The header image for today’s offering is courtesy of The Productive Woman and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering speaks of the COVID-19 disaster, Yours Truly dedicates it to all persons, of whatever age or location, who have suffered further illness, or injuries, or disabilities, from an infection of the COVID-19 virus itself, or from the COVID-19 “vaccines” they have in their bodies; or, who have passed away from complications related to an infection of the COVID-19 virus itself, or from issues induced from the COVID-19 “vaccines” they have in their bodies.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for AI-generated content. There may be AI-generated content (images, text, etc.) in certain linked URLs in today’s offering. If readers wish to add AI-generated content to today’s discussion thread, they must identify it as such. Thank you.
>>>>>>>>>>>>>>>>>>>>
Today’s offering is the Year-End Wrap-Up Edition. It has been a year of implementation of some of the Make America Healthy Again agenda of President Donald Trump 47 and of HHS Secretary Robert F. Kennedy, Jr.
It has also, sadly, been a year of health issues and of losses among the denizens of The Q Tree. Susan Sampson (DePat / Deplorable Patriot) and Georgia Swink Smith (GL/FL) have departed this world and are badly missed. There are those at The Q Tree who have lost family members, dear friends, and other loved ones, who are badly missed. May all of the deceased rest in eternal Peace under the Wings of the Almighty God. There are also those at The Q Tree who are still dealing with health issues. SteveInCO decided to leave the blog; our good Kalbokalbs has taken over the Saturday article spot. If Yours Truly has left anyone out, apologies: it is not intentional. The Q Tree soldiers on.
Links to The COVID-19 Information Files: Part One: https://www.theqtree.com/2024/11/01/health-friday-open-thread-11-1-2024-the-covid-19-vaccines-information-file-part-one/; Part Two: https://www.theqtree.com/2025/03/07/health-friday-3-7-2925-open-thread-the-covid-19-informaiton-file-part-two-the-virus-itself-and-the-vaccines/; Part Three: https://www.theqtree.com/health-friday-11-21-2025-open-thread-the-covid-19-information-file-part-three-compendium/.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
It appears that HHS Secretary Robert F. Kennedy, Jr., is taking steps to rein in the decades-long “strangle-hold” that Big Pharma has on that department. Two examples: One: cutting $500 million in development grants under BARDA for further research and development of mRNA-based “vaccines.” Please see: https://www.hhs.gov/press-room/hhs-winds-down-mrna-development-under-barda.html, 5 August 2025. BARDA is the Biomedical Advanced Research and Development Authority, a division of ASPR (Administration for Strategic Preparedness and Response, itself a division of the United States Public Health Service.) BARDA, ASPR, and the United States Public Health Service are all under the purview of the Department of Health and Human Services. And, Two: terminating millions of dollars in grants to the American Academy of Pediatrics, after that organization sued HHS over changes that HHS Sec. Kennedy and others made to the “recommended vaccination schedules” of the CDC. Please see: https://www.nbcnews.com/health/health-news/hhs-cuts-millions-grants-american-academy-pediatrics-rcna249769, “HHS cuts millions in grants to the American Academy of Pediatrics,” 17 December 2025.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
Some recent COVID-19 news:
First, a new paper by Dr. Peter A. McCullough, et al., proving that the modRNA COVID-19 “vaccines” do indeed induce cancer and other types of serious adverse medical conditions among the “vaccinated” [1], [2]. Please see the screenshot of the Abstract of this paper, below:

The above paper takes the place of the earlier one by McCullough, et al., on the same subject; an earlier paper which was published, then had thousands of views online, before it was abruptly Removed by the publisher. This earlier paper has vanished; only the Removal notice is available to see.
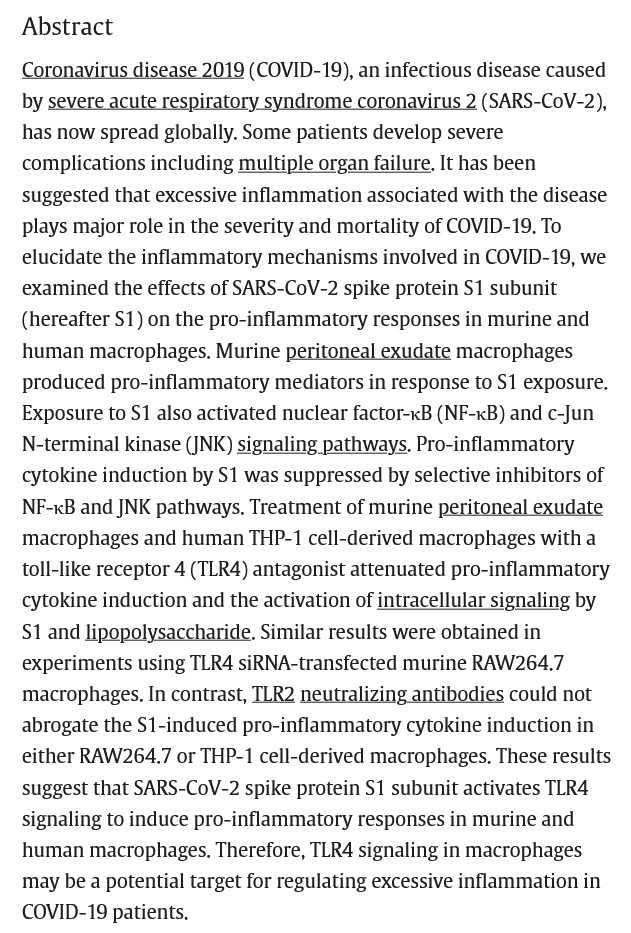
Second, a recently-published paper by Dasa He., et al., which demonstrates that chemotherapy can “awaken” dormant cancer cells [3]. Please see the Abstract and the Graphical Summary from this paper, below. Note: the entire article is available only via institutional access; or, via subscription access; or, via article purchase.


Third, this, from https://www.2ndsmartestguyintheworld.com/p/80-lawsuits-against-hospitals-to, “80 Lawsuits Against Hospitals To Administer IVERMECTIN To Sick COVID Patients”, 24 December 2025. Please see the screenshot from the article, below:
There is an embedded video interview with Dr. Bret Weinstein, PhD, on this situation. The information regarding the lawsuits is taken from the book by Dr. Pierre Kory, MD, The War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the Pandemic (available on https://www.amazon.com/.)
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
The “freight train-like approach” of the next “Plandemic”, this one of Avian Influenza (and, likely, an Avian Influenza that will be “cobbled together” from elements of multiple strains of this virus AND lab-tested to make sure that the strain that is created is deadly to birds, animals, and humans alike), is steadily gathering steam. Two of the most recent developments in this situation are below:
First: https://jonfleetwood.substack.com/p/bill-gates-cepi-revives-moderna-mrna, “Bill Gates’ CEPI Revives Moderna mRNA Bird Flu Vaccine Development With $54M Investment After HHS Terminated Funding”, 19 December 2025. HHS Secretary Kennedy, Jr., had terminated grants totaling over $700 Million dollars to Moderna in May of 2025 related to research and development of mRNA-1018, the company’s modRNA-based Avian Influenza “vaccine.”
Second: https://jonfleetwood.substack.com/p/usdas-bird-flu-test-matches-bird, “USDA’s Bird Flu Test Matches Bird and Cow DNA, Not Just Viral DNA: BLAST Data”, 20 December 2025. Mr. Fleetwood put the the USDA’s current Avian Influenza PCR test through the BLAST software (Basic Local Alignment Search Tool, provided by the United States government), and discovered that the test results data reveal exact matches for multiple DNA genome codes in both birds and cows. In other words, the USDA’s current Avian Influenza PCR test is not only NOT accurate — it can result in multiple “false positives” for Avian Influenza infection. Please see the screenshot from the article, below:

Yours Truly firmly believes that the groundwork for a “worldwide Avian Influenza pandemic” is in the final stage of development. This is something to “be on the lookout” about.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
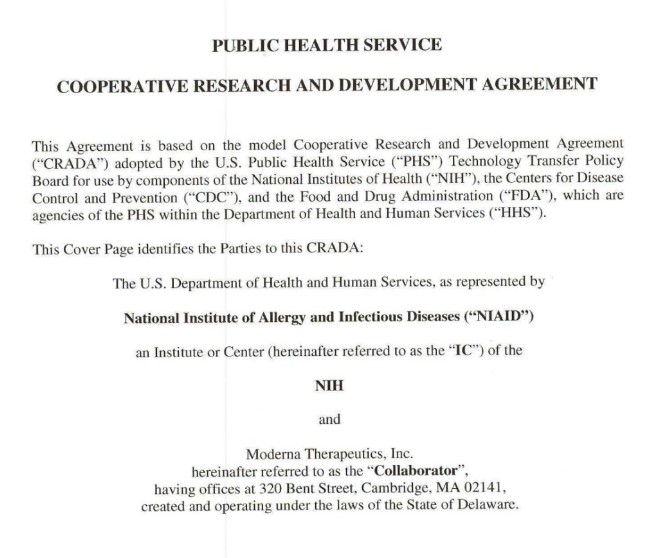
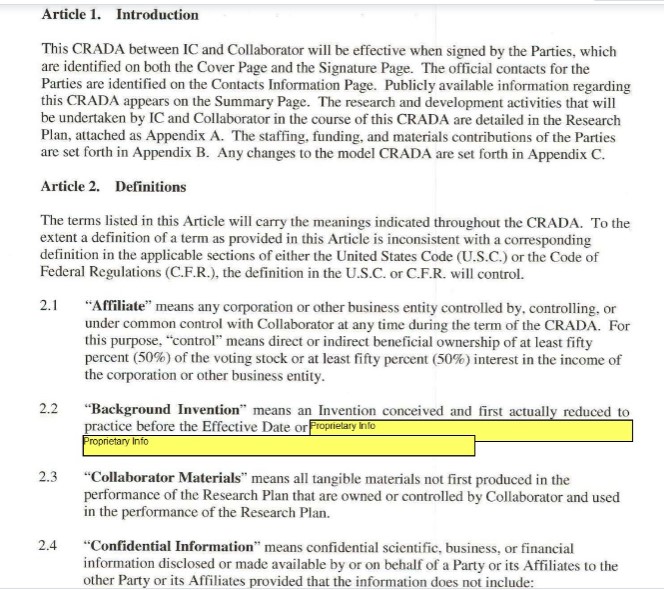
Finally, Katherine Watt closed her Bailiwick News Substack this month. Ms. Watt did enormous and detailed research into the legal documents between the United States Army, the Department of Health and Human Services, and Pfizer-BioNTech and Moderna, related to the development of the COVID-19 virus itself, and the development of the modRNA COVID-19 “vaccines.” A selection of her research has been archived here: https://bailiwicknewsarchives.wordpress.com/. Yours Truly wishes her well.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
THE COVID-19 “VACCINES” — ALL OF THEM — MUST BE REMOVED FROM THE MARKET AND FROM USE IN THE UNITED STATES. NOW. PERIOD.
ALL GAIN-OF-FUNCTION RESEARCH, NO MATTER ON WHAT DRUG OR “VACCINE”, MUST STOP. NOW. PERIOD.
THERE. MUST. BE. ACCOUNTABILITY.
THERE. MUST. BE. JUSTICE.
THERE. MUST. BE. TRUTH.
Peace, Good Energy, Respect: PAVACA
(Intellectual Property Notice and Disclaimer: With the exception of published papers and websites listed in today’s post, the ideas and conclusions in this post are by PAVACA. Proper credit must be given to PAVACA if ideas and conclusions from today’s post are used by other blog writers, by podcasters, on social media, or in print media.)
References:
[1]: “Synthetic messenger RNA vaccines and transcriptomic dysregulation: Evidence from new-onset adverse events and cancers post-vaccination.” Von Ranke NL, Zhang W, Anokhin P, Hulscher N, McKernan K, McCullough P, Catanzano J. World J Exp Med 2025; 15(4):11386. https://doi.org/10.5493/wjem.v15.i4.113869. 20 December 2025.
[2]: “BREAKING: Our CENSORED Study Showing mRNA Injections Induce Severe Genetic Disruption Linked to Cancer and Chronic Disease Is Now Peer-Reviewed and Published.” https://www.thefocalpoints.com/p/breaking-our-censored-study-showing. 19 December 2025.
[3]: “Chemotherapy awakens dormant cancer cells in lung by inducing neutrophil extracurricular traps.” Dasa He, et al. https://doi.org/10.1016/j.cell.2025.06.007. Cancer cell. 2025 Sep8; 43(9):1622-1636.e7. Epublished 3 July 2025.