; to all persons, of whatever age or location, who have COVID-19 “vaccine”-induced injuries, illnesses, and/or disabilities; and, to all persons, of whatever age or location, who have passed away from either an infection of the COVID-19 virus itself, or from the negative effects of the COVID-19 “vaccines” they had in their body.
“Dr. Martin Makary, MD, MPH, Commissioner, United States Food and Drug Administration (FDA)
10903 New Hampshire Ave., Silver Spring, MD, 20993
Dear Dr. Martin Makary:
Greetings. This letter is in reference to certain questions that the writer poses regarding the FDA, under your leadership, still promoting the use of the COVID-19 “vaccines” (actually, mRNA gene therapies) in the United States. This includes the modRNA COVID-19 “vaccine” COMIRNATY, by Pfizer-BioNTech; the modRNA COVID-19 “vaccines” SPIKEVAX and NEXSPIKE, by Moderna; and, the “inactivated virus” COVID-19 “vaccine” NUVAXOVID, by Novavax. Thank you in advance for your attention. The questions follow:
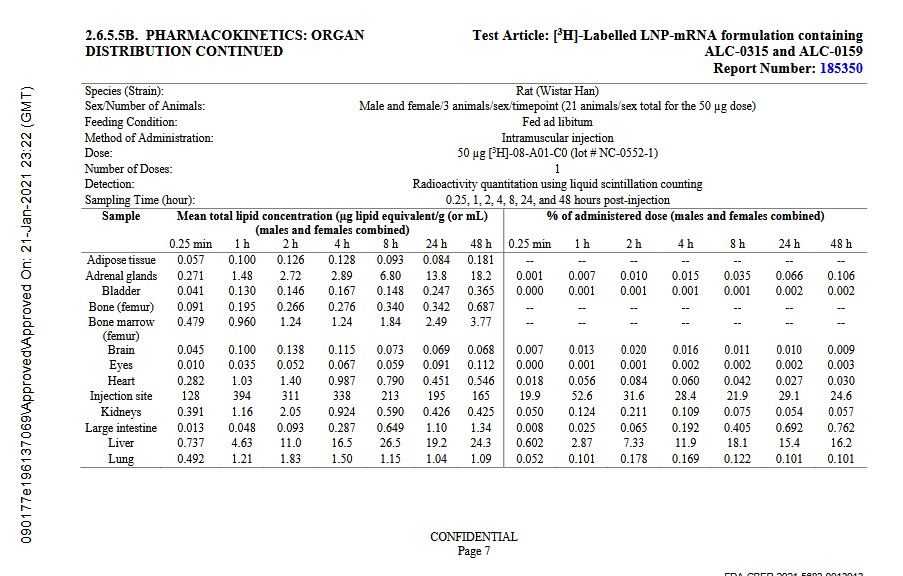
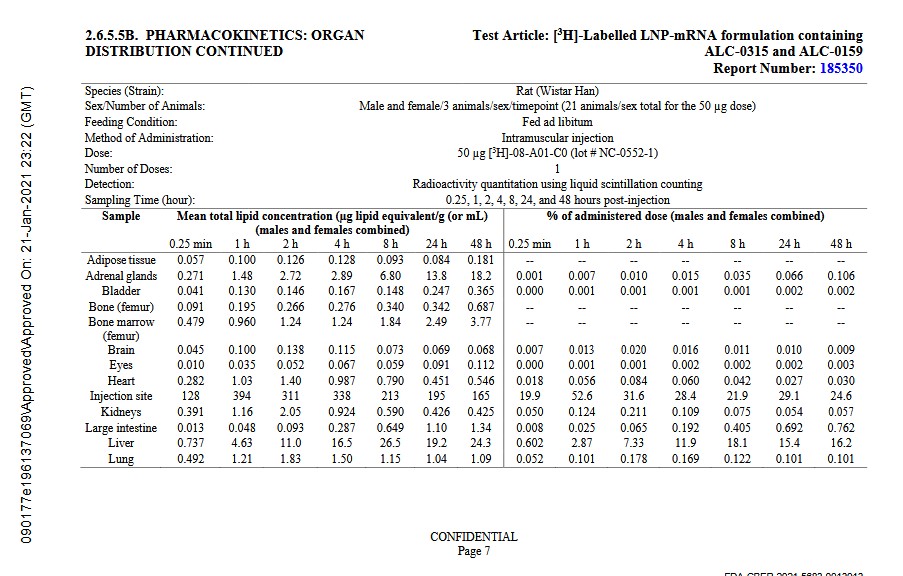
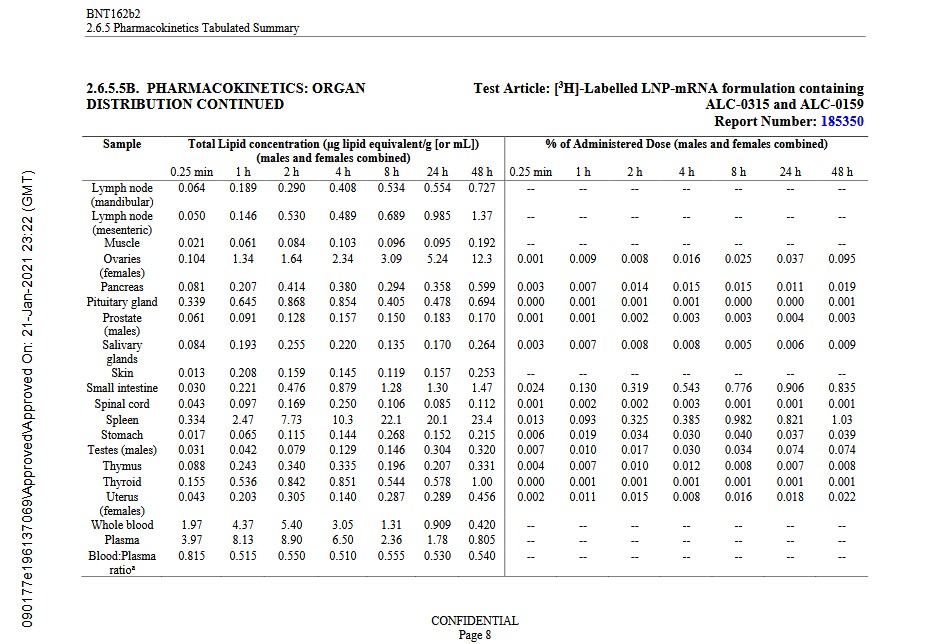
Question One: Have you read through the report on BNT162b2 that Pfizer-BioNTech submitted to the FDA on 21 January 2021, regarding the Pharmacokinetics tests results for this modRNA COVID-19 “vaccine” (which was subsequently approved by the FDA in 2022 under the name COMIRNATY)?
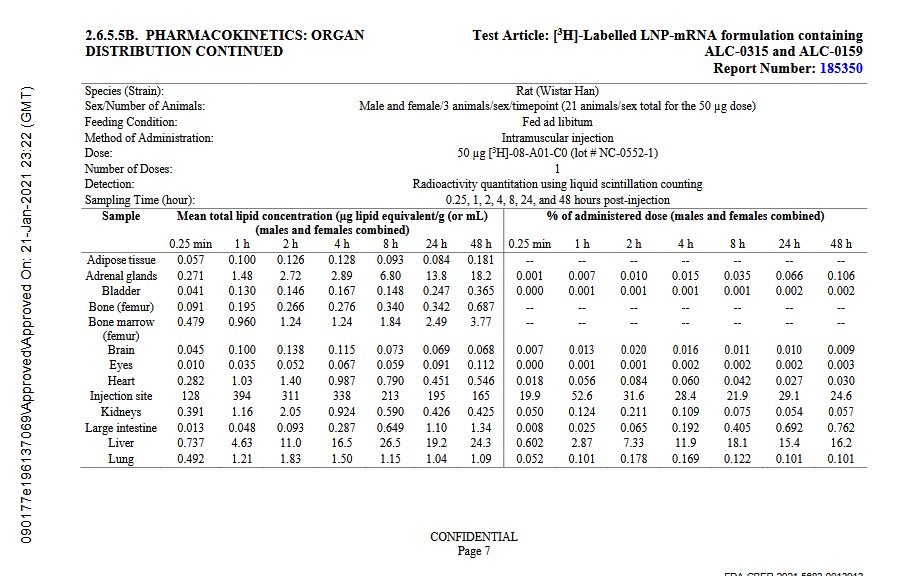
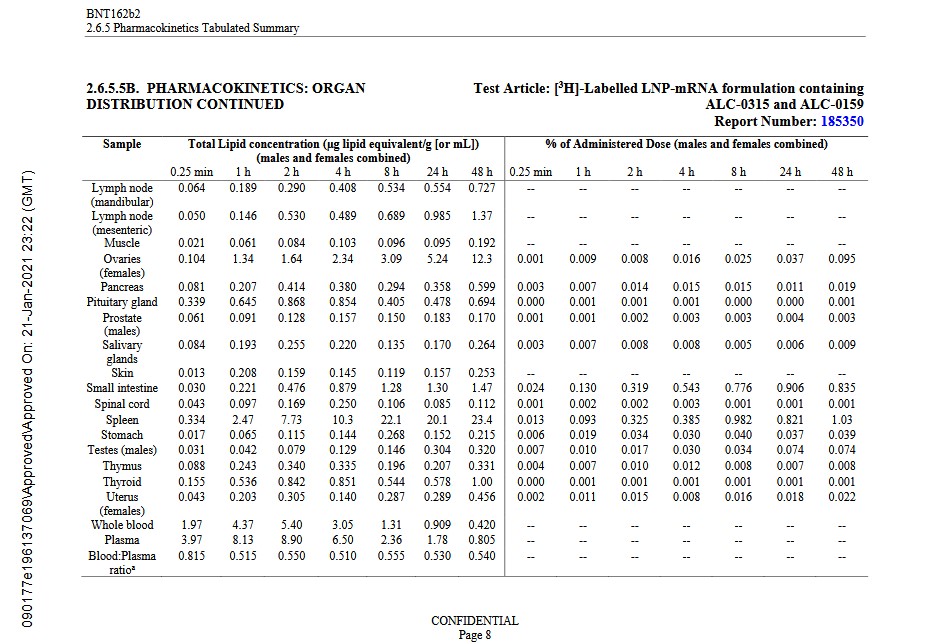
Would you please answer, in detail, your reasoning behind the continued FDA approval of COMIRNATY based on the results of this report? The report is found here: https://phmpt.org/wp-content/uploads/2022/03/125742_S1_M2_26_phramkin-tabulated-summary.pdf, “BNT162b2 2.6.5 Pharmacokinetics Tabulated Summary”, time-stamped by the FDA on 21 January 2021 at 23:22 (GMT), and starting with FDA CBER document identification number FDA-CBER-2021-5683-0013907. For your convenience, images of Page 7 and Page 8 of this report are below; first, Page 7:
And, Page 8:
The writer of this letter assumes that you understand that the BNT162b2 formulation used in the Wistar lab rats experiments above is the same formulation that the FDA granted the initial EUA to for use in the United States on 11 December 2020.
Question Two: Have you read through the Post-marketing Experience report on BNT162b2 that Pfizer-BioNTech submitted to the FDA on 30 April 2021? In particular, have you read through the APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST section of this report, which begins on Page 30? The report is found here: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, “BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports”, time-stamped by the FDA on 30 April 2021 at 09:26 (GMT), starting with FDA CBER document identification number FDA-CBER-2021-0000054. The APPENDIX 1.section covers only those serious adverse events reports to Pfizer-BioNTech that were submitted between 11 December 2020 (the date that the FDA granted the initial EUA for BNT162b2 to be used in the United States), and 28 February 2021 — a period of fewer than 12 weeks.There are over 1,200 different listings of serious adverse events reports in theAPPENDIX 1. section of the document.
Would you please answer, in detail, your reasoning behind the continuing FDA approval of COMIRNATY, given this document? Would you please answer, in detail, your reasoning why the FDA would simply accept this document without demanding an investigation of why there are so many different serious adverse events reports for BNT162b2? For you convenience, an image of Page one of theAPPENDIX 1.section (Page 30 of the report document) is below:
TheAPPENDIX 1.section of the report runs from Page 30 to Page 38.
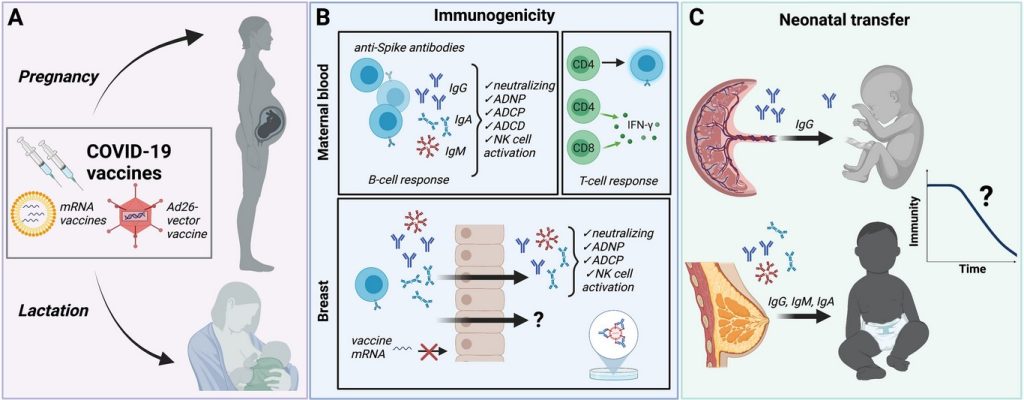
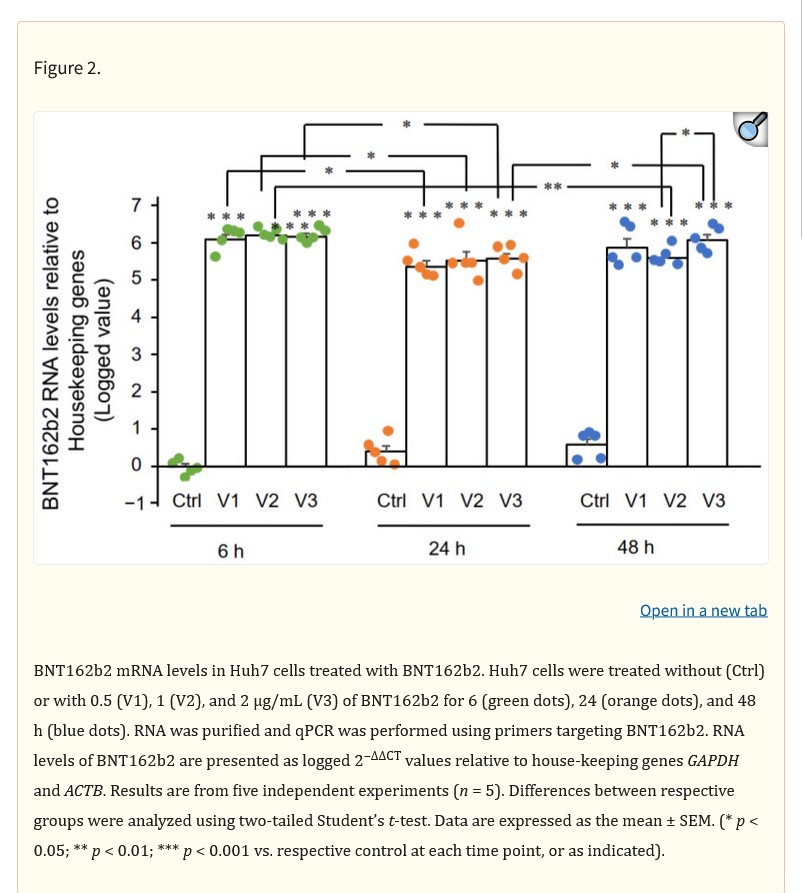
Question Three: Have you read the paper, published in the journal Frontiers in Cellular and Infection Microbiology on 15 September 2021, in which the authors prove that both the modRNA COVID-19 “vaccines” of Pfizer-BioNTech and of Moderna, and the viral vector COVID-19 “vaccines” (for example, of Janssen), cross the placenta of a COVID-19 “vaccinated” pregnant woman and enter into the body and brain of the fetus she is carrying? And, that, similarly, these “vaccines” also cross into the breast milk of the nursing mother who was “vaccinated”, therefore also entering into her nursling’s body and brain? The paper is found here: https://doi.org/10.3389/fcimb.2021.735394, “COVID-19 Vaccination in Pregnancy and Lactation: Current Research and Gaps in Understanding”, Lydia L. Shook, Parisa N. Fallah, Jason N. Silberman, Andrea G. Edlow, 15 September 2021. For your convenience, a screenshot of Figure 1 from the paper is below:
Which means, according to the graphic above from the paper, that the fetus and the nursling will get COVID-19 “vaccinated” along with the mother, due to the ingredients and mechanisms that cross into the placenta and/or the breast milk from the “vaccinated” mother. The natural immune systems of a fetus or of a nursling child are not mature enough, or strong enough, to handle the antibody-manufacturing demands of the COVID-19 “vaccines” that involuntarily enter their body and brain via the “vaccinated” mother.
Would you please describe, in detail, your reasoning for the FDA continuing to recommend COVID-19 “vaccination” of pregnant women, and/or breastfeeding mothers, based on the Frontiers In paper report?
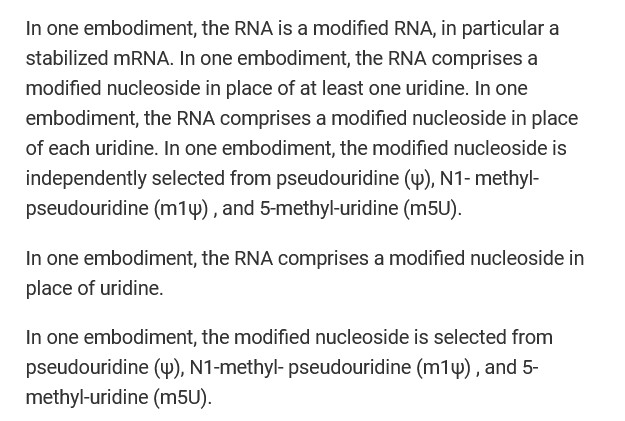
Question Four: Are you aware that the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna, contain N1-Methylpseudouridine,a lab-created compound, that replaces the natural RNA in the Uridine of the “vaccinated” person’s body with this compound? Are you aware that N1-Methylpseudouridine was specifically created and included in the modRNA COVID-19 “vaccines” because this lab-created compound facilitates the entry of the ingredients of these “vaccine” into every cell of the “vaccinated” person’s body? Are you aware that, by replacing the RNA of the natural Uridine in the “vaccinated” person’s body, the multiple beneficial functions of Uridine RNA are damaged or lost? Are you aware that, among the multiple beneficial functions of Uridine RNA include cognitive elements (learning, memory), and emotional/psychological elements (mood regulation?) Are you aware that N1-Methylpseudouridine is present in all COVID-19 “vaccines” by Pfizer-BioNTech? For your convenience, please see:https://www.theqtree.com/2024/11/08/health-friday-11-8-2024-open-thread-the-insidious-n1-methylpseudouridine-in-the-covid-19-vaccines/; and, https://www.theqtree.com/2025/03/21/health-friday-3-21-2025-open-thread-more-on-the-n1-methylpseudouridine-in-the-modrna-covid-19-vaccines/. The Patent Declarationby Pfizer-BioNTech for BNT162b2, which describes the inclusion of N1-Methylpseudouridine in this “vaccine”, and what it does, is found here: https://patents.google.com/patent/WO2021213945A1/en. For reference, the following screenshot is from this Patent Declaration:
Would you please explain, in detail, your reasoning behind why the FDA should continue to approve for use in the United States, an injectable (the Pfizer-BioNTech modRNA COVID-19 “vaccine”) that specifically includes a lab-created compound (N1-Methylpseudouridine) which replaces natural Uridine RNA — and that this replacement is performed without the advance knowledge and consent of the person receiving this “vaccine?”
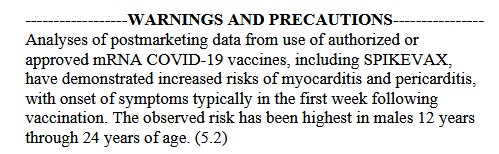
Question Five: The writer of this letter assumes that you, Dr. Makary, are aware that the modRNA COVID-19 “vaccines” induce cardiovascular issues and conditions, such as, myocarditis and pericarditis. This would mean induction of these conditions by the Pfizer-BioNTech modRNA COVID-19 “vaccine” (COMIRMATY); or, by the Moderna modRNA COVID-19 “vaccine” (SPIKEVAX.) The writer of this letter will focus on the Moderna product. ThePackage Insertfor the Moderna modRNA COVID-19 “vaccine”,SPIKEVAX,is found here: https://www.fda.gov/media/155675/download. For your convenience, screenshots of the the following portions of this document are below; first, theWarnings and Precautionssection:
The writer of this letter notes that theWarnings and Precautionsare not enclosed in a “Black Box Warning.” Why is this the case?
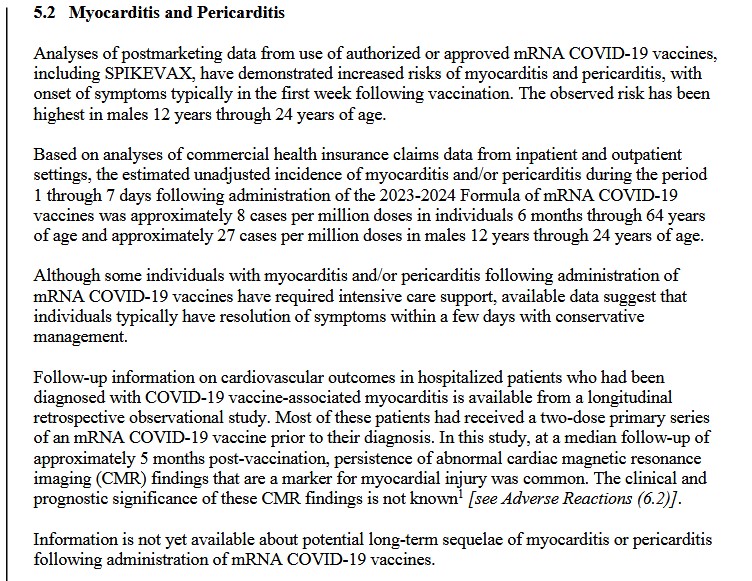
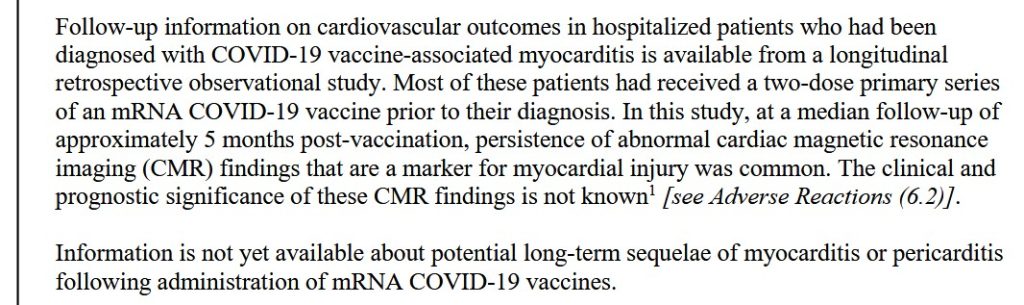
Then, from section5.2 Myocarditis and Pericarditis:
And, from section6.2 Postmarketing Experience:
There actually is information available regarding the potential for long-term sequelae of myocarditis or pericarditis after taking COVID-19 “vaccines.” It is here:https://doi.org/10.61577/ijcri.2025.100001, “Myocarditis after SARS-CoV-2 Infection and COVID-19 Vaccination: Epidemiology, outcomes, and new perspectives”, M. Nathaniel Mead, Jessica Rose, William Makis, Kirk Milhoan, Nicolas Hulscher, and Peter A. McCullough, 20 March 2025. For your convenience, a screenshot of theAbstract of this paper is below:
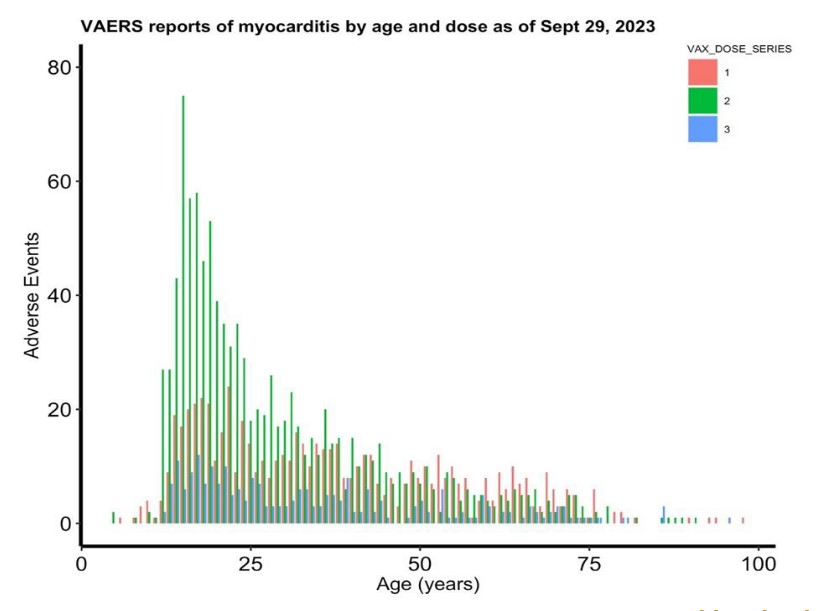
And, Figure 6 from the paper, VAERS reports of myocarditis after COVID-19 “vaccination”:
Would you please describe, in detail, your reasoning why the FDA needs to continue to promote the use of the modRNA COVID-19 “vaccines” in the United States, for any age group, based on the paper above?
Finally, Question Six: Would you please describe, in detail, what medical school and/or Residency classes you took in which you learned that it was acceptable for patients to be given injections of an mRNA gene therapy treatment platform (in this case, the modRNA COVID-19 “vaccines”) without that injectable first having gone through a rigorous testing and analysis protocol beforehand?
Sincerely,
An independent COVID-19 researcher for the past five and a half years.”
The COVID-19 “vaccines” — ALL of them — must be removed from the market and from use. Now.
The header image of a vintage laboratory for today’s offering is courtesy of Adobe Stock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Yours Truly has checked today’s offering for AI-generated content. To the best of her knowledge and belief, there is none, except perhaps for AI-generated images embedded in certain links. If readers wish to post AI-generated content to the discussion thread of today’s offering, they must cite their source. Thank you.
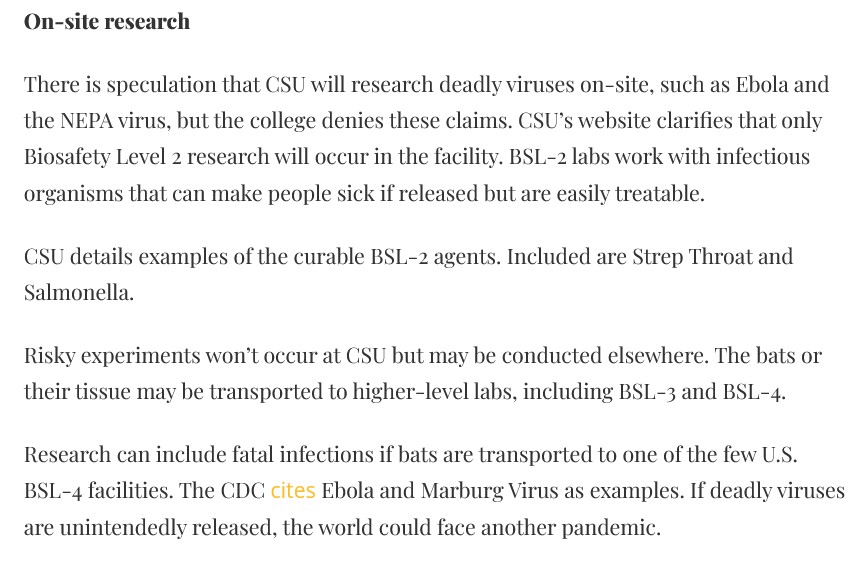
Today’s offering contains more proof that, even though the United States government has “officially” paused Gain-of-Function experiments, these experiments are still continuing. Please see: https://www.theqtree.com/2025/08/29/health-friday-8-29-2025-open-thread-gain-of-function-research-is-still-going-on/. This time, there are two separate facilities in the United States that are performing the Gain-of-Function (GoF) work. The first is the new “bat experiments lab” at Colorado State University at Fort Collins, CO. The second is the laboratory at Georgia State University at Atlanta, GA. Bear with Yours Truly: the end of the post is the “punch line.” Yours Truly makes it clear at the start that there is no intent to “cast aspersions” on the research of any of the persons mentioned in today’s offering, or on the current Acting Director of the NIAID.
And, guess what? The “new bat research facility” in Fort Collins also has BSL-2 level labs: A screenshot from the Yellow Scene article is below:
The entire situation at CSU raises other questions: One, will professors ALSO “mix in” with students at this “bat breeding and research” facility? And, Two, why is CSU attempting to be the “United States version” of the Wuhan Institute of Virology, which is what the “new bat research facility” at CSU appears to be?
And, now, turning to the second issue, the continuing Gain-of-Function experiments with Avian Influenza viruses going on in the United States —- this time, at Georgia State University in Atlanta. Please see: https://jonfleetwood.substack.com/p/us-and-south-korean-scientists-lab, “U.S. and South Korean Scientists Lab-Engineer Frankenstein Bird Flu Viruses in Georgia: Journal ‘Virology'”. 14 September 2025. The GoF experiments at GSU, supported by an NIH grant, were performed by South Korean scientists who are ALSO be professors at Georgia State University, with a couple of said professors ALSO having ties to South Korean institutions. Yours Truly will also present **interesting information** regarding the scope of this research at GSU by one particular author of the paper just cited. Please see the screenshot below, from the Fleetwood article:
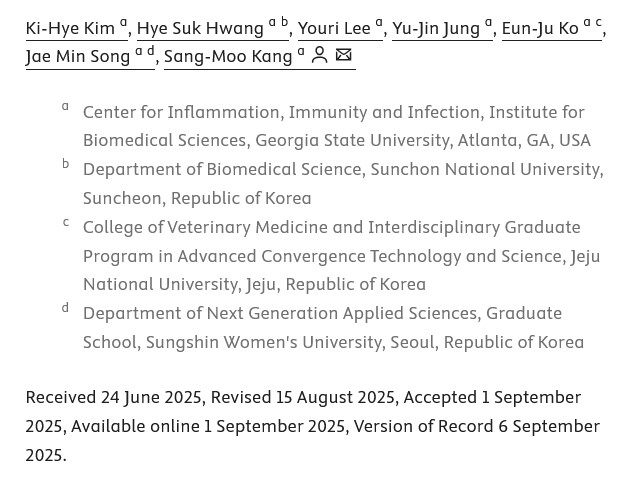
The paper cited in the Fleetwood article is here: https://doi.org/10.1016/j.virol.2025.110674, “Interferon-y receptor signaling is critical for balanced immune activation and protection against influenza after vaccination”, Sang-Moo Kang, et al., 6 September 2025. A screenshot of the list of the paper’s authors and their affiliations is below, from the paper itself:
Note that the TITLE of the paper does NOT mention what type of influenza was the study subject (in this case, it was Avian Influenza.) More on this aspect later on in today’s offering.
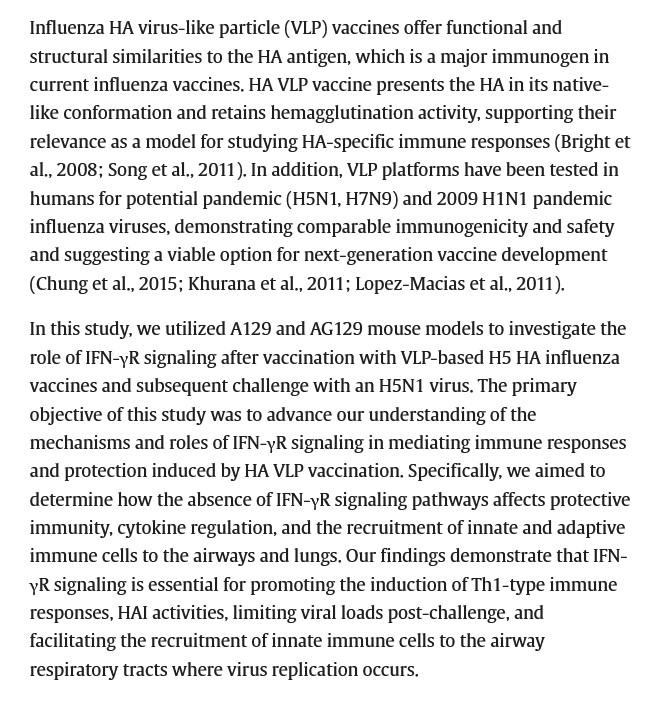
Following are screenshots from sections of the paper that are available online. Note: the entire paper is available only through institutional access, or through paid access.
Note the “clues”: “universal vaccination”; aged populations”; “multiple influenza proteins”; “translational science”; “cross protective efficacy.” However, the “multiple influenza proteins” that were experimented with in the paper cited above were not regular “seasonal flu viruses” — they were strains of H5N1, the Avian Influenza virus.
It appears that Dr. Kang has also used some of the AI154656 NIH grant on other research and papers, such as for this paper: https://doi.org/10.1016/j.vaccine.2025.127206, “Intranasal vaccination with multi-neuraminidase and M2e virus-like particle vaccine results in greater mucosal immunity and protection against influenza than intramuscular injection”, Sang-Moo Kang, et al., Version of Record 7 May 2025. Again, this is “Dr. Kang and his gang” at work; the exception here is that the researchers for this paper are all affiliated only with Georgia State University. And, again, the entire paper is available only through institutional access or through paid access. Keep in mind the emphasis of the paper on “intranasal vaccine delivery.”
This particular paper is the result of Dr. Kang’s, et al., research using another “mixture” of influenza viruses — H1N1 (“swine flu”, a subtype of Influenza A), plus H3N2 (a non-human influenza virus in pigs that can infect humans, https://oklahoma.gov/health/health-education/acute-disease-service/disease-information/influenza-a-h3n2-variant-.html), plus H5N1 Avian Influenza. Screenshots from the “snippets” of this paper that are available online are below: the Abstract; a portion of the Viruses section; and, a portion of the Acknowledgements section:
It appears that the paper purports to prove that the intranasal method of “vaccine delivery” is superior to the current intramuscular (injection) method. It is also clear that experiments that were performed were Gain-of-Function work — this time, combining various Influenza A subtypes (“swine flu” that infects humans; “swine flu” that can infect humans; and, Avian Influenza); plus, Influenza B. It is also clear that these experiments were designed to have maximum effect on the CD4 – CD8 cells and the IgG system. By the way, neuraminidase is an important component in the spread of influenza virus in human lungs. Interferon-y (IFN-y) is an element that is important in the regulation of immune and inflammatory responses, among other functions.
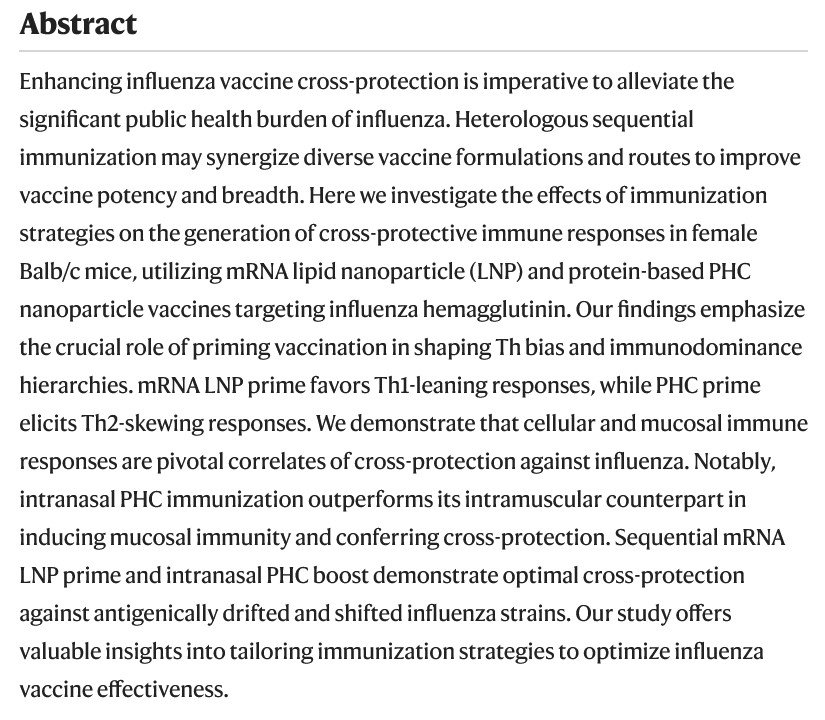
**** There is one more paper by “Dr. Kang and Gang” at GSU that bears scrutiny; this one, published in July 2024: https://doi.org/10.1038/s41467-024-50087-5, “Enhancing cross-protection against influenza by heterologous sequential immunization with mRNA LNP and protein nanoparticle vaccines”, Sang-Moo Kang, et al., 10 July 2024. This paper describes Gain-of-Function experiments not only with various influenza viruses (H3N2 and H7N9 [H7N9 is an Avian Influenza virus that is particularly lethal to humans who get infected with it]); it also describes what can only be Gain-of-Function experiments with “delivery methods” for the TWO different kinds of influenza “vaccines” that use EITHER lipid nanoparticles, OR use PHC (a protein-based nanoparticle.) Several screenshots from this paper are below, starting with the Abstract; then, Figure 1.; followed by a portion of the Discussion section:
The LNPs (lipid nanoparticles) used in the “mRNA initial series vaccine” in the experiments in the above paper are: DOTMA (cationic lipid, used in gene therapies, enhances gene transfection); DOPE (enhances intracellular “delivery” of the “vaccine” ingredients); and, DMG-PEG2000 (nanoparticle version of polyethylene glycol; one of the two LNPs in the Moderna modRNA COVID-19 “vaccines”, the other being SM-102.)
It appears that this paper describes how a “multi-delivery method” of a 2-injection series of a modRNA influenza “vaccine”, followed by a 1-dose “booster” of an intranasal modRNA influenza “vaccine”, is the “optimal” method for “cross-protection” against infection.
The “PUNCH LINE” section of today’s offering follows:
**** In fact, it appears that the above paper claims that modRNA influenza “vaccine” intramuscular injection (IM injection) is now to be considered as “priming the pump” for the subsequent use of modRNA intranasal delivery of the influenza “vaccine” in order to have “sufficient protection” against infection. In other words — TWO types of “delivery methods” need to used.
The above paper was funded by NIH grants R01AI101047 and R01AI143844 to “Dr. Kang and Gang” researcher Bao-Zhong Wang. Dr. Wang, by the way, seems to be from Communist China, having earned his PhD from the Chinese Academy of Sciences in 2003.
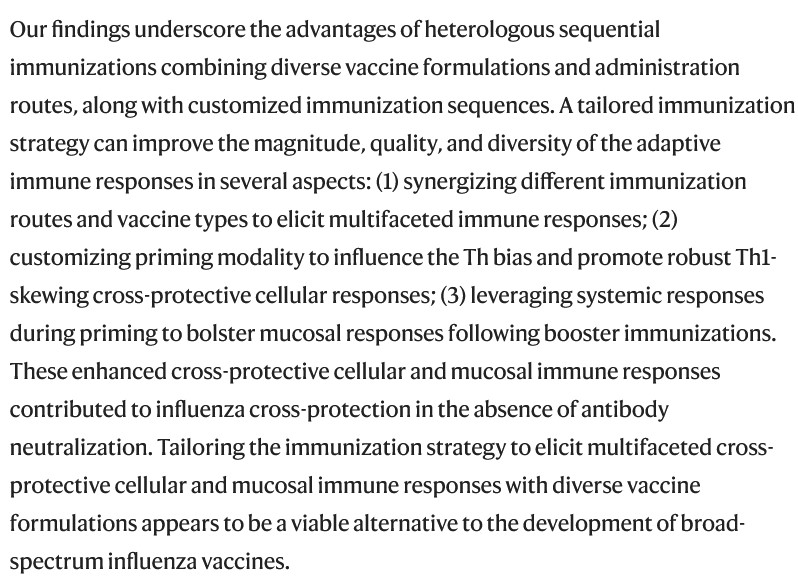
Which brings Yours Truly back to the “Broadly Protective Influenza Vaccine” Patent that is owned by Dr. Jeffery Taubenberger, a “career employee” of the NIH who is now the Acting Director of the NIAID. Yours Truly has written about this scientist in the Health Friday offering of 29 August 2025, cited above in today’s offering. This is the “Universal Influenza Vaccine” that Dr. Taubenberger developed at the NIH: https://www.techtransfer.nih.gov/tech/tab-3388, “Broadly Protective Influenza Vaccine Comprising a Cocktail of Inactivated Avian Influenza Viruses”, published 6 July 2020. A screenshot from this page is below:
Note the “intranasally or intramuscularly” in the above statement.
All of the foregoing appears to point in the direction of a “universal influenza vaccine” that includes various types of influenza viruses (“swine flu”; Avian influenza; Influenza B); that would require at least three doses of a “vaccine” to have “sufficient protection”; and, that the “delivery methods” of the three doses appears to be 2 intramuscular injections of a modRNA plus cationic lipid nanoparicles “vaccine” to “prime the pump”, plus 1 “booster dose” of an intranasal modRNA plus PHC-nanoparticle “vaccine” to “provide sufficient protection” from infection. And, that this situation is being “influenced”, so to speak, by the “new direction” of the NIAID, led by Acting Director Dr. Jeffery Taubenberger.
One must ask: Why is there so much emphasis on a “universal influenza vaccine” that combines elements of “swine flu” viruses, of various Avian Influenza viruses, and, of the Influenza B virus? Why is there an emphasis on “aged populations” in the Gain-of-Function experiments described above in today’s offering?
The free header image for today’s offering is courtesy of Dreamstime.com/ and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering speaks of the disaster of the COVID-19 “vaccines” (Bioweapon Toxin Injections), Yours Truly dedicates it to all those persons who have taken these “vaccines” and have since suffered injuries, illnesses, or disabilities, resulting from them; and, to the memory of all those persons who have taken these “vaccines” but who then passed away due to their deleterious effects. The foregoing is not a kind of “boilerplate” — it is to help ensure that those who have suffered from taking these “vaccines” are not forgotten.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except perhaps for AI-generated images in certain of the linked URLs in the post. If readers wish to post AI-generated content in the discussion thread for today’s offering, they must cite their source. Thank you.
“For the first six weeks, the vaccine is ineffective.” Not so fast. The following is proof that the COVID-19 “vaccines” are “effective” —not in the “official government statements” ways (“prevention of COVID-19”; “reducing risk of severe infection and death from COVID-19”, etc.), but insteadin the multiple negative ways in which these injectables weredesigned to be, and are still designed to be, from the moment they are injected into a person’s body. Please note: the list below is not exhaustive. The following are examples of what may be termed the “Actual Efficacy” of the modRNA COVID-19 “vaccines”:
Theykill: https://kirschsubstack.com/p/new-analysis-of-the-czech-covid-vaccines, “New analysis of the Czech COVID vaccine data reveals that the mRNA shots were deadly for all ages. They should be pulled from the market.”, 28 August 2025. Please see the screenshot from this article, below, which shows that death occurred in COVID-19 “vaccinated” persons in the Czech Republic within a month after said “vaccination“:
The death rates from COVID-19 “vaccination” began to rise on 1 June 2021, the start date of the statistical analysis timefrane on the chart above.
They cause myocarditis and/or pericarditis among the COVID-19 “vaccinated“: The “primary source material” proof on this situation is furnished by Pfizer-BioNTech itself — the BNT162b2 Post-authorization report that the company gave to the FDA on 30 April 2021. The report is found here: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, “5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENTS REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021”, by Worldwide Safety, Pfizer-BioNTech. The APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST section begins on Page 30 of this report. This section lists the 1,291 types of serious adverse events reported among persons who took BNT162b2 between 11 December 2020 (the date that the FDA granted the initial Emergency Use Authorization (EUA) for this modRNA COVID-19 “vaccine”), and the end of February 2021 — a span of only 79 days (11.2 weeks.) Please see Page 6 of the APPENDIX 1 section (Page 35 of the report), where “Myocarditis” listed; and, Page 7 of the same section (Page 36 of the report), where “Pericarditis” is listed. Screenshots of the salient portions of each page are below; first, of Page 6:
And, of Page 7:
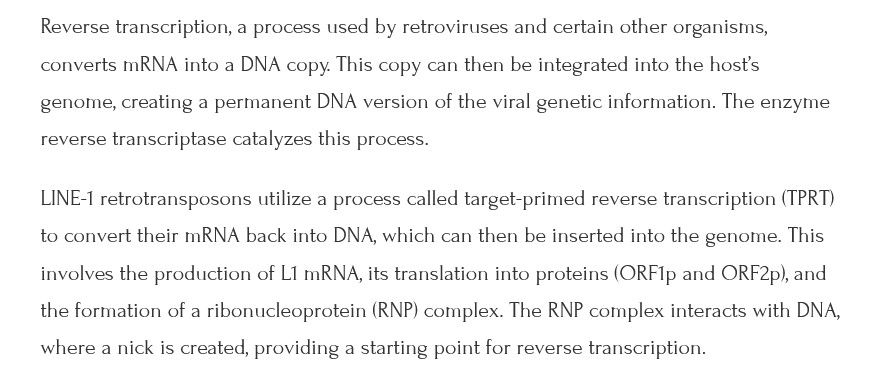
Theycausepermanent alteration of the DNA of the LINE-1 cells of the COVID-19 “vaccinated” person’s body(this permanent alteration is accomplished within 48 hours after “vaccination”): Please see: https://doi.org/10.3390/cimb44030073, “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Markus Alden, Yang De Marinis, et al., 22 February 2022. Figure 2 from this paper is below. BNT162b2 is reverse transcribed into LINE-1 human liver cells within 48 hours post-“vaccination”, resulting in permanent alteration of the DNA of these cells:
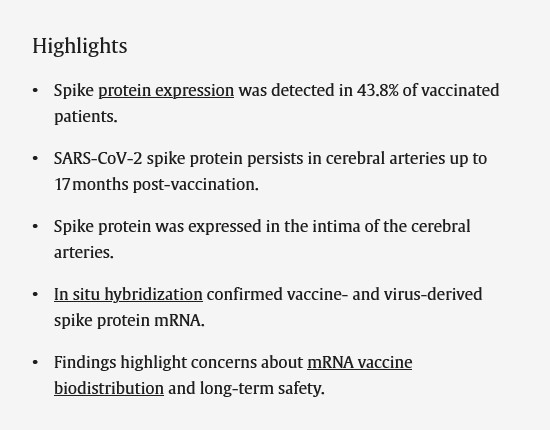
Theycross the Blood-Brain Barrier and facilitate entry of the spike protein into the cerebral arteries: Please see https://doi.org/10.1016/j.jocn.2025.111223, “Expression of SARS-CoV-2 spike protein in cerebral Arteries: Implications for hemhorragic stroke Post-mRNA vaccination.”, Nakao Ota, et al., June 2025. A screenshot of the Highlights section of this paper is below:
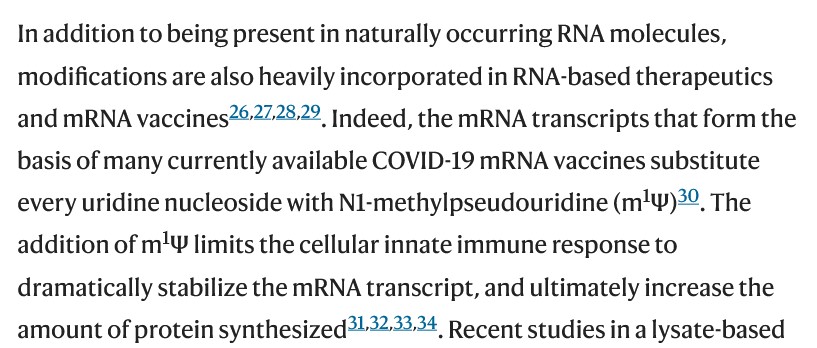
Theyreplace all of the RNA of the natural Uridine in the “vaccinated” person’s body with the lab-created compound, N1-Methylpseudouridine. This replacement “turns off” the functions of the natural Uridine. The N1-Methylpseudouridine then acts as a “facilitator” for the spread of the ingredients of the modRNA COVID-19 “vaccines” throughout the body; and, via the vagus nerve (which natural Uridine helps to regulate the functions and mechanisms thereof), into the brain. Please see https://www.nature.com/articles/s41467-024-51301-0, “N1-Methylpseudouridine and pseudouridine modifications modulate mRNA decoding during translation”, Kristin S Koutmou, et al., 16 September 2024. A screenshot of a portion of the Introduction of this paper is below:
“Substitute” the RNA of the Uridine is a fancy way of saying, “Destroys the RNA, then replaces it with N1-Methylpseudouridine.”
By the way, the “primary source document” regarding the fact that N1-Methylpseudouridine destroys all of the natural RNA of the Uridine in the “vaccinated” person’s body (along with details and descriptions of the other ingredients in BNT162b2, such as the inclusion of lipid nanoparticles) is found in the Worldwide Patent declaration for BNT162b2 by Pfizer-BioNTech. This document was published on 28 October 2021. It is found here: https://patents.google.com/patent/WO2021213945A1/en, “CORONAVIRUS VACCINE”, by Pfizer-BioNTech. Click on “Download PDF” for the entire document.
They cause serious Central Nervous System (CNS) issues, since they cross the Blood-Brain Barrier: Multiple CNS issues result from modRNA COVID-19 “vaccination”; among them, new-onset Multiple Sclerosis. Again, the “primary source document” for this is the 5.3.6 Post-Authorization report cited above. Please see the salient portion of Page 6 of the APPENDIX 1. section of this report (Page 35 of the report), below:
Please also see: https://doi.org/10.1016/j.jneuroim.2021.577785, “New diagnosis of multiple sclerosis in the setting of mRNA COVID-19 vaccine exposure”, Karlo Toljan, et al., 9 December 2021. A screenshot of section 3.2 Case 2 from this paper is below:
They accumulate COVID-19 “vaccine” ingredients (modRNA, spike protein, lipid nanoparticles, and all the other elements of this injectable) in every organ and area of the “vaccinated” body: Please see another “primary source document” from Pfizer-BioNTech regarding this situation. The document is found here: https://icandecide.org/wp-content/uploads/2022/03/125742_S1_M2_26_pharmkin-tabulated-summary.pdf, “BNT162b2 2.6.5 Pharmacokinetics Tabulated Summary”, by Pfizer-BioBNTech. The company gave this document to the FDA on 21 January 2021. Page 7 and Page 8 of the document are below; first, Page 7:
And, Page 8:
Please note that these accumulations begin to occur within 30 minutes after injection with BNT162b2. Please also note that the formulation used in the Wistar lab rats experiments above is the same formulation that was granted the initial FDA Emergency Use Authorization for use in the United States on 11 December 2020; and was subsequently FDA-approved under the name COMIRNATY.
In terms of the “waning efficacy” of the COVID-19 “vaccines”: It was shown in the large Penn State University study of 2022 that COVID-19 “vaccine efficacy” wanes badly by the fifth month after “vaccination”; in fact, the “efficacy” begins to wane well before that. Please see https://doi.org/10.1186/s12879-022-07418-y, “SARS-CoV-2 vaccine effectiveness against infection, symptomatic and severe COVID-19: a systematic review and meta-analysis”, Paddy Ssentengo, et al., 7 May 2022. A screenshot of the Results section of this paper is below:
VE = Vaccine Effectiveness
It is also known that the COVID-19 “vaccines” do not prevent COVID-19 infection; they do not prevent death from COVID-19 infection in “vaccinated” persons; they do not prevent the spread of the virus; and, that any “efficacy” from these injectables wanes almost completely well before seven months post-“vaccination.” In short, the COVID-19 “vaccines” are ineffective in what they were / are “officially” designed to do. On the other hand, these injectables are “effective” in causing “vaccine”-induced injuries, illnesses, disabilities, and death.
HHS Secretary Kennedy, Jr.: All COVID-19 “vaccines” must be pulled off the market and removed from use. Now.There is no rational reason why these injectables are still being authorized, approved, or administered. The Amendment 12 to the PREP Act regarding COVID-19 Medical Countermeasures, signed by former HHS Secretary Xavier Becerra in December 2024, must be rescinded. Bring those who lab-created the COVID-19 “vaccines” brought to account. Get Ivermectin, Hydroxychloroquine, Vitamin C, Vitamin D, Azithromycin / Doxycycline, Zinc, NAC, and Quercetin all FDA-approved for prevention and treatment of COVID-19 infection. Get these items made readily available to the general public and also to medical professionals.
The header image for today’s offering is courtesy of https://genesdev.cshlp.org/content/37/21-24/948.full, “LINE-1 retrotransposition and its regulation in cancers: implications for therapeutic opportunities”, Carlos Mendez-Dorantes, and Kathleen H. Burns, 13 December 2023.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering speaks of the disaster of COVID-19 (the COVID-19 virus itself, and the COVID-19 “vaccines”), Yours Truly dedicates it to all persons, of whatever age or location: who have contracted a COVID-19 infection and recovered from it, but who also have residual complications from the infection; who have suffered COVID-19 “vaccine”-induced injury, illness, disability, or “Long COVID”; or, who have passed away, either from complications from an infection of the COVID-19 virus itself, or from COVID-19 “vaccine”-induced issues caused by these “vaccines” they had in their body.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except for perhaps some AI-generated images embedded in links cited in today’s offering. If readers wish to include any AI-generated content in today’s discussion thread, they must cite their source. Thank you.
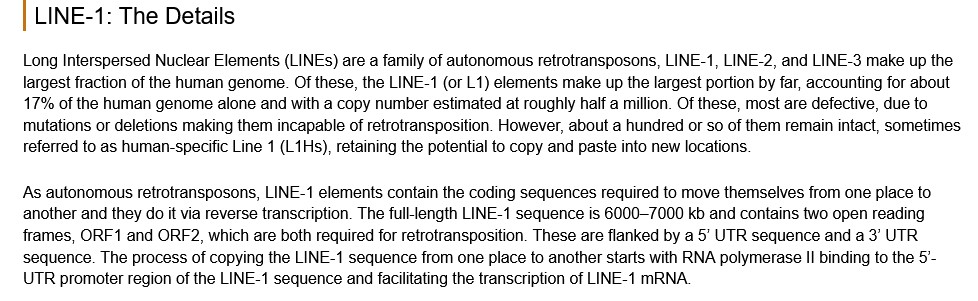
Today’s offering is Part One of two. It is not a lesson on human anatomy or on human genetics: it is a presentation of some of the most-recent information regarding the dangers and deadliness of the COVID-19 “vaccines” (Bioweapon Toxin Injections.) Yours Truly will emphasize at the start that more and more information that exposes these dangers and deadliness is coming out by the week — the “information trickle” of previous years regarding this situation is becoming a torrent. There is also information that potentially links some of the deleterious effects of the COVID- 19 “vaccines” back to the original Wuhan Hu1 SARS-CoV-2 (COVID-19) virus itself. Please bear with me: what may look like “diffuse parts” are all important pieces of the whole.
There is some “background information” that is necessary to “lay the groundwork” for the rest of today’s offering. Yours Truly begins here, with a paper by Ralph Baric, PhD, of the University of North Carolina, Chapel Hill, from 2006. The paper is found here: https://www.jcvi.org/sites/default/assets/projects/synthetic-genomics-options-for-governance/Baric-Synthetic-Viral-Genomics.pdf, “Synthetic Viral Genomics: Risks and Benefits for Science and Society”, Ralph S. Baric, PhD. In Yours Truly’s opinion, this paper can be viewed as a “blueprint” for the future Gain-of-Function (GoF) lab-experimentation with, and the lab-creation of, viruses such as the Wuhan Hu1 SARS-CoV-2 (COVID-19) virus; and the more-recent GoF experiments with strains of the H5N1 (Avian Influenza) virus. Please see the screenshots from Dr. Baric’s 2006 paper, below:
YT: Note the mentions, right at the start in the paper, about “biological warfare” and “biodefense.”
YT: The above images are from the Baric 2206 paper. Figure 4b appears to “outline” how to lab-create (Gain-of-Function work) of “synthetic coronavirus” genome codes.
There is also something else of interest to point out regarding one of the References in the 2006 Baric paper: Reference 45. The referenced paper is found here: https://www.embopress.org/doi/full/10.1038/sj.emboj.7600640, “Receptor and viral determinants of SARS- coronavirus adaptation to human ACE2.”, Li, W., et al., 24 March 2005. This paper discusses the GoF experiments performed to determine and then lab-create elements of various rat and palm civet coronaviruses to the ACE2 receptor cells of humans. Recall that rat and civet coronaviruses experiments were performed at the Wuhan Institute of Virology in the process of lab-creating the SARS-CoV-2 (COVID-19) virus itself. Please see the screenshots from the paper, below. The first is from the authors’ “summary” a the top of the paper; the second is the end of the Discussion section of the paper:
Ralph Baric, PhD, was also working on the “cross-species adaptation and transmission” aspects of SARS- coronaviruses. For example, this paper: https://pmc.ncbi.nlm.nih.gov/articles/PMC2838128/, “Recombination, Reservoirs, and the Modular Spike: Mechanisms of Coronavirus Cross-Species Transmission”, Rachel L Graham, Ralph S Baric, 11 November 2009. The paper specifically discusses Spike 1 residues and ACE2 receptor cells in coronaviruses found in Himalayan palm civets; bats; and raccoon dogs — and the possibility that these coronaviruses can “leap” to humans.
And, Second, from ActiveMotif (https://www.activemotif.com/blog-line-1, “LINE-1 Elements: Walk the LINE-1”, Michelle Tetrault Carlson, PhD, 13 September 2022):
LINE-1 cells are found throughout the human body. LINE-1 aberrations are involved in the following conditions: Genetic disease; cancers (lung; ovarian; bladder; colon; breast; brain [glioma]; and, liver.) LINE-1 aberrations / changes are also involved in aging and “aging related diseases” (per the article above, in the “LINE-1 and Aging” section.)
LINE-1 (also called L1) cells have been studied for some time; in particular, the association between L1 “retrotransposition” and disease. This is important in the context of what will be discussed next.
L1 cells can be “retrotransposed.” This will create “genetic instability.” Such retrotransposition can occur as an aberration resulting from genetic predisposition in the body. Please see: https://doi.org/10.1016/S0092-8674(02)00839-5, “Human L1 Retrotransposition Is Associated with Genetic Instability”, David E. Symer, et al., 9 August 2002. The Abstract from this paper is below:
This paper also discusses the role of SV40 in L1 retrotransposition. In addition, there is a section entitled, “L1 Is an Engine for Genetic Change.”
“Transposed” L1 cells can be involved in the establishment of cancers: https://doi.org/10.1101/gad.351051.123, “LINE-1 retrotransposition and its deregulation in cancers: implications for therapeutic opportunities”, Carlos Mendez-Dorantes, Kathleen H. Burns, 13 December 2023. Please see the screenshot from this paper (a graphical “process image” of L1 being “retrotransposed”), below:
The alarm bells have been ringing regarding the dangers of LINE-1 (L1) retrotranposition (“reverse transcription”) effect of the modCOVID-19 “vaccines” for some time. Examples: the “Maurol, et al.” paper of March 2022: https://www.hilarispublisher.com/articles/intracellular-reverse-transcription-of-covid19-mrna-vaccine-eminvitroem-in-human-cell-87770.html, “Intracellular Reverse Transcription of COVID-19 mRNA Vaccine In-Vitro in Human Cell.”, Maurol, Luisette Mauro, Naseer Almukthar, Tarro Giulio, and Gamal abdul Hamid, et al., J Genet DNA Res6(2022):116. Please see the screenshot from this article, below:
YT: Note the mention of a timeframe of 5-10 years that is needed to study the effects of the “transcription activity.” Keep this in mind when reading the end of today’s offering.
Then, there is the “Alden, et al.” paper from April 2022: https://www.mdpi.com/1467-3045/44/3/73, “Intracellular Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Markus Alden, Yang De Marinis, et al., 11 April 2022. Please see the screenshots from this paper, below. The first is from the paper itself; the second, an image of the Pfizer-BioNTech BNT162b2 reverse transcription of DNA, is Slide 14 from the Doctors for COVID Ethics article (https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, Michael Palmer, MD, and Sucharit Bhakdi, MD, August 2022):
And, the “Acevedo-Whitehouse and Bruno” paper from February 2023: https://doi.org/10.1016/j.mehy.2023.111015, “Potential health risks of mRNA-based vaccine therapy: A hypothesis”, K. Acevedo-Whitehouse, R. Bruno, 6 February 2023. Please see the screenshots from this paper, below; the first is part of the Abstract; the second is the end of the Consequences and discussion section:
This harks back to the information that there are natural reasons for DNA alteration in a person’s body (for example, inherited genetic aberrations.) **** However, the issue here is the fact that the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna contain ingredients and mechanisms that deliberately and permanently alter the DNA of the human LINE-1 cell lines of any person who takes these “vaccines” — even one injection of them. This includes DNA alteration in the body of a fetus of an expectant mother who takes modCOVID-19 “vaccines”, due to the fact that these “vaccines” cross the placenta and into the body of the fetus. (And, by the way, those same ingredients and mechanisms are present in all “descendant clone” modRNA COVID-19 “vaccines” made by these companies, including the “booster shots” and the “latest version formula” injectables. This is because these are based on, and contain elements of, the original modRNA COVID-19 “vaccines” by these companies.)
Then, the second screenshot, below:
YT: **** Please read this phrase again, from Dr. McCullough, regarding the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna: “…sadly, both Pfizer and Moderna do permanently alter DNA via reverse transcription.” It is the “permanently alter DNA via reverse transcription” effects from these injectables that the COVID-19 “vaccinated” in the United States and all over the world are starting to present. It is impossible that the FDA did not know about the potential DNA-altering effects of the modRNA COVID-19 “vaccines” — especially after scientific papers were published which demonstrated that this indeed is the case.
Another piece of the situation has just been published: According to the CDC, 76.4% of all American adults have at least one chronic disease (2023 figures), compared to baseline 2013 figures. The CDC paper is here: https://cdc.gov/pcd/issues/2025/04_0539.htm#ContribAff, “Trends in Multiple Chronic Conditions Among US Adults, By Life Stage, Behavioral Risk Factor Surveillance System, 2013 – 2023”, Kathleen B. Watson, MD, et al., 17 April 2025. All of the authors of this paper are either employees of the CDC; or, of the United States Uniformed Health Services. While it is true that chronic diseases, such as arthritis, can develop for many reasons during adult years, there is NOT ONE WORD in this paper regarding COVID-19 “vaccination” in this age group (18 years – 65+ years) being involved in the increase of any of the chronic diseases that are listed. In other words — the CDC still has its “head firmly in the sand” regarding the dangers and deadliness of the modRNA COVID-19 “vaccines”, and the role of these “vaccines” in inducing and/or aggravating multiple types of chronic conditions.
**** What are “COVID-19 “vaccinated” Joe or Jane Average American” going to do when they find out and understand (which they will, eventually) that the most fundamental “building block” of their body — their DNA — was deliberately and permanently altered without their knowledge or consent, if they took any injection of a Pfizer-BioNTech or a Moderna modRNA COVID-19 “vaccine”?That it doesn’t matter when the “vaccine” injection was put into their body, or how many injections? That their modRNA COVID-19 “vaccinated” children ALSO had their DNA deliberately and permanently altered without their parents’ or guardian’s knowledge or consent?That the state and local governments who “mandated” or legislated that the modRNA COVID-19 “vaccines” be taken by their children in order for them to attend school were complicit in the DNA alteration in their children?
**** What will “COVID-19 “vaccinated” Joe or Jane Average American” do when they find out and understand (which they will, eventually)that the altered DNA in their “vaccinated” body will “lurk” in the body and brain, creating permanent dysfunction of multiple organs of said body, until a modRNA COVID-19 “vaccine”-induced injury, illness, or disability presents later on? That is very likely no “cure” or “turning the clock back” for this altered DNA in the “vaccinated” body?
**** What will “COVID-19 “vaccinated” Joe or Jane Average American” do when they find out and understand (which they will, eventually)that the medical professionals they trusted when they took the modRNA COVID-19 “vaccines” have betrayed them at the most basic level —“Do No Harm”— by not doing the investigation which would have alerted them to this danger — but, which medical professionals, instead, followed the CDC / FDA / AMA mantras of, “The COVID-19 vaccines are safe and effective”, and “The known and potential benefits of the COVID-19 vaccines outweigh the known and potential risks”?
The people who included the elements and mechanisms in the Pfizer-BioNTech and Moderna modRNA COVID-19 “vaccines” that guarantee the deliberate and permanent reverse-transcription of the LINE-1 DNA of every COVID-19 “vaccinated” person; the people who knew about these reverse-transcription elements and mechanisms, but still allowed EUAs and “FDA full approval” of these “vaccines” to proceed; the people who intentionally withheld vital information regarding the real dangers and deadliness of the modRNA COVID-19 “vaccines” from President Trump45 during “Operation Warp Speed”; the people who, even today, are still “recommending” COVID-19 “vaccination” for anyone of any age (paging Dr. Martin Makary, current FDA Commissioner) — all must answer for their actions.All modRNA COVID-19 “vaccines” must be removed from use and pulled off the market — now.
The featured vintage image of a laboratory for today’s offering is courtesy of iStock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except perhaps for AI-generated images in links included in today’s post. If readers wish to add any AI-generated content to the discussion thread today, they must cite their source. Thank you.
Today’s offering is about the “under-the-table” work, the “being performed but under another name” work, the “grandfathered-in” work, of Gain-of-Function (GoF) experiments that are onoing. These GoF experiments involve experiments with mRNA-based platforms; with “inactivated virus” platforms; and, with “novel delivery” platforms.These GoF experiments are being funded by “private Big Money”; and, by the United States government (in other words, with taxpayer money.)This post is long; please bear with me.
It is now well-known that the COVID-19 disaster was a product of GoF experiments, of two types: One, the GoF work that was performed in various labs (the Baric Lab at UNC, Chapel Hill; the Wuhan Institute of Virology, Wuhan, Communist China; the United States Army biological weapons labs at Ft. Detrick, Maryland, among others.) And, Two, the GoF work that was performed using the lab-created Wuhan Hu1 SARS-CoV-2 virus itself as the foundation for the modRNA (aka mRNA) COVID-19 “vaccines” that were developed by numerous companies, among them: PfizerUSA (at the company’s Pearl River, New York, facility; and, at other facilities); and, BioNTech (Mainz, Germany); Moderna (with the NIAID in Bethesda, Maryland, and at other facilities) — for use in the United States and also world-wide. (Note: PfizerUSA and BioNTech are separate companies that operate as a “joint venture” called Pfizer-BioNTech. PfizerUSA and BioNTech each have a separate CEO [Chief Executive Officer].)
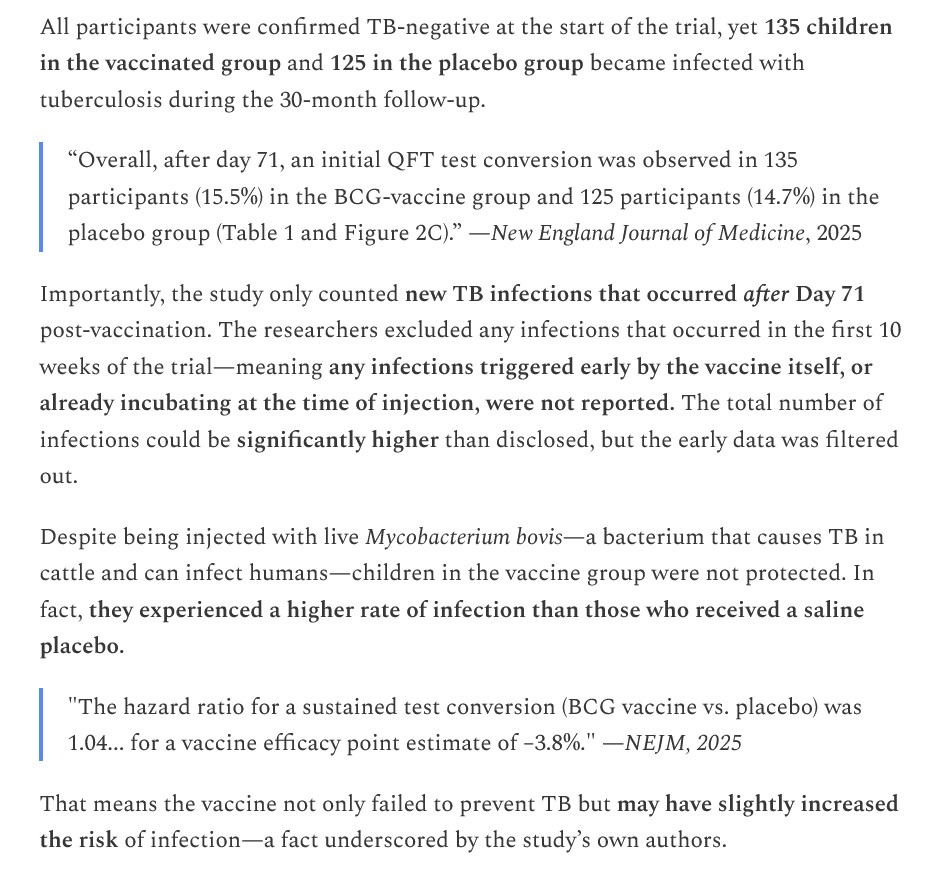
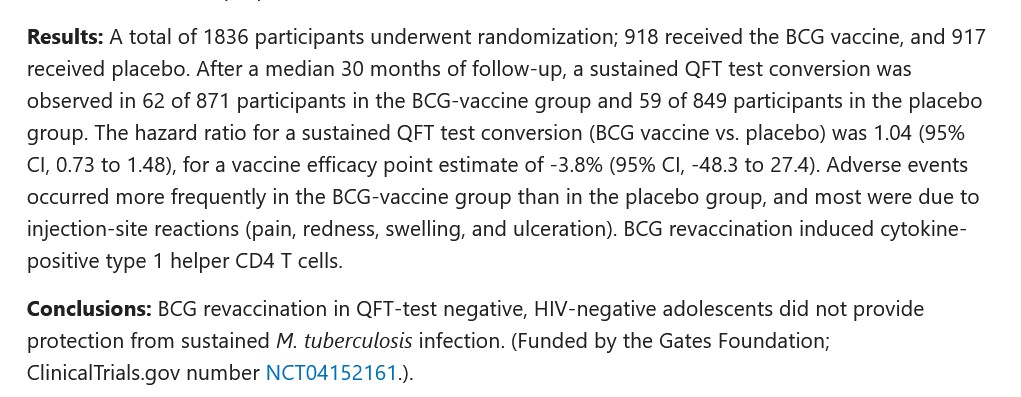
Regarding the first Jon Fleetwood article: The 260 study subject children were living in South Africa, and were between the ages of 10 and 18 years. They were confirmed by to be HIV-negative at the time they were added to the study subject pool. They were injected with the Danish tuberculosis vaccine BCG1331 strain (Bacille Calmette-Guerin). The Package Insert for this vaccine is here: https://nibsc.org/documents/ifu/07-270.pdf. The BCG1331 strain is the Mycobacteriumbovis strain, which causes tuberculosis in cattle and can also cause the disease in humans, especially in HIV-compromised persons. Please see the screenshot from the Fleetwood article, below:
The paper that resulted from the study is here: https://doi.org/10.1056/NEJMoa2412381, “BCG Revaccination for the Prevention of Mycobacterium tuberculosis Infection”, Alexander C Schmidt, et al., 8 May 2025. Please see the screenshot from this paper, below:
In other words, 260 children now have tuberculosis because of the BCG1331 strain vaccine that they were injected with. And that Bill Gates funded this “human guinea-pig experiment.” But there’s more — the Fleetwood article also describes the Bill Gates-fundedMycobacterium bovis experiments at the University of Texas, performed in 2012, that resulted in a what may be called a “turbo-charged Gain-of-Function” version of this tuberculosis bacterium. The paper that was published from the 2012 study is here: https://doi.org/10.1016/S1472-9792(13)70007-6, “Mycobacterium tuberculosis MtrAY102C is a gain-of-function mutant that potentially acts as a constitutively active protein”, Akash T Satsangi, et al., published December 2013.
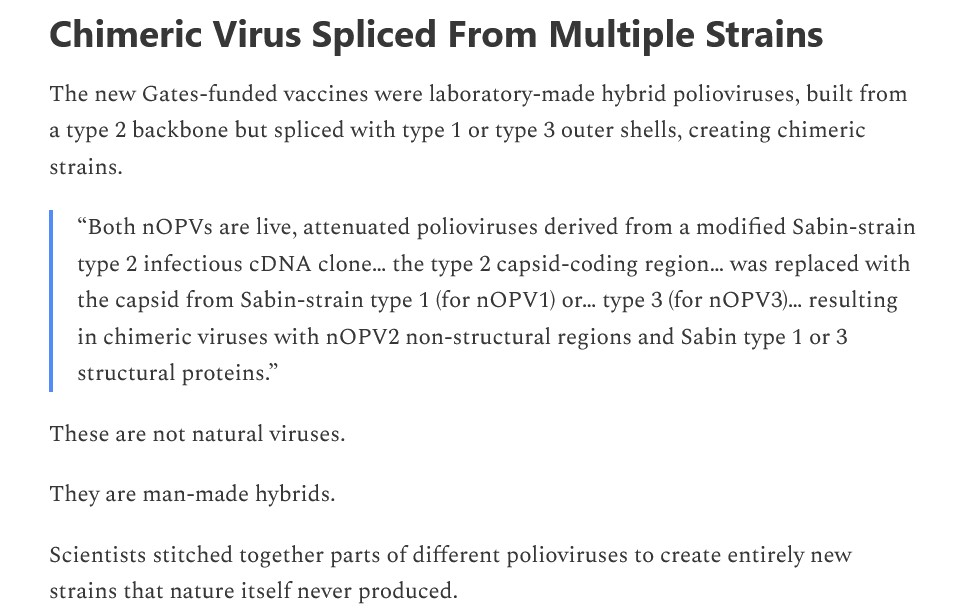
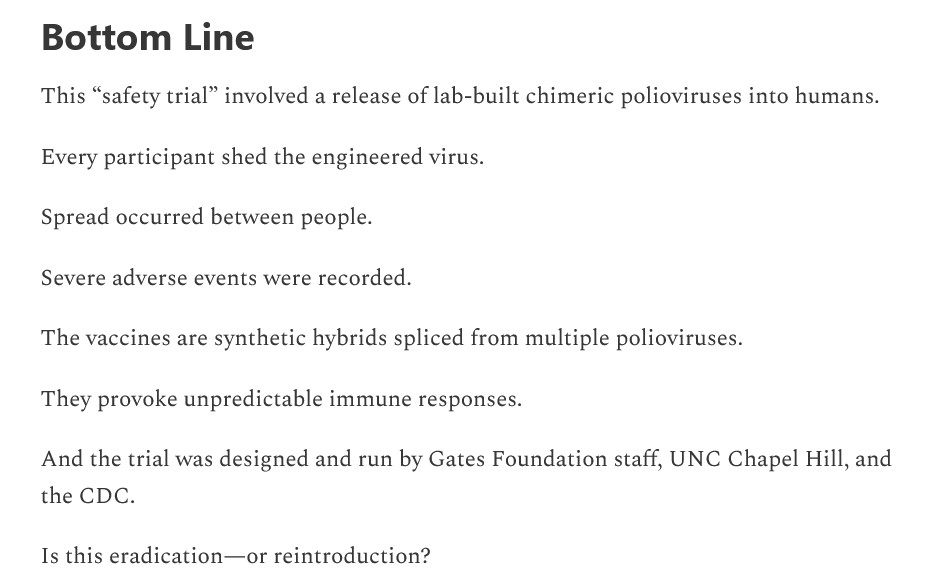
Regarding the second Fleetwood article: Another Bill Gates-funded effort, this time about a lab-created chimeric polio oral “vaccine” that was tested on human subjectsin the United States. The study results are nothing short of terrifying. Please the screenshot from the Fleetwood article, below:
There was a 100% incidence of “shedding” of this lab-created chimeric oral polio “vaccine.” Six human subjects were released from the study when it was found that testing of their stool showed they had possibly contracted the oral vaccine virus from other study subjects. Several human subjects had severe adverse reactions to this lab-created chimeric oral polio “vaccine.” This lab-created chimeric oral polio “vaccine” caused “unexpected” interactions with the type 2 poliovirus.
The team that lab-created this chimeric oral polio “vaccine” were from medical centers across the United States, including: University of North Carolina, Chapel Hill; University of Vermont; and, Dartmouth. The paper that was published from the study is here: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(25)00285-3/fulltext, “Safety and immunogenicity of novel live attenuated type 1 and type 3 oral poliomyelitis vaccines in healthy adults in the USA: a first-in-human, observer-masked, multicentre, phase 1 randomized controlled trial”, Laina D Mercer, PhD, et al., 13 August 2025. The clinical trial for this lab-created chimeric polio virus “vaccine” is listed here: https://clinicaltrials.gov/study/NCT04529538. Again, from the Fleetwood article:
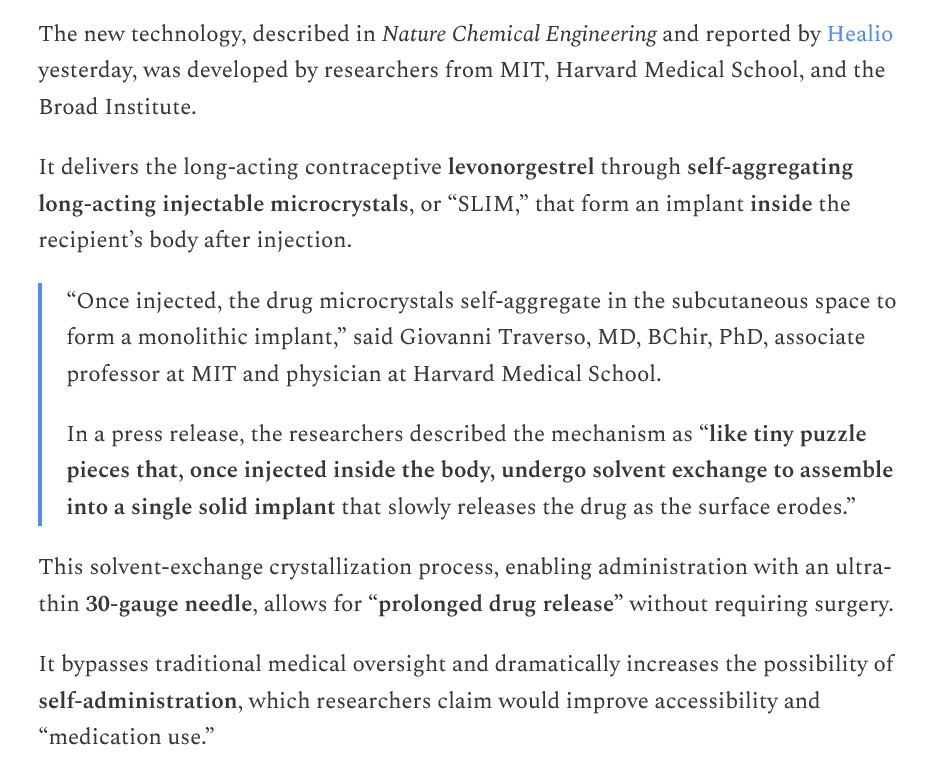
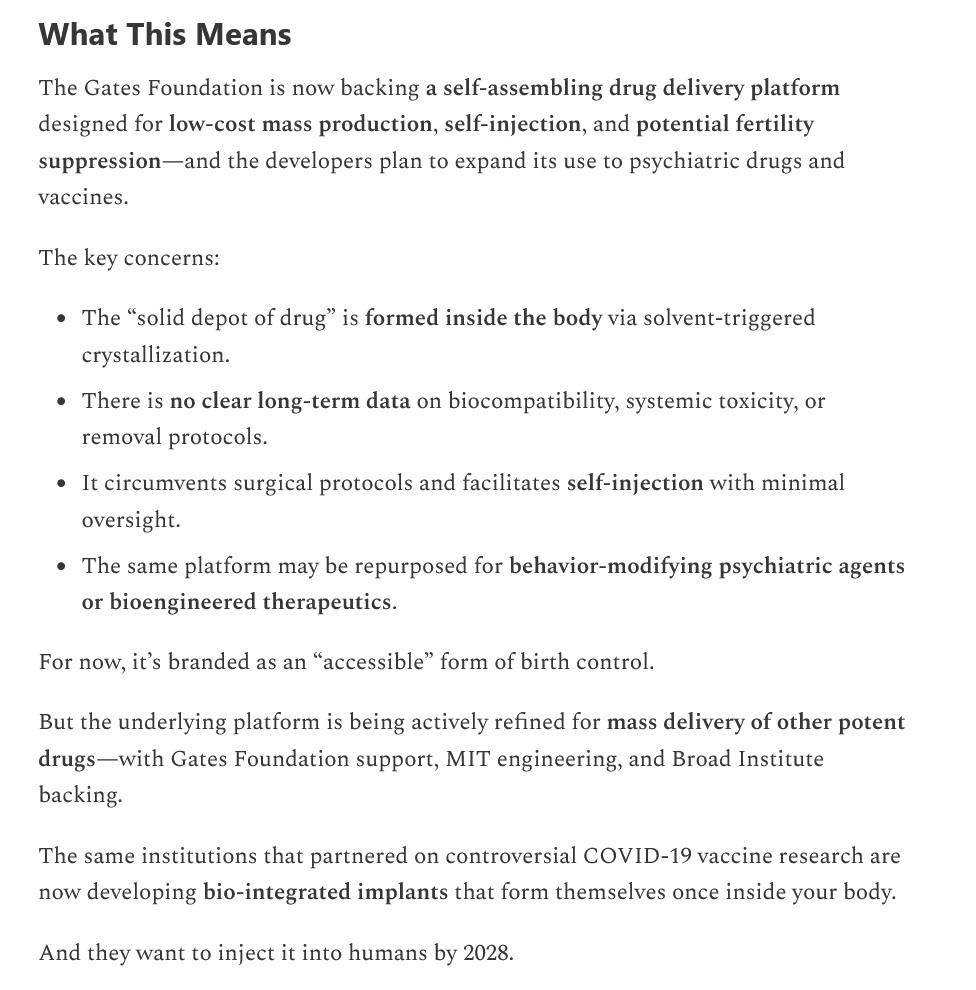
Regarding the third Fleetwood article: Bill Gates has funded the creation of a new technology, called “SLIM microneedle”, which injects “microcrystals” of a contraceptive drug (levonorgestrel) into the body of a female; and, which microcrystals then”self-assemble” into an “implant” inside her body. Please see the screenshot from the Fleetwood article on this situation, below:
This type of “self-injected, self-assembly inside the body” approach has profound implications. Please see below, again from the Fleetwood article:
The paper that was published on this issue is here: https://www.nature.com/articles/s44286-025-00194-x, “Self-aggregating long-lasting injectable microcrystals”, Vivian K. Feig, et al., 24 March 2025. Note how “self-assembling” has magically become “self-aggregating” — in some attempt to hide the fact that the microcrystals really do “self-assemble?”
The SLIM “delivery system” for the contraceptive levonorgestrel (called “LNG” in the paper above) uses a solvent called Benzyl Benzoate (called “BB” in the paper above.) The paper describes the experiments performed to find the “right combination” of levonorgestrel + Benzyl Benzoate to create the SLIM delivery system — the “winning delivery system candidate” was named “LNG-BB.” Benzyl Benzoate is clearly dangerous. Part of Section 4 FIRST AID MEASURES from the MSDS Safety Sheet on Benzyl Benzoate from Spectrum Chemical (https://www.spectrumchemical.com/) is below:
And this is the “long-lasting solvent” that is used in the SLIM microneedle “self-aggregating” delivery system for levonorgestrel. Which means that this solvent will be acting in the body of the female who uses this delivery system for this drug for an (undetermined) amount of time.
Now, on to a recent GoF experiment, this one funded by NIH / NIAID, at the University of Pittsburgh. This GoF experiment resulted in the lab-creation of a chimeric H5N1 Avian Influenza virus strain that could infect dairy cattle. Jon Fleetwood wrote about this situation, here: https://jonfleetwood.substack.com/p/nih-funded-pennsylvania-researchers, “NIH-Funded Pennsylvania Researchers Build New Frankenstein Bird Flu Virus: ‘Journal of Virology'”, 26 August 2025. Vesicular stomatitis virus (VSV) is a virus that infects horses and cattle. In humans, Stomatitis infection can result in HSV-1 (the “cold sore” virus: per https://my.clevelandclinic.org/health/diseases/stomatitis-oral-mucositis.) However, the researchers at the University of Pittsburgh concentrated on “splicing” an element of VSV with H5N1. The paper that was published from this experiment is here: https://doi.org/10.1128/jvi.00621-25, “Dairy cattle herds mount a characteristic antibody response to highly pathogenic H5N1 avian influenza viruses”, Kevin R. McCarthy, et al., 25 August 2025. Please see the screenshots from the Fleetwood article on this issue, below:
Isn’t it “convenient timing” that this “new, chimeric VSV + H5N1 virus” comes on the heels of the announcement by the White House on 5 May 2025, that Gain-of-Function research would be stopped — but it appears that “certain contracts” would be permitted to “finish out”? And, that one of those “certain contracts” is with Arcturus Therapeutics for its self-amplifying RNA (saRNA) Avian Influenza “vaccine”, ARCT-2304? The White House announcement is here: https://www.whitehouse.gov/presidential-actions/2025/05/improving-the-safety-and-security-of-biological-research/. The news release related to the second quarter 2025 financial update and “pipeline progress” for Arcturus Therapeutics in which ARCT-2304 is mentioned, is here: https://www.biospace.com/press-releases/arcturus-therapeutics-announces-second-quarter-2025-financial-update-and-pipeline-progress, 12 August 2025. The clinical trial for ARCT-2304 is registered here: https://clinicaltrials.gov/study/NCT06602531; which, by the way, has NO saline-only Placebo control group; the only “control groups” in the study will be injected with a “control vaccine” or a “placebo vaccine” (which last, in and of itself, is not a true Placebo.)
And now, regarding something else: the GoF experiments that resulted in the lab-creation of an Avian Influenza “vaccine” which is a “Cocktail of Inactivated Avian Influenza Viruses”, a patent owned by Dr. Jeffery Taubenberger, a “career medical employee” of HHS and the federal government, and who is also the current Acting Director of the NIAID (National Institute of Allergy and Infectious Diseases, previously headed by Dr. Anthony Fauci), and who now is in control of the $500 Million dollars that was pulled from mRNA research activities in May 2025.This “bird flu vaccine cocktail” contains BPL (Beta-propiolactone), a known carcinogen.
The NIH TechTransfer information on this “cocktail” invention by Dr. Taubenberger is here: https://www.techtransfer.nih.gov/tech/tab-3388, “Broadly Protective Influenza Vaccine Compromising a Cocktail of Inactivated Avian Influenza Viruses”. Sounds “benign,” yes? Until one starts reading the actual Patent document itself, found here: https://image-ppubs.uspto.gov/dirsearch-public/print/downloadPdf/11369675, filed 21 July 2020. The following are screenshots from the Patent document:
Note it appears that Dr. Taubenberger was experimenting with as many as sixteen different strains of Avian Influenza to lab-create his “cocktail vaccine.”
Note it appears that Dr. Taubenberger is perfectly all right with “vaginal” and “rectal” administration of his “cocktail vaccine.”
Note that the Patent was registered in July 2020 — which can only mean that work on the experiments to lab-create this “Avian Influenza cocktail vaccine” must have begun at least nine months earlier. This would place the commencement of the experiments around October 2019 — just before the COVID-19 original virus was unleashed on on the world.
And THIS ingredient is part of the “Avian Influenza Cocktail Vaccine” of Dr. Jeffery Taubenberger, two possible methods of administration of which are INTRANASAL or INHALED, per the Patent document images above?
It is not enough that HHS Secretary Robert F. Kennedy, Jr., terminated 22 contracts for mRNA research in May of this year, but allowed “certain contracts” for mRNA (and saRNA) research to “finish out.” It is not enough that the White House announced a ban on Gain-of-Function research, since this type of research is still going on — funded by “private Big Money”, and/or by the NIH / NIAID (in other words, the United States government). The entire Gain-of-Function situation must be stopped, from all funding sources and on all levels of research and experimentation — until there are clear, firm, and enforceable regulations and restrictions on who can perform this type of research; that such research can only be permitted under strict circumstances; that such research must be under tight supervision; and, that such research can only be performed where there is a clear need in the area of public health —not what amounts to a “chimeric fishing expedition” to lab-create viruses. It is time for any and all “go-along-to-get-along” activities to stop — such as, bowing to the “demand” by Sen. Dr. Bill Cassidy for his “cooperation” in “working with” HHS as regards hiring, or anything else. By the way — Sen. Dr. Cassidy has received donations from multiple pharmaceutical entities (United Health, AstraZeneca, Pediatrix Medical Group, and so on: per Open Secrets (https://opensecrets.org/.) And — that the further development of the above-discussed “Avian Influenza Cocktail Vaccine” must be stopped.
HHS Secretary Kennedy, Jr.: Please understand that the “career medical bureaucrats” in the CDC, the FDA, and the other divisions of the HHS, are not inclined to your views. They want “the good old days” of these divisions brought back. They are working “behind the scenes” in some instances, and in other instances, out in the open, to obstruct, delay, and thwart your efforts to clean up HHS and “re-tool” the department to reflect Make American Healthy Again. There is even what may be called “soft interference” by persons not employed by HHS such as, Sen. Dr. Cassidy.
The header image of smallpox vaccination in Paris in 1905 used in today’s offering is courtesy of Alamy and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering speaks of the disaster of COVID-19, Yours Truly dedicates it to all persons, of whatever age or location, who have suffered injuries, illnesses, or disabilities, either COVID-19 “vaccine”-induced, or as the result of a COVID-19 infection; and, to all persons, of whatever age or location, who have passed away either from the negative effects of the COVID-19 “vaccines” they had in their bodies, or as the result of a COVID-19 infection.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except for AI-generated images that may be included in links in today’s offering. If readers wish to add any AI-generated content to the discussion thread today, they must cite their source. Thank you.
“Clean Sweep.” This means completely dismantling the FDA (the Food and Drug Administration); the NIH (the National Institutes of Health); and, the NIAID (the National Institute of Allergy and Infectious Diseases), all of which are divisions of the United States Department of Health and Human Services (HHS) — and completely rebuilding them from the top down. Why “Clean Sweep” for these divisions? Because it is becoming more apparent by the week that they are more devoted to using “career” medical bureaucrats/officials, many of whom are “holdovers” from the “Collins / Fauci era” in the NIH and NIAID; they are more devoted to injecting American citizens with the proven-dangerous, proven-deadly COVID-19 “vaccines” than they are to approving readily-available, cheap drugs (such as, Ivermectin) and other therapeutics (such as, Zinc) to prevent or to treat COVID-19 infection; and, they are more devoted to pushing through injectables via “Fast Track” or “accelerated approval” methods, rather than taking the time to fully test and analyze test data. “Completely rebuilding them from the top down” means establishing entirely redesigned divisions that are fully devoted to the betterment of the public health.
Yours Truly presents a transcript of the op-ed published in the Washington Post on 12 August 2025 by Dr. Jay Bhattacharya, the current Director of the NIH (National Institutes of Health); the op-ed appears here: https://www.washingtonpost.com/opinons/2025/08/12/nih-mrna-vaccines-jay-bhattacharya/, “Jay Bhattacharya: Why the NIH is pivoting away from mRNA vaccines”, 12 August 2025. Yours Truly provides her personal commentary, which will appear in Bold and surrounded in brackets. (The Washington Post op-ed is behind a paywall; Yours Truly is indebted to Shannon Joy, whose X tweet has the entire article: https://xcancel.com/ShannonJoy/status/1956140133474034025.) Note: Yours Truly will make it clear that the commentary is done with all due respect to Dr. Jay Bhattacharya, MD.
The transcript: “The U.S. Department of Health and Human Services’ decision to wind down its mRNA vaccine development activities marks a necessary pivot in how we steward public health innovation in vaccines. The right path requires us to consider the inherent strengths and weaknesses of a technology as well as any alternatives, along with public attitudes and experience with the technology. The mRNA platform is promising technology. I do not dispute its potential. In the future, it may yet deliver breakthroughs in treating diseases such as cancer, and HHS is continuing to invest in ongoing research in oncology and other complex diseases.”
[YT: First of all, if HHS is truly going to “wind down” mRNA vaccine development, why is Moderna being allowed to progress to Phase 3 clinical trials of its modRNA “vaccine” against CMV (Cytomegalovirus), mRNA-1647? This “vaccine” contains six different mRNA sequences, two different antigens, the dangerous lipid nanoparticle SM-102 (the same LNP that is in the Moderna modRNA COVID-19 “vaccine”, SPIKEVAX), and apparently targets both the IgG immune system cells and the CD4-CD8 cells of the body. Please see: https://doi.org/10.1128/jvi.01603-23, “Characterization of humoral and cellular immunologic responses to an mRNA-based human cytomegalovirus vaccine from a phase 1 trial of healthy adults”, Kai Wu, et al.; J Virol. 2024 Mar 25;18(4):e01603-23. Please refer to Fig. 2 and Fig.4. Secondly, the current modRNA (aka mRNA) COVID-19 “vaccines” have demonstrated that they do not have “inherent strengths”: in fact, they only have what may be called “inherent dangers.” These “inherent dangers” include: altering of the LINE1 Human Liver cell line; replacement of natural Uridine RNA with the lab-created N1-Methylpseudouridine; crossing the Blood-Brain Barrier to attack areas of the brain that are not protected by this barrier (for example, the Pituitary Gland); causing autoimmune attack on heart tissue via aggregation of lymphocytes induced by the COVID-19 “vaccines” in that organ; and, causing infiltration of lymphocytes in lung tissue. Regarding the DNA alteration, and heart and lung damage, caused by the COVID-19 “vaccines”, please see: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, Michael Palmer, MD, and Sucharit Bhakdi, MD, Slide 9 through Slide 14. Thirdly, why on Earth is oncology (cancer study, diagnosis, and treatment) included in the phrase “and other complex diseases?” Yours Truly calls this a writing mistake; however, one believes someone should have proofread the op-ed for “context or syntax” issues before publication.]
“But as a vaccine intended for broad public use, especially during a public health emergency, the platform has failed a crucial test: earning public trust. No matter how elegant the science, a platform that lacks credibility among the people it seeks to protect cannot fulfill its public health mission.”
[YT: The “public trust” for the COVID-19 “vaccines” was destroyed when it was proven that hundreds of persons who took these injectables passed away from immediate heart attacks induced by them just after being injected; when “vaccinated” persons began to present with myocarditis or pericarditis after being injected; when stillbirths and miscarriages began to be reported among pregnant women who had been injected; and much, much more. And, by the way, the initial modRNA COVID-19 “vaccine” rollout in December 2020 was intended for the elderly and for healthcare workers; it was when the “COVID-19 health emergency” was declared in March 2021 that the “vaccines” began to be “mandated” for all persons. “Elegant science?” Does “elegant science” include the kind of “science” that was rushed through the initial EUAs for the modRNA COVID-19 “vaccines” without proper testing and data analyses?]
“It is critical to understand the development of the mRNA coronavirus vaccines in the context of the very successful Operation Warp Speed launched during the first Trump administration.”
[YT: Does “the development of the mRNA coronavirus vaccines” include the fact that neither Pfizer-BioNTech, nor Moderna, had never previously brought a successful mRNA injectable to market prior to “Operation Warp Speed?” And that Dr. Albert Bourla, DVM, the CEO of PfizerUSA, admitted on video that he had been “convinced” by Pfizer scientists to use the then-new and unproven mRNA technology in a COVID-19 “vaccine?” (10 March 2022, “Albert Bourla on why mRNA technology was “counterintuitive” to producing an effective vaccine”, https://www.youtube.com/watch?v=t9_YRw7jBF4.)]
“Operation Warp Speed represented a paradigm shift in how the government should invest in new technologies and solutions and embrace strategic investments in public-private partnerships, innovation in trial design and removal of bureaucratic red tape to allow parallel rather than sequential vaccine development. It produced a new vaccine in record time and also helped develop a successful monoclonal antibody.”
[YT: Really? “Embrace strategic partnerships in public-private partnerships?” What about that “public-private partnership” document between the NIAID and Moderna, which includes development of RNA-based vaccines, and that was filed with the SEC in 2015, several years BEFORE the COVID-19 disaster? That “partnership” is still going on, with patent-ownership sharing, royalty payments sharing, “partnering” in developing new COVID-19 “vaccines”, and so on, until at least 2041. “Innovation in trial design?” — Meaning the “Next Gold Generation Standard”, announced in May 2025, in which lab testing with animals using humane, safe protocols, then progressing to better and safer human-subject testing, may well be replaced with “Petri-dish testing” only” for new “vaccines”? “Parallel vaccine development?” — Meaning that “Universal Vaccine” that’s touted in the “Next Gold Generation Standard?”]
“Unfortunately, the Biden administration did not manage public trust in the coronavirus vaccines, largely because it chose a strategy of mandates rather than a risk-based approach and did not properly acknowledge Americans’ growing concerns regarding safety and effectiveness.”
[YT: So, “risk-based approach?” Like the “risk populations chart” in the “opinion piece” that Dr.Martin Makary and Dr. Vinay Prasad published in the New England Journal of Medicine in May 2025 (https://doi.org/10.1056/NEJMsb2506929, “An Evidence-Based Approach to Covid-19 Vaccination”— a chart in which, for example, even healthy pregnant women are considered to be at “risk” for “severe complications from COVID-19” and should get COVID-19 “vaccinated?” And what about the statements about how the “known and potential benefits of the for COVID-19 vaccines outweigh the known and potential risks?” — like the one here: https://www.cdc.gov/vaccines/covid-19/planning/children/6-things-to-know.html, “6 Things to Know about COVID-19 Vaccination for Children.“]
“Consider the data: In a late 2024 Pew Research Center survey, 60 percent of American adults reported no intention of getting an updated coronavirus mRNA vaccine despite the Center for Disease Control and Prevention’s advice that nearly all adults receive yet another dose. As of late April 2025 (the latest data published reported by the CDC), only 13 percent of children between the ages of 6 months and 17 years had received an updated coronavirus vaccine, even though the Biden-era CDC had placed the vaccine on the childhood immunization schedule.”
[YT: It appears that the real reason behind why “only 13 percent of children between the ages of 6 months and 17 years had received an updated coronavirus vaccine” is that their parents or guardians have concluded that these “vaccines” are more dangerous than helpful. And how did these adults come to this conclusion? Because of the news spreading that these “vaccines” cause myocarditis / pericarditis in children; because of the news spreading that these “vaccines” do not prevent COVID-19 infection, but instead actually damage the “vaccinated” person’s immune system, making it vulnerable to COVID-19 infection; and so on. In Yours Truly’s opinion, the COVID-19 “vaccines” have no place in the CDC Childhood Immunization Schedule whatever — due to the foregoing and other reasons.]
“In 2021, the Biden administration’s HHS spent nearly a billion dollars on a campaign supporting the coronavirus vaccine, the most expensive pharmaceutical campaign in history. The government spent the money on a vast number of TV, radio and internet spots, which misinformed the American public that the vaccine would protect them from contracting and spreading covid. Nevertheless, just a few years later, less than half the U.S. adult population will heed the CDC’s guidance. Some outlets have blamed the poor coronavirus mRNA vaccine uptake on poor messaging or “anti-vax” counter-messaging. But the Biden administration made suppression of speech — and a mandate for all on the vaccines — into a priority.”
[YT: Perhaps Dr. Bhattacharya should look at the FDA Package Insert for the modRNA COVID-19 “vaccine”, COMIRNATY (Pfizer-BioNTech), section 1 INDICATIONS AND USAGE. The Package Insert is here: https://www.fda.gov/media/151707/download. Notice that the FDA officially states that COMIRNATY is “to prevent coronavirus disease 2019 (COVID-19.)” Is the FDA “spreading misinformation?”
“The failure was thus not a communications problem. It is a trust problem due to the Biden administration’s scientific overreach, public pressure and, frankly, arrogance.”
[YT: Does this mean that “the new FDA”, and the “Next Generation Gold Standard”, and the “accelerated approval” of “vaccines” that may be lab-created in Petri-dishes will somehow magically restore public trust?]
“In addition to the trust problem, the mRNA technology has special biological features that make it different from other vaccines in that it (ideally) instructs our cells to produce proteins that subsequently invoke an immune response. To do so with complete confidence about vaccine safety and efficacy requires an exact understanding of dosage, biodistribution and off-target effects. Unfortunately, we fall short in all three. We lack clarity on how much antigen each mRNA molecule produces, where in the body the mRNA product winds up, how long it stays in the body, and whether unintended proteins are created.”
[YT: Unfortunately, this paragraph, in Yours Truly’s opinion, “has more holes than a Swiss cheese.” First: the mRNA “vaccines” do instruct the cells of the “vaccinated” person to “invoke an immune response”: that “response”, among other things, causes multiple types of autoimmune attack within the COVID-19 “vaccinated” person’s body — for example, in the heart (please refer above to the article by Doctors For COVID Ethics.) Second: Perhaps Dr. Bhattacharya would like to read this report, which Pfizer-BioNTech gave to the FDA in January 2021, regarding the biodistribution of BNT162b2 (FDA-approved in 2022 as COMIRNATY.) The report is here: https://phmpt.org/wp-content/uploads/2022/03/125742_S1_M2_pharmkin-tabulated-summary.pdf, “MODULE 2.6.5. PHARMACOKINETICS TABULATED SUMMARY.” Yours Truly has included images of Page 7 and Page 8 of this report, which are the Biodistribution Tables for BNT162b2. (The BNT162b2 used in this experiment is the same one that was granted the initial FDA for use in the United States in December 2020.) Third: Stephanie Seneff, PhD, and Greg Nigh, wrote back in 2021 about the unintended consequences of the mRNA COVID-19 “vaccines” creating “unintended proteins.” Their paper is here: https://www.semanticscholar.org/paper/Worse-Than-the-Disease-Reviewing-Some-Possible-of-Seneff-Nigh/, “Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19”, 16 June 2021, International Journal of Vaccine Theory, Practice and Research 2(1), May 10,2021 Page 389 – 430. The point is: there is an “exact understanding” of multiple aspects regarding the mRNA COVID-19 “vaccines” already.]
“From a regulatory perspective, getting approval for a vaccine with such inherent uncertainties should be difficult.”
[YT: Agreed— except that the “new FDA” is doing exactly that already (such as the recent FDA “approval” without any human trials testing of the “2025-2026 Formula COVID-19 Vaccines” by Pfizer-BioNTech, by Moderna, and by Novavax.)]
“Still, I do not believe the mRNA vaccines caused either mass harm on the one hand or saved 14 million lives on the other. Those estimates swing wildly based on speculative modeling, not concrete evidence. A recent modeling study conluded that the global coronavirus vaccination campaign saved 2.5 million lives from 2020 to 2024, mainly among the elderly.”
[YT: “Still I do not believe the mRNA vaccines caused either mass harm…” Really, Dr. Bhattacharya? Did you read through the OpenVAERS website? (https://openvaers.com/) Have you read through the thousands of actual reports of persons who took a COVID-19 “vaccine” and then either died from the injection, or had serious medical issues afterwards from the injection? Are you saying that these reports are “wildly based on speculative modeling?” Are you saying that these reports are not “concrete evidence?” Are you dismissing the extensive work of Ed Dowd, who analyzes statistical reports of claims from insurance companies, claims that have skyrocketed since the COVID-19 “vaccine” rollout in 2021? https://phinancetechnologies.com/, then click on the “Our Projects” PDF brochure on the webpage to find the “Current Projects” section, then click on any of the green arrows.]
“The scientific controversy over the vaccine’s effect on mortality rages on. Science isn’t propaganda agenda. It’s humility.”
[YT: Real science is truth. There isn’t a “controversy” about the “vaccine’s effect on mortality” — the COVID-19 “vaccines” have increased mortality across the board and across the world. Have you read Steve Kirsch’s Substack, Dr. Bhattacharya? (https://kirschsubstack.com/). Mr. Kirsch’s Substack has many articles that quote studies which show that the COVID-19 “vaccines” increase mortality across the board. However, since Mr. Kirsch is not a medical professional, that removes him from “credibility” in the medical professional world, as far as the NIH is concerned? It doesn’t matter that Mr. Kirsch makes his living from collecting and analyzing data (financial and medical)?]
“And when public health officials stopped communicating with humility, we lost much of the public, an absolute necessity for any vaccine platform.”
[YT: Actually: It’s when public health officials withheld the truth about the dangers and the deadliness of the COVID-19 “vaccines” (which the FDA knew about back in early 2021 — please see here: https://phmpt.org/wp-content/uploads/2022/11/5.3.6-postmarketing-experience.pdf, “5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021.” Please go to the APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST section.) — and the public had to find out the truth themselves — that public health officials “lost much of the public.”]
“I am not here to litigate the past. I am here to chart a better path forward. That is why the NIH, under the leadership of HHS Secretary Robert F. Kennedy, Jr., is investing in new vaccine technologies based on whole-virus inactivated vaccines, which offer a broader immune response and have a longer track record of safety and public acceptance.”
[YT: So, here, apparently, is the “kernel” of the op-ed. Dr. Bhattacharya is not interested in anything related to how dangerous and deadly the current types of COVID-19 “vaccines” have been, and still are. “Let bygones be bygones and just move on” seems to the situation. Not so fast, Doctor. And that “whole-virus inactivated vaccine” scheme that is central to the “Next Generation Gold Standard?” The “Universal Vaccine?” Which, according to the “Next Generation Gold Standard” ethos, may be developed in Petri-dishes in federal government-based facilities only? And the PATENT for which “Universal Vaccine” is owned by the current Acting Director of NIAID, Dr. Jeffery Taubenberger? (https://www.techtransfer.nih.gov/tech/tab-3388)]
“We are continuing the Operation Warp Speed model of investing in technology with the most potential to help Americans.”
[YT: And, will this “continued” Operation Warp Speed model again be done in such a way that important information is deliberately withheld from President Trump47, as was the case with the original Operation Warp Speed in President Trump’s first term?]
“We will move forward with scientific rigor, transparency, and humility. At the NIH, we will fund promising research based not on hype, but on evidence. And I will continue to use my platform to communicate candidly in public conversations where debate and disagreement are welcomed.”
[YT: “Humility” is always a good thing. So is TRUTH.]
“We are entering a new era of public health, grounded not in wishful thinking or performative consensus, but in open inquiry and respect for the American people’s intelligence. The only to rebuild trust is to earn it — one honest conversation at a time.”
[YT: The “one honest conversation at a time” must include the honest admission by the NIH / NIAID / FDA / CDC, that the entire COVID-19 “vaccine” disaster could have been prevented through FDA approval of using re-purposed items to prevent or to treat COVID-19 infection: Ivermectin, Hydroxycholorquine, Doxycycline, Zinc and Vitamin D supplementation. There are plenty of peer-reviewed, published scientific papers which prove that these work. Instead, the FDA, TO THIS DAY, still refuses to approve the use of these items to prevent or to treat COVID-19. Can you explain why this is still the case, Dr. Bhattacharya?]
The free header image for today’s offering is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As today’s offering is related, in part, to the disaster of the COVID-19 “vaccines”, Yours Truly dedicates it to all persons who have contracted injures, illnesses, or disabilities, induced or aggravated by the COVID-19 “vaccines” that were injected into their bodies; and, to the memory of all persons who have passed away from the negative effects of the COVID-19 “vaccines” that were injected into their bodies.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except for perhaps AI-generated images in any of the linked URLs below. If readers wish to post any AI-generated content in today’s discussion thread, they must cite their source. Thank you.
There are two sections to today’s Special Report offering: the first section, regarding the now-proven linkage of COVID-19 “vaccine boosters” to increases in cancer and in general mortality; the second section, regarding what appears to be the potential emergence of the “next plandemic” in Communist China. Please bear with Yours Truly: one does not want to “weary by recitals”, as the Duc de Saint-Simon once wrote — but there is a lot of information, multiple screenshots, and so on. The evolving knowledge regarding the disaster called COVID-19 (the virus itself, and the “vaccines”) is gaining speed with each passing day. This evolving knowledge base is important to understand in light of the developments regarding the new information about the “Chikungunya outbreak” currently in China, and which is apparently spreading to other countries (shades of the original COVID-19 virus itself outbreak in China.)
First section, the linkage between COVID-19 “booster vaccines” with increases in cancer and in general mortality. COVID-19 “vaccine boosters” means any injection of a “latest version” of a COVID-19 “vaccine.” This includes the FDA- approved 2025-2026 “new formula COVID-19 vaccine versions” of the Pfizer-BioNTech modRNA COVID-19 “vaccine”, COMIRNATY; of the Moderna modRNA COVID-19 “vaccine”, SPIKEVAX; and, of the Novavax COVID-19 “vaccine”, NUVAXOVID.
Yours Truly begins here: https://slaynews.com/news/renowned-oncologist-sounds-alarm-cancer-deaths-now-surging-among-covid-boosted/, “Renowned Oncologist Sounds Alarm: Cancer Deaths Are Now Surging Among Covid-Boosted”, by Frank Bergman, 6 August 2025. There is an embedded video statement by Prof. Dr. Angus Dalgleish (St. George’s, University of London.) Dr. Dalgleish warns, in no uncertain terms, that it is the suppression of T-cell immune cells in the body of the COVID-19 “vaccine boosted” that is causing the surge of cancer among these persons. Please see the screenshot from the Slay News article, below:
The paper referenced above is here: https://www.researchsquare.com/article/rs-6899448/v2, “Factors contributing to the sharp rise in excess mortality in Japan since 2021”, Atsushi Takahashi, 17 July 2025. This paper is a pre-print. Please see the screenshots from this paper, below. They are: portions of the Results section; Figure 4; and, Figure 9:
The identifier names are those of the Prefectures in Japan that were studied. Even with taking other factors into consideration (examples: the size and population of the various Prefectures; the number of adults in age brackets in the Prefectures; whether or not a Prefecture was “rural” in character and location, as compared to “urban”), it is clear that the increase in mortality is tied to an increased amount of COVID-19 “vaccine boosters” that were administered.
The peer-reviewed paper on the Japan study is here: https://doi.org/10.3390/cancers17122006, “Repeated COVID-19 Vaccination as a Poor Prognostic Factor in Pancreatic Cancer: A Retrospective, Single-Center Cohort Study”, Makoto Abue, et al., 16 June 2025.
Yours Truly has written extensively for the board here regarding the damage / destruction of the natural immune system of the person who takes COVID-19 “vaccines.” These injectables were designed to attack, damage / destroy the CD4 – CD8 immune system cells. These injectables were designed to attack, damage / destroy the IgG3 immune system “fighter” cells, while at the same time, fostering the increase of IgG4 immune system “tolerate and never clear” cells. This damage / destruction increases with each injection of a modRNA COVID-19 “vaccine”, including injections of the “latest formula version” of said “vaccines”, which includes the “2025-2026 Formula versions” of said “vaccines” (COMIRNATY [Pfizer-BioNTech]; SPIKEVAX [Moderna]; and, NUVAXOVID[Novavax.])
The “Seneff and Nigh” paper of 10 May 2021 discusses how “immune system imprinting” in the the body of persons who take the COVID-19 “vaccines” have the potential to result in what the authors call “unintended consequences.” The paper is available here: https://dpbh.nv.gov/uploadedFiles/dpbhnvgov/content/Boards/BOH/Meetings/2021/SENEFF-1.PDF, “Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19”, Stephanie Seneff and Greg Nigh; International Journal of Vaccine Theory, Practice, and Research 2(1), May 10, 2021, Page 38-79. Please see the screenshots from this article, below. They are: the Abstract; the “Unprecedented” box; and, Figure 2.
Second section, regarding the potential for the “next plandemic” to come from Communist China. This has to do with the current emergence of mosquito-borne Chikungunya infections in several areas of China, which has resulted in various government-enforced measures. There is also an ** interesting connection ** to the United States involved in this situation.
What is Chikungunya? It is a virus transmitted by the bite of an infected female mosquito of (usually) the Aedes aegypti or the Aedes albopictus species. (As an aside: female mosquitos of these species can also transmit Dengue fever via bites.) The virus that is transmitted causes joint pain and fever; these can progress to severe. Most people infected with Chikungunya, however, make a full recovery. The virus is an RNA alphavirus. Please see: https://my.clevelandclinic.org/health/diseases/25083-chikungunya; there is a screenshot from this article, below:
Two recent articles regarding the Chikungunya outbreak in China: the first, here: https://jessicar.substack.com/p/the-new-pending-plandemic-is-it-scheduled, “The new pending “plandemic” — is it scheduled for November?”, by Jessica Rose, PhD, 12 August 2025. Dr. Rose makes it clear that the “alphavirus + saRNA-LNP platform” (self-amplifying RNA + lipid nanoparticles “vaccine” platform) is based on the VEEV alphavirus (Venezuelan Equine Encephalitis Virus.) Please see the screenshots from her article, below:
**** Note the mention of immune system issues that are induced in persons who are COVID-19 “vaccinated”, and how this can potentially severely complicate any infection by Chikungunya.
The second article is here: https://www.2ndsmartestguyintheworld.com/psyop-25-scamdemic-update-chinese, “PSYOP-25 SCAMDEMIC UPDATE: Chinese Authorities Mandating Blood Tests, Releasing Lab Mosquitoes to Fight Chikungunya Outbreak”, 13 August 2025. Please see the screenshots from this article, below:
The founder of the “mosquito lab” in Guangzhou is Dr. Zhiyong Xi. Please see the screenshot below from the above link:
Which work, at least in part, is being funded by NIAID (division of NIH — both divisions part of HHS.)
Which begs the following questions: WHY is Dr. Zhiyong XI still doing mosquito research in the United States if he founded a mosquito study lab in Communist China? WHY is Dr. Zhiyong Xi’s research at Michigan State University being funded, at least in part, by the NIH / NIAID?
There are two “FDA-approved vaccines” against Chikungunya: IXCHIQ, and VIMKUNYA. BOTH of these “vaccines” were FDA-approved under “accelerated approval” methods. Please see the screenshots, below, from the Package Inserts for these injectables. First, from the Package Insert for IXCHIQ (https://ixchiqhcp.com/PI-new.pdf):
Note the presence of Aluminum Hydroxide as an adjuvant in VIMKUNYA.
NOTE THAT THE “EXACT MECHANISM OF PROTECTION’ HAS NOT BEEN DETERMINED FOR EITHER IXCHIQ OR FOR VIMKUNYA. In other words, the United States government (via the FDA) is fine with injecting people with these “vaccines” WITHOUT THE FDA KNOWING THE EXACT MECHANISMS OF PROTECTION FOR EITHER OF THEM. What are the “CHIKV-specific immune responses” that these injectables supposedly elicit?
And, by the way, both IXCHIQ and VIMKUNYA can be “shed” onto newborn children if the expectant mother is sick with a virus (this is called viremia) at the time of delivery. A pregnant female who takes either one of the above “vaccines” runs the risk of contracting “viral viremia.” Neither IXCHIQ, nor VIMKUNYA have had proper testing for potential effects on pregnant females, their fetuses, or their newborns (section 8.1 Pregnancy in either Package Insert.)
All of the above begs the following questions: Does HHS Sec. Robert F. Kennedy, Jr., know about these Chikujgunya “vaccines”? Does he know that the FDA approved them under “accelerated approval” methods? Does he understand that the FDA does NOT know the “exact mechanism of protection” for either IXCHIQ or VIMKUNYA? Does Dr. Martin Makary (FDA Commissioner) know about this situation? Do either Sec. Kennedy, Jr., or Dr. Makary know that “career FDA types” in the CBER division signed the FDA Approval Letters for IXCHIQ (signed by R. Douglas Pratt, MD, 6 August 2025) and for VIMKUNYA (signed by David C. Kaslow, MD, 14 February 2025)?
Yours Truly will again emphasize that it is critically important for all persons, whether COVID-19 “vaccinated” or not, to follow some type of COVID-19 spike protein mitigation / prophylaxis protocol. It is also critically important that all persons, whether COVID-19 “vaccinated” or not, to do all they can to build and maintain their general health, and the health of their immune system, so as to be in the best shape possible.