“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
This is a very open-ended post. The goal is to get YOUR thoughts, opinions, and theories.
Without getting too deep, I can tell you that we are seeing a LOT of COVID in my world. It seems to be everywhere. But some apparent attempts to get masks going again are fizzling out fast, thank goodness.
So I’m curious what others are seeing. But beyond that, we’ve had almost 5 years of COVID in this world – maybe more.
Time for reassessment – particularly prior to the election.
Time for some fresh ground reports.
What think you about COVID?
Tell us what you’re seeing and thinking, please!!!
This post is part of Health Friday, a series of offerings related to Big Pharma, vaccines, general health, and associated topics. However, the discussion will not be limited to what is presented today; it is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here. “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
What Yours Truly presents in this series, as in her previous blog posts for this board, is not medical advice — they are based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to please consult a healthcare practitioner regarding health concerns or conditions.
Today’s post in the Health Friday series regards the ongoing efforts by what Yours Truly calls Establishment Medicine to minimize, marginalize, and/or outright punish those healthcare professionals (especially physicians) who speak the truth about the COVID-19 virus itself and the COVID-19 “vaccines.”
For purposes of the post today, Yours Truly begins here: ABIM: “Follow the consensus, not the science. Saving lives is not a priority.”, from The Burning Platform, a post by Steve Kirsch. This details the American Board of Internal Medicine revoking the certifications of Dr. Pierre Kory and Dr. Paul Marik. The Washington Post and other media outlets gloated over this, trumpeting that the “medical disinformation spread” by these physicians (such as, that Ivermectin and Hydroxychloroquine can prevent and cure COVID-19 infections; and, that the modRNA COVID-19 “vaccines” are dangerous) was finished. Yours Truly’s presentation focuses on the ABIM decision regarding Dr. Kory.
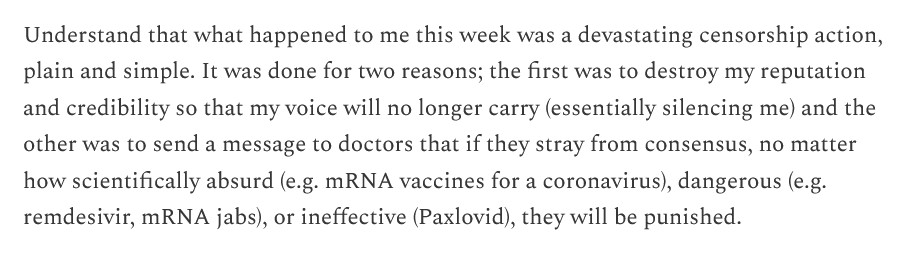
Dr. Pierre Kory is a co-founder of COVID-19 Critical Care (FLCCC): https://covid19criticalcare.com/. He has been, and is, since the beginning of the disaster of COVID-19 and the COVID-19 “vaccines”, a leading voice in exposing the truth of this situation, along with being a champion of using Ivermectin and Hydroxychloroquine to prevent a COVID-19 infection and to treat COVID-19 infected patients. Until this month, Dr. Kory held three board certifications from the American Board of Internal Medicine — until this happened: The American Board of Internal Medicine Revoked All 3 of My Board Certifications, 17 August 2024. This is a big deal. Here’s why: By this action, the American Board of Internal Medicine (ABIM) removed Dr. Kory’s ability to have hospital privileges; it removed his ability to hold an academic position; and, it removed his ability to work in a medical clinic or other facility where other physicians hold ABIM certifications. Dr. Kory can still practice medicine in a private clinic where there no ABIM physicians; or, he can work independently in a clinic that he himself establishes. Below are three screenshots from Dr. Kory’s article:
Note the above third screenshot. To remove the ability of physicians to “think out of the box” will be, in Yours Truly’s opinion, to implement “one-size-fits-all Establishment Medicine.” And this is not all — this approach will (if it hasn’t already) spill over into the CMS (Medicare / Medicaid) system, making it almost impossible for persons covered under this system to find physicians who want to “think out of the box.”
The history of medical board certification in the United States began in 1917. A brief history can be found here: www.ncbi.nim.nih.gov/pmc/articles/PMC2394686/, “Professionalism and Accountability: The Role of Specialty Board Certification”, by Christine K. Cassell, MD, and Eric S. Holmhoe, MD, 2008. There are multiple entities that grant board certifications to physicians. Two of them are: the American Board of Medical Specialties (ABMS) www.abms.org/, which grants certifications in 40 specialties and 89 “sub-specialties”; and, the American Board of Internal Medicine (ABIM) www.abim.org/, which grants certifications in 14 specialties. In essence, board certification, which was at one time was an “add-on” to a physician’s already-established reputation and expertise is now anecessity — there is hardly a hospital, or a medical school, or a group practice that will consider hiring a physician who does not have a board certification, or is not working toward one. And, with the advent of “get board certified or forget about being hired”, comes what Yours Truly will call “the potential tyranny” of the granting entity over the physician who is board certified. There is continuing education and exams to renew the certifications; all of these cost money. There is “oversight” on the physician who obtains board certification — for example, are there any complaints from patients? Does the physician “spread misinformation” about things like the COVID-19 “vaccines” and/or “unapproved treatments” for COVID-19 infection? The granting entity can “charge” a physician who has board certification with “spreading misinformation” and/or “treating a patient with unapproved drugs”; the physician has to “defend” themself before the granting board in order to keep or to renew their certification(s). The granting entity has the sole power to either renew or to revoke the physician’s certification(s).
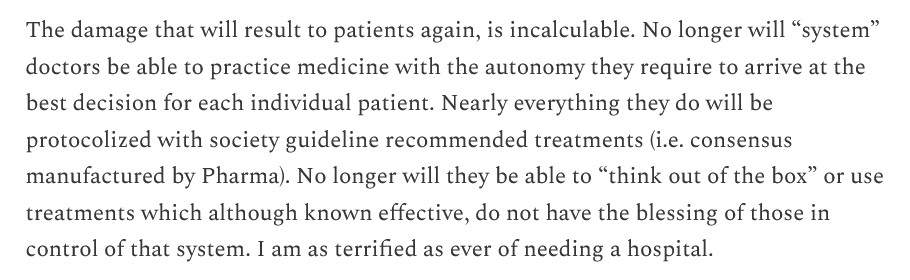
An opposite point of view on board certification is expressed here: Is Board Certification Overrated?, by Robert Anthony, 2010 (copyright 2010 by UBM). Below is a portion of the article:
Which appears, in Yours Truly’s opinion, to imply that a physician who is not board certified is somehow “lacking” in skills and knowledge and, perhaps, does not “meet a higher standard.”
Perhaps the most damning statement by Dr. Kory regarding the ABIM revoking his board credentials is this one, from his blog article referred to above:
Read the above again. The ABIM has removed Dr. Kory’s ability to see patients in a hospital. He can’t participate in insurance plans — which means that any patient he sees in his own clinic must pay for all services, tests, and so on, out of pocket. This may include charges that would normally be covered by Medicare / Medicaid. He will have to carry less medical malpractice insurance. All of these can potentially mean that patients who need his services but cannot pay cash for them, are also potentially shut out from his services. His article above needs to be read: in it, he “exposes the underbelly” of the ABIM.
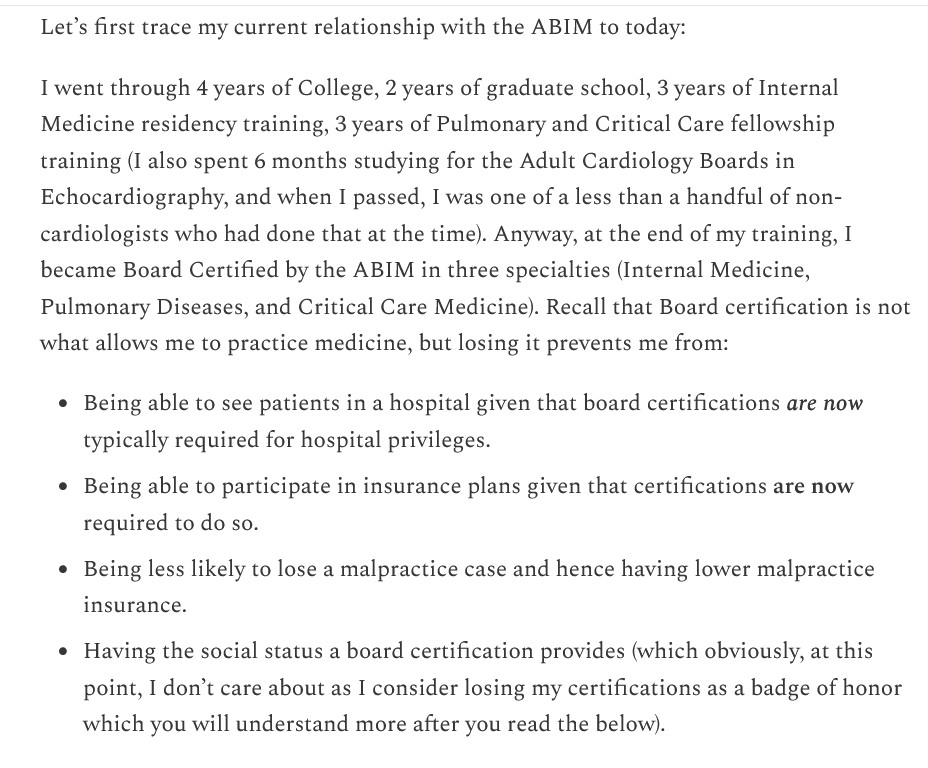
Dr. Meryl Nass (https://merylnass.substack.com/) also had her board certification revoked by the ABIM. The organization did not even bother to tell her that this was done: https://merylnass.substack.com/p/kory-and-marik-were-just-stripped, “Kory and Marik were just stripped of their specialty board certifications. So was I, but the ABIM never even bothered to tell me”, 14 August 2024. Dr. Nass also, in another blog post, reveals what may one item behind what the ABIM is doing — the organization apparently wants to replace the physicians whose certifications were revoked with medical doctors from foreign countries: https://merylnass.substack.com/p/after-stripping-doctors-of-their, “After stripping doctors of their credentials and making it impossible to practice ethical medicine, the ABIM wants to bring in foreign medical doctors as replacements”, 24 August 2024. Below is a JPG of the ABIM’s statement, shared by Dr. Nass from another physician:
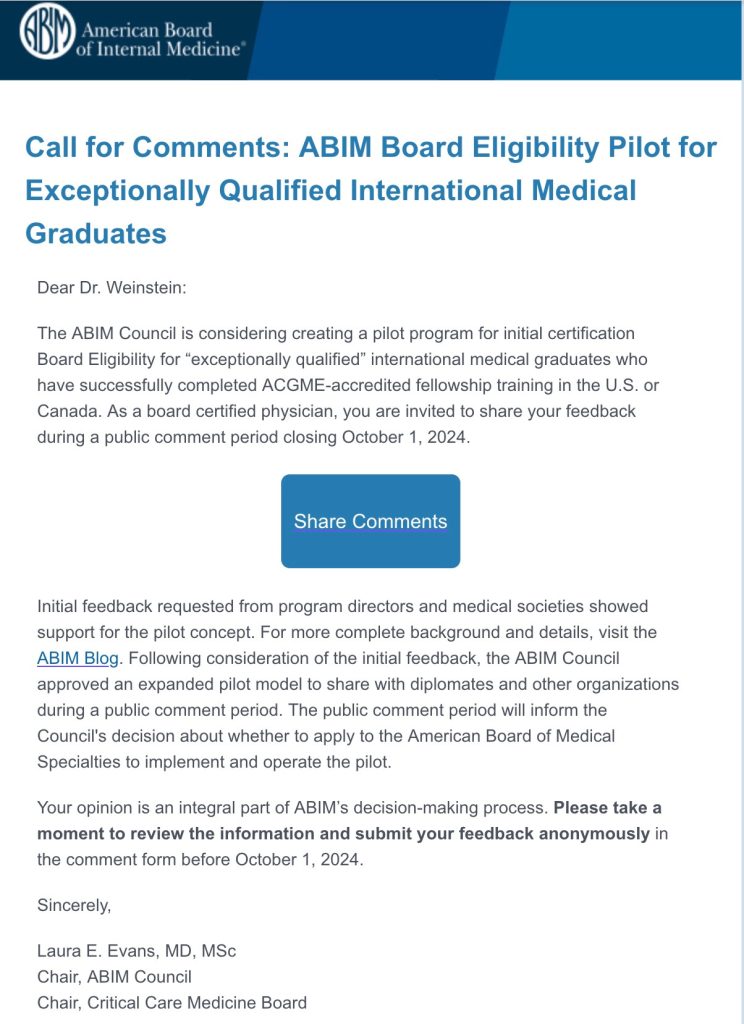
To add another aspect to the discussion, Yours Truly believes there ** may ** be some involvement of the AMA (American Medical Association) in the revoking of board certifications: AMA adopts new policy aimed at addressing public health disinformation, 13 June 2022. Below is a screenshot from the press release:
Note the penultimate point regarding “specialty boards.” In Yours Truly’s opinion, the AMA is one of the bastions of what may be called “Establishment Medicine” (the others being entities such as: the CDC; the FDA; the medical schools of Harvard University, Stanford University, Cornell University, etc.)
Let’s say that a board-certified physician, “fully vaccinated and boosted” who “followed the science”, after watching “vaccinated and boosted” patients, colleagues, perhaps even family members, begin to present with “the doctors are baffled” medical issues; or, perhaps, a cancer that was in remission that has returned. Let’s say that this physician starts to feel a little uneasy regarding the modRNA COVID-19 “vaccines” and does a little research — perhaps, by reading a blog or two written by someone like Dr. Kory; perhaps, by reading some published scientific literature regarding “first onset of psychosis after SARS-CoV-2 vaccination” (there are multiple papers discussing this that can be found online.) Let’s say that this physician comes to the realization that the modRNA COVID-19 “vaccines” are not “safe and effective”, but instead are the opposite. Let’s say this physician has board-certification renewal coming up in a few months. And, to top it off, let’s say that this physician has a family to provide for, a mortgage to pay, and medical school debt to pay off. What is this physician to do? — without jeopardizing the job, the board certification, perhaps even the License to Practice Medicine? It is Yours Truly’s opinion that this kind of situation is starting to “bubble under the surface” of more than one physician currently in practice. It is not an easy situation to be in.
Where does this situation leave the patient? If the physician who discovers that the modRNA COVID-19 “vaccines” (actually, gene therapy and modification injections [the DNA of the “vaccinated” person is changed by the ingredients and mechanisms of these “vaccines”]) are ineffective and dangerous, but doesn’t / can’t say a word to the patient to not take them — doesn’t this violate the oath of “First, Do No Harm” that the physician swore upon receiving the degree of Doctor of Medicine? If the physician who finds out, for example, that Paxlovid has a high “rebound infection” percentage, but doesn’t / can’t say a word to the patient to not take this combo-drug but substitute, say, Hydroxychloroquine, Zinc, and Vitamin D to combat a COVID infection — doesn’t this silence put the patient at risk? One in Five Experience Rebound COVID After Antiviral Drug, New Study Shows, 13 November 2023. The article regarding the DNA change made by the modRNA COVID-19 “vaccines” is here: https://doctors4covidethics.com/wp-content/uploads/2022/08/causality-article. “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, by Michael Palmer, MD, and Sucharit Bhakdi, MD, 18 August 2022. Slide 14 of this article is a graphic showing how the DNA of the COVID-19 “vaccinated” person is changed by the Pfizer-BioNTech modRNA COVID-19 “vaccine.”
How did the ABIM, the ABMS, and the other privately-run board certification granting entities in the United States come to have such power over the practice of medicine and over the physicians who obtain board certification? (There are literally dozens of these boards: www.americanboardcosmeticsurgery.org/so-what-does-physician-board-certification-actually-mean/, 7 February 2019.) To Yours Truly, it appears that they possibly used a combination of influence, lobbying, personal connections with medical schools, and other “tactics.” The result may well be an “authority” that these certification boards created and arrogatedto themselves, in the name of “ensuring quality delivery of healthcare by qualified physicians.” While this may have been a true and worthy aspiration previously, it seems it has “evolved” into “Follow these dictates, or else.”
And, from there, where does this potentially go? If a physician is stripped of board certification(s), that physician can still practice medicine — unless their state medical licensing board (perhaps with the involvement of the AMA, please see above in today’s post) decides to “charge” the physician with “spreading disinformation to the public” in “violation” of the diktats of Establishment Medicine. The physician now faces the possibility of losing the License to Practice Medicine. The case of Dr. Carrie Madej, DO, comes to mind. (Doctors of Osteopathy are medical doctors who have somewhat different training from MDs, but who are recognized and licensed to practice medicine and write prescriptions.) She was brought up on similar “charges” by the medical licensing board of Georgia. After a protracted fight, Dr. Madej ultimately decided to surrender her License to Practice Medicine in 2023. (Recall that Dr. Madej was one of the first to demonstrate that the modRNA COVID-19 “vaccines” contain substances that appeared to be strange.)
And, from there, where does the potential for innovation in medicine go? If physicians (especially board-certified physicians) have to, in effect, constantly “look over their shoulder” and “toe the line” to Establishment Medicine, doesn’t this affect the potential to come up with new theories and to investigate them? — such as in, using drugs in “off-label” circumstances to help patients? — such as in, using Hydroxychloroquine to prevent or treat COVID-19 infection, instead of injecting a patient with a modRNA COVID-19 “vaccine” that changes that patient’s DNA and can also lead to the appearance of myocarditis or even to the death of the patient? Instead of hospitalized COVID-19 infected patients being put on ventilators and given Remdesivir, a drug that can kill the patient instead of helping the patient? Why Remdesivir Failed: Preclinical Assumptions Overestimate the Clinical Efficacy of Remdesivir for COVID-19 and Ebola, Victoria C. Yan and Florian L. Muller, 17 September 2021.
Yours Truly will say it is vitally important that all persons, COVID-19 “vaccinated” or not, to have and keep their natural immune system in the best condition possible; to become educated regarding any prescription medication that they take; and, to research any medical injectables that are recommended / required that they be given.
“For you shall know the truth, and the truth shall make you free.” John 8:32
The above image of a physician performing a vaccination is courtesy of Google Images and The New York Times.
This post is the first of “Health Friday”, a new series of offerings related to Big Pharma, vaccines, general health, and related topics. It is an honor and privilege to contribute this series to the board. Since today’s post relates to COVID-19 and the COVID-19 “vaccines”, it is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023. However, the discussion will not be limited to what is presented today; it is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here. “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
What Yours Truly writes in this series, as in her previous blog posts for this board, is not medical advice — they are opinions based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to please consult a healthcare practitioner regarding health concerns or conditions.
And now, to dive in. There is a lot to “unpack.”
The modRNA COVID-19 “vaccines” induce IgG4-related disease (IgG4-RD.)IgG4-related disease(IgG4-RD) is a term that covers multiple medical conditions, ranging from neurological to ocular to cardiovascular to respiratory to gastrointestinal to urogenital. Since it is a chronic inflammatory condition, there can be more than one location of an IgG4-RD associated ailment within the patient’s body. Please see: https://en.wikipedia.org/wiki/IgG4-related_disease, “IgG4-related disease”, which has a list of symptoms in reported cases of IgG4-RD, and a list of body area sites that can be affected by IgG4-RD. The first instance of what is now called IgG4-RD was discovered in 1892 by Johann von Mikulicz, who diagnosed an “inflammatory disease of the salivary glands” in a patient (this condition was later called Mikulicz’ disease.) In 2021, Hamano et al. found elevated IgG4 levels in patients with Autoimmune Pancreatitis (AIP.) Please see: https://ojrd.biomedicalcentral.com/articles/10.1186/s13023-014-0110-z, “IgG4-related disease: an orphan disease with many faces”, Herwig Pieringer, et al., 16 July 2014. It appears that an issue with obtaining a true diagnosis of an IgG4-related disease is that many of the presenting elements can “mimic” other conditions, such as cancer or non-Hodgkin’s lymphoma. In addition, IgG4-RD can simply not present symptoms at all, until the patient concludes that “something is going on here.” In terms of the presenting symptoms of an IgG4-RD disease, there are, among others: storiform fibrosis (“spindle-shaped” cells that can, with collagen fibers, form a “flowing arrangement”); and, eosinophilia (high elevation of a type of white blood cell [eosinophils] that supports the natural immune system.) Please see: https://academic.oup.com/mr/article/31/3/529/6300281, “The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD”, Hisamori Umehara, et al., 4 May 2021. (Note: the entire article is restricted access.) Below is a portion from “IgG4-Related Disease” from StatPearls – NCBI Bookshelf, an article by Sudheer Nambiar and Tony I. Oliver (www.ncbi.nlm.nih.gov/books/NBK499825):
There are some IgG4-RD conditions that may be genetically-based; one example is Autoimmune Pancreatitis (AIP.) Please see: https://pubmed.ncbi.nlm.nih.gov/31104539/, “Genetic analysis of IgG4-related disease”, Yuki Ishikawa and Chikashi Terao, 7 June 2020. (Note: again, the entire article is restricted-access.) On the other hand, another IgG4-RD condition, Autoimmune Lymphoproliferative Syndrome (ALPS) appears to strike children. In addition, IgG4-RD conditions can be “immune-mediated” (meaning, the body’s immune system response is either inappropriate or excessive); and/or “autoimmune” (meaning, the body’s immune system attacks healthy tissues in the body.)
Yours Truly will examine the presence of eosinophilia as an indicator of IgG4-RD. This is an important “marker.” And it ties into the modRNA COVID-19 “vaccines” — the COVID-19 “vaccinated” person’s natural immune system being damaged and/or destroyed by the ingredients and mechanisms of these “vaccines”; and, with repeated injections of these “vaccines” compounding this damage and/or destruction.
The first item is a blog article by Dr. Jessica Rose, PhD: https://jessicar.substack.com/p/igg4-related-disease-and-igg4-means, “IgG4-related disease (IgG4RD) means FIBROSIS and organ destruction”, 28 December 2022. It is now known that the modRNA COVID-19 “vaccines” induce a “class switch” in the COVID-19 “vaccinated” person’s natural immune system; this “class switch” is the damage and/or destruction of IgG3 immune system cells (these cells help to fight off infections and other enemies that “invade” the natural immune system), replacing IgG3 cells with increased numbers of IgG4 cells (these cells help to allow the body to “tolerate” assaults to the natural immune system.) Repeated injections of modRNA COVID-19 “vaccines” exacerbate this process: please see https://doi.org/10.1126/sciimmunol.ade2798, “Class switch toward non inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination”, Irrgang P, et al., 22 December 2022. Notice the title: “non inflammatory”, “spike-specific”, “IgG4”, and “repeated SARS CoV-2 mRNA vaccination.” IgG4-RD conditions can present as non-inflammatory (the patient doesn’t notice anything wrong for some period of time, see above in today’s post); however, the IgG4 levels in the patient are high upon examination. Below is a portion of the Introduction of the above paper. Note: Comirnaty was the non-United States version of the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2. Comirnaty and BNT162b2 are the same product. Note 2: the 2023-2024 Comirnaty modRNA COVID-19 “vaccine” was given full FDA approval for use in the United States on 23 September 2023 for persons age 12 above: www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-receive-us-fda-approval-2023-2024-covid; the version that the FDA authorized (the “2023-2024 Formula COVID-19 Vaccine” by the same company) was for persons age 6 months through 11 years of age (www.fda.gov/media/167211/download.)
Note that the IgG4 cell increase extended for months after the second injection of Comirnaty and was further increased after the third injection. This correlates to the original “two-injection Primary Series” plus the original “booster shot” of Comirnaty that millions of persons took between December 2020 and early 2022. This would also include, since the formulations were the same, of the “Primary Series” and the original “booster shot” of BNT162b2 that were taken by millions of persons in the United States from December 2020, until Comirnaty was given full FDA approval in the United States on 8 July 2022 for persons age 12 and older (at which point, BNT162b2 was “replaced” by Comirnaty except for use in persons age 6 months to 11 years; the FDA authorized the “Pfizer-BioNTech COVID-19 Vaccine” for this age group.) This “product name situation” may seem a little confusing: at bottom, it had to with removal of liability for the “vaccine” manufacturer. This will be discussed at a later date.) Note also that “VOC” means Variants of Concern (in other words, the Delta, the Omicron, the XBB.1.5 variants of the SARS-CoV-2 [COVID-19] virus, and so on.)
The second item is here: www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021, given by Pfizer-BioNTech to the FDA on 30 April 2021. This report covers Adverse Event Reports that were submitted to the company between 11 December 2020 (the date on which the FDA in the United States granted the initial Emergency Use Authorization (EUA) for BNT162b2 to be used in the United States, 21 December 2020 (the date on which the EMA (European Medicines Agency) granted its initial EUA for BNT162b2 to be used in Europe / Scandinavia; and, 28 February 2021. The APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST, which begins on Page 30 of this report, lists over 1,200 different types of medical adverse events that were reported to Pfizer-BioNTech from the worldwide EUA start dates above. On Page 3 and Page 4 of the APPENDIX 1. (Page 32 and Page 33 of the report), there are the following Adverse Events of Special Interest listed: Eosinopenia; Eosinophilic fasciitis; Eosinophilic granulomatosis with polyangiitis; Eosinophilic oesophagitis. On Page 5 of the APPENDIX 1. (Page 34) of the report, there is listed: Immunoglobulin G4 related disease. On Page 8 of the APPENDIX 1. (Page 37 of the report) there is listed: Sjogren’s syndrome (another type of IgG4-RD.) These are a few of the IgG4-RD types of reports that are listed in the APPENDIX 1. section. Thus, the FDA knew, on 30 April 2021, that BNT162b2 “vaccination” induces IgG4-related disease conditions. Yet, the FDA did nothing to stop the continuing rollout of BNT162b2.
A third item is here: https://mole.substack.com/cp/147758416, a 15 August 2024 cross-post from Lioness of Judah Ministry, “German Study Links Covid Shots to Surge in VITAL ORGAN DAMAGE among Children”. The study found that there was a large increase of organ damage induced by BNT162b2 in children in Germany ages 5 to 11 years old. The study is here: https://journals.lww.com/pidj/fulltext/9900/delayed_induction_of_noninflammatory_sars_cov_2.959.aspx, “Delayed Induction of Noninflammatory SARS-CoV-2 Spike-Specific IgG4 Antibodies Detected 1 Year After BNT162b2 Vaccination in Children”. Kobbe, Robin MD, et al., 30 July 2024. The IgG4 antibodies were detected after the second dose of BNT162b2 (in other words, after the “Primary Series” of two BNT162b2 injections was completed.)
And, a fourth item is here, related to COVID-19, the COVID-19 “vaccines” and autoimmune conditions: https://wmcresearch.substack.com/p/long-covid-is-an-autoimmune-disease, “Long COVID is an Autoimmune Disease: Injecting Mice with IgG from Long COVID Patients Induces Symptomology”, by Walter M Chesnut, 4 June 2024. Mr. Chesnut has long posited that the spike protein of the COVID-19 virus itself contains elements that attack the natural immune system of the body of a person infected with this virus; and that the COVID-19 virus itself can induce what is now called “Long COVID.” Yours Truly will add the opinion that the difference between “Long COVID” in a person who is “unvaccinated” against COVID-19, and “Long COVID” in a COVID-19 “vaccinated” person, is this: the natural immune system of the “unvaccinated” person still has the potential to not only fight off a COVID-19 infection, but also to mitigate or eliminate the chance that “Long COVID” may result from the infection; whereas, the natural immune system of the COVID-19 “vaccinated” person has been damaged (or worse), resulting in a much larger potential for “Long COVID” (both in presentation and in duration.)
Yours Truly believes that the COVID-19 virus itself, and the ingredients and mechanisms of the modRNA COVID-19 “vaccines” (one of these ingredients being a “lab-modified” form of the RNA of said virus), both attack the natural immune system of the body. The COVID-19 “vaccines” have been shown to damage and/or destroy the IgG3 cells of the body’s natural immune system (these cells help to fight off viruses, etc.), replacing these with increased amounts of IgG4 cells (“toleration facilitator” cells.) In Yours Truly’s opinion, one of the important details here is the targeting of HLA cells (human leukocyte antigen cells, a type of white blood cells) by the COVID-19 virus itself, and, by extension, the COVID-19 “vaccines.”
And, from this paper: www.ncbi.nlm.nih.gov/pmc/articles/PMC10864075, “HLA-DRB1 Is Associated with Therapeutic Responsiveness in IgG4-related disease”, Motohisa Yamamoto, et al., 23 May 2024:
Note that one of the most-recommended and used treatments for IgG4-RD conditions is glucocorticoids (steroids); and that cessation of treatment likely results in relapse of the condition. But, long-term use of glucocorticoids have risks, including high blood pressure and Cushing’s Disease. Please see: www.webmd.com/multiple-sclerosis/what-are-glucocorticoids.
Yours Truly will posit that the lab-created SARS-CoV-2 (COVID-19) virus itself, with the lab enhancements made to the mRNA of this virus to create the modRNA of the COVID-19 “vaccines” (such as the SV40 African Green Monkey cancer promoter gene piece in BNT162b2), plus the addition of dangerous lipid nanoparticles (ALC-0159 and ALC-0315 in BNT162b2 and its “descendant” COVID-19 “vaccines”; and, SM-102 in the Moderna mRNA-1273 modRNA COVID-19 “vaccines” and its “descendant” COVID-19 “vaccines”) and other ingredients in these “vaccines” — have been, and continue to be, designed to wreak as much havoc and damage on the human race as possible. This havoc and damage includes that done to the body’s natural immune system, its elements, mechanisms, and responses. Recall that the “descendant” modRNA COVID-19 “vaccines” use the original (lab-enhanced) SARS-COV-2 (COVID-19) virus modRNA that was present in the earlier versions of these “vaccines”, but in smaller amounts. Therefore, in one’s opinion, the potential exists for immune system damage in persons who take these “descendant” modRNA COVID-19 “vaccines.”
Until fairly recently, it was not known HOW, or the DETAILS behind WHY, the COVID-19 virus itselfand the COVID-19 “vaccines” have such potential for havoc and damage — all that was beginning to present were, and are, the ADVERSE EFFECTS of the virus and especially of the “vaccines”: turbo-cancers; miscarriages; Bell’s Palsy; deaths; the Adverse Events of Special Interest listings of negative effects induced by BNT162b2 in the APPENDIX 1. cited above. It is now starting to become more clear as to what SPECIFIC elements likely used in the creation of both the SARS-CoV-2 virus itself, and in the development of the modRNA COVID-19 “vaccines.” Yours Truly will posit that one of these SPECIFIC elements is something that attacks and compromises at least one important component of the human body’s immune system: the antigen site of the human leukocyte protein DRB1 (HLA-DRB1.) It took time, effort, and large amounts of funding to investigate these SPECIFIC elements; to experiment with them to ascertain the damage that could be caused; then, to “insert” these elements into the SARS-CoV-2 virus itself, and, by extension, into the modRNA COVID-19 “vaccines.” And, as the passage of time obscures or obliterates “fingerprints” of the damage done by the COVID-19 “vaccines” in the “vaccinated” individual, the involvement of these “vaccines” may well become harder and harder to trace (even though the damage is continuing in the “vaccinated” person, since one of the mechanisms of said “vaccines” is to change the DNA of the person who takes them.) Below is Slide 14 from the Palmer, MD and Sucharit, MD, article regarding what the COVID-19 “vaccines” do to the “vaccinated” person’s body. Slide 14 shows how the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2 changes the DNA of the “vaccinated” person:
Yours Truly will emphasize that it is of the utmost importance that all persons, COVID-19 “vaccinated” or not, have and maintain the highest degree possible of natural immune system health. A healthy diet is one of many ways to support and maintain a healthy natural immune system. Here is an article on this topic: www.medicalnewstoday.com/articles/322412, “The best foods for boosting your immune system”, by Lana Burgess, 10 July 2018. Among other ways to help the natural immune system are lifestyle changes, regular exercise, taking supplements, and addressing stress, as discussed here: www.healthline.com/nutrition/how-to-boost-immune-health, “9 Ways to Boost Your Body’s Natural Defenses”, by SaVanna Shoemaker, RDN, 1 April 2020. Yours Truly will add the opinion that avoiding unnecessary antibiotics and “certain injectables” are additional items to consider.
The above is a vintage image of mass vaccination. (Courtesy Google Images.)
This series on the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
The origination of today’s post begins here: www.dossier.today/p/double-digits-biden-admin-tells-americans, “Double Digits: Biden Admin tells Americans that it’s soon time for their 10th Covid shot“, by Jordan Schachtel, 13 June 2024. (Mr. Schachtel wrote about the ninth COVID-19 “vaccine” injection here: www.dossier.today/p/dose-number-nine-cdc-panel-green, “Dose number NINE: CDC panel green lights yet another Covid mRNA shot“, 29 February 2024. The CDC recommended that persons over age 65 take another “booster shot” of either the Pfizer-BioNTech or of the Moderna “2023-2024 Formula COVID-19 Vaccine” of these manufacturers.) A person age 65 or older, if that person adhered to every CDC recommendation regarding taking a COVID-19 “vaccine” injection since December 2020 (when the FDA granted first Emergency Use Authorization (EUA) to Pfizer-BioNTech and to Moderna for these companies’ “flagship” modRNA COVID-19 “vaccines” (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), would have taken injection number nine starting on 28 February 2024.
Today’s post is long. There is a large amount of information to “unpack.” Stay with me here.
Note the language regarding the “selection of a specific JN.1 lineage SARS-CoV-2 strain…” More about that later.
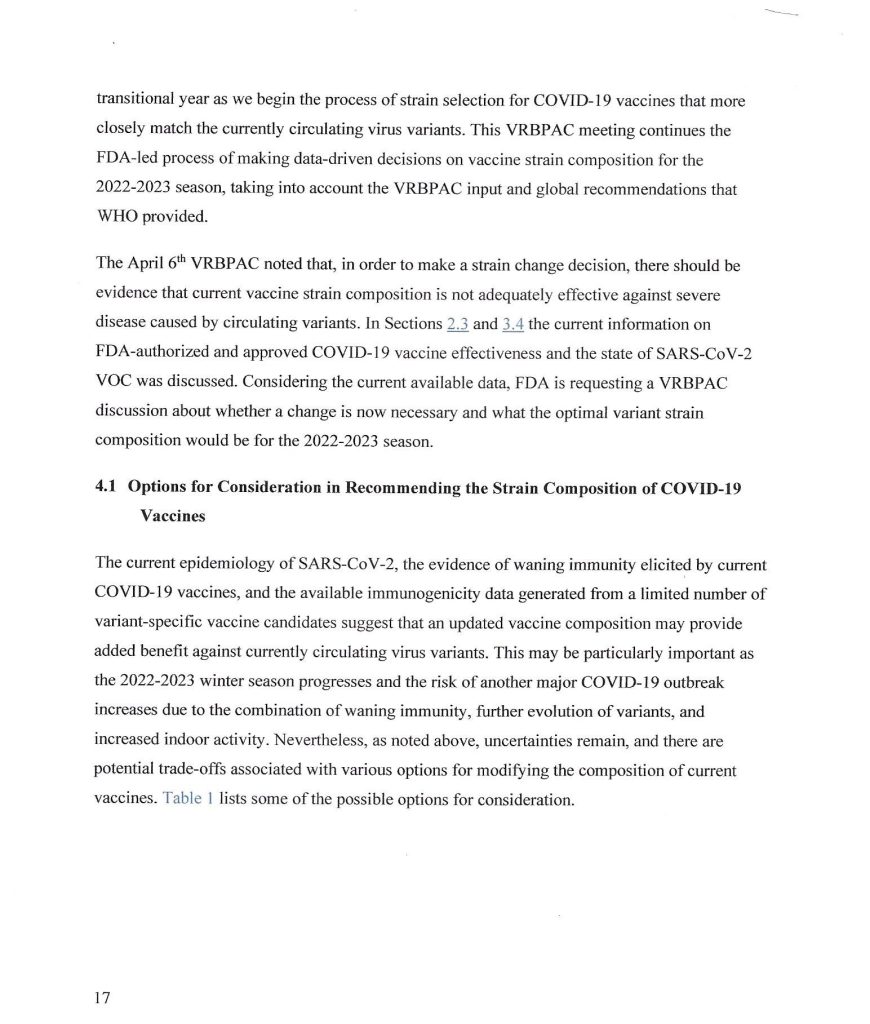
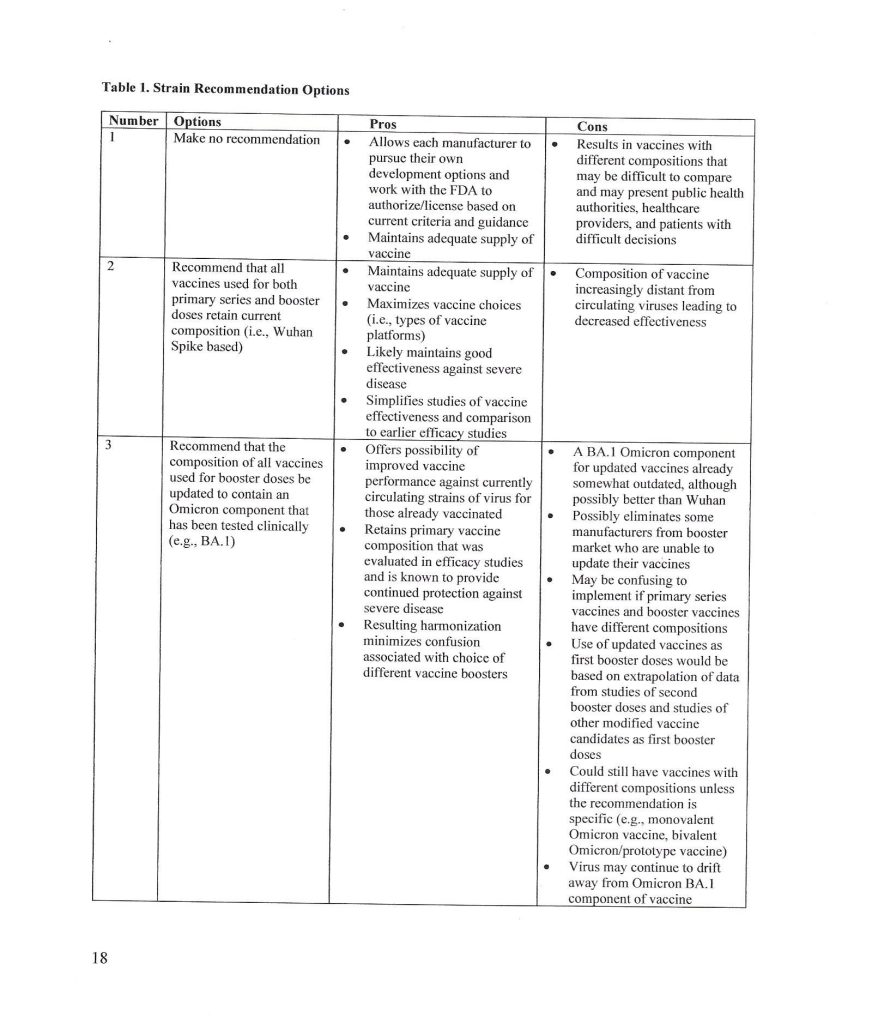
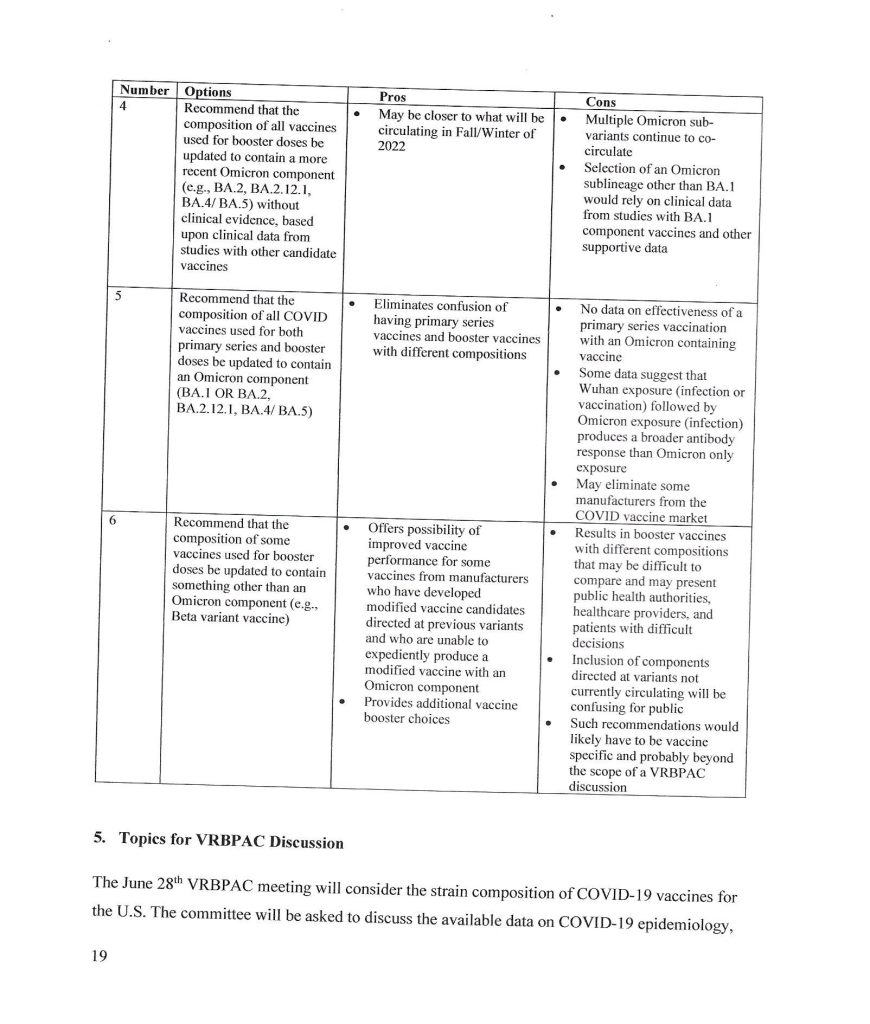
The trail behind the 5 June 2024 FDA announcement begins with the VRBPAC Briefing Document for the meeting held on 28 June 2022: www.fda.gov/media/159452/download, “FDA Briefing Document Vaccines and Related Biological Products Advisory Committee Meeting June 28, 2022.” It was at this meeting that the FDA “codified” the types of “strain composition recommendations” that the agency would use regarding “new versions” of COVID-19 “vaccines.” Yours Truly presents page 17, page 18, and page 19 of this document:
It appears that the FDA simply decided that it would be permissible for the agency to authorize a new COVID-19 “vaccine” strain composition along what, in Yours Truly’s opinion, may be called “very flexible” options. For example, the Pfizer-BioNTech XBB.1.5 COVID-19 “vaccine”, which was FDA authorized in the fall of 2023, had test results only from mouse testing prior to FDA authorization. Following are: The link to the Pfizer-BioNTech slide presentation about this “vaccine” to the CDC’s ACIP committee (Advisory Committee on Immunization Practices) meeting of 12 September 2023; and, an image of slide CC4 from this presentation. First, the presentation: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-09-12/10-COVID-Modjarrad-508.pdf.
Second, slide CC-4 from the above presentation:
The XBB.1.5. Pfizer-BioNTech COVID-19 “vaccine” had only been given as a single injection to humans in the company’s clinical trial; a clinical trial which had only just begun prior to the ACIP meeting. Slide CC-5 of the presentation, the start of the company’s human trial of this “vaccine”, is below:
Slide CC-6 of the presentation has to do with the mouse studies of this “vaccine”, which were of longer duration.
Notwithstanding the above, the FDA authorized the use of the company’s XBB.1.5 COVID-19 “vaccine” on 11 September 2023 (in Yours Truly’s opinion, it appears that the ACIP meeting of 12 September 2023 was a “catch-up” formality.) It also appears (again, in Yours Truly’s opinion), that the FDA used a very loose interpretation of “Option 4” on page 18 of the FDA Briefing Document above in granting the EUA for this “vaccine”.
** Now, on to the latest “new version” of the COVID-19 “vaccines”, the “2024-2025 Formula COVID-19 Vaccines”, that the FDA authorized in June 2024.
The following linked items are important regarding background information related to this situation and to the FDA: First, the FDA document, stating that the agency would “align” its COVID-19 “vaccine” antigen composition to the recommendations of the World Health Organization’s TAG-CO-VAC recommendations: www.fda.gov/media/179139/download (the TAG-CO-VAC recommendation for the “2024-2025 Formula COVID-19 Vaccines” was to use the JN.1 strain); second, the FDA document regarding “considerations and recommendations” for the “2024-2025 Formula COVID-19 Vaccine” composition: www.fda.gov/media/179145/download; third, the FDA announcement of the 5 June meeting of its VRBPAC committee (Vaccines and Related Biological Products Advisory Committee.): www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-june-5-2024-meeting-announcement. From this last link, chick on “Event Materials” to see the slide presentations and other items that were discussed at this meeting.
Two important items from the “Event Materials” list: the FDA Briefing Document; and the VRBPAC roster for this meeting. First, the FDA Briefing Document: www.fda.gov/media/179003/download; and, second, the VRBPAC roster for this meeting: www.fda.gov/media/179225/download. The roster for the 5 June 2024 meeting has some “familiar” members and speakers: Paul Offit, MD; and Peter Marks, MD (director of CBER [Center for Biologics Evaluation the Research of the FDA]); and, among the “Temporary Voting Members”, are: Bruce Gellin, M.D., M. PH., the Chief of Global Public Health Strategy for the Rockefeller Foundation; and, Melinda Wharton, M.D., M. PH., Associate Director of Vaccine Policy of the CDC. (Italics mine)
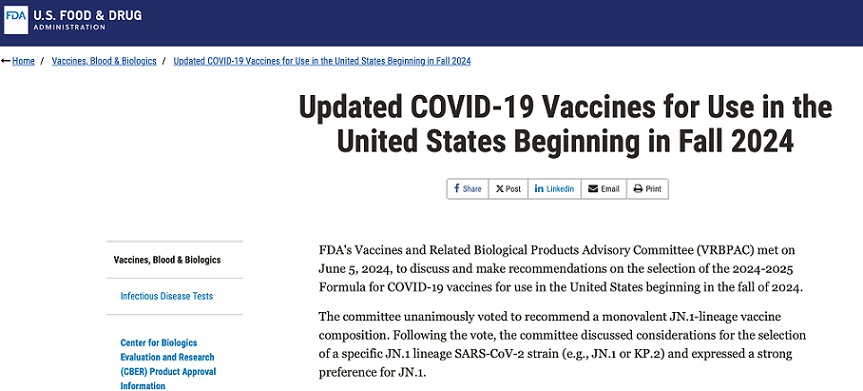
The VRBPAC members voted unanimously to endorse the Pfizer-BioNTech, the Moderna, and the Novavax “2024-2025 Formula COVID-19 Vaccine” by these companies, based on the presentations of these companies’ representatives at the meeting. Yours Truly can find noregistered human clinical trials performed in advance of the 5 June VRBPAC meeting by Pfizer-BioNTech, or by Moderna, or by Novavax, for any “2024-2025 Formula COVID-19 Vaccine”; that would indicate that any “clinical trials” were performed in these companies’ facilities on mice; and that any “human trials” were also performed in these companies’ facilities, prior to the meeting. The FDA then issued the agency’s original announcement of 7 June 2024: www.fda.gov/news-events/press-announcements/fda-roundup-june-7-2024; and, a screenshot from this announcement:
Note in particular “…the selection of a specific JN.1 lineage SARS-CoV-2 strain (e.g., JN.1. or KP.2) and expressed a strong preference for JN.1.” Here’s where it starts to “get interesting.”
What was it that happened? Part of the answer lies in the fact that the NIH and Moderna co-own the patents (and, therefore, share the royalties) for the Moderna “flagship” modRNA COVID-19 “vaccine”, mRNA-1273. This agreement would extend to “descendant clone COVID-19 vaccines” by Moderna. www.citizen.org/article/modernas-mrna-1273-vaccine-patent-landscape/. The NIH’s Dale and Betty Bumpers Vaccine Research Center (part of NIAID — which Dr. Anthony Fauci led from November 1984 until his retirement in December 2022) and Moderna co-developed mRNA-1273. https://covid19.nih.gov/news-and-stories/nih-vaccine-research-center; a screenshot from the article is below:
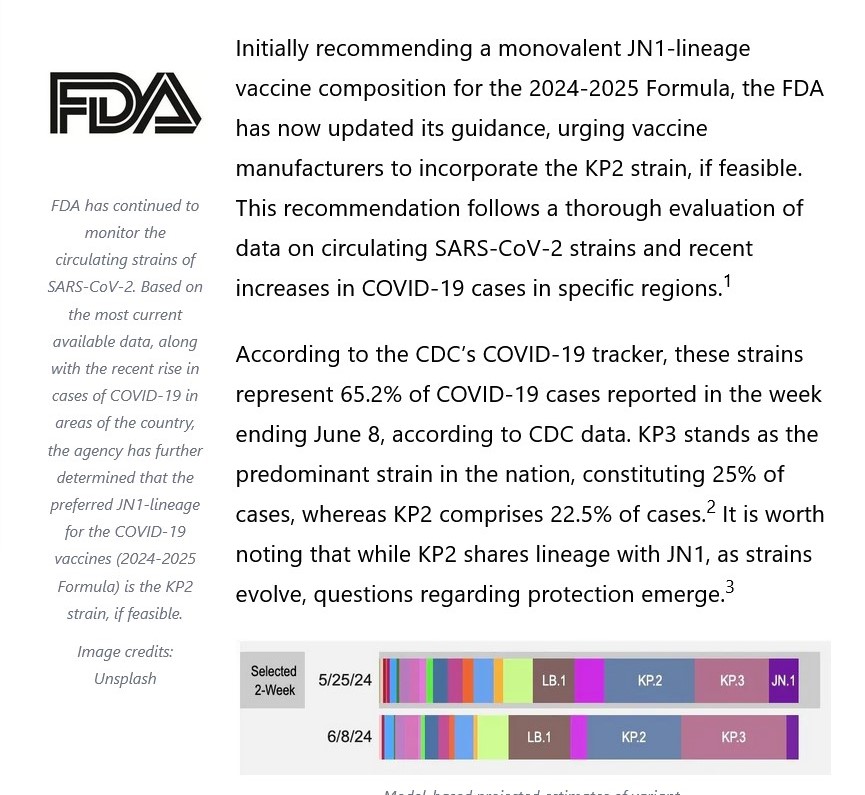
The other part of the answer is that Moderna was already developing a KP.2 strain COVID-19 “vaccine” for 2024-2025. This, and the FDA’s decision to shift away from the JN.1 strain to the KP.2 strain, are described in this post at Sasha Latypova’s blog: https://sashalatypova.substack.com/p/all-roads-lead-to-resilience, “All Roads lead to Resilience. FDA is removing competitors for the Pentagon & CIA’s baby…Moderna”, 23 June 2024.
However, there’s yet another detail in play here, regarding the FDA’s switch, “based on evaluation of the most recent circulating strains of COVID-19”, from JN.1 to KP.2 — the CIA and the Pentagon. Here is a screenshot from Sasha Latypova’s Substack article:
But wait, there’s more! Resilience lists multiple “partners”, such as the Mayo Clinic. The company also, apparently, has a “partnership” with the United States Army’s Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense https://resilience.com/learn/partnerships. Below is a screenshot from this website:
It appears, then, in Yours Truly’s opinion, that the FDA was perhaps “reminded” of the”details” regarding the NIH-Moderna co-ownership (and royalties – sharing) agreement related to Moderna’s modRNA COVID-19 “vaccines”; and, the role of the CIA-Pentagon-National Resilience (aka Resilience) in manufacturing the mRNA used in the Moderna COVID-19 Omicron “booster vaccines” — and the KP.2. strain is indeed a “descendant strain” in the Omicron lineage (as is the JN.1 strain.) Hence, the FDA’s 2024-2025 COVID-19 “vaccine” strain “sudden switch” announcement of 13 June 2024, only one week after the agency gave the nod to the JN.1 strain.
In Yours Truly’s opinion, it is statistically, medically, and ethically impossible for a new vaccine (let alone any COVID-19 “vaccine”) to be developed; tested (on lab animals, then on human subjects); the test data thoroughly collated and analyzed for “safety and efficacy” on both lab animals and on human subjects; then, which data is presented to the CDC / FDA for consideration; then, these agencies doing their own “due diligence” research; then, and only then, being granted an EUA by the FDA; then, and only then, manufactured for use in humans — in a time span of fewer than three to five years, let alone within a time span of only a few months. It appears, again in Yours Truly’s opinion, that the CDC and the FDA are playing “fast and loose” with the health and safety of the people who choose (or will be “mandated”) to take the “2024-2025 Formula COVID-19 Vaccine.” And, also, that “other entities” are in play here to perhaps “influence” decision making by these agencies.
All of above is in addition to the fact that the COVID-19 “vaccines” (actually, gene therapy injections) have caused, are causing, and will cause, multiple health issues, serious adverse reactions, and deaths, in those who are “vaccinated.” Just two of the most recent discoveries: One, the COVID-19 “vaccines” can cause brain damage, an article by Dr. William Makis: www.globalresearch.ca/brain-damage-covid-19-mrna-vaccines/5861012, “Brain Damage Caused by COVID-19 mRNA Vaccines”, 26 June 2024. Below is a screenshot from Dr. Makis’ article:
The second most recent discovery, that the COVID-19 “vaccines” reduce life expectancy (even in “all-cause” analysis) among COVID-19 “vaccinated” persons, by Dr. Peter A. McCullough: https://petermcculloughmd.substack.com/p/breaking-publication-a-critical-analysis, “BREAKING Publication — A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, 1 July 2024. The peer-reviewed paper is here: https://doi.org/10.3390/microorganisms12071343, “A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, Marco Alessandria, et al., published 30 June 2024. Below is a screenshot from the Conclusions section of this paper:
In Yours Truly’ opinion, it is apparent at “half a glance” that the COVID-19 “vaccines” (actually, gene therapy injections) must be completely withdrawn for human use until these products have been fully investigated, and then re-designed, before being re-introduced for human use; and, that there is no “co-ownership” or sharing of royalties between a government agency and a COVID-19 “vaccine” manufacturer; and, that there is no involvement of the United States military in the development or manufacture of such products.
This series on the COVID-19 virus and the COVID-19 “vaccines” is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
Human beings shed items from their bodies every day: hair (and dandruff); tears; nasal mucus when blowing the nose or in sneezing; saliva; urine and feces; dead skin cells; sweat — among other things. They also shed particles of viruses — for example, of the “common cold” virus. They shed particles of vaccines — for example, of the Zaire ebolavirus vaccine, ERVEBO (www.fda.gov/media/133748/download, the Package Insert for ERVEBO; please refer to section 12.3 Pharmacokinetics, subsection Shedding). Today’s post will discuss the shedding of the COVID-19 virus itself, and of the COVID-19 “vaccines” (including the “2023-2024 Formula COVID-19 Vaccines.”) For purposes of today’s presentation, the trail begins with some details about how the COVID-19 virus itself works. Note: the knowledge base of exactly what is contained in the mRNA and spike protein of the original Wuhan Hu1 SARS-CoV-2 (COVID-19) virus; and, exactly what is contained in the modRNA and the other elements within the COVID-19 “vaccines”, is an evolving situation.
The following article, published on www.statnews.com/ on 10 April 2020 (before any COVID-19 “vaccine” had been authorized or approved for use), is about how the SARS-CoV-2 virus itself enters into human cells via the ACE2 receptors www.statnews.com/2020/04/10/coronavirus-ace-2-receptor/, “The coronavirus sneaks into cells through a key receptor. Could targeting it lead to a treatment?”, by Kate Sheridan.) From the article: “In a healthy person, the ACE2 receptor chops up two forms of a protein called angiotensin to keep blood pressure stable, among other things. SARS and the novel coronavirus, however, use the receptors to infiltrate cells,…The virus can latch onto ACE2 and sneak inside, replicating itself inside the cell and then wreaking havoc throughout the body.” According to Wikipedia, ACE2 receptor cells, found in the intestines, kidney, testes, gallbladder, and heart, regulate blood pressure in the body. However, the SARS-CoV-2 spike protein damages the endothelium by “downregulating” the ACE2 receptor ability. The endothelium is a layer of cells lining the interior surfaces of blood vessels and of lymphatic vessels.
A paper in Nature was published on 10 May 2021 of a study of 31 SARS-CoV-2-infected patients in Italy. The data were collected between November 2019 (from seven healthy controls) and from 31 COVID-19 infected patients (hospitalized), prior to publication in May 2021. The treatments administered to the infected patients were Tocilizumab (an immunosuppressant drug), and Anakinra (a drug that treats Rheumatoid Arthritis), as no COVID-19 “vaccine” had yet been authorized or approved for use. The paper is found here: https://pubmed.ncbi.nlm.nih.gov/33972535/, “Identification and characterization of a SARS-CoV-2 specific CD8+T cell response with immunodominant features”; Pia Kvistborg, et al. (click on the DOI link for the full paper.) The authors of the paper were investigating the connection between the COVID-19 virus and its effects specifically on the CD8+ cells of the human body. What they found was quite interesting: the COVID-19 virus itself does indeed target many of the epitopes related to the CD8+ cells of the human immune system (an epitope is part of an antigen that is “recognized” by the immune system via antibodies, B cells, and T cells.)
Another paper, published on 31 July 2023, investigated the effects of the SARS-CoV-2 virus on the CD4 cells of the human body (https://doi.org/10.7554/eLife.84790, “SARS-CoV-2 uses CD4 to infect T helper lymphocytes”, Marcelo A. Mori, et al. Among the findings of this paper is that the SARS-CoV-2 virus attacks the ACE2 receptors of the CD4 lymphocyte cells.
Therefore, it was known as early as April 2020 that the SARS-CoV-2 (COVID-19) virus itself attacks and damages important cells and mechanisms of the body of an infected person. What about the COVID-19 “vaccines?” It may be assumed that, since the COVID-19 “vaccines” contain the mRNA and spike protein elements of the original Wuhan Hu1 virus, these same elements are also contained in the COVID-19 “vaccines” — in addition to lab-engineered modifications to the mRNA, plus lipid nanoparticles and certain excipients (for lists of the excipients, please see: https://doi.org/10.1016/j.jnma.2022.08.003, “Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273) COVID-19 vaccines and hypersensitivity reactions”, Hannah N. Haq, et al., published 29 October 2022.) In the “Trougakos, et al. paper” of 20 April 2022, it was presented that the COVID-19 “vaccines” bind the spike protein to the ACE2 receptors in the body and contribute to what the paper calls “vaccination-related AEs” (Adverse Events.) The paper is found here: https://doi.org/10.1016/j.molmed.2022.04.007, “Adverse effects of COVID-19 mRNA vaccines” the spike hypothesis”, Ioannis P. Trougakos, et al. Figure 1 from the paper, below, shows how the lipid nanoparticles (LNPs) in the COVID-19 “vaccines” move the spike protein and its modRNA around in the cell structure of the “vaccinated” person’s body. Note the “Furin cleavage-S1 shedding” on the figure:
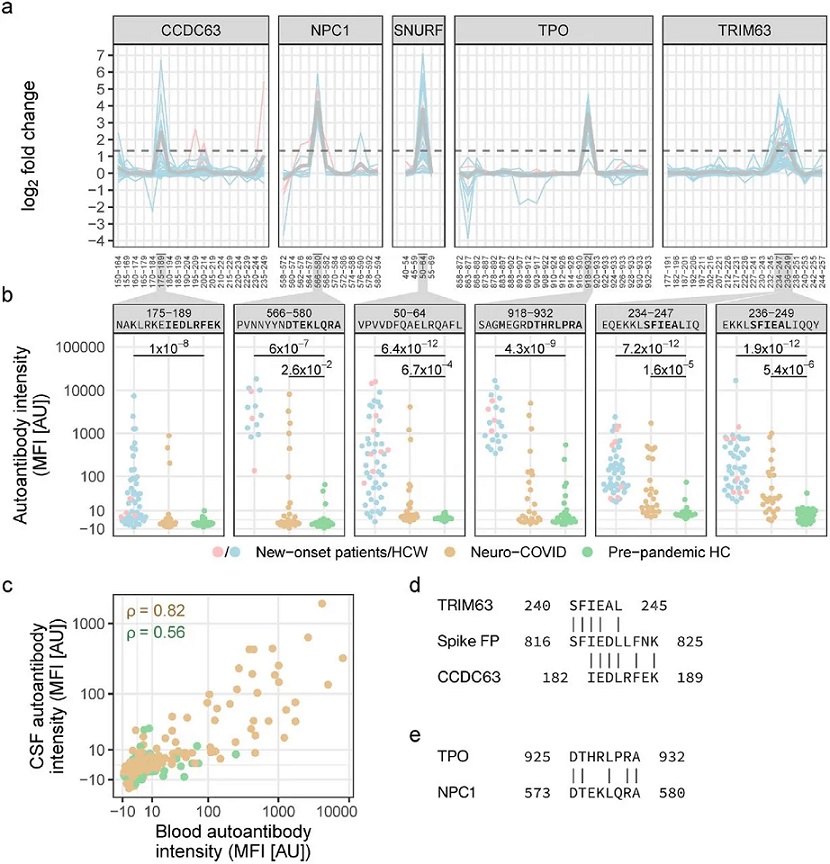
Yours Truly now turns to “The Elephant in the Room” — the phenomena of shedding of the COVID-19 virus itself; and the shedding of elements of the COVID-19 “vaccines.” The first aspect, the shedding of the COVID-19 virus itself, is presented and discussed here: https://wmcresearch.substack.com/p/new-onset-autoantibodies-after-any, “New Onset Autoantibodies After Any Exposure to the Spike Protein of SARS-CoV-2”, by Walter M Chesnut. This article discusses, among other items, a paper published in February 2024, https://doi.org/10.1101/2024.02.15.24302857, “Prevalent and persistent new-onset autoantibodies in mild to severe COVID-19”, Peter Nilsson, et al. Yours Truly presents Figure 1 from this paper, an example of epitope mapping in neuro-COVID patients:
An autoantibody is an antibody made by the immune system that can attack one (or more) of the body’s own proteins; Graves’ Disease is an example of a condition induced by autoantibodies.
The Cleveland Clinic recognized, in 2022, that elements of the COVID-19 virus can be shed into the air: https://my.clevelandclinic.org/health/diseases/21214-coronavirus-covid-19, “Coronavirus, COVID-19”, dated 3 January 2022. In this article, people were warned away from “close contact” with COVID-19 infected persons. “Close contact”, in the article, was defined as, “…being within 6 feet of an infected person from a cumulative total of 15 minutes or more over a 24-hour period.” The article also states that the virus can be spread via “respiratory droplets released into the air when an infected person coughs, sneezes, talks, sings or breathes near you.” (Yours Truly is aware that the “stay 6 feet away rule” is arbitrary, considering that aerosols [sneezes, for example] travel a lot farther than six feet and also at quite high speeds.)
So, it is known that the COVID-19 virus itself can be shed by an infected person into the air, and by an infected person onto another person. What about the shedding of elements and particles of the COVID-19 “vaccines” by a “vaccinated” person? This aspect is fueling new research that is being studied, compiled, and published (again, another piece of the evolving knowledge base regarding the virus and the “vaccines.”) For purposes of today’s post, Yours Truly will present the current findings of two such researchers: Dr. Ana Mihalcea, MD, PhD; and Dr. Pierre Kory, MD, co-founder of COVID-19 Critical Care Alliance (FLCCC); a paper co-authored by Stephanie Seneff, PhD; and a paper co-authored Jessica Rose, PhD, and Peter A. McCullough, MD, et al.
Dr. Mihalcea has conducted several darkfield microscopic investigations into the shedding of COVID-19 “vaccine” elements and particles from “vaccinated” persons. One of her blog articles about her findings is here: https://anamihalceamdphd.substack.com/p/darkfield-live-blood-analysis-c19, “Darkfield Live Blood Analysis C19 Unvaccinated Blood. C19 Vax Shedding And Environmental Exposure Has Not Slowed Down”, published 23 January 2024. The image below is from her blood analysis of an “unvaccinated” person who was in close contact with a COVID-19 “vaccinated” person. Note the presence of unusual structures in this person’s blood:
Another of Dr. Mihalcea’s articles on her findings is here: https://anamihalceamdphd.substack.com/p/environmental-filaments-uv-light, “Flourescent Filaments Coming Out of C19 Vaccinated Individuals Skin Glowing Under UV Light: Darkfield Microscopy”, published 28 January 2024. This article discusses what appear to be filaments of luciferase that were “shed” from COVID-19 “vaccinated” persons onto their skin. For further reference regarding the presence of luciferase in the COVID-19 “vaccines,” please see: www.nature.com/articles/s41541-023-00751-6, “Effect of mRNA-LNP components of two globally-marketed COVID-19 vaccines on efficacy and stability”, Lizhou Zhang, et al. Section Results of this paper discusses the experiments with the firefly luciferase contained in the Pfizer-BioNTech COVID-19 “vaccine” LNP, ALC-0315, as compared to the firefly luciferase contained in the Moderna COVID-19 “vaccine” LNP, SM-102.
Dr. Pierre Kory is investigating the COVID-19 “vaccines” shedding phenomenon and is writing about it in his Substack. Here is his compendium post on the issue: https://pierrekorymedicalmusings.com/p/mrna-vaccine-shedding-of-spike-protein, “mRNA Vaccine Shedding Of Spike Protein: State Of the Scientific and Clinical Evidence”, published 20 February 2024. There is a searchable PDF of the report here: https://covid19criticalcare.com/wp-content/uploads/2024/02/Shedding-of-COVID-mRNA-Vaccines-A-review-of-evidence-2024-02-03.pdf. Yours Truly urges interested persons to read through this report, especially starting on Page 15, SUMMARY OBSERVATIONS OF OVER 1000 CLINICAL REPORTS OF SHEDDING; and continuing on Page 23, CLINICAL GUIDANCE. The entire report has many “clickable” underlined hyperlinks to documents, other reports, clinical trials, and so on. His COVID-19 “vaccines” shedding series begins here: https://pierrekorymedicalmusings.com/p/shedding-of-covid-mrna-vaccine-components, “”Shedding” of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1″, published 1 November 2023 (there are links to the other eight parts of the series at the end of Part 1.)
Stephanie Seneff, PhD, and Greg Nigh published a paper in May 2021 on multiple possible “unintended consequences” of the COVID-19 “vaccines.” The paper is found here: International Journal of Vaccine Theory, Practice, and Research 2(1), May 10, 2021, pages 38 – 79, “Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19.” Yours Truly presents part of page 62 of the paper:
Yours Truly now turns to the peer-reviewed paper published in Cureus on 24 January 2024, and which paper was suddenly retracted by Cureus on 26 February 2024: www.cureus.com/articles/203052-covid-19-mrna-vaccines-lessons-learned-from-the-registrational-trials-and-global-vaccination-campaign#1/, “COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign”, M. Nathaniel Mead, Russ Wolfinger, Jessica Rose, Kris Denhaerynck, Steve Kirsch, Peter A. McCullough. (Cureus and its parent company, Springer / Nature have since been sued for $250 million in damages by Steve Kirsch on behalf of himself and the other co-authors of the paper, as it was not retracted by the authors themselves; nor was it retracted with their consent.) The paper presents and discusses the flawed, incomplete, and data-manipulated COVID-19 “vaccine” clinical trials. It also states the following, per the screenshot from the paper, below:
So, now it is known that both the COVID-19 virus itself, and elements of the COVID-19 “vaccines”, do shed. What are people, “vaccinated” and, especially, “unvaccinated” people, to do — stay away from others, including “vaccinated” friends and family? Go back to wearing the (mostly useless, except for certain healthcare settings, etc.) masks, the disposable gloves, the washing of clothes in hot water, etc.? Go back to “self-limiting” exposure to places like grocery stores, healthcare providers’ offices, and so on? Avoid all “unnecessary” travel? Are all people supposed to consider themselves to be COVID-19 “vaccinated,” either via injection or via shedding of COVID-19 “vaccine” elements by “vaccinated” persons?
The following is not professional medical or healthcare advice — they are only ideas and possible suggestions. In addition, since the investigation of COVID-19 virus shedding and COVID-19 “vaccines” shedding is an another evolving aspect of the entire situation, Yours Truly is not, and cautions against, “leaping to certain conclusions,” although ongoing research is uncovering important things; therefore, the following are presented as personal opinions for all people, “vaccinated” and “unvaccinated”, to consider:
It is important to make sure that one’s own general health and natural immune system are brought up to, and maintained, in the best shape possible: to avoid / prevent infection by the COVID-19 virus itself, and / or to be impacted by shedding of the COVID-19 virus from infected persons; and / or to be impacted by the shedding of COVID-19 “vaccines” elements by “vaccinated” persons. This could possibly include dietary changes, vitamins and supplements as needed, and so on. Note: Speak with a healthcare provider regarding possible interactions between certain supplements and any prescription drugs that a person may be taking: for example, Nattokinase can interact with prescription blood thinners or with aspirin.
It is important that regular mild to moderate exercise, especially walking, be undertaken for 30 minutes a day, at least five days of the week. This could also include activities such as gardening, Yoga, and so on.
It is important that techniques to reduce stress and eliminate unnecessary stressors be part of one’s life and practiced daily.
It is important to have and keep a positive connection to the Almighty God, or to whatever Benevolent Divine Force that one believes in.
It is important to follow a COVID-19 prevention / treatment / spike protein detox program — by COVID-19 “vaccinated” persons; by “unvaccinated” persons; and/or, by persons who have been infected by COVID-19 and have recovered — such as the programs outlined, for example, at COVID-19 Critical Care (FLCCC Alliance https://covid19criticalcare.com/); or, through working with a medical professional who believes in such a program; or, through working with a reputable Naturopathic Doctor, herbalist, Traditional Chinese Medicine or Ayurvedic Medicine practitioner.
It is important that COVID-19“vaccinated” personsdo their own due diligence regarding the dangers of the COVID-19 “vaccines”, and decide for themselves whether or not to continue taking them.
It may be prudent, if a person feels “coming down with” an illness, or doesn’t feel “up to par,” to politely decline attendance at activities or events that were previously planned, in order to stay home and take care of oneself, and/or to seek medical care.
For some further information on the truth about the COVID-19 virus itself, and about the COVID-19 “vaccines”, please see:
This series of posts regarding the ongoing issues of COVID-19 and the COVID-19 “vaccines” is dedicated to the memory of Yours Truly’s cousin Bill, who passed away “suddenly and unexpectedly” in September 2023. Today’s post is addressed to medical professionals who had any COVID-19 “vaccines” (in reality, gene therapy injections) injected into their bodies since 11 December 2020. This post is not “accusatory” in nature: Yours Truly is curious. One will make it clear at the outset that there are vaccines and other injectables that are useful: For examples, the Rabies vaccine and the injectable form of Heparin. One will also make it clear that the following questions regarding the modRNA COVID-19 “vaccines” are not “tin-foil hat” or “conspiracy theory” in nature — all of them are based on the writings and researching of medical doctors and scientists who want to find out the truth about these particular “vaccines.” There are many other questions that must be asked; Yours Truly is presenting a few of the most important ones from a personal point of view in today’s post.
Dear COVID-19 “Vaccinated” Medical Professional:
With all due respect for your education and expertise, there now must be serious questions raised concerning the COVID-19 “vaccines” that were rushed into use in the United States and all over the world. These questions are especially important given the increasing numbers of reports of COVID-19 “vaccine”-induced injuries, illnesses, disabilities, and deaths, among those who have taken, and/or continue to take, these “vaccines.”
The first question that must be raised is: Are you aware that the FDA knew, back on 30 April 2021, that the modRNA COVID-19 “vaccine” by Pfizer-BioNTech, BNT162b2, is involved in the inducement of over 1,200 types of medical diseases and conditions? Here is the document that Pfizer-BioNTech gave to the FDA on that date: https://phmpt.org/document/5-3-6-postmarketing-experience.pdf, 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021. Please see page 30 of this report, APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST. The report is also found here: https://phmpt.org/document/5-3-6-postmarketing-experience.pdf. The document is FDA time-stamped 30 April 2021. Yours Truly will point out that this report covers only between 11 December 2020 (the date of the initial EUA granted by the FDA for BNT162b2 to be used in the United States) and 28 February 2021. The list of Adverse Events of Special Interest begins with 1p36 deletion syndrome; other diseases, disorders, and events mentioned include: Cardiac arrest; Cerebral thrombosis; Demyelination; Guillain-Barre syndrome; hepatic disorders; immune system disorders; pulmonary disorders; Myocarditis; neurological disorders; and, Pericarditis; among many others.
The second question that must be raised is: Are you aware that the modRNA COVID-19 “vaccines” made by Pfizer-BioNTech (these include BNT162b2; this company’s previous “booster” COVID-19 “vaccines”; and this company’s current “2023-2024 Formula COVID-19 Vaccine”) contain two dangerous lipid nanoparticles, ALC-0159 and ALC-0315, both of which are for research use only? Here are the Safety Data Sheets for these lipid nanoparticles: For ALC-0159: https://cdn.caymanchem.com/cdn/msds/34336m.pdf; and, for ALC-0315: https://cdn.caymanchem.com/cdn/msds/34337m.pdf. On page one of each of these Safety Data Sheets, there is the following language: “Application of the substance / the mixture This product is for research use – Not for human or veterinary diagnostic or therapeutic use.” In addition, are you aware that the modRNA COVID-19 “vaccines” made by Moderna (these include mRNA-1273; this company’s previous COVID-19 “booster vaccines”; and this company’s current “2023-2024 Formula COVID-19 Vaccine”) contain the dangerous lipid nanoparticle, SM-102, which is for research purposes only? Here is the Safety Data Sheet for this lipid nanoparticle: https://cdn.caymanchem.com/cdn/msds/33474m.pdf. On page one of this Safety Data Sheet, there is the exact same language in the section “Application of the substance / the mixture” as is listed for ALC-0159 and for ALC-0315 in their respective Safety Data Sheets: “This product is for research use – Not for human or veterinary diagnostic or therapeutic use.” (As an aside, ALC-0149 and ALC-0315 are described only by their chemical component names in the FDA-issued Fact Sheet for the Pfizer-BioNTech “2023-2024 Formula COVID-19 Vaccine”: www.fda.gov/media/167211/download; please see under section 11 DESCRIPTION. However, ALC-0159 and ALC-0315 are called by their proper names in the FDA document, www.fda.gov/media/172019/download, Emergency use Authorization (EUA) for an Unapproved Product Review Memorandum, dated 23 June 2023, section 7.1 Chemistry Manufacturing and Control (CMC) Information.)
The third question that must be raised is: Are you aware that the COVID-19 “vaccines” can, and do, “shed” components of these products from “vaccinated” persons to un-“vaccinated” persons? Dr. Pierre Kory has an extensive series of articles on his blog relating to this phenomenon: https://pierrekorymedicalmusings.com/; please see Part One of this series: https://medicalmusings.com/p/shedding-of-covid-mrna-vaccine-components, published 1 November 2023.
The fourth question that must be asked is: Are you aware that the COVID-19 “vaccines” can, and do, damage the blood vessels, heart tissue, and lung tissue, of persons who have these “vaccines” in their bodies? Please refer to: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, Michael Palmer, MD, and Sucharit Bhakdi, MD. Yours Truly presents page nine of this paper, which is self-explanatory:
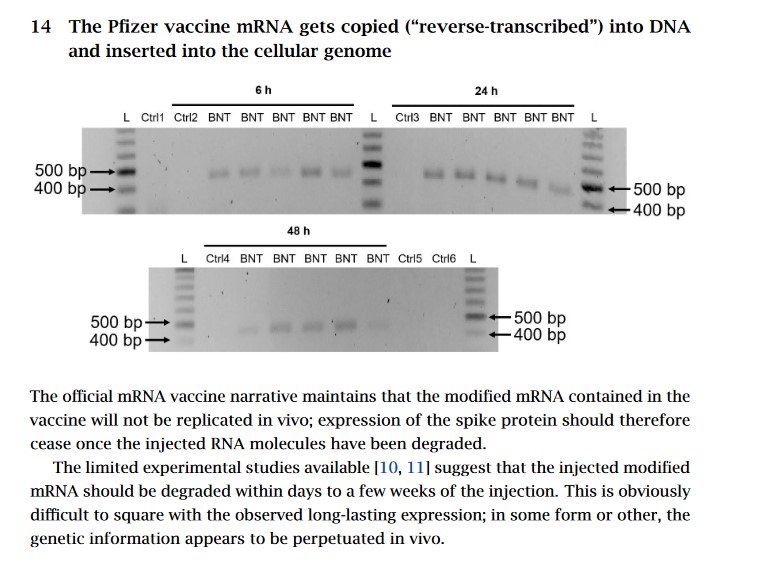
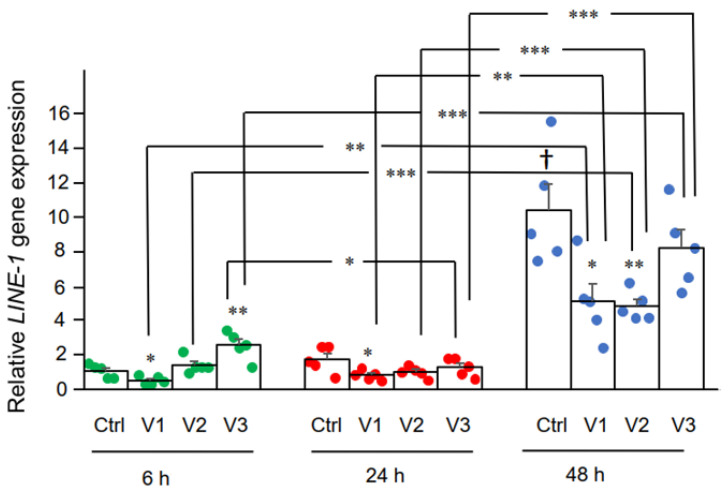
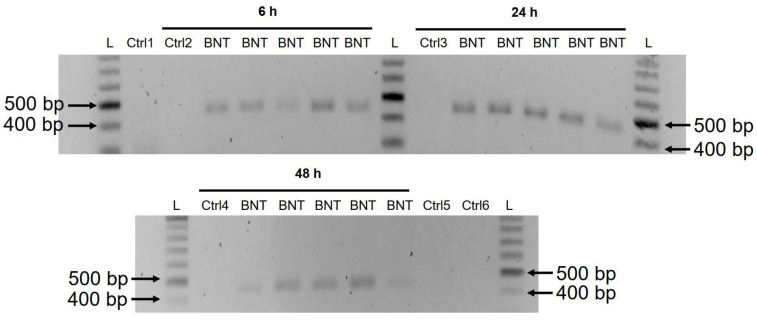
The fifth question that must be asked is: Are you aware that the modRNA Pfizer-BioNTech COVID-19 “vaccine”, BNT162b2, changes the DNA of the LINE-1 Human Liver7 cell line? Please refer to: https://doi.org/10.3390/cimb44030073, “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Yang De Marinis, et al. Yours Truly presents two images from this paper: The first, of DNA expression induced in BNT162b2-treated Human Liver7 cells in LINE-1; the second, of DNA amplicons induced by BNT162b2-treated Human Liver7 cells in LINE-1.
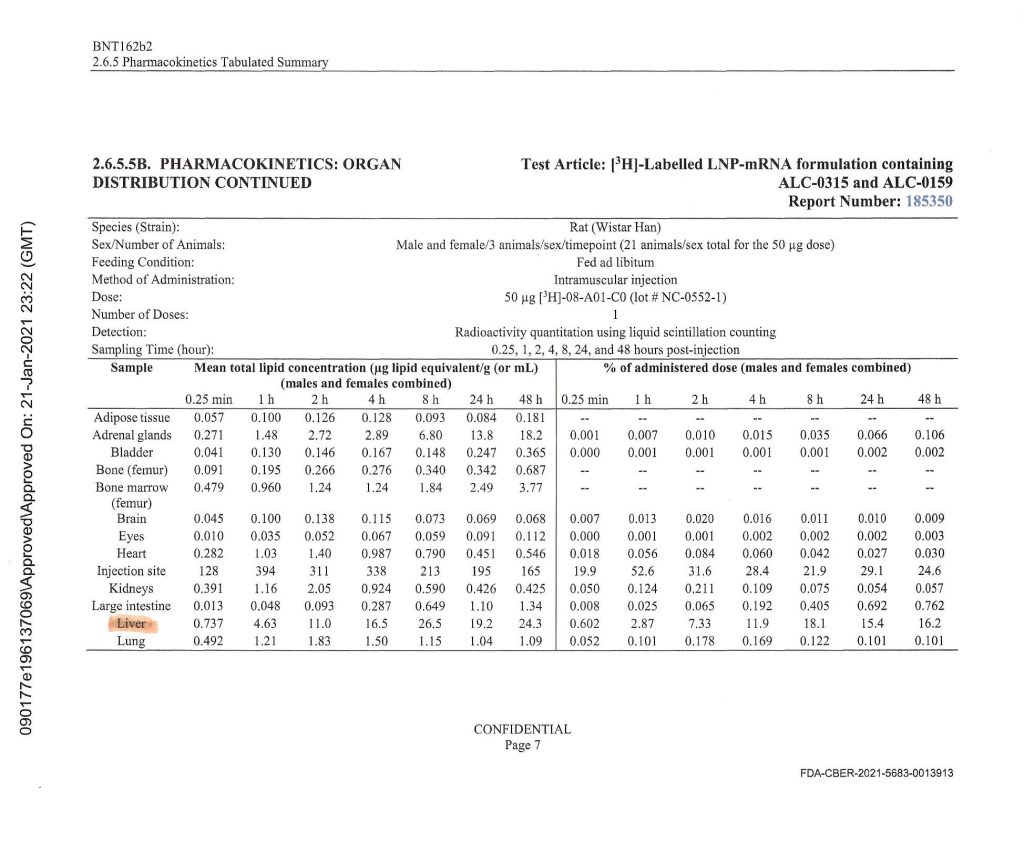
Notice the heavy accumulation of BNT162b2 in the livers of the Wistar lab rats that were used in this experiment conducted by Pfizer-BioNTech. This was the same BNT162b2 Pfizer-BioNTech modRNA COVID-19 “vaccine” that was later injected into human patients (with ingredients amounts calibrated for human use.)
Yours Truly will note that the CDC changed the definitions of “vaccine” and “vaccination” in 2021, after the rollout of the COVID-19 “vaccines” (gene therapy injections.) One suspects that this was done to “shoe-horn in” these products under the aegis of “vaccines.” Please refer to: www.johnlocke.org/the-cdc-changed-its-definitions-of-vaccine-and-vaccination-and-keeps-changing-its-definition-of-fully-vaccinated/. However, the FDA states clearly, on page four of the Fact Sheet for Healthcare Providers for the administration of the “2023-2024 Formula COVID-19 Vaccine” by Pfizer-BioNTech, that this product is to prevent coronavirus disease (COVID-19), not to “protect against serious illness from COVID-19”, as the CDC states. Please refer to: www.fda.gov/media/167211/download, page four, under section 1 EMERGENCY USE AUTHORIZATION; and to www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html under What You Need to Know.
Finally, there is this paper, published on 24 January 2024: https://doi.org/10.7759/cureus.52876, “COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign”, M. Nathaniel Mead, Peter A. McCullough, et al. Yours Truly presents part of the Abstract of this paper:
Sincerely, with Good Energy, Peace, and Respect, PAVACA
PAVACA: BFA (2), Carnegie-Mellon University; MA, Duquesne University. Reading and writing about COVID-19 and the COVID-19 “vaccines” since March 2020. Also interested in Pharmacy and in the impacts of Big Pharma. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 – 2018), First Professor of the Darden School of the University of Virginia, available at www.amazon.com/, www.barnesandnoble.com/, and www.authorhouse.com/.
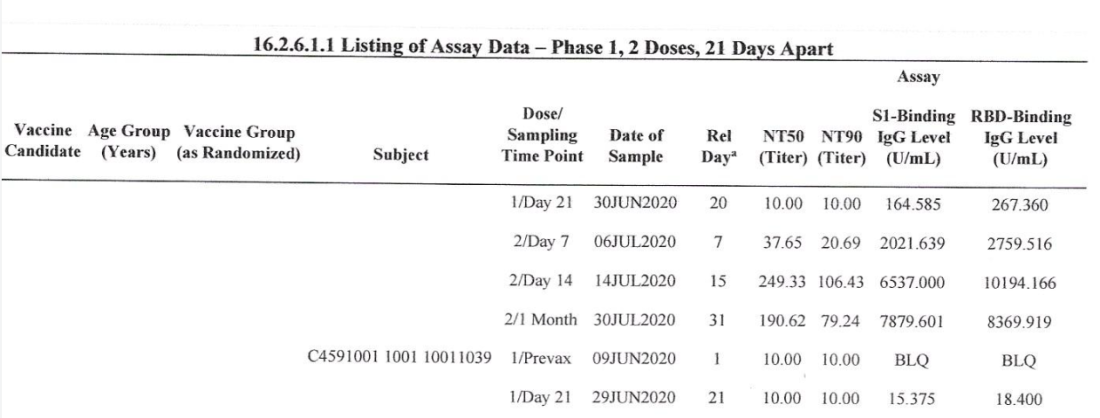
The above chart listing is from a Pfizer-BioNTech document obtained via FOIA, showing the IgG binding results of a few of the C4591001 human test subjects for the company’s “flagship” COVID-19 “vaccine”, BNT162b2. The document was given to the FDA on 19 September 2020. BNT162b2 was granted the initial EUA for use in the United States in December 2020.
This series on the disaster of COVID-19 and the COVID-19 “vaccines” is dedicated to Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
Today’s offering will present and discuss some aspects of the emergence of “turbo-cancers” that appear in people who get injections of the COVID-19 “vaccines” (actually, gene therapy shots.) Today’s presentation is not an “magnum opus” compilation, but rather an adjunct to more understanding of the issue. It will not discuss the presence of the SV40 cancer promoter code that was discovered recently in the modRNA COVID-19 “vaccines” — that is an issue to be addressed in another post. What will be presented today is the role of IgG4-engendered cancer onset and/or relapse due to “vaccination” by the modRNA COVID-19 “vaccines.”
Without “wearying by recitals”, the story begins with a short presentation on the Ig system of the human body. This system consists of five different Ig cell types: IgM; IgD; IgA; IgE, and IgG. IgA and IgG cells can be divided into subclasses. What are called “subclass switches” within the IgA class and IgG class are regulated via interaction with the T cells of the human body. The Ig system is basically an infection-fighter system. It needs to be in balance in order for this work to be successfully performed. Imbalances of the Ig system can result in the incidence of various medical disease conditions, such as autoimmune diseases and asthma. Some people have inherited imbalances of their Ig system. Today’s offering will confine itself to the IgG class.
The IgG class of cells can be divided into four separate subclasses: IgG1; IgG2; IgG3; and IgG4. Robert H. Pointer wrote the following regarding the IgG class in general: “Firstly, IgG neutralizes pathogens such as viruses and bacteria by binding to key pathogen surface proteins and preventing interaction of the pathogen with host cells. In doing so, the antibody [of the IgG cell] neutralizes the ability of the pathogen to enter host cells and replicate.” (Encyclopedia of Immunology, Second Edition, 1998, “Immunoglobulin G” chapter; bolding is mine.)
Please read those two sentences above by Prof. Pointer again. Now look again at the chart at the top of today’s offering, which shows the high binding ability of the Pfizer-BioNTech modRNA COVID-19 “vaccine”, BNT162b2, to the cells of the human subjects who took this “vaccine” in the C4591001 clinical trial of said “vaccine.” This is the same BNT162b2 “vaccine” formula that was granted the initial EUA by the FDA in December 2020 for use in the United States. It is also the same BNT162b2 “vaccine” formula (under both the name, “Pfizer-BioNTech COVID-19 Vaccine” and under the name, “COMIRNATY”) that was used in the United States until the spring of 2023, at which time it was removed from use in this country and was substituted with the “2023-2024 Formula COVID-19 Vaccine” by the same company. BNT162b2 is still used in other countries. It appears that two of the main goals of BNT162b2 (a modRNA COVID-19 “vaccine”) were, and are (both in the BNT162b2 “vaccine”, AND in the basic formulation of the current “2023-2024 Formula COVID-19 Vaccine”),to evade the “vaccine” recipient’s natural IgG class cells’ “detection and fight” capability; and, to compromise the “vaccine” recipient’s natural IgG class cells’ ability to DENY ACCESS tothe “vaccine” into the cells of the recipient’s body (this, via the use of the lipid nanoparticles ALC-0159 and ALC-0315 in these “vaccines.”),
Yours Truly now turns to https://jessicar.substack.com/p/igg4-and-cancer-a-mechanism-of-action, “IgG4 and cancer – a mechanism of action for cancer relapse and onset”, published on 30 December 2022. Dr. Rose describes how IgG4 class cells can, by “class switching” (also called “Fab Arm Exchange”) due to chronic exposure to an antigen, literally “turn around” their normal antibody function of tumor suppression into tumor progression. Dr. Rose then goes on to discuss this phenomenon in light of the modRNA COVID-19 “vaccines” and how these injections introduce “highly immunogenic protein” into the body of the “vaccine” recipient, which then induces “continuous antigen stimulation by the injectables’ contents and their by-products” (Italics mine.) She ends her article with: “My take home message: This could be potentiating relapses of cancers previously in remission and also new and rare cancer appearances.” In my opinion, this is particularly troubling, since nobody really knows how long the modRNA, the spike protein, and the ALC-0159 and ALC-0315 lipid nanoparticles remain in the “vaccine” recipient’s body; especially if that “vaccine” recipient continues to get modRNA COVID-19 “vaccine booster shots” to “complete a catch-up series”, or the “2023-2024 Formula COVID-19 Vaccine” made by Pfizer-BioNTech and also by Moderna.
We now turn to the work of Dr. Ryan Cole, the pathologist. He has been sounding the alarm over the presence of turbo-cancers in his modRNA COVID-19 “vaccinated” patients for over a year (and for which, he is now fighting the “professional misconduct charges” that were served against him by the Washington State medical licensing board. Please refer to https://vigilantnews.com/post/turbo-death-from-turbo-cancers-were-in-trouble-says-dr-ryan-cole, from 10 October 2023. Dr. Cole makes it clear that the “vaccines” do not actually cause cancer; they “cause immune suppression. They cause a disruption and a dysregulation of your immune system that normally is what would fight cancer.” (Another way, in my opinion, of saying the IgG4 “class switch” induced by the modRNA COVID-19 “vaccines” that turns this class of cells’ normal function of fighting tumors into, instead, allowing tumors to grow.)
The “Vidarsson paper” from 2014 describes the IgG subclasses, what they do, and what can happen when one or more of these subclasses are either deficient or increased too much: www.frontiersin.org/articles/10.3389/fimmu.2014.00520/full, “IgG subclasses and allotypes: from structure to effector functions”, Gestur Vidarsson et al. Please see the section “IgG4” about how the IgG4 subclass works; and the section “IgG4 Fab Arm Exchange.”
IgG4 cells will also change in the unborn child and in its pregnant mother due to modRNA COVID-19 “vaccination.” Here is a graphic showing these changes:
The above graphic is from here: https://doi.org/10.1101/2023.05.01.538955, “Diverging maternal and infant cord antibody functions from SARS-CoV-2 infection and vaccination in pregnancy”, Emily H. Adhikari, et al. From the Introduction: “After mRNA vaccination [of the pregnant mother], the primary form of immunity transferred to the fetus is antibodies, specifically IgG.” (Bolding mine)
Two blog posts by Igor Chudov provide more information. The first is from 21 October 2022: www.igor-chudov.com/p/cancer-rates-are-increasing-and-may, “Cancer Rates are Increasing — and May Get Much Worse.” In this post, Mr. Chudov discusses the 9-sigma increase in cancer rates in the United States and a similar rise in the UK. At the time of this post (a little over one year ago), there was suspicion regarding the reason why the modRNA COVID-19 “vaccines” were engendering an increase in cancer diagnoses: the suspicions rested on the use of the “faux” pseudouridine in the “vaccines”; the discovery of “loose DNA” in the “vaccines”; and the genotoxicity of the spike protein itself. By December, 2022, Mr. Chudov was on the trail of the IgG4-induced immune system damage engendered by the “vaccines”: www.igor-chudov.com/p/booster-caused-immune-tolerance-explains, “Booster-Caused IgG4 Immune Tolerance Explains Excess Mortality and “Chronic Covid.” Here, the following paper was referenced regarding the IgG4 “class switch”: www.science.org/doi/10.1126/sciimmunol.ade2798, “Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination”, Pascal Irrgang et al. (In other words, a “class switch” to the “tolerate but don’t clear” IgG4 cells.) The latest post by Mr. Chudov on the issue, that is very specific, is from 26 November 2023: www.igor-chudov.com/p/hyperprogressive-cancers-due-to-covid, “‘Hyperprogressive’ Cancers Due to COVID-Vaccine-Caused IgG4 Antibodies.” The take away from this post: “…IgG4 drives malignancy and aggressiveness of the real-life cancers they observed.” Here is a graphic from Mr. Chudov’s post, taken from this paper: https://jitc.bmj.com/content/8/2/e000661, “An immune evasion mechanism with IgG4 playing an essential role in cancer and implication for immunotherapy”, Hui Wang et al.
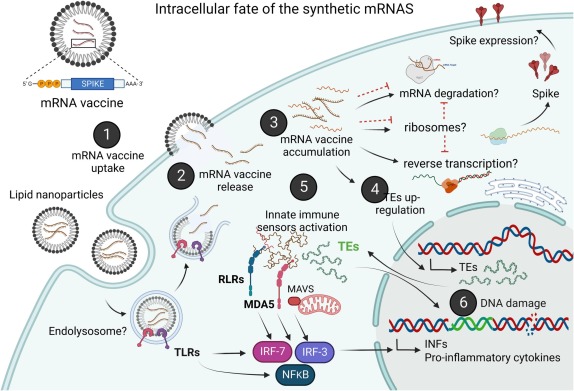
Finally, there is this: https://doi.org/10.1016/j.mehy.2023.111015, “Potential health risks of mRNA-based vaccine therapy: A hypothesis”, by K. Acevedo-Whitehouse and R. Bruno, published on 25 January 2023. It appears that an important key to understanding the mechanisms of the modRNA COVID-19 “vaccines” that can induce sufficient immune system suppression in the “vaccinated” person’s body it that these “vaccines” employ N1-methylpseudouridine. (This ingredient “evades” the body’s natural “immune system defense mechanism.”) The paper also discusses “other contaminants” in the “vaccines” that “…could further alter immune recognition and deregulate immune signalling pathways,…it is not unreasonable to assume that mRNA-based vaccines could induce sustained inflammation and a persistent anti-viral cellular state in various tissues.” (Italics mine) Yours Truly is including a graphic from the paper of what the synthetic RNA “vaccines” do to the cells of the “vaccine” recipient:
Now, as to the COVID-19 virus itself: There are elements within the virus itself that can cause immune system damage; that can change, damage, or destroy B-cells and CD-class cells in the body of the person who contracts a case of the virus; and may have other elements that can pave the way for cancer tumor onset or relapse. Yours Truly refers to this paper, from September 2020 (this was when BNT162b2 was in “clinical trials”): https://doi.org/10.1126/science.abc8511, “Deep immune profiling of COVID-19 patients reveals distinct immunotypes with therapeutic implications”, Divij Matthew et al. Prof. Matthew and his colleagues demonstrate concerning changes in B-cells and CD8 cells in certain COVID-19 infected patients. Certain immunotypes among the patients studied were more affected than others. From the Abstract: “Whereas immunoglobulin G (IgG) levels reportedly drop slightly ~8 weeks after symptom onset (24, 25), recovered patients maintain high spike protein-specific IgG titers (6, 26).” (Bolding mine)
Another view of the toxic properties of the COVID-19 virus itself, especially regarding the inducement of cancer, is here: https://wmcresearch.substack.com/p/sars-cov-2-the-spike-protein-and, “SARS-CoV-2, the Spike Protein and Oncogenesis”, published on 2 November 2023. Walter M. Chesnut discusses his conclusion that the SARS-CoV-2 virus itself, plus its spike protein, change ALL the following body functions: DNA Repair; Cell Division; Apoptosis (natural cell death); Cellular Differentiation; and Cell-Cell Contact/Communication.
So, if the COVID-19 virus itself and its spike protein have properties that can engender the circumstances for cancer tumor onset, growth, and/or relapse, what makes the modRNA COVID-19 “vaccines” even more dangerous in this regard? One will point to the use of the ALC-0159 and ALC-0315 lipid nanoparticles in these “vaccines”, which facilitate entry of the “vaccine” ingredients to every cell of the recipient’s body; and, to the use of the N1-methylpseudouridine in these “vaccines” which “evade” the natural “enemy detection and destruction” processes of the “vaccine” recipient’s body.
In Yours Truly’s opinion, it took time, effort, and detailed investigation, to lab-create the SARS-CoV-2 (COVID-19) virus itself and its spike protein; and, it took time, effort, and detailed investigation, to lab-create and assemble the ingredients (including the COVID-19 virus itself, and its spike protein) that were, and are, present in the modRNA COVID-19 “vaccines.” The FDA knew, back in the summer of 2020, and certainly on 30 April 2021, how dangerous the modRNA COVID-19 “vaccine” BNT162b2 was, and is. Please refer to: www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, FDA time-stamped on 30 April 2021. In fact, the FDA, on that date, knew that at least one IgG4 “class switch” condition was occurring in BNT162b2 “vaccinated” persons — Thrombotic thrombocytopenic purpura (an IgG4 autoimmune disease), listed on page 38 of the report.
Of course, cancer can, and does, occur for other reasons than being engendered by COVID-19 “vaccination” or infection. There are many contributing factors — from genetic predisposition to smoking to accumulated immune system dysfunction, among others. However, while it can be fairly argued that the COVID-19 virus itself, with its spike protein, AND the modRNA COVID-19 “vaccines” based on said virus and its spike protein can, and do, engender cancer tumor growth and/or relapse — the modRNA COVID-19 “vaccines” are more dangerous in this regard. One can posit that it may be valuable for people to learn about family members have/had cancer; what history of cancer “runs in the family”, if any; about family members who have/had immune system issues; and so on. It is absolutely valuable for all people to be in, and remain in, the best physical shape and the best mental-health shape possible. It is absolutely valuable to follow a COVID-19 prevention/prophylaxis protocol.