The above image is courtesy of a Substack post by Jessica Rose, PhD: https://jessicar.substack.com/p/the-immunological-mechanism-of-action, “The immunological mechanism of action for lost immunity, a shift to tolerance (and autoimmunity?) from the shots”, 27 December 2022.
Health Friday is a series of posts related to Big Pharma, vaccines, general health, and associated topics. Since today’s post is related to the COVID-19 virus itself, and to the COVID-19 “vaccines”, it is dedicated to the memory of Yours Truly’s COVID-19 “vaccinated” late brother, Sam, and to her late cousin, Bill; and to all people, of any age or location, who have passed away from the negative effects (direct or indirect) of the COVID-19 “vaccines” that they took. The discussion today is not limited to what is presented in the post: It is an Open Thread.
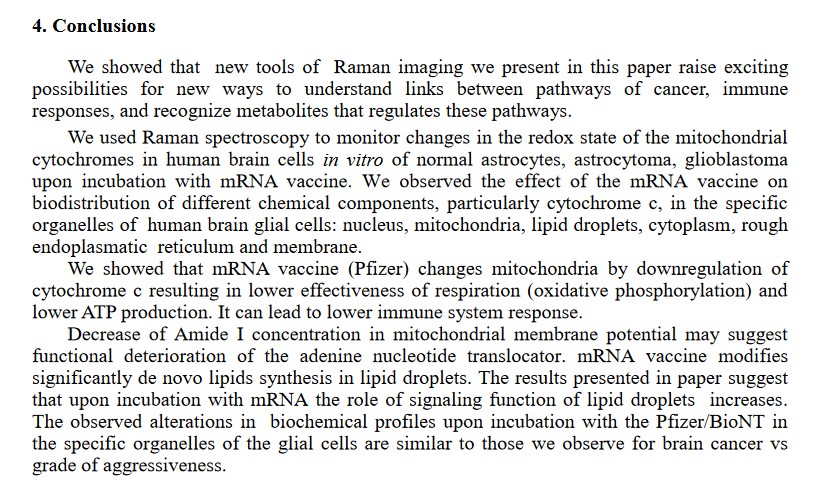
Today’s Health Friday post is about what the COVID-19 “vaccines” do to the “vaccinated” person’s natural immune system. It is also about what the COVID-19 virus itself does to a person’s natural immune system. The bottom lines are: One: the modRNA COVID-19 “vaccines” severely damage or even destroy the natural immune system of the person who takes these “vaccines”, with the damage or destruction increasing with each additional injection of them. Two: the COVID-19 virus itself can damage the natural immune system. Three: it is more possible to repair and support the immune system of a person who is non-COVID-19 “vaccinated.”
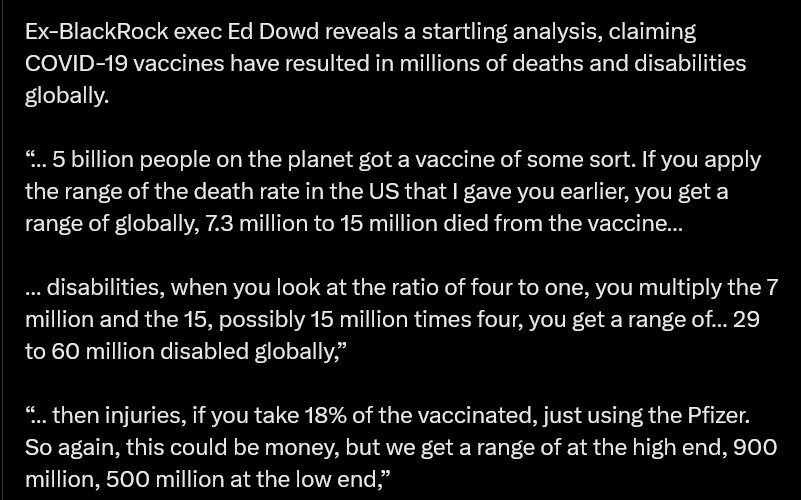
Yours Truly begins with these: first, https://x.com/tpvsean/status/1862616283738501504. Two screenshots of this tweet are below:

And, this: https://x.com/leejohnson/status/1862619457706770458. Two screenshots of this tweet are below:

Actually, Yours Truly respectfully disagrees with the title of the above book: in her opinion, it should read: Bill Gates I Want to Kill Three-Quarters of You, and Control the Survivors.
There. Must. Be. Justice.
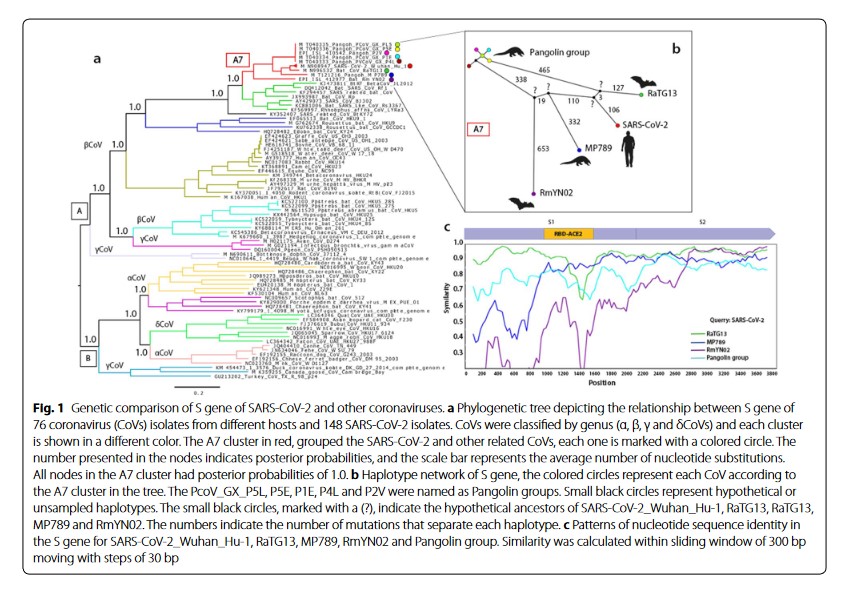
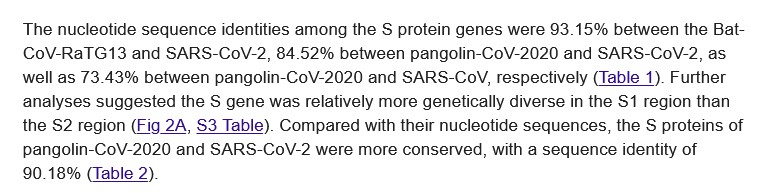
There are several aspects that make up today’s post. *** Yours Truly is firmly convinced that the SARS-CoV-2 virus itself was designed and lab-created, AND the modRNA COVID-19 “vaccines” were / are designed and lab-created, as bioweapons. These lab-created bioweapons attack the immune system of the human body; damage and/or destroy important components of the immune system of the human body; and, in the case of the modRNA “vaccines”, keep this damage and/or destruction going for an indefinite period of time in the “vaccinated” person’s body. Also — Yours Truly will present evidence that — wait for it — the pangolin-CoV MP789 virus genome is an integral part of the situation.
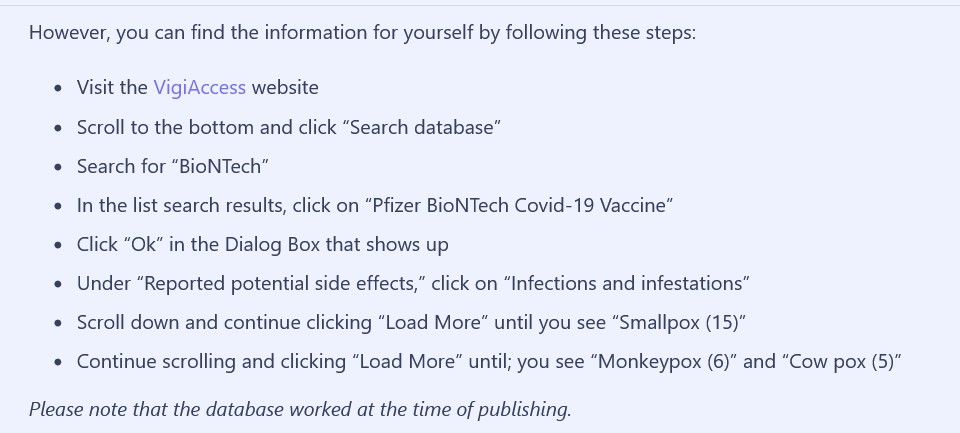
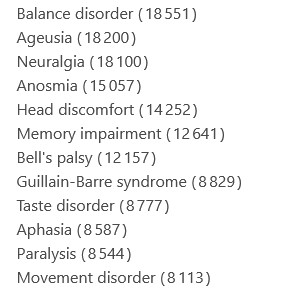
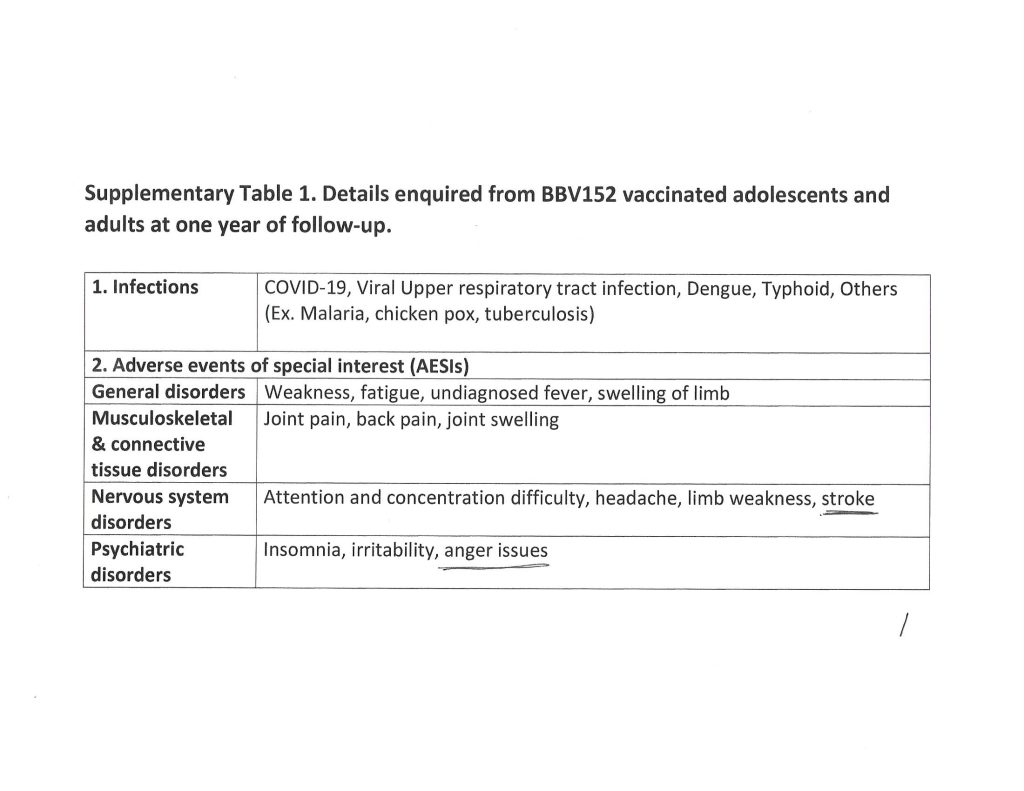
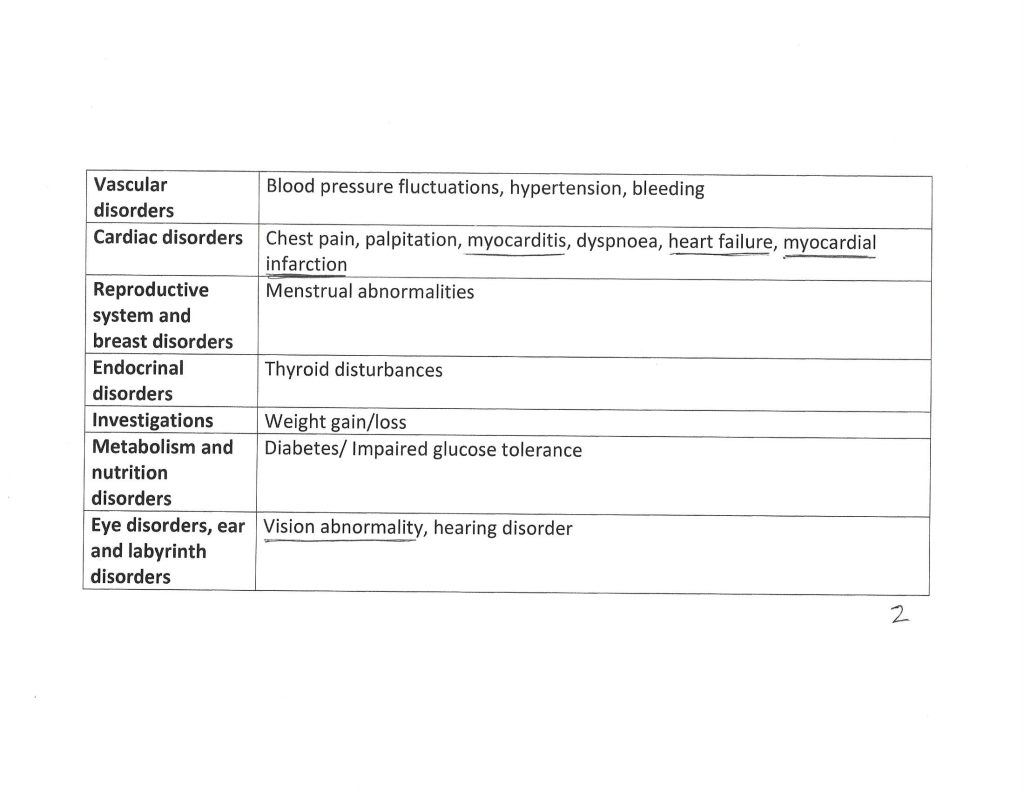
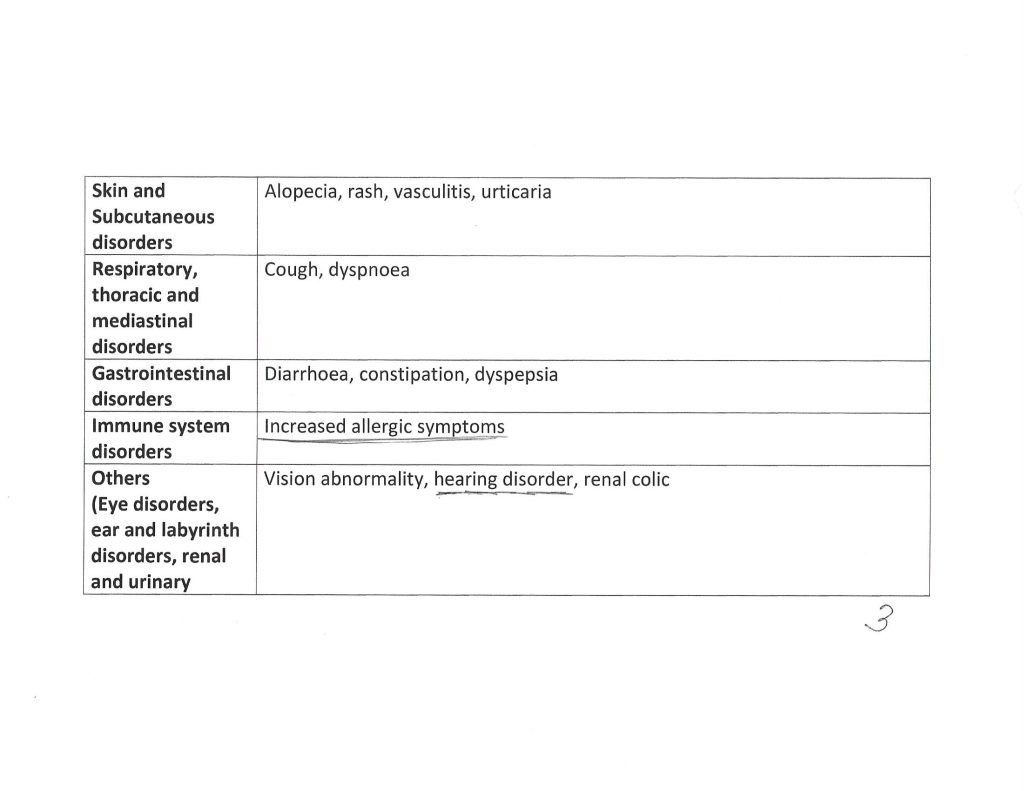
To begin: The 5.3.6 Postmarketing Experience document that Pfizer-BioNTech submitted to the FDA on 30 April 2021: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, 5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162b2) Received Through 28-Feb-2021. Below are two screenshots from the Appendix 1: List of Adverse Events of Special Interest section of this document:
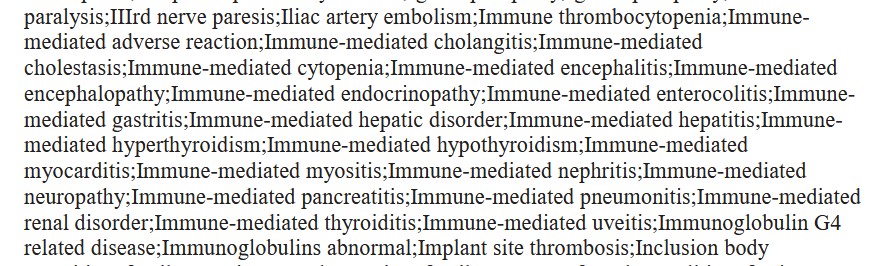
The above are autoimmune and immune-mediated medical conditions that were reported in the first two months after the rollout of the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2 among persons who took this “vaccine” during that period. Notes: BNT162b2 is the basis of all subsequent formulations of the COVID-19 “vaccine” injectables by this company (since 2022, marketed under the brand name COMIRNATY); and, there are other listings of autoimmune and immune-mediated conditions in the Appendix 1. of the above report.
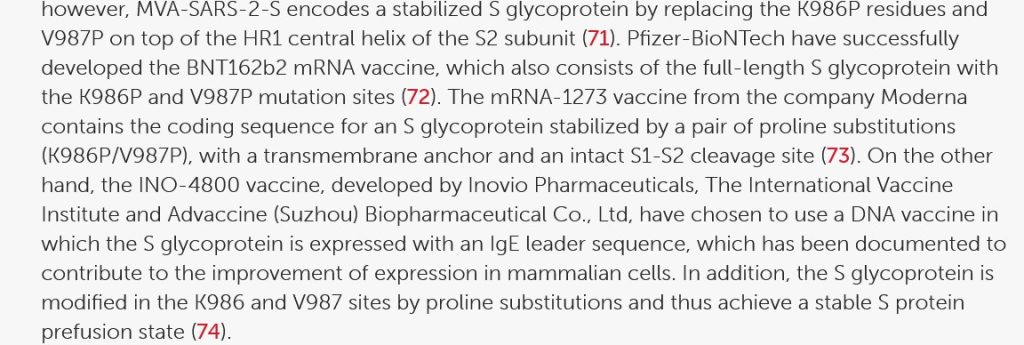
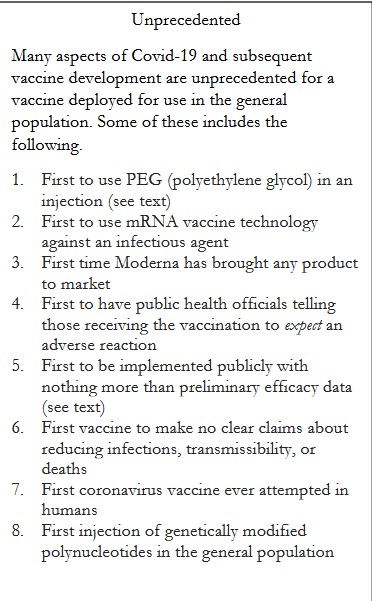
Yours Truly now turns to a 2021 paper by Stephanie Seneff, PhD: https://doi.org/10.56098/ijvtpr.v2i1.23, “Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19”, 10 May 2021. Dr. Seneff points out that only the spike protein was used for the modRNA in the Pfizer-BioNTech and in the Moderna COVID-19 “vaccines” (BNT162b2 and mRNA-1273, respectively.) A screenshot from this paper is below, listing the “firsts” regarding the modRNA COVID-19 “vaccines”:
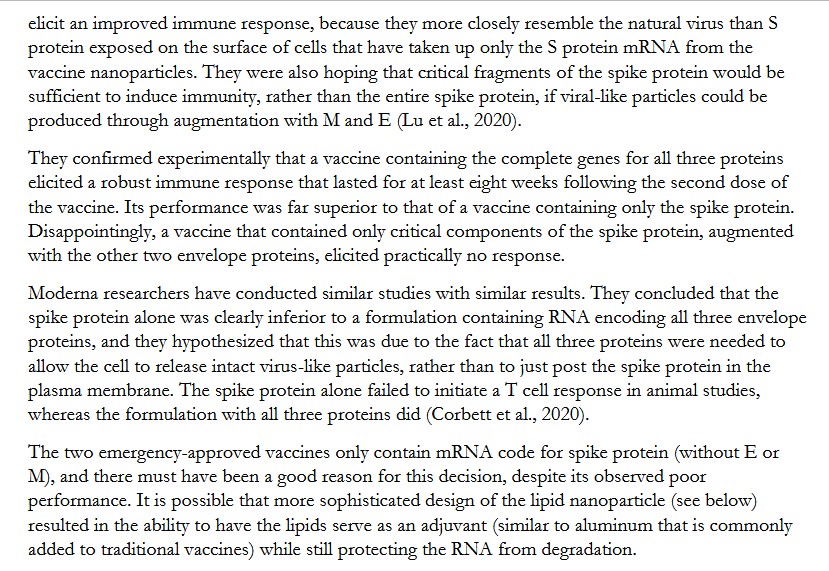
Dr. Seneff references a 2020 paper by Lu, et al., regarding an important discovery about the SARS-CoV-2 virus itself: https://pmc.ncbi.nlm.nih.gov/articles/PMC7429369/, “A COVID-19 mRNA Vaccine Encoding SARS-CoV-2 Like Particles Induces a Strong Antiviral-like Response in Mice.” The authors make it clear that there are three separate-but-important components in the SARS-CoV-2 virus itself: the membrane (M); the envelope (E); and, the spike protein (S). Another screenshot from the Seneff paper is below, regarding this issue:
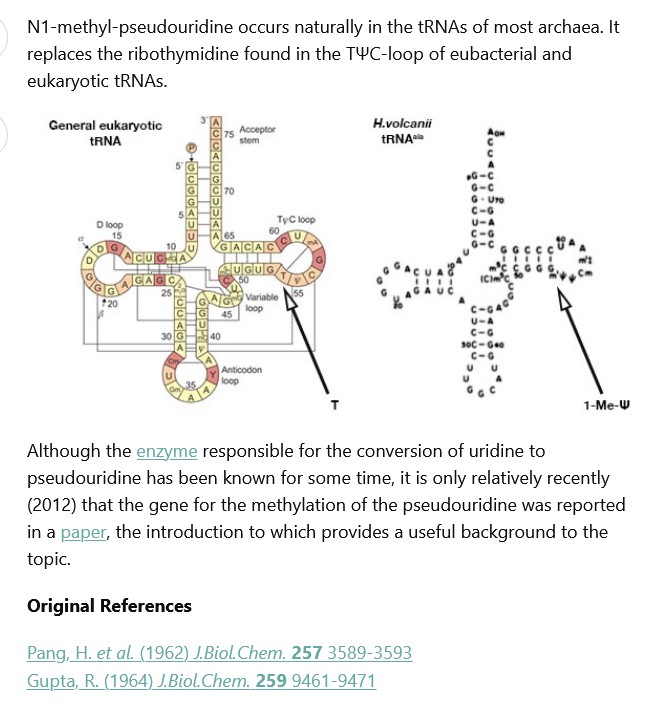
Why is it important to know that Pfizer-BioNTech and Moderna chose only the spike protein of the SARS-CoV-2 virus itself as the basis for their respective modRNA COVID-19 “vaccines”? Yours Truly hypothesizes that, in so doing, it was then possible for them to create a modRNA that would have the most potential to damage the persons taking these respective modRNA COVID-19 “vaccines.” The Lu, et al., 2020 paper, cited above, also describes how the authors created various “prototype” COVID-19 “vaccines.” These “prototype vaccines” were lab-produced using various ingredients — one of which was — wait for it — N1-Methylpseudouridine; as well as one “prototype vaccine” that used Uridine. The authors concluded that N1-Methylpseudouridine was “superior” in creating “neutralizing antibodies.” Please refer to Figure 1. and its description underneath from this paper, where N1-Methylpseudouridine is used in the “Lane 5 proto-type vaccine” of the experiments. In Yours Truly’ opinion, it is within the realm of possibility that Pfizer-BioNTech, or Moderna, or both, knew of the Lu, et al., research.
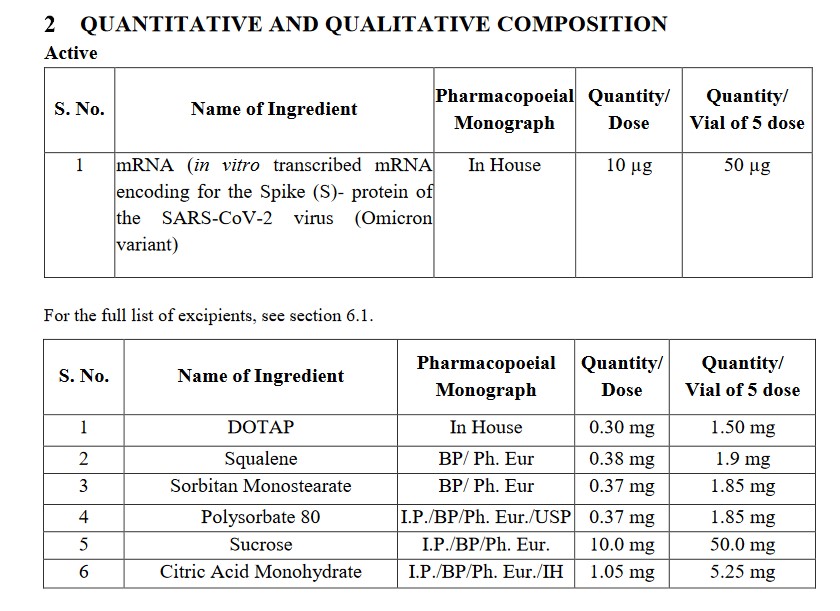
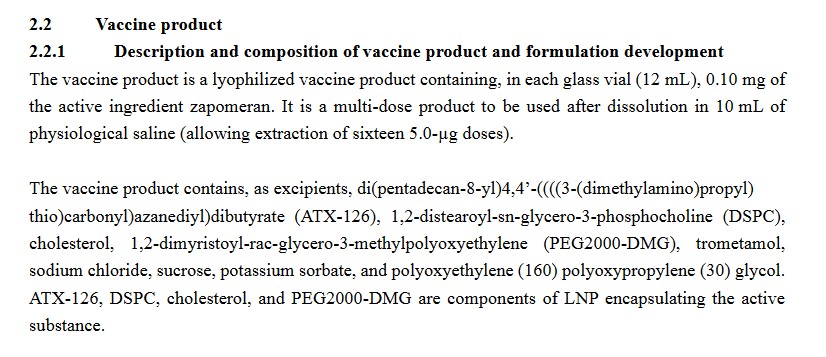
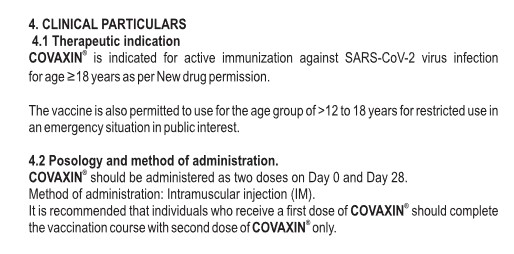
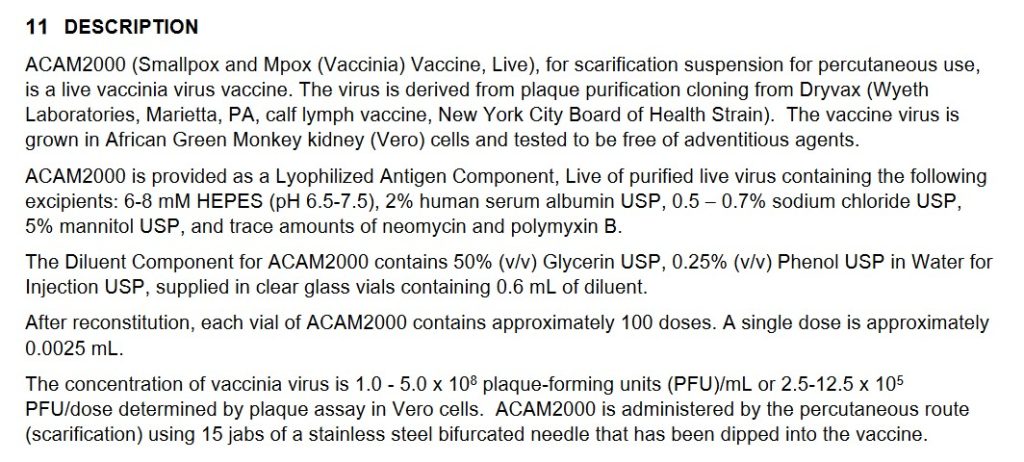
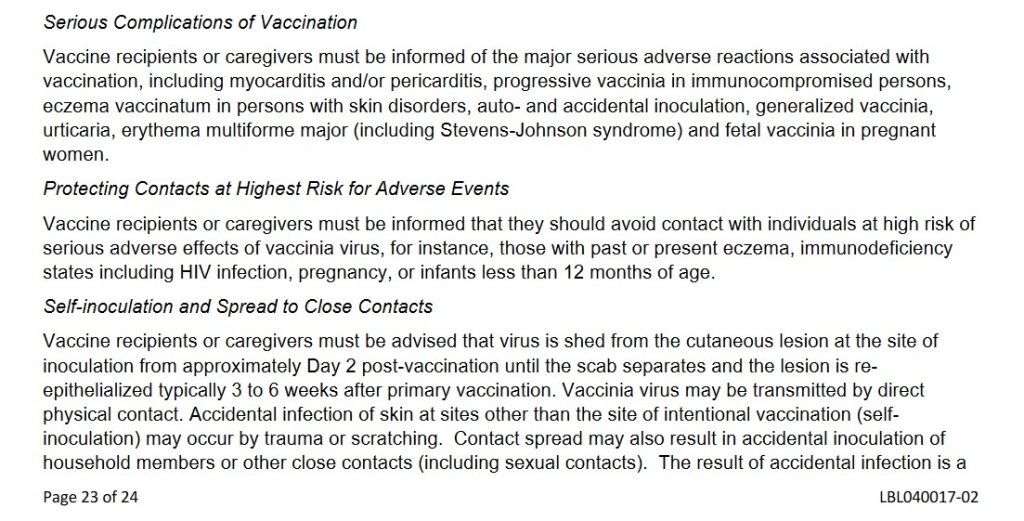
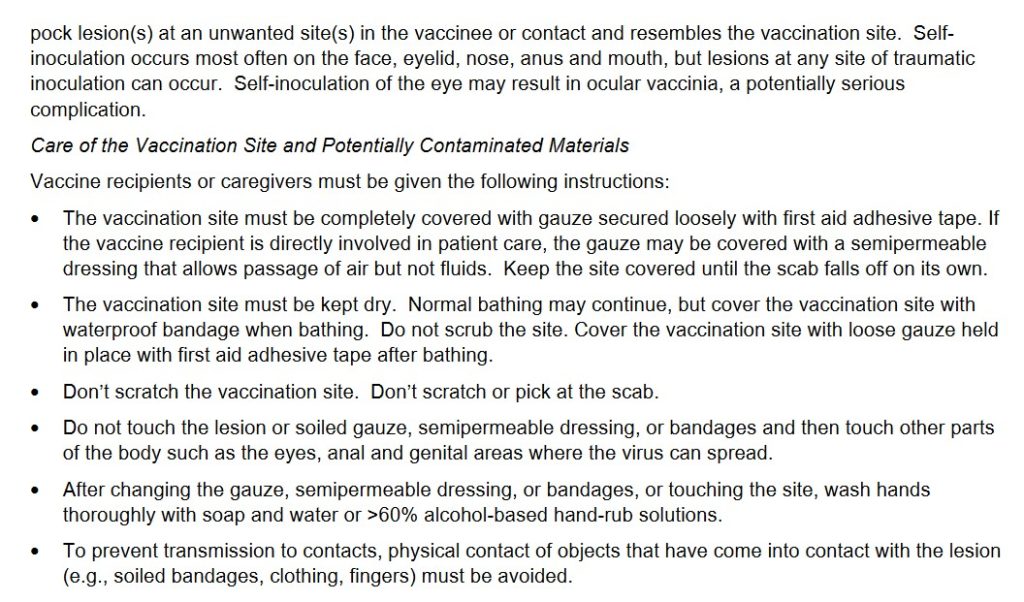
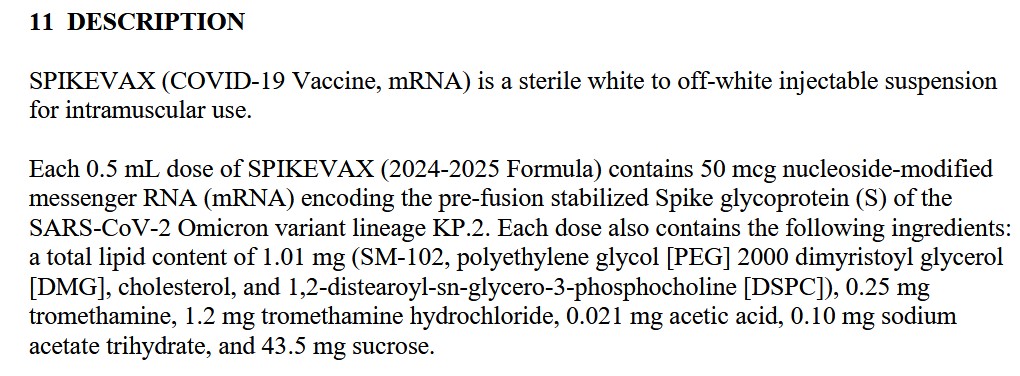
Below are screenshots of section 11 Description of the Pfizer-BioNTech (COMIRNATY) “2024-2025 Formula COVID-19 vaccine”; and, of section 11 Description of the Moderna (SPIKEVAX) “2024-2025 Formula COVID-19 vaccine.” There is no mention in either one of the membrane or of the envelope of the original Wuhan Hu1 SARS-CoV-2 virus; there is only the mention of the spike protein:

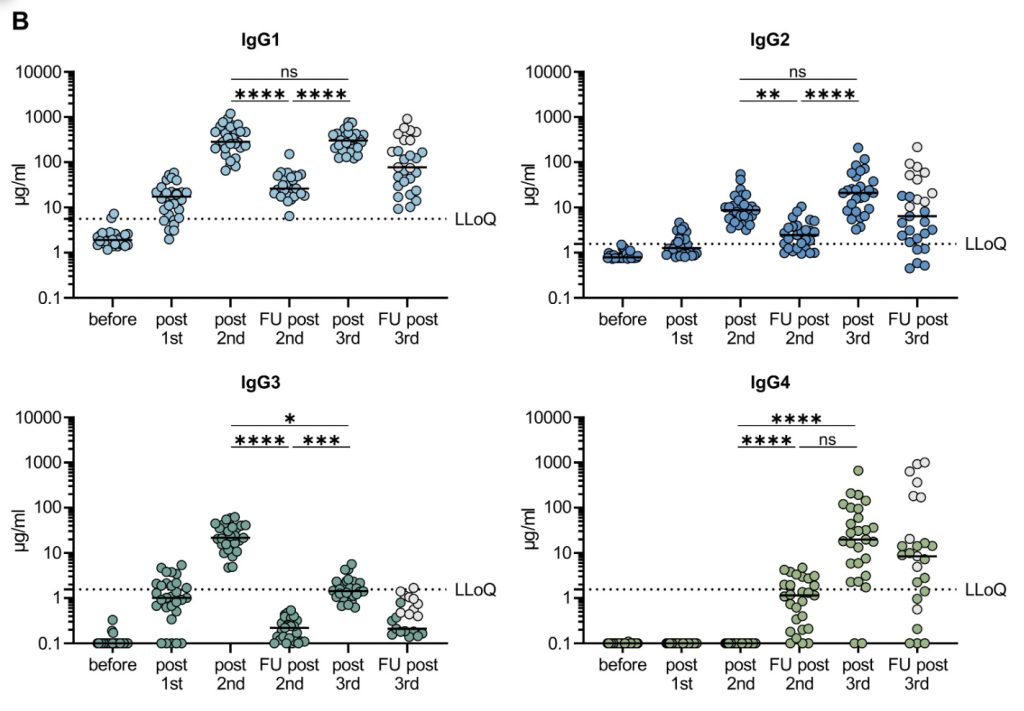
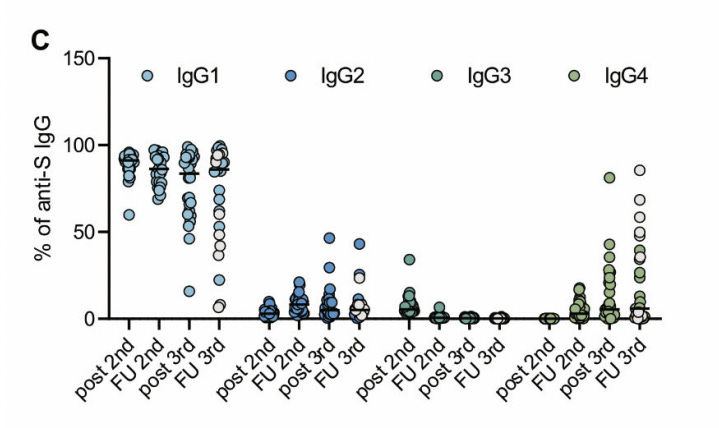
The modRNA COVID-19 “vaccines” damage and/or destroy crucial IgG3 immune system cells in the “vaccinated” person’s body (the “fight it off” element), and instead foster the increase of IgG4 immune system cells (the “tolerate but never clear” element). Please refer to the Jessica Rose, PhD, post at the top of today’s post. Below is another figure from her post, from the Supplementary Materials of this 2022 paper (cited in the post): www.science.org/doi/10.1126/sciimmunol.ade2798, “Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination”, Pascal Irrgang, et al., 22 December 2022. This image, from Figure 2: Figure S1 of the paper, clearly shows the decimation of IgG3 (“fight it off”) immune system cells, and the increase of IgG4 (“tolerate it”) immune system cells, after repeated modRNA COVID-19 “vaccinations”:
And, also from the Irrgang, et al., paper:
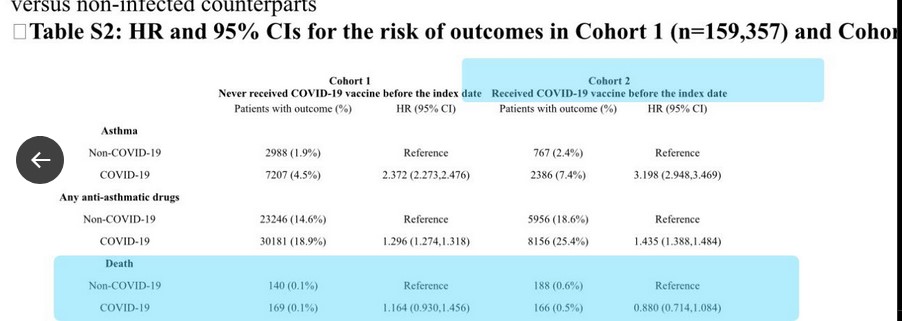
Those who are COVID-19 “vaccinated”, especially if they take repeated injections of these “vaccines”, are the slowest to “clear” a COVID-19 infection: https://pmc.ncbi.nlm.nih.gov/articles/PMC9258747/, “Duration of Shedding of Culturable Virus in SARS-CoV-2 Omicron (BA.1) Infection”, Julie Boucau, Ph.D., et al., published in the New England Journal of Medicine, 21 July 2022. The salient figure from this Letter to the Editor is below:
Please refer to the second and third column percentages. These “tell the tale.”
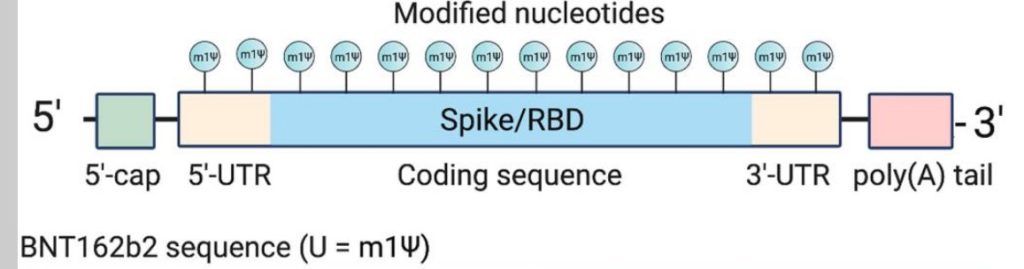
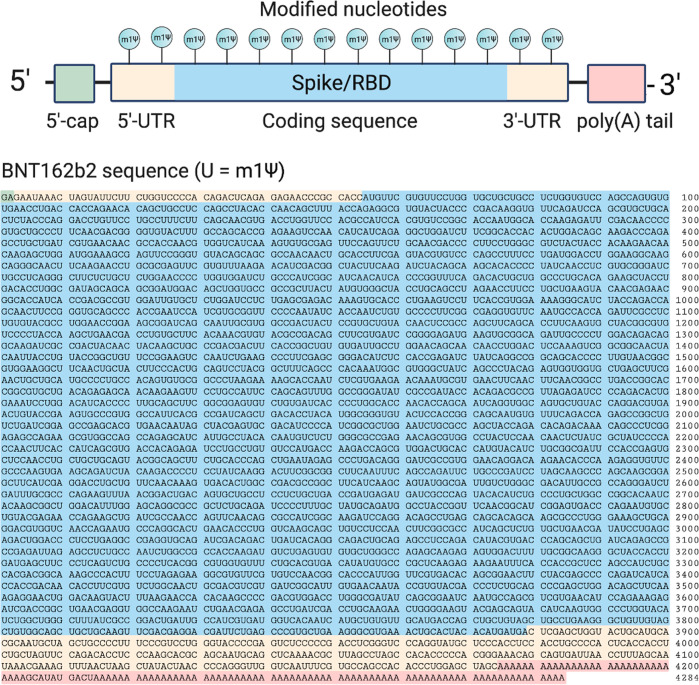
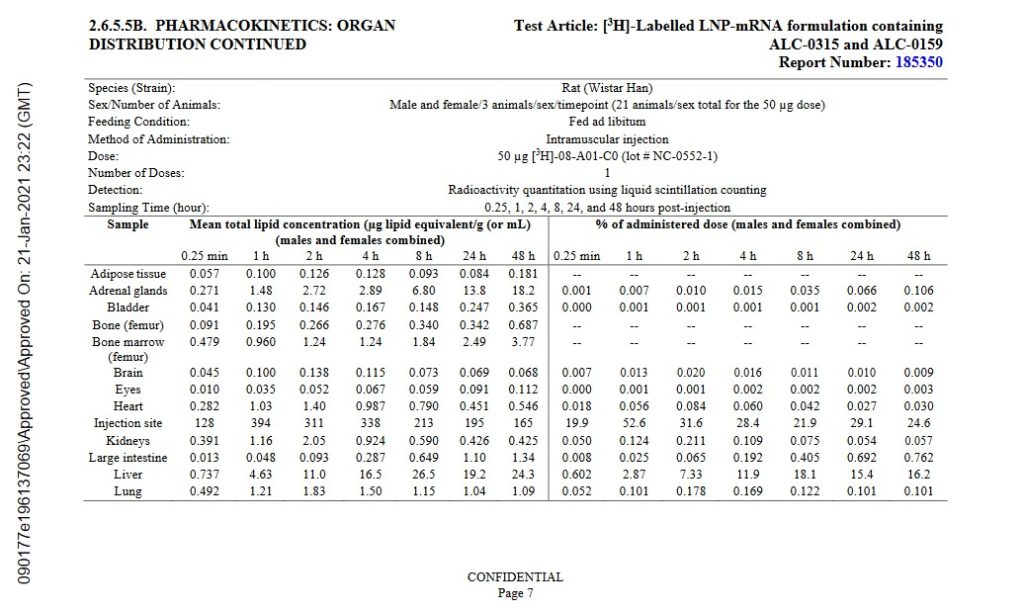
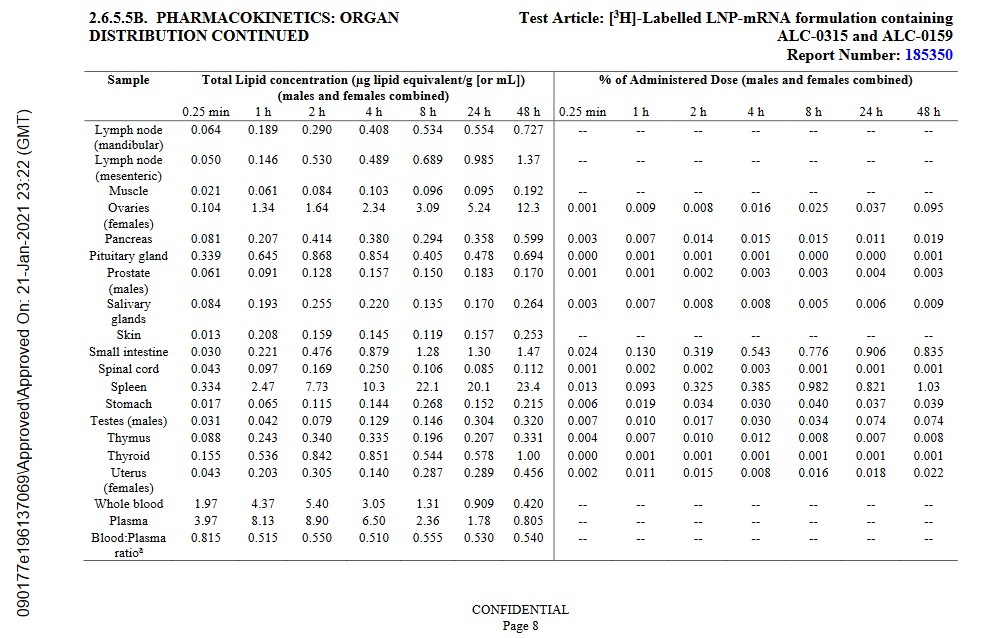
Yours Truly has written extensively regarding the modRNA COVID-19 “vaccines”, some of their ingredients, and what damage these injectables do to the body and brain of the “vaccinated” person. Please refer to: www.theqtree.com/2024/11/08/health-friday-11-8-2024-open-thread-the-insidious-n1-methylpseudouridine-in-the-modrna-covid-19-vaccines/; www.theqtree.com/2024/11/01/health-friday-open-thread-11-1-2024-the-covid-19-information-file-part-one/; and, www.theqtree.com/2024/10/18/health-friday-10-18-2024-special-edition-neurological-effects-of-the-covid-19-vaccines-physical-and-psychological/, for examples. These “vaccines” contain, among other ingredients, the following that assist in the mechanisms of said injectables: the lab-created lipid nanoparticles ALC-0159, ALC-0315, SM-102, and PEG2000-DMG, which spread the “vaccines” to every cell of the “vaccinated” person’s body; and, N1-Methylpseudouridine (present in both the Pfizer-BioNTech and in the Moderna modRNA COVID-19 “vaccines”), which replaces the natural Uridine of the “vaccinated” person’s body with a lab-created combination of “fake Uridine” plus a form of methane. Recall that natural Uridine is an incredibly important RNA which assists or manages many bodily functions — including brain functions and emotions.
This leads to the next part of today’s post: the SARS-CoV-2 virus itself, which is the foundation of the modRNA COVID-19 “vaccines.”
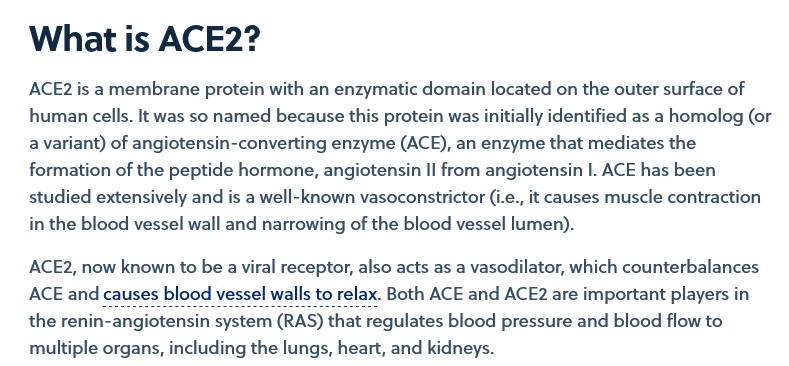
The lab-created SARS-CoV-2 (COVID-19) virus itself attacks the body (and brain) of a person infected with this virus in several ways. One way is that the virus “attaches” itself to the ACE2 receptor cells of the body. ACE2 stands for “angiotensin-converting enzyme 2” cells. What these cells do is discussed here: www.cas.org/recources/cas-insights/ace2-covid-19-target, by Angela Zhou, 15 December 2022. A screenshot of this article is below:
The spike protein of the SARS-CoV-2 virus itself dysregulates (“downregulates”) the functions of the ACE2 receptor cells in the body of the infected person: https://doi.org/10.1101/2020.12.04.409144, “SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE2”, Yuyang Lei, et al., 4 December 2020. “Endothelial function” is the range of functions of the vascular endothelium. Endothelial cells release elements that control the opening and closing of the arteries.
Also, the COVID-19 virus itself “mimics” the proteolytic activation of human ENaC cells: https://doi.org/10.7554/eLife.58603. “SARS-CoV-2 strategically mimics proteolytic activation of human ENaC”, Praveen Anand, et al., 26 May 2020. ENaC stands for “Epithelial sodium channel” (an ion channel); this element has an important role in kidney function, the immune system, and vasculature. “Proteolysis” has to do with protein breakdown in the body.
The SARS-CoV-2 virus itself attacks, damages, and/or destroys, the CD4 cells of the human body. Please refer to: https://doi.org/10.1101/2020.09.25.20200329, “SARS-CoV-2 uses CD4 to infect T helper lymphocytes”, Natalia S Brunetti, et al.; paper published in 2020, version of record 31 July 2023. A screenshot of the Abstract from this paper is below:
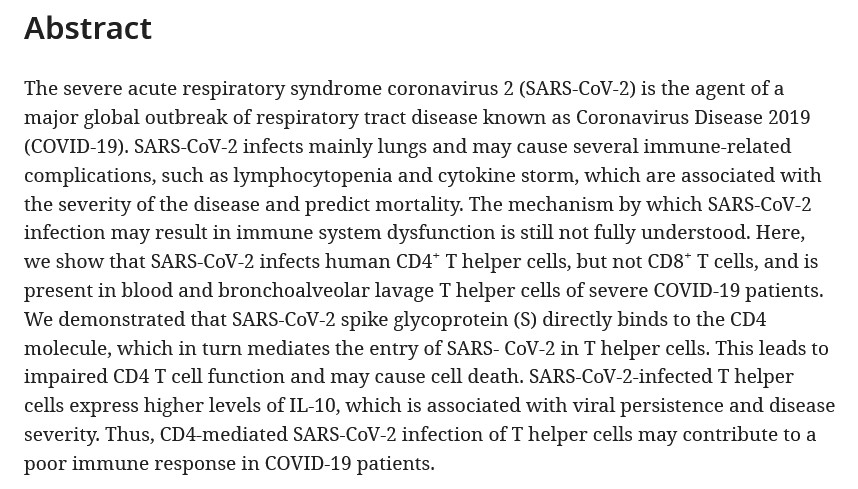
Note that damaged CD4 cells are a component in HIV infection; also, note again that, since the original SARS-CoV-2 virus itself is the foundation for the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna, the “attack and damage” elements and mechanisms described above are present in said “vaccines.”
For further information regarding how the spike protein of the SARS-CoV-2 virus itself works in the human body, please refer to the ongoing research of Walter M Chesnut: https://wmcresearch.substack.com/.
And now, another visit with our shy, nocturnal scaly anteater, the Pangolin:

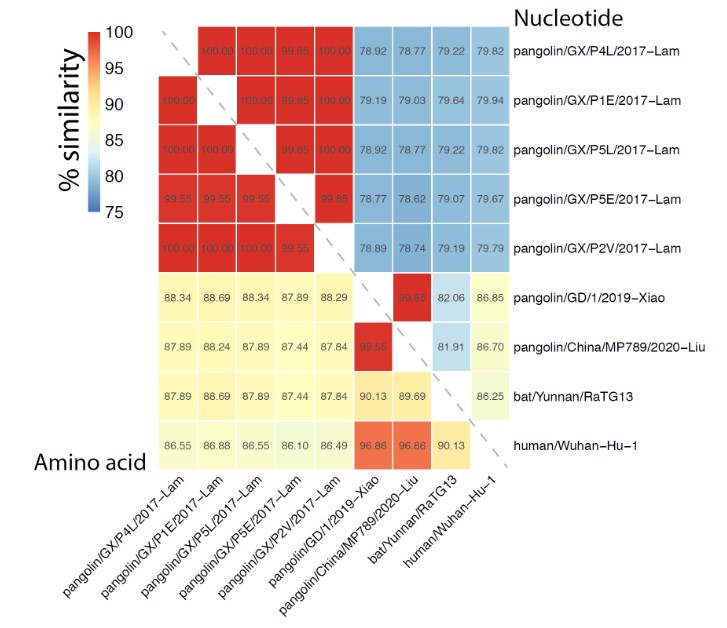
Yours Truly has written about this mammal, and of how the PRRARSV (or RRAR or RRARSV, depending on which scientific paper one reads) genome code in the original SARS-CoV-2 virus itself was lab-manipulated from the pangolin-CoV MP789 to include this code; for example: www.theqtree.com/2024/11/22/health-friday-11-22-2024-open-thread-lets-talk-about-prrarsv-the-backdoor-key/. It appears that the pangolin-CoV MP789 genome code was “mixed in” with the bat-CoV RaTG13 genome code in the lab experiments that created SARS-CoV-2. However, Yours Truly has discovered something else about pangolin-CoV MP789: It “binds” better to human ACE2 receptor cells, compared to the bat-CoV RaTG13!
The story behind this discovery begins here: www.crick.ac.uk/news/2021-02-05_pangolin-coronavirus-could-jump-to-humans. This article led to the following link: www.nature.com/articles/s41467-021-21006-9, “Structure and binding properties of Pangolin-CoV spike glycoprotein inform the evolution of SARS-CoV-2”, Antoni G. Wrobel, et al., 5 February 2021. A screenshot from the Discussion section of this paper is below:
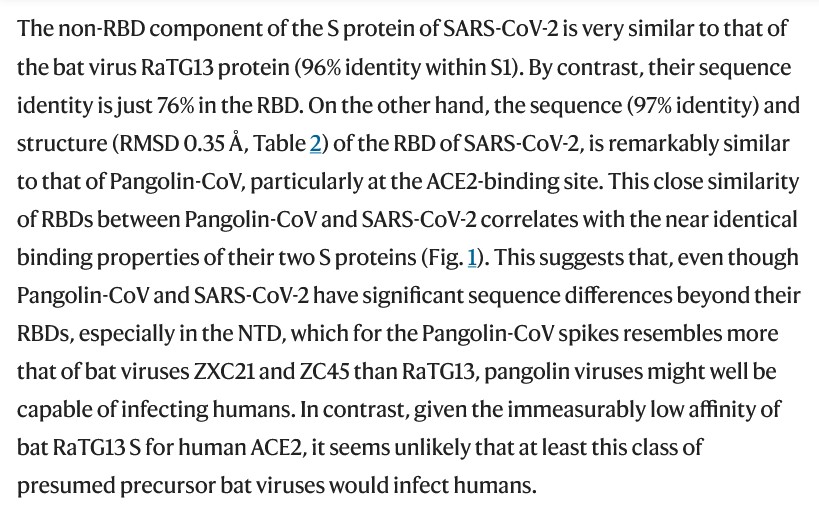
It would appear, then, that the pangolin-CoV MP789 genome has much more to do with the lab-creation of the SARS-CoV-2 virus itself (and, by extension, the modRNA COVID-19 “vaccines”) than at first meets the eye. This is not to discount the use of genome code elements from the bat-CoV RaTG13 in the lab-creation process of the virus itself; nor to discount the other coronavirus code elements that were “mixed in” from monkey, civet, and other animal coronaviruses. In Yours Truly’s opinion, those who lab-created the SARS-CoV-2 virus itself were searching for a genome code that could most effectively attack and compromise human ACE2 receptor cells and the mechanisms of these cells. They found what they were looking for in the pangolin-CoV MP789 genome code. However, it is crucial to understand that those who lab-created the SARS-CoV-2 virus itself did not also add N1-Methylpseudouridine to it — this compound was added to the modRNA COVID-19 “vaccines.” And therein, again in Yours Truly’s opinion, lies an important difference between the SARS-CoV-2 (COVID-19) virus itself, and the presence of this virus in the modRNA-COVID-19 “vaccines.” It is the difference between a non-COVID-19 ” vaccinated” person being infected with the SARS-CoV-2 virus itself and recovering (even if there are complications), because the natural Uridine in the non-COVID-19″vaccinated” person’s body is still operative to help regulate many body functions and mechanisms that can assist in recovery; whereas, in the COVID-19 “vaccinated” person’s body, the natural Uridine has been replaced with N1-Methylpseudouridine (thereby literally erasing the potential for natural Uridine to work.)
Is it, then, a foregone conclusion that the natural immune system of the COVID-19 “vaccinated” person is so severely damaged, or even destroyed, especially with that person taking more and more injections of these “vaccines”, that there is no hope for any possible repair or restoration of it? In the case of the RNA of Uridine being replaced by N1-Methylpseudouridine, some things can be done to supplement the body: consuming Uridine-containing foods, such as beets, goat cheese, walnuts, and broccoli. There is some promising research on the use of a compound, called 5-FU, to help repair Uridine RNA: https://doi.org/10.3389/frnar.2023.1248236, “RNA damage: the forgotten target of clinical compounds”, by Nicole Simms and John R.P. Knight. In the case of damaged CD4 cells, there are natural methods to increase the body’s healthy CD4 cell count. Please refer to: www.medicalnewstoday.com/articles/how-to-boost-cd4-count-naturally, by Charlotte Lillis, 16 July 2024. Supplementation with Vitamin D, multivitamins, and probiotics are mentioned in this article.
Finally, Yours Truly firmly believes that the SARS-CoV-2 virus itself is not “just another virus” or “just another flu virus.” Au contraire: this virus itself was lab-created from a “palette” of animal coronaviruses (the pangolin-CoV MP789 in particular, with the bat-CoV RaTG13 close behind) to be as damaging as possible, even deadly, to the human body — in other words, a bioweapon. Yes, a non-COVID-19 “vaccinated” person may become infected with the SARS-CoV-2 virus itself, and recover well; however, there may be “residual damage” from the virus itself remaining for some period of time in their body. There is also the phenomenon of “COVID-19 vaccine shedding” from COVID-19 “vaccinated” persons onto others, including onto non-COVID-19 “vaccinated” persons, to consider: as these “vaccines” contain elements in them that make this virus, as well as the “vaccines” themselves, more dangerous and/or deadly. Does this mean that non-COVID-19 “vaccinated” persons should avoid contact with other persons, especially COVID-19 “vaccinated” persons? No — what it does mean, however, is that it is imperative to have, and maintain, the highest possible degree of health of the body’s natural immune system.
There. Must. Be. Justice.
Peace, Good Energy, Respect: PAVACA