The free vintage public health poster from World War II about washing the hands is courtesy of Open Culture and Google Images.
Health Friday is a series of information regarding Big Pharma, vaccines, general health, and associated topics.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats by Yours Truly, of which readers should be aware. They are linked here. Note One: Yours Truly has checked today’s offering for any AI-generated content. Other than AI-generated images that may be embedded in URL links, to the best of her knowledge and belief, there is none. If readers wish to post any AI-generated content in today’s discussion thread, they must cite their source. Note Two: Nothing in today’s offering is intended to be, nor shall it be construed as, what might be termed “character assassination” regarding HHS Sec. Kennedy, Jr., or any employee (current or former) of the FDA or of the CDC. Thank you.
Today’s offering is about one topic: It is past time to: first, to shut down the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) divisions of the United States Department of Health and Human Services (HHS); then, second, to rebuild these agencies from top to bottom so that they truly serve the public health of Americans.
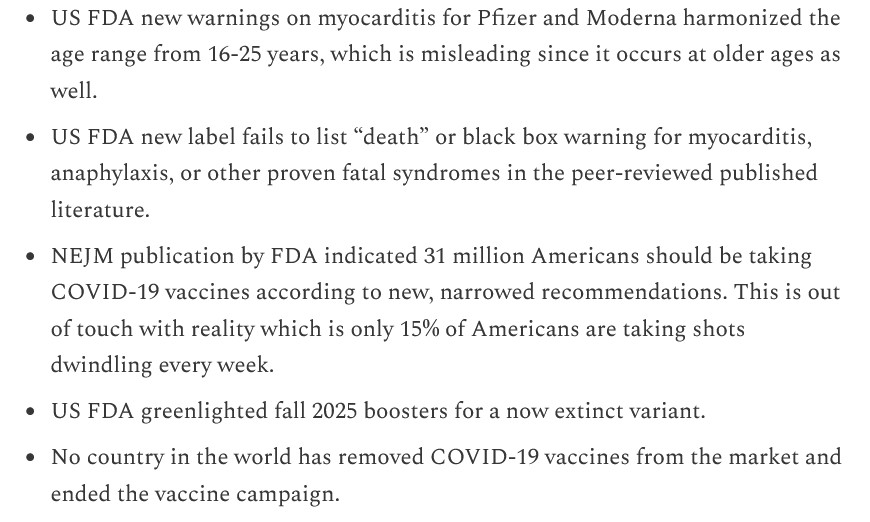
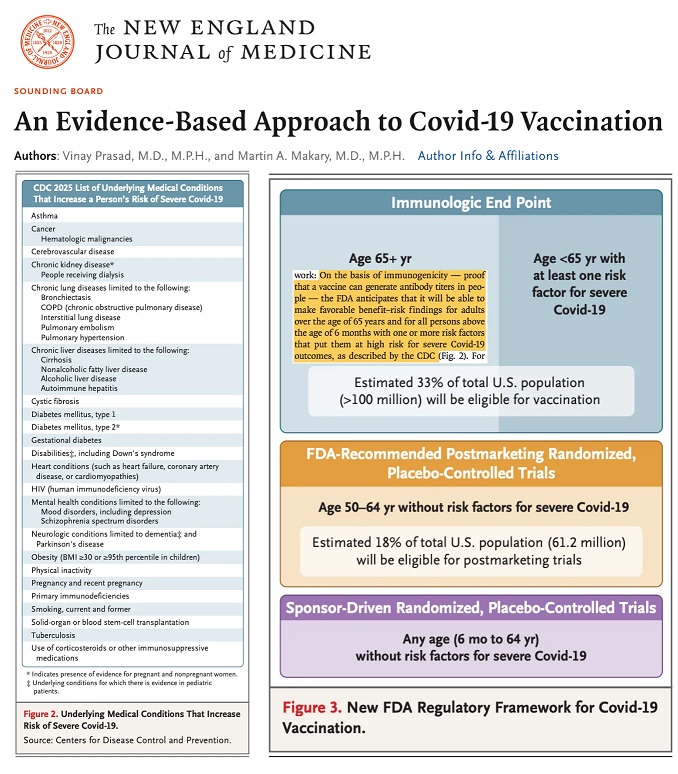
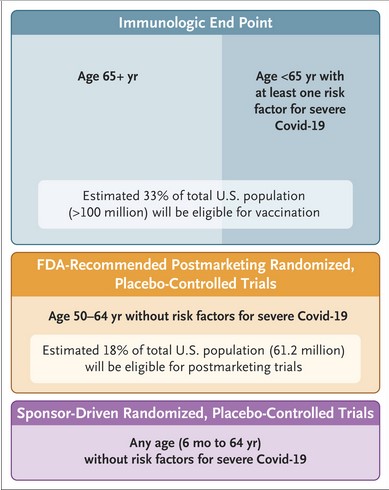
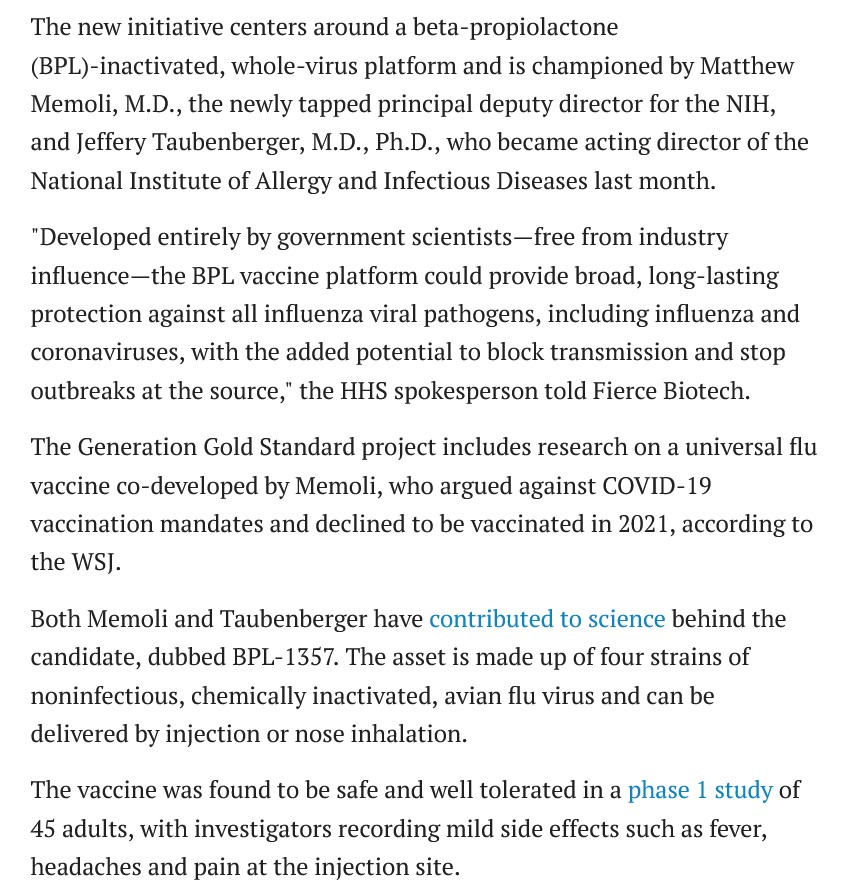
Yours Truly begins here: https://sashalatypova.substack.com/p/another-day-another-episode-of-the, “Another day, another episode of the new FDA lying just like the old FDA…plus self dealing by MAHA Action”, by Sasha Latypova, 28 July 2025. This article regards certain statements by Dr. Martin Makary, the current Commissioner of the FDA. Ms. Latypova worked in Big Pharma for her professional career, designing and helping to implement clinical studies for drugs. She retired from her career when she realized that, in Yours Truly’s opinion, she concluded that it was all part of a “shell game” that was played by Big Pharma. Since retiring, Ms. Latypova has begun a new endeavor: to expose this “shell game.” There are those who may differ with certain of Ms. Latypova’s opinions; however, Yours Truly believes that she is right on the mark on multiple issues. Please see the screenshot from her article, below:


The Latypova 28 July article discusses several aspects of what appears to Yours Truly to be two things: first, an internecine war going on within the FDA; and, second, deep and potentially catastrophic conflicts of interest within certain key employees of the FDA regarding their personal prejudices versus the line of their duties within the FDA. The transcript portion above is from an interview with Dr. Martin Makary (current FDA Commissioner) by Jan Jekielek of American Thought Leaders (ATL) of 16 July 2025; the second screenshot is Ms. Latypova’s considered opinion as to what is going on “behind the scenes.” The Jekielek tweet about this interview, with an embed of the interview itself, is here: https://x.com/JanJekielek/status/1945560472909906288.
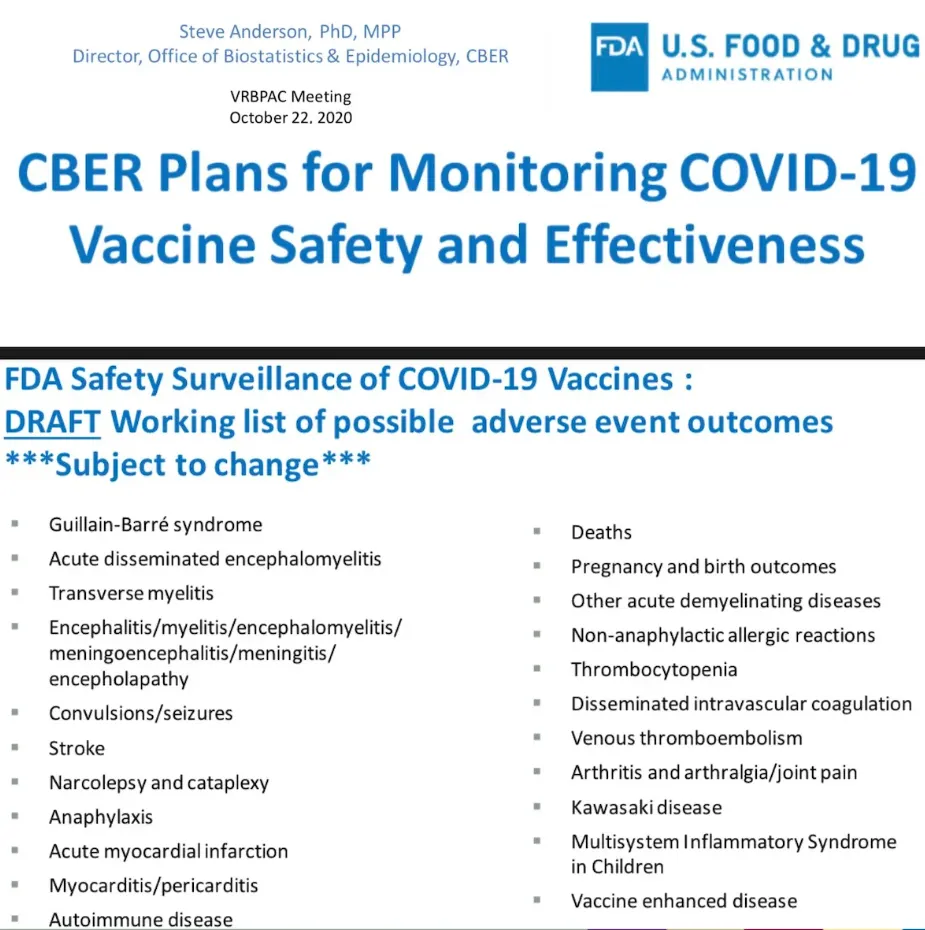
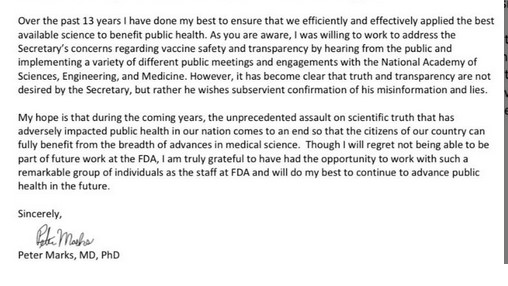
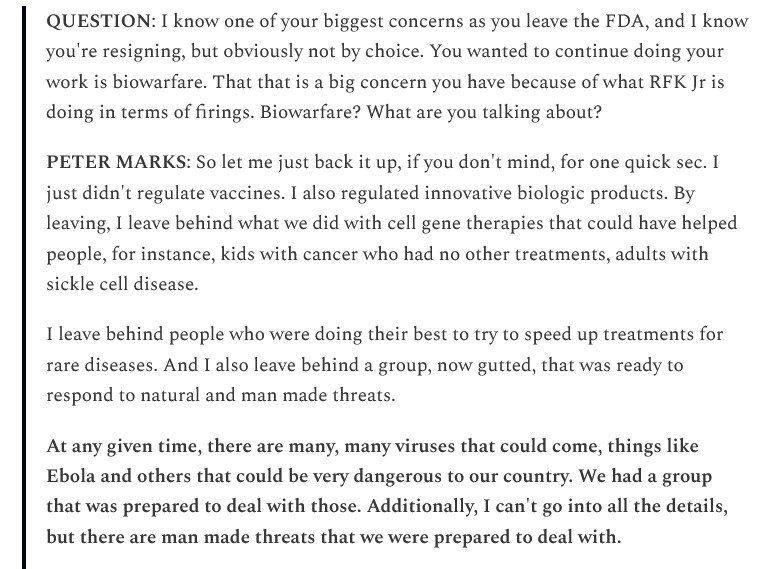
Yours Truly now turns to the case of Dr. Vinay Prasad, the now-former head of the CBER division of the FDA (Center for Biologics Evaluation and Research.) The CBER division of the FDA is responsible, among other duties, to make sure that “biological products” (drugs, vaccines, and so on) are “safe and effective” and are available “to those who need them” (https://www.fda.gov/about-fda/fda-organization/center-biologics-evaluation-and-research-cber). Dr. Prasad joined CBER as the new Director in May 2025, and he resigned abruptly on 29 July 2025. Sasha Latypova wrote the following article about the situation: https://sashalatypova.substack.com/p/breaking-vinay-prasad-is-out-from, “Breaking: Vinay Prasad is out from the FDA!”, 29 July 2025. Please see the screenshot from this article, below:

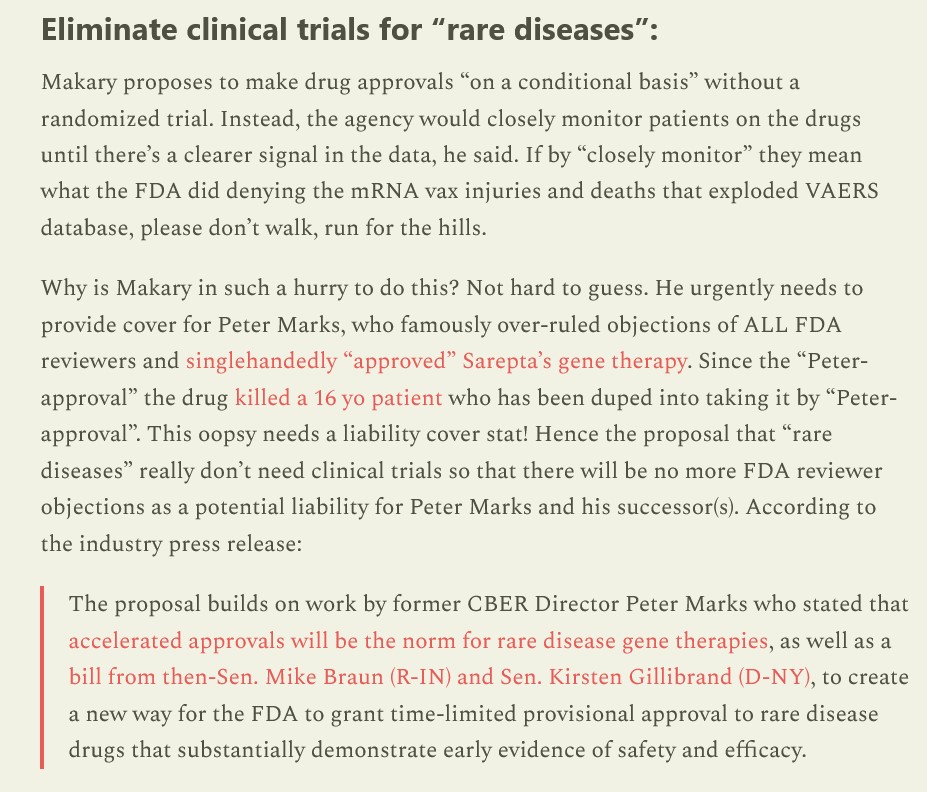
About the Sarepta decision: please see https://sashalatypova.substack.com/p/sarepta-plot-thickens, 25 July 2025, and the screenshot from this article, below:

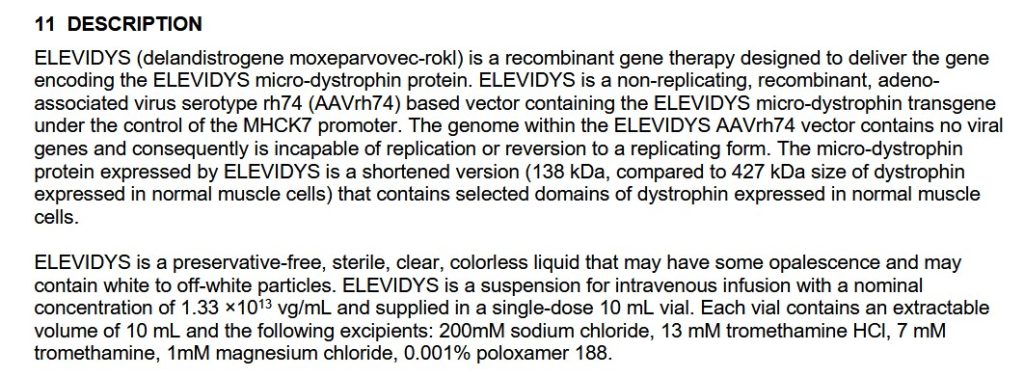
Dr. Prasad was an opponent of the FDA re-instating the use of Elevidys for young people with Duchenne Muscular Dystrophy who can still walk (as opposed to the 18 July 2025 FDA request that the drug be stopped for all Duchenne Muscular Dystrophy patients.) He was overruled by Dr. Martin Makary.
The Latypova article above presents an argument that the FDA re-instatement of Elevidys is profound on several levels — among them, funding for the drug’s manufacturing company, Sarepta. And there are other “ripple effects” from this re-instatement: please see the screenshot of the stock value of Sarepta related to the FDA withdrawal of the drug; then, to the FDA re-instatement:

Yahoo Finance has this article regarding Sarepa, funding, and the Elevidys situation: https://finance.yahoo.com/news/fda-ask-sarepta-halt-elevidys-193245811.html. Please see the screenshot from this article, below:

Elevidys, by the way, has a list of adverse effects and other complications; among them is acute liver injury (this is what killed the patients who passed away after being treated with Elevidys.) Please see the Package Insert for this drug, available here: https://www.drugs.com/pro/elevidys.html, “Sarepta Refused FDA’s Request to Halt Elevidys Shipments”, 18 July 2025.
Regarding the departure of Dr. Prasad from the FDA’s CBER division, there are several “pieces to the puzzle” (and some of these “pieces” are still unknown.) However, Yours Truly has been able to trace the following:
ONE: Please see the items above in today’s offering related to the Sarepta / Elevidys situation and the involvement of Dr. Prasad.
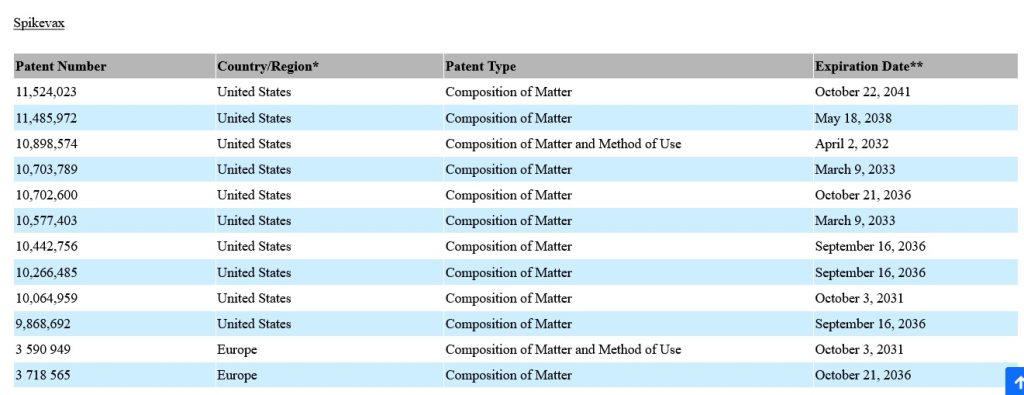
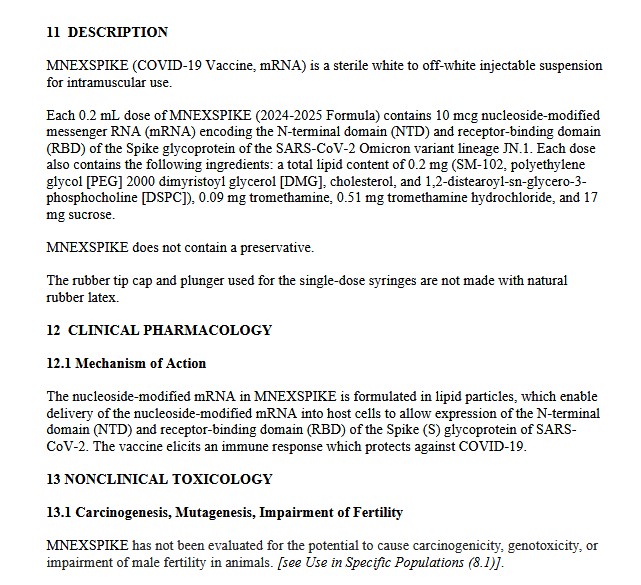
TWO: It was Dr. Vinay Prasad who signed off on the Moderna modRNA COVID-19 “vaccine” SPIKEVAX being used on babies and young children ages 6 months to 11 years old. This “FDA full approval” was signed on 9 July 2025. Dr. Prasad did this signing off on his own authority as Director of the FDA’s CBER division, and without informing HHS Sec. Kennedy, Jr., who was on vacation. However, there is another aspect of the issue: Did Dr. Prasad confer with, and/or communicate with, Dr. Martin Makary, either in advance of, or after, this signing off? Please see: https://www.thegatewaypundit.com/2025/07/now-we-know-who-approved-spikevax-vaccine-children/, “Now We Know the Official Who Approved the Spikevax Vaccine for Children While Robert Kennedy Jr. Was Allegedly on Vacation”, by Jim Hoft, 31 July 2025. Please see a screenshot from this article, below:

THREE: The investigative reporter, Laura Loomer, posted multiple items regarding Dr. Prasad that, in his own words, paint him as a believer in left-wing political positions; as a person who actually despises President Donald Trump 47; and more. The 2nd Smartest Guy in the World Substack article on the Laura Loomer investigation is here: https://www.2ndsmartestguyintheworld.com/p/breaking-vinay-prasad-is-out-at-the, “BREAKING: Vinay Prasad is Out at the FDA”, 30 July 2025. Please see the screenshots from this article, portions of Ms. Loomer’s X posts of her investigation, below:



Laura Loomer’s X post is here: https://x.com/LauraLoomer/status/1947103566239289523.
Last, but not least, is the situation now at the CDC (Centers for Disease Control and Prevention.) The United States Senate, on a strictly “party-line vote”, just confirmed Susan Monarez, PhD, who had been serving as Acting Director of the agency, to be Director of the CDC. Dr. Monarez is a well-known proponent of “vaccines save lives.” Please see: https://apnews.com/article/susan-monarez-cdc-director-senate-hearing-rfk-c7c883f604711238643a9ffd1681bcc0, “CDC nominee Susan Monarez sidesteps questions about disagreements with RFK in Senate hearing”, by Jonel Aleccia, 25 June 2025. Please see the screenshots from this article, below:


Note Dr. Monarez’s emphasis on the role of “public health interventions, including immunizations…”.
Yours Truly’s opinion on all the above in today’s offering is that there are real and divisive issues with the FDA and the CDC, who both appear to be in opposition to HHS Secretary Robert F. Kennedy, Jr. In her opinion, it is time to shut down both agencies and to rebuild them from top to bottom, so that the new entities truly reflect their duty to serve the public health of Americans.
FLASH! JUST ON THE WIRES NOW: https://www.politico.com/newsletters/politico-pulse/2025/07/31/why-trump-ordered-ouster-of-fda-official-00485966, 31 July 2025. It appears that it was President Trump 47 himself who ordered the firing of Dr. Vinay Prasad, overruling both HHS Sec. Robert F. Kennedy, Jr., and Dr. Martin Makary, who opposed Dr. Prasad’s ouster. (Since it’s POLITICO, perhaps a “measure of salt” should be in order… it’s that “people with knowledge of the decision” stuff in the POLITICO article.)
THERE. MUST. BE. ACCOUNTABILITY.
THERE. MUST. BE. JUSTICE.
THERE. MUST. BE. TRUTH.
Peace, Good Energy, Respect: PAVACA