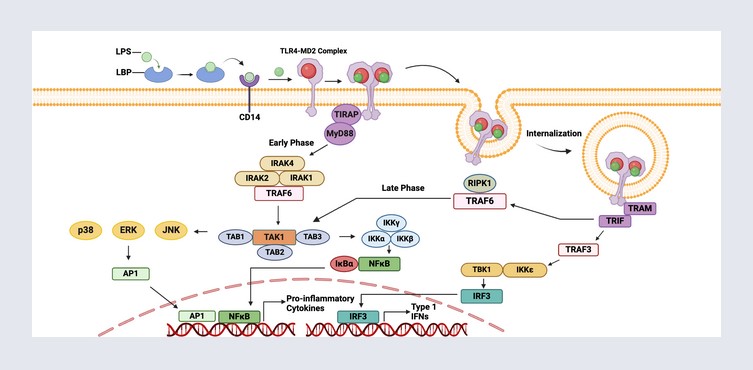
The above image of TLR Signalling Pathways is courtesy of BioFinder and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering is related to the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created Biological Toxin Weapons.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post any AI-generated content in today’s discussion thread, they must cite their source. Thank you.
And now, to the reader’s Edification Smorgasbord, a “feast of information” regarding just how dangerous and potentially deadly mRNA-1283 (mNEXSPIKE) is, Yours Truly offers the following Menu:
APPETIZER: WHAT IS TLR4?
TLR4 (aka Toll-like receptor 4) is a transmembrane protein that exists across a cell membrane. TLR4 functions as a kind of “sensing device” within the body. It detects foreign bacteria and viruses. When a foreign element is detected by TLR4, it begins to send messages to the natural immune system to activate the immune response. TLR4 is crucial to the correct functioning of the natural immune system. Please see the screenshots below for more information:
Citation: https://en.wikipedia.org/wiki/Toll-like_receptor_4
Citation: https://doi.org/10.1016/j.intimp.2007.05.016, “Toll-like receptors in inflammation, infection and cancer”, Keqiang Chen, et al., October 2007. Found via: https://www.sciencedirect.com/topics/immunology-and-microbiology/tlr4.
FIRST COURSE: THE FDA APPROVES “mNEXSPIKE” IN MAY 2025:
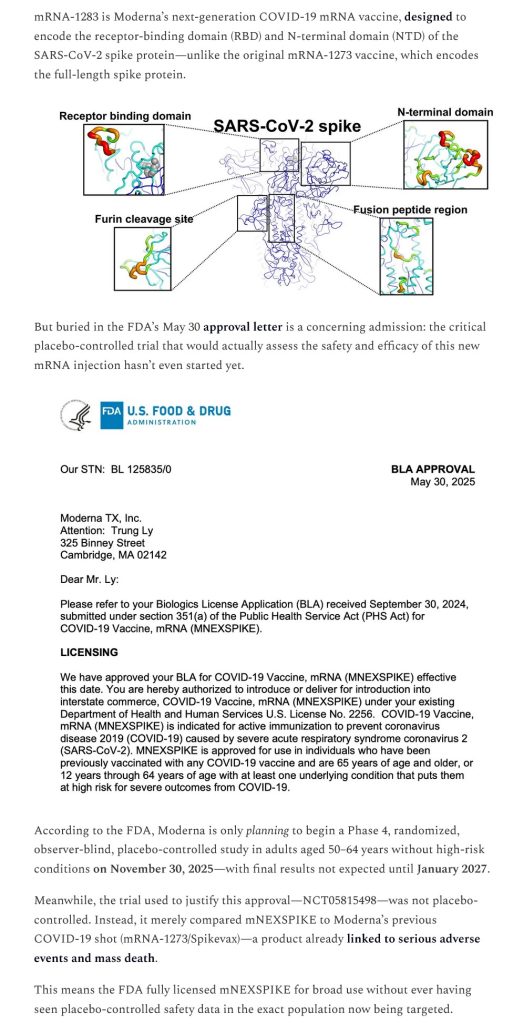
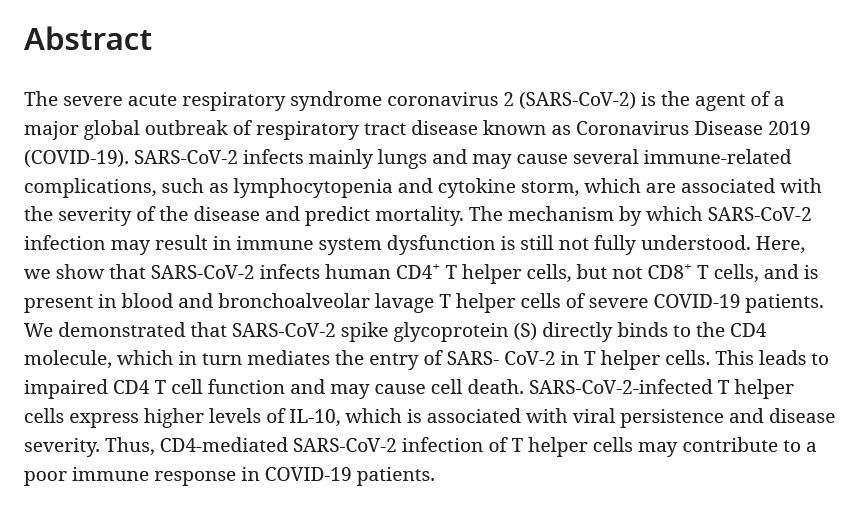
The “newest version” COVID-19 “vaccine”, mRNA-1283 (aka mNEXSPIKE), was “fully approved” by the FDA on 30 May 2025. Yours Truly wrote about this situation here: https://www.theqtree.com/2025/06/01/stop-press-edition-hhs-secretary-robert-f-kennedy-needs-to-resign-now/. This “vaccine” claims to be “more effective” in “preventing” an infection of COVID-19. The claim is based on the fact that mRNA-1283 (aka mNEXSPIKE) uses “only” the S1 protein and the N sector of said S1 protein of the COVID-19 virus spike protein, as opposed to using the entire spike protein (as in mRNA-1273, the original “flagship” modRNA COVID-19 “vaccine” by Moderna.) Please see: https://doi.org/10.1093/infdis/jiaf022, “Safety and Immunogenicity of SARS-CoV-2 Spike Receptor-Binding Domain and N-Terminal Domain mRNA Vaccine”, Spyros Chalkias, et al., 15 April 2025 (most of the authors of this “informational paper” are either affiliated with Moderna, or are employees of Moderna.) A screenshot of the Background section of the Abstract of this paper is below:
At first glance, this “new development” by Moderna may appear to be a “positive” achievement. However, there are other issues that arise:
First, there is the fact that the S1 protein of the SARS-CoV-2 virus contains both the RCB (Receptor-Binding Domain) AND the N-terminal domain of the virus. It is the RCB that allows the virus to “attach” itself , or to “dock” itself, to cells in the body — for example, to the ACE2 cell receptors; and, to TLR4 cells. The N-terminal domain is the “end part” of the S1 protein; it is a “free” group at the end of the protein, while, at the same time, it “initiates” a polypeptide chain.
Second, there is the fact that the S1 protein of the SARS-CoV-2 virus interacts with TLR4 cells. Yours Truly begins with this: https://news-medical.net/news/20210510/Research-suggests-Pfizer-BioNTech-COVID-19-vaccine-reprograms-innate-innate-immune-responses.aspx, Sally Robertson, B.Sc., 10 May 2021. Please see the following screenshots from this article:

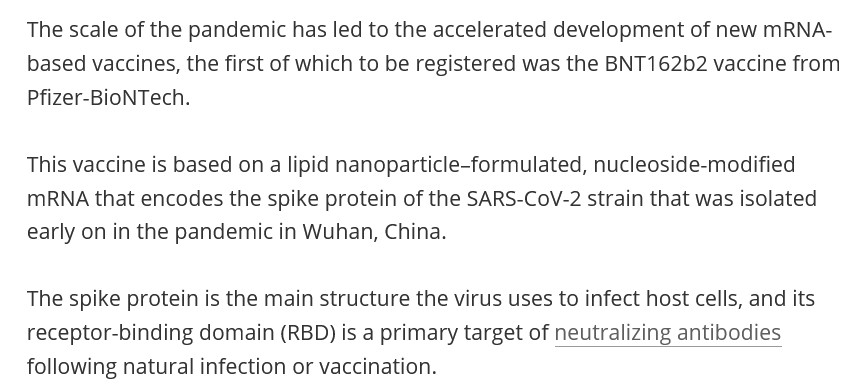
While the above article refers to the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2, the modRNA COVID-19 “vaccine” from Moderna, mRNA-1273, also targets the RBD, which interacts with TLR4 cells in the “vaccinated” person’s body. In addition, all of the modRNA “descendant clone” COVID-19 “vaccines” by both companies also use the RBD, there interacting with TLR4 cells in the “vaccinated / boosted” person’s body.
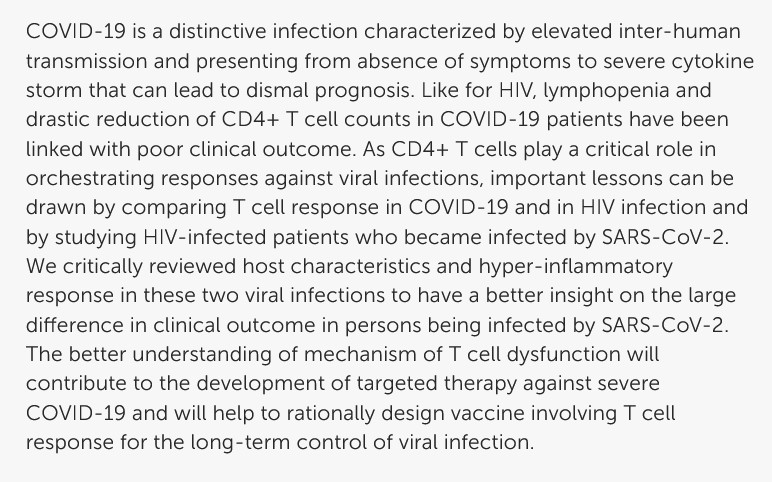
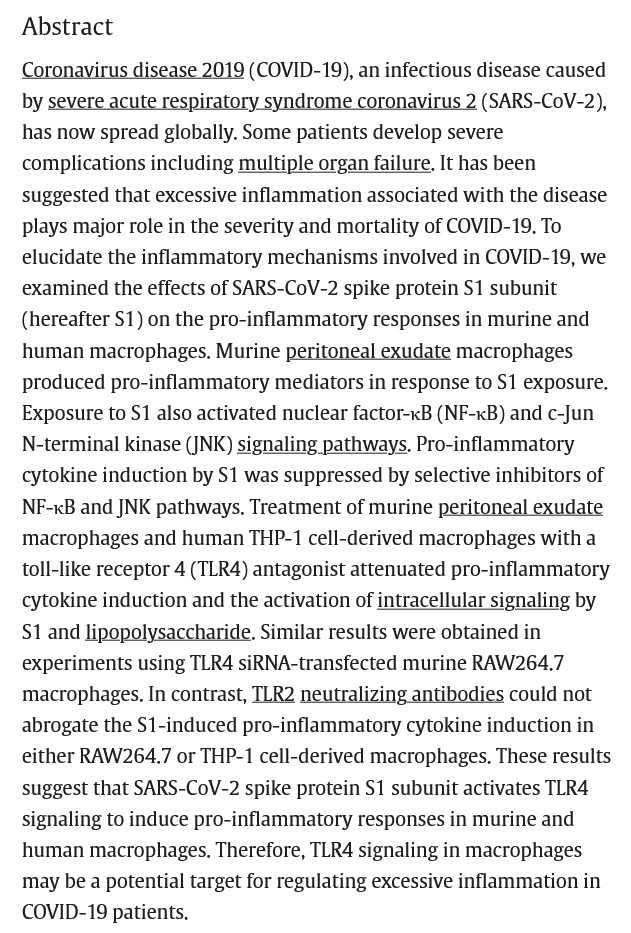
TLR4 cells are also present in multiple areas and organs of the body. The modRNA COVID-19 “vaccines” will interact with these cells. This is due to the fact that the S1 protein of the SARS-CoV-2 virus contains certain amino acids residues (numbers 1-1208) that interact with TLR4 cells. Please see: https://doi.org/10.1016/j.heliyon.2021.306187, “SARS-CoV-2 spike protein S1 subunit induces pro-inflammatory responses via toll-like receptor 4 signaling in murine and human macrophages”, Ken Shirato, Takako Kizaki, February 2021. A screenshot of the Abstract of this paper follows:
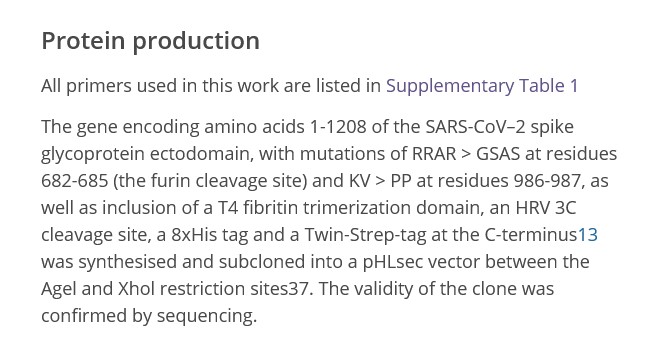
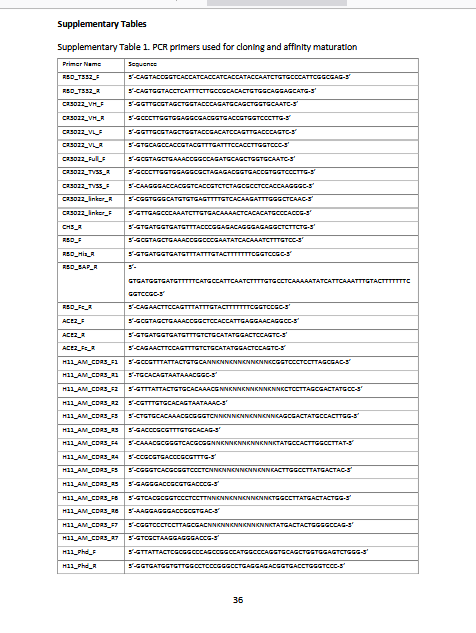
Regarding the S1 amino acids residues 1-1208 and TLR4, please see this paper, from 2020: https://europepmc.org/article/ppr/ppr170060, ” Structural characterization of a nanobody derived from a naive library that neutralizaes SARS-CoV-2″, M Dumoux, et al., 1 June 2020. Below are screenshots from the Methods section and from a portion of the Supplementary Table section of this paper (the Supplementary Table portion shows some of the gene code for the S1 1-1208 residues):
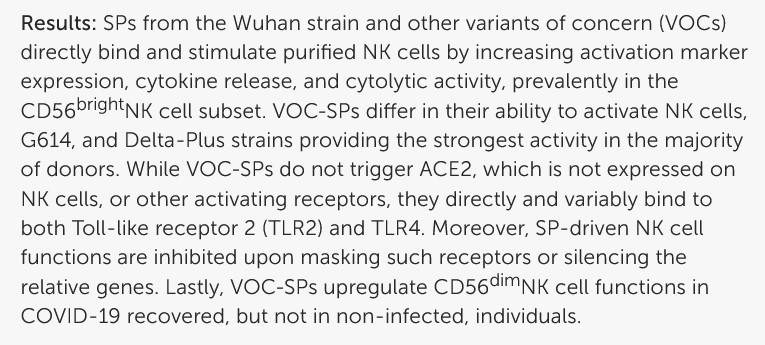
Further information regarding SARS-CoV-2 spike protein and its interaction with TLR4 is found here: https://doi.org/10.3389/fimmu.2024.1368946, “TLR2/4 are novel activating receptors for SARS-CoV-2 spike protein on NK cells”. Nadine Landolina, et al., 30 May 2024. “NK” stands for “Natural Killer” cells in the body. A screenshot from this paper is below:
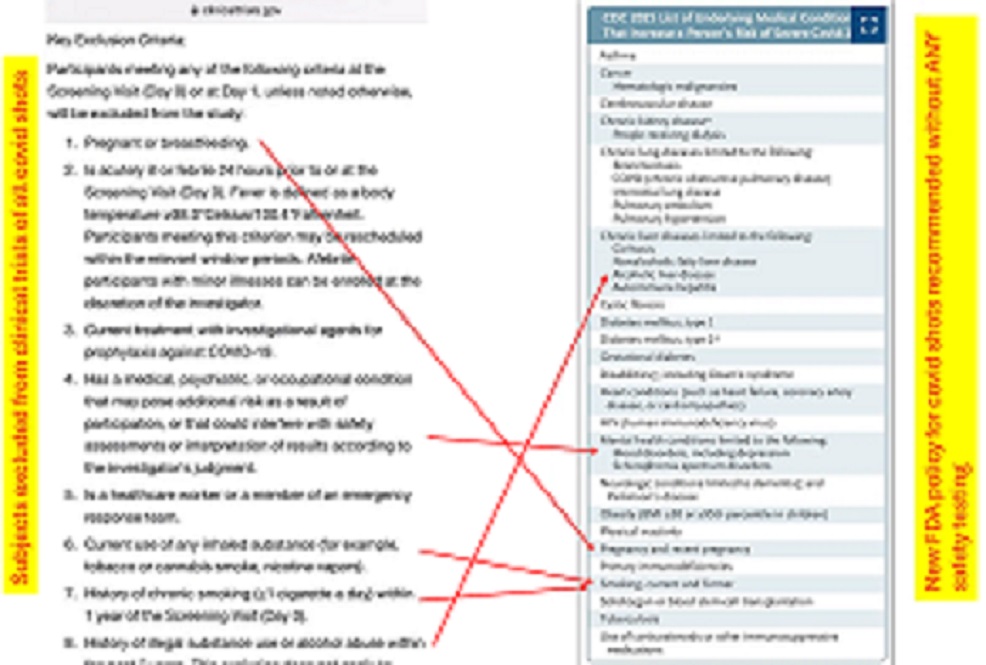
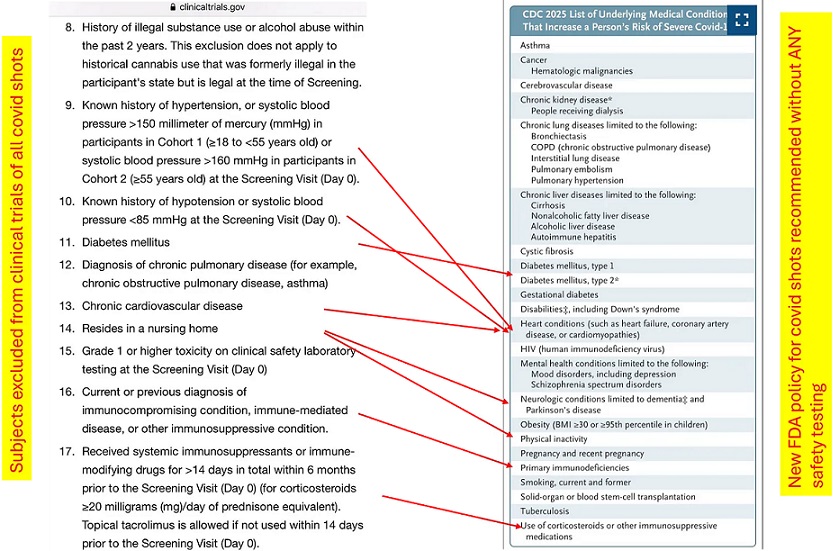
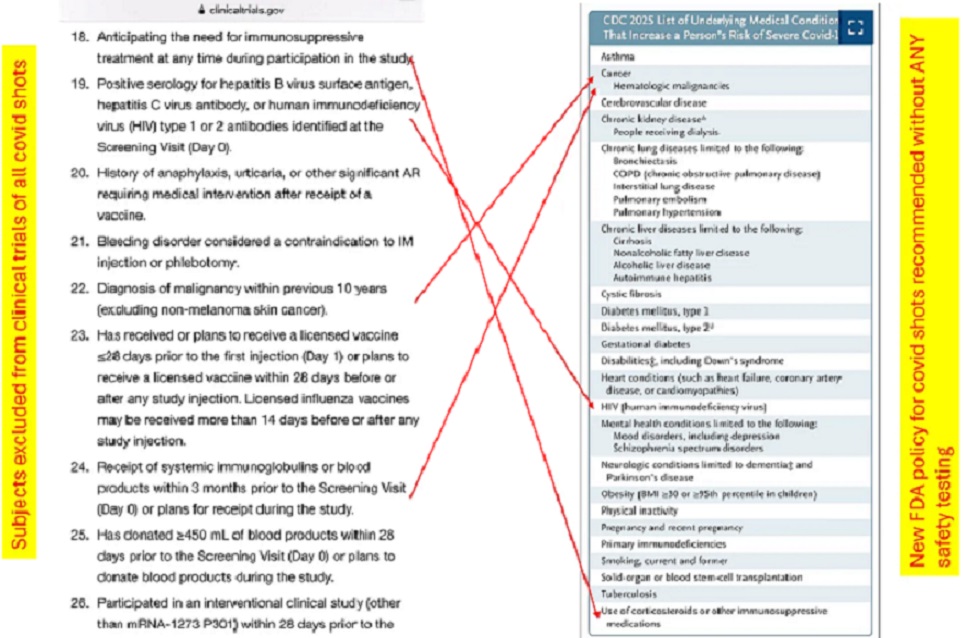
Then, there is the issue of clinical trial used by the FDA to “justify” the “full approval” of mRNA-1283 (aka mNEXSPIKE), NCT05137236 (https://clinicaltrials.gov/study/NCT05137236.) There was NO Placebo Control Group in this study. The study participants (study subjects) were injected with the following Moderna modRNA COVID-19 “vaccines”: mRNA-1273; OR, mRNA-1283; OR, mRNA-1283.211; OR, mRNA-1283.529. Why was there no Placebo Control Group? Assuming that the study subjects knew, in advance, they would be injected with any one of FOUR different variations of a modRNA COVID-19 “vaccine”, were they fine with that?
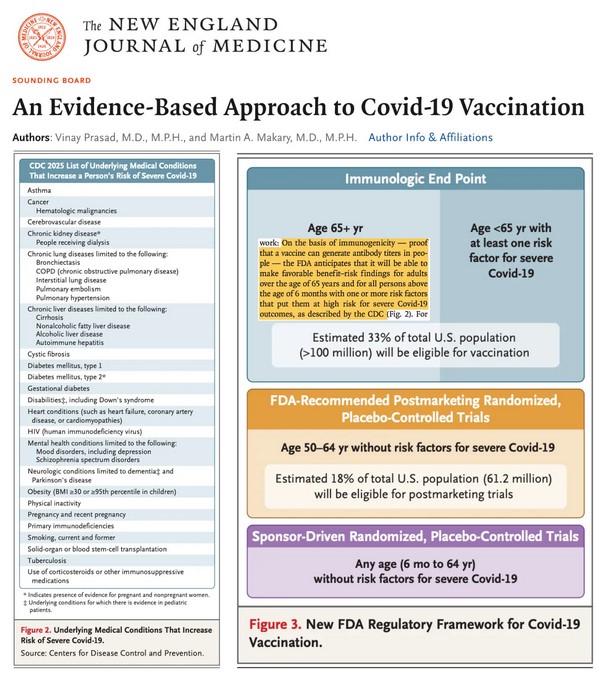
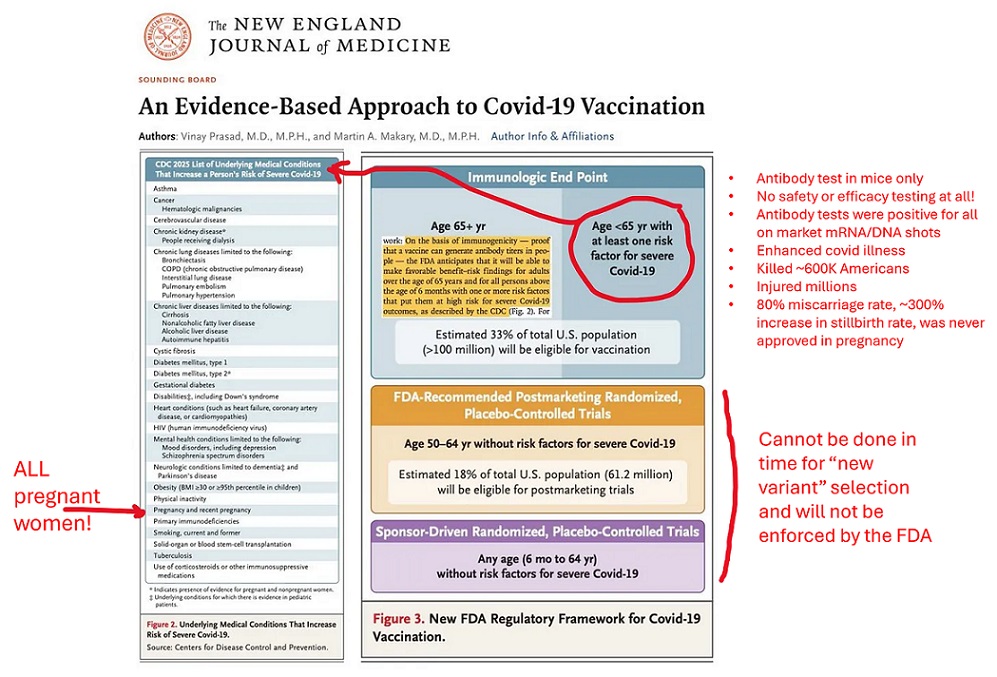
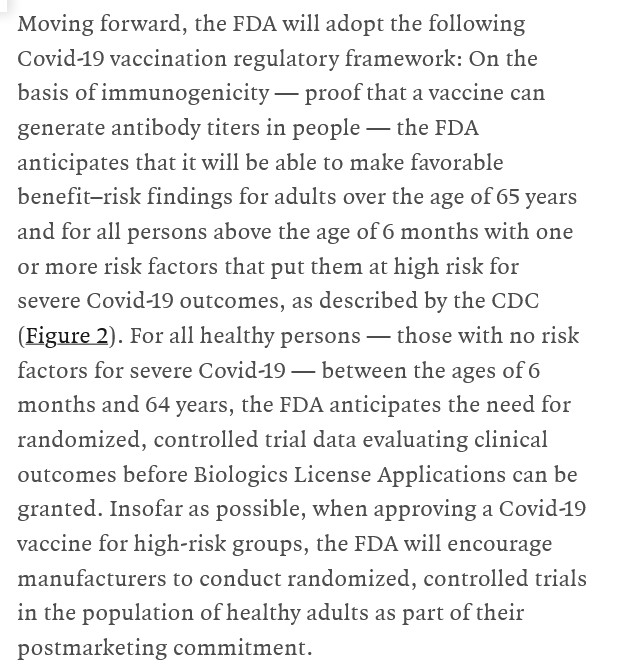
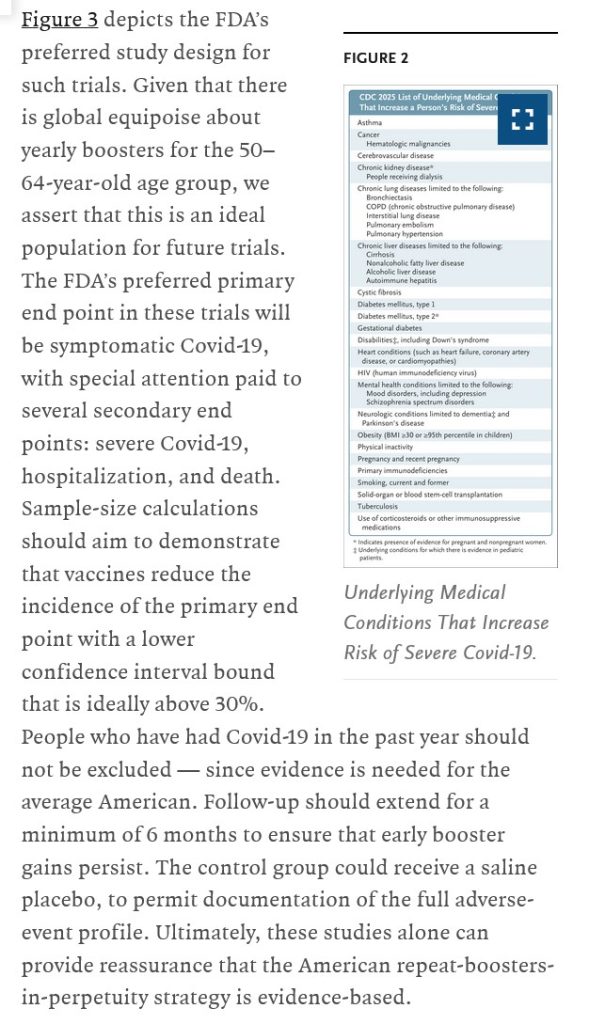
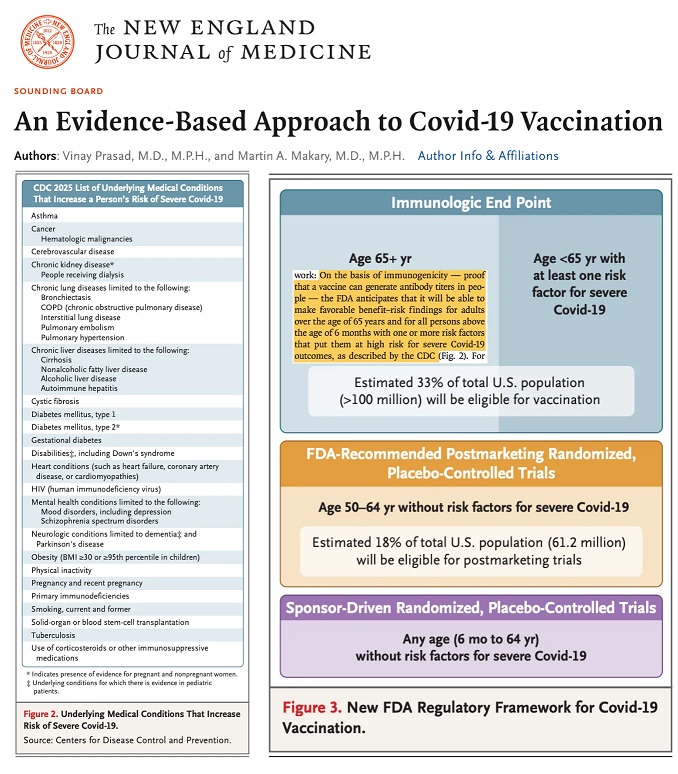
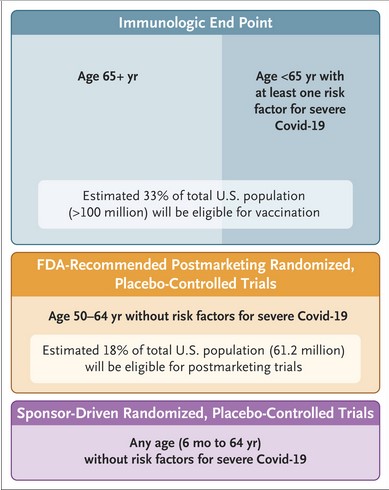
And, there is the “opinion piece” by Dr. Martin Makary (FDA Commissioner) and Dr. Vinay Prasad (new head of the FDA’s CBER division), regarding the “new approach” that the FDA will use for COVID-19 “vaccines.” Please see:
SECOND COURSE: WHAT DOES THE modRNA COVID-19 “VACCINE”, mNEXSPIKE, CONTAIN?
Please see the FDA-issued Fact Sheet for Healthcare Providers (aka the Package Insert) for mRNA-1283, mNEXSPIKE: https://www.fda.gov/media/186738/download. Below is a screenshot of section 11 Description, section 12 Clinical Pharmacology, and section 13 Nonclinical Toxicology of this document:
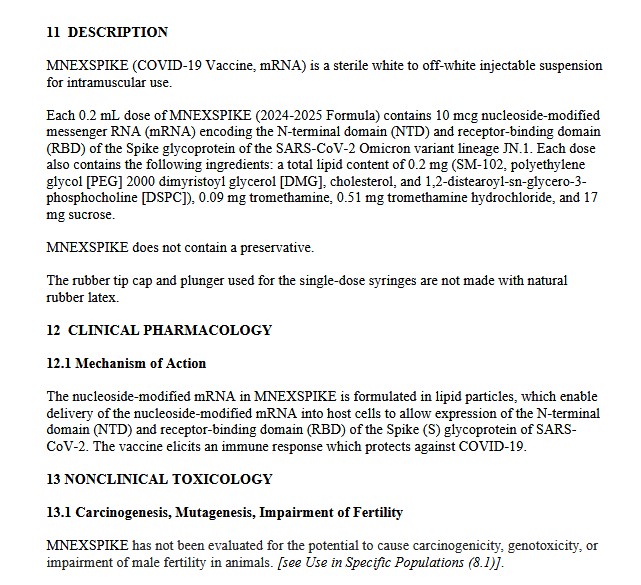
Which plainly states that mNEXSPIKE contains the same types of dangerous, deadly lipid nanoparticle and excipient that all the other modRNA COVID-19 “vaccines” by Moderna contain: SM-102, and PEG2000-DMG. This means that mNEXSPIKE will be rapidly spread into every cell in the “vaccinated” person’s body. It is also clear that mNEXSPIKE has NOT been tested for mutation potential, cancer-inducement potential, or reproductive impairment potential.
Yours Truly then performed a search to ascertain whether or not mNEXSPIKE contains N1-methylpseudouridine. She has written extensively on this board about this lab-created “fake Uridine plus a form of methane”, which completely replaces the natural RNA in the Uridine in the body. Recall that natural Uridine is crucial to multiple body functions and mechanisms: regulation of mood, of learning and memory, and of “gut-brain connection” functions. Lo and behold, the US Patent for mRNA-1283 (aka mNEXSPIKE) does have language describing “various types” of pseudouridine, including N1-methylpseudouridine, are used in all of Moderna’s modRNA COVID-19 “vaccines” — which would also include mNEXSPIKE. The US Patent for mRNA-1283 is found here (US 20240382581A1): https://patents.google.com/patent/US20240382581A1/en?q=(mRNA-1283)&oq=mRNA-1283, “Pan-human coronavirus vaccines”, ModernaTX, published 21 November 2024. Please see sections 0120, 0121, 0122, and 0123 of this document for descriptions of the “various types” of pseudouridine.
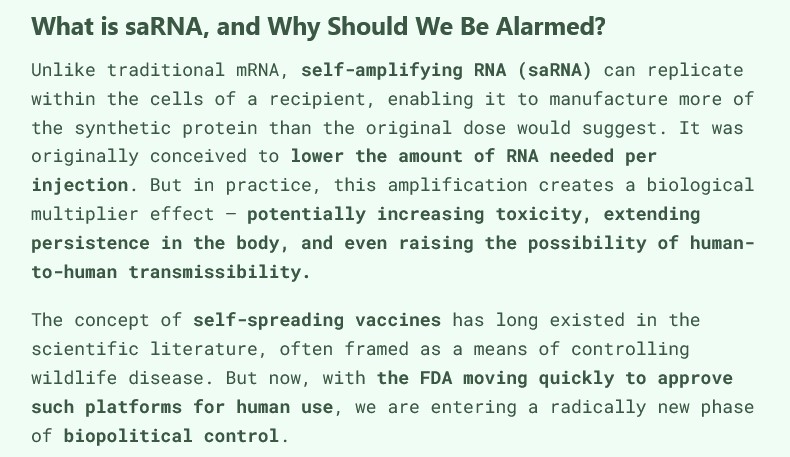
Lastly, there is the question as to whether mNEXSPIKE contains any saRNA (self-amplifying RNA) component. Yours Truly searched for information regarding this, since the IM dose (intramuscular injection dose) of this COVID-19 “vaccine” is a very small amount — 0.2mL. She found this, which appears to be a “dancing all around the truth” description of this “vaccine.” Please see: https://synapse.patsnap.com/article/what-is-mrna-1283-used-for?, 28 June 2024. A screenshot from this article is below:
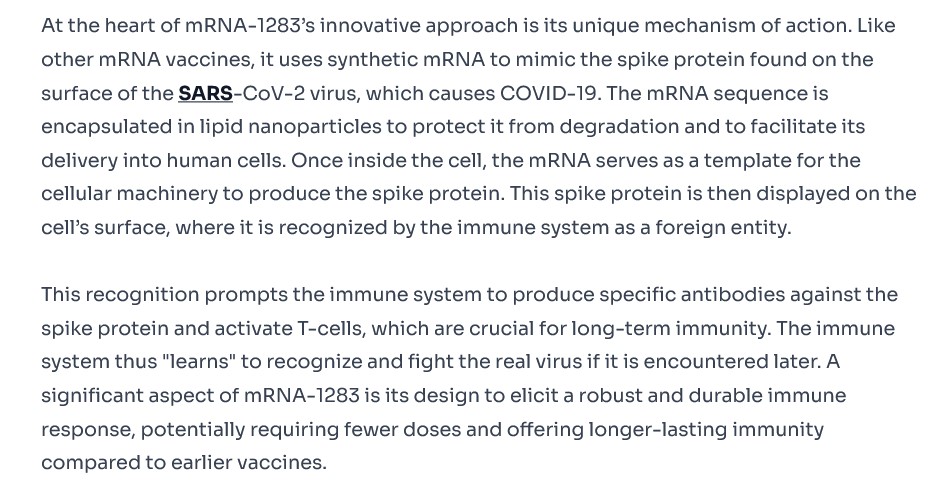
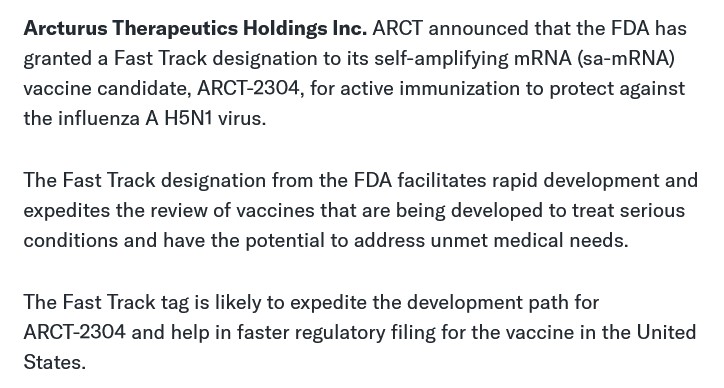
Read the last sentence in the second paragraph above, especially “…a robust and durable immune response, potentially requiring fewer doses and offering longer-lasting immunity compares to other vaccines.” Sounds like a description of the saRNA H5N1 “vaccine”, KOSTAIVE, currently approved for use in the EU / Scandinavia, and in Japan; and, a version of which “vaccine” is to begin clinical trials in the United States (NCT06602531), under the name ARCT-2304.
DESSERT AND BEVERAGES: REACTIONS AND QUESTIONS:
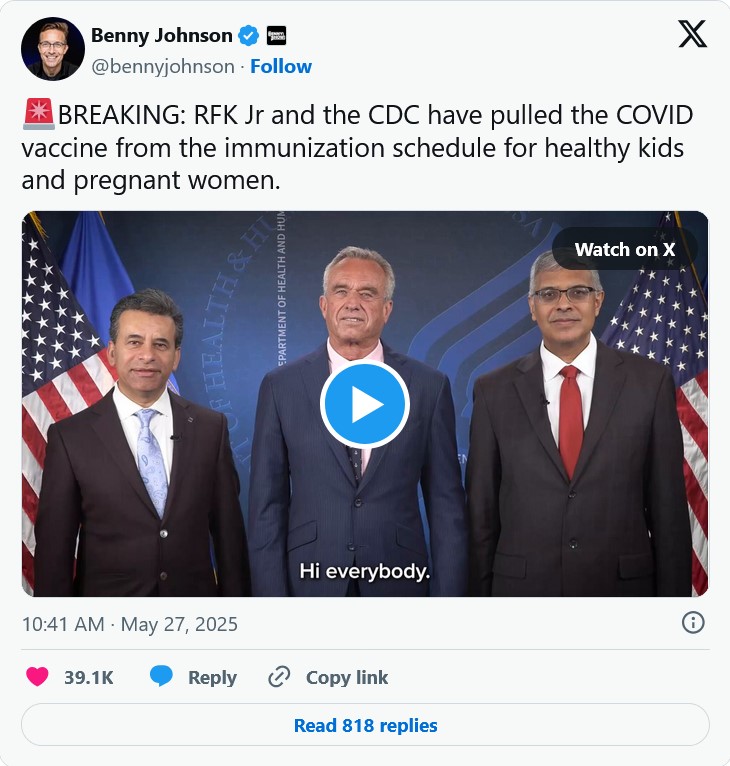
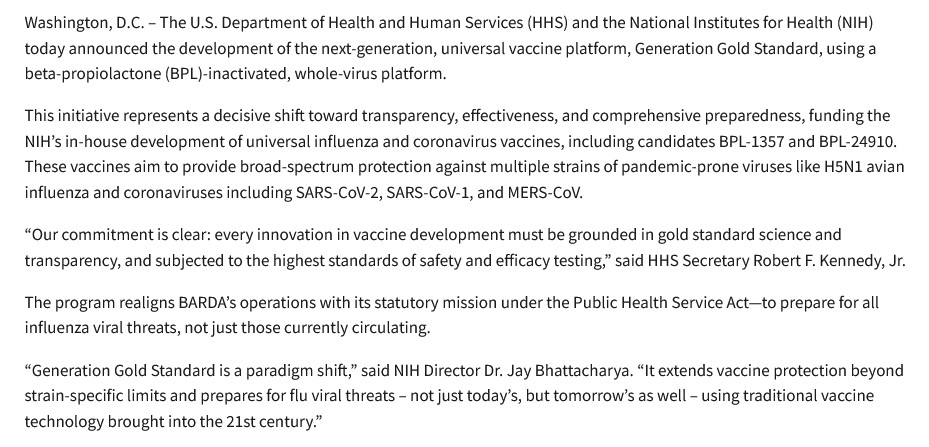
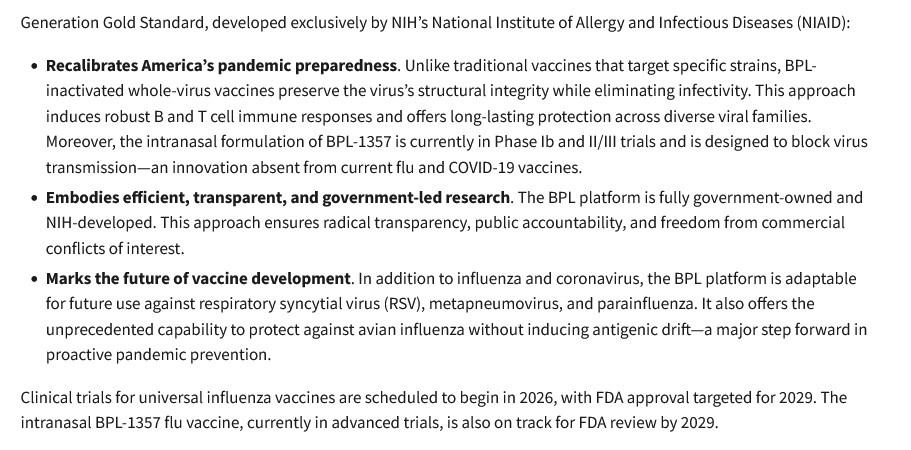
First, this: https://www.thefocalpoints.com/p/maha-movement-flabbergasted-covid, “MAHA Movement Flabbergasted COVID-19 Vaccines Remain on Market”, Peter A. McCullough, MD, MPH, 2 June 2025. There is an embedded interview with Dr. McCullough in this article, along with a linked copy of the “Kabuki Theater performance” regarding “stopping” the COVID-19 “vaccines” in the United States by Dr. Martin Makary (FDA), Dr. Jay Bhattacharya (NIH DIrector), and HHS Secretary Robert F. Kennedy, Jr., on 27 May 2025. A screenshot from the McCullough article is below, giving his views on the current situation:
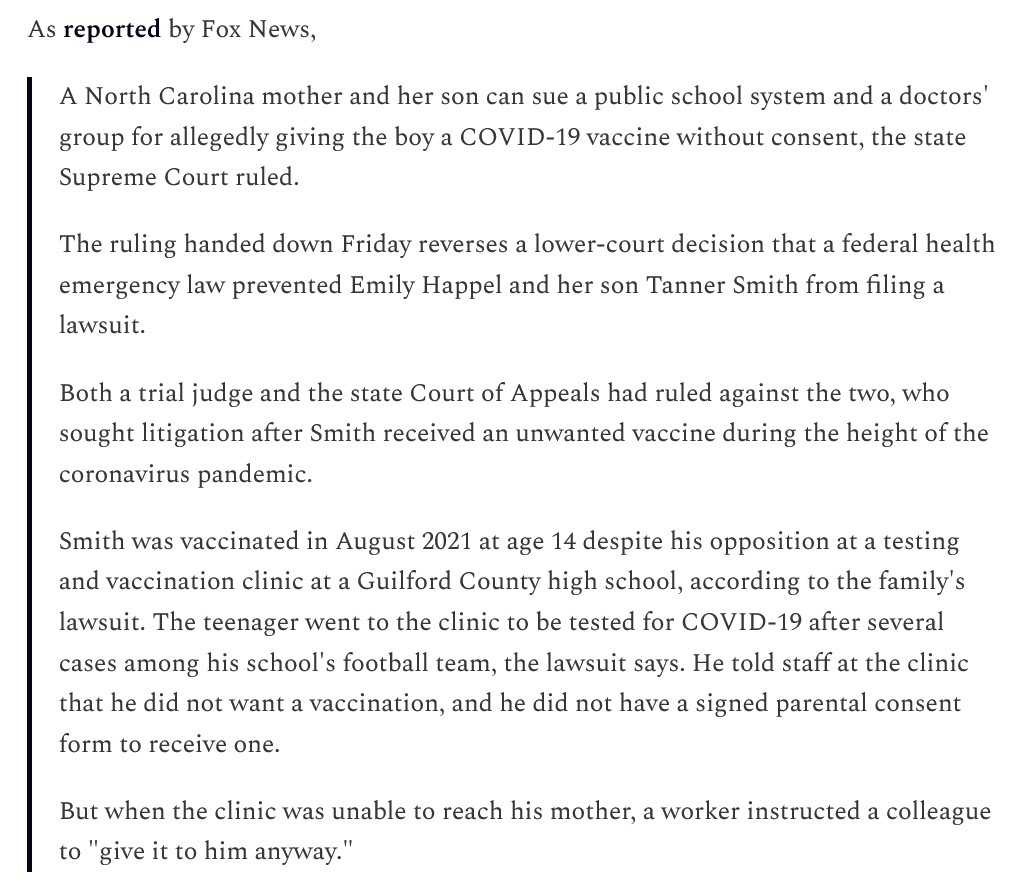
Second, this tweet, from Dr. William Makis: https://x.com/MakisMD/status/1930296443434348771, 4 June 2024. Two screenshots from his tweet are below: first, a statement from HHS Secretary Kennedy, Jr.; and, second, from Dr. Makis:


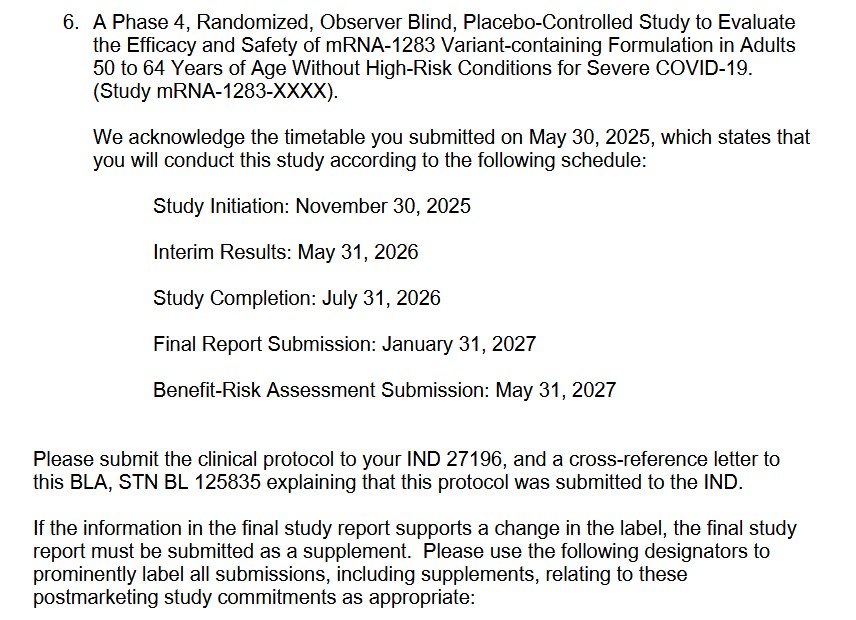
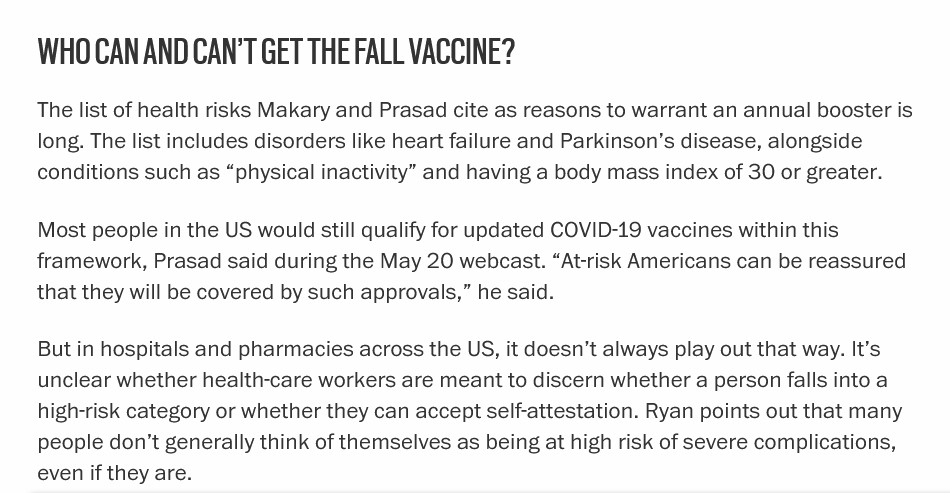
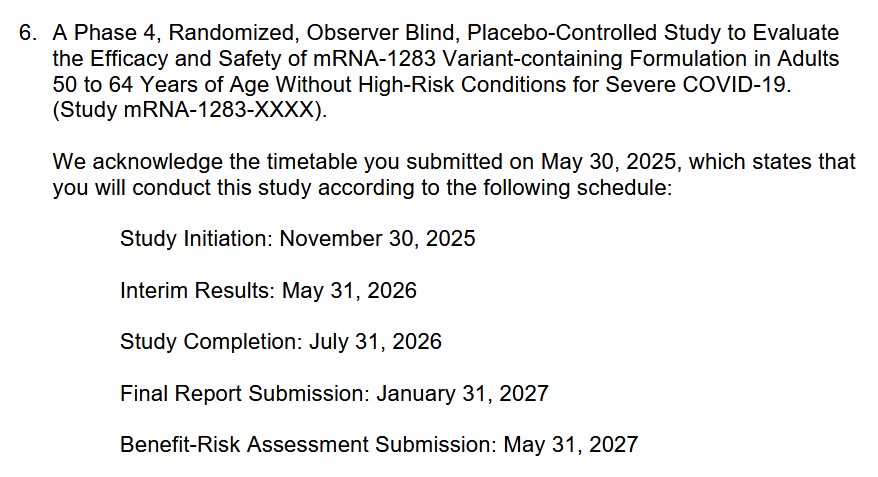
Questions, posed by Yours Truly: Why did the FDA “fully approve” a “new”, modRNA COVID-19 “vaccine” that specifically targets person over age 65, and persons who “fit” a detailed list of “persons at risk of severe COVID-19 infection”, as complied by Dr. Martin Makary and Dr. Vinay Prasad? Why was there a “Kabuki Theater performance” on 27 May 2025 by Drs. Makary and Bhattacharya, along with HHS Secretary Kennedy, Jr., when it was obvious by that date that the FDA “full approval” of mNEXSPIKE was “a done deal”? Why did the FDA issue an Approval Letter to Moderna for mNEXSPIKE that has so many “caveats”, “requests for more information”, and an “order” for the company to perform a Phase 4 clinical study on the “vaccine” — a “vaccine” that the FDA had just “fully approved”? Please see: https://www.fda.gov/media/186740/download; and, the screenshot of Page 9 of this document, regarding the “order” for the Phase 4 study, below:
More questions, posed by Yours Truly: How many elderly persons are going to be pressured / cajoled / “mandated” (by the nursing home or care facility where they live), to take mNEXSPIKE? Will they be told that this injectable is “safer” than mRNA-1273, “because the dose is smaller”? What about persons who “fit” into the multiple categories of “persons at high risk for severe COVID-19 infection” according to Drs. Makary and Prasad? What pressure will these persons be subjected to in order to get them to agree to take mNEXSPIKE? Finally, will people be told the truth that mNEXSPIKE, just because it does not contain the S2 portion of the SARS-CoV-2 spike protein, is NOT “mRNA-1273 Lite” — but, rather, it is another version of a dangerous, potentially deadly modRNA COVID-19 ‘”vaccine”?
Peace, Good Energy, Respect: PAVACA