“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
Author: PAVACA
BFA in Piano; BFA in Music Education; MA in Leadership. Retired professional musician and soprano, teacher, composer, accompanist/coach. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 - 2018), First Professor of the Darden School of the University of Virginia. Writes under the names of: M.E. Forbes; M.E.C. Forbes; PAVACA.
Today’s post is a Placeholder Open Thread for our good Gail Combs. Hoping that all is well with her.
Please, Civil Discussion is practiced here. Please do not give the modern-day version of Cato the Elder the opportunity to show “enmity” to the board.
However, to kick things off, there is this: www.theburningplatform.com/2024/10/01/urgent-the-left-is-going-to-war-on-the-first-amendment/, by Alex Berenson. It appears that John Kerry, who flies around in private aircraft, is making it quite clear that if he and the WEF have their way, free speech will have a large, red “X” target painted on it. Mr. Kerry, who supposedly will “decide” what is “disinformation” and who is “spreading disinformation”, made the following statement during the WEF meeting at which he spoke on Wednesday 25 September:
The above image from an old medical-scientific journal is from PeopleImages, via Google Images.
This post is part of Health Friday, a series of offerings related to Big Pharma, vaccines, general health, and associated topics. The discussion is not limited to what is presented today; it is an Open Thread. However, since this presentation is about a COVID-19 “vaccine”, the post is dedicated to the memory of Yours Truly’s cousin Bill, who died “suddenly and unexpectedly” in September 2023.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here: “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
The U Tree is for “argue it out” interactions. There is a “Featured” article at this site for use as a “Rescue Thread.”
The “third site”, in case the above two are inaccessible.
Civil discussion is practiced here. The excellent and timely Rules of our late, good Wheatie prevail:
One: No food fights.
Two: No running with scissors.
Three: If you bring snacks, bring enough for everyone.
Please follow the added Guidelines from Wolf Moon. Please do not give the modern-day version of Cato the Elder the opportunity to show “enmity” to the board.
The extra items: What Yours Truly presents in this series, as in her other blog posts to this board, is not medical advice — the are opinions and hypotheses based on her over 4 1/2 years (and continuing) of reading about, researching out, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to consult a healthcare practitioner regarding health concerns or conditions.
The Health Friday post today concerns the impending Retraction of a peer-reviewed and published paper that details long-term COVID-19 “vaccine”-induced injuries in North India. The paper was submitted to Springer for review and publishing on 9 January 2024; it was accepted (it had passed the peer-review process); and it was published on 13 May 2024. Here is a free-access version (to read the entire paper on Springer, one has to either access through an institution, or to pay for a copy): www.qeios.com/read/JK7IBA/pdf, “Long-Term Safety Analysis of the BBV152 Coronavirus Vaccine in Adolescents and Adults: Findings from a 1-Year Prospective Study in North India”, Upinder Kaur, et al., 13 May 2024. The study was conducted at Banaras Hindu University in India. BBV152 is another name for the COVAXIN COVID-19 “vaccine”, developed by Bharat BIotech of India in cooperation with Indian Council on Medical Research (ICMR) – National Institute of Virology. ICMR receives “royalty payments” for each dose of COVAXIN that is administered, as does Bharat Biotech (Sound familiar? — as in, the co-development, co-ownership of patents, and sharing of “royalty payments” between the NIAID and Moderna for the modRNA COVID-19, mRNA-1273?)
The Kaur, et al., paper referenced above was published by Springer on 13 May 2024. Almost immediately, the attacks began on the paper, the authors, and the publisher — with articles like this one: https://timesofindia.indiatimes.com/india/1-in-3-covaxin-recipients-hit-by-adverse-events-study/articleshow/110187284.cms, “1 in 3 Covaxin recipients hit by adverse events: Study”, 17 May 2024. On 18 May 2024, the ICMR demanded that Springer retract the paper (Yours Truly: nothing like causing panic in a government agency when the truth is published about a “vaccine” that the agency is pushing as “safe and effective,” especially when that agency is also getting “royalty payments” for the use of the “vaccine”, is there?). But, the attack on Springer and the authors didn’t end there. In July 2024, Bharat Biotech filed a lawsuit against Springer and the authors (some of the authors are students), demanding retraction of the paper and the payment of damages to Bharat Biotech of $600,000 US dollars (50 million Indian rupees.) In addition, the lawsuit accused the paper’s authors of defamation against the company, included with a demand for separate damages to be paid to the company for defamation. Despite sworn statements from the authors that no defamation was intended or written into the paper; and, despite the fact that Nitin Joshi, the editor of the Springer journal (Drug Safety) in which the study appeared, was one of the reviewers who approved the study for publishing, it was Joshi who notified the authors on 28 August 2024 that he was going to have the paper retracted. He confirmed this decision in an email to the authors on 17 September. However, as the defamation lawsuit is now in court, the study is still available on the internet.
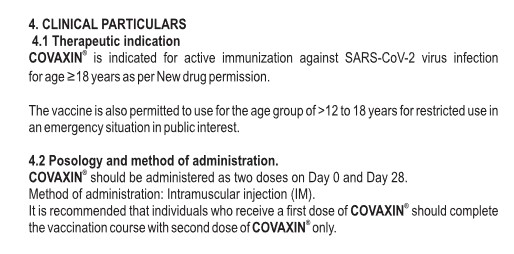
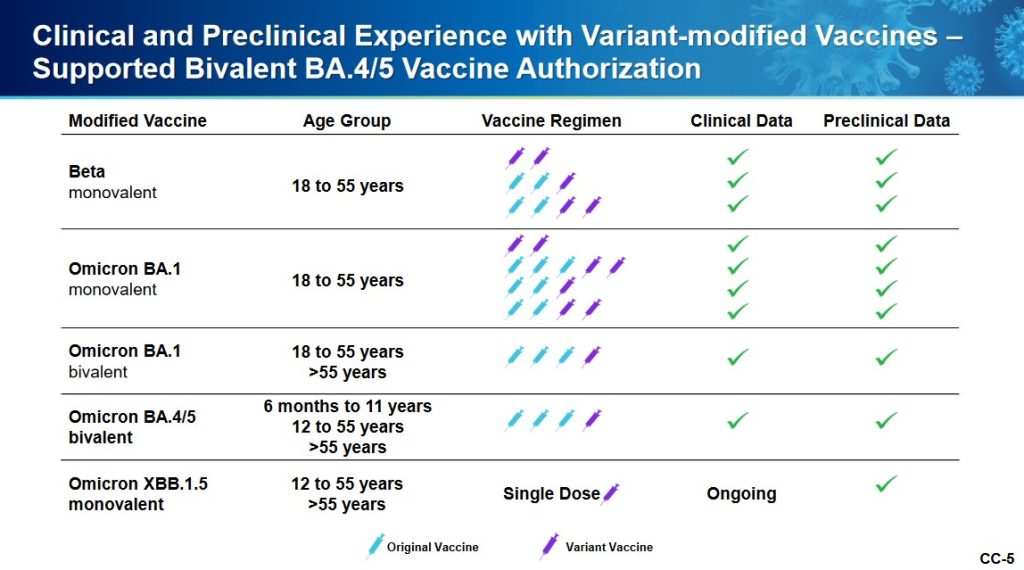
What is BBV152/COVAXIN? It is an “inactivated whole virion vaccine” (whole virus vaccine) for “active immunization” against COVID-19. It is not an mRNA-based/modRNA-based COVID-19 “vaccine”, although it does use an “ancestral wave strain” of the original Wuhan Hu1 SARS-CoV-2 virus (in other words, a strain from the Wuhan Hu1 virus that occurred before the Beta, Delta, or Omicron strains.) The Package Insert for COVAXIN is here: www.bharatbiotech.com/images/covaxin/covaxin-pack-insert.pdf. Below is an image from the Package Insert:
Per Wikipedia, 363,774,435 persons in India had been “vaccinated” with at least one dose of COVAXIN as of 4 March 2023.
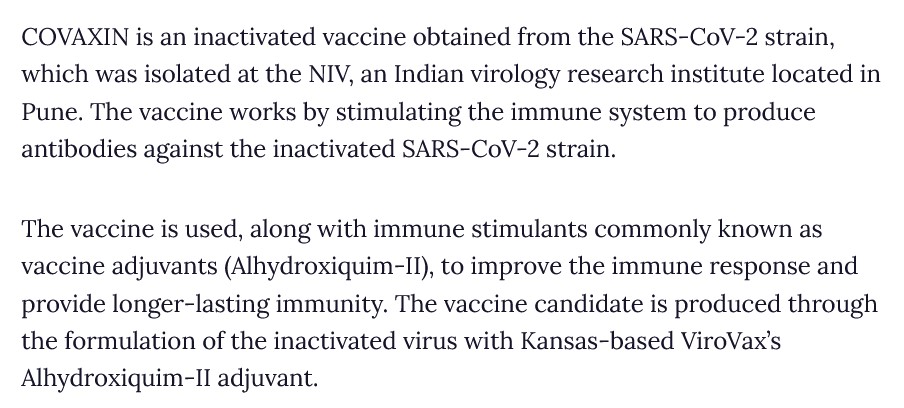
However, the COVAXIN Package Insertdoes not actually describe how the “vaccine” works (the “Mechanism of Action.”) Yours Truly found something along the lines of the necessary information here: www.clinicaltrialsarena.com/projects/covaxin-bbv152-for-the-treatment-of-covid-19/?cf-view&cf-closed, “COVAXIN (BBV152) for the Treatment of Covid-19, India”, 28 June 2022. Below is a screenshot from this article:
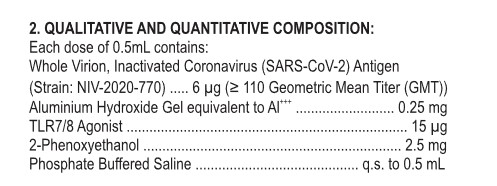
But, COVAXIN has been hailed by the Indian government about being “the first indigenous COVID-19 vaccine in India” (www.bharatbiotech.com/covaxin.html.) Why is ViroVax involved? (More on this later in the post.) Back to the Package Insert for COVAXIN. Below is a screenshot of the ingredients used in this “vaccine”:
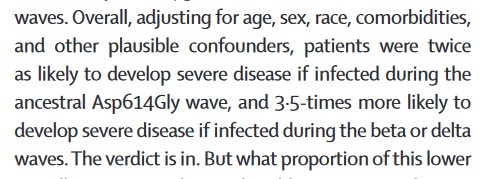
Looking further into the ingredients list, starting with the NIV-2020-770 strain of SARS-CoV-2: please refer to this paper: www.ncbi.nlm.nih.gov/pmc/articles/PMC7825810/, “Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: a double-blind, randomised Phase 1 trial”, Krishna Mohan Vadrevu, et al., May 2021. It appears that NIV-2020-770 (the “inactivated whole virion”) is part of the Asp614Gly variant chain of the SARS-CoV-2 virus. The Asp614Gly variant itself is apparently part of the “ancestral wave” of the original Wuhan Hu1 SARS-CoV-2 virus; and, it is “not as serious” as the Beta or the Delta waves of the virus. Please refer to this article: www.thelancet.com/pdfs/journals/langlo/PIIS2214-109X(22)00199-1.pdf, Vol.10, July 2022, a Comment “Decoding the next SARS-CoV-2 variant”, by Jeremy Nel and WD Francois Venter. Below is a screenshot of a portion from the Comment:
Thus, BBV152/COVAXIN cannot be considered to be one of the “most recent” types of COVID-19 “vaccines”, as it does not include any elements before the Beta, Delta, or Omicron variants.
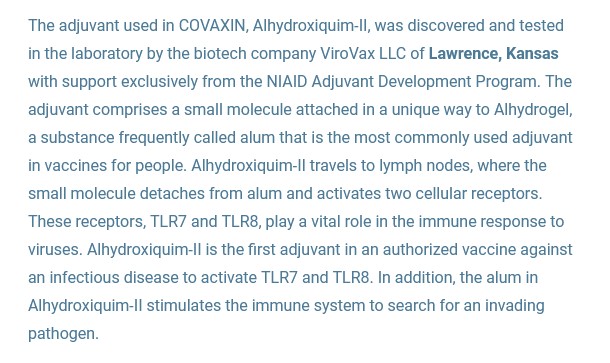
The Aluminium Hydroxide Gel in the ingredients (it is an “excipient” [“adjuvant]”): this is also called “Algel-IMDG” and “Alhydroxiqium-II” — in other words, it is a hydrogel. It was invented by ViroVax LLC of Lawrence, Kansas, under the aegis of the EpscoR Idea Foundation (part of the National Science Foundation in the United States), and with funding by the NIAID. This is the ViroVax / United States government connection. Here is a screenshot from an article by the EpscoR Idea Foundation on this “success story” (www.epscorideafoundation.org/success-stories/kansas-adjuvant-developed-with-nih-funding-enhances-efficacy-of-indias-covid-19-vaccine):
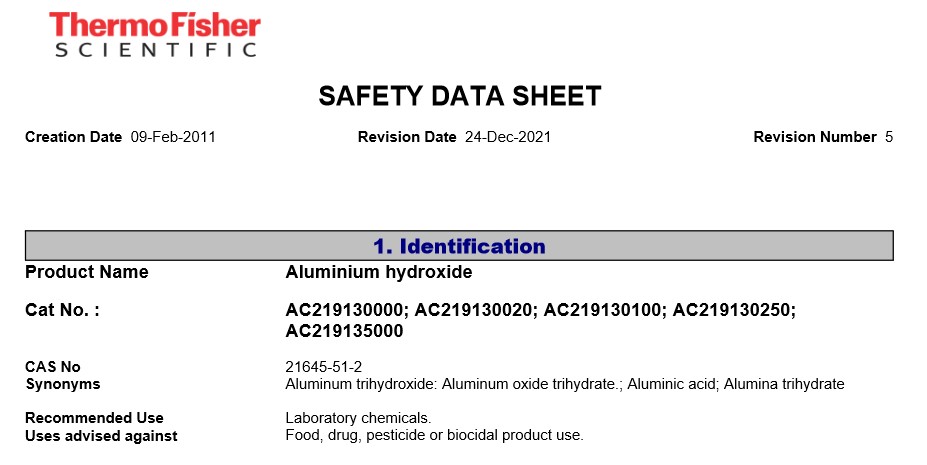
Note that Alhydroxiqium-II targets the lymph nodes of the person who takes COVAXIN. So, while this excipient is not exactly a lipid nanoparticle (LNP), it, in Yours Truly’s opinion, basically functions like an LNP in targeting the lymph nodes for delivery of the “vaccine payload” of COVAXIN; and, by “stimulating” the “vaccinated” person’s natural immune system to go and “search” for invading pathogens. By the way, Aluminium Hydroxide Gel is not to be used in foods, drugs pesticides, or “biocidal” products — see the screenshot below, from the search on Fisher Scientific (ThermoFisher) about this chemical, Page 1:
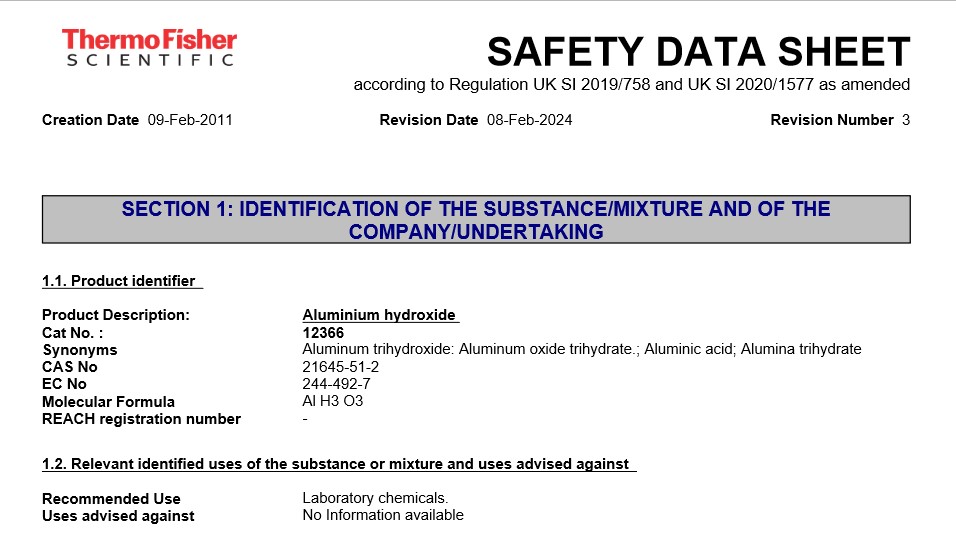
HOWEVER, it appears that FisherScientific had a “change of heart” since December 2021 regarding the “Uses advised against” for Aluminium Hydroxide — below is their MSDS Safety Sheet as of February 2024, Page 1:
Here is another source for an MSDS Safety Sheet, this one specifically for Aluminium Hydroxide Gel:www.oxfordlabfinechem.com/msds/ALUMINIUMHYDROXIDEGEL.pdf. Please see section 3Hazards Identification; and section 11Toxicological Information Special Remarks on Other Toxic Effects on Humans. Below is part of the Special Remarks portion of section 11:
The TLR7/8 excipient (adjuvant) in COVAXIN: This one is used in immunotherapy, including in the treatment of HIV-1. Please see: https://doi.org/10.3389/fmicb.2023.1033448, “Novel TLR7/8 agonists promote activation of HIV-1 latent reservoirs and human T and NK cells”, Yangyang Li, et al., 26 January 2023. This begs the question, Why is an HIV-1 immunotherapy treatment element being used in a COVID-19 “vaccine?” This also, in Yours Truly’s opinion, removes any consideration of COVAXIN to be labeled a “vaccine” — it is actually a gene therapy/immunotherapy injectable.
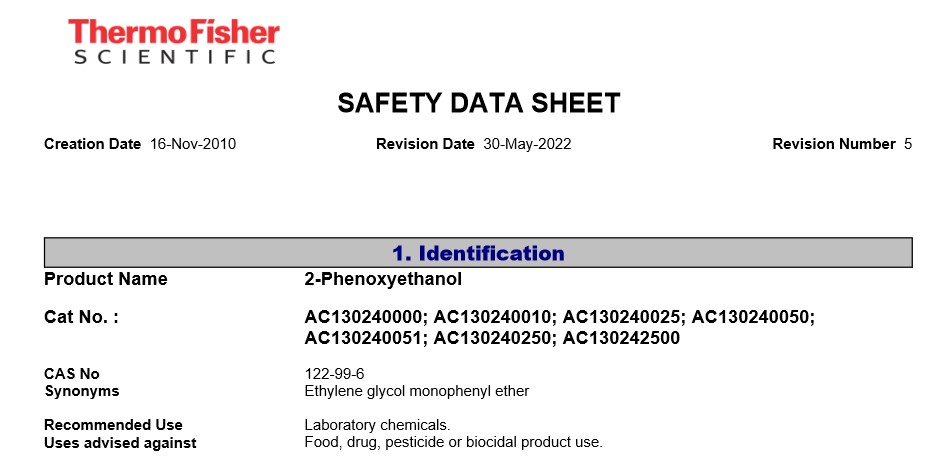
And, the 2-Phenoxyethanol excipient (adjuvant) in COVAXIN. Below is a screenshot portion of the Fisher Scientific (ThermoFisher) MSDS Safety Sheet for this chemical, Page 1:
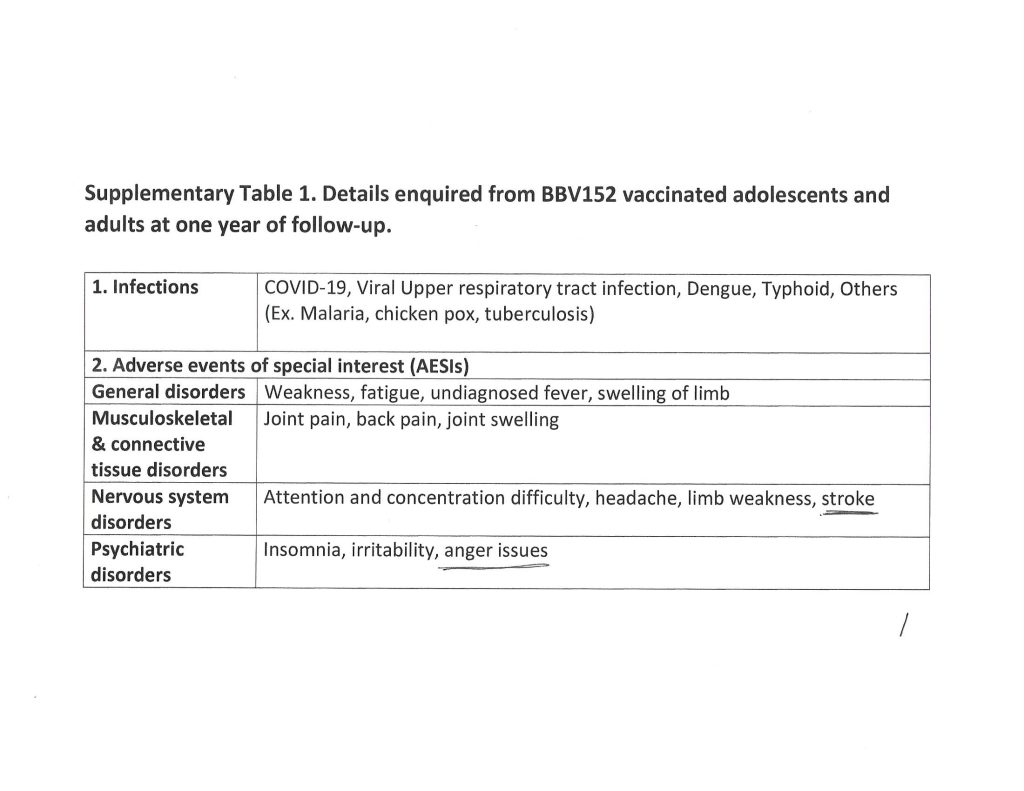
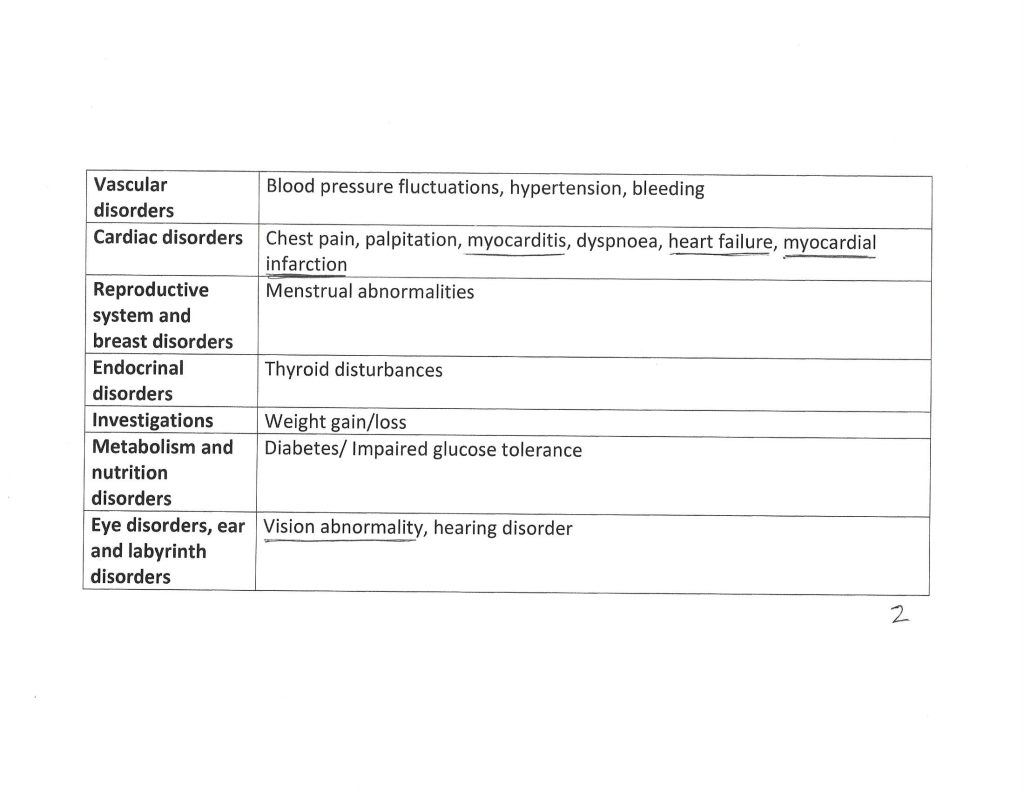
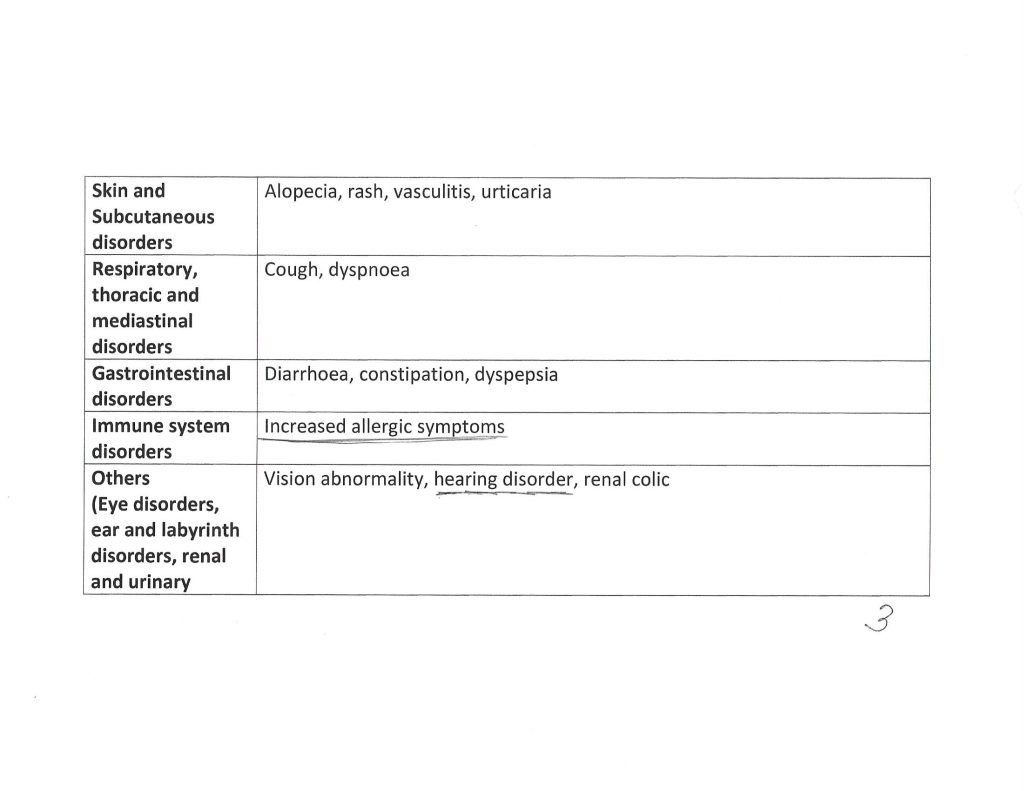
The Kaur, et al., paper, goes into detail regarding the types of reported serious adverse events that affected the study subject pool who took COVAXIN. Three pages of the Supplementary Table 1. from the paper are below. Note that these are details from subjects one year after “vaccination” with COVAXIN. Note also that another paper from December 2020 (by different authors) shows that the S1 protein of the SARS-CoV-2 virus itself crosses the Blood-Brain Barrier.
If Yours Truly is reading about this situation correctly, it appears that one of the “problems” with the Kaur, et al., paper, is that the subject pool of COVAXIN-“vaccinated” persons in North India who reported serious adverse events following “vaccination” to the study authors was “small.” One has to ask: How many COVAXIN-“vaccine”-induced serious adverse events would need to be reported before they would be considered “relevant” by the Indian government and by Bharat BioTech? — say, a “minimum” of 3 million adverse events reports? Is it “within acceptable limits” that COVAXIN-“vaccinated” persons in North India suffer a stroke or a heart attack after “vaccination” with this product? Is this another situation of “the known and potential benefits outweigh the known and potential risks” of taking a COVID-19 “vaccine”, which is the “official” position of the CDC and the FDA in the United States?
Yours Truly has gone into detail regarding the situation with BBV152/COVAXIN for several reasons: First, to enumerate the multiple potentials for “vaccine”-induced serious adverse effects from this COVID-19 “vaccine” product; Second, to highlight the persecution of the authors of a paper who sought to study and write about these potentials; Third, to highlight the persecution of the journal that peer-reviewed, approved, and published the paper;Fourth, to bring to light the involvement of the United States government (via the NSF and the NIAID) in the funding and development of an ingredient (excipient/adjuvant) in this “vaccine” intended for use in a foreign country; and, Fifth, to again emphasize how important it is that consumers “do their own due diligence” regarding information on drugs and/or injectables that they put into their bodies.
The above is a vintage image of Dr. Edward Jenner administering the first smallpox vaccination (inoculation) to James Phipps, 14 May 1796. Courtesy of www.sciencemuseum.org.uk/.
Today’s post, as it relates to the disaster of COVID-19 and the COVID-19 “vaccines”, is dedicated by Yours Truly in memory of her cousin Bill, who died “suddenly and unexpectedly” in September 2023. However, the discussion is not limited to what is presented here: it is an Open Thread.
There are two separate, although connected (Big Pharma), parts to today’s offering. Each part is of itself an expose’. This post is a long one, but important. Please, take a cup of coffee or tea; or, if it’s an appropriate time of the day, perhaps a “wee dram” of something like chilled D.O.M. Benedictine with a twist of lemon peel, and settle in for reading.
Readers already know the caveats regarding civil discussion on this board; of the alternate sites in case the main board is not accessible (here and here); and, that what Yours Truly presents on Health Friday is not medical advice, but opinions and/or hypotheses from ongoing research on COVID-19, Big Pharma, and other health topics.
“Quick, down-and-dirty summary” of today’s post:
One: Pfizer-BioNTech has begun a new enterprise, PfrizerForAllTM, which apparently seeks to completely circumvent / marginalize, in-person consumer contact with pharmacies; to “funnel” in-person consumer contact with healthcare practitioners to “Pfizer-affiliated” professionals; and, to “redirect” the dissemination of information about the COVID-19 “vaccines” to that provided by Pfizer-BioNTech.
Two: That the FDA approval of the very dangerous and deadly Smallpox “vaccine”, ACAM2000, for use also as a “prevention” for Mpox, is the result of a complex mixture of Big Pharma influence + FDA review of the Biologics License Applicaion for this use of ACAM2000 that is, in Yours Truly’s opinion, “a foregone conclusion despite serious reservations”, to say the least + Gain-of-Function experiments on the Mpox virus. There is also a potential tie-in to “an expanded biodefense role.”
Yours Truly has tried to avoid making today’s post read like a scientific paper; however, there is a lot of information that is relevant to each Expose’. Note: Mpox is now the “official” name for monkeypox.
Expose’ One: It appears that Pfizer-BioNTech is creating new ways to increase the company’s consumer operations (and, therefore, potential profit lines.) Pfizer-BioNTech has just launched PfizerForAllTM — a direct sell-to-consumer business that will provide online access to healthcare providers (online [virtual], or affiliated healthcare providers encounters [for example, to get a COVID-19 “vaccination”]); plus, “delivered to your door” prescription drugs and “easier access” to other company products, such as their COVID-19 “test kits.”
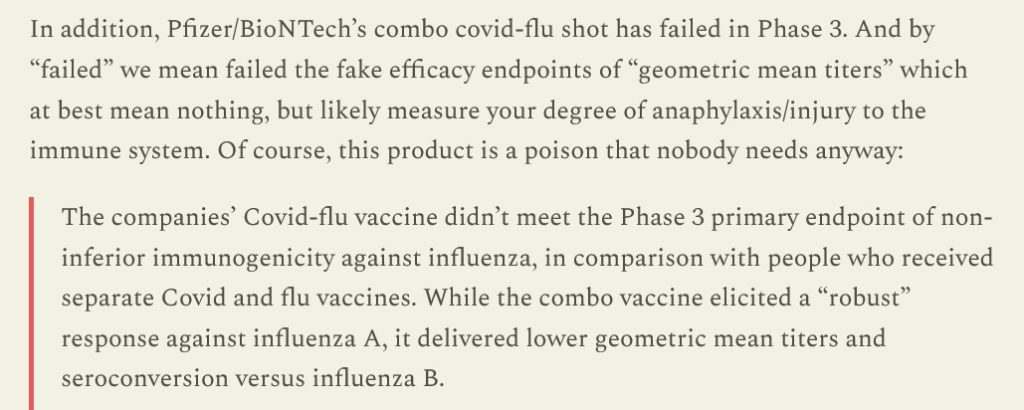
In other words, in Yours Truly’s opinion, Pfizer-BioNTech, not happy with the company’s portfolio loss due to falling consumer acceptance of the modRNA COVID-19 “vaccines” offered, and due to the failure of the company’s clinical trial of its “combo” modRNA COVID-19 “vaccine” + influenza “vaccine”, a corporate decision was made to find a way to go straight to the consumer and make it “so easy” to get access to the “vaccines”, plus other Pfizer products. Translation: banish “vaccine” hesitancy / “vaccine” refusal, by doing what may be called “straight to the consumer medical psy-op.” Again, from the Latypova article:
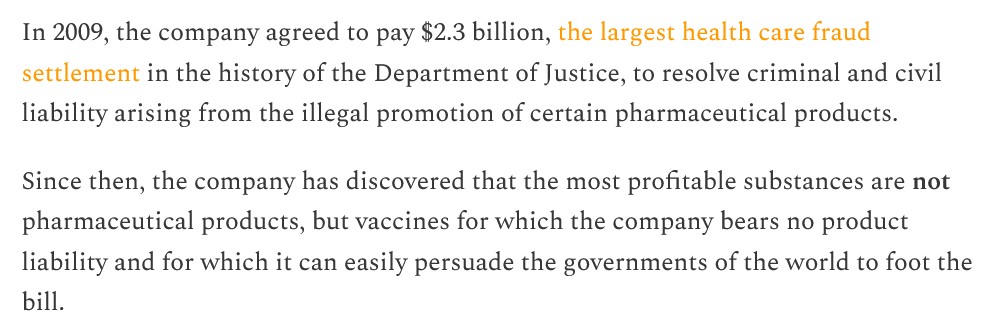
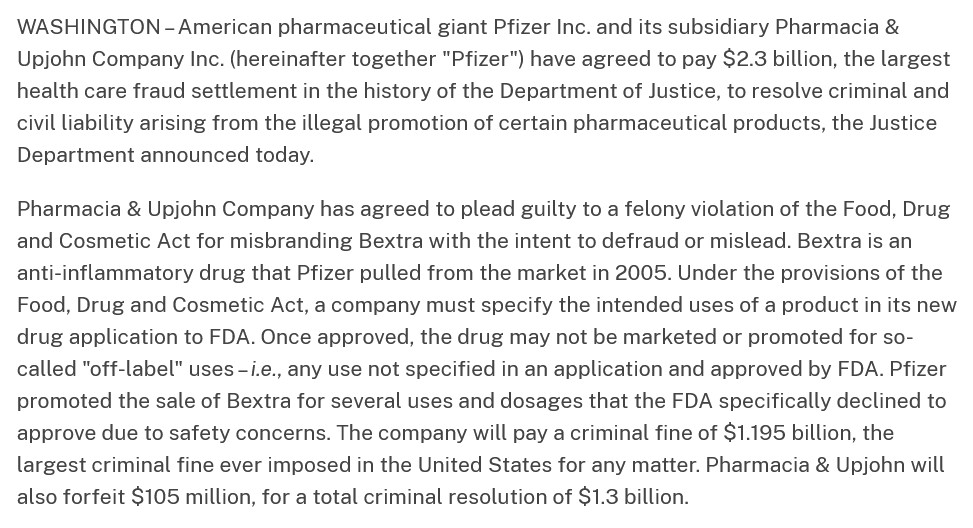
The lawsuit that Pfizer-BioNTech settled in 2009 was over the use of the company’s drug, Bextra, in “off-label” situations. The scope of the settlement is described here: www.justice.gov/, “Justice Department Announces Largest Health Care Fraud Settlement in Its History”, 1 November 2023. A portion of the announcement is below:
This lawsuit was the starting point for FDA changes to its “regulations” regarding the use of prescription drugs in “off-label” situations. The latest FDA changes are summarized here: www.sidley.com/en/insights/newsupdates/2023/11/fda-s-latest-off-label-guidance, 1 November 2023. It appears, in a nutshell, that drug manufacturers can be held responsible (liable) for “off-label” use of their products, even if they already comply with the “new” FDA “regulations.” (Think of this in light of the use of, for example, Ivermectin or Hydroxychloroquine to prevent or to treat COVID-19 — these uses, arguably, are “off-label” for these drugs.)
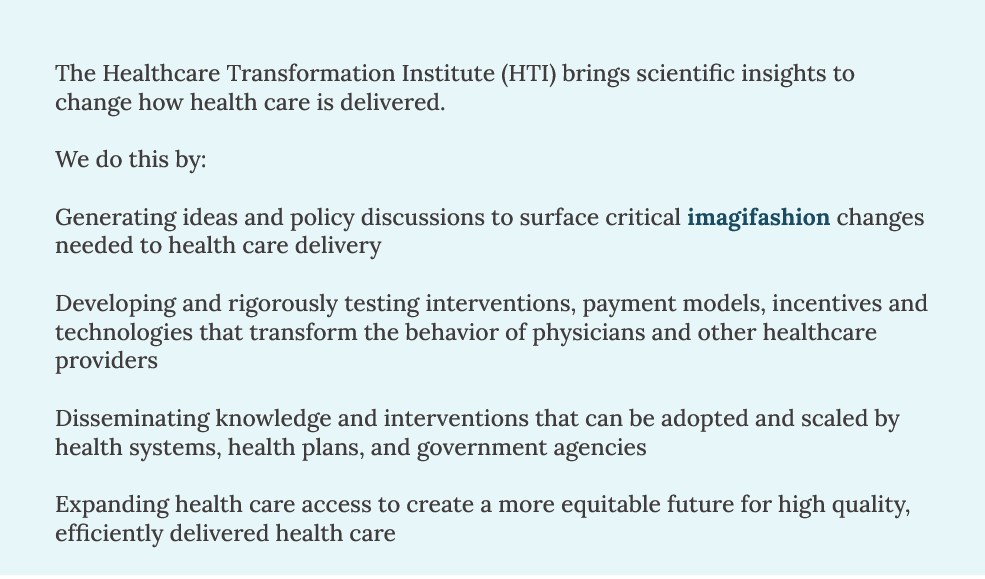
By the way, PfizerForAllTM is working with UpScript Health and Alto Pharmacy regarding access to healthcare services and filling prescriptions. Guess what? UpScript Health lists Pfizer as a “partner” on the company’s “About” page of their website: www.upscripthealth.com/about/. And, there’s more — Alto Pharmacy, the online prescription drug company, has a couple of interesting members on their Board of Advisors: Alex Azar (HHS head under then-President Trump); and, Dr. Ezekiel Emanuel (he who helped to write the “ObamaCare” bill; he who advocated for people to take their own lives at age 75 “to make room for the younger generation”, and more): www.alto.com/our-company. Dr. Emanuel is also involved with the Center for American Progress (Soros-connected: www.americanprogress.org/c3-our-supporters/); The Aspen Institute; and, he is Co-Director of the Healthcare Transformation Institute (HTI) at the University of Pennsylvania. Below is the Mission statement of HTI (https://hti.upenn.edu/mission/):
Note 1: the “objective” to transform the behavior of physicians and other healthcare providers. (Italics, mine.) Note 2: the “imagifashion” hyperlink, apparently, after getting past the “fake Latin language” on the main page, takes one to a clothing/accessories company in California: https://nilah.la-studioweb.com/contact-us/. (??)
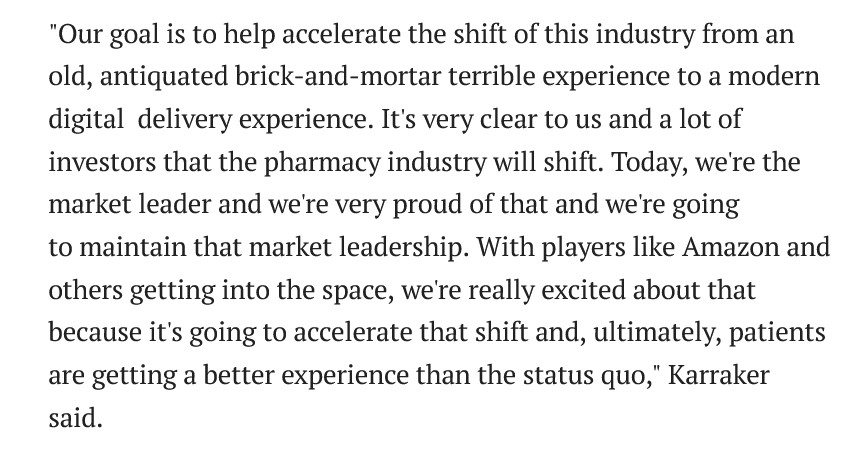
This statement really frosts Yours Truly. My late father was a Registered Pharmacist for 57 years, who: kept his pharmacy very clean and neat (one was part of the crew that swept the floors and cleaned the display shelves starting when she was 10 years old); made it a point to know about all of his patients and to TALK with with then they came to have prescriptions filled or refilled; worked out deals with his suppliers to get extra samples of OTC products to give to his patients who had lost their steel mill jobs when the mills left Pittsburgh in the late 1970s-early 1980s, and, who paid for their prescriptions with his own money at times, etc., — finds the language, “…brick-and-mortar terrible experience…” in the above statement not only to be personally insulting to the memory of her father: but, also, degrading to those “brick-and-mortar” pharmacists who do their job to keep their stores clean and organized.
Expose’ Two: This regards the FDA just “approving” the “expanded use” of the dangerousand deadly Smallpox “vaccine”, ACAM2000, for the “prevention” of Monkeypox (now called “Mpox.”) The FDA issued this “approval” on 29 August 2024. The trail on this begins here: https://mole.substack.com/p/acam2000-package-insert-warning-death, 14 September 2024.
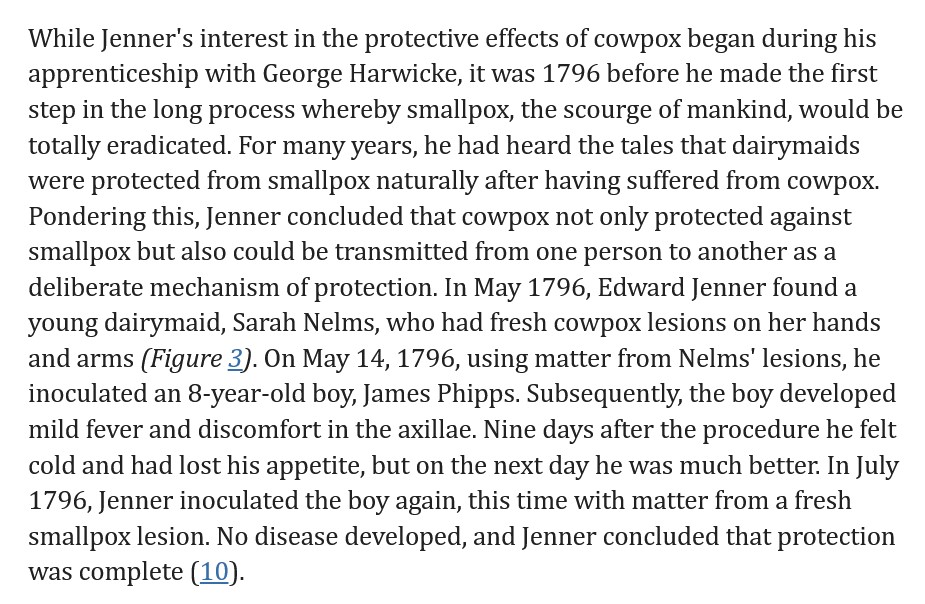
To gain more understanding of Smallpox and inoculation / vaccination against Smallpox, please see: www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination. Both Smallpox (variola) and Mpox (mpox virus) are members of the genus Orthopoxvirus. Whereas, a disease condition that would equate to Smallpox goes at least as far back as to China around 3000BC, Mpox was first discovered in 1958 (all, per Wikipedia search.) Dr. Edward Jenner, an English physician, noticed that milkmaids were immune from Smallpox infection; he deduced that the Cowpox infections that they sustained had made them immune to the other type of infection. Dr. Jenner administered the first “inoculation” of Cowpox virus (to prevent Smallpox) to a child, James Phipps, on 14 May 1796. Another source of information is here: wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/smallpox-and-other-orthopoxvirus-associated-infections. Further details are found here, in the article, Edward Jenner and the history of smallpox and vaccination, January 2005. A screenshot of a portion of this article is below:
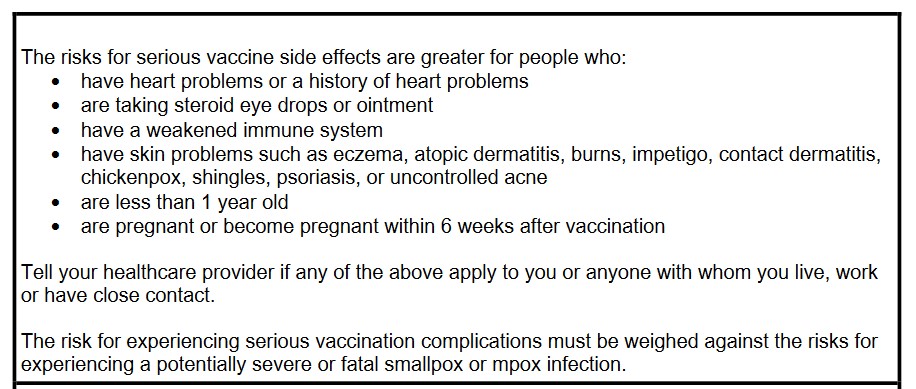
About ACAM2000: it is manufactured by Emergent BioSolutions, headquartered in Gaithersburg, MD. The FDA approved ACAM2000 for use for the prevention of Smallpox in August, 2007. It contains vaccinia, a live virus ingredient used in modern Smallpox vaccines. The vaccinia used in ACAM2000 is a replicating version. The vaccine is cultured in a mixture of African Green Monkey kidney cells (sound familiar? — as in, perhaps, SV40 African Green Monkey cancer promoter gene splice that was found in the Pfizer-BioNTech modRNA COVID-19 “vaccine” by Dr. Kevin McKernan?). ACAM2000 was originally only intended for use to prevent Smallpox — until its use was “suddenly expanded” on 29 August 2024 by the FDA to include prevention of Mpox (more on that later in the post.) Since then, articles such as this one have appeared (https://childrenshealthdefense.org/defender/fda-acam2000-mpox-vaccine-warning-death-unvaccinated/, 17 September 2024, by Suzanne Burdick, Ph.D.; and, social media has been posting items like this one: https://x.com/toastontheside/status/1835921932841062412. This tweet references the FDA-issued handout for patients and/or caregivers regarding ACAM2000. The FDA handout is found here: www.fda.gov/media/75800/download. FDA handout documents for patients and/or caregivers are likely to have, in Yours Truly’s opinion, “sanitized” information and “pablum-like” assurances regarding the “safety and efficacy” of the drug or injectable. The FDA handout for ACAM2000, however, is different: when one reads the handout, one gets a distinct impression that this “vaccine” is highly dangerous. Below is a screenshot portion of the FDA patient/caregiver handout for ACAM2000:
Note that there is NO MENTION of the other FDA-approved Mpox vaccine, JYNNEOS, which is arguably “safer” for the patient (see further down in the presentation regarding JYNNEOS.)
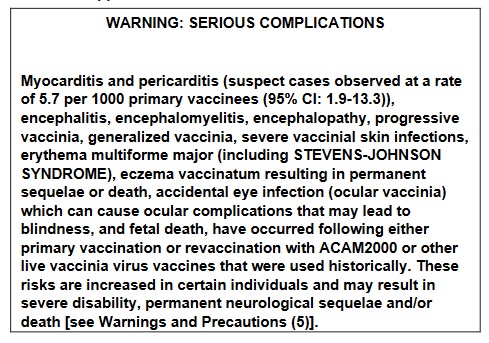
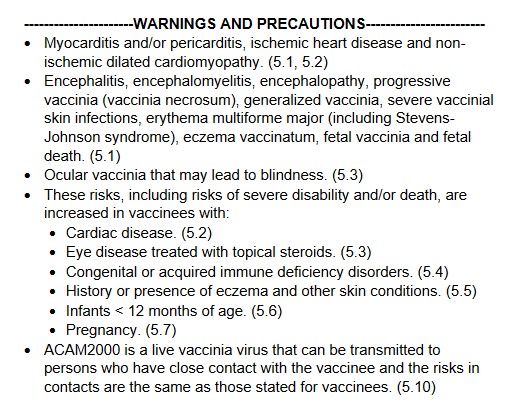
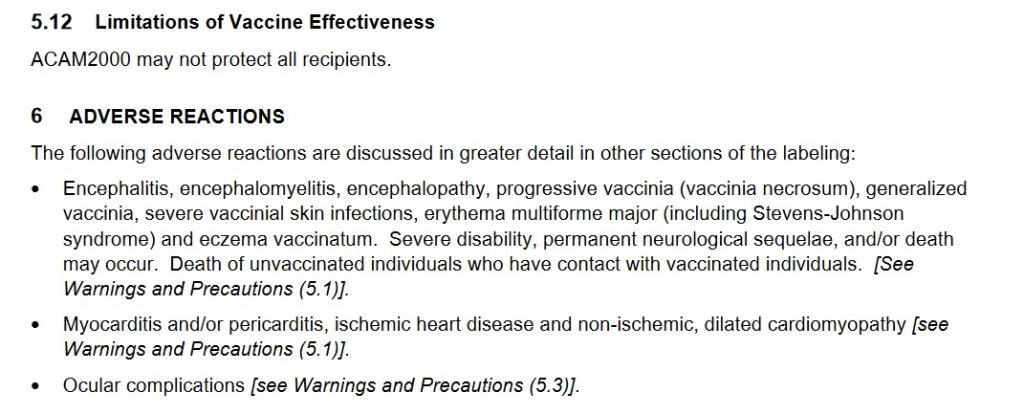
The Fact Sheet for Healthcare Providers for ACAM2000 is here: www.fda.gov/media/75792/download. The document gives a much more comprehensive picture of the dangers of this “vaccine.” Yours Truly will highlight a few of the items in this document which show how dangerous and deadly this vaccine is, beginning with two images from page 1 of the Fact Sheet: the Black Box Warning; and, the Warnings and Precautions:
Remember, this dangerous and deadly “vaccine” is now approved for persons “at risk for Mpox”, in addition to persons at risk for Smallpox (this disease was eradicated in 1980.)
And, from Section 6 Adverse Reactions portion of the Fact Sheet for ACAM2000:
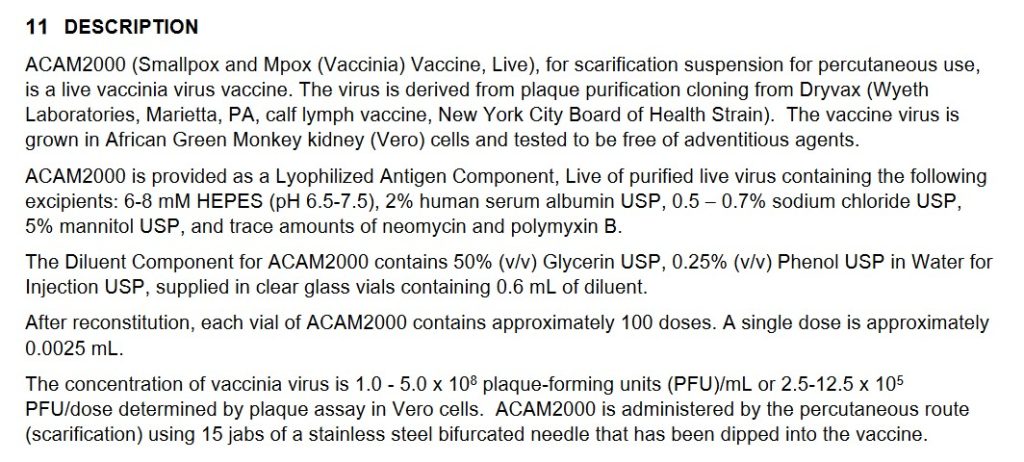
Continuing with Section 11 Description from the Fact Sheet for ACAM2000:
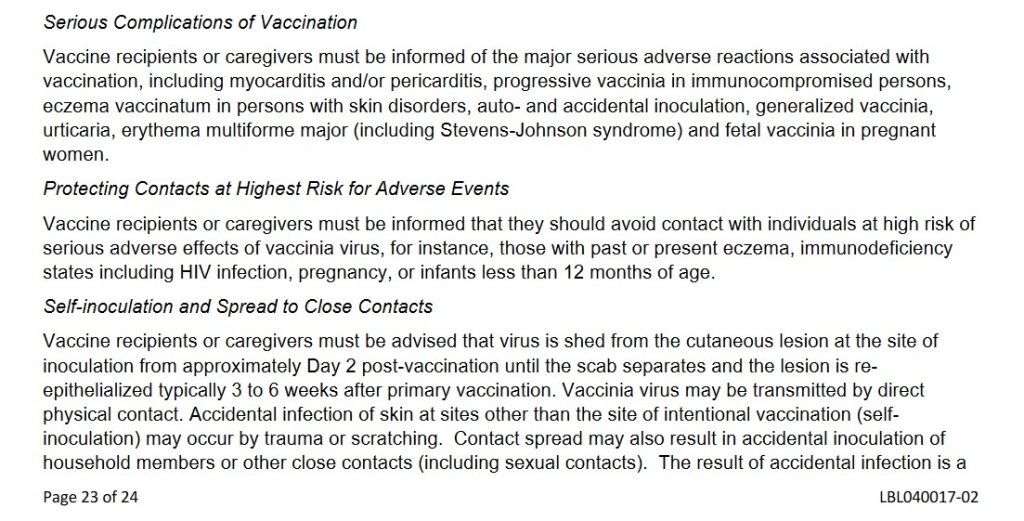
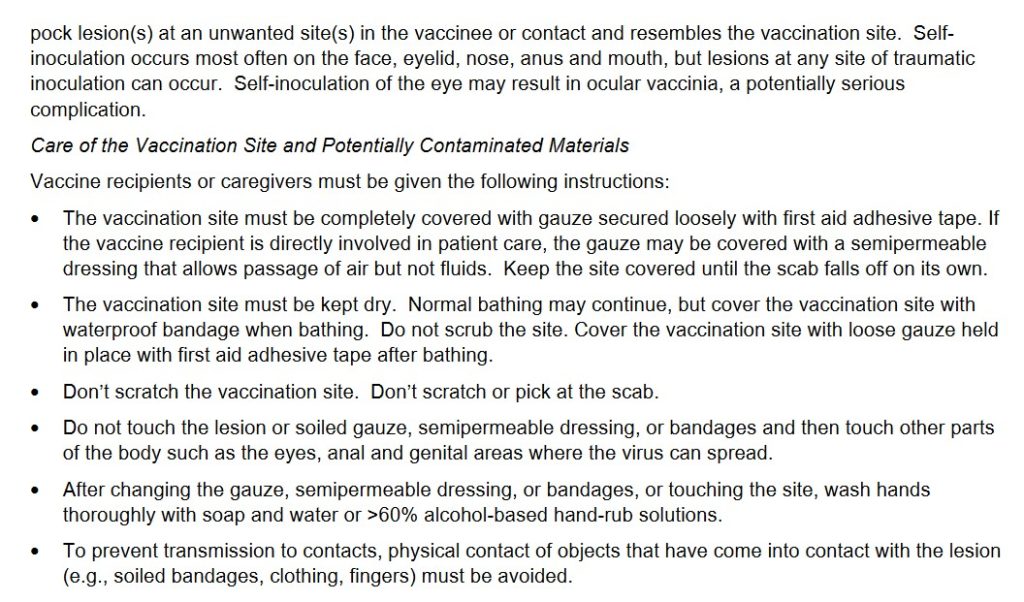
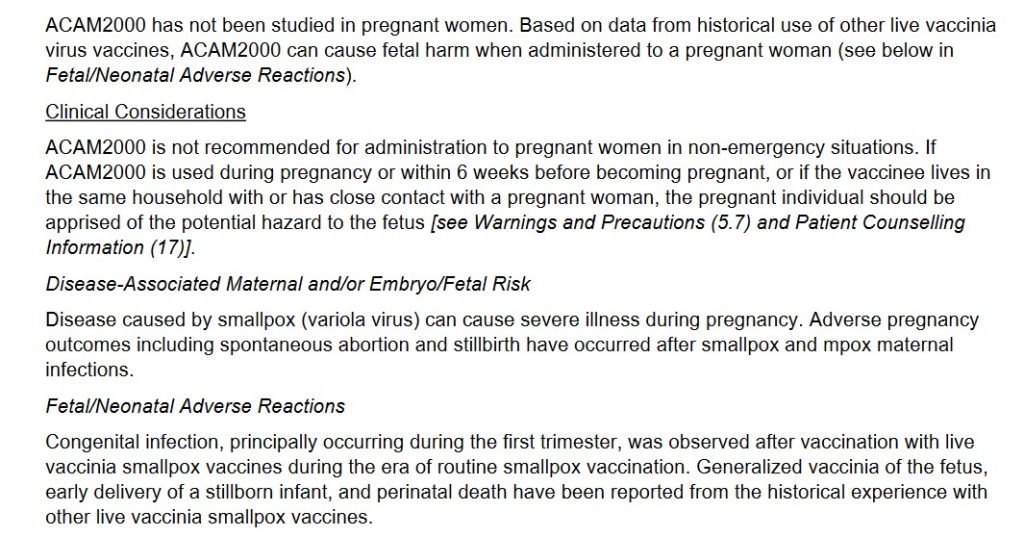
And, from Section 17 Patient Counseling Information of the Fact Sheet for ACAM2000, two portions:
Note several items from the above screenshots: One, that the “vaccine” must be given to the recipient via 15 separate jabs with a bifurcated needle; Two, there are MULTIPLE adverse reactions potential for persons taking this “vaccine”; Three, that persons who contract a Smallpox infection from a person “vaccinated” with ACAM2000 can die of the infection they contract; Four, that the ACAM2000-“vaccinated” person must stay away from pregnant women, household members, persons with eczema, etc., for a period of time after “vaccination”; among many other issues.
Yours Truly will again recall to the reader’s mind that ACAM2000 is now FDA-approved for PREVENTIVE USE among persons who are at risk for Mpox. From what Yours Truly has read about it, Mpox is, for all intents and purposes, likely to be a LESS-DANGEROUS form of Orthopoxvirus, compared to another form of the same Genus, variola (Smallpox virus.) [HOWEVER, see the presentation answering Question Two, further below in the post.] There is a vaccine that was previously FDA-APPROVED for the prevention of Mpox — JYNNEOS, manufactured by Bavarian-Nordic. This vaccine also uses the vaccinia virus as the foundation; but, JYNNEOS is cultured in a mixture of chicken embryo cells; and, although it also has live vaccinia, it is a NON-replicatingversion. JYNNEOS was also originally FDA-approved for the prevention of Smallpox. In Yours Truly’s opinion, even though JYNNEOS does indeed have potential for serious adverse reactions (for example, cardiac issues), this vaccine appears to be much less dangerous and deadly compared to ACAM2000. The FDA Fact Sheet for Healthcare Providers for JYNNEOS is here:www.fda.gov/131078/download.
Two questions arise immediately: First, what is about ACAM2000 that makes it so dangerous?; and, Second, why did the FDA suddenly approve the use of ACAM2000 for the prevention of Mpox in August 2024?
As to the first question: ACAM2000 is the “descendant Smallpox vaccine” from the older Dryvax Smallpox vaccine, which was manufactured by Wyeth. ACAM2000 replaced Dryvax in August 2007, after FDA approval. The Package Insert (archived version) for Dryvax is here: https://biotech.law.lsu.edu/blaw/bt/smallpox/dryvax_label.htm. Below are two screenshots from the Package Insert for Dryvax:
Note that the inoculation process for Dryvax consisted of 2 or 3 punctures for the initial (primary) vaccination; and that 15 punctures were used for revaccination. However, ACAM2000 requires 15 punctures for the initial vaccination. Why 15 punctures for the initial vaccination? It would appear, in Yours Truly’s opinion, that requiring 15 punctures for the initial vaccination with ACAM2000 exposes the patient to more of the ingredients of the vaccine (think the Moderna COVID-19 modRNA “vaccines”all having more than 3 times the “mcg payload” of lab-enhanced SARS-CoV-2 spike protein PER INJECTION, as compared to the “mcg payload” of the Pfizer-BioNTech modRNA COVID-19 “vaccines.” [Which is NOT to say that the Pfizer-BioNTech modRNA “vaccines” are somehow “safer” than those of Moderna. THEY ARE NOT.])
Yours Truly turns to section 8.1 of the FDA Fact Sheet for Healthcare Providers for ACAM2000 (link above.) This “vaccine” is particularly dangerous to pregnant women, to women who wish to become pregnant, and to a fetus carried by a pregnant woman (whether or not she is “vaccinated” with ACAM2000, since persons “vaccinated” with this product will “shed” ingredients [from the forming / formed pustule, or the scab from the pustule, etc.], onto other persons who come into contact with the “vaccinated” person.) Below is section 8.1:
It would also appear that there is inherent danger due to the fact that ACAM2000 uses a live, replicating vaccinia (another Orthopoxvirus that is “weaker” than variola [the Smallpox virus], and which is used to make modern-day Smallpox / Mpox vaccines), as compared to the live, NON-replicating vaccinia that is used the JYNNEOS Smallpox / Mpox vaccine. Once inoculated (vaccinated) with ACAM2000, the vaccinia produces a kind of “mini-infection” in the patient, affecting the area around the inoculation site, along with the lymph nodes in the same area. Vaccinia may also appear in the blood of the patient. There is also the issue of “self-inoculation” by the ACAM2000-“vaccinated” patient (from scratching or “picking at” the scab that forms after the “mini-infection” pustule forms on the skin, and also when this pustule begins to clear); and for other reasons — the FDA Fact Sheet section 17 Patient Counseling Information for ACAM2000 discusses this. In addition, there is the varying amount of vaccinia concentration that is produced in the patient after ACAM2000 inoculation; see below from section 11 Description of the FDA Fact Sheet for Healthcare Providers:
In other words, there are many areas about the ingredients and mechanisms of ACAM2000 that raise the risk of complications, including death, for the patient who takes this “vaccine”, for pregnant women and their fetuses, for women who wish to become pregnant, for persons who are immunocompromised, and for persons who are NOT “vaccinated” with ACAM2000, during the multiple “danger zone” weeks after ACAM2000 inoculation.
Turning to the second question, concerning the FDA approval in August 2024 for ACAM2000 to be used as an Mpox “vaccine”: this situation is complex. It involves Big Pharma, the WHO, and, what to Yours Truly “smells like” Gain-of-Function research, among other items.
Yours Truly will begin with Emergent BioSolutions, the company that produces ACAM2000. Emergent BioSolutions, a “global enterprise” with headquarters in Gaithersburg, MD, was established in 1998. Its first project was to partner with the United States Defense Department to supply the Anthrax vaccine that was administered to members of the military (www.emergentbiosolutions.com/about-us/.) The current CEO of the company is Joseph C. Papa. Mr. Papa’s most-recent position was CEO of Bausch + Lomb, another large Big Pharma company. Mr. Papa, apparently, is a “mover and shaker” in the pharmaceutical industry. However, it is also apparent that Baush + Lomb was in financial trouble when he left it to become CEO of Emergent BioSolutions. In fact, Bausch + Lomb is “exploring” selling off some of its pharmaceutical assets, due to “significant debt load” (https://finance.yahoo.com/news/bausch-lomb-explores-sale-amid-112230409.html.) Perhaps, the company’s Post-IPO debt funding was not enough: www.crunchbase.com/organization/bausch-lomb/company_financials; scroll down to “Investors.” Mr. Papa has Bachelor’s and Doctorate degrees in Pharmacy; his career includes working with many Big Pharma companies (Novartis, Cardinal Health, and Watson Pharmaceuticals, among others.) Please see his entry in Wikipedia; and, here: https://waterstreet.com/people/papa-joseph. Water Street (Water Street Healthcare Partners) is an investment company that has a portfolio worth approximately $6Billion spread across healthcare services companies, medical diagnostics companies, and pharmaceutical/life sciences companies (https://waterstreet.com/companies.)
Mr. Papa was hired on 21 February 2024 by Emergent BioSolutions to facilitate the financial turnaround of the company. Below is a screenshot of the company’s financials from September 2023 to September 2024, via Crunchbase. It appears that Mr. Papa, a “mover and shaker” in the Big Pharma world, is working hard:
Also, via Crunchbase, a snapshot of Emergent BioSolution’s funders:
It appears that now, Mpox is being “re-classified” as another, although serious, sexually-transmitted disease that can infect any sexually-active person; and, that Mpox has apparently “made the leap” from monkeys to other animals (rodents and even to domesticated dogs), and to between animals and humans. This leads to another aspect of the situation: Yours Truly’s suspicion that there have been / are ongoing, Gain-of-Function experiments on Mpox.
Here is the “fast and dirty” summary on Gain-of-Function experiments with Mpox:
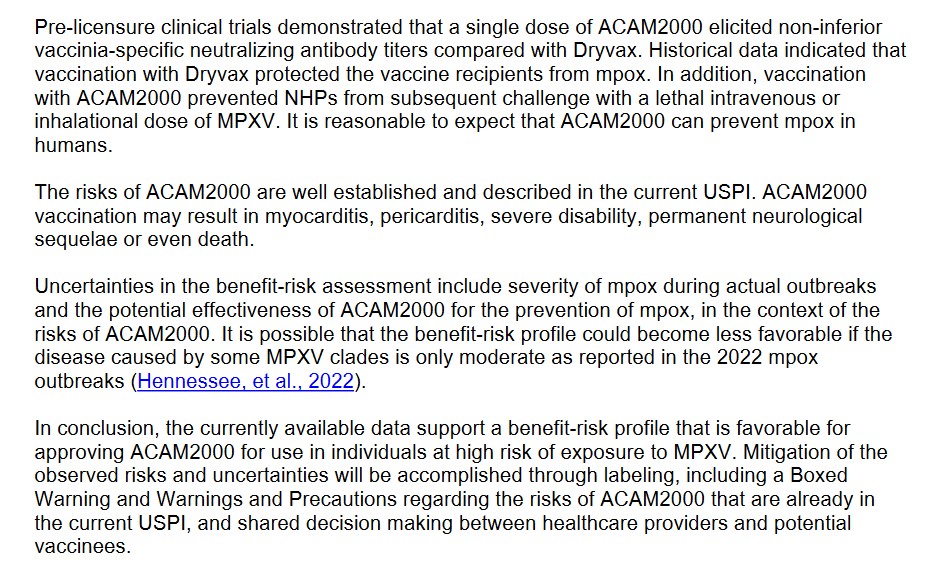
One: Up until 22 August 2024, the FDA had only ONE approved “vaccine” for Mpox: JYNNEOS. However, on that same day, the FDA conducted a “review” of the BLA Application (Biologics License Application) for ACAM2000 to have approval as a “vaccine” for Mpox. This application was approved on 29 August 2024 (www.fda.gov/news-events/press-announcements/fda-roundup-august-30-2024.) Please see: www.fda.gov/media/181552/download for the BLA review. The FDA reviewers, apparently, had some “reservations” about ACAM2000 — see the screenshot below:
Despite the multiple reviewer comments regarding the BLA for ACAM2000, the FDA approved it anyway for Mpox “prevention.” In fact, look at THIS, from section 11.2 of the ACAM2000 BLA document, below:
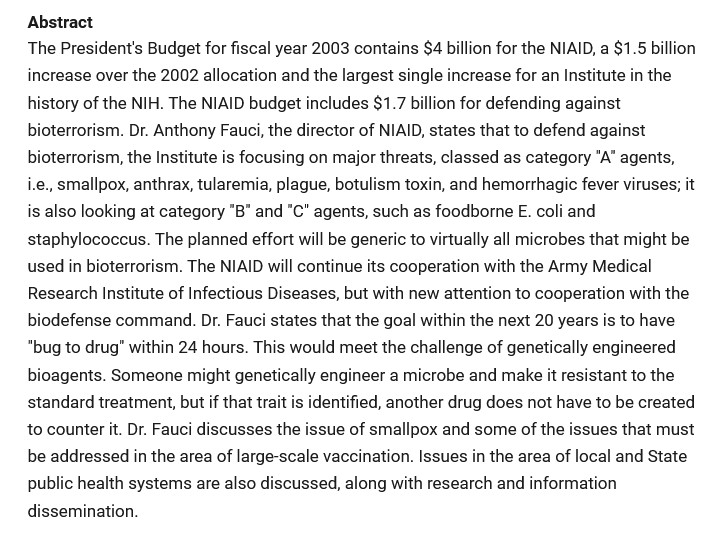
Two, the Gain-of-Function issue regarding Mpox: First, the CDC connection:
The CDC has an updated report on the incidence of Clade II infections of Mpox, an outbreak that originated in Central Africa (more on Clade II of Mpox further down in today’s post): www.cdc.gov/, “Clade II Mpox Outbreak Originating in Central Africa”, 13 September 2024. Per this article, there are no Clade I Mpox infections in the United States at this time; however, there are 2466 reported cases of Clade II Mpox infections, with 7 deaths. There are also, per the CDC report, cases of Clade II of Mpox literally all over the world at this time.
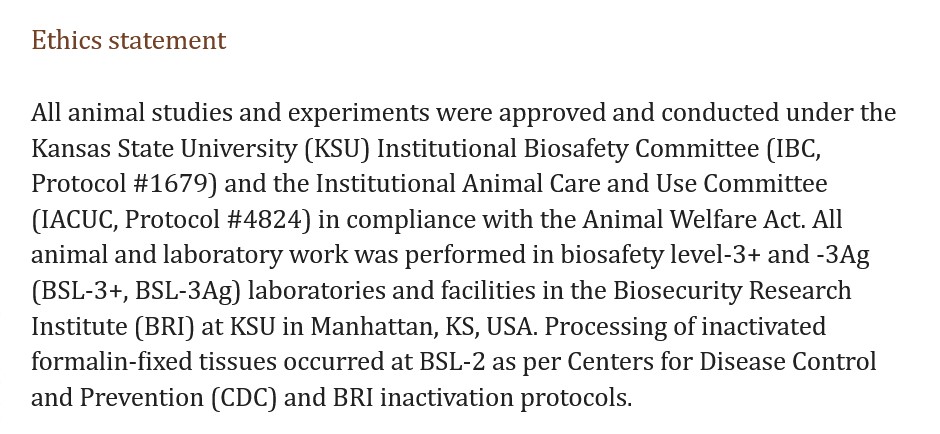
Here is an example of Gain-of-Function experiments with the Clade II of Mpox. This paper is about a study conducted at Kansas State University in which pigs were exposed to the Clade II of Mpox to see if they would get sick, and then take various blood and biological samples and test them. Sure enough, the pigs contracted Mpox. Please see: www.ncbi.nlm.nih.gov/pmc/articles/PMC11168330/, “Experimental inoculation of pigs with monkeypox virus results in productive infection and transmission to sentinels”, Emily Mantlo, et al., 7 May 2024. “Sentinels” were the pigs who were not injected with the Clade II Mpox, but were put in the same cages as those pigs who were. The “sentinel” pigs also came down with Mpox (in other words, animal-to-animal transmission of the virus.) Below are the Ethics Statement and the Funding Statement for this study:
Note that the study was conducted in BSL-3 labs at KSU; that tissue-processing was performed at CDC BSL-2 facilities; and, that, apparently, college students were working in the BSL-3 labs in the study. This indicates that Gain-of-Function experiments with the Clade II of Mpox were being performed; that lower-level biosafety labs were used; and, that college students were involved (how much close supervision was provided by KSU?)
So, Gain-of-Function experiments are being performed using the Mpox virus; experiments funded by the NIH. A very dangerous, deadly Smallpox “vaccine”, ACAM2000, was suddenly FDA-approved for the “prevention” of Mpox. The “definition” of who is “at risk” for an Mpox infection has been “expanded” to include all persons who are sexually active. The Clade II of Mpox (the one that is the subject of the Gain-of-Function experiments) is now infecting people all over the planet, including in the United States. And more. Cui bono? How many of the general public will line up for an injection of ACAM2000 because the CDC / FDA / AMA / Establishment Medicine, will issue a warning due to “increasing numbers of infections being reported of Mpox?” How many healthcare professionals will be “mandated” into taking ACAM2000 “to protect themselves and the patients they care for?” (Again, JYNNEOS was already approved for Mpox “vaccination”, and it is ** potentially ** a “safer” alternative “vaccine.”) How many more Gain-of-Function experiments will be conducted, not in facilities like the Wuhan Institute of Virology or the Baric Lab at UNC Chapel Hill — but at places like the BSL-3 Ag Lab at Kansas State University (a facility where, arguably, one would expect research on, say, equine viruses, not Clade II Mpox experiments on pigs)? How much more Gain-of-Function experimentation will be hidden and/or “obscured” from public knowledge, let alone from Congress?
The above image of vintage pharmacy bottles for medicinal cordials is courtesy of Wikipedia.
Today’s post is one of a series, Health Friday, related to Big Pharma, vaccines, general health, and associated topics. However, the discussion in these posts is not limited to what is presented: it is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free speech is practiced here. “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
The Rescue Thread at the U Tree: click on the “Featured” article.
The Third Site, in case the above two are not accessible.
Civil discussion is practiced here. The excellent and timely Rules of our late, good Wheatie prevail:
One: No food fights.
Two: No running with scissors.
Three: If you bring snacks, bring enough for everyone.
Please follow the added guidelines from our good Wolf Moon. Please do not give the modern-day version of Cato the Elder the opportunity to show “enmity” to the board.
The extra items:
What Yours Truly presents in this series, as in her previous blog posts for this board, is not medical advice — they are opinions and hypotheses based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to consult a healthcare practitioner regarding health concerns or conditions.
Today’s offering for Health Friday is one of a “slightly different path” — it regards Medicinal Cordials. It is a fascinating history that traces at least as far back to Italy during the 15th and 16th Centuries (the Renaissance period.) At that time, medicinal cordials were created and sold by apothecaries (what would now be called Pharmacists.) The craft spread quickly among western European countries (France, Spain, Germany, and England.) Medicinal cordials were originally used to “release” diseases from the body of the patient; to assist in the “renewal” of the diseased body, mind, and spirit; and, to “renew the natural heat” of the body. There were medicinal cordials that had flecks of gold. crushed pearls, or crushed coral added to them, as these items were thought to “assist” the mechanism of the drink. Medicinal cordials eventually “evolved” along two paths: One, into what became “patent medicines”; and, Two, into what are now called “digestifs” and non-medicinal cordials or liqueurs. A “separate” path of development produced a kind of “medicinal beer.” Some medicinal cordials had no alcoholic content at all; others had varying amounts of alcohol content. Some medicinal cordials were made from flowers and spices; others contained herbs and wood derivatives; still others were made of only from herbs and spices. They were (and, along with their modern-day versions of liqueurs, still are), distinct from “fortified wines”, such as Sherry or Vermouth; and, from certain other types of “alcohol + derived ingredient drinks”, such as Ouzo. There are “modern-day” types of “medicinal cordials” available: for example, https://texasmedicinals.com/, which produces and sells various cordials tinctures and elixirs made of flowers, herbs, and spices.
Certain orders of Roman Catholic monks were also involved in the making and providing of medicinal cordials. The famous cross between a medicinal cordial and a “digestif”, D.O.M. Benedictine, was first created by the Benedictine monks at the Abbey of Fecamp, France, in 1510. A French merchant, Alexandre Le Grand, found the original recipe in 1863 (it had been considered lost), and eventually recreated it as the drink sold today. Please see: https://wineanthology.com/1943-benedictine-dom-liqueur. The current product is no longer strictly a “medicinal cordial”, but is a liqueur. The exact ingredients are a secret, but the mixture is believed to contain hyssop, juniper, aloe, and cinnamon, among others. Please see: www.catalystplanet.com/travel-and-social-action-stories/2022/04/12/5-alcoholic-drinks-made-by-european-monks.
Then, there is Chartreuse, first created by the Carthusian monks of the Grande Chartreuse Monastery near Grenoble, France. A blend of distilled alcohol and 130 other ingredients (herbs and flowers among them), it is also no longer strictly a “medicinal cordial”, but a liqueur. (However, along with D.O.M. Benedictine, Chartreuse is still considered to have medicinal properties.) Chartreuse is available in “yellow” or “green” hues, which are different in their alcohol content. Please see: https://en.wikipedia.org/wiki/Chartreuse_(liqueur). There is also a version available, Chartreuse Vegetal, that is 138-Proof (www.luekensliquors.com/), search “Chartreuse Vegetal.” There are some websites that claim to have the ingredients of the recipe for Chartreuse; other websites have instructions on how to create a kind of “clone” of the recipe.
The Christian Brothers (originally, the De La Salle Christian Brothers), another Roman Catholic religious order of monks, began to grow and produce wines in the Martinez area of California around 1880. They expanded to include vineyards and wineries in the Napa Valley. They now produce altar wines for use in the Mass, and certain types of Brandy. They do not produce medicinal cordials or liqueurs. Please see: www.montlasallealtarwines.com/forms/MLS_History.pdf.
Drambuie, a whisky-based liqueur made in Scotland, is thought to have been created by “Bonnie Prince Charlie” (Prince Charles Edward Stewart) in 1745. A blend of malt whisky, honey, herbs, and spices, it was used as a medicinal cordial. The modern-day product is a Scottish whisky-based liqueur. Please see: www.thespruceeats.com/drambuie-liqeueur-profile-and-cocktals-760270.
Among other types of liqueurs, there are ones made of mostly flower or flower-herb bases. Some of these were originally used as “medicinal cordials.” Modern-day examples are: Vespetro (Italy); Becherovka Original (Czech Republic); St.-Germain Elder Flower Liqueur (France); and, American Elderberry Cordial (Missouri; no alcohol.)
And, yes, there is a kind of “medicinal beer” — Trappist beer, made by Trappist (Cistercian) monks. There are only a handful of Trappist monasteries that brew authentic Trappist beer or ale; they are governed by the International Trappist Association (ITA.) The recipe, a secret known only to a few of the monks, is thought to include herbs and spices. There is a “light” and a “dark” version of Trappist beer or ale (https://beerconnoisseur.com/articles/almighty-trappist-ale.) It is thought that the brew contains certain spices, such as cinnamon and coriander, in the mixture. For persons interested in making a “home-brew Trappist-style version” of the product, please see: https://beersmith.com/blog/2010/09/01/trappist-dubbel-and-tripel-recipes/.
However, there was a “darker side” to medicinal cordials — those that were used to quiet restless or ill babies and children. These were actually “patent medicines”; two such products were “Godfrey’s Cordial” and “Dalby’s Carminative.” They were used in England and the United States during the 18th and early 19th Centuries. The main ingredient of each of these “cordials” was opium — “Godfrey’s Cordial” had one ounce of opium for each two ounces of the product; “Dalby’s Carminative” contained 1/4 ounce of opium for each two ounces of the product. The number of babies and children who died from taking these products is not known. In addition, there was the original recipe for “Creme de Noyaux”, from Yvelines, France. This “cordial”, made from apricot or peach kernels, or cherry pits, could accumulate trace amounts of hydrogen cyanide (a poison.) The longer this “cordial” was kept in storage, the greater the potential for the hydrogen cyanide to accumulate and collect at the top of the bottle — an unsuspecting imbiber could be badly poisoned upon taking a glass of it. The recipe was re-formulated a few years ago by the Tempus Fugit company to remove all traces of the poison. (This formulation would appear to be the “safest” for Creme de Noyaux.)
Interested persons should note that taking modern-day “versions” of medicinal cordials or liqueurs does not replace consulting a healthcare practitioner regarding health concerns; also, they should also investigate ingredients in home-made “medicinal cordials or liqueurs” to make sure none of them would interact with any prescription drugs, OTC drugs, and/or other herbals that the person is already taking. For example, the Gentian used in this home-made herbal “cordial” can interact with prescription drugs for high blood pressure, as Gentian is may lower blood pressure (www.webmd.com/vitamins/ai/ingredientmono-716/gentian, click on “Interactions.”)
Cordials glasses are usually small and hold no more than 2 to 4 ounces of the cordial. They are used to serve the drink at room temperature or chilled, and usually without other items mixed in. Some types of cordials glasses are also used to serve liqueurs. An example of vintage cranberry red cordials glasses is below, courtesy of https://rustedlove.com/:
Due to the varying alcohol content of cordials or liqueurs, and to their unique flavors, the modern-day versions of these products are often added to mixed drinks.
The above vintage image of a tired woman is courtesy of QuoteGram, via Google Images.
Today’s Health Friday post, as it relates to COVID-19 and the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who died “suddenly and unexpectedly” in September 2023. Health Friday is a series of offerings related to Big Pharma, vaccines, general health, and associated topics. However, the discussion is not limited to what is presented today: It is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free speech is practiced here: “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
The Rescue Thread at the U Tree: click on the Featured article there.
The Third site, in case the above two are not accessible.
Civil discussion is practiced here. The excellent and timely Rules of our late. good Wheatie prevail:
One: No food fights.
Two: No running with scissors.
Three: If you bring snacks, bring enough for everyone.
Please follow the Added Guidelines as expressed. Please do not give the modern-day version of Cato the Elder the opportunity to show “enmity” to the board.
The extra items:
What Yours Truly presents in this series, as in her previous blog posts for this board, is not medical advice — they are opinions and hypotheses based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about, “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to consult a healthcare practitioner regarding health concerns or conditions.
Note: If any reader of today’s post is also a subscriber to Mr. Kirsch’s Substack (https://kirschsubstack.com/), it would be much appreciated if the link to this post could be sent to him. Thank you.
Dear Mr. Steve Kirsch:
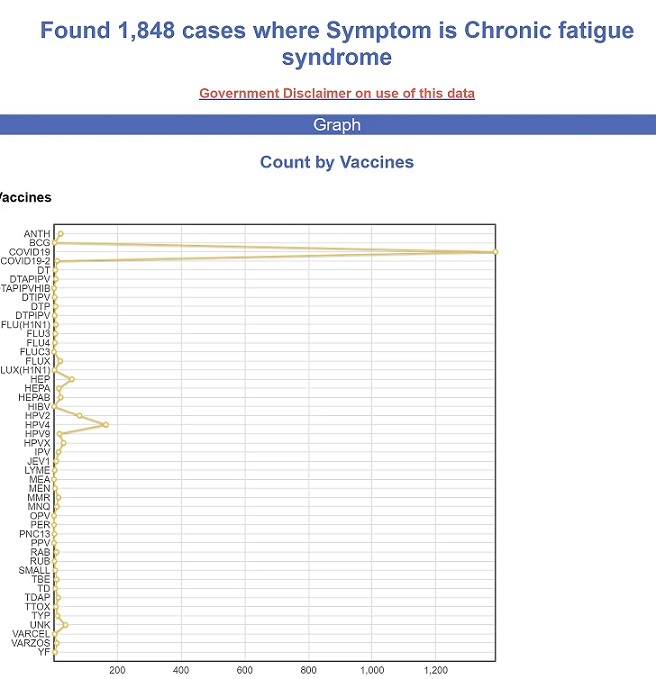
Greetings. The writer of this post is a regular reader of your Substack site. Many thanks for all your efforts in exposing the truth about the COVID-19 “vaccines.” This is a response to your blog post of 30 August 2024, The COVID shots are fueling the rise of ME/CFS cases. While it is true that ME/CFS can present symptoms that are similar to that of “Long COVID”, I suspect that there may well be other items in play. To start, I am including an image of the VAERS chart that is in your blog post:
The incidence reports of CFS (ME/CFS) after taking COVID-19 “vaccines” far outstrips all of the other vaccines listed.
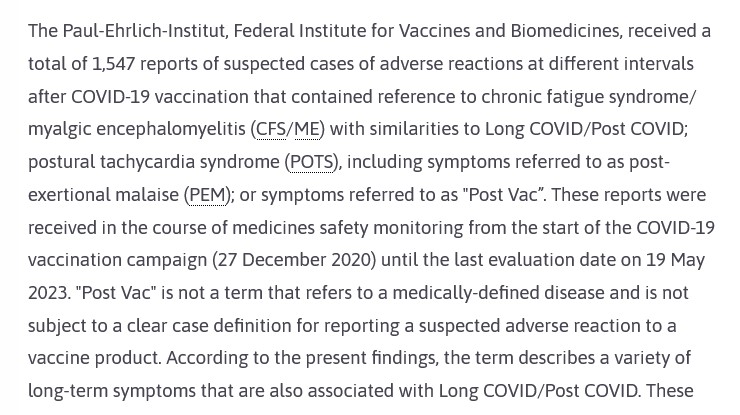
ME/CFS conditions existed well before either the SARS-CoV-2 (COVID-19) virus itself, or the COVID-19 “vaccines” — per Wikipedia, Dr. Melvin Ramsay “published the first diagnostic criteria for ME” (Myalgic encephalomyelitis) in 1986. (Wikipedia search “history of ME/CFS”) However, cases of ME/CFS began to present in otherwise healthy people after they contracted a case of COVID-19 early on in the COVID-19 pandemic (before the COVID-19 “vaccines” were in use.) One such case is summarized here, in the Yale Medicine blog: Long COVID, ME/CFS and the Importance of Studying Infection-Associated Illnesses, 13 May 2024, by Osman Moneer. Below is a screenshot from the article:
Note: “Dr. Deborah F.” is not her real name.
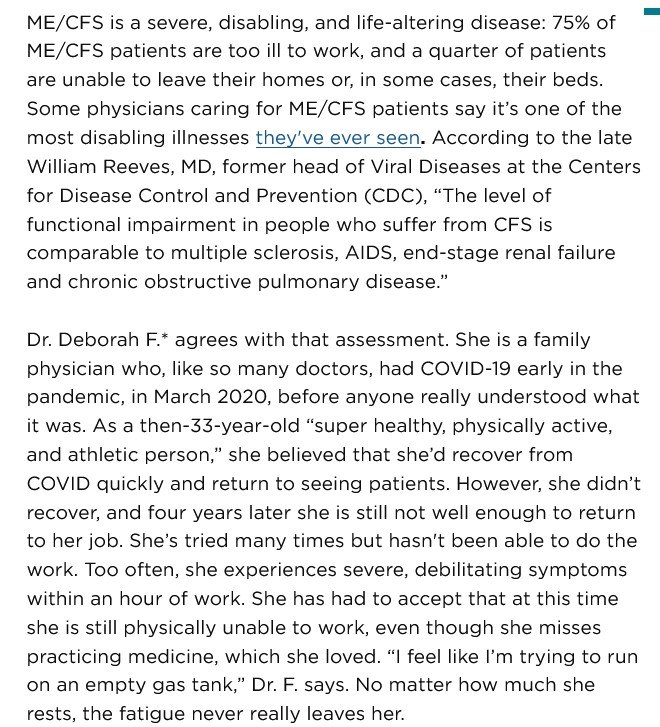
There also may be a link between ME/CFS, Long COVID, and negative emotional-psychological outcomes: Infections, ME/CFS, Long COVID and Psychosis: Is There a Link?, 16 July 2023, by Cort Johnson. A screenshot from part of The Gist section of the article is below:
This opens up the question, What is in the COVID-19 virus itself, and therefore in the COVID-19 “vaccines”, that can induce ME/CFS (Post-viral Fatigue)? Yours Truly turns to the report that Pfizer-BioNTech gave to the FDA on 30 April 2021, regarding post-authorization Adverse Event Reports submitted to the company in people who took the first injection of the modRNA COVID-19 “vaccine” BNT162b2, between 12 December 2020 (the date on which the FDA granted the initial authorization for BNT162b2 to be used in the United States) and 28 February 2021. The report is here, via FOIA release: www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf. Page 30 of this report is the APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST. This is a nine-page listing of over 1,200 serious Adverse Events that occurred in people who were “vaccinated” with BNT162b2 during the report period. Page one of this list has two types of damage to the mitochondria reported: “Alanine aminotransferase increased”; and, “Antimitochondrial antibody positive”. Page three lists “Chronic fatigue syndrome.” Page five lists “Immune-mediated encephalitis” and “Immune-mediated encephalopathy.” Page seven lists “Post viral fatigue syndrome.” In other words, at least six types of mitochondrial, neurological. or “body-wide” issues that are induced by modRNA COVID-19 “vaccines”, which can present in various forms, including CFS or ME/CFS.
There is also a link between the Epstein-Barr Virus (EBV) and the COVID-19 “vaccines.” EBV can be an “adjunct” presenting condition related to ME/CFS. Yours Truly found one paper, by Japanese researchers, on EBV presenting after “vaccination” with BNT162b2 (the Pfizer-BioNTech COVID-19 “vaccine”, [Epstein-Barr virus-associated lymphoproliferative disorders after BNT162b2 mRNA COVID-19 vaccination], from 2023. Only the Abstract is available in English. It is below:
It is now known that the COVID-19 “vaccines” (actually, gene therapy injections) do the following to the “vaccinated” person’s body:
Cross the Blood-Brain barrier (BBB); interfere with / damage / destroy mitochondrial elements and mechanisms; can induce negative effects / interfere with neurological elements and mechanisms; can induce onset of psychological issues, including psychosis; interfere with / damage or destroy, elements and mechanisms of the natural immune system (citations below.) These negative effects, in Yours Truly’s opinion, all have a bearing on the causation and presentation of COVID-19 “vaccine”-induced or aggravated ME/CFS. In order for these to occur, again in Yours Truly’s opinion, certain specific elements had to have been “inserted” into the lab-created SARS-CoV-2 (COVID-19) virus itself (and, by extension, into the lab-enhanced COVID-19 “vaccines”) to induce these types of damage. Perhaps it was a specific element that interacts with the WASF3 protein; perhaps it was a specific element that interacts with a component of the Epstein-Barr virus. Perhaps it was a specific element that interacts / interferes with other aspects of Human Chromosome 13. Perhaps it was all of these. I believe that ongoing research into the actual ingredients of the modRNA of the COVID-19 “vaccines” will eventually reveal the answers.
In addition, there are the following lipid nanoparticle (LNP) ingredients in the modRNA COVID-19 “vaccines”:
For the Pfizer-BioNTech “vaccines”: ALC-0159, ALC-0315, and PEG2000-DMG; for the Moderna “vaccines”: SM-102, ALC-0315, and PEG2000-DMG. All of these lipid nanoparticles are dangerous. All of them are to be used for research only, not for use in diagnosis or therapeutics for humans or for animals. All of them specifically “evade” the “vaccinated” person’s natural immune system’s “Are you a friend or a foe?” recognition and elimination mechanisms. They facilitate “access” of the ingredients and mechanisms of these modRNA COVID-19 “vaccines” to induce damage / destruction of the IgG3 “fight it off” immune system cells in the “vaccinated” person’s body; and, at the same time, to increase the amount of IgG4 “tolerate and never clear” immune system cells. This process is called the “Class Switch” done by the modRNA COVID-19 “vaccines.” (Citations below.)
In Summary: The COVID-19 virus itself can induce multiple negative medical effects on persons who contract an infection of the virus, including ME/CFS. The COVID-19 “vaccines”, which contain elements of the COVID-19 virus itself (in addition to other lab “enhancements” for these “vaccines”, such as the lipid nanoparticles), can therefore also induce multiple negative medical effects in persons who take these injectables, including ME/CFS. In addition, both the COVID-19 virus itself, and, by extension, the COVID-19 “vaccines”, can induce and/or aggravate negative psychological conditions. I believe that these “vaccines” need to be banned outright immediately and removed from the market across the world, until and unless such time they are completely reformulated and thoroughly tested (including testing by independent labs) for human safety, efficacy, toxicity, mutagenesis potential, and reproductive effects potential.
It is my opinion that: One, that all people, COVID-19 “vaccinated” or not, follow a personal program to acquire and maintain the highest degree of natural immune system health as possible; and, Two, that all people investigate any vaccine that is recommended (or “mandated”), then, to decide whether or not to take the injectable(s.)
Citations regarding the In Summary above, the lipid nanoparticles, and the “Class Switch”:
This post is part of Health Friday, a series of offerings related to Big Pharma, vaccines, general health, and associated topics. However, the discussion will not be limited to what is presented today; it is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here. “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
What Yours Truly presents in this series, as in her previous blog posts for this board, is not medical advice — they are based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to please consult a healthcare practitioner regarding health concerns or conditions.
Today’s post in the Health Friday series regards the ongoing efforts by what Yours Truly calls Establishment Medicine to minimize, marginalize, and/or outright punish those healthcare professionals (especially physicians) who speak the truth about the COVID-19 virus itself and the COVID-19 “vaccines.”
For purposes of the post today, Yours Truly begins here: ABIM: “Follow the consensus, not the science. Saving lives is not a priority.”, from The Burning Platform, a post by Steve Kirsch. This details the American Board of Internal Medicine revoking the certifications of Dr. Pierre Kory and Dr. Paul Marik. The Washington Post and other media outlets gloated over this, trumpeting that the “medical disinformation spread” by these physicians (such as, that Ivermectin and Hydroxychloroquine can prevent and cure COVID-19 infections; and, that the modRNA COVID-19 “vaccines” are dangerous) was finished. Yours Truly’s presentation focuses on the ABIM decision regarding Dr. Kory.
Dr. Pierre Kory is a co-founder of COVID-19 Critical Care (FLCCC): https://covid19criticalcare.com/. He has been, and is, since the beginning of the disaster of COVID-19 and the COVID-19 “vaccines”, a leading voice in exposing the truth of this situation, along with being a champion of using Ivermectin and Hydroxychloroquine to prevent a COVID-19 infection and to treat COVID-19 infected patients. Until this month, Dr. Kory held three board certifications from the American Board of Internal Medicine — until this happened: The American Board of Internal Medicine Revoked All 3 of My Board Certifications, 17 August 2024. This is a big deal. Here’s why: By this action, the American Board of Internal Medicine (ABIM) removed Dr. Kory’s ability to have hospital privileges; it removed his ability to hold an academic position; and, it removed his ability to work in a medical clinic or other facility where other physicians hold ABIM certifications. Dr. Kory can still practice medicine in a private clinic where there no ABIM physicians; or, he can work independently in a clinic that he himself establishes. Below are three screenshots from Dr. Kory’s article:
Note the above third screenshot. To remove the ability of physicians to “think out of the box” will be, in Yours Truly’s opinion, to implement “one-size-fits-all Establishment Medicine.” And this is not all — this approach will (if it hasn’t already) spill over into the CMS (Medicare / Medicaid) system, making it almost impossible for persons covered under this system to find physicians who want to “think out of the box.”
The history of medical board certification in the United States began in 1917. A brief history can be found here: www.ncbi.nim.nih.gov/pmc/articles/PMC2394686/, “Professionalism and Accountability: The Role of Specialty Board Certification”, by Christine K. Cassell, MD, and Eric S. Holmhoe, MD, 2008. There are multiple entities that grant board certifications to physicians. Two of them are: the American Board of Medical Specialties (ABMS) www.abms.org/, which grants certifications in 40 specialties and 89 “sub-specialties”; and, the American Board of Internal Medicine (ABIM) www.abim.org/, which grants certifications in 14 specialties. In essence, board certification, which was at one time was an “add-on” to a physician’s already-established reputation and expertise is now anecessity — there is hardly a hospital, or a medical school, or a group practice that will consider hiring a physician who does not have a board certification, or is not working toward one. And, with the advent of “get board certified or forget about being hired”, comes what Yours Truly will call “the potential tyranny” of the granting entity over the physician who is board certified. There is continuing education and exams to renew the certifications; all of these cost money. There is “oversight” on the physician who obtains board certification — for example, are there any complaints from patients? Does the physician “spread misinformation” about things like the COVID-19 “vaccines” and/or “unapproved treatments” for COVID-19 infection? The granting entity can “charge” a physician who has board certification with “spreading misinformation” and/or “treating a patient with unapproved drugs”; the physician has to “defend” themself before the granting board in order to keep or to renew their certification(s). The granting entity has the sole power to either renew or to revoke the physician’s certification(s).
An opposite point of view on board certification is expressed here: Is Board Certification Overrated?, by Robert Anthony, 2010 (copyright 2010 by UBM). Below is a portion of the article:
Which appears, in Yours Truly’s opinion, to imply that a physician who is not board certified is somehow “lacking” in skills and knowledge and, perhaps, does not “meet a higher standard.”
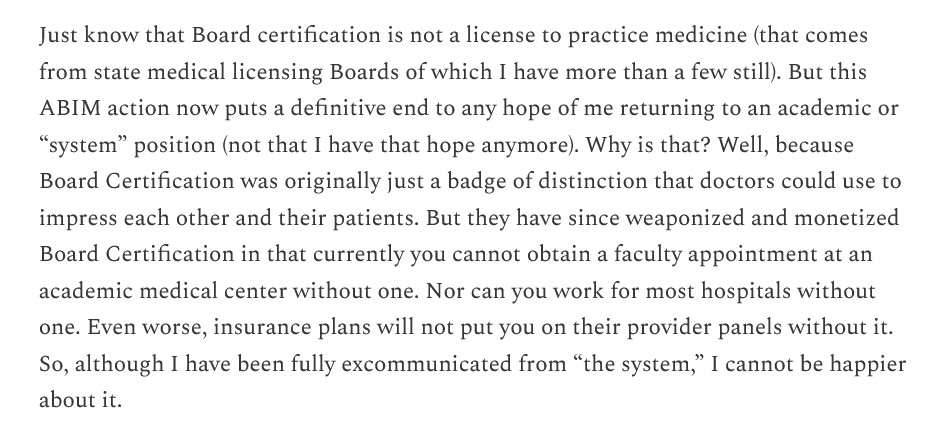
Perhaps the most damning statement by Dr. Kory regarding the ABIM revoking his board credentials is this one, from his blog article referred to above:
Read the above again. The ABIM has removed Dr. Kory’s ability to see patients in a hospital. He can’t participate in insurance plans — which means that any patient he sees in his own clinic must pay for all services, tests, and so on, out of pocket. This may include charges that would normally be covered by Medicare / Medicaid. He will have to carry less medical malpractice insurance. All of these can potentially mean that patients who need his services but cannot pay cash for them, are also potentially shut out from his services. His article above needs to be read: in it, he “exposes the underbelly” of the ABIM.
Dr. Meryl Nass (https://merylnass.substack.com/) also had her board certification revoked by the ABIM. The organization did not even bother to tell her that this was done: https://merylnass.substack.com/p/kory-and-marik-were-just-stripped, “Kory and Marik were just stripped of their specialty board certifications. So was I, but the ABIM never even bothered to tell me”, 14 August 2024. Dr. Nass also, in another blog post, reveals what may one item behind what the ABIM is doing — the organization apparently wants to replace the physicians whose certifications were revoked with medical doctors from foreign countries: https://merylnass.substack.com/p/after-stripping-doctors-of-their, “After stripping doctors of their credentials and making it impossible to practice ethical medicine, the ABIM wants to bring in foreign medical doctors as replacements”, 24 August 2024. Below is a JPG of the ABIM’s statement, shared by Dr. Nass from another physician:
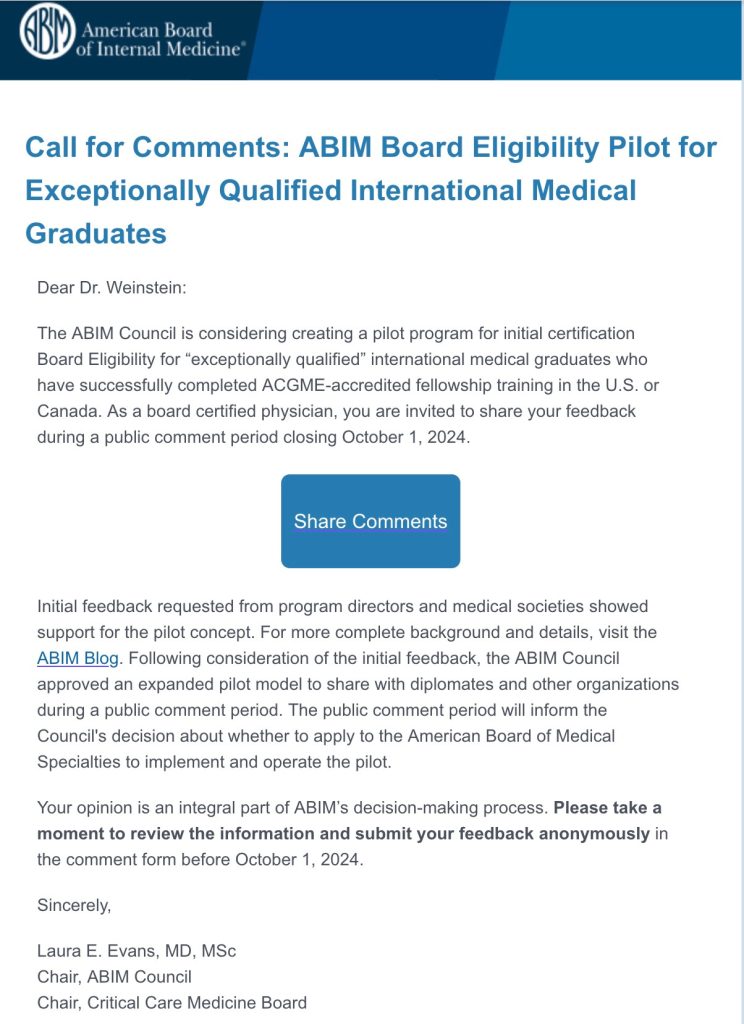
To add another aspect to the discussion, Yours Truly believes there ** may ** be some involvement of the AMA (American Medical Association) in the revoking of board certifications: AMA adopts new policy aimed at addressing public health disinformation, 13 June 2022. Below is a screenshot from the press release:
Note the penultimate point regarding “specialty boards.” In Yours Truly’s opinion, the AMA is one of the bastions of what may be called “Establishment Medicine” (the others being entities such as: the CDC; the FDA; the medical schools of Harvard University, Stanford University, Cornell University, etc.)
Let’s say that a board-certified physician, “fully vaccinated and boosted” who “followed the science”, after watching “vaccinated and boosted” patients, colleagues, perhaps even family members, begin to present with “the doctors are baffled” medical issues; or, perhaps, a cancer that was in remission that has returned. Let’s say that this physician starts to feel a little uneasy regarding the modRNA COVID-19 “vaccines” and does a little research — perhaps, by reading a blog or two written by someone like Dr. Kory; perhaps, by reading some published scientific literature regarding “first onset of psychosis after SARS-CoV-2 vaccination” (there are multiple papers discussing this that can be found online.) Let’s say that this physician comes to the realization that the modRNA COVID-19 “vaccines” are not “safe and effective”, but instead are the opposite. Let’s say this physician has board-certification renewal coming up in a few months. And, to top it off, let’s say that this physician has a family to provide for, a mortgage to pay, and medical school debt to pay off. What is this physician to do? — without jeopardizing the job, the board certification, perhaps even the License to Practice Medicine? It is Yours Truly’s opinion that this kind of situation is starting to “bubble under the surface” of more than one physician currently in practice. It is not an easy situation to be in.
Where does this situation leave the patient? If the physician who discovers that the modRNA COVID-19 “vaccines” (actually, gene therapy and modification injections [the DNA of the “vaccinated” person is changed by the ingredients and mechanisms of these “vaccines”]) are ineffective and dangerous, but doesn’t / can’t say a word to the patient to not take them — doesn’t this violate the oath of “First, Do No Harm” that the physician swore upon receiving the degree of Doctor of Medicine? If the physician who finds out, for example, that Paxlovid has a high “rebound infection” percentage, but doesn’t / can’t say a word to the patient to not take this combo-drug but substitute, say, Hydroxychloroquine, Zinc, and Vitamin D to combat a COVID infection — doesn’t this silence put the patient at risk? One in Five Experience Rebound COVID After Antiviral Drug, New Study Shows, 13 November 2023. The article regarding the DNA change made by the modRNA COVID-19 “vaccines” is here: https://doctors4covidethics.com/wp-content/uploads/2022/08/causality-article. “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, by Michael Palmer, MD, and Sucharit Bhakdi, MD, 18 August 2022. Slide 14 of this article is a graphic showing how the DNA of the COVID-19 “vaccinated” person is changed by the Pfizer-BioNTech modRNA COVID-19 “vaccine.”
How did the ABIM, the ABMS, and the other privately-run board certification granting entities in the United States come to have such power over the practice of medicine and over the physicians who obtain board certification? (There are literally dozens of these boards: www.americanboardcosmeticsurgery.org/so-what-does-physician-board-certification-actually-mean/, 7 February 2019.) To Yours Truly, it appears that they possibly used a combination of influence, lobbying, personal connections with medical schools, and other “tactics.” The result may well be an “authority” that these certification boards created and arrogatedto themselves, in the name of “ensuring quality delivery of healthcare by qualified physicians.” While this may have been a true and worthy aspiration previously, it seems it has “evolved” into “Follow these dictates, or else.”
And, from there, where does this potentially go? If a physician is stripped of board certification(s), that physician can still practice medicine — unless their state medical licensing board (perhaps with the involvement of the AMA, please see above in today’s post) decides to “charge” the physician with “spreading disinformation to the public” in “violation” of the diktats of Establishment Medicine. The physician now faces the possibility of losing the License to Practice Medicine. The case of Dr. Carrie Madej, DO, comes to mind. (Doctors of Osteopathy are medical doctors who have somewhat different training from MDs, but who are recognized and licensed to practice medicine and write prescriptions.) She was brought up on similar “charges” by the medical licensing board of Georgia. After a protracted fight, Dr. Madej ultimately decided to surrender her License to Practice Medicine in 2023. (Recall that Dr. Madej was one of the first to demonstrate that the modRNA COVID-19 “vaccines” contain substances that appeared to be strange.)
And, from there, where does the potential for innovation in medicine go? If physicians (especially board-certified physicians) have to, in effect, constantly “look over their shoulder” and “toe the line” to Establishment Medicine, doesn’t this affect the potential to come up with new theories and to investigate them? — such as in, using drugs in “off-label” circumstances to help patients? — such as in, using Hydroxychloroquine to prevent or treat COVID-19 infection, instead of injecting a patient with a modRNA COVID-19 “vaccine” that changes that patient’s DNA and can also lead to the appearance of myocarditis or even to the death of the patient? Instead of hospitalized COVID-19 infected patients being put on ventilators and given Remdesivir, a drug that can kill the patient instead of helping the patient? Why Remdesivir Failed: Preclinical Assumptions Overestimate the Clinical Efficacy of Remdesivir for COVID-19 and Ebola, Victoria C. Yan and Florian L. Muller, 17 September 2021.
Yours Truly will say it is vitally important that all persons, COVID-19 “vaccinated” or not, to have and keep their natural immune system in the best condition possible; to become educated regarding any prescription medication that they take; and, to research any medical injectables that are recommended / required that they be given.
“For you shall know the truth, and the truth shall make you free.” John 8:32
The above image of a physician performing a vaccination is courtesy of Google Images and The New York Times.
This post is the first of “Health Friday”, a new series of offerings related to Big Pharma, vaccines, general health, and related topics. It is an honor and privilege to contribute this series to the board. Since today’s post relates to COVID-19 and the COVID-19 “vaccines”, it is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023. However, the discussion will not be limited to what is presented today; it is an Open Thread.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here. “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
What Yours Truly writes in this series, as in her previous blog posts for this board, is not medical advice — they are opinions based on her over 4 1/2 years (and continuing) of reading about, researching about, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to please consult a healthcare practitioner regarding health concerns or conditions.
And now, to dive in. There is a lot to “unpack.”
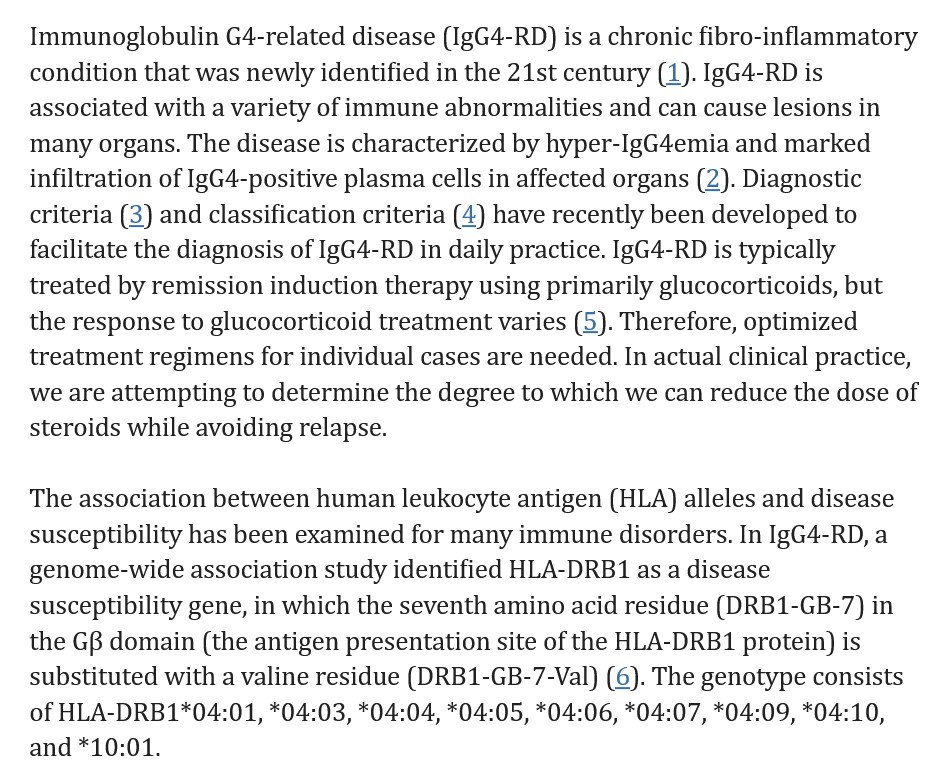
The modRNA COVID-19 “vaccines” induce IgG4-related disease (IgG4-RD.)IgG4-related disease(IgG4-RD) is a term that covers multiple medical conditions, ranging from neurological to ocular to cardiovascular to respiratory to gastrointestinal to urogenital. Since it is a chronic inflammatory condition, there can be more than one location of an IgG4-RD associated ailment within the patient’s body. Please see: https://en.wikipedia.org/wiki/IgG4-related_disease, “IgG4-related disease”, which has a list of symptoms in reported cases of IgG4-RD, and a list of body area sites that can be affected by IgG4-RD. The first instance of what is now called IgG4-RD was discovered in 1892 by Johann von Mikulicz, who diagnosed an “inflammatory disease of the salivary glands” in a patient (this condition was later called Mikulicz’ disease.) In 2021, Hamano et al. found elevated IgG4 levels in patients with Autoimmune Pancreatitis (AIP.) Please see: https://ojrd.biomedicalcentral.com/articles/10.1186/s13023-014-0110-z, “IgG4-related disease: an orphan disease with many faces”, Herwig Pieringer, et al., 16 July 2014. It appears that an issue with obtaining a true diagnosis of an IgG4-related disease is that many of the presenting elements can “mimic” other conditions, such as cancer or non-Hodgkin’s lymphoma. In addition, IgG4-RD can simply not present symptoms at all, until the patient concludes that “something is going on here.” In terms of the presenting symptoms of an IgG4-RD disease, there are, among others: storiform fibrosis (“spindle-shaped” cells that can, with collagen fibers, form a “flowing arrangement”); and, eosinophilia (high elevation of a type of white blood cell [eosinophils] that supports the natural immune system.) Please see: https://academic.oup.com/mr/article/31/3/529/6300281, “The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD”, Hisamori Umehara, et al., 4 May 2021. (Note: the entire article is restricted access.) Below is a portion from “IgG4-Related Disease” from StatPearls – NCBI Bookshelf, an article by Sudheer Nambiar and Tony I. Oliver (www.ncbi.nlm.nih.gov/books/NBK499825):
There are some IgG4-RD conditions that may be genetically-based; one example is Autoimmune Pancreatitis (AIP.) Please see: https://pubmed.ncbi.nlm.nih.gov/31104539/, “Genetic analysis of IgG4-related disease”, Yuki Ishikawa and Chikashi Terao, 7 June 2020. (Note: again, the entire article is restricted-access.) On the other hand, another IgG4-RD condition, Autoimmune Lymphoproliferative Syndrome (ALPS) appears to strike children. In addition, IgG4-RD conditions can be “immune-mediated” (meaning, the body’s immune system response is either inappropriate or excessive); and/or “autoimmune” (meaning, the body’s immune system attacks healthy tissues in the body.)
Yours Truly will examine the presence of eosinophilia as an indicator of IgG4-RD. This is an important “marker.” And it ties into the modRNA COVID-19 “vaccines” — the COVID-19 “vaccinated” person’s natural immune system being damaged and/or destroyed by the ingredients and mechanisms of these “vaccines”; and, with repeated injections of these “vaccines” compounding this damage and/or destruction.
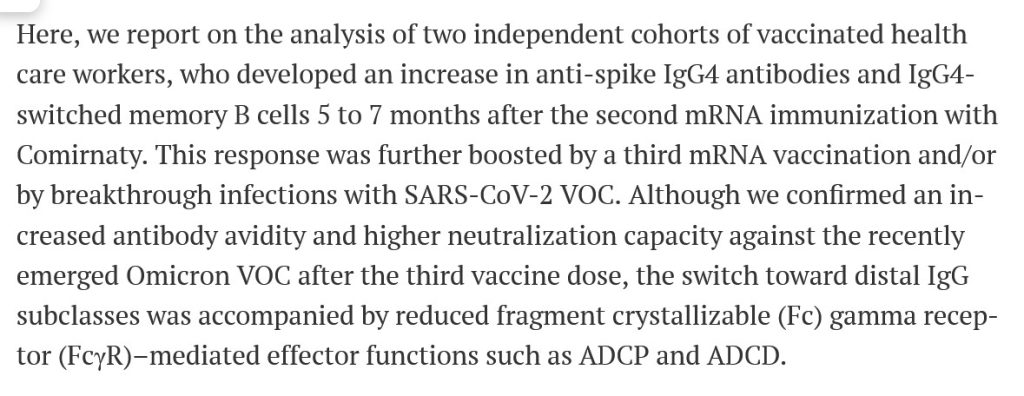
The first item is a blog article by Dr. Jessica Rose, PhD: https://jessicar.substack.com/p/igg4-related-disease-and-igg4-means, “IgG4-related disease (IgG4RD) means FIBROSIS and organ destruction”, 28 December 2022. It is now known that the modRNA COVID-19 “vaccines” induce a “class switch” in the COVID-19 “vaccinated” person’s natural immune system; this “class switch” is the damage and/or destruction of IgG3 immune system cells (these cells help to fight off infections and other enemies that “invade” the natural immune system), replacing IgG3 cells with increased numbers of IgG4 cells (these cells help to allow the body to “tolerate” assaults to the natural immune system.) Repeated injections of modRNA COVID-19 “vaccines” exacerbate this process: please see https://doi.org/10.1126/sciimmunol.ade2798, “Class switch toward non inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination”, Irrgang P, et al., 22 December 2022. Notice the title: “non inflammatory”, “spike-specific”, “IgG4”, and “repeated SARS CoV-2 mRNA vaccination.” IgG4-RD conditions can present as non-inflammatory (the patient doesn’t notice anything wrong for some period of time, see above in today’s post); however, the IgG4 levels in the patient are high upon examination. Below is a portion of the Introduction of the above paper. Note: Comirnaty was the non-United States version of the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2. Comirnaty and BNT162b2 are the same product. Note 2: the 2023-2024 Comirnaty modRNA COVID-19 “vaccine” was given full FDA approval for use in the United States on 23 September 2023 for persons age 12 above: www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-receive-us-fda-approval-2023-2024-covid; the version that the FDA authorized (the “2023-2024 Formula COVID-19 Vaccine” by the same company) was for persons age 6 months through 11 years of age (www.fda.gov/media/167211/download.)
Note that the IgG4 cell increase extended for months after the second injection of Comirnaty and was further increased after the third injection. This correlates to the original “two-injection Primary Series” plus the original “booster shot” of Comirnaty that millions of persons took between December 2020 and early 2022. This would also include, since the formulations were the same, of the “Primary Series” and the original “booster shot” of BNT162b2 that were taken by millions of persons in the United States from December 2020, until Comirnaty was given full FDA approval in the United States on 8 July 2022 for persons age 12 and older (at which point, BNT162b2 was “replaced” by Comirnaty except for use in persons age 6 months to 11 years; the FDA authorized the “Pfizer-BioNTech COVID-19 Vaccine” for this age group.) This “product name situation” may seem a little confusing: at bottom, it had to with removal of liability for the “vaccine” manufacturer. This will be discussed at a later date.) Note also that “VOC” means Variants of Concern (in other words, the Delta, the Omicron, the XBB.1.5 variants of the SARS-CoV-2 [COVID-19] virus, and so on.)
The second item is here: www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021, given by Pfizer-BioNTech to the FDA on 30 April 2021. This report covers Adverse Event Reports that were submitted to the company between 11 December 2020 (the date on which the FDA in the United States granted the initial Emergency Use Authorization (EUA) for BNT162b2 to be used in the United States, 21 December 2020 (the date on which the EMA (European Medicines Agency) granted its initial EUA for BNT162b2 to be used in Europe / Scandinavia; and, 28 February 2021. The APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST, which begins on Page 30 of this report, lists over 1,200 different types of medical adverse events that were reported to Pfizer-BioNTech from the worldwide EUA start dates above. On Page 3 and Page 4 of the APPENDIX 1. (Page 32 and Page 33 of the report), there are the following Adverse Events of Special Interest listed: Eosinopenia; Eosinophilic fasciitis; Eosinophilic granulomatosis with polyangiitis; Eosinophilic oesophagitis. On Page 5 of the APPENDIX 1. (Page 34) of the report, there is listed: Immunoglobulin G4 related disease. On Page 8 of the APPENDIX 1. (Page 37 of the report) there is listed: Sjogren’s syndrome (another type of IgG4-RD.) These are a few of the IgG4-RD types of reports that are listed in the APPENDIX 1. section. Thus, the FDA knew, on 30 April 2021, that BNT162b2 “vaccination” induces IgG4-related disease conditions. Yet, the FDA did nothing to stop the continuing rollout of BNT162b2.
A third item is here: https://mole.substack.com/cp/147758416, a 15 August 2024 cross-post from Lioness of Judah Ministry, “German Study Links Covid Shots to Surge in VITAL ORGAN DAMAGE among Children”. The study found that there was a large increase of organ damage induced by BNT162b2 in children in Germany ages 5 to 11 years old. The study is here: https://journals.lww.com/pidj/fulltext/9900/delayed_induction_of_noninflammatory_sars_cov_2.959.aspx, “Delayed Induction of Noninflammatory SARS-CoV-2 Spike-Specific IgG4 Antibodies Detected 1 Year After BNT162b2 Vaccination in Children”. Kobbe, Robin MD, et al., 30 July 2024. The IgG4 antibodies were detected after the second dose of BNT162b2 (in other words, after the “Primary Series” of two BNT162b2 injections was completed.)
And, a fourth item is here, related to COVID-19, the COVID-19 “vaccines” and autoimmune conditions: https://wmcresearch.substack.com/p/long-covid-is-an-autoimmune-disease, “Long COVID is an Autoimmune Disease: Injecting Mice with IgG from Long COVID Patients Induces Symptomology”, by Walter M Chesnut, 4 June 2024. Mr. Chesnut has long posited that the spike protein of the COVID-19 virus itself contains elements that attack the natural immune system of the body of a person infected with this virus; and that the COVID-19 virus itself can induce what is now called “Long COVID.” Yours Truly will add the opinion that the difference between “Long COVID” in a person who is “unvaccinated” against COVID-19, and “Long COVID” in a COVID-19 “vaccinated” person, is this: the natural immune system of the “unvaccinated” person still has the potential to not only fight off a COVID-19 infection, but also to mitigate or eliminate the chance that “Long COVID” may result from the infection; whereas, the natural immune system of the COVID-19 “vaccinated” person has been damaged (or worse), resulting in a much larger potential for “Long COVID” (both in presentation and in duration.)
Yours Truly believes that the COVID-19 virus itself, and the ingredients and mechanisms of the modRNA COVID-19 “vaccines” (one of these ingredients being a “lab-modified” form of the RNA of said virus), both attack the natural immune system of the body. The COVID-19 “vaccines” have been shown to damage and/or destroy the IgG3 cells of the body’s natural immune system (these cells help to fight off viruses, etc.), replacing these with increased amounts of IgG4 cells (“toleration facilitator” cells.) In Yours Truly’s opinion, one of the important details here is the targeting of HLA cells (human leukocyte antigen cells, a type of white blood cells) by the COVID-19 virus itself, and, by extension, the COVID-19 “vaccines.”
And, from this paper: www.ncbi.nlm.nih.gov/pmc/articles/PMC10864075, “HLA-DRB1 Is Associated with Therapeutic Responsiveness in IgG4-related disease”, Motohisa Yamamoto, et al., 23 May 2024:
Note that one of the most-recommended and used treatments for IgG4-RD conditions is glucocorticoids (steroids); and that cessation of treatment likely results in relapse of the condition. But, long-term use of glucocorticoids have risks, including high blood pressure and Cushing’s Disease. Please see: www.webmd.com/multiple-sclerosis/what-are-glucocorticoids.
Yours Truly will posit that the lab-created SARS-CoV-2 (COVID-19) virus itself, with the lab enhancements made to the mRNA of this virus to create the modRNA of the COVID-19 “vaccines” (such as the SV40 African Green Monkey cancer promoter gene piece in BNT162b2), plus the addition of dangerous lipid nanoparticles (ALC-0159 and ALC-0315 in BNT162b2 and its “descendant” COVID-19 “vaccines”; and, SM-102 in the Moderna mRNA-1273 modRNA COVID-19 “vaccines” and its “descendant” COVID-19 “vaccines”) and other ingredients in these “vaccines” — have been, and continue to be, designed to wreak as much havoc and damage on the human race as possible. This havoc and damage includes that done to the body’s natural immune system, its elements, mechanisms, and responses. Recall that the “descendant” modRNA COVID-19 “vaccines” use the original (lab-enhanced) SARS-COV-2 (COVID-19) virus modRNA that was present in the earlier versions of these “vaccines”, but in smaller amounts. Therefore, in one’s opinion, the potential exists for immune system damage in persons who take these “descendant” modRNA COVID-19 “vaccines.”
Until fairly recently, it was not known HOW, or the DETAILS behind WHY, the COVID-19 virus itselfand the COVID-19 “vaccines” have such potential for havoc and damage — all that was beginning to present were, and are, the ADVERSE EFFECTS of the virus and especially of the “vaccines”: turbo-cancers; miscarriages; Bell’s Palsy; deaths; the Adverse Events of Special Interest listings of negative effects induced by BNT162b2 in the APPENDIX 1. cited above. It is now starting to become more clear as to what SPECIFIC elements likely used in the creation of both the SARS-CoV-2 virus itself, and in the development of the modRNA COVID-19 “vaccines.” Yours Truly will posit that one of these SPECIFIC elements is something that attacks and compromises at least one important component of the human body’s immune system: the antigen site of the human leukocyte protein DRB1 (HLA-DRB1.) It took time, effort, and large amounts of funding to investigate these SPECIFIC elements; to experiment with them to ascertain the damage that could be caused; then, to “insert” these elements into the SARS-CoV-2 virus itself, and, by extension, into the modRNA COVID-19 “vaccines.” And, as the passage of time obscures or obliterates “fingerprints” of the damage done by the COVID-19 “vaccines” in the “vaccinated” individual, the involvement of these “vaccines” may well become harder and harder to trace (even though the damage is continuing in the “vaccinated” person, since one of the mechanisms of said “vaccines” is to change the DNA of the person who takes them.) Below is Slide 14 from the Palmer, MD and Sucharit, MD, article regarding what the COVID-19 “vaccines” do to the “vaccinated” person’s body. Slide 14 shows how the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2 changes the DNA of the “vaccinated” person:
Yours Truly will emphasize that it is of the utmost importance that all persons, COVID-19 “vaccinated” or not, have and maintain the highest degree possible of natural immune system health. A healthy diet is one of many ways to support and maintain a healthy natural immune system. Here is an article on this topic: www.medicalnewstoday.com/articles/322412, “The best foods for boosting your immune system”, by Lana Burgess, 10 July 2018. Among other ways to help the natural immune system are lifestyle changes, regular exercise, taking supplements, and addressing stress, as discussed here: www.healthline.com/nutrition/how-to-boost-immune-health, “9 Ways to Boost Your Body’s Natural Defenses”, by SaVanna Shoemaker, RDN, 1 April 2020. Yours Truly will add the opinion that avoiding unnecessary antibiotics and “certain injectables” are additional items to consider.
The above image is of mass vaccination against smallpox in Paris in 1905. (Courtesy, Getty Images.)
Today’s post will trace what ** may be ** a “sleight-of-hand” that started out with Xavier Becerra, the Secretary of the United States government Department of Health and Human Services, giving the “Go-Ahead” for the use of the H5N1 Avian Influenza “vaccine”, AUDENZ, in anticipation of a potential “bird flu pandemic” in the United States; but, which since has been “transformed” into the American Medical Association just issuing new CPT codes for an Avian Influenza “vaccine” for a different strain, called H5N8. Meanwhile, the CDC / FDA / United States government, are all sending out warnings related to the H5N1 strain. Stay with Yours Truly, it gets even better — “Mais, mon Dieu!” — the twists and turns! This post is a kind of “snapshot” of the situation — it is an evolving issue.
For purposes of today’s post, the trail begins here: www.ernst.senate.gov/imo/media/doc/fowl_play_squeal.pdf, the letter that Sen. Jodi Ernst (R-Iowa) sent to USDA Secretary Tom Vilsack on 14 February 2024. In this letter, Sen. Ernst demands answers regarding United States government funding of what appears to be Gain-of-Function research experiments on Avian Influenza viruses; which experiments involve a scientist linked to the Chinese Communist Party. Yours Truly can find to date, no response from Sec. Vilsack to Sen. Ernst. A screenshot of Page 1 of her letter is below:
Yours Truly now turns to this: www.aha.org/news/headline/2024-07-23-hhs-broadens-emergency-declaration-facilitate-response-bird-flu-other-viruses-pandemic-potential, “HHS broadens emergency declaration to facilitate response to bird flu, other viruses with pandemic potential”, dated 23 July 2024, which “expanded” the 2013 amendment to the Federal Food, Drugs, and Cosmetics Act to now include “other viruses” that may have “pandemic potential.” The document, from HHS Secretary Xavier Becerra, specifically mentions three types of Avian Influenza strains: H1N1 (from 2009); H7N9 (from the 2013 amendment);, and H5N1 (from the 24 March 2024 USDA statement regarding H5N1 infections in dairy cows in Kansas and in Texas.) https://public-inspection.federalregister.com/2024-16247.pdf. Below is a screenshot from the AHA (American Hospital Association) press release:
And, for reference, here is the Congressional Research Service Legal Sidebar document related to what the HHS Secretary can “declare” under the PREP Act (including removing liability options), updated 21 July 2023: https://crsreports.congress.gov/product/pdf/LSB/LSB10730, “The PREP Act and COVID-19, Part 2: The PREP Act Declaration for COVID-19 Countermeasures.”
Meanwhile, the USDA had already issued a press release regarding how dairy farmers can apply to receive expanded livestock assistance to compensate for milk production lost due to their cows infected with H5N1: www.usda.gov/media/press-releases/2024/06/27/usda-begin-accepting-applications-expanded-emergency-livestock, “USDA to Begin Accepting Applications for Expanded Emergency Livestock Assistance Program to Help Dairy Producers Offset Milk Loss Due to H5N1”, dated 27 June 2024.
So, it would appear that the HHS gave the “go-ahead” for a kind of “EUA” regarding the use of the protein-subunit H5N1 “vaccine”, AUDENZ (a supply is already in the National Vaccine Stockpile); and, for the increased production of this “vaccine.” What follows is a “closer look” at AUDENZ. Yours Truly will begin with the FDA-issued Fact Sheet for healthcare providers for this “vaccine”: www.fda.gov/media/135020/download; three screenshots from the document are below. The first screenshot shows clearly that there was no Placebo group (Control/saline group) in at least two clinical trials for AUDENZ. The second screenshot shows clearly that no Toxicology studies were performed for AUDENZ. The third screenshot is Page 10 of the Fact Sheet.
Note this language in the first screenshot: “In both Studies 1 and 2, all SAEs appeared unrelated to study treatment.” This indicates at least two important details: One, that Serious Adverse Events (SAEs) did occur during at least two clinical trials of AUDENZ; and, Two, that these Serious Adverse Events were not considered to be related to the clinical trials for AUDENZ. This is the same type of language that Pfizer-BioNTech used regarding Serious Adverse Events that occurred during the (shortened and data-compromised) clinical trials for the company’s “flagship” COVID-19 modRNA “vaccine” BNT162b2. Note also that a “complete dose series” for AUDENZ is two separate doses of 0.5mL each, for all age groups age six months and up. AUDENZ uses an adjuvant (an ingredient that facilities the activities of the injectable) called MF59. MF59 is a squalene-based, oil-in-water adjuvant. The Safety Data Sheet for MF59 is here: https://file.medchemexpress.com/batch_PDF/HY-153206/MF59-SDS-MedChemExpress.pdf. The product is listed as “Not a hazardous product or mixture” in section 2.2 of this document. However, reading further down the same document, one finds all sorts of contradictory information in the sections on “First Aid Measures”, on “Handling and Storage”, on “Exposure Controls”, and more.
Note also the list of reported adverse events in section 6.2 of Page 10, above. These are same types of adverse events reactions to the Pfizer-BioNTech modRNA COVID-19 “vaccine”, BNT162b2, in the post-authorization report that this company gave to the FDA on 30 April 2021; and in reports to VAERS; and, which are listed within the FDA-issued Fact Sheet for Healthcare Providers for the “2023-2024 Formula COVID-19 Vaccine” by Pfizer-BioNTech (www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf; www.openvaers.com/; www.fda.gov/media/167211/download?attachment. Very troubling are the listings in section 6.2 of Page 10 above in the AUDENZ fact sheet for “convulsions”; “demyelination”; “encephalitis”; and, “Guillain-Barre’ syndrome.”
A blog post by Dr. Jessica Rose, PhD, on 27 June 2024, presents a summary of clinical trial for AUDENZ (NCT02839440), in which she proves that the fatality rate is 1/200 chances for AUDENZ: https://jessicar.substack.com/p/1200-chance-of-death-in-context-of, “1/200 chance of death in context of new bird flu injection – 5 times higher than placebo according to clinical trial.” NCT02839440 did have a Placebo control group, (Scroll down the blog post to the discussion of this clinical trial for AUDENZ.)
To date, Yours Truly can find no exact set of CPT Codes for AUDENZ. The closest item found is here: www.hhs.gov/guidance/document/flu-shot-coding-0; the listing is “Q2039 Influenza virus vaccination otherwise specified.”
AUDENZ is produced by CSL Seqirus, part of the much-larger CSL multinational drug company. Following is a JPG of the list of CSL offices and locations, sourced from: www.csl.com/:
The United States government awarded CSL Seqirus a contract to produce millions of doses of an Avian Influenza “vaccine” in May 2024: www.cslseqirus.us/news/csl-seqirus-announces-us-government-award-in-response-to-avian-influenza. The “vaccine” will be manufactured by the CSL Seqirus facility at Holly Springs, North Carolina. This facility was built in partnership with BARDA (Biomedical Advanced Research and Development Authority), a department of the United States government. The Avian Influenza “vaccine” that this facility will manufacture is “cell-based”, as opposed to “egg-based”; with a six-month “turnaround” for production: www.csl.com/we-are-csl/our-business-and-products/csl-seqirus/csl-seqirus-manufacturing-technologies. Below are two images from the article related to this facility:
Note that whatever Avian Influenza cell-based “vaccine” from the CSL Seqirus facility at Holly Springs will use the MF59 adjuvant. (By the way, MF59 is trademarked by Novartis AG, which was acquired by CSL.)
So far, it appears that the H5N1 strain of Avian Influenza is the one that the United States government is focused upon. However, here’s where the trail veers to another path.
Please refer back to the American Hospital Association press release above in today’s post. Note this language: “The amendment now applies to pandemic influenza A viruses and others with pandemic potential, such as the current H5N1 strain of bird flu…” (Italics, Yours Truly) In Yours Truly’s opinion, this is “a hole big enough to drive a truck through” — or, perhaps, another strain of Avian Influenza.
The following article beings to “lift the curtain” on what ** may ** really be going on — which, again in Yours Truly’s opinion, appears to be a kind of “sleight-of-hand”: www.naturalnews.com/2024-07-26-fda-grant-eua-mrna-bird-flu-vaccines.html, “Pandemic 2.0 ready to go: FDA to grant emergency use authorization (EUA) to mRNA bird flu shots, just like what happened with COVID“, by Ethan Huff. And, “right out of the gate”, the article begins with this:
But, wasn’t the “upcoming potential bird flu pandemic” supposed to be the H5N1 strain that the government is warning about? Where does the H5N8 strain come in? According to Wikipedia, the H5N8 strain of Avian Influenza is “is typically not associated with humans.” https://en.wikipedia.org/wiki/Influenza_A_virus_subtype_H5N8. Very few humans have contracted a case of H5N8; this virus strain predominates among wild birds. However, the mortality rate among wild birds infected with H5N8 is “at least 75%”, again according to the Wikipedia article above.
What’s going on here? The picture is, to say the least, somewhat “murky.” There are, however, a few potential clues. Among them is this: www.pennmedicine.org/news/news-releases/2024/may/penn-researchers-develop-experimental-mrna-avian-flu-vaccine, dated 23 May 2024. Note on the screenshot, below, from the article, the language regarding “a specific type of the H5N1 virus”; and, that animals other than wild birds were being used for the experiments:
And, a fourth clue is here: https://clinicaltrials.gov/ct2/show/NCT05874713, a clinical trial that appears to be in the “wrapping-up” stages regarding testing an mRNA-based H5N8 “vaccine.” Below is a screenshot from the Clinical Trials webpage for this clinical trial:
Note the very low test subject enrollment (480 persons); the presence of the MF59 adjuvant in the H5N8 “vaccine” candidate used in the clinical trial; and, a “two-dose” series of “primary run” injections of the “vaccine” candidate, followed by a “booster shot” on Day 209 for the H5N8 “vaccine” candidate.
There are three other clinical trials of an H5N8 “vaccine” listed on the https://clinicaltrials.gov/ website: NCT02624219 (Completed); NCT05975840 (Active); and, NCT03014310 (Completed.) All of these clinical trials were/are Phase I or Phase I/II. None of them have a Placebo/saline control group. Each of them have fewer than 600 subjects (NCT02624219 had 275 test subjects.) Two of these three other clinical trials have the NIAID as the Sponsor.
What does all this mean? Is it possible that the current H5N1 “Avian Influenza infecting cattle, cows, and domesticated pets, in addition to poultry” situation, while it is indeed occurring, is also a sort of “Look, squirrel!” to distract from something that may be more dangerous?: from, perhaps, Gain-of-Function experiments on the H5N8 strain of the Avian Influenza (recall that this strain has a 75%+ mortality rate among the wild birds that it infects); plus, perhaps. the development of “vaccines” for this “perhaps-enhanced” H5N8 strain, which may include the millions of doses of an “Avian Influenza cell-based vaccine” that will be manufactured at the CSL Seqirus facility in North Carolina? In other words, “Pandemic 2.0”?
The above is a vintage image of mass vaccination. (Courtesy Google Images.)
This series on the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
The origination of today’s post begins here: www.dossier.today/p/double-digits-biden-admin-tells-americans, “Double Digits: Biden Admin tells Americans that it’s soon time for their 10th Covid shot“, by Jordan Schachtel, 13 June 2024. (Mr. Schachtel wrote about the ninth COVID-19 “vaccine” injection here: www.dossier.today/p/dose-number-nine-cdc-panel-green, “Dose number NINE: CDC panel green lights yet another Covid mRNA shot“, 29 February 2024. The CDC recommended that persons over age 65 take another “booster shot” of either the Pfizer-BioNTech or of the Moderna “2023-2024 Formula COVID-19 Vaccine” of these manufacturers.) A person age 65 or older, if that person adhered to every CDC recommendation regarding taking a COVID-19 “vaccine” injection since December 2020 (when the FDA granted first Emergency Use Authorization (EUA) to Pfizer-BioNTech and to Moderna for these companies’ “flagship” modRNA COVID-19 “vaccines” (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), would have taken injection number nine starting on 28 February 2024.
Today’s post is long. There is a large amount of information to “unpack.” Stay with me here.
Note the language regarding the “selection of a specific JN.1 lineage SARS-CoV-2 strain…” More about that later.
The trail behind the 5 June 2024 FDA announcement begins with the VRBPAC Briefing Document for the meeting held on 28 June 2022: www.fda.gov/media/159452/download, “FDA Briefing Document Vaccines and Related Biological Products Advisory Committee Meeting June 28, 2022.” It was at this meeting that the FDA “codified” the types of “strain composition recommendations” that the agency would use regarding “new versions” of COVID-19 “vaccines.” Yours Truly presents page 17, page 18, and page 19 of this document:
It appears that the FDA simply decided that it would be permissible for the agency to authorize a new COVID-19 “vaccine” strain composition along what, in Yours Truly’s opinion, may be called “very flexible” options. For example, the Pfizer-BioNTech XBB.1.5 COVID-19 “vaccine”, which was FDA authorized in the fall of 2023, had test results only from mouse testing prior to FDA authorization. Following are: The link to the Pfizer-BioNTech slide presentation about this “vaccine” to the CDC’s ACIP committee (Advisory Committee on Immunization Practices) meeting of 12 September 2023; and, an image of slide CC4 from this presentation. First, the presentation: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-09-12/10-COVID-Modjarrad-508.pdf.
Second, slide CC-4 from the above presentation:
The XBB.1.5. Pfizer-BioNTech COVID-19 “vaccine” had only been given as a single injection to humans in the company’s clinical trial; a clinical trial which had only just begun prior to the ACIP meeting. Slide CC-5 of the presentation, the start of the company’s human trial of this “vaccine”, is below:
Slide CC-6 of the presentation has to do with the mouse studies of this “vaccine”, which were of longer duration.
Notwithstanding the above, the FDA authorized the use of the company’s XBB.1.5 COVID-19 “vaccine” on 11 September 2023 (in Yours Truly’s opinion, it appears that the ACIP meeting of 12 September 2023 was a “catch-up” formality.) It also appears (again, in Yours Truly’s opinion), that the FDA used a very loose interpretation of “Option 4” on page 18 of the FDA Briefing Document above in granting the EUA for this “vaccine”.
** Now, on to the latest “new version” of the COVID-19 “vaccines”, the “2024-2025 Formula COVID-19 Vaccines”, that the FDA authorized in June 2024.
The following linked items are important regarding background information related to this situation and to the FDA: First, the FDA document, stating that the agency would “align” its COVID-19 “vaccine” antigen composition to the recommendations of the World Health Organization’s TAG-CO-VAC recommendations: www.fda.gov/media/179139/download (the TAG-CO-VAC recommendation for the “2024-2025 Formula COVID-19 Vaccines” was to use the JN.1 strain); second, the FDA document regarding “considerations and recommendations” for the “2024-2025 Formula COVID-19 Vaccine” composition: www.fda.gov/media/179145/download; third, the FDA announcement of the 5 June meeting of its VRBPAC committee (Vaccines and Related Biological Products Advisory Committee.): www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-june-5-2024-meeting-announcement. From this last link, chick on “Event Materials” to see the slide presentations and other items that were discussed at this meeting.
Two important items from the “Event Materials” list: the FDA Briefing Document; and the VRBPAC roster for this meeting. First, the FDA Briefing Document: www.fda.gov/media/179003/download; and, second, the VRBPAC roster for this meeting: www.fda.gov/media/179225/download. The roster for the 5 June 2024 meeting has some “familiar” members and speakers: Paul Offit, MD; and Peter Marks, MD (director of CBER [Center for Biologics Evaluation the Research of the FDA]); and, among the “Temporary Voting Members”, are: Bruce Gellin, M.D., M. PH., the Chief of Global Public Health Strategy for the Rockefeller Foundation; and, Melinda Wharton, M.D., M. PH., Associate Director of Vaccine Policy of the CDC. (Italics mine)
The VRBPAC members voted unanimously to endorse the Pfizer-BioNTech, the Moderna, and the Novavax “2024-2025 Formula COVID-19 Vaccine” by these companies, based on the presentations of these companies’ representatives at the meeting. Yours Truly can find noregistered human clinical trials performed in advance of the 5 June VRBPAC meeting by Pfizer-BioNTech, or by Moderna, or by Novavax, for any “2024-2025 Formula COVID-19 Vaccine”; that would indicate that any “clinical trials” were performed in these companies’ facilities on mice; and that any “human trials” were also performed in these companies’ facilities, prior to the meeting. The FDA then issued the agency’s original announcement of 7 June 2024: www.fda.gov/news-events/press-announcements/fda-roundup-june-7-2024; and, a screenshot from this announcement:
Note in particular “…the selection of a specific JN.1 lineage SARS-CoV-2 strain (e.g., JN.1. or KP.2) and expressed a strong preference for JN.1.” Here’s where it starts to “get interesting.”
What was it that happened? Part of the answer lies in the fact that the NIH and Moderna co-own the patents (and, therefore, share the royalties) for the Moderna “flagship” modRNA COVID-19 “vaccine”, mRNA-1273. This agreement would extend to “descendant clone COVID-19 vaccines” by Moderna. www.citizen.org/article/modernas-mrna-1273-vaccine-patent-landscape/. The NIH’s Dale and Betty Bumpers Vaccine Research Center (part of NIAID — which Dr. Anthony Fauci led from November 1984 until his retirement in December 2022) and Moderna co-developed mRNA-1273. https://covid19.nih.gov/news-and-stories/nih-vaccine-research-center; a screenshot from the article is below:
The other part of the answer is that Moderna was already developing a KP.2 strain COVID-19 “vaccine” for 2024-2025. This, and the FDA’s decision to shift away from the JN.1 strain to the KP.2 strain, are described in this post at Sasha Latypova’s blog: https://sashalatypova.substack.com/p/all-roads-lead-to-resilience, “All Roads lead to Resilience. FDA is removing competitors for the Pentagon & CIA’s baby…Moderna”, 23 June 2024.
However, there’s yet another detail in play here, regarding the FDA’s switch, “based on evaluation of the most recent circulating strains of COVID-19”, from JN.1 to KP.2 — the CIA and the Pentagon. Here is a screenshot from Sasha Latypova’s Substack article:
But wait, there’s more! Resilience lists multiple “partners”, such as the Mayo Clinic. The company also, apparently, has a “partnership” with the United States Army’s Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense https://resilience.com/learn/partnerships. Below is a screenshot from this website:
It appears, then, in Yours Truly’s opinion, that the FDA was perhaps “reminded” of the”details” regarding the NIH-Moderna co-ownership (and royalties – sharing) agreement related to Moderna’s modRNA COVID-19 “vaccines”; and, the role of the CIA-Pentagon-National Resilience (aka Resilience) in manufacturing the mRNA used in the Moderna COVID-19 Omicron “booster vaccines” — and the KP.2. strain is indeed a “descendant strain” in the Omicron lineage (as is the JN.1 strain.) Hence, the FDA’s 2024-2025 COVID-19 “vaccine” strain “sudden switch” announcement of 13 June 2024, only one week after the agency gave the nod to the JN.1 strain.
In Yours Truly’s opinion, it is statistically, medically, and ethically impossible for a new vaccine (let alone any COVID-19 “vaccine”) to be developed; tested (on lab animals, then on human subjects); the test data thoroughly collated and analyzed for “safety and efficacy” on both lab animals and on human subjects; then, which data is presented to the CDC / FDA for consideration; then, these agencies doing their own “due diligence” research; then, and only then, being granted an EUA by the FDA; then, and only then, manufactured for use in humans — in a time span of fewer than three to five years, let alone within a time span of only a few months. It appears, again in Yours Truly’s opinion, that the CDC and the FDA are playing “fast and loose” with the health and safety of the people who choose (or will be “mandated”) to take the “2024-2025 Formula COVID-19 Vaccine.” And, also, that “other entities” are in play here to perhaps “influence” decision making by these agencies.
All of above is in addition to the fact that the COVID-19 “vaccines” (actually, gene therapy injections) have caused, are causing, and will cause, multiple health issues, serious adverse reactions, and deaths, in those who are “vaccinated.” Just two of the most recent discoveries: One, the COVID-19 “vaccines” can cause brain damage, an article by Dr. William Makis: www.globalresearch.ca/brain-damage-covid-19-mrna-vaccines/5861012, “Brain Damage Caused by COVID-19 mRNA Vaccines”, 26 June 2024. Below is a screenshot from Dr. Makis’ article:
The second most recent discovery, that the COVID-19 “vaccines” reduce life expectancy (even in “all-cause” analysis) among COVID-19 “vaccinated” persons, by Dr. Peter A. McCullough: https://petermcculloughmd.substack.com/p/breaking-publication-a-critical-analysis, “BREAKING Publication — A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, 1 July 2024. The peer-reviewed paper is here: https://doi.org/10.3390/microorganisms12071343, “A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, Marco Alessandria, et al., published 30 June 2024. Below is a screenshot from the Conclusions section of this paper:
In Yours Truly’ opinion, it is apparent at “half a glance” that the COVID-19 “vaccines” (actually, gene therapy injections) must be completely withdrawn for human use until these products have been fully investigated, and then re-designed, before being re-introduced for human use; and, that there is no “co-ownership” or sharing of royalties between a government agency and a COVID-19 “vaccine” manufacturer; and, that there is no involvement of the United States military in the development or manufacture of such products.
The above image is from the Textbook of Anatomy and Physiology, by Kimber, Gray, and Stackpole. Published by The Macmillan Company; eleventh edition, 1944. (Image courtesy of Laurel Leaf Farm.)
This post, part of a series on the disaster of COVID-19 and the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023. Today’s offering will speak to what might be called a “tangential” issue: the American Medical Association (the AMA.) Yours Truly will make it clear at the outset that today’s post is not to be construed as a “hit piece” on the AMA; also, that there arelikely many members of the AMA who are not “beholden” to blindly accept everything that the AMA publishes. The point of today’s piece, in one’s opinion, is that the current AMA apparently sees itself as a sort of “arm” of “establishment medicine” (in other words, of the FDA and the CDC); in addition to becoming an organization that advocates what may be called “medico-political” viewpoints. First, before discussing the AMA Edhub, some items about the organization:
It is fair to posit that the American Medical Association (also referred to as the AMA) is the largest and most powerful medical doctor organization in the United States. The AMA has also become, arguably, the most powerful medical organization lobbyist in the United States House of Representatives and the United States Senate.
The American Medical Association is a “heavy-spender” lobbyist to the United States federal government, spending at least $15 million per year in this effort since 1998: www.influencewatch.org/non-profit/american-medical-association/ (this article also has a history of the AMA, the organization’s views on healthcare policies, and so forth); in the year 2022 alone, the AMA spent $21,060,000 on federal government lobbying, per Open Secrets: www.opensecrets.org. A screenshot of the Influence Watch report on the AMA is below. Note that the AMA owns the exclusive rights to the medical expenditure reimbursement codes system for Medicare and Medicaid (the CPT codes.) This entails the payments of “rights and royalties” to the AMA. For further information, please refer to: https://microwize.com/why-do-i-have-to-pay-a-fee-to-use-cpt-code/, 14 December 2022.
The AMA has a “membership dues schedule”, ranging from $20 for a 1-year medical student membership, through a $420 per year dues fee for a “Regular practice” physician who belongs to the AMA. And, there are other types of membership available (corporate and e-membership.) www.amanet.org/membership/. There are other types of corporate and institutional memberships available through the AMA Foundation, also called the “Roundtable.” (https://amafoundation.org/donors/corporate-donors/). A screenshot of the “Silver Level” corporate donor list to the AMA is below (the “Silver Level” requires a $30,000 contribution to the AMA Foundation, presumably paid each year by each donor company):
Two other areas of AMA effort are in physician Continuing Education and in publishing. Members of the AMA who are licensed medical doctors can fulfill their Continuing Education accreditation through courses offered by the organization. These courses are offered via various methods: www.ama-assn.org/topics/contuning-medical-education. The AMA also publishes a journal, known as JAMA (Journal of the American Medical Association): https://jamanetwork.com/. The website is open-access, and there are hundreds of peer-reviewed articles from thirteen different JAMA specialty journals available for public reading for several months after articles are published. As might be expected, the AMA advocates for what might be called “establishment medicine” — for example, championing FDA-authorized or FDA-approved treatments and drugs for COVID-19 infection.
Yours Truly will include part of the Abstract (below) of a recent paper published in JAMA, regarding people who mistrust “establishment medicine” (in other words, they may mistrust FDA-authorized or FDA-approved) treatments for COVID-19. This paper, in Yours Truly’s opinion, demonstrates the AMA’s official attitude towards those who question or refuse “establishment medicine” treatment of COVID1-19 and pursue other, alternative treatments — that these people are “being misled” by “misinformation” and may use that “misinformation” to avoid “health-promoting behaviors.” The paper is found here: https://jamanetwork.com/journals/jama-health-forum/fullarticle/2809985, “Misinformation, Trust, and Use of Ivermectin and Hydroxychloroquine for COVID-19”, Roy H. Perlis, MD, et al., published 29 September 2023. Dr. Perlis is Associate Editor of JAMA Network Open.
It appears that the AMA is “leading the charge” on “medico-political” topics, such as “climate change”, DEI (Diversity, Equity, and Inclusion), “equity of access to care” for illegal immigrants, “gender equity”, and more.
This leads to the AMA EdHub discussion.
The AMA EdHub website features online courses and Continuing Education (CME) fulfillment modules for physician members (https://edhub.ama-assn.org). These courses and modules are presented in various ways: webinars; video and/or audio courses; papers to be read; and so on. One does not have to be a member of the AMA in order to access and read many of the courses and modules; in fact, the AMA states that, “The AMA EdHub is open to anyone.” (https://education.ama-assn.org/help/, the “FAQ’s” section); interested persons simply open an account. However, only licensed physicians who belong to the AMA can fulfill their CME credits using the AMA EdHub. https:///edhub.ama-assn.org/pages/ama-cme, section “Target Audience“; and, www.ama-assn.org/member-benefits/personal-member-benefits-discounts/ama-ed-hub-member-benefits.
On other hand, the AMA EdHub provides a good “snapshot” of the current modes of thought in “establishment medicine”, as well as current trends in treatment and in the teaching of medical school students, among other topics. For example, there are CME modules and online courses related to DEI; to “anti-racism in medicine”; “equitable patient care”; and other what may be termed “medico-political” topics areas. Here is a link to one such example, a CME module: https://edhub.ama-assn.org/clinical-problem-solvers-antiracism-podcast/audio-player/18843339, “Episode 23 – Anti-Blackness, Anti-Fatness, and Food Shaming”, 9 January 2024. This somewhat over one hour audio module (with a Transcript that can be read) can be used, after the physician takes the Quiz, to earn one CME credit. The Learning Objectives listed for this module are: “1. Explain how anti-fatness and food shaming culture in the US is rooted in anti-Blackness 2. Describe the intersection of policing and the court systems with anti-fatness and food shaming 3. Identify ways to navigate clinical interactions with patients while respecting them and affirming their experiences with food and fatness.”
The AMA Edhub also has a department devoted to “health equity” — https://edhub.ama-assn.org/ama-center-health-equity. From the main page of the link: “Education from AMA Center for Health Equity AMA’s online education to empower individuals ad organizations, in healthcare and beyond, in advancing racial justice and equity.”
It appears that one area of particular emphasis in the AMA Center for Health Equity has to do with “gun violence prevention” — through “education” of medical students, practicing physicians, and patients — and working with the United States Congress. Here is a link to a recent video CME fulfillment presentation from the AMA Center for Health Equity: https://edhub.ama-assn.org/ama-center-health-equity/video-player/18867531, “Prioritizing Equity: Embracing Public Safety and Health for Improved Firearms Violence Prevention“, 2 April 2024. This video presentation has a Transcript that can be read. It appears, from reading the Transcript, that the AMA’s position on “gun violence prevention” goes beyond working through the criminal justice system. According to Dr. Megan Ranney, MD, one of the speakers interviewed on the video, “…it’s about separating someone from the potential to access a firearm at that moment of desperation, anger, impulsivity, hopelessness.” Dr. Ranney also states that, “…the amount of violence that youth are exposed to in urban neighborhoods far outstrips the amount of violence that people are exposed to in the military.” (Italics added)
The AMA EdHub has other areas of interest that offer online CME courses for AMA physician members, among them: promoting “race-conscious” admissions to higher education, including to medical schools: and, courses from The Fenway Institute, an organization that advocates for LGBTQIA+ and Transgender issues and persons. Here are links to examples of these AMA EdHub areas of interest: https://edhub.ama-assn.org/ama-center-health-equity/audio-player/18868328, 2 April 2024; “The SCOTUS Affirmative Action Ruling The Cost to the Physician Workforce and Historically Minoritized Communities (with a Transcript that can be read); and, https://edhub.ama-assn.org/fenway-institute-edu/video-player/18638799, 2 September 2021, “Affirming Care for People with Intersex Traits.”
In Yours Truly’s opinion, understanding the AMA EdHub is an important part in understanding how the AMA works to influence healthcare treatment practices, healthcare policies; and the United States Congress, through the AMA’s lobbying efforts.