“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
Author: PAVACA
BFA in Piano; BFA in Music Education; MA in Leadership. Retired professional musician and soprano, teacher, composer, accompanist/coach. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 - 2018), First Professor of the Darden School of the University of Virginia. Writes under the names of: M.E. Forbes; M.E.C. Forbes; PAVACA.
The above free vintage image of Thankfulness is courtesy of iStock and Google Images.
Health Friday is a series of posts devoted to Big Pharma, vaccines, general health, and associated topics. However, the discussion is not limited to what is presented today: It is an Open Thread.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
Today’s Health Friday post is devoted to Thankfulness. Beginning with:
Thankfulness for our gracious host, Wolf Moon, who provides The Q Tree as a haven of good cheer, encouragement, support, knowledge, and camaraderie to the online family that are denizens of this particular Tree. We are there for each other, in good times and in difficult times.
Thankfulness for the authors on this board, including our host, for their contributions and their expertise: for the Reminders of the Word of God; for the Physics lessons (Yours Truly’s eyes no longer glaze over at the mere mention of Physics or Astronomy); for the in-depth political / DeepState/ economic Analyses; for the adherence to Truth; for the Sharing of knowledge, of history, of research, of poetry; and so much more, that they bring.
Thankfulness for every commenter on this board, for their bonhomie and constancy.
Continuing with:
Thankfulness that Donald Trump, after surviving two assassination attempts, was re-elected President of the United States.
Thankfulness that there will be a chance that the corruption and deceit rampant in both houses of Congress, and in the White House, can be exposed and cleansed.
Thankfulness that breaches among individuals’ families and friends can be repaired; that our beloved country can be healed of divisiveness; that the United States of America can be restored to her rightful role as a Representative Republic, instead of as a “modern-day application” of the type of “despotic democracy” that helped to undermine, then ruin, ancient Greece.
Thankfulness that the entire truth behind the premeditated disaster of the COVID-19 itself and the COVID-19 “vaccines” can finally be brought to light; that the millions of “vaccinated” persons who are “vaccine”-injured or “vaccine”-disabled can be recognized, and their stories be told; that those who have passed away (either directly or indirectly) from the negative effects of the COVID-19 “vaccines” they took will not have died in vain; and, that Justice will be accomplished regarding those who created this virus, and those who developed these dangerous, deadly “vaccines” for worldwide use.
Thankfulness for this:
Thankfulness, above all, to the Supreme Being who is the Divine Force behind the Founding Fathers of this great land: the Founding Fathers who wrote the Declaration of Independence, the Constitution, and the original Bill of Rights.
The above free vintage image of a scientist at work is courtesy of StockCake and Google Images.
As Gail Combs is apparently still in “locked out” mode for publishing posts (via WordPress, or **some other entity**), our host, Wolf Moon, gave the go-ahead for Yours Truly to do a Placeholder Open Thread for today. I am indebted to our host for this opportunity, as further information has surfaced regarding the role of the pangolin-CoV MP789 virus in the lab-creation of the SARS-CoV-2 (COVID-19) virus itself. Since today’s post concerns the COVID-19 virus itself, and the COVID-19 “vaccines”, it is dedicated to the memory of Yours Truly’s COVID-19 “vaccinated” brother Sam, and to her cousin Bill; and to all persons, of whatever age and location, who have passed away from the negative effects of the COVID-19 “vaccines” that they had in their bodies. However, the discussion is not limited to what is presented here: It is an Open Thread. Bear with me: there are a couple of surprising details coming up. There is a General Summary at the end of the post.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
To Begin: What will be called the “Part 1 Presentation” of the role of the PRRARSV genome code of the pangolin-CoV MP789 in the lab-creation of the SARS-CoV-2 virus itself is here: www.theqtree.com/2024/11/22/health-friday-11-22-2024-open-thread-lets-talk-about-prrarsv-the-backdoor-key/. Yours Truly presented evidence that: One: the pangolin-CoV MP789 virus genome code has “an uncanny similarity” to the PRRARSV genome code that was inserted into the genome code of the SARS-CoV-2 virus itself; Two: that this insertion occurred during the lab-creation process for the genome code of the SARS-CoV-2 virus itself; Three: that this insertion is at or very near the S1-S2 furin cleavage site in the genome code of the SARS-CoV-2 virus itself; Four: that the bat-coronavirus RaTG13 coronavirus also has a role to play in the lab-creation of the genome code of the SARS-CoV-2 virus itself, although the pangolin-CoV MP789 coronavirus genome code has more “areas of similarity” to the SARS-CoV-2 virus genomecode; and, Five: that taxpayer-funded Gain-of-Function experiments were {most likely] used to perform all of the above, and most likely, at the Wuhan Institute of Virology.
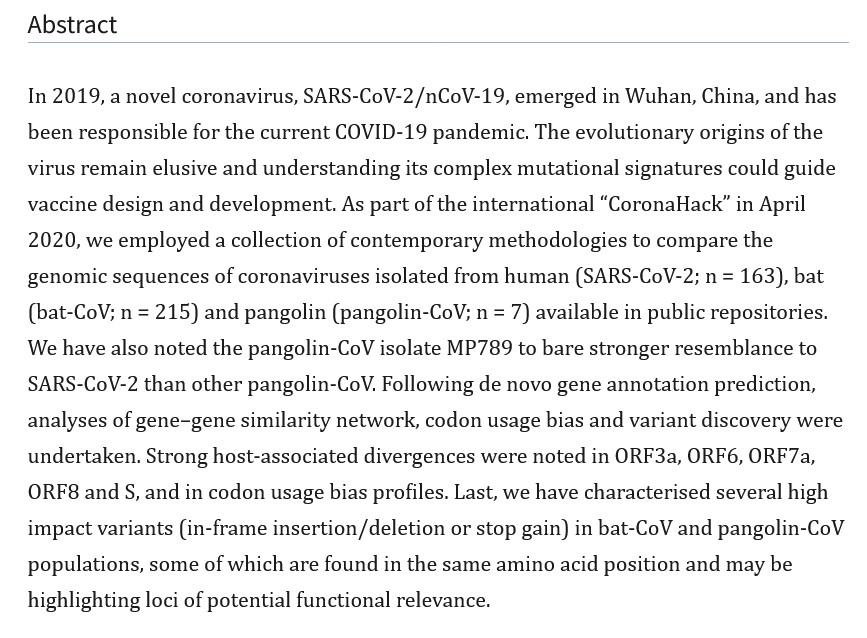
In 2020, the year after the SARS-CoV-2 virus itself was beginning to ravage the world, and when COVID-19 “vaccines” had not yet been granted Emergency Use Authorizations by the FDA in the United States, by the EMA (European Medicines Agency), or by other agencies, a plethora of scientific papers and articles were written and published: papers and articles in which the researchers attempted to pinpoint exactly how the SARS-CoV-2 virus itself came into being. Many of these papers and articles examined the role(s) that various animal coronaviruses may have played in the emergence of the SARS-CoV-2 virus itself: for examples, by “natural evolution”; or, by “recombination” of coronavirus genomes among animals via cross-infection; or, by a “sudden appearance.” These investigations and their published results pre-date the confirmation within the past 18 months that Gain-of-Function experiments at lab facilities, most notably the Wuhan Institute of Virology, were the foundation of the lab-created disaster called the SARS-CoV-2 virus itself (links to Congressional reports on this situation are in the “Part 1 Presentation” Health Friday post, see above.) One such year 2020 scientific paper is the “Dimonaco, et al.” paper: https://pmc.ncbi.nlm.nih.gov/articles/PMC7823979/, “Computational Analysis of SARS-CoV-2 and SARS-Like Coronavirus Diversity in Human, Bat and Pangolin Populations”, Nicholas J. Dimonaco, et al., 30 December 2020. A screenshot of the Abstract of this paper is below:
The Health Friday post cited above discusses Yours Truly’s hypothesis that the pangolin-CoV MP789 coronavirus genome code was chosen, along with the important but actually less-similar bat coronavirus RaTG13 genome code, as the main virus genome that were used to create the SARS-CoV-2 virus itself genome. Today’s post, in Yours Truly’s opinion, presents evidence that “clinches the deal” on the choice of the pangolin-CoV MP789 genome code as the primary one for insertion into the SARS-CoV-2 virus itself genome code — however, the evidence comes from a surprising source.
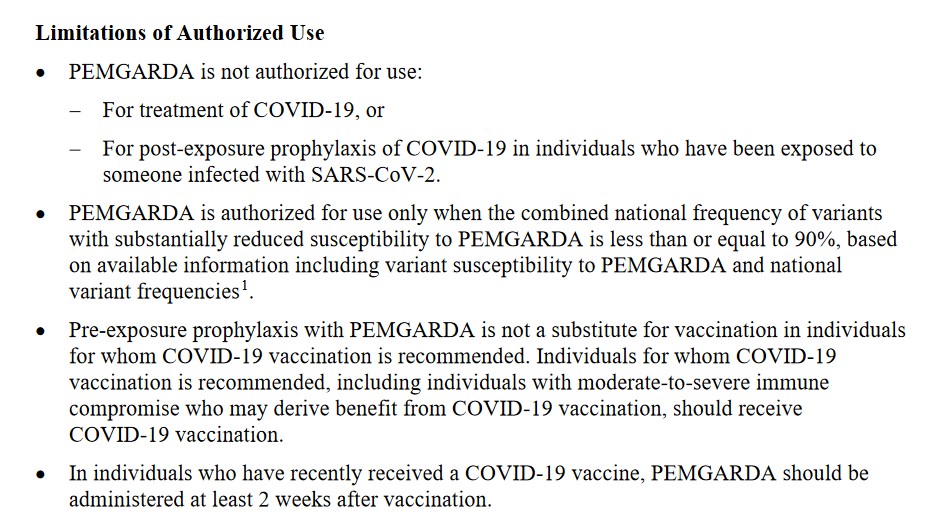
This is the link to the FDA-issued document for healthcare professionals for PEMGARDA: www.fda.gov/media/177067/download (note: PEMGARDA is also called Pemivibart in this document.) There have been no studies performed for PEMGARDA regarding carcinogenicity, mutagenicity, or impairment of fertility (section 13 Nonclinical Toxicology of the FDA document.) Persons who have been prescribed PEMGARDA need to take the infusion (IV) of the drug every 3 months (page 15 of the FDA document.) Also, PEMGARDA is not to be used as a “substitute” for COVID-19 “vaccination” (page 15 of the FDA document.) More details from the section Limitations of Authorized Use of the FDA document are below:
There is a slew of other warnings (including Black Box warnings), cautions, and restrictions regarding PEMGARDA in the FDA document.
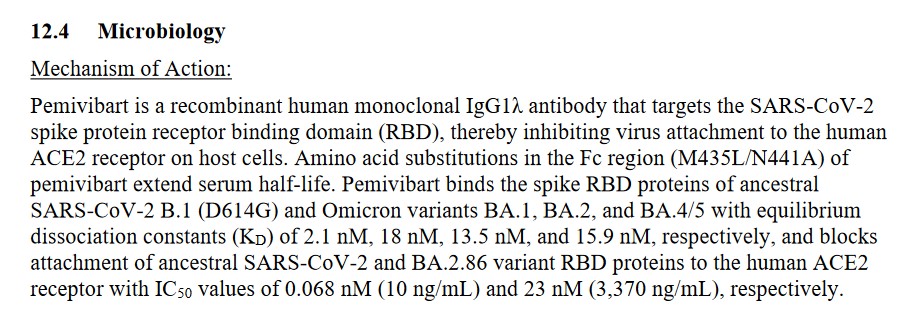
Here is a screenshot of section 12.4Mechanism of Action of the FDA document on PEMGARDA (aka Pemivibart):
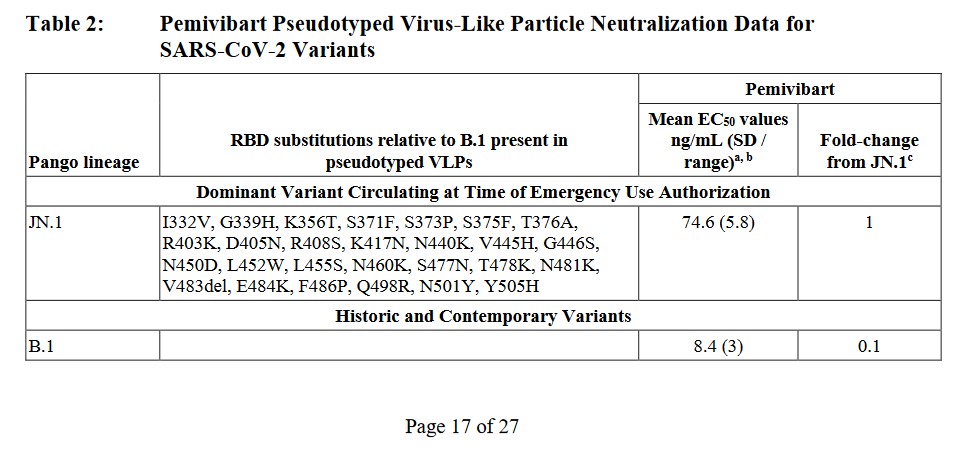
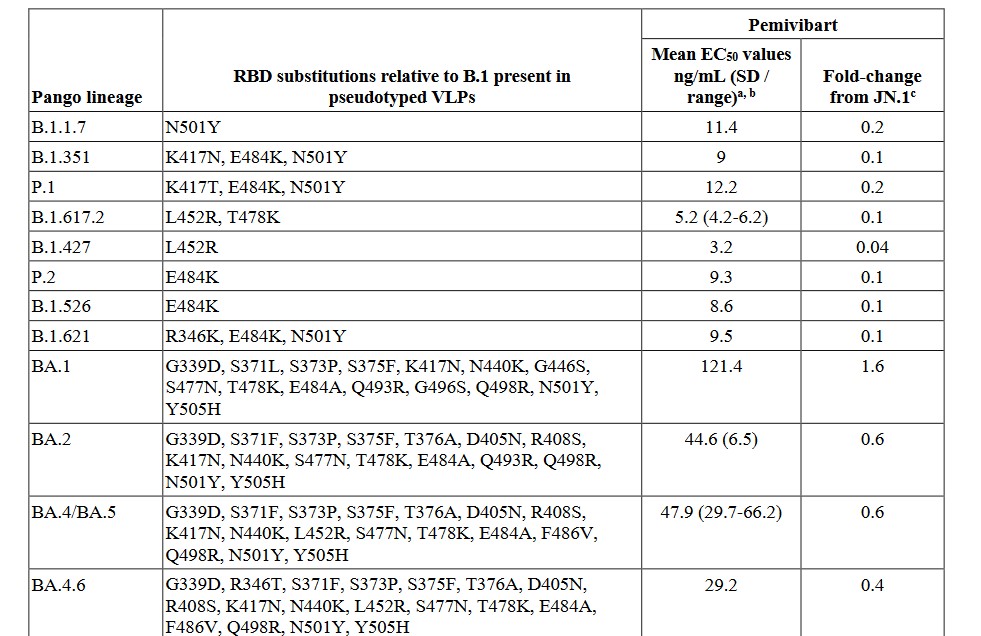
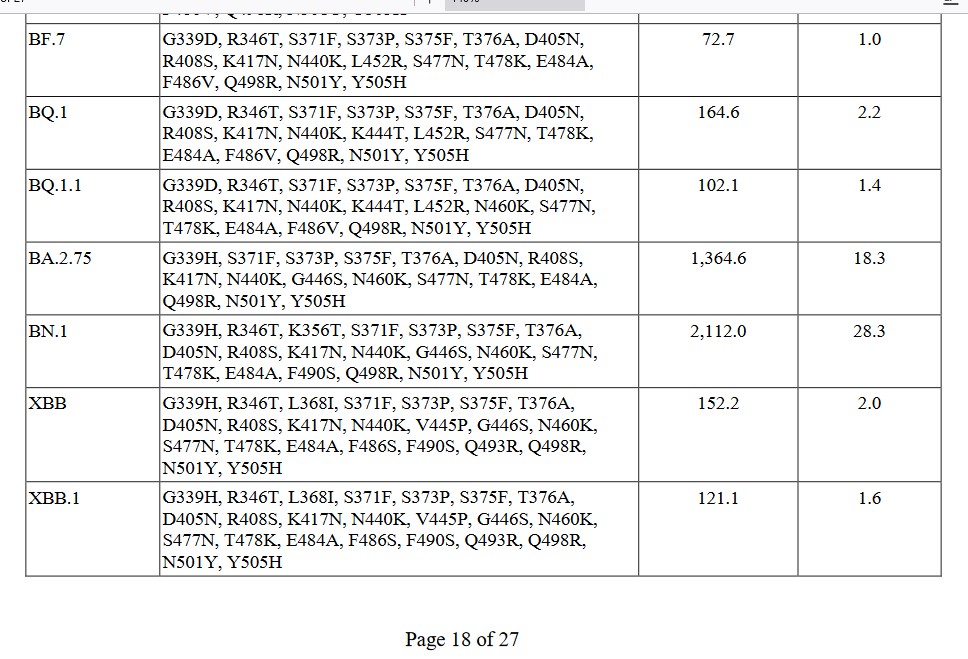
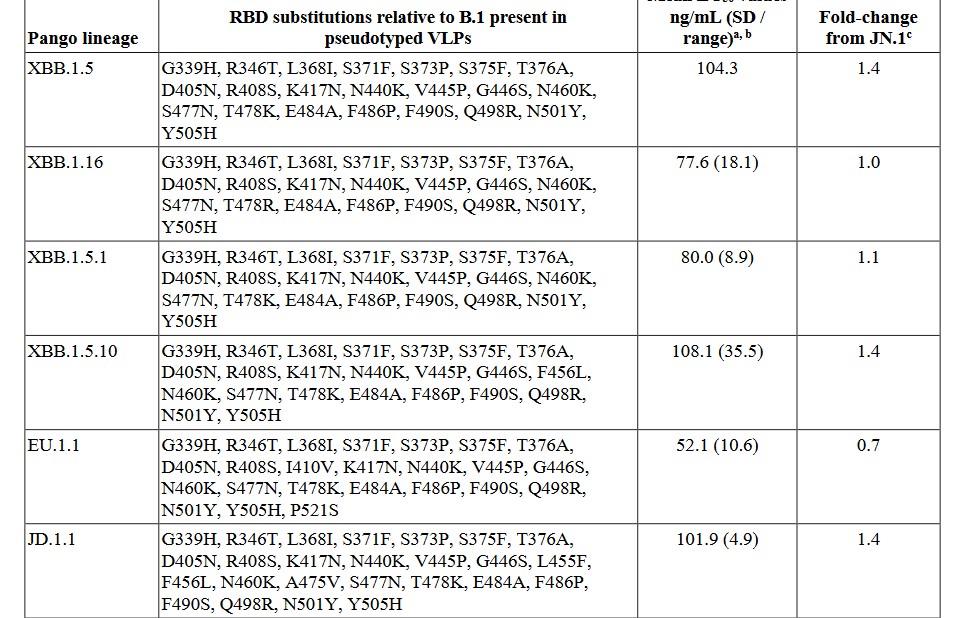
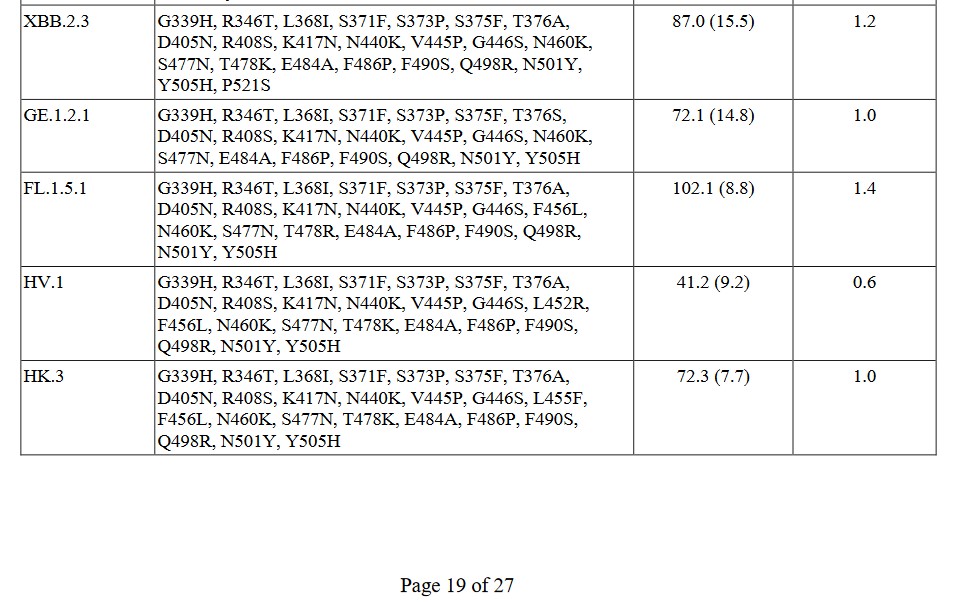
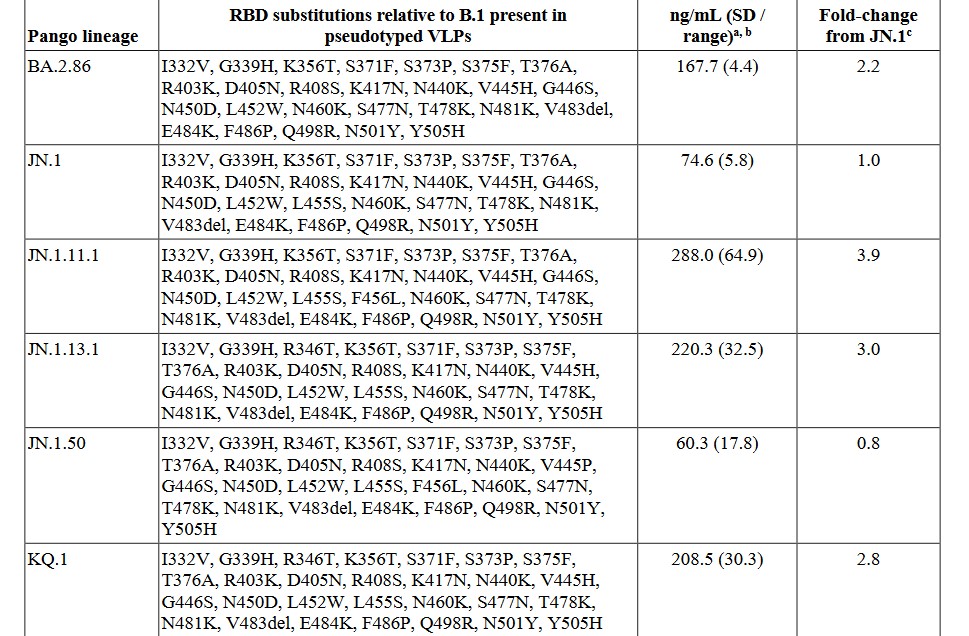
****And now, for the pangolin-CoV connection: This is found in the FDA document on PEMGARDA, Table 2. Yours Truly is including screenshots of Table 2., below. Please look at the screenshots carefully. There are seven screenshots. This is the list of SARS-CoV-2 variants that PEMGARDA is ** allegedly ** supposed to help “guard against.” The bottom line here is: Virtually every SARS-CoV-2 variant is derived from a pangolin-CoV genome code (most likely that of pangolin-CoV MP789) that was “blended in” along with the bat-CoV RaTG13 genome code in the lab-creation of the original SARS-CoV-virus itself. The giveaway is “Pango lineage” at the top of the variants columns. (Note: due to screenshot size constraints, some of the variant lists are broken up: however, EVERY variant column clearly states Pango lineage at the top left.)
The question that comes to mind is: Why is PEMGARDA being promoted as a “pre-exposure prophylaxis” against a COVID-19 infection in immunocompromised persons; or, for that matter, for any person, COVID-19 “vaccinated” or not? The answer is that the FDA still does not recognize, authorize, or recommend, the use of Ivermectin, Hydroxycholorquine, Zinc, Quercetin, Vitamin D, or other “non-FDA-authorized or approved” drugs or treatments for prophylaxis for COVID-19 infection; or for COVID-19 infection treatment. While there may be need for PEMGARDA to be used for certain patients in narrow circumstances, it is Yours Truly’s opinion that it is vastly less expensive and effective to use Ivermectin, Hydroxycholorquine, Zinc, Quercetin, and Vitamin D in the large majority of situations to prevent infection by COVID-19.
Then, there is the issue of what Yours Truly will call “Universal Immune System Compromise from COVID-19 Vaccination.” It is her firm opinion that any person who has ever taken a COVID-19 “vaccine” has a compromised immune system. This is due to the ingredients and the mechanisms of the COVID-19 “vaccines” themselves; in which the critical IgG3 “fight it off” immune system cells of the “vaccinated” person are damaged and/or destroyed, and the growth of IgG4 “tolerate but never clear” cells is increased. This process increases with each successive COVID-19 “vaccine booster” injection (which would include injections of the “latest version” of said “vaccines.”) Please see: https://jessicar.substack.com/p/igg4-cd4s-and-why-the-lnpmrna-platform, “IgG4, CD4s and why the LNP/mRNA platform should be prohibited”, by Jessica Rose, Ph.D., 14 August 2023.
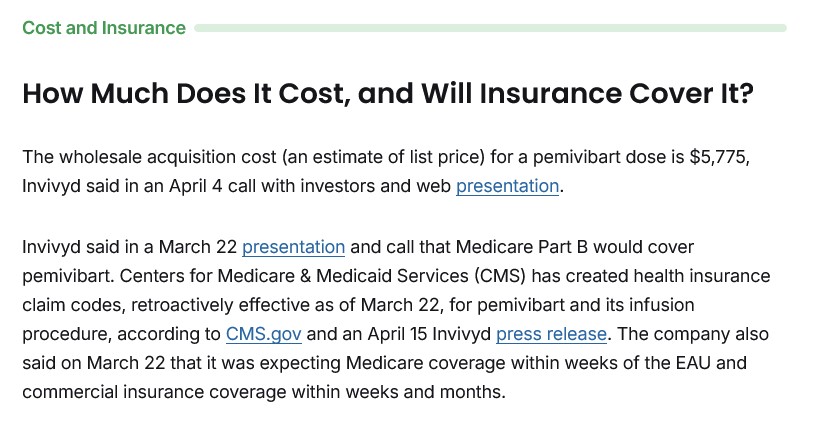
PEMGARDA (aka Pemivibart) is an expensive drug. For example, below is a screenshot from www.patientpower.info/ regarding the cost per treatment for PEMGARDA. This is the non-insurance covered cost:
Recall that the FDA document on PEMGARDA cited above states that persons who are prescribed to take this drug need to repeat the treatment every 3 months.
General Summary: One: Yours Truly presented the first of the hypothesis regarding the use of the pangolin-CoV MP789 in the lab-creation of the original SARS-CoV-2 virus itself (the original Wuhan Hu1 COVID-19 virus itself) in the Health Friday post of 15 November 2024. Two: there is a large amount of scientific papers and articles published in 2020, with researchers investigating various hypotheses regarding a “combination” of animal coronaviruses in nature that produced the original SARS-CoV-2 virus itself. This research was performed prior to the confirmation that the SARS-CoV-2 virus itself was the product of Gain-of-Function lab-creation, most likely at the Wuhan Institute of Virology, using coronaviruses from various animals, including the bat-CoV RaTG13 and the pangolin-CoV MP789. Four: the pangolin-CoV MP789 virus genome has the “closest overall match similarity” to the genome of the SARS-CoV-2 virus itself. Five: there is a new FDA “pre-exposure prophylaxis and antiviral” drug, PEMGARDA, that is administered by infusion (IV) only, and only for certain types of immunocompromised persons. Six: the FDA-issued Fact Sheet for PEMGARDA clearly shows, in Table 2. of the document, that the SARS-CoV-2 variants that PEMGARDA is to “guard against” are virtually all derived from what the document states is “Pango lineage.” Seven: the FDA still does not recognize, authorize, or approve, of the use of Ivermectin, Hydroxycholorquine, and other effective alternatives for COVID-19 infection prevention or treatment.
The above free vintage image of a lock being picked is courtesy of Google Images.
Health Friday is a series related to Big Pharma, vaccines, general health, and associated topics. Since today’s offering is related to the COVID-19 disaster — the SARS-CoV-2 (COVID-19) virus itself; and, to the COVID-19 “vaccines” — it is dedicated to the memory of Yours Truly’s “vaccinated” late brother Sam, and her late cousin Bill; and to all persons of any age who have died as a result of either an infection from the COVID-19 virus itself, or to the negative effects (direct or indirect) of the COVID-19 “vaccines” that they took. However, the discussion is not limited to what is presented today: It is an Open Thread.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
Today’s post includes several “puzzle pieces.” Each one is integral to the whole. Please bear with me. There is a General Summary at the end of the post.
To Begin: A post from our host, Wolf Moon: www.theqtree.com/2023/05/01/pfizer-and-moderna-vaccines-both-contain-the-prrarsv-key-to-the-cell-nucleus/. This post is one of several on the topic of the “PRRARSV Backdoor Key” that is present in both the Pfizer-BioNTech and in the Moderna modRNA COVID-19 “vaccines.” One of the papers cited in the post is “the Mehedi paper”, found here: https://doi.org/10.3389/fmicb.2023.1073789. “Nuclear translocation of spike mRNA is a novel feature of SARS-CoV-2”, Masfique Mehedi, et al., 26 January 2023. This paper proves that the PRRARSV code in the SARS-CoV-2 virus genome is only there, and not in either the SARS-CoV virus genome or the MERS-CoV virus genome. There are links to other important papers in the Wolf Moon post. Yours Truly is grateful to our host for doing serious investigation into this subject.
There has been speculation that the PRRARSV code may be related to snake venom. This also has been discussed by our good host in other of his posts on the subject. While Yours Truly believes that some type of snake venom that contains all or some of the PRRARSV code may be in play, she has an additional hypothesis on the PRRARSV code presence in the modRNA COVID-19 “vaccines” — and in the SARS-CoV-2 virus itself.
And, Now: May I present — the Pangolin (PAN-go-lin.)
Pangolins are shy, nocturnal mammals that are covered with scales; they are also called “scaly anteaters.” They resemble anteaters in body shape and length; however, Pangolins are covered with hard, keratin-like scales from the head to the tip of the tail. During the day, they remain in their burrows; at night, they emerge to hunt for and eat ants and termites. Their living habitat ranges from areas in Africa to India to southern Asia. As their meat, scales, and other body parts, are consumed as exotic foods, or are used in folk and traditional medicine in certain areas of the world, the Pangolin is listed as an endangered species. It is illegal to hunt or trap Pangolins, or to keep them as pets. However, because of their meat, scales, and other body parts, Pangolins are among the most-trafficked animals in the world (https://en.wikipedia.org/wiki/Pangolin.)
The above image of a Pangolin is courtesy of the International Fund for Animal Welfare and Goggle Images.
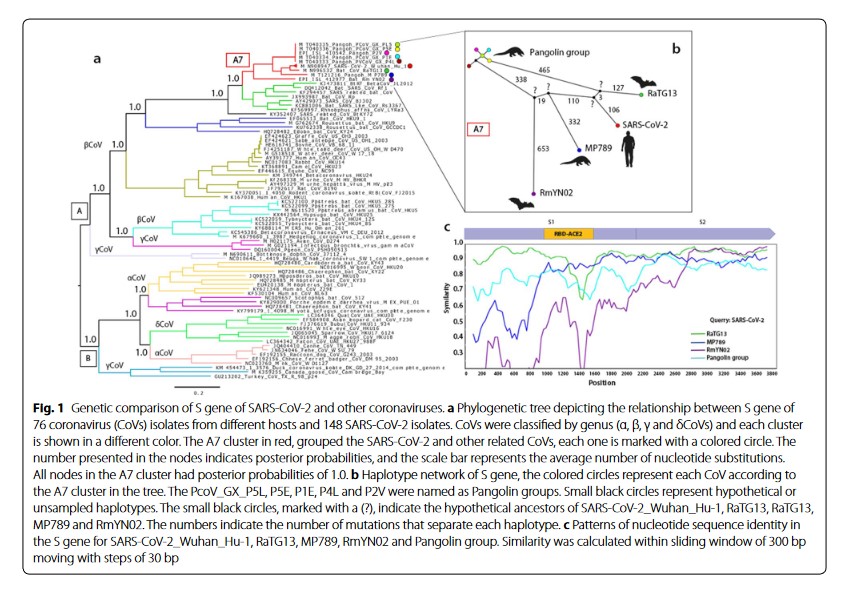
Pangolins, like other animals, have coronaviruses. And here is where the story gets interesting. One such Pangolin coronavirus is “pangolin-CoV MP789.” It appears that the RBD (Receptor Binding Domain) is this virus has an “uncanny” similarity to the RBD of the SARS-CoV-2 virus. In fact, it is been posited that the RBD of the SARS-CoV-2 virus resulted from a “recombination” of those of the bat-CoV RaTG13 virus and the pangolin-CoV MP789 virus. Below is Figure 1 of the “Morales-Espinosa, et al. paper” on this subject:
The “Morales-Espinosa, et al. paper” is found here: https://pmc.ncbi.nlm.nih.gov/articles/PMC7450963/, “The receptor binding domain of SARS-CoV-2 spike protein is the result of an ancestral recombination between the bat-CoV RatG13 and the pangolin-CoV MP789”, Rosario Morales-Espinosa, et al., 27 August 2020.
There is a plethora of scientific papers, articles, and scientific/medical blog posts related to the “probable” or “hypothetical” or “uncanny” similarity between Pangolin-CoV and SARS-CoV-2. Yours Truly will provide a sampling, below. Most of these papers, articles, and blog posts were written between 2020 and late 2022.
One: A scientific article by researchers in the CCP: www.cell.com/current-biology/pdf/S0960-9822(20)30360-2.pdf, “Probable Pangolin Origin of SARS-CoV-2 Associated with COVID-19 outbreak”, Tao Zhang, et al., 6 April 2020. A screenshot of part of the Conclusion of this article is below:
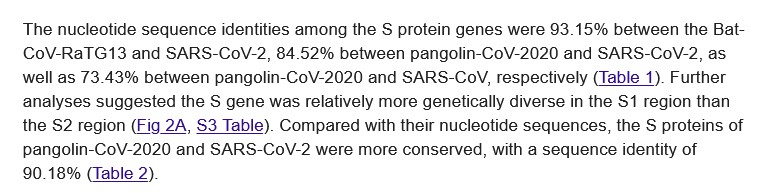
Two: Another 2020 paper, this one with an important mention in the Results section regarding the very high similarity of the S proteins in the pangolin-CoV genome and the SARS-CoV-2 genome: https://doi.org/10.1371/journal.ppat.1008421, “Are pangolins the intermediate host of the 2019 novel coronavirus (SARS-CoV-2)?”, by Ping Liu, et al., 14 May 2020. A screenshot of the section of the Results is below:
Three: Another scientific paper from 2020: https://doi.org/10.1101/2020.0707.184374. “Single source of pangolin CoVs with a near identical spike RBD to SARS-CoV-2”, Chan, Y.A., and Zhan, S.H., 31 October 2020. A screenshot from this paper is below:
Recall that it is only recently that the “the SARS-CoV-2 virus came from nature”, “the SARS-CoV-2 virus came from the ‘wet markets’ in Wuhan” claims have been proven incorrect. While there are still scientific papers and articles being published to “prove” the “came from nature” claims, what these papers and articles do not seem to explore, in Yours Truly’s opinion, are the Gain-of-Function experiments with various coronaviruses (including the pangolin-CoVs) that took place at the Wuhan Institute of Virology in the process of lab-creating the SARS-CoV-2 virus itself. These Gain-of-Function experiments used elements found in nature (bat coronaviruses, civet coronaviruses, pangolin coronaviruses, rabbit coronaviruses, monkey coronaviruses, etc.) to “build” the SARS-CoV-2 virus itself. Here, for example, is a 2022 scientific article regarding the claims that the virus came from nature: www.science.org/content/article/evidence-suggests-pandemic-came-nature-not-lab-panel-says, “Evidence suggests pandemic came from nature, not a lab, panel says”, 10 October 2022, by Jon Cohen.
Which leads into the discussion of the Wuhan Institute of Virology’s experiments with pangolin coronaviruses.
It is obvious that the Wuhan Institute of Virology conducted coronavirus experiments with bats, civets, monkeys, and pangolins, in the process of creating the SARS-CoV-2 virus.
Which leads to the next discussion, regarding PRRARSV and the furin cleavage site in the SARS-CoV-2 virus genome. Bear with Yours Truly here: this is an important piece of the puzzle.
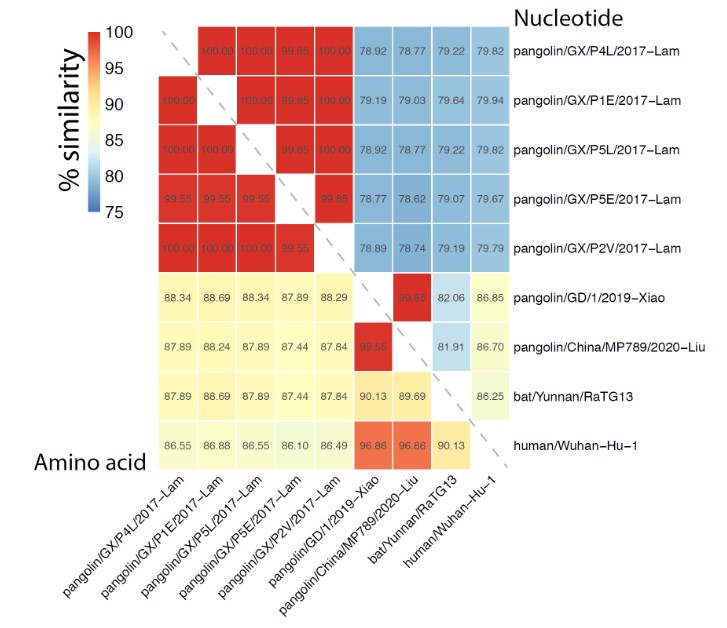
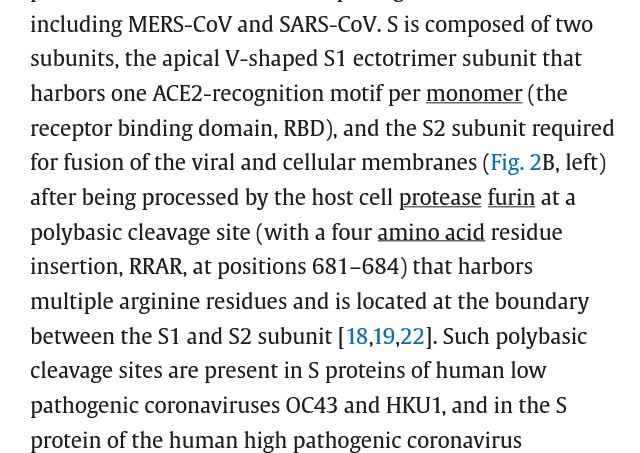
PRRARSV is located at the S1-S2 furin cleavage site on the SARS-CoV-2 virus genome, from a scientific paper in September 2020: https://doi.org/10.1016/j.lfs.2020.118056, “Structural features of coronavirus SARS-CoV-2 spike protein: Targets for vaccination”. by Ariane Sternberg and Cord Naujokat, 15 September 2020. A screenshot from section 2 of this paper is below:
The redoubtable Walter M Chesnut expands on this, and how PRRARSV assists in the translocation of the modRNA spike protein in the SARS-CoV-2 virus into every cell in the human body: https://wmcresearch.substack.com/p/prrarsv-the-furin-cleavage-site-a. “PRRARSV—The Furin Cleavage Site: A Nuclear Localization Signal that Translocates the Spike and its mRNA to the Nucleus Inducing H3.3 histone Deposition and Rapid Aging”, 10 April 2023. Below is the National Cancer Institute definition of a histone (www.cancer.gov/publications/dictionaries/cancer-terms/def/histone):
In other words, the PRRARSV present in the SARS-CoV-2 virus enters the cell, assists the spike protein of the SARS-CoV-2 virus to enter the nucleus of the cell, and interferes with the H3.3 histone in the DNA of the cell.
There are four “inserts” that were introduced into the SARs-CoV-2 virus genomeduring the process that lab-created the SARS-CoV-2 virus. These four “inserts” were first isolated and described in the “Pradhan paper” from 2020. This paper was Retracted and suppressed almost as soon as it appeared. However, it can be found here: https://medicalveritas/org/wp-content/uploads/2020/02/Pradhan-et-al-Coronavirus-HIV-paper.pdf. A screenshot of Table 1. from the paper is below. The “PRRAR” code is “Insert 4”:
In addition, Figure 2. of this paper has the SARS-CoV-2 virus genome spelled out, with the position of each of the four “inserts.”
This leads to further proof that the PRRARSV code is indeed part of the SARS-CoV-2 virus itself. For example: https://jessicar.substack.com/p/it-turns-out-that-the-prrarsv-motif, “It turns out that the “PRRRARSV” motif is more than a furin-cleavage site”, 1 October 2022. Dr. Rose performed her own analysis of the PRRARSV code in the SARS-CoV-2 virus genome. She proves that the PRRARSV code is indeed the fourth “insert” into the virus genome. A screenshot of her analysis is below:
What does this all mean? It means the following:
General Summary:
One: The Pangolin, a shy, nocturnal mammal that is covered in keratin-like scales and eats ants and termites, also is prone to having a coronavirus, called pangolin-CoV. This virus has a genome code that is “quite similar” in some ways to the SARS-CoV-2 virus itself genome code. One of these “similarities” is a genome code called “RRSV” or “PRRAR”, depending on the research paper on the topic.
Two: There are four “unique inserts” in the SARS-CoV-2 virus itself genome. The fourth “insert” is the PRRARSV code. The PRRARSV code interferes with the important H3.3 histone in the DNA of every cell in the body of the person who is infected by SARS-CoV-2 (the COVID-19 virus) or who is infected with the SARS-CoV-2 virus itself.
Three: The PRRARSV code was possibly derived from experiments with a type of snake venom; unless otherwise proven, it certainly was derived from experiments with the pangolin-CoV genome code.
Four: The experiments with the PRRARSV code were conducted at the Wuhan Institute of Virology in the process of the lab-creation of the SARS-CoV-2 virus itself.
Five: Since the COVID-19 “vaccines” use the Wuhan Hu1 SARS-CoV-2 virus itself as the basis for these injectables, the PRRARSV code is therefore present in these “vaccines.” This means that all persons who have ever taken a COVID-19 “vaccine” have been exposed to the PRRARSV code. To date, nobody knows exactly how long the ingredients and mechanisms of the COVID-19 “vaccines” remain at work in the “vaccinated” person’s body. In fact, the COVID-19 “vaccines” are designed to trick the “vaccinated” person’s body into thinking it has a COVID-19 virus infection, forcing the “vaccinated” person’s body to make large amounts of antibodies to fight off the “fake COVID-19 infection”: www.brandeis.edu/magazine/2020/fall/inquiry/vaccine.html, “On the cusp of a COVID-19 Vaccine”, by Lawrence Goodman. A screenshot from the article is below, quoting Dr. Drew Weissman of the University of Pennsylvania Perelman School of Medicine:
Six: Un-vaccinated” persons who contract a COVID-19 virus itself infection, and are therefore exposed to the PRRARSV code, can still mitigate and/or defeat the effects of the damage done by the virus itself if the person has a healthy immune system. On the other hand, COVID-19 “vaccinated” persons, in addition to being exposed to the PRRARSV code present in the “vaccines”, are also exposed to the other ingredients in the “vaccines”, such as N1-Methylpseudourdine. N1-Methylpseudouridine replaces the natural Uridine in the “vaccinated” person’s body, and also evades the natural immune system components and mechanisms in the COVID-19 “vaccinated” person’s body. COVID-19 “vaccinated” persons therefore have their natural immune systems damaged or destroyed, making it difficult or even impossible to mitigate and/or defeat the damage done by the “vaccines.”
Yours Truly will posit, based on the research and writing that she has been engaged in about the COVID-19 virus itself, and the COVID-19 “vaccines”, since March 2020: that any un-“vaccinated” person, of any age, who has had a COVID-19 virus itself infection; or, any person, of any age, who has had a COVID-19 “vaccine” put into their body — has been injured by the negative effects of the virus itself, or by the negative effects of the “vaccines.” In addition, COVID-19 virus itself infected persons, and COVID-19 “vaccinated” persons, have died from the effects of the infection or the “vaccine.” One will also say that the COVID-19 “vaccines” have added ingredients and mechanisms that make these injectables more dangerous and deadly than the COVID-19 virus itself. Finally, the outcomes of infection by the COVID-19 virusitself, andthe negative outcomes from taking the COVID-19 “vaccines”, were, and are, planned and intentional.
It is now, in Yours Truly’s opinion, imperative that all persons make it their business to have and to maintain their natural immune system in the best possible condition.
It is now time to bring to account all of the multiple agencies, scientists, and other entities involvement (including the United States military) in the development of the lab-created SARS-CoV-2 virus itself: of the COVID-19 “vaccines”; and in the processes that resulted in the granting of Emergency Use Authorization and/or Full Approval of these “vaccines” without proper protocol adherence to rigorous testing and clinical trials for the said “vaccines.” It is now time to stop all further use of any COVID-19 “vaccine” until the above accountability is fully undertaken and finished, It is now time for all government agencies, medical organizations, and medical practitioners to recognize that Ivermectin and Hydroxycholoquine are inexpensive and vastly effective treatments for COVID-19 infection and for COVID-19 infection prophylaxis. It is now time to stop the use of Paxlovid and Remdesivir as “officially approved” treatment for COVID-19 infection, as both of these drugs have significant negative side effects, including a high “rebound COVID infection” rate for Paxlovid, and kidney damage and/or death for Remdesivir; and to substitute the use of Ivermectin or Hydroxycholoquine.
The above free image of Justice is courtesy of Pixabay and Google Images.
Health Friday is a series of posts devoted to Big Pharma, vaccines, general health, and associated topics. However, the discussion is not limited to what is presented in today’s offering: It is an Open Thread.
As today’s Health Friday post is related to the COVID-19 disaster (the virus itself, and the COVID-19 “vaccines”; and, to the governmental and Big Pharma tyranny over the lives and livelihoods of millions of people “in the name of Science” related to the COVID-19 disaster), it is dedicated to the memory of Yours Truly’s COVID-19 “vaccinated” late brother Sam, and her late cousin Bill; and to the memory of all other persons of any age who have passed away since 11 December 2020, either directly or indirectly, due to the COVID-19 “vaccines” they have taken. May they rest in eternal Peace.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats by Yours Truly, of which readers should be aware, and which are all linked here.
Donald Trump was just overwhelmingly re-elected to be the next President of the United States. It appears that he will appoint Robert F. Kennedy, Jr., to be Secretary of the Department of Health and Human Services. Mr. Kennedy, Jr., has vowed to end the “stranglehold” that the FDA, the CDC, Big Pharma, and “Establishment Medicine” have imposed on the American people for decades. It also appears that he plans to re-organize the FDA into an agency that actually does its job in protecting the health of the American people. One of his efforts, in Yours Truly’s opinion, needs to be investigating the exact “reorganization” changes that the FDA began to implement within that agency on 1 October 2024: www.fda.gov/about-fda/fda-organization/fda-modernization-efforts-establishing-unified-human-foods-program-new-model-field-operations-and.
In addition, there is much to be accomplished regarding holding multiple persons, agencies, and other entities accountable for the damage that has already been done to the general public health of Americans, in addition to the health of people all over the world, due to the COVID-19 disaster. While Yours Truly is notadvocating a “re-do” of the French Revolution, there must be ways to hold these multiple persons, agencies, and other entities to account. Please see www.midwesterndoctor.com/p/new-data-exposes-the-corruption-behind, “New Data Exposes the Corruption Behind the COVID Response”, 12 November 2024. A screenshot of the start of this blog post is below:
The following Listsbarely scratch the surface:
List One: Dr. Anthony Fauci (former head of the NIAID); Dr. Francis Collins (former head of NIH); Dr. Deborah Birx (White House Coronavirus response team under then-President Trump); Dr, Stephen Hahn (former Commissioner of the FDA); Dr. Robert Califf (current Commissioner of the FDA); Dr. Robert Redfield and Dr. Rochelle Walensky (former Directors of the CDC); Dr. Mandy Cohen (current Director of the CDC); Ralph Baric, Ph.D. (UNC, Chapel Hill); Peter Daszak, Ph.D. (EcoHealth Alliance); and, Dr. Eric Rubin (VRBPAC committee, FDA “We’re never gonna know if it’s effective unless we start giving it” — related to the committee’s recommendation to give the COVID-19 “vaccines” to children.) If Dr. Zheng-li Shi (Wuhan Institute of Virology) can be extradited from Communist China, that would be a good addition to the list.
The above article contains a link to the archived CDC document.
Regarding Dr. Anthony Fauci: Please watch the short video clip of leaked testimony from a Congressional hearing in which Dr. Fauci spoke. Listen to his comments. Listen to them again. At 0:23 in the clip, Dr. Fauci states: “And it’s been proven that when you make it difficult for people in their lives, they lose their ideological bullshit and they get vaccinated.” (Bolding mine). The video clip is here: https://x.com/LisaLu/status/1855788234392932353.
List Two: Albert Bourla, DVM (CEO of PfizerUSA); Stephane Bancel (CEO of Moderna); Alex Gorsky (former CEO of Johnson & Johnson.)
List Three: Alex Azar (former), and Xavier Becerra (current), Secretaries of the Department of Health and Human Services; Kathy Hochul, Governor of New York; Tom Wolf, former Governor of Pennsylvania; Gretchen Whitmer, Governor of Michigan.
List Four: United States Department of Defense Secretaries Patrick M. Shanahan, Mark Esper, Christoper C. Miller (former, 2018-2021); and, Lloyd Austin (current). United States Army Chiefs of Staff Gen. Mark A. Milley, Gen. James C. McConville (2015 through August 2023); and, Gen. Randy A. George (current.) These, all in relation to the United States Defense Department’s and the United States Army’s previous and (likely) current involvement in the development, manufacture, and distribution of the Pfizer-BioNTech modRNA COVID-19 “vaccines”; and, to the forced “mandate” that all US military personnel be COVID-19 “vaccinated.” www.documentcloud.com/downloads/22028603-pfizer-base-agreement, July 2018; www.hhs.gov/sites/default/files/pfizer-inc-covid-19-vaccine-contract.pdf, 21 July 2021; www.law.cornell.edu/uscode/text/10/4022.
List Five: Bill Gates; Kelly L. Moore, MD, MPH (director of https://immunize.org/); Mark Green (former), and Samantha Power (current), Administrators of the United States Agency for International Development (www.usaid.gov/; also via https://usaidmomentum.org/.)
Readers are invited to add names to these lists, and/or to create other lists.
The above free vintage image of DNA/RNA and lab equipment is courtesy of Google Images.
Health Friday is a series that discusses Big Pharma, vaccines, general health, and associated topics. Today’s post goes down several “rabbit holes”; Yours Truly believes they are all relevant to the core observation of the piece. There are multiple screenshots, and also a General Summary at the end. The discussion today is not limited to what is presented here: It is an Open Thread. As the post involves items related to the COVID-19 modRNA “vaccines”, it is dedicated to the memory of Yours Truly’s “fully vaccinated and boosted” brother Sam, who passed away last week due to complications from, among other things, “sudden-onset dementia”; and, to the memory of her cousin Bill, who “died suddenly and unexpectedly” in September 2023. May they rest in eternal Peace.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and caveat items from Yours Truly, of which readers should be aware. These are all linked here.
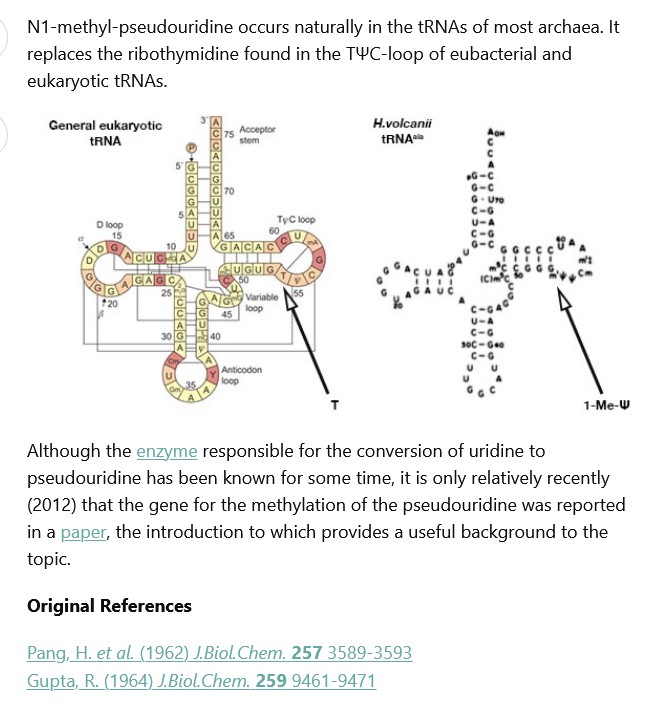
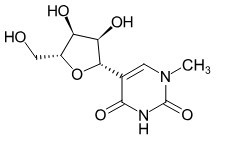
Today’s post is about one of the ingredients of the modRNA COVID-19 “vaccines”: a lab-synthesized version N1-Methylpseudouridine.
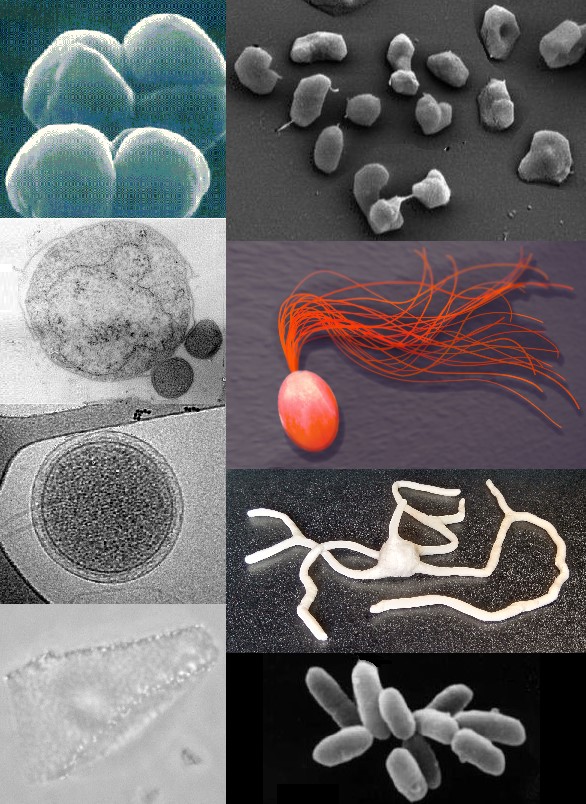
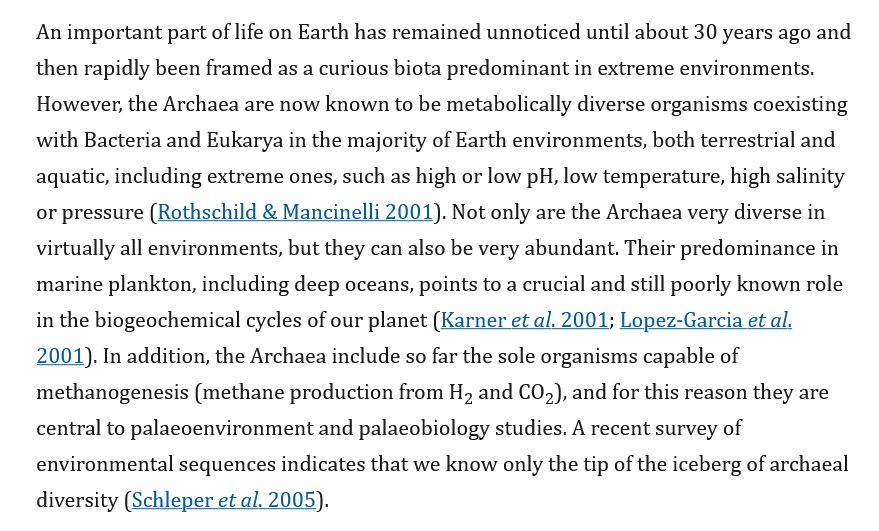
To begin: Once upon a time, a very long time ago (say, about 2.7 billion years ago), an organism domain evolved into being on the Earth. The name of this organism is Archaea. It is a “middle-position” domain between the domains of Eukaryotes and of Bacteria. Archaea gradually evolved into multiple types of Phyla (a position between Kingdom and Class in taxonomic rank.) Archaea are a large part of what is called microbiota (a “range” of microorganisms that include Archaea, bacteria, fungi, and viruses.) Archaea are literally “all over the place”, including in the human gut microbiome, the plankton in the waters of the Earth, and in the Earth’s soil. Archaea can “communicate” with each other through a kind of “cross-talk.” The various types of this microorganism can exist in all kinds of places and in conditions of extreme heat or extreme cold. Archaea are a kind of “recycling center” for carbon, nitrogen, and sulfur, depending on where it lives. Methanogen Archaea “…play an important role in the decay of organic matter…”, such as would be seen in a swamp. (Remember this for later in the post.) https://en.wikipedia.org/wiki/Archaea. Below is an image of some types of Archaea:
More information about Archaea and what it does is here: https://pmc.ncbi.nlm.nih.gov/articles/PMC1578729/, “The origin and evolution of Archaea: a state of the art”, by Simonetta Gribaldo and Celine Bochier-Armanet, 9 May 2006. A portion of the Introduction of this paper is below:
Again, remember the reference to methanogensis related to Archaea for further down in today’s post.
Then, there is Uridine.
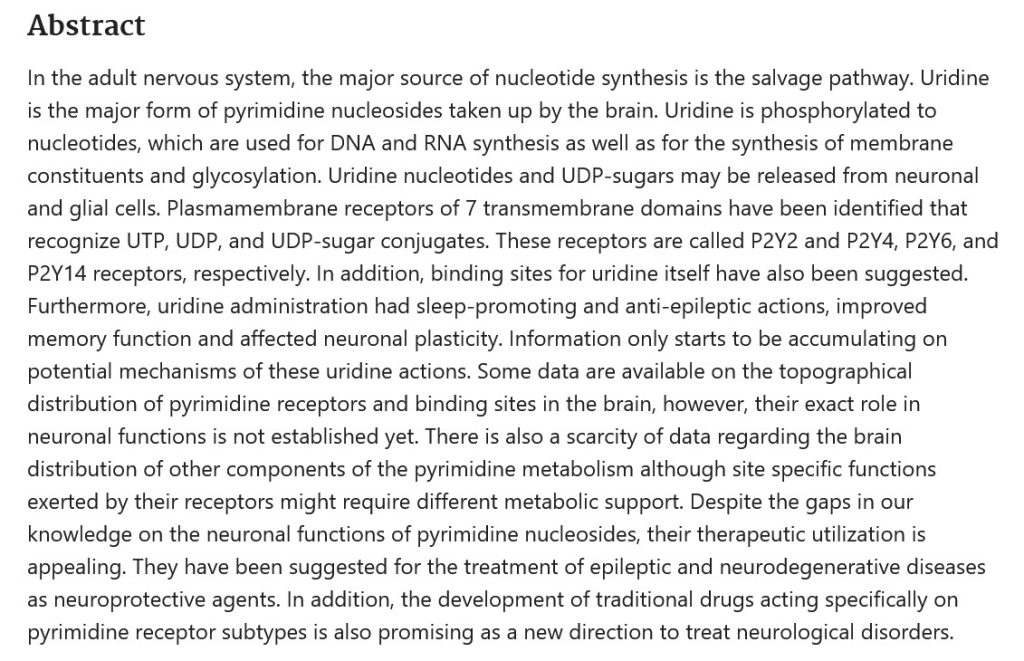
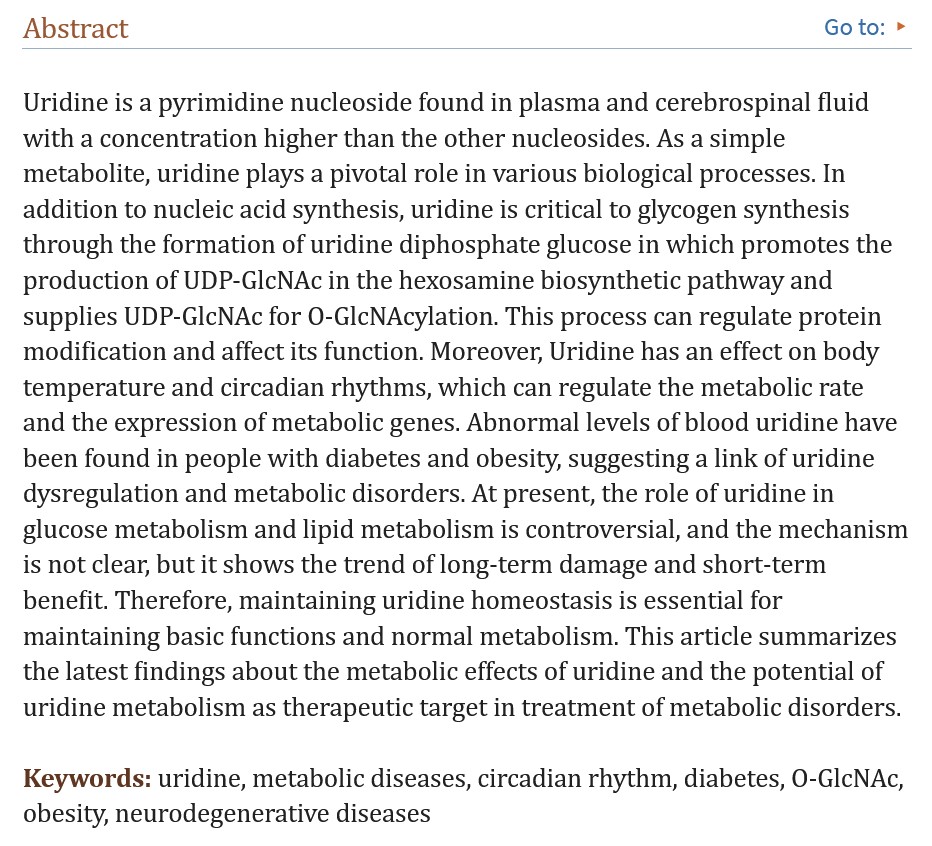
Uridine is an RNA component that is manufactured by the Liver in the human body. It is either synthesized from foods that contain Uridine in the RNA of the food; or, if the body is not taking in sufficient food sources, Uridine production shifts to the adipose tissues (fat tissues) of the body. The importance of Uridine presence in the human body cannot be over-emphasized. Uridine crosses the Blood-Brain Barrier and helps to regulate mood, dopamine release, and other functions of the brain; It can help to mitigate Alzheimer’s Disease; it helps to regulate body temperature and circadian rhythm; it helps in tumor decrease; it has profound positive effects on the Central Nervous System; and more: https://pmc.ncbi.nlm.nih.gov/articles/PMC10937367/, “Uridine and its role in metabolic diseases, tumors, and neurodegenerative diseases”, Yueyuan Yang, et al., 28 February 2024. Food sources of Uridine include beer; Brewer’s Yeast; beets; tomatoes; goat’s milk and cheese; organ meats (liver, etc.); fish; molasses; and, walnuts: https://en.wikipedia.org/wiki/Uridine; and, https://pubmed.ncbi.nlm.nih.gov/21401985/, “Uridine function in the central nervous system”, Juliana Kardos, et al., 2011. Below is the Abstract from the Kardos, et al., paper:
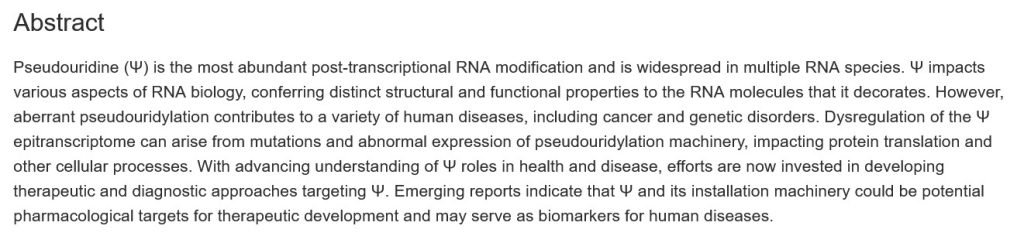
Natural Pseudouridine (as opposed to the lab-created versions) appears in the RNA of the human body. It is a “by-product” of RNA mechanisms in the body. It is also found in yeast and in E. coli (https://en.wikipedia.org/wiki/Pseudouridine.) If one or more of the mechanisms involved in the creation of Pseudouridine become “aberrant”, this can contribute to the onset of cancer or to certain types of genetic disorders (www.cell.com/trends/pharmacological-sciences/fulltext/S0165-6147(22)00058-X. “Decoding pseudouridine: an emerging target for therapeutic development”, Jonas Cerneckis, et al., June 2022. The Abstract of the Cerneckis, et al., paper, is below:
The exact mechanisms and consequences of Pseudouridine are a fairly recent “hot topic” for research, including in the fields of gene therapy and vaccine development. In fact, several COVID-19 “vaccines” have been developed that use Pseudouridine as an ingredient; however, it appeared that this element was lacking in “efficiency” regarding its ability to replace Uridine in the body; and, in fact, Pseudouridine, in this context, created “unintended proteins.” (www.science.org/content/article/mrna-vaccines-may-make-unintended-proteins-there-s-no-evidence-harm. “mRNA vaccines may make unintended proteins, but there’s no evidence of harm”, by Gretchen Vogel. The use of Pseudouridine in the COVID-19 “vaccines” was superseded by the use of the element that is the main topic of today’s post: N1-Methylpseudouridine.
Recall that Archaea has various manifestations, including ones that are called Methanogens. Naturally-occurring N1-Methylpseudouridine is found in the soil: one type, Streptomyces lincolnensis (Nebraska origin), forms the basis for the antibiotic lincomycin: www.drugs.com/mtm/lincomycin.html. (Note: this antibiotic is used for severe cases of bacterial infections in persons who are allergic to penicillin.) Lincomycin has a “sister” drug, clindamycin. (https://journals.asm.org/doi/10.1128/aem.02091-18, “TetR-Type Regulator of Lincomycin Biosynthesis in Streptomyces lincolnensis“, Yurong Xu, et al., 13 December 2018.)
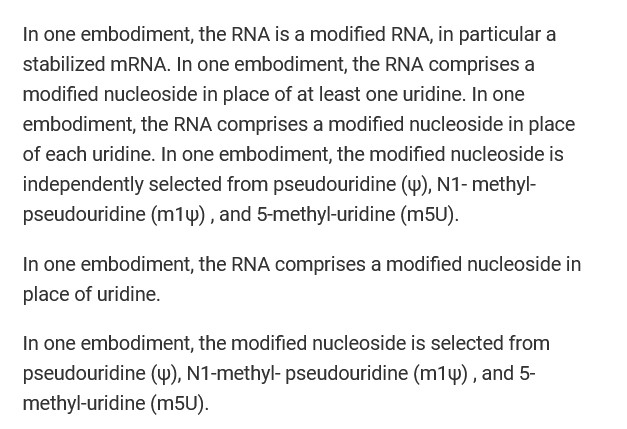
When ruminating animals (cows, for example) take in N1-Methylpseudouridine from the grass that grows in soil that has Archaea producing this element, it passes through the animal’s body and is released; as solid waste, or as gas (that “cow methane” that the environmentalists are so upset about.) The human body, in its evolved wisdom, “recognizes” that naturally-occurring N1- Methylpseudouridine is not Uridine, and usually will eliminate it. However, this is not the case regarding the type of N1-Methylpseudouridine in the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna: In these injectables, the element not only is a “lab-synthesized and enhanced” form; in this form, it is deliberately included in the “vaccines” to replace the natural Uridine in the body of the “vaccinated” person. This Uridine replacement is done for two reasons: One, to “increase” the utilization of the modRNA COVID-19 “vaccines” in the “vaccinated” persons’ body; and, Two, to evade and/or destroy the “vaccinated” person’s body’s natural capability to “recognize” the foreign element and to eliminate it. Yours Truly will repeat this: The natural Uridine RNA of the “vaccinated” person’s body is replaced with the “lab-synthesized and enhanced” version of N-1 Methylpseudouridine in the modRNA COVID-19 “vaccines.”
Please refer back in today’s post regarding the multiple beneficial activities of naturalUridine in the human body. These multiple beneficial activities are either depleted or completely replaced by the “lab-synthesized and enhanced” version of N-1 Methylpseudouridine in the modRNA COVID-19 “vaccines” — in order for the ingredients and mechanisms of these injectables to work in the “vaccinated” person’s body.
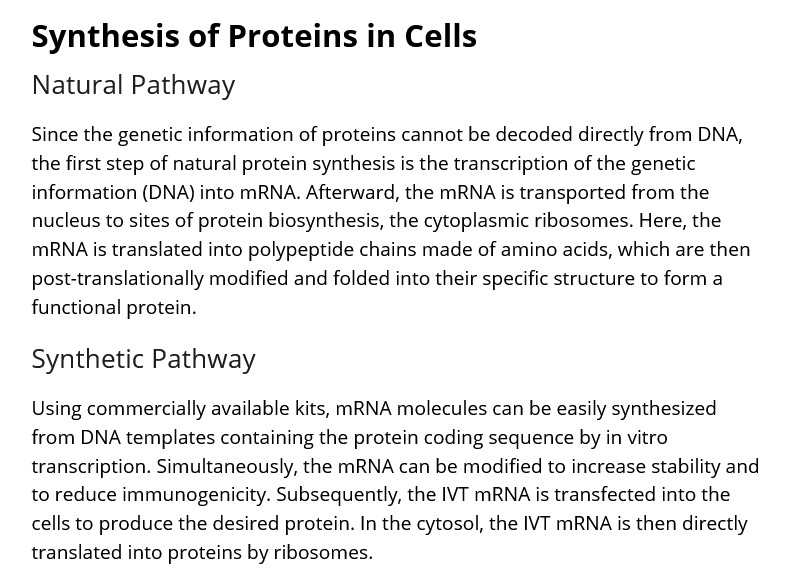
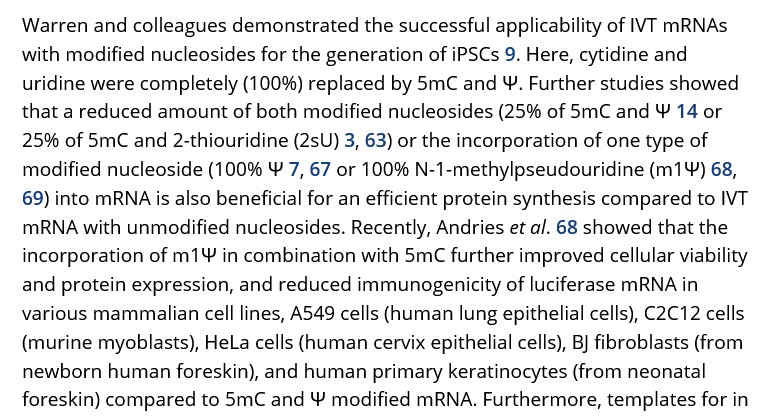
Experiments using various “lab-synthesized and enhanced” forms of N1-Methylpseudouridine have been in process for some time. An important paper that describes this type of experimentation is here: https://doi.org/10.1002/stem.2402, “Concise Review: Application of In Vitro Transcribed Messenger RNA for Cellular Engineering and Reprogramming: Progress and Challenges”, Andreas Behring et al., 2 June 2016. Below are three screenshots from this paper, beginning with a portion of the section Protein Synthesis in Cells:
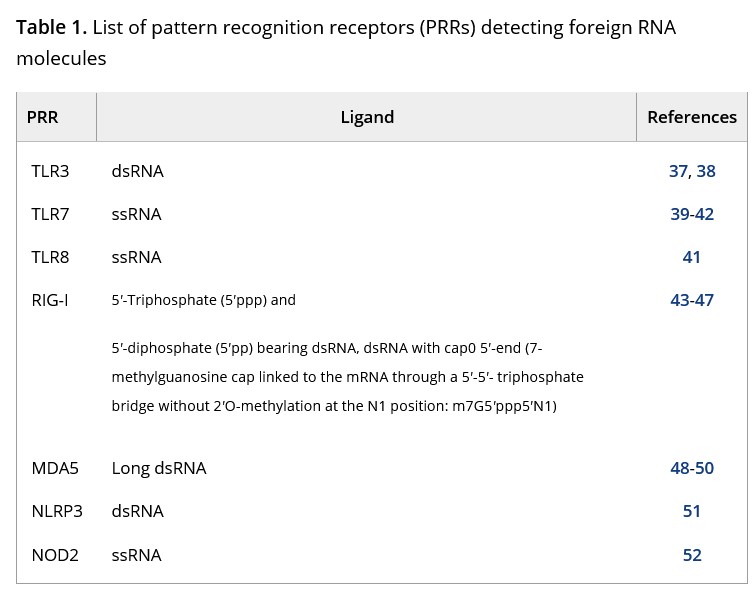
Followed by Table 1 of the above paper, listing the natural immune system responses when “foreign RNA” is detected in the human body (the numbered links lead to various papers):
And, followed by a portion of the section Modifications of the Synthetic mRNAs from the Behring, et al., paper:
Note the mention of “100% replacement” of Uridine.
The type of N1-Methylpseudouridine used in the Pfizer-BioNTech and in the Moderna modRNA COVID-19 “vaccines” is a “lab-synthesized and enhanced and turbo-charged” version. It is called N1-Methylpseudouridine-5′-Triphosphate. Below is the entry from one commercial lab where this version can be purchased (the N-1081 is the catalog number at TriLink Biotech for the compound):
Below is a screenshot of the chemical construction of this version of N1-Methylpseudouridine used in the modRNA COVID-19 “vaccines”, sold by New England Biolabs:
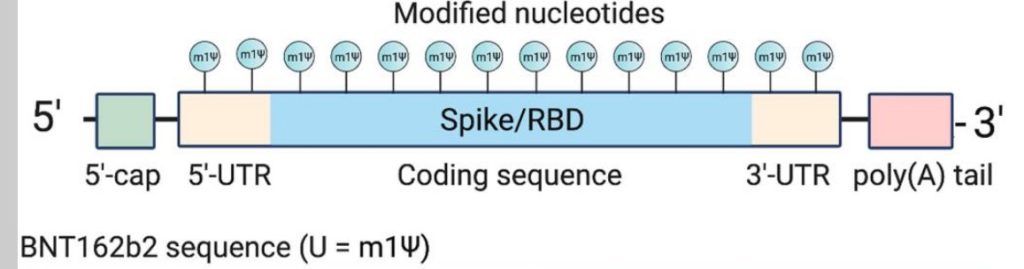
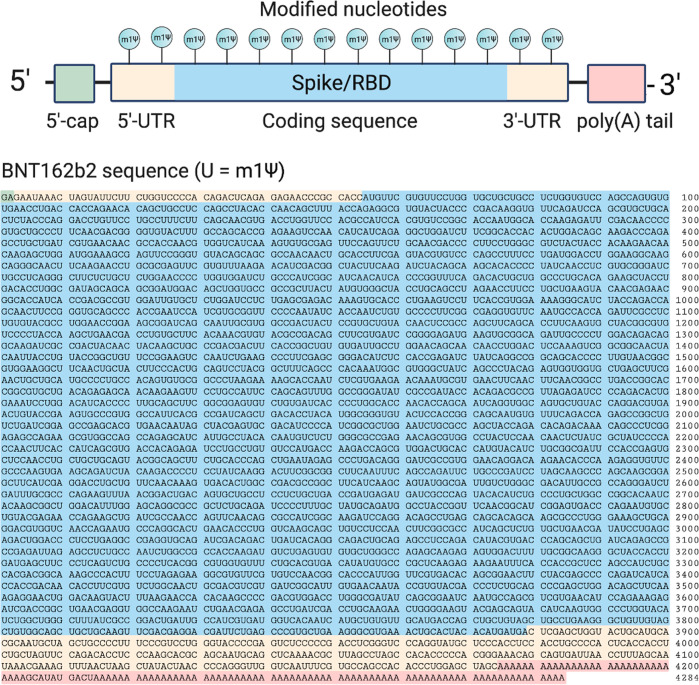
Where was this “lab-synthesized and enhanced and turbo-charged” version of N1-Methylpseudouridine inserted in the modRNA of the SARS-CoV-2 spike protein for use in the modRNA COVID-19 “vaccines”? On both ends of the RBD (Receptor Binding Domain) area of the SARS-CoV-2 virus spike protein (https://pmc.ncbi.nlm.nih.gov/articles/PMC80433204, “Modifications in an Emergency: The Role of N1-Methylpseudouridine in COVID-19 Vaccines”, Kellie D. Nance, Jordan L. Meier, 6 April 2021. This important paper describes the process of how this ingredient truncates the body’s natural immune mechanisms and processes that would normally “recognize” this element as a “foreign RNA” and eliminate it. Below is a screenshot from the paper of the location on the RBD section of the SARS-CoV-2 spike protein where this “foreign RNA” was inserted (the light pink areas mark the beginning and end of the insertion):
And, from the above paper, a screenshot of the entire SARS-CoV-2 virus spike protein code as used by Pfizer-BioNTech for the company’s “flagship” modRNA COVID-19 “vaccine”, BNT162b2. The areas that were used to “insert” the coding sequence changes for the synthesized, enhanced, and “turbo-charged” version of N1-Methylpseudouridine are marked in pink:
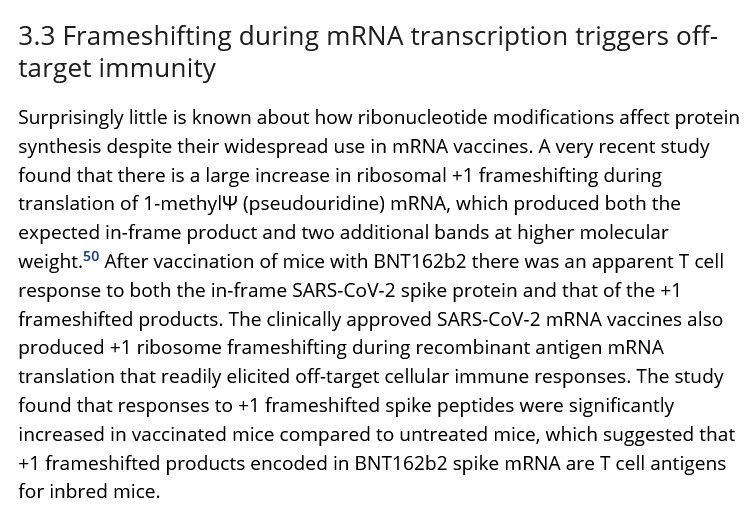
The use of forms of N1-Methylpseudouridine is being touted as “the best approach” for inclusion in mRNA products. This is because N1-Methylpseudouridine “does a better job” of replacing the natural Uridine in the “vaccinated” person’s body:https://doi.org/10.1038/s41598-022-17249-1, “N1-methyl-pseudouridine is incorporated with higher fidelity than pseudouridine in synthetic RNAs”, Jennifer Ong, et al., July 2022. However, there are problems with this situation; among them, the evidence that “frameshifting” is induced: https://doi.org/10.13140/RG.2.2.36710.40005, “Ribosomal frameshifting and misreading of mRNAs in COVID-19 vaccines produce “off-target” proteins and immune responses eliciting safety concerns: Comment on UK study by Mulroney et al.”, David M Wiseman, Jessica Rose, et al., December 2023. The National Cancer Institute defines “ribosomal frameshifting” as follows, below (www.cancer.gov/publication/dictionaries/genetics-dictionary/def/frameshift-mutation):
In other words, a kind of “unintended consequence” from using things like “lab-synthesized and enhanced and turbo-charged” forms of N1-Methylpseudouridine in modRNA COVID-19 “vaccines.” Dr. Peter McCullough’s important take on this issue is here: https://doi.org/10.1002/prp2.1218, “Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination”, Peter A. McCullough, et al., 12 June 2024. Below is a screenshot of a portion of this paper:
In other words, the frameshifting induced in the COVID-19 “vaccinated” person’s body via the use of synthesized, enhanced, and “turbo-charged” N1-Methylpseudouridine in the injectable is pervasive and long-lasting.
To summarizethe above: N1-Methylpseudouridine, as it is used in the “synthesized, enhanced, and turbo-charged” form found in the modRNA COVID-19 “vaccines”, replaces the body’s natural Uridine (by 100%) in the “vaccinated” person’s body; it assists in the evasion of the body’s natural immune system by these “vaccines”; it assists in the mechanisms of action of these”vaccines” in the body; and it negates the multiple beneficial effects that natural Uridine provides for the body. It replaces the body’s natural Uridine with a combination of what is basically an element (Pseudouridine) that is, at best, a “by-product” of RNA and can cause cancer, plus a “turbo-charged” methylation of Pseudouridine. Yes, a form of methane. Recall that the modRNA COVID-19 “vaccines” cross the Blood-Brain Barrier and enter the brain of the “vaccinated” person’s body. Recall that the modRNA COVID-19 “vaccines” are spread throughout the “vaccinated” person’s body via the dangerous lipid nanoparticles present in these “vaccines.” The result, in Yours Truly’s opinion, is a recipe for disaster. It is inconceivable that the scientists at Pfizer-BioNTech and at Moderna did not know how Uridine works, and how important it is for the human body. In Yours Truly’s opinion, the replacement of Uridine with the “lab-synthesized, enhanced, and turbo-charged” version of N1-Methylpseudouridine was “acceptable” in order to use the modRNA COVID-19 “vaccines” as a vehicle for human cellular modification and “reprogramming”, in addition to assisting in the mechanisms of these “vaccines.”
To the best of Yours Truly’s knowledge so far, Uridine RNA that has been replaced by the N1-Methylpseudouridine form described in today’s post does not “regenerate” in the “vaccinated” person’s body. It may help to Uridine-rich foods (see above in the post), perhaps along with taking a Uridine supplement (the use of Uridine supplementation, in Yours Truly’s opinion, would need to be discussed with a healthcare professional); and for the COVID-19 “vaccinated” person to at least consider refusing to take any further injections of modRNA COVID-19 “vaccines.”
General Summary: The modRNA COVID-19 “vaccines” manufactured by Pfizer-BioNTech and by Moderna contain a “lab-synthesized, enhanced and turbo-charged” version of an element that occurs in the microorganism domain called Archaea. This Archaean element is called N1-Methylpseudouridine. The version in the modRNA COVID-19 “vaccines” is called N1-Methylpseudouridine-5′-Triphosphate. Once inside the “vaccinated” person’s body, this ingredient replaces an important RNA component in the human body, called Uridine. Uridine has multiple beneficial benefits and mechanisms in the human body. It is found in the RNA of various foods, such as beets, goat’s milk and cheese, walnuts, and in beer. N1-Methylpseudouridine-5′-Triphosphate appears to have no natural benefits for the human body; its use in the modRNA COVID-19 “vaccines” is as a vehicle for human cellular modification and “reprogramming”; and, to assist in the mechanisms of these “vaccines.”
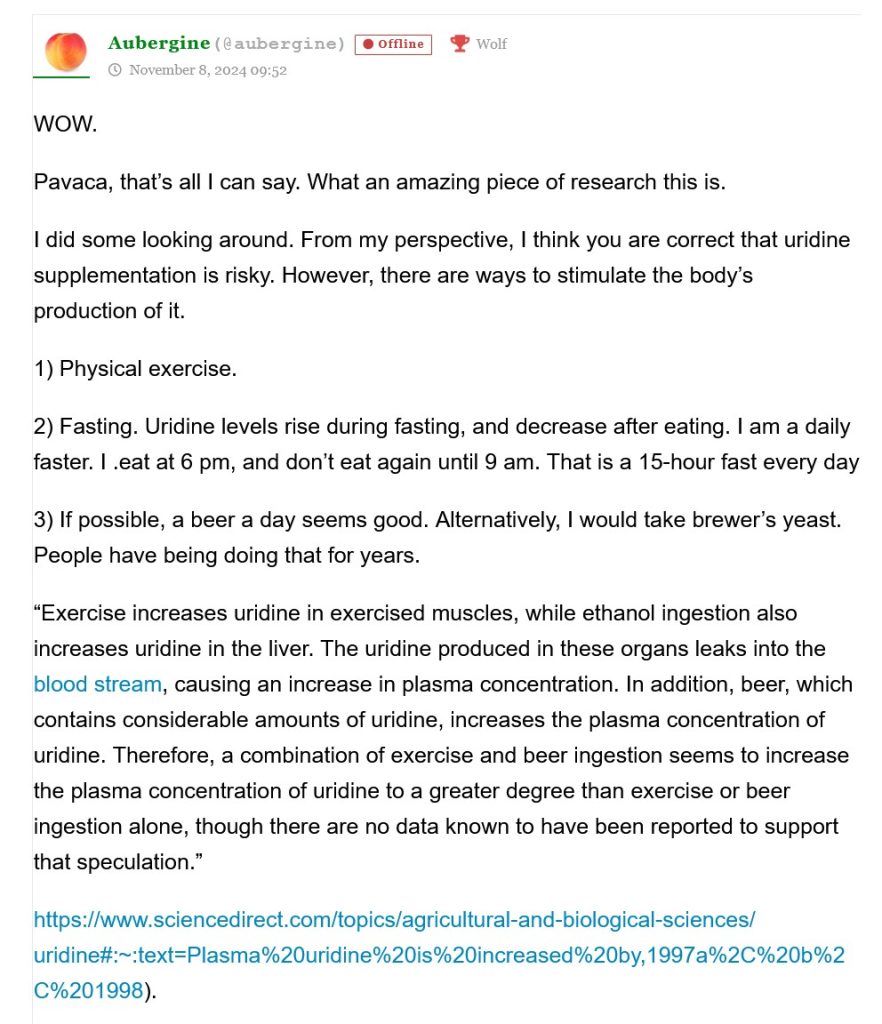
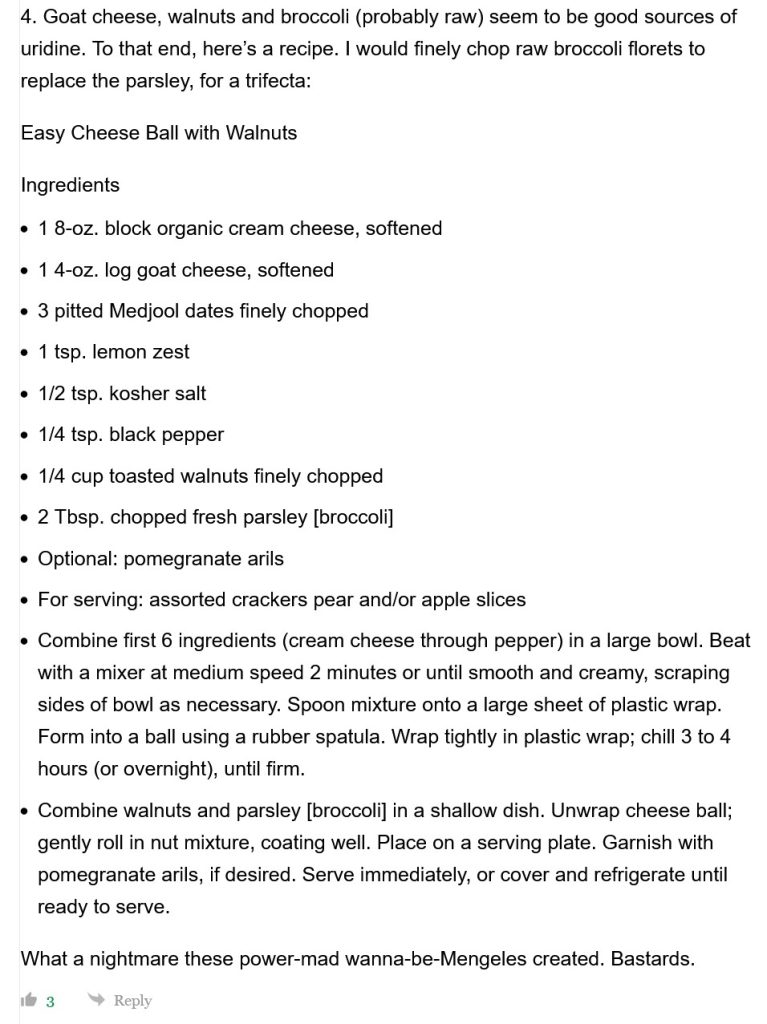
UPDATE, Friday 8 November 2024: At the suggestion of SteveInCO, the following comment from Aubergine is included regarding natural assistance for Uridine production in the body (two screenshots, below). Thank you, Aubergine!
Salads with goat cheese and walnuts can work. So can raw broccoli spread with a mixture of goat cheese, a little pepper, and a little Balsamic vinegar.
The above vintage image of a Rolodex is courtesy of CSA Images via Google Images.
Today’s Health Friday is a very Special Edition.
God Bless You, my brother Sam — 24 November 1948 – 29 October 2024.
Requiescat in pace aeterna, et Lux Perpetua luceat tibi. You are now with your beloved wife in the next world. Have a wonderful new life together there. “Till we all meet again.”
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and caveat items from Yours Truly, all linked here, of which readers should be aware. The discussion today is not limited to what is presented below — it is an Open Thread.
Health Friday today is a list of links to various scientific papers and articles, blog posts, and other items, regarding the COVID-19 “vaccines” injections (gene therapy injections.) Today’s list is not exhaustive; it is part of an ongoing project. The discoveries that reveal more of the truth about these dangerous and deadly injections, and the items that are published about these discoveries, are increasing by the month. Readers may know some of the information presented below already; other items may be new. And, while the fact is that the COVID-19 “vaccines” have been, and are, inducing injuries, illnesses, disabilities, and deaths in “vaccinated” people all over the planet — there are things that they can do to mitigate, reduce, or perhaps even eliminate, the damage that these “vaccines” have done, and are doing, to their bodies (these links are at the end of The List, Part One.) In addition, in Yours Truly’s opinion, there is one important item that COVID-19 “vaccinated” persons need to at least consider: Do not take any more COVID-19 “vaccine” injections; and, Do not allow these injections to be given to minor children.
The list, Part One:
Three books,: Two, by Naomi Wolf, Ph.D., and Amy Kelly: The Pfizer Papers: Pfizer’s Crimes Against Humanity; and, The Moderna Papers: Moderna’s Crimes Against Humanity. Search by title at https://books.google.com/; and, the third, by Dr. Pierre Kory, MD: The War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the Pandemic; available at www.amazon.com/.
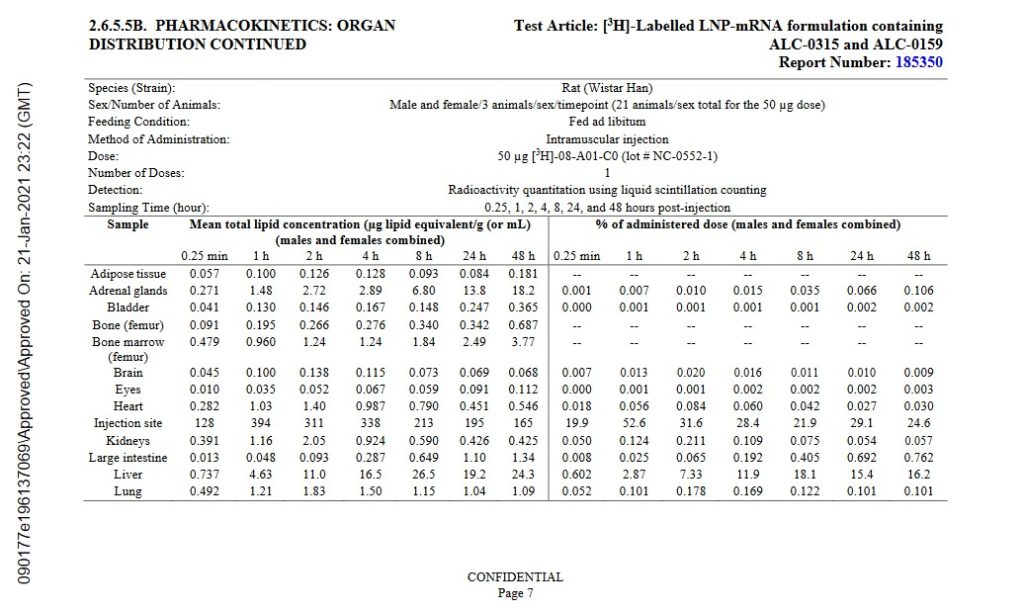
https://icandecide.org/wp-content/uploads/2022/03/125742_S1_M2_26_pharmkin-tabulated-summary.pdf, BNT162b2 Module 2.6.5. Pharmacokinetics Tabulated Summary, FDA time-stamped 21 January 2021. The agency knew, as of this date, that the Pfizer-BioNTech modRNA COVID-19 “vaccine”, BNT162b2, spreads throughout the body of the “vaccinated” person. However, the agency had already granted the initial EUA for this injectable to be used in the United States. This report should have been the signal to the FDA that all use of BNT162b2 needed to be suspended, pending further investigation and testing. The FDA did nothing of the kind: in fact, the agency granted “full approval” of BNT162b2, under the name COMIRNATY. Please see Page 7 and Page 8 of this report, below, which shows the whole-body biodistribution of BNT162b2:
www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports, FDA time-stamped 30 April 2021. This report, given by Pfizer-BioNTech to the agency, contains an Appendix 1. List of Adverse Events of Special Interest at the end of the report. The Appendix 1. lists over 1,200 different types of adverse events medical conditions and illnesses, including death, resulting in persons who took BNT162b2 between 11 December 2020 (the date on which this “vaccine” was granted the initial EUA by the FDA for use in the United States) and 28 February 2021. The FDA knew about this on 30 April 2021. This report should have been another signal for the agency to suspend all use of BNT162b2 pending further investigation and testing, but the FDA did nothing to stop the continuing rollout of this injectable.
Scientific papers and/or articles:
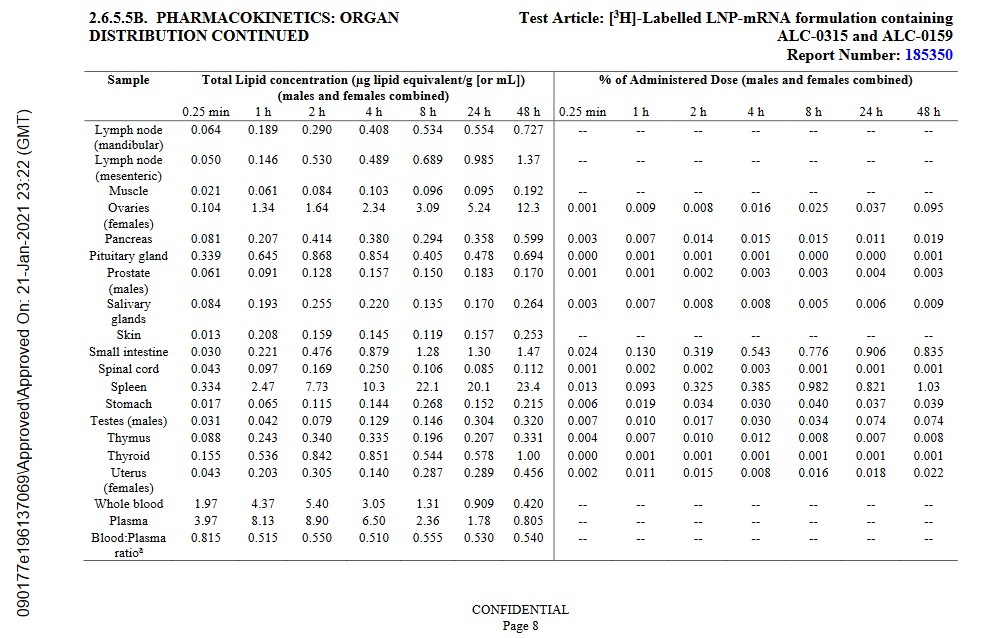
The Pfizer-BioNTech modRNA COVID-19 “vaccines” cross the Blood-Brain Barrierand negatively affect the cells of the “vaccinated” person’s brain. Below is section 4. Conclusions of the paper by H. Abramczyk, et al. (https://doi.org/10.1101/2022.03.02.482639, “Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System: human brain normal glial and glioma cells by Raman imaging”, 2022):
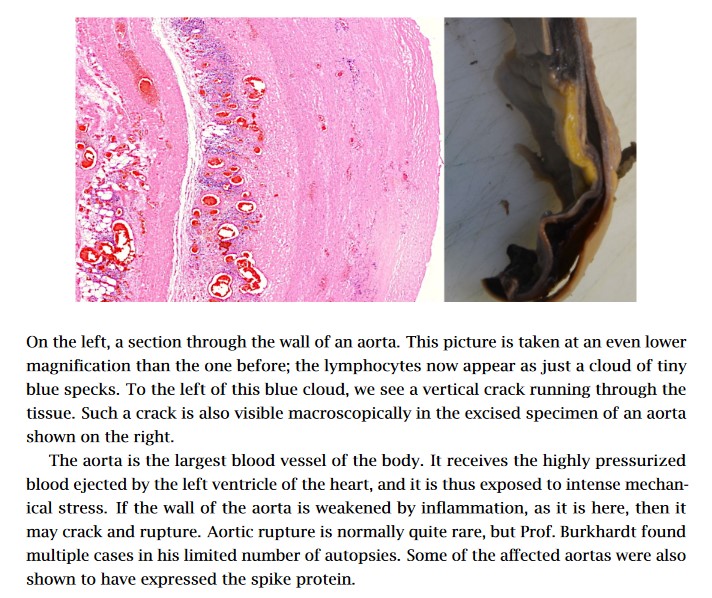
The COVID-19 “vaccines”damage the lungs, the cardiovascular system, and the heart of the personwho takes these “vaccines.” Please see the slides in this 2022 article: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, by Michael Palmer, MD, and Sucharit Bhakdi, MD. Below, for example, is Slide 10 from the article, showing lymphocytes lining the aorta prior to aortic rupture in a COVID-19 “vaccinated” person (from the autopsy):
ThePfizer-BioNTech modRNA COVID-19 “vaccines” change the DNA of the person who takes these injectables. This is the “Markus Alden, et al” 2022 paper (https://doi.org/10.3390/cimb44030073, “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Markus Alden, et al., February 2022.) The DNA that is reverse transcribed is the LINE-1 of the human liver cell line Huh7.
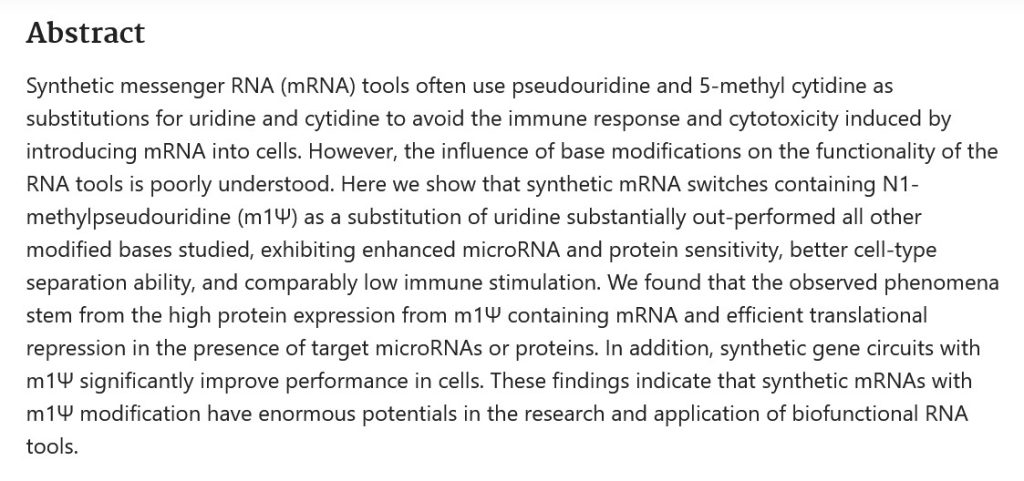
The Pfizer-BioNTech modRNA COVID-19 “vaccines” replace the RNA in Uridine, an important component produced by the liver, in persons who take these injectables. This is done by the mechanism of the N-1 Methylpseudouridine that is added to these “vaccines.” (https://pubmed.ncbi.nlm.nih.gov/32090264, “N1-Methylpseudouridine substitution enhances the performance of synthetic mRNA switches in cells”, Callum JC Parr, et al., April 2020.) Uridine helps to regulate mood, among other functions. In addition to the Parr, et al., paper above, there is also this, regarding negative neurological effects induced by the COVID-19 “vaccines”: www.theqtree.com/2024/10/18/health-friday-10-18-2024-special-edition-neurological-effects-of-the-covid-19-vaccines-physical-and-psychological/.
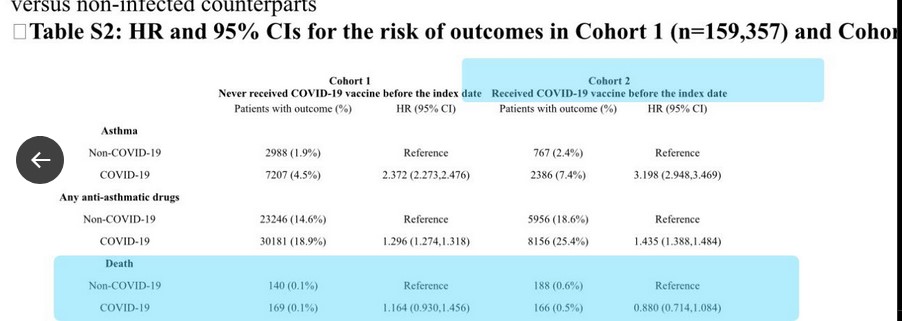
The paper referred to: https://doi.org/10.1007/s15010-024-02329-3. “The association between COVID-19 vaccine/infection and new-onset asthma in children–based on the global TriNetX database”, Chia-Chi Lung, et al., (June 2024.) This study is actually a “two-fer”: First, the COVID-19 “vaccines” induce new-onset asthma in children; and, second, children are at risk of dying from the COVID-19 “vaccines.”
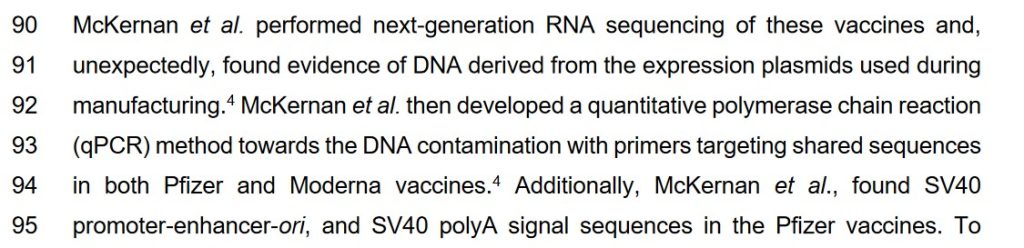
There are DNA “fragments” in the COVID-19 “vaccines”; and, there is a piece from the gene code of the SV40 cancer promoter from the African Green Monkey in the Pfizer-BioNTech modRNA COVID-19 “vaccines.“ The “McKernan, et al. paper” describes both of these negative effects. Below is a screenshot of a portion of the Introduction of this paper:
The “McKernan, et al.” paper: www.researchgate.net/publication/374870815, “DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events.”, Kevin McKernan, David Jeremiah Speicher, et al. (2023.)
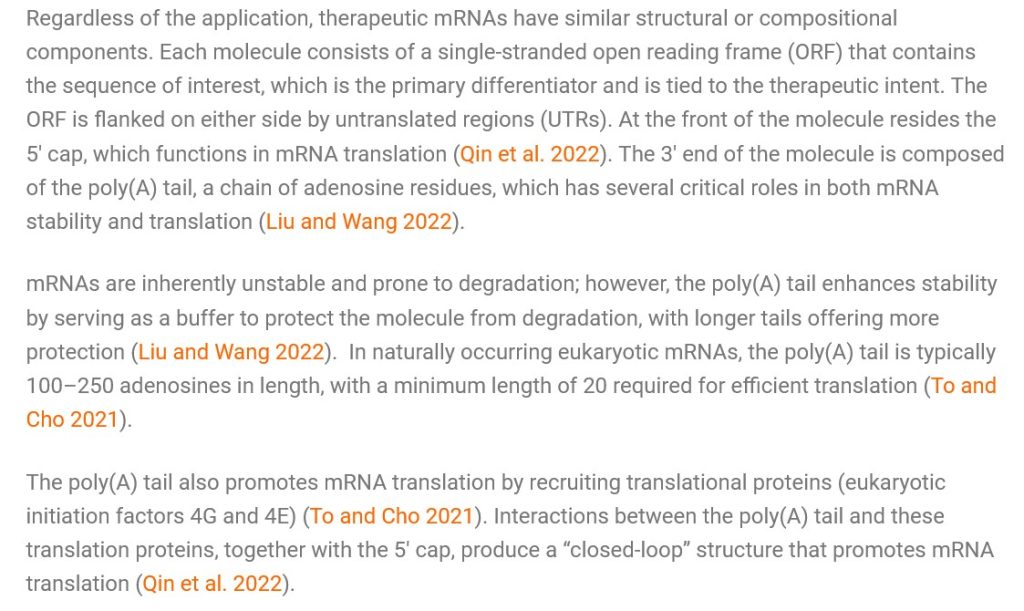
**** The “placement” of the SV40 cancer promoter gene piece in the polyA tail of the modRNA COVID-19 “vaccines”, in Yours Truly’s opinion, was deliberate. The following quotation is from an article by Marwan Alsarraj in August 2023: “In mRNA therapeutics, the poly(A) tail drives the efficacy of the mRNA molecules…” The article: www.bioradiations.com/polya-tails-in-mrna-based-therapeutics-823/, “Poly(A) Tails: A Critical Quality Attribute in mRNA-based Therapeutics”, 8 August 2023. Below is a screenshot from this article:
**** In Yours Truly’s opinion, the “closed loop” produced by the interactions of the poly(A) tail and the “translation proteins” means that the changes that the COVID-19 “vaccines” make to the DNA (via the SV40 cancer promoter gene piece in these “vaccines”) and to the RNA (via the N-1 Methylpseudouridine in these “vaccines”) of COVID-19 “vaccinated” persons can likely be permanent.
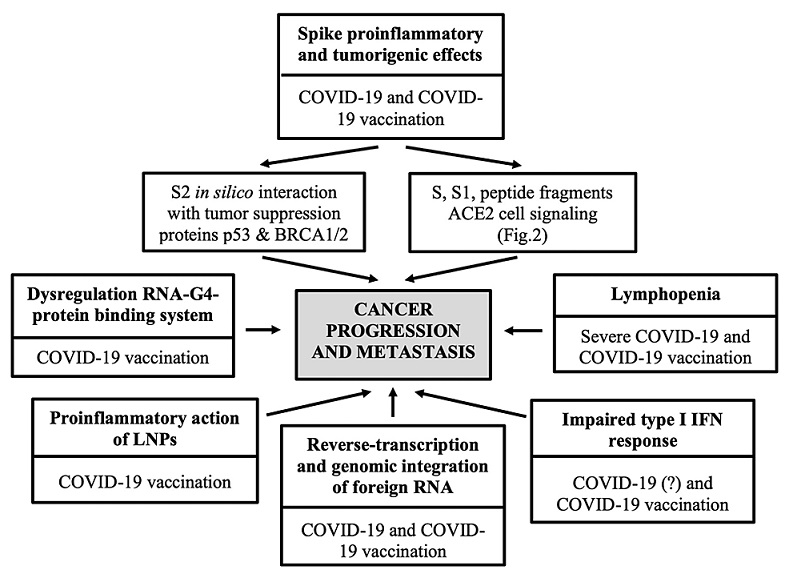
The COVID-19 “vaccines” can induce cancer, including what is called “turbo-cancer” in “vaccinated” persons; they can also induce “re-establishment” of previously under control or even previously cured cancers in “vaccinated” persons. The “vaccines” do this, among other ways, via the mechanisms of the SV40 cancer promoter gene (see above); and, the damage the “vaccines” do to the p53 cancer tumor suppressor protein in the body. Please see: www.theqtree.com/2023/11/29/the-covid-19-vaccines-pave-the-way-for-turbo-cancers-and-a-note-on-the-virus-itself/. Please also see: https://doi.org/10.7759/cureus.50703, “SARS-CoV-2 Vaccination and the Multi-Hit Hypothesis of Oncogenesis”, Raquel Valdes Angues and Yolanda Perea Bustos, (2023.) Below is a screenshot from the Review section of this paper:
In addition, please watch the video linked to this tweet (a presentation by British surgeon Dr. James Royle): https://x.com/SaiKate108/status/1851199741276602449. At 1:42 in the video, Dr. Royle describes what he sees in COVID-19 “vaccinated” patients who present with cancer: “…out of the blue, [the] liver [is] filled with large, round tumor masses.” Please refer up in today’s post at the Pfizer-BioNTech biodistribution amounts of BNT162b2 (Page 7 of the company’s Pharmacokinetics Tabulated Summary report): the accumulation of the dangerous lipid nanoparticles carrying the modRNA of this “vaccine” is 24.3mcg per gram (or mL) in the livers of the lab rats 48 hours after BNT162b2 was injected into them.Notice that the amount had steadily increased post-injection before it was measured at 48 hours post-injection. Also, note that BNT162b2 is the basis for all other modRNA COVID-19 “vaccines” manufactured by this company. **** In Yours Truly’s opinion, the liver was “targeted” as a major accumulation area for the lipid nanoparticles and for the other ingredients of BNT162b2, due to the number of body mechanisms and functions it regulates or assists in regulating. Please the Introduction, below, of the NIH StatPearls book, Physiology, Liver, by Arjun Kalra, et al. (StatPearls Publishing, January 2024):
COVID-19 virus and COVID-19 “vaccine” detox / mitigation protocols:https://covid19criticalcare.com/ (FLCCC Alliance); https://americasfrontlinedoctors.org/ (AFLDS); www.mercola.com/ (Dr. Joseph Mercola, MD; must sign up to access); www.americaoutloud.shop (Dr. Peter McCullough’s Wellness Company site.) Note: this is not an exhaustive list, and does not include herbal medicine, natural medicine, or other allopathic / osteopathic / homeopathic medicine sites.
Yours Truly has been researching, reading, and writing about the COVID-19 virus and the COVID-19 “vaccines” since March 2020. What readers find in the Health Friday posts are opinions and hypotheses based on this research and reading: it is not medical advice.
The uncovering of the truth about the dangerous, deadly COVID-19 “vaccines” is an ongoing, evolving issue. It is Yours Truly’s considered opinion that, with some exceptions, any person who has taken any COVID-19 “vaccine” since 11 December 2020 is at risk for adverse events, including COVID-19 “vaccine”-induced illness, injury, disability, or even death from these injectables. The COVID-19 “vaccines” have proven to not be “safe and effective.” Those who developed these injectables, knowing (or even suspecting) that they were not, and are not, “safe and effective”; and those who “mandated” their use, who coerced people into getting them, and who continue to push them, must be held accountable.
Detail of a partially blurred periodic table of the elements. Focus on Carbon.
The above image of part of the Periodic Table is courtesy of Google Images.
Today’s post is part of Health Friday, a series devoted to issues related to Big Pharma, vaccines, general health, and associated topics. The discussion is not limited to what is presented here: It is an Open Thread.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, caveat items from Yours Truly, and other information that readers should know. They are all linked here. Since today’s post is related to the COVID-19 “vaccines” injectables (gene therapy injections), it is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
The post today is not an exhaustive interpretation of the “Diblasi, et al. paper.” In fact, the paper raises many other questions that demand answers: several sets of questions (from Yours Truly) are listed in the post. Yours Truly is also aware that a certain person is attempting online to “debunk” this paper, to the point of labeling it as a “hoax”; one finds it difficult to agree with such a conclusion. Stay with me, a certain amount of “preliminary” items are presented in the post to assist in the general framework. There is a General Summary at the end of the post.
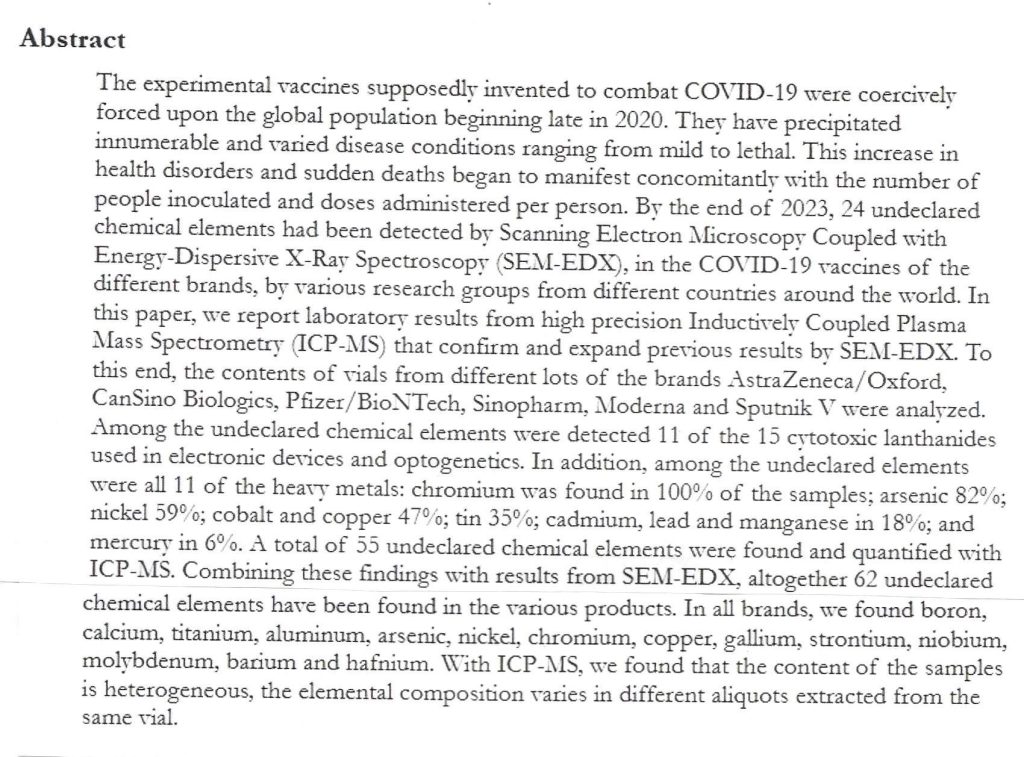
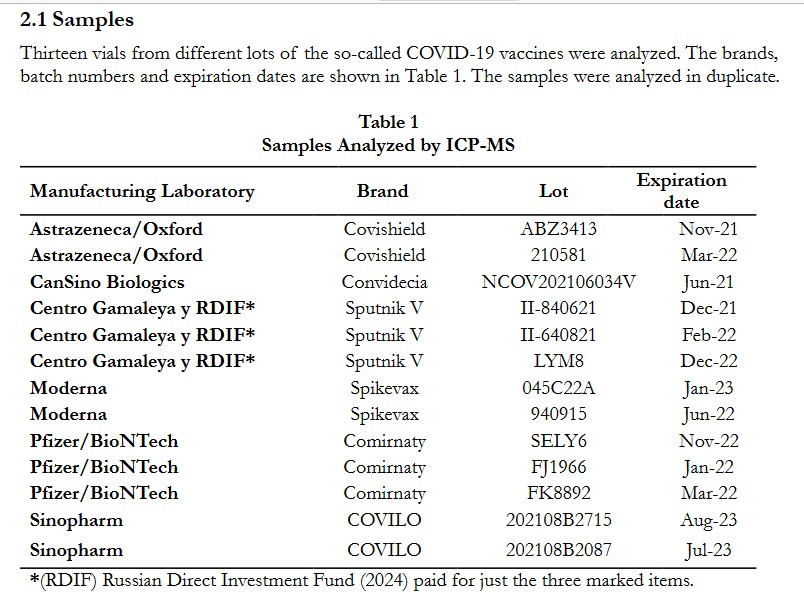
The tweet leads to this link: https://childrenshealthdefense.org/defender/undeclared-chamicals-heavy-metals-covid-vaccines/, 55 Undeclared Chemical Elements — Including Heavy Metals — Found in COVID Vaccines, by Brenda Baletti, Ph.D., 15 October 2024. This, in turn, led to the “Diblasi, et al. paper”: https://doi.org/10.56098/mt1njj52, At Least 55 Undeclared Chemical Elements Found in COVID-19 Vaccines from AstraZeneca, CanSino, Moderna, Pfizer, Sinopharm and Sputnik V, with Precise ICP-MS, Lorena Diblasi, Martin Monteverde, David Nonis, Marcela Sangorrin, 11 October 2024 (International Journal of Vaccine Theory, Practice, and Research, Vol. 3 No.2 (2024): Injuries, Causes, and Treatments, Part 2.)
The Abstract of the paper:
Note that the there was a total of 62 undeclared chemical elements found, all told, in the COVID-19 “vaccines” injectables (gene therapy injections) that were tested by the authors. Note also that the COVID-19 “vaccines” (gene therapy injections, hereafter termed GTI) that were tested comprised various “platforms”: modRNA (Pfizer-BioNTech and Moderna; viral vector (AstraZeneca/Oxford, CanSino Biologics, and Sputnik V), and whole inactivated virus (Sinopharm.) (All “platform” descriptions, per Wikipedia.)
The Samples List of the “vaccines” tested, from the paper:
Below are the results for the Moderna “vaccine” samples, from the paper; note that, as of October 2022, 37.50% of COVID-19 “vaccinated” persons in the United States had taken at least one dose of this “vaccine” (mRNA-1273/SPIKEVAX.) https://en.wikipedia.org/wiki/COVID-19_vaccination_in_the_United_States
The results for the Pfizer-BioNTech “vaccine” samples, from the paper; note that, as of October 2022, 59.43% of COVID-19 “vaccinated” persons in the United States had taken at least one dose of this “vaccine” (BNT162b2/COMIRNATY.) https://en.wikipedia.org/wiki/COVID-19_vaccination_in_the_United_States
Given that the Pfizer-BioNTech COVID-19 “vaccine” (GTI) has the higher percentage of persons who were “vaccinated” with it, Yours Truly will restrict the discussion as it relates to this post to the results of the Pfizer-BioNTech tests. In addition, results of six isotope types (chemical element types) from the last two assay dates — 3/11/2023 and 3/1/2024, are underlined by Yours Truly. These six are: Lithium (Li); Aluminum (Al); Vanadium (V); Chromium (Cr); Arsenic (As); and, Barium (Ba.)
The higher the number of protons and neutrons in a chemical element, the more “mass” the chemical element has.
Yours Truly will remind readers that the Pfizer-BioNTech COVID-19 “vaccines” (GTI) cross the Blood-Brain Barrier, in addition to accumulating in organs and areas throughout the body of the person who takes this “vaccine.” Please see Page 7 and Page 8 of the company’s report on the biodistribution of their COVID-19 “vaccine” injectable BNT162b2 (now COMIRNATY), below:
Proceeding now to the underlined chemical elements items in the last two assays of BNT162b2 / COMIRNATY, from the Diblasi, et al., paper. Note: sections of information regarding this chemical element (Arsenic), and the other five underlined chemical elements in the last two assays of this “vaccine”, are from the Royal Society of Chemistry (RSC) online entries; other sources of information for each one will be text-hyperlinked. First, Lithium (Li):
Aluminum (Al) effects on the body: neurological toxicity, encephalopathy, among others: https://doi.org/10.3238/arztebl.2017.0653, “The Health Effects of Aluminum Exposure”, Katrin Klotz, et al.
Lithium, Aluminum, Vanadium, and Chromium are metals of various degrees of hardness (“heavy metals.”) Arsenic is a “semi-metal.” Barium is a “soft, alkaline earth metal.” (All, per Wikipedia.)
Questions that arise, first set: Why are there so many chemical elements in BNT162b2/COMIRNATY? Why did Pfizer-BioNTech not “declare” almost all of them? Were each of the chemical elements that the company added to BNT162b2/COMIRMATY separately tested for toxicity prior to inclusion in the product? Was there some sort of “collusion” among the developers of the various COVID-19 “vaccines” (GTIs) that were tested along the lines of, “You put ABC chemical elements into your product, we’ll put XYZ chemical elements into our product, and we’ll see how it goes”? Why does it appear that the amounts of these chemical elements reduce, increase, or “disappear” from the products from one test assay to another of the same “vaccine”? Does that have to do with the other technologies that seem to be in these “vaccines” — other technologies such as, “self-assembling” items? Or, such as, a kind of “incubation period” that is “built into” the product? If either, or both, of these are the case, what does that mean to the mechanisms of these “vaccines” once they are injected into the human body? What about COVID-19 “vaccine shedding” www.theatree.com/2024/03/25/the-elephant-in-the-room-shedding-of-both-the-covid-19-virus-itself-and-the-covid-19-vaccines/? For examples, Ruthenium and Lead are absorbed by the skin; and, Arsenic can be absorbed by the skin.
For an important comparison: One other item, the ICP-MS test results for the Russian COVID-19 “vaccine” (GTI), Sputnik V. Recall that this “vaccine” is made of the whole inactivated virus of SARS-CoV-2; it is the only “vaccine” that was tested that was based on this. Below are the test results:
Yours Truly included the Sputnik V test results because this COVID-19 “vaccine” is not modRNA-based. And yet, look at the test results for this product. The same six chemical elements that Yours Truly underlined in the BNT162b2/COMIRNATY test results are ALSO in Sputnik V: Lithium; Aluminum; Vanadium; Chromium; Arsenic; and Barium. Even if Aluminum is discounted (since various forms of Aluminum are used as “excipients / adjuvants” for COVID-19 “vaccines” injectables (GTIs), that leaves the other five chemical elements as being present in both products.
Questions that arise, second set: What does this mean? Could it possibly mean that the SARS-CoV-2 (COVID-19) virus itself had chemical elements “lab-included” while it was being lab-created at the Wuhan Institute of Virology? If this is so, what about the other chemical elements on the test results list?
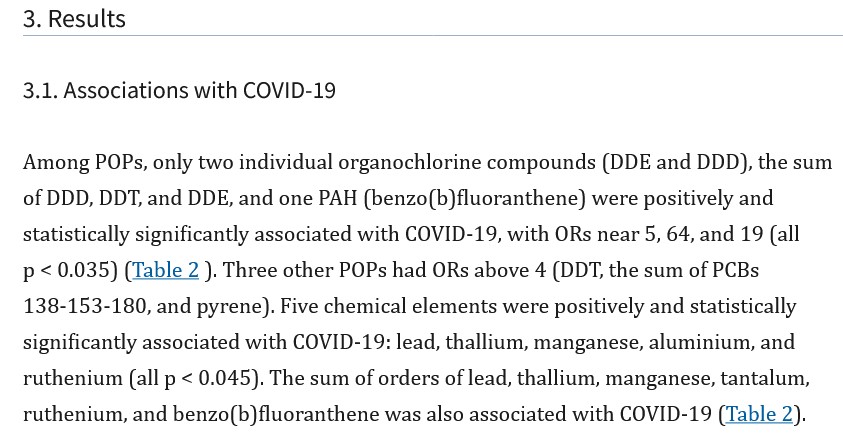
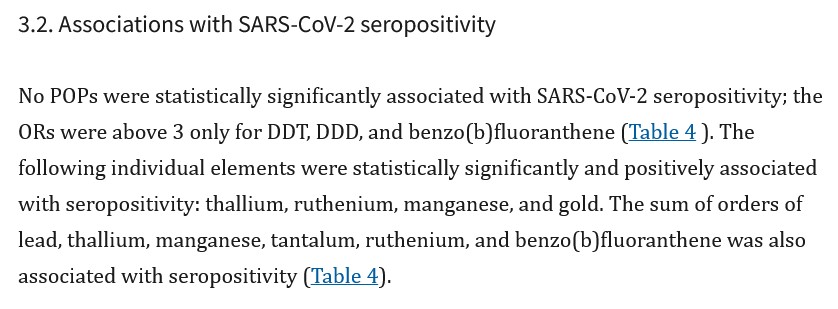
A paper published in 2023 (but using data from patients infected by the COVID-19 virus itself, and/or the SARS-CoV-2 virus,from before any COVID-19 “vaccine” was in use, or just after BNT162b2 was first authorized for use), gives, in Yours Truly’s opinion, a clue https://doi.org/10.1016/j.envres.2023.115419, “Individual blood concentrations of persistent organic pollutants and chemical elements, and COVID-19: A prospective cohort study in Barcelona”, Miquel Porta, et al., 4 February 2023. The cohort patients in this study were infected with the COVID-19 virus itself, or the SARS-CoV-2 virus, between mid-February 2020 and 24 January 2021.Below are two screenshots from this paper:
The Porta, et al., paper lists in the Tables the pollutants and chemical elements that were found in the COVID-19 virus itself infected patients. Among them: Lead (Pb); Arsenic; Cadmium (Cd); Mercury (Hg); Thallium (Tl); Bismuth; (Bi) Molybdenum; (Mo) Iron (Fe); Zinc (Zn); Cobalt; (Co) Chromium; Tantalum (Ta); and, Ruthenium (Ru).
The Porta, et al., paper lists in the Tables the pollutants and chemical elements that were found in the SARS-CoV-2 infected patients. Among them: Ruthenium; Tantalum; Lead; DDT; and, Thallium.
“Lifestyle” factors, such as smoking (current, past, stopped) are accounted for in the Porta, et al., study. Even removing pollutants that would be found in cigarette smoke (naphthalene and Cadmium among them), that leaves chemical elements such as Ruthenium, Tantalum, and Thallium that were found in the blood of the patients in the Porta, et al., study. And, that the presence of these chemical elements was persistent — lingering after the infection was resolved. By the way, Ruthenium and Thallium are radioactive. Barium is a “radiographic contrast agent” (in, for example, the “barium milkshake” test.)
Questions that arise, third set: What about the other chemical elements found in the various COVID-19 “vaccines”, per the Diblasi, et al., study? Were these “lab-included” into the “excipients / adjuvants” used in these “vaccines”? Were these “lab-included” into the Wuhan Hu1 SARS-COV-2 samples that were used by the companies developing and/or manufacturing these “vaccines” (samples that presumably, at least the start of the pandemic, came from the WIV? Did these companies decide of themselves to include them?
The COVID-19 “vaccines” injectables (GTIs) contain: the modRNA (lab-enhanced from the Wuhan Hu1 SARS-CoV-2 virus) in the COVID-19 “vaccine” injectables that use this platform; the SV40 African Green Monkey cancer promoter gene piece in the Pfizer-BioNTech “vaccine” injectables (https://doi.org/10.31219/osf.io/mjc97, “DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events”, David J. Speicher, et al., 19 October 2023; DNA fragments in both the Pfizer-BioNTech and in the Moderna COVID-19 “vaccine” injectables (see paper cited above); dangerous lipid nanoparticles (ALC-0159, ALC-0315 in the Pfizer-BioNTech COVID-19 “vaccine” injectables; SM-102 in the Moderna COVID-19 injectables); polyethylene glycol “excipients / adjuvants” (PEG2000-DMG); and, numerous chemical elements, including heavy metals (Vanadium; Chromium); radioactive elements (Thallium); Arsenic;Ruthenium; and, Lithium. These are the ingredients that COVID-19 “vaccinated” persons age 18 and older have in their bodies. These are the ingredients that adults allow their children to be COVID-19 “vaccinated” with. No one knows exactly how long the COVID-19 “vaccines” work inside the body of the “vaccinated” person.
What about the SARS-CoV-2 virus itself? Yours Truly opines that this may contain, among other items: mixed RNA/mRNA coronavirus elements and pieces from various animal sources (bats; monkeys; civets; pangolins); Chromium; Cobalt; Zinc; Arsenic; Molybdenum; Ruthenium; Cadmium; Gold (Au); Thallium; and, Lead. There are heavy metals among these.
“Chelation” is a method used to remove heavy metals from the body. The use of chelation is controversial. Physicians can prescribe certain medications to assist in removing heavy metals from the body. An article on a heavy metal “detox diet” is here: www.healthline.com/health/heavy-metal-detox, “Heavy Metal Detox Diet”, by Kiara Anthony, 13 September 2023.
Questions that arise, fourth set: What, if anything, did Dr. Anthony Fauci know about the inclusion of numerous chemical elements into the Pfizer-BioNTech COVID-19 “vaccine” injectables? What did Dr. Francis Collins (Dr. Fauci’s superior at the NIH) know? What did Albert Bourla (CEO of PfizerUSA) know? What did Dr. Deborah Birx know? What did the FDA know? What did the CDC know?
En Fin: At what point will people, horrified at the deaths, disabilities, illnesses, and injuries, being inflicted on their COVID-19 “vaccinated” family members, friends, and colleagues, realize that “they’ve been had”? At what point will people realize that the “official narrative” of, “the COVID-19 vaccines are safe and effective” means that these injectables are NOT safe; and, that “effective” means the amount of damage these injectables have done/continue to do, to the bodies of the “vaccinated”? At what point do people realize that the “official narrative” of, “the known and potential risks outweigh the known and potential risks” of the COVID-19 “vaccines” was, and is, a lie? — and that the COVID-19 “vaccines” are “all risk and no benefit”? (https://kirschsubstack.com/p/the-covid-vaccine-all-risk-no-benefit, by Steve Kirsch, 4 October 2024.)
General Summary: It is now known (per the Diblasi et al., paper) that the COVID-19 “vaccines” (GTIs) contain numerous chemical elements, some of which are radioactive, and others of which are metals and/or “rare Earth” elements. It is now known that the COVID-19 virus itself likely contains chemical elements, at least three of which (Chromium, Thallium, and Lead) are heavy metals; and that at least one of which (Thallium) is radioactive. It is now known that (per the Porta, et al. paper) that these chemical elements are persistent in the body of a person who was infected with the COVID-19 virus itself but who has recovered. It is now known that chemical elements are found in the modRNA-based and in the whole inactivated virus-based COVID-19 “vaccine” (GTI) injectables. There are many questions that arise from these discoveries that demand answers.
The above word-cloud image about memory loss is courtesy of Google Images.
This post is part of Health Friday, a series devoted to Big Pharma, vaccines, general health, and associated topics. Today’s offering, a Special Edition, is in honor of Yours Truly’s “fully vaccinated and boosted” brother, who was just diagnosed with “sudden-onset dementia.” Yours Truly will make it clear that one is not a medical doctor; one is not treating my brother; and, this post is a “narrative primer” on negative neurological effects from the COVID-19 “vaccines”, the Pfizer-BioNTech COMIRNATY (BNT162b2) modRNA COVID-19 “vaccine” in particular.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and, certain extra items that readers should be familiar with. They are all linked here.
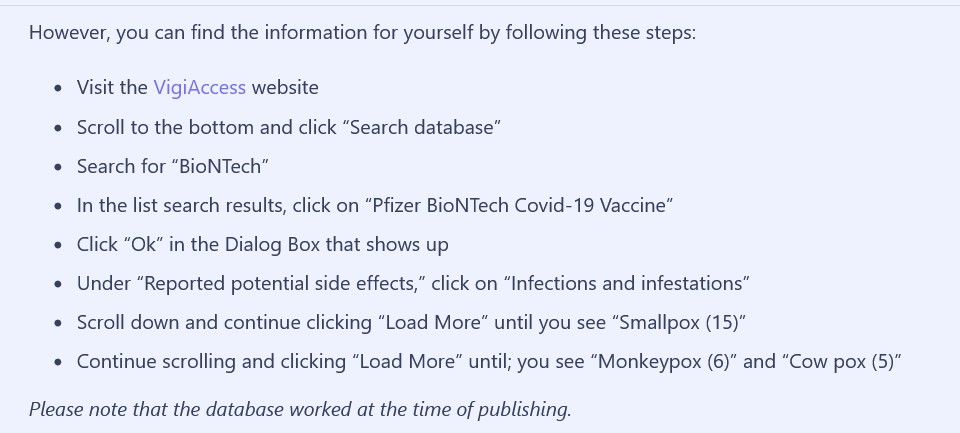
The World Health Organization (WHO) has a website, www.vigiaccess.org/, that lists “side effects” reported in persons who took COVID-19 “vaccines.” The Mole article describes how the VigiAccess search was performed to find “Monkeypox” as a “side effect” of the Pfizer-BioNTech COVID-19 “vaccine”, BNT162b2. A screenshot of the search protocol is below:
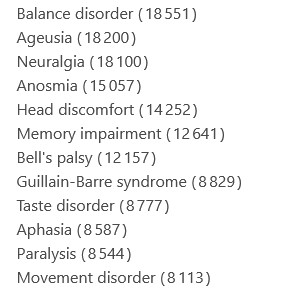
Yours Truly performed a VigiAccess search for reported memory problems (dementia is considered to be a form of “memory impairment.”) This is what I did:
Clicked on “Pfizer BioNTech COVID-19 Vaccine” on the list that came up
Clicked “OK” on the “Dialog” box
Under “Reported potential side effects”, I clicked on “Nervous system disorders” — and found a long list. A screenshot of a portion of this list shows “Memory impairment”:
These are only the reported cases of conditions that are considered to be “side effects” of BNT162b2. It can be argued that there are many multiples more “side effects” cases from BNT162b2 that are not reported for some reason. Yours Truly also performed searches on the VigiAccess list under “Psychiatric disorders”, and under “Metabolism and nutrition disorders”, as certain other details were given to one in phone conversations related to the situation which raised interest.
The balance of today’s post will be presented in a “quasi-scientific paper” form. With the exceptions of some in-line references, scientific paper, blog and/or article citations will be numbered in the text with [“number”], and listed at the end of the post. Hypotheses and opinions of Yours Truly (H/O) will be delineated by Bold text with Italics. A General Summary will be included at the end of the post.
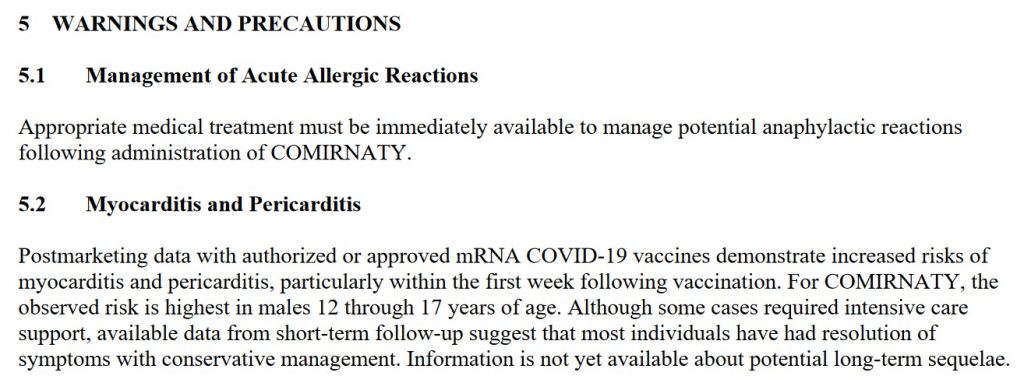
First: A Short Narrative Summary of What Occurs When a Person is Injected with the Pfizer-BioNTech modRNA “Vaccine” COMIRNATY: The “vaccine” here is the 2024-2025 Formula COMIRNATY COVID-19 “vaccine” (which, by the way, contains elements of BNT162b2, the original Pfizer-BioNTech modRNA COVID-19 “vaccine.”) Each “vaccine” dose is either supplied in a single-dose vial, with the dose to be administered withdrawn for injection; or, is in a pre-filled syringe ready for administration. (H/O)Upon “vaccination”, the person’s body immediately sends an “enemy detected” signal to the brain. The person’s body may react from fainting to chills to nausea, among other physical responses: see Sections 5.1 and 5.2 of the COMIRNATY 2024-2025 Fact Sheet, below [1]:
The lipid nanoparticles in the “vaccine” quickly begin to spread the contents of the injection throughout the “vaccinated” person’s body. This process is called biodistribution. Images of page 7 and page 8 of the January 2021 Pfizer-BioNTech Pharmacokinetics Tabulated Summary of the company’s modRNA COVID-19 “vaccine”, BNT162b2, are below [2]. Yours Truly will again emphasize that BNT162b2 is the basis for all of the Pfizer-BioNTech modRNA COVID-19 “vaccines”, including the COMIRNATY 2024-2025 Formula.
Note the accumulations in the Brain, the Liver, and the Large Intestine.
Note the accumulations in the Pituitary Gland, the Thymus Gland, and the Small Intestine. The intestines produce 90% of the body’s Serotonin. Serotonin is a neurotransmitter that is involved in the emotional / psychological / cognitive processes of the brain (per Wikipedia.)
Why is there accumulation of BNT162b2 in the Pituitary Gland? This small organ, called the “master gland” of the body, produces or directs many important hormones. Together with the hypothalamus, the pituitary gland work together to serve as the “brain’s central command center to control vital bodily functions”, according to Yours Truly’s online search at the Cleveland Clinic. These functions include breathing, stress response, reproduction, blood pressure, and more. (H/O): BNT162b2 and/or COMIRNATY is a “vaccine” to supposedly “prevent” a COVID-19 virus infection, not to work like a sort of pituitary gland treatment vehicle.
At least one of the lipid nanoparticles (LNPs) in COMIRNATY, ALC-0159 (but listed under its chemical component name), affects the thymus gland of the “vaccinated” person’s body. The thymus gland is “the primary lymphoid organ of the immune system” (per Wikipedia). The Abstract of a paper [3] that explains how ALC-0159 and other PEG-based LNPs work in the body is below:
While the lipid nanoparticles (LNPs) in COMIRNATY are spreading the ingredients of this “vaccine” throughout the “vaccinated” person’s body, the “vaccine” is using the PRRARSV “backdoor key” (an element which is only in the SARS-CoV-2 virus; and therefore, by extension, the modRNA COVID-19 “vaccines”) to facilitate entry of the “vaccine” ingredients into every cell in the “vaccinated” person’s body [4},[5]. (H/O)At the same time, the ingredients and mechanisms of COMIRNATY (BNT162b2) are beginning to work on inducing accelerated aging in the “vaccinated” person’s body, all the way down to the mitochondrial level [6]. Dao-Fu Dai, et al., wrote a paper in 2014 on how oxidative stress affects the mitochondria and the aging process [7].
N1-Methylpseudouridine is present in all versions of COMIRNATY (BNT162b2), starting with the “original version” of this “vaccine”, BNT162b2. N1-Methylpseudouridine is a synthetic form of Uridine. Uridine is an important nucleoside for neurological processes, for the central nervous system, and other body processes. It is found only in RNA. Below is the Abstract of the Yueyuan Yang, et al., paper that the mechanism of Uridine in the body [8]:
The importance of Uridine cannot be minimized. This RNA element is produced in the Liver. Uridine helps to regulate mood; it also assists in the release of dopamine in the brain. Dopamine is a neurotransmitter that “affects emotions, behavior, and movement” (per WebMD.)
The purpose of N1-Methylpseudouridine in COMIRNATY is twofold: One, to “supersede” / “overwrite” the mechanisms of the natural Uridine in the “vaccinated” person’s body; and, Two, to enhance the mechanism of COMIRNATY in “mRNA switches in cells” of the “vaccinated” person’s body (Callum JC Parr, et al.) [9]. Below is the Abstract of this paper:
Yours Truly will blow the lid off the deliberate inclusion of N1-Methylpseudouridine in BNT162b2 (COMIRNATY.) This chemical was specifically added to the “vaccine” to replace the processes of natural Uridine; and, to evade the body’s natural immune system’s “enemy detection and elimination” elements and mechanisms. Below are screenshots from the Global Patent for BNT162b2, 28 October 2021 [10}:
Note that this appears to be a tacit admission that Gain-of-Function experiments were performed to create the modRNA in BNT162b2.
Note that this appears to be an admission that self-amplifying RNA (saRNA) can be used in Pfizer-BioNTech COVID-19 “vaccines.”
In addition to the “replacing” of uridine with N1-Methylspeudouridine in the body of the person “vaccinated” with COMIRNATY, the DNA of that person’s body is also being changed; please see Slide 14 of this article for a graphic of how the modRNA COVID-19 “vaccines” change the DNA.
Meanwhile, the newly-COMIRNATY-“vaccinated” person’s body, having “detected” an “enemy within the gates” (the “vaccine”), is sending out “all-out effort” signals to the body’s natural immune system to manufacture large amounts of cells to “fight off” the “detected enemy.” These natural immune system cells include CD4 cells, CD8 cells, IgG3 cells, and lymphocytes. However, the ingredients and mechanisms of the “vaccine” hamper, damage, and/literally destroy these natural immune system cells, via the “class switch” [11]; while, at the same time, inducing oxidative stress and cell death at the mitochondrial level all over within the “vaccinated” person’s body; and, also, inducing a state (of a still-unknown timeframe) of “faux SARS-CoV-2 infection” in the “vaccinated” person’s body [12]. A screenshot from this University of Maryland Medical System is below; note the last sentence:
The “rationale” behind the development and use of the modRNA COVID-19 “vaccines” is that the human body is not capable, of itself, to detect and “fight off” an infection by the SARS-CoV-2 virus; the body must have “assistance” in the form of the modRNA COVID-19 “vaccines” and their mechanisms. (H/O)However, it can be fairly argued that, given the multiple Adverse Events reports regarding COMIRNATY to VAERS and to VigiAccess, that this “vaccines” needs much more thorough R&D processes, testing on lab animals and then on humans, and extensive data collection and analyses, before this “rationale” can be fully proven. Pfizer-BioNTech rushed BNT162b2 into production, into securing the initial Emergency Use Authorization from the FDA in December 2020, and into this modRNA COVID-19 “vaccine” being used on the general public, before any of the above were fully undertaken. Pfizer-BioNTech and the FDA knew, back in April 2021, that BNT62b2 could, and did, cause hundreds of serious Adverse Events [13].
Second: Physical Neurological Effects of the COVID-19 “Vaccines”: These negative effects are somewhat “easier” to identify, as they can present with unmistakable symptoms. From the Appendix 1. List of Adverse Events of Special Interest in the 5.3.6 Cumulative Analysis document on BNT162b2 that was cited above, some examples: Page 2: Brain stem embolism; Brain stem mycoplasmal (encephalitis); Central nervous system lupus; Cerebellar artery thrombosis; Cerebral venous thrombosis. Page 3: Demyelination; Embolic stroke; Encephalitis autoimmune; Encephalitis post-immunisation. Page 4: Epilepsy; Epileptic psychosis; Grey matter heterotopia; Guillain-Barre syndrome. Page 5: IIIrd nerve paralysis; Immune-mediated encephalitis; IVth nerve paresis. Page 6: Meningitis; Multiple sclerosis; Neuritis; Neuromyelitis optica spectrum disorder; Neuropsychiatric lupus. Page 9: Thrombotic stroke; XIth nerve paralysis.
Bell’s Palsy is also reported after BNT162b2 “vaccination” [14].
In other words, COMIRNATY (and BNT162b2) damage multiple mechanisms and processes of the brain that result in physical medical conditions and/or illnesses. This “vaccine” damages the sheath coverings of the nerves, including of the spinal cord (Demyelination.) This “vaccine” causes brain inflammations of various types (Encephalitis.) This “vaccine” causes stroke. This “vaccine” causes nerve paralysis. And more. (H/O) This “vaccine” can also potentially aggravate existing physical neurological conditions and/or illnesses, including ones that were under control before the patient was COVID-19 vaccinated.”
There is also what may be considered a “hybrid” condition, since it involves both physical and psychological symptoms, and since can be brought on by either an infection by the COVID-19 virus itself, or by COVID-19 “vaccination”: Long COVID (also called Long Vax.) Long COVID appears to be an “overraction of the immune system” [15]. Physical symptoms include blood pressure swings, fatigue, and “brain fog.” Psychological symptoms include depression, anxiety, and even PTSD [16]. The FLCCC Alliance has articles on Long COVID / Long Vax.
Third: Psychological Effects of the COVID-19 “Vaccines”: The Blood-Brain Barrier (BBB) consists of “closely-spaced cells” that act as a protective barrier to keep many substances from reaching the brain. Below is the National Cancer Institute definition of the Blood-Brain Barrier [17]:
However, COMIRNATY (and the BNT162b2 before it) were specifically developed to cross the Blood-Brain Barrier and to damage glial cells of the brain, down to the mitochondrial level [18]. A screenshot of section 4. Conclusions of this paper is below:
Recall that COMIRNATY (and the BNT162b2 before it) contain the lipid nanoparticle, ALC-0159. This lipid nanoparticle, one of the four within the “vaccine”, assists in the spread of the “vaccine” to all areas of the “vaccinated” person’s body, including into the brain.
Does the crossing of the Blood-Brain Barrier by COMIRNATY (and the BNT162b2 before it) also affect the psychological processes of the brain? The answer is, Yes: and, most likely, via the use of the N1-Methylpseudouridine in this “vaccine.” Recall that natural uridine, (which is one of the nucleosides that make up the RNA of the body) is produced by the liver. Uridine influences the brain by assisting in regulating mood, behavior, movement, and more. N1-Methylpseudouridine was deliberately included in COMIRNATY (and the BNT162b2 before it) to replace the natural uridine in the “vaccinated” person’s body with a created “faux uridine” (see the screenshots from the BNT162b2 Global Patent document, above in the post.) This chemical was chosen because it was “more effective” than the other two chemicals listed in the Global Patent documentation screenshot above in the post.
The Roh, et al., paper of 28 May 2024 traced a potential association between COVID-19 “vaccination” and the onset of Alzheimer’s disease(AD)and also of Mild Cognitive Impairment(MCI)[19]. A screenshot from this paper is below:
While there is not yet a proven association between MCI and the onset of dementia, the potential is higher for onset of dementia in persons who have MCI [20].
At the same time, there is documented proof that COVID-19 “vaccination” can cause psychosis. Examples of papers published on this topic are: the “Aljeshi paper” [21]; the “Borodina, et al., paper” [22];, the “Lazarevna, et al.” paper [23]; the “Morz paper” [24]; and, the “Laxmi and Grover paper” (psychosis diagnosed months after COVID-19 “vaccination”[25].
Yours Truly will again emphasize that one is not a medical doctor; nor am I treating my brother. (H/O) However, I believe there is sufficient evidence to at least consider the possibility that COMIRNATY (BNT162b2) modRNA COVID-19 “vaccinated” persons are at risk of numerous negative effects to the brain, both physical and psychological, induced by this “vaccine”; AND, since it is unknown exactly how long the elements and mechanisms of COMIRNATY (BNT162b2) work in the “vaccinated” person’s body, the possibility also exists that the potential for any physical or psychological neurological negative effects from this “vaccine” may actually increase with additional injections of COMIRNATY (BNT162b2.)
General Summary: One: The Pfizer-BioNTech modRNA COVID-19 “vaccine” COMIRNATY (and, the company’s modRNA COVID-19 “vaccine” BNT162b2 before it) can induce multiple negative physical and psychological neurological side effects and/or Adverse Events conditions in persons who take these “vaccines.”Two: COMIRNATY (and BNT162b2) contain dangerous lipid nanoparticles, among them, ALC-0159, which quickly spread the ingredients of this “vaccine” throughout the “vaccinated” person’s body, including to the brain, the intestines, and the pituitary gland. Three: COMIRNATY (and BNT162b2) contain the lab-created chemical, N1-Methylpseudouridine, which replaces the natural Uridine in the “vaccinated” person’s RNA. Four: Pfizer-BioNTech included N1-Methylpseudouridine in the formulation COMIRNATY (and BNT162b2) and stated this in the company’s Global Patent documentation for this “vaccine.” Five: Pfizer-BioNTech tacitly admitted that Gain-of-Function experiments were performed in the development of BNT162b2, per the Global Patent documentation for this “vaccine.” Six: Pfizer-BioNTech admitted that self-amplifying RNA (saRNA) can be used in COVID-19 “vaccines”, per the Global Patent documentation for this “vaccine.”
In addition, the following may be of interest: One: A blog article by Alex Swanson, M.S., on uridine, 30 November 2020; and, Two: The FLCCC protocol on recovering from COVID-19 “vaccination.”
The list of citations follows. Peace, Good Energy, Respect: PAVACA
[1]www.fda.gov/media/151707/download, Full Prescribing Information for COMIRNATYR (COVID-19 Vaccine, mRNA) suspension for injection, for intramuscular use 2024-2025 Formula
[5]https://doi.org/10.1101/2022.09.27.509633, Nuclear translocation of spike mRNA and protein is a novel pathogenic feature of SARS-CoV-2, Sarah Sattar, et al., 27 Sept. 2022
[9]https://pubmed.ncbi.nlm.nih.gov/32090264/, N1-Methylpseudouridine substitution enhances the performance of synthetic mRNA switches in cells, Callum JC Parr, et al., 6 Apr. 2020
[14]https://doi.org/10.1016/S1473-3099(21)00451-5, Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: a case series and nested case-control study, Eric Yuk Fai Wan, PhD, et al. 16 Aug. 2021
[18]https://doi.org/10.1101/2022.03.02.482639, Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System: human brain normal glial and glioma cells by Raman imaging, H. Abramczyk, et al., 2 Mar. 2022
[19]https://doi.org/10.1093/qjmed/hcae103, A potential association between COVID-19 vaccination and development of alzheimer’s disease, Jee Hoon Roh, et al., 28 May 2024
[22]https://doi.org/10.24869/psyd.2022.377, First Episode of Psychosis Following the COVID-19 Vaccination – A Case Series, Tonka Borodina, et al., 18 May 2022
[24]https://doi.org/10.3390/vaccines10101651, A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19, Michael Morz, 1 Oct. 2022
The above blurred image of persons attending a conference is courtesy of Google Images and Vecteezy.
Today’s Health Friday offering is one a of a series devoted to Big Pharma, vaccines, general health, and associated topics. The discussion is not limited to what is presented in today’s post: it is an Open Thread.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and other items that readers should be familiar with. They are all linked here.
This post will be diving into some “interesting” rabbit-holes. Stay with Yours Truly — I believe they are all interconnected. There is a General Summary at the end of the post.
Note: the scientific paper referred to by Dr. Nevradakis is here: www.preprints.org/manuscript/202406.0060/v1, “Proximal Origin of Epidemic Highly Pathogenic Avian Influenza H5N1 Clade 2.3.4.4b and Spread by Migratory Waterfowl”, Nicolas Hulscher, John Leake, Peter McCullough, 3 June 2024; click on “Download PDF” to read or save the paper. The authors suspect Gain-of-Function to be in play. Below is the Abstract of the paper:
Since this paper is a preprint; and, that it may be a target for Retraction; Withdrawal; or, Reissue with “new conclusions” that would reflect pressure on the paper’s authors and/or the publisher, Yours Truly suggests that interested readers download or make a hard copy of the preprint version.
The International Bird Flu Summit was held in Fairfax, Virginia, on 2 – 4 October 2024. This is the website for the “summit”: https://birdflusummit.com/. Here is the Brochure for the “summit”: https://birdflusummit.com/Bird Flu Summit Brochure.pdf. Reading through these “summit” websites, one gets the distinct impression of a general tone that “a Bird Flu pandemic” is about to occur; and, that various “interventions”, “command and control” methods, and “monitoring and dismantling” of “misinformation” detected on social media platforms, etc., will be “necessary” as part of a “coordinated response.”
Taking a look at the Brochure for the “Bird Flu Summit”, here is a portion of one of the “overview” pages:
Seems innocuous enough. However, moving on in the Brochure, one finds this:
And, further along in the Brochure, there is this:
Military involvement? “Inter-agency Communication and Resource Allocation”? What is “Seamless Response”?
John Leake, who works with Dr. Peter McCullough, attended this “summit.” Here is his take: https://petermcculloughmd.substack.com/p/at-the-bird-flu-summit, 2 October 2024. Yours Truly agrees with his impression that the speakers at the “summit” were “middle-of-the-road, rather than barn-burning experts” (my phrase.) One also agrees with the impression that the “summit” was all about “a Bird Flu pandemic being just around the corner.” However, this is NOT to minimize the potential for something like a “bird flu epidemic / pandemic” occurring — either from a “natural cause”: or, by another “lab leak.” Here is another view on the situation: www.theburningplatform.com/2024/09/22/could-bird-flu-be-the-october-surprise/, by Clayton J. Baker, MD.
FLASH! — The McCullough Foundation just got a demand from one of the speakers at the “Bird Flu Summit”, Syra Madad, PhD, to delete a video that John Leake and Nicolas Hulscher (another McCullough Foundation member) made of a Question-and-Answer session between Mr. Leake and herself at the “summit.” Dr. Madad is the coordinator of the upcoming New York City “Bird Flu Response Conference.” Please see here: https://petermcculloughmd.substack.com/p/mccullough-foundation-receives-bird, “McCullough Foundation Receives Bird Flu Summit Censorship Demand”, 9 October 2024. Below is a portion of the article:
The transcript of the video follows in the article (the video was deleted.) Below is a portion of the transcript, followed by an assessment by Mr. Leake:
Turning to the entity that “presented” the event (Ginkgo Biosecurity), and the entity that “produced” the event (SyllabusX): this is where the “rabbit holes” emerge; and, something that Yours Truly will call the Big Pharma-Government-Medical Complex (BPGMCTM) comes into the situation. Yours Truly defines BPGMC as an “interwoven cooperation” among Big Pharma, Federal government agencies regarding development / funding / support (including the Department of Defense), institutional investors, private investors, and “Establishment Medicine” (CDC, FDA, AMA, etc.)
First, the “producer” of the “Bird Flu Summit”, SyllabusX. The company’s address and phone number: 1900 Campus Commons Dr., Suite 100, Reston, VA 20191; phone number: 703.466.0011. The company was founded in 2017. SyllabusX has its “fingers in many pies” regarding producing conferences and other events on student safety and security, on technology for educators, on health and biosecurity, and more (https://syllabusx.com/home-2; and, https://syllabusx.com/about-us.) (Note: it is not easy to find information online about this company, especially as regards financials. A couple of sources that Yours Truly found: https://pitchbook.com/profiles/company/520513-39#overview; and, www.zoominfo.com/c/syllabusx-inc/480230653.) It appears that SyllabusX is a “privately-held company.”
The Chief Research Officer of SyllabusX is Ahmed Al Faraj (www.linkedin.com/in/ahmed-al-faraj; Note: this link may not work, unless the reader first joins LinkedIn.) And here’s where the issue gets, IMO, interesting. It appears that Mr. Faraj graduated with a B.S. in Economics from the University of Kansas School of Business in 2006. His languages are listed as, “Native or bilingual proficiency” in Arabic.
Before starting SyllabusX, Mr. Faraj previously worked for a company called New-Fields Exhibitions, headquartered in Dubai (https://inf.ae/.) While at New-Fields Exhibitions, Mr. Faraj held positions as Program Manager, Education & Public Health Group; and. as Program Manager, Defense Business Group. Below are two screenshots from the type of work he performed while at New-Fields Exhibitions:
Mr. Faraj also previously worked for a company called AdvanFort. He was the Chief Operating Officer of this company. AdvanFort is owned by a person called Samir Farajallah. His son, the then-Chief Operating Officer, was called Ahmed Farahjallah. AdvanFort is “a US private maritime security company”, per Wikipedia. The company was founded in 2007, and its headquarters office is in Herndon, VA (www.advanfort.com/.) A vessel owned by AdvanFort was involved in an international maritime incident in 2014. One of the stories that covers this incident is here: www,bbc.com/news/uk-england-34095843, 7 September 2015, “AdvanFort accused of abandoning British men facing India trial.” As a result of this incident, AdvanFort withdrew from membership in SAMI (the Security Association for the Maritime Industry): https://gcaptain.com/sami-responds-accusations-from-advanfort/, 2 April 2014. (Interested readers may want to compare the photo of Ahmed Faraj on the SyllabusX LinkedIn site, to the photo of Samir Farajallah and Ahmed Farajallah that is in the BBC article linked above. In one’s opinion, the “Ahmed” in these photos is the same person, with a perhaps 10-year gap between the photos. One has no objection to people wishing to change their names — this is simply an interesting item.)
It appears that Ginkgo BioWorks has quite a bit of funding. Below are screenshots from https://tracxn.com/:
And, some institutional funders:
The United States government is also funding the biosecurity arm of Ginkgo BioWorks:www.dfc.gov/media/press-releases/dfc-approves-11-billion-loan-ginkgo-bioworks-expand-its-commercial-biosecurity, “DFC Approves $1.1 Billion Loan to Ginkgo BioWorks to Expand its Commercial Biosecurity Business to Combat COVID-19 on a Global Scale”, 25 November 2020. DFC is the U.S. International Finance Development Corporation. Below is a screenshot from the article:
It would appear that Ginkgo BioWorks was involved in the “rapid deployment” of those PCR tests and antigen tests for COVID-19 at the start of the pandemic; and, also in the production of “two key raw materials for nucleic acid-based vaccines” (the modRNA COVID-19 “vaccines”.) Below is a blog post from April 2020 by Jason Kelly, another Ginkgo BioWorks co-founder, regarding the company’s partnership with Moderna in the production of the modRNA COVID-19 “vaccine”, mRNA-1273, along with other of that company’s mRNA “vaccines”:
Yours Truly has not, to date, found information as to the exact “raw materials” that Mr. Kelly is referring to.
Recall that the NIH/NIAID and Moderna co-developed mRNA-1273, co-own the patents of this modRNA COVID-19 “vaccine”, and share in the “royalty payments” for the sales and administration of this “vaccine” (and its “descendant clone” modRNA COVID-19 “vaccines.”)
Ginkgo BioWorks also “has its fingers in many pies”, including the bio-engineering of elements for gene therapy: www.ginkgobioworks.com/offerings/gene-therapy-services/. One such “service” is the bio-engineering of bacteria for treatment of diseases, such as cancer: www.ginkgobioworks.com/2023/01/09/engineering-bacteria-for-cancer-patient-treatment-with-prokarium/ (Prokarium is another “partner” with Ginkgo BioWorks.) The bacteria to be bio-engineered is a type of Salmonella bacteria, which will be used for “delivery of RNA payloads to treat cancer patients.” (Salmonella is “the most common form of food poisoning the in the U.S.”, according to the Cleveland Clinic. This brings up two questions: One, “Why is a bacteria related to food poisoning going to be used to treat cancer patients?”; and, Two, “How is this Salmonella bacteria going to be bio-engineered — is it going to be “sanitized” to be a beneficial element?”)
In Yours Truly’s opinion, Ginkgo BioWorks is a company to keep “on the radar.” It is acquiring other “partner companies” at a rapid rate. It is expanding its “services” into the gene-therapy sector. It is a “partner” with Moderna (and, therefore, by extension the NIH / NIAID.) In general, one has no objection to a company wishing to increase its profit margin and/or the number of its partner companies; at issue here are the following factors: the bio-engineering of DNA; the use of “automated tools” for engineering / manufacturing “raw materials” for gene-therapy treatments and/or “vaccines”; and the tie-in with the federal government.
General Summary: One: The International Bird Flu Summit was held in Fairfax, Virginia, earlier this month. The general tone of the “summit” was that a “bird flu epidemic / pandemic outbreak” is likely to occur, and soon. Two: The “summit” covered many topics related to epidemic / pandemic response, “command and control” methods, and how “seamlessly” federal, state and local governments and the military can “work together” in the response. Three: the “producer” of the “summit” was SyllabusX, a company that manages events ranging from student security to biosecurity to health education. SyllabusX is based in Virginia. Its Chief Research Officer is Ahmed Al-Faraj, who had previously (apparently) worked for his father’s company, AdvanFort, and (actually) for several other companies. Four: The “presenter” of the “summit” was Ginkgo Biosecurity (Ginkgo BioWorks), a company that offers “services” ranging from commercial biosecurity to bio-engineering to gene therapy research. This company, based in Massachusetts, has “deep funding” from many sources, including from the U.S. government. It has multiple “partners” in R&D, including Moderna. Ginko BioWorks was founded by students and scientists from MIT, including Tom Knight, the “godfather” of “DNA hacking” and of “synthetic biology.” Five: It appears that Ginkgo BioWorks, and, possibly, SyllabusX, are part of what may be called the Big Pharma-Government-Medical Complex (BPGMCTM), the “reach” of which runs far and wide.
Yours Truly will again emphasize the importance of having, and maintaining, the highest degree of health possible of the body’s natural immune system.
The above image of lab equipment is courtesy of Google Images and Public Domain Pictures.
Today’s offering for Health Friday concerns what is called self-amplifying RNA (saRNA.) As the presentation includes discussion of saRNA COVID-19 “vaccines”, this post is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
Readers already know about the Important Wolf Moon Notifications, the importance of Civil Discussion, the Rules of our late, good Wheatie, and the caveats regarding Health Friday posts by Yours Truly. Links to these items can be found here. NOTE: Since this post is detailed and there are multiple areas to cover, Yours Truly has added Summaries of certain sections, and a General Summary at the end.
Before one begins: It is well known that the modRNA and the viral vector COVID-19 “vaccines” currently in use have been, and are, a disaster on multiple fronts. Not only do they induce literally thousands of negative medical and psychological effects in the bodies of those who took them and who take them now; these “vaccines” also cause death. The numbers of COVID-19 “vaccinated” persons presenting with COVID-19 “vaccine”-induced illnesses, injuries, disabilities, or “died suddenly and unexpectedly” are increasing by the month. Nobody knows exactly how long, or in what amount, the elements and mechanisms of the COVID-19 “vaccines” work in the “vaccinated” person’s body: what IS known, is that whatever “protection” is conferred by these “vaccines” is short-lived, while, at the same time, the “vaccine” mechanisms linger on in the body for an indeterminate period of time. Yours Truly has written extensively for this board regarding this situation. For further information, please see websites such as these: https://kirschsubstack.com/ (Steve Kirsch); https://petermcculloughmd.substack.com/ (Peter McCullough, MD); and, https://phinancetechnologies.com/HumanityProjects/Projects.htm#Nav_ExcessDeaths (Ed Dowd, statistician.)
At the same time, the development of new types of COVID-19 “vaccines”, as well as new types of “vaccine delivery” (intranasal, oral, and aerosol, for examples) goes on apace. One of the “newest” types of COVID-19 “vaccines” uses what is called self-amplifying RNA, or saRNA.
The concept of saRNA is the use of a small amount of RNA (or mRNA) in an injectable. Once introduced into the body of the patient, the saRNA theoretically goes to work, “re-creating itself.” (Think RNA or mRNA being turned into a “Xerox copier” inside the “vaccinated” person’s body.) The “goal” of saRNA is for the agent to “re-create itself” inside the “vaccinated” person’s body for a certain amount of time and in some amount. The patient’s body is “instructed” by the saRNA to “recognize” and produce antibodies against certain “enemies”, such as viruses. The theory is that a smaller amount of saRNA initially introduced into the body, followed by the “Xerox copier effect”, then followed by “instructing” the body to “recognize” and fight off certain “enemies”, will make saRNA a “more effective use” of mRNA in injectables.
Basically,saRNA COVID-19 “vaccines” turn the “vaccinated” person’s body into a “Xerox copier” (which, apparently, the “vaccinated” person’s body CANNOT stop, slow down, or mitigate) for the ingredients (and, by extension, the mechanisms) of the saRNA “vaccine.” Today’s post is a primer about saRNA COVID-19 “vaccines.”
****** Summary: In other words, saRNA injectables **may**, at some point down the road, have **some** benefits. In the meantime — NONE of these types of injectables (GEMCOVAC, Kostaive) have been SUFFICIENTLY AND THOROUGHLY INVESTIGATED AND TESTED FOR USE ON HUMANS. But they are being approved ANYWAY, and are being injected into the bodies of unsuspecting persons who buy into the “Look, this shot has less mRNA than the ones you took before, and it’ll work better!” hype.
****** Look closely at the above graphic. It appears that the basic schema of saRNA is a “double-layer” of saRNA “replicons” that create a “subgenomic RNA.” This, in turn, creates the “Xerox copier” response which forces the body of the saRNA “vaccinated” person to endlessly produce immune system response— and for “at least” as long as 28 days after such “vaccination.”
Please see this paper regarding a discussion of saRNA “vaccine” design: https://doi.org/10.1016/j.tibtech.2023.05.007, “Rise of the RNA machines — self-amplification in RNA vaccine design”, Jerome D.G. Comes, et al., 14 June 2023. Below is the Abstract of this paper:
Note the language about “,…at least in theory” advantage of saRNA “vaccines.” Also note the last sentence — saRNA can “persist for a month.” In fact,nobody really knows how long saRNA elements will “persist” in the body of the person who takes this type of “vaccine” — NO long-term clinical trial or study has been performed using this technology.
On 28 November 2023, the Japanese Government approved the use of the saRNA COVID-19 “vaccine”, ARCT-154 (also called LUNAR-COVID-19 and Kostaive) for “active immunization” (translation: “prevention”) against COVID-19 for persons age 18 and older. Kostaive was developed by CSL / Arcturus (remember this company? Yours Truly took the lid off it here: www.theqtree.com/2024/08/02/the-hhs-gave-the-go-ahead-to-use-an-h5n1-vaccine-but-the-ama-just-issued-new-cpt-codes-for-an-h5n8-vaccine/.) This “vaccine” was to have supplies ready for administration by physicians or hospitals by mid-December 2023.
CSL / Arcturus, the Japanese government, and media outlets were quick to herald this “first-ever saRNA COVID-19 “vaccine.” Except — there already was an saRNA COVID-19 “vaccine” approved and in use, since 2022, in India: GEMCOVAC. Perhaps what CSL / Arcturus, the Japanese government, and media outlets should have mentioned the fact that Kostaive is modRNA-based from the J.1. Omicron SARS-CoV-2 variant (along with other “familiar” manufacturing methods, see below in today’s post); whereas GEMCOVAC based on an “ancestral variant” (in other words, the Beta variant) of the original Wuhan Hu1 SARS-CoV-2 virus.
Before Yours Truly presents information on Kostaive, she will first discuss GEMOCOVAC. This is in order to present further background information on saRNA technology as applied in COVID-19 “vaccines.” Stay with me — this is all germane to the situation:
Looking at GEMCOVAC, one can get the beginning of a picture of how saRNA COVID-19 “vaccines” work. The “latest version” of this “vaccine” is called GEMCOVAC-OM. Below is a portion of the SmPC pdf for this product (https://gemcovac.com; scroll down the page to GEMCOVAC-OM SmPC (pdf) and click “Download”):
The BA.1. Omicron variant of SARS-Co-V-2 is the basis for this “vaccine.” It is not strictly modRNA (however, recall that ALL of the “descendant variants” of the original Wuhan Hu1 SARS-CoV-2 virus contain elements of that original lab-created virus).
Of the excipients (in other words, the adjuvants): per Wikipedia, DOTAP (1,2-Dioleoyl-3-trimethylammonium propane) is a chemical used in fabric softeners, but also is used as a lipid nanoparticle in vaccines. Squalene: below is Page 1 of the FisherScientific MSDS Safety Data Sheet for this chemical (www.fishersci.com/):
Continuing: for polysorbate 80, again from Fisher Scientific, Page 1 of the MSDS Safety Data Sheet:
And, here is the Mechanism of Action for GEMCOVAC-OM, from the Package Insert (see the link above):
Note the language, “…which is reported to interact with host cells receptors (ACE-2.)” (Italics mine.) The developer and manufacturer (GENNOVA) of this “vaccine” can’t exactly quantify how the product works.
Yours Truly now turns to Kostaive, (ARCT-154) the saRNA COVID-19 “vaccine” that was approved by the Japanese government in November 2023.
Note the language in the above regarding “…the potential for extended duration of protection while using lower doses of mRNA compared to existing mRNA vaccines.” (Italics mine) Again, nobody knows exactly how long this “extended duration” period is; nobody knows exactly how much “Xerox copying” of the altered mRNA in Kostaive occurs during this period in the “vaccinated” person’s body; and, nobody knows exactly what effects this “Xerox copying” of the altered mRNA in Kostaive will have in the “vaccinated” person’s body. In other words, anyone who takes Kostaive, or any saRNA “vaccine”, in Yours Truly’s opinion, is being used a “human lab rat” — just as people were used / are still being used, as “human lab rats” for the modRNA COVID-19 “vaccines.”
And, here is the Report of the Deliberation Results (which contains the information about Kostaive that led to its approval) from the Japanese Ministry of Health, Labour, and Welfare: www.pmda.go.jp/files/000269813.pdf. This report is an interesting read. There are numerous “blacked-out” areas, reminding one of the blacked-out areas in certain publicly-released Pfizer-BioNTech reports that the company gave to the FDA regarding that company’s modRNA COVID-19 “vaccine” BNT162b2. HOWEVER, section 2.1 Active Substance for Kostaive states that this saRNA “vaccine” contains elements from the original Wuhan Hu1 SARS-CoV-2 virus, plus elements from the Omicron variant strain. More information on this is found on Page 4 of the document. Below is a portion of this page:
Looking at the above, starting with the D614G mutation, the Abstract from the Zhang, et al. paper on this (https://doi.org/10.1038/s41467-020-19808-4, “SARS-CoV-2 spike-protein D614G mutation increases virion spike density and infectivity”, Lizhou Zhang, et al., 26 November 2020. The paper was researched and published before any COVID-19 “vaccine” was authorized for use):
In other words, the D614G element causes the SARS-CoV-2 virus to be more infective.
Looking at V987P, part of the section Full-Length S Glycoprotein Vaccines from this paper: https://doi.org/10.3389/fimmu.2021/701501, “SARs-CoV-2 Vaccines Based on the Spike Glycoprotein and Implications of New Viral Variants”, Daniel Martinez-Flores, et al., 11 July 2021):
In other words, if V987P was “good enough” for Pfizer-BioNTech and for Moderna to use in their modRNA COVID-19 “vaccines”, it apparently was “good enough” to be used in Kostaive.
The K986P protein used in Kostaive: please see here: www.rcsb.org/structure/6zp1. This viral protein, along with V987P above, are BOTH on the Arg S1/S2 cleavage site on the SARS-CoV-2 virus genome. (FURIN CLEAVAGE SITE, anyone?)
The R682G, R683S, and R685S proteins used in Kostaive: please see here: https://doi.org/10.1038/s41467-022-32665-7, “Omicron SARS-CoV-2 mutations stabilize spike-up RBD conformation and lead to a non-RBM-binding monoclonal antibody escape”, Zhennan Zhao, et al., 24 August 2022. If appears that these proteins help to create a “one-RBD-up conformation.” Below is a portion of the Abstract of this paper:
In other words, these proteins increase the immune system attack from the Omicron SARS-CoV-2 variants by making Omicron “stick better” to the ACE2 receptor cells in the human body.
****** Summary: It appears, then, that Kostaive contains one protein from the original Wuhan Hu1 SARS-CoV-2 virus genome (D614G); two proteins from the “ancestral line” of the SARS-CoV-2 virus (K986P and V987P); and three proteins of the Omicron SARS-CoV-2 variant (R682G, R683S, and R685S.) See below in the post for more information on these items.
One more ingredient of Kostaive, mRNA-2105: This ingredient is derived from the Venezuelan Equine Encephalitis virus (VEEV.) Below is section 4.R.1. of the Deliberations Results document discussing this:
The question that immediately occurs regarding the above: How can Arcturus (the manufacturer of Kostaive) state that mRNA-2105 cannot be “incorporated into host cell DNA”? How is Arcturus absolutely sure that there is zero reverse transcription potential or ability in Kostaive? This is similar to the same statements from Pfizer-BioNTech about BNT162b2 “cannot change the DNA of the vaccinated individual” — which has been proven to be false (please see: here, Slide 14.)
****** Summary of the above: What Yours Truly is getting at here is that Kostaive appears to be the end-product of: ONE: a lab-created mixture of the dangerous D614G element from the original Wuhan Hu1 SARS-CoV-2 virus, plus, various elements of earlier SARS-CoV-2 mutations; TWO: NO long-term clinical trials, NO safety studies for Toxicity, use on pregnant women, etc.; THREE: the “Process 2”-type manufacturing method (“culturing” the lab-enhanced mRNA for the “vaccine” in a “bath” of E. coli); FOUR: using lipid nanoparticles, one of which (ATX-126) has never been used before in an injectable); FIVE: what appears to be a “pro-forma” Deliberation Results document on Kostaive that raises more questions than it answers; and, SIX: approval by the Japanese government for use on humans without a thorough investigation of the above. Related to point SIX: below is the list of Approval Conditions that were imposed along the approval of Kostaive for use in Japan, from the Deliberations Results document:
By the way, these Approval Conditions read very much like the ones that the FDA imposed on Pfizer-BioNTech along with that agency’s EUA for BNT162b2.
Regarding Kostaive itself, more particulars:
The ingredients of Kostaive are listed in section 2.2 Vaccine Product of the report. A screenshot of this section is below:
Kostaive contains at least three separate types of LNPs (lipid nanoparticles): ATX-126; DSPC; and, PEG2000-DMG. Below is a portion of the MSDS Safety Data Sheet for ATX-126:
Section 2.2.3 of the Deliberation Results document for Kostaive discusses the manufacturing process for Kostaive. It appears that Kostaive ALSO “switched” from a “Process A” manufacturing method over to a “Process B” manufacturing method. (Recall that the Pfizer-BioNTech BNT162b2 was “switched” from its “Process 1” manufacturing method over to a “Process 2” manufacturing method):
One more item from the Deliberation Results document for Kostaive, again on the ATX-126 lipid nanoparticle used in this “vaccine.” It confirms that this “novel excipient” (adjuvant) has not been used before in a “vaccine.”
Yours Truly will again emphasize that other sections of the DeliberationResults document on Kostaive make it clear that NO studies were performed for numerous items, such as Toxicity, potential for impairment of reproduction, and so on. By the way, buried in the document is a “passing reference mention” that the “Process B” manufacturing method for this “vaccine” uses E. coli as the “culturing medium” for the “enhanced” mRNA in the product. (The “Process 2” manufacturing method for BNT162b2 and its “descendant” COVID-19 “vaccines” also uses E. coli.) It also appears that the use of Kostaive on pregnant women in clinical trials was “inconclusive”; this “vaccine” should be taken by pregnant women only if the situation so warrants.
Also: Kostaive is to be taken as a “primary series” of two separate injections, 28 days apart; with a “booster” taken about three months later. The question that arises is: If it is true that the saRNA in Kostaive is active, including installing numberless “Xerox copiers” of itself in the “vaccinated” person’s body for AT LEAST 28 days AFTER the initial injection, WHY is there a need for ANOTHER injection around Day 28? And a “booster” after that?
******BUT — AND THIS IS A HUGE BUT — TAKE ANOTHER LOOK AT SECTION 2.2.1 OF THE DELIBERATION RESULTS DOCUMENT FOR KOSTAIVE:
Look at the “active ingredient” item, “zapomeran.” What is zapomeran? It is a “drug” that contains the RNA of the Venezuelan Equine Encephalitis Virus (VEEV or VEE) in an saRNA form. It is ALSO manufactured by ARCTURUS (CSL.) It is unclear if it is being used in other types of COVID-19 “vaccines” other than Kostaive. Please see: https://synapse.patsnap.com/drug/510bcf7ef75649278b284a94663c69f6. Scroll down the page to R&D Status to see that zapomeran has already been approved in the EU; Norway; Iceland; and Liechtenstein; but in what final form it is used, is also unclear. NOTE 1: It has been impossible to find a complete list of ingredients for zapomeran. One would not be surprised to learn that the names Kostaive and zapomeran may, in some respects, be “interchangeable.” NOTE 2: It is not easy to find information on zapomeran. Yours Truly has encountered “504 Bad Gateway” error messages when going back to recheck a couple of the links to zapomeran in this post.
Looking further into VEEV (or VEE), there is this article: https://ceh.vetmed.ucdavis.edu/health-topics/venezuelan-equine-encephalitis-vee, by Amy Young, 28 August 2020. This virus can affect horses, donkeys, or zebras. VEEV is transmitted to these animals by infected mosquitos that bite them. It can cause severe disease or death by infecting the brain and the central nervous system. Humans who contract VEEV can also become severely ill and can also die from it. Another paper, discussing the RNA of VEEV (VEE),by Sarah E. Hickson and Jennifer L. Hyde, is here.
****** VERY IMPORTANT:The SARS-CoV-2 spike proteins in zapomeran are the same ones that are in Kostaive. These were discussed above in the post. Turning to the nsP proteins (non-structural proteins) in zapomeran (hyperlinks to papers are embedded), as these elements are also apparently contained in Kostaive:
****** SUMMARY:IT APPEARS, THEN, THAT KOSTAIVE CONTAINS ZAPOMERAN, WHICH INCLUDES THE VENEZUELAN EQUINE ENCEPHALITIS RNA; PLUS, SIX LAB-ENHANCED/LAB-ISOLATED GENOME CODES OF SARS-CoV-2; AND, FOUR NON-STRUCTURAL PROTEINS, ONE OF WHICH IS A ROTAVIRUS TOXIN. KOSTAIVE ALSO CONTAINS DANGEROUS LIPID NANOPARTICLES (SUCH AS ATX-126.) THESE ARE ALL PRESENT IN THIS saRNA COVID-19 “VACCINE” PRODUCT. RECALL THAT LIPID NANOPARTICLES WILL HELP TO SPREAD A “VACCINE” THROUGHOUT THE ‘VACCINATED” PERSON’S BODY, INCLUDING CROSSING THE BLOOD-BRAIN BARRIER.
Why on Earth is a COVID-19 “vaccine” that contains the RNA of an equine brain inflammation virus (a virus that comes from infected mosquitos that bite equine animals) being used on humans? A “vaccine” that is engineered to create an unknown number of “Xerox copiers” of the “vaccine” elements into the body of the “vaccinated” person? A “vaccine” that contains six apparently lab-enhanced/lab-isolated genome codes from the SARS-CoV-2 virus or its variants? What does an equine brain inflammation virus have in common with SARS-CoV-2? What if a person who has already taken, say, five or six injections of a modRNA COVID-19 “vaccine” decides to take Kostaive? Could an saRNA COVID-19 “vaccine” somehow “interact” with the modRNA COVID-19 “vaccine” elements already in that person’s body?
****** GENERAL SUMMARY: saRNA “vaccines” for COVID-19 are already being used (GEMCOVAC in India); and are being approved for use (Kostaive in Japan.) The technology for saRNA is not fully developed and not fully tested; the COVID-19 “vaccines” that use saRNA contain “lab-enhanced”/”lab-isolated” genome codes of the SARS-CoV-2 virus or its variants; saRNA COVID-19 “vaccines” contain lipid nanoparticles — and, in the case of Kostaive, an LNP (ATX-126) that has never been used before in an injectable; that no studies have been performed on saRNA COVID-19 “vaccines” regarding Toxicity, the effects on reproductive potential, and so on; and, that Kostaive contains the RNA of the Venezuelan Equine Encephalitis Virus. And yet, these products are being hailed as “the vaccines of the future.” And, the people taking them are again being used as “human lab rats.”