The featured vintage image of a laboratory for today’s offering is courtesy of iStock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none, except perhaps for AI-generated images in links included in today’s post. If readers wish to add any AI-generated content to the discussion thread today, they must cite their source. Thank you.
Today’s offering is about the “under-the-table” work, the “being performed but under another name” work, the “grandfathered-in” work, of Gain-of-Function (GoF) experiments that are onoing. These GoF experiments involve experiments with mRNA-based platforms; with “inactivated virus” platforms; and, with “novel delivery” platforms. These GoF experiments are being funded by “private Big Money”; and, by the United States government (in other words, with taxpayer money.) This post is long; please bear with me.
It is now well-known that the COVID-19 disaster was a product of GoF experiments, of two types: One, the GoF work that was performed in various labs (the Baric Lab at UNC, Chapel Hill; the Wuhan Institute of Virology, Wuhan, Communist China; the United States Army biological weapons labs at Ft. Detrick, Maryland, among others.) And, Two, the GoF work that was performed using the lab-created Wuhan Hu1 SARS-CoV-2 virus itself as the foundation for the modRNA (aka mRNA) COVID-19 “vaccines” that were developed by numerous companies, among them: PfizerUSA (at the company’s Pearl River, New York, facility; and, at other facilities); and, BioNTech (Mainz, Germany); Moderna (with the NIAID in Bethesda, Maryland, and at other facilities) — for use in the United States and also world-wide. (Note: PfizerUSA and BioNTech are separate companies that operate as a “joint venture” called Pfizer-BioNTech. PfizerUSA and BioNTech each have a separate CEO [Chief Executive Officer].)
Three articles by Jon Fleetwood start today’s offering. The first is here: https://jonfleetwood.substack.com/p/260-children-infected-with-tubersulosis, “260 Children Infected With Tuberculosis in Gates-Funded Study Injecting Children with Live Mycobacterium bovis Bacteria: “New England Journal of Medicine'”, 8 May 2025. The second is here: https://jonfleetwood.substack.com/p/new-bill-gates-funded-chimeric-polio, “New Bill Gates-Funded Chimeric Polio Vaccine Sheds 100% in Recipients, Spread Documented: ‘The Lancet’ Journal”, 18 August 2025. The third is here: https://jonfleetwood.substack.com/p/bill-gates-funds-slim-microneedle, “Bill Gates Funds ‘SLIM’ Microneedle Tech That Self-Assembles Inside the Body”, 24 April 2025.
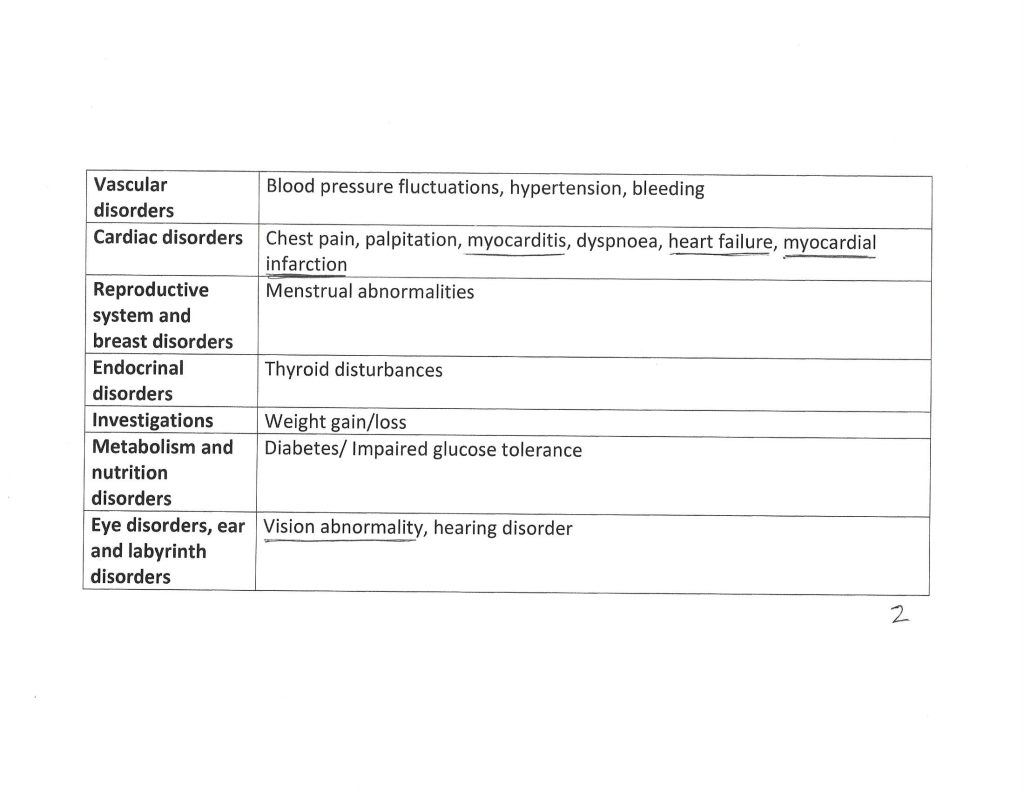
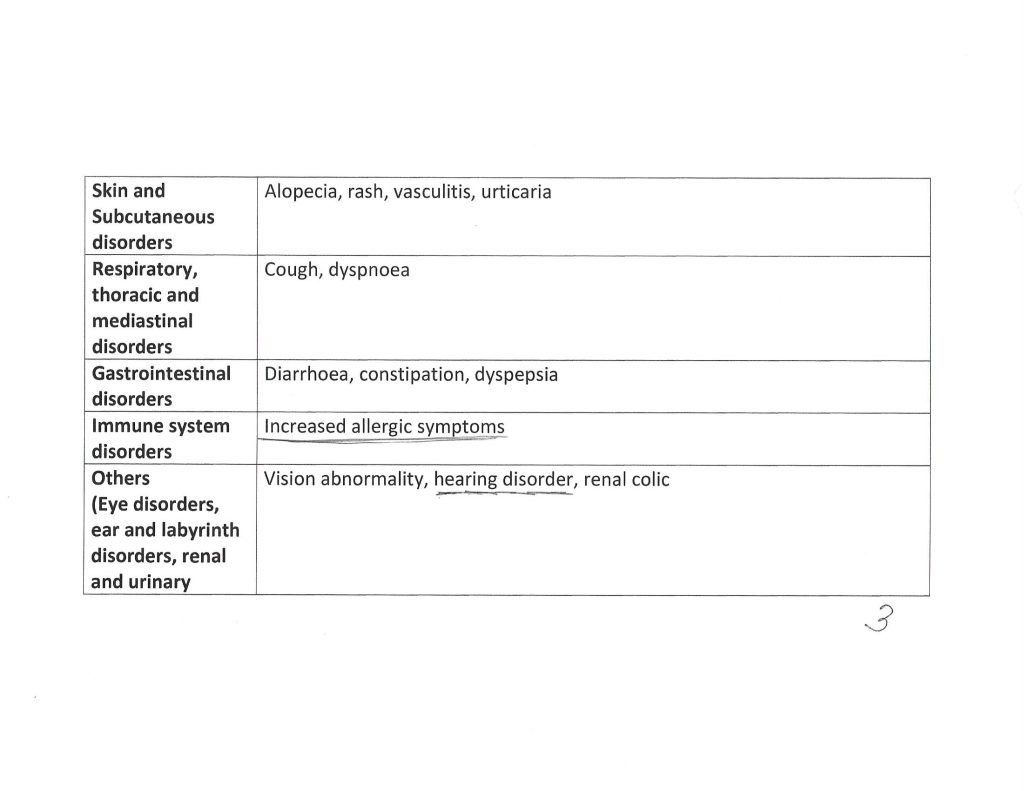
Regarding the first Jon Fleetwood article: The 260 study subject children were living in South Africa, and were between the ages of 10 and 18 years. They were confirmed by to be HIV-negative at the time they were added to the study subject pool. They were injected with the Danish tuberculosis vaccine BCG1331 strain (Bacille Calmette-Guerin). The Package Insert for this vaccine is here: https://nibsc.org/documents/ifu/07-270.pdf. The BCG1331 strain is the Mycobacterium bovis strain, which causes tuberculosis in cattle and can also cause the disease in humans, especially in HIV-compromised persons. Please see the screenshot from the Fleetwood article, below:
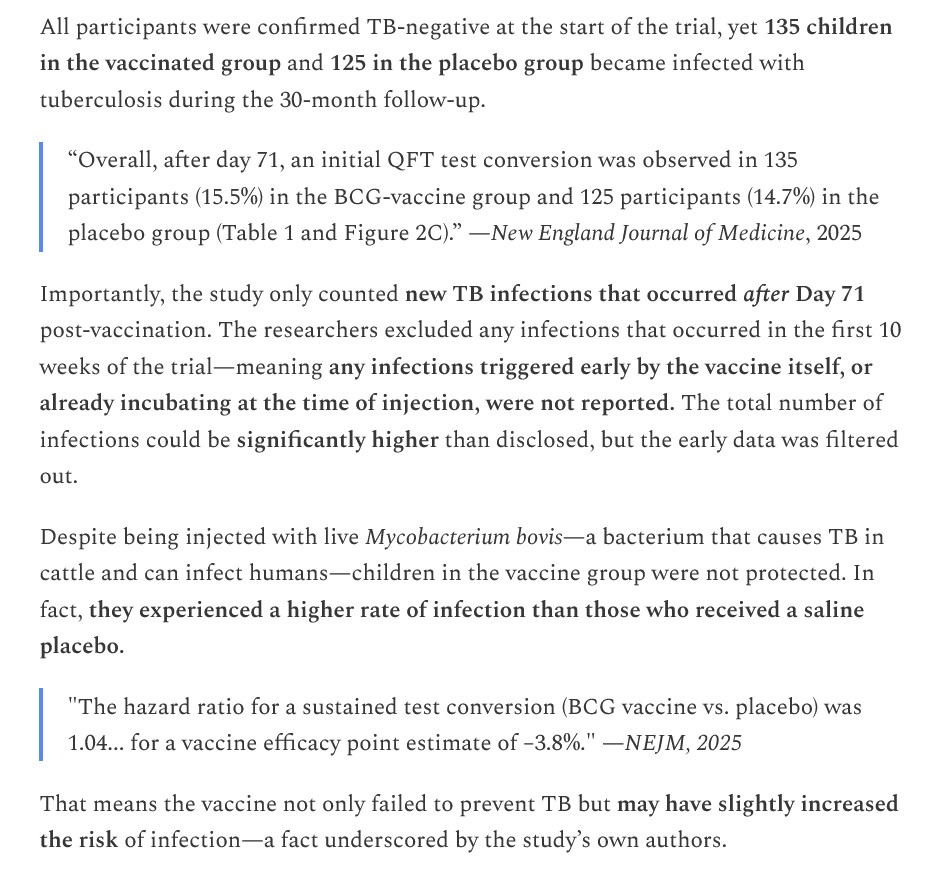
The paper that resulted from the study is here: https://doi.org/10.1056/NEJMoa2412381, “BCG Revaccination for the Prevention of Mycobacterium tuberculosis Infection”, Alexander C Schmidt, et al., 8 May 2025. Please see the screenshot from this paper, below:
In other words, 260 children now have tuberculosis because of the BCG1331 strain vaccine that they were injected with. And that Bill Gates funded this “human guinea-pig experiment.” But there’s more — the Fleetwood article also describes the Bill Gates-funded Mycobacterium bovis experiments at the University of Texas, performed in 2012, that resulted in a what may be called a “turbo-charged Gain-of-Function” version of this tuberculosis bacterium. The paper that was published from the 2012 study is here: https://doi.org/10.1016/S1472-9792(13)70007-6, “Mycobacterium tuberculosis MtrAY102C is a gain-of-function mutant that potentially acts as a constitutively active protein”, Akash T Satsangi, et al., published December 2013.
Regarding the second Fleetwood article: Another Bill Gates-funded effort, this time about a lab-created chimeric polio oral “vaccine” that was tested on human subjects in the United States. The study results are nothing short of terrifying. Please the screenshot from the Fleetwood article, below:
There was a 100% incidence of “shedding” of this lab-created chimeric oral polio “vaccine.” Six human subjects were released from the study when it was found that testing of their stool showed they had possibly contracted the oral vaccine virus from other study subjects. Several human subjects had severe adverse reactions to this lab-created chimeric oral polio “vaccine.” This lab-created chimeric oral polio “vaccine” caused “unexpected” interactions with the type 2 poliovirus.
The team that lab-created this chimeric oral polio “vaccine” were from medical centers across the United States, including: University of North Carolina, Chapel Hill; University of Vermont; and, Dartmouth. The paper that was published from the study is here: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(25)00285-3/fulltext, “Safety and immunogenicity of novel live attenuated type 1 and type 3 oral poliomyelitis vaccines in healthy adults in the USA: a first-in-human, observer-masked, multicentre, phase 1 randomized controlled trial”, Laina D Mercer, PhD, et al., 13 August 2025. The clinical trial for this lab-created chimeric polio virus “vaccine” is listed here: https://clinicaltrials.gov/study/NCT04529538. Again, from the Fleetwood article:
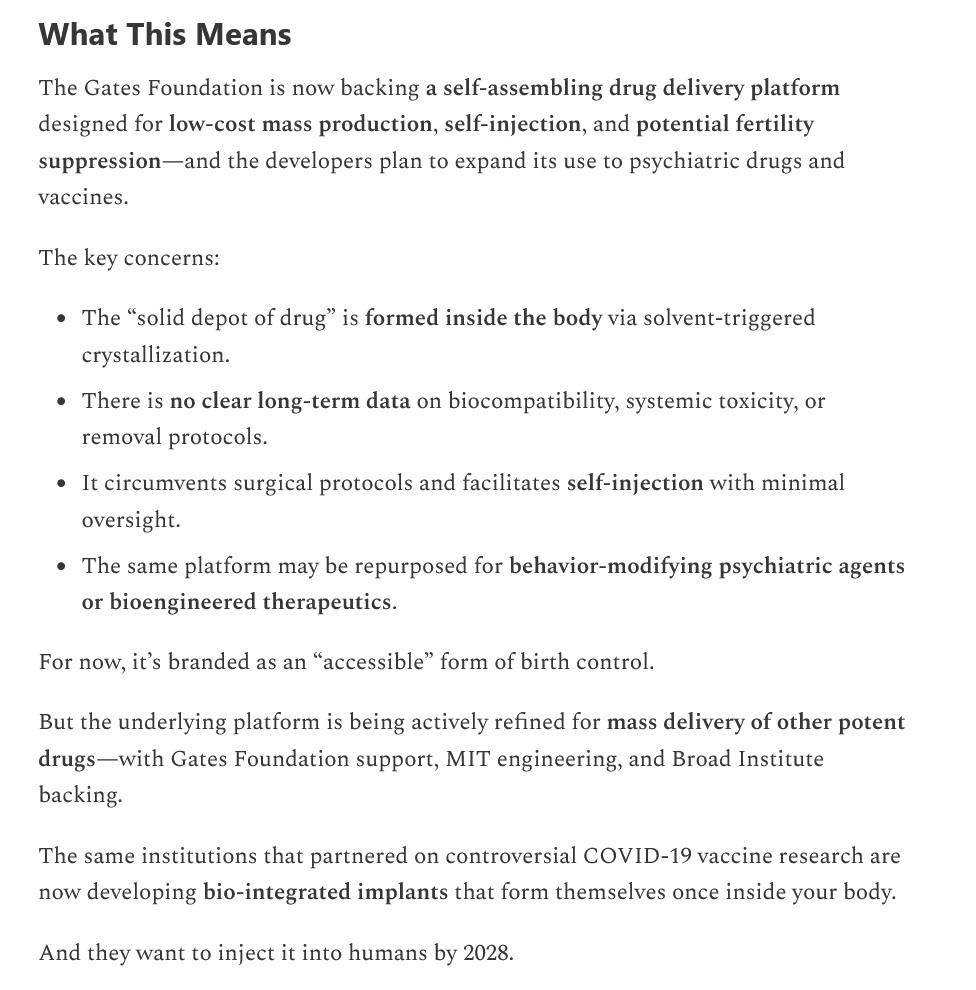
Regarding the third Fleetwood article: Bill Gates has funded the creation of a new technology, called “SLIM microneedle”, which injects “microcrystals” of a contraceptive drug (levonorgestrel) into the body of a female; and, which microcrystals then”self-assemble” into an “implant” inside her body. Please see the screenshot from the Fleetwood article on this situation, below:
This type of “self-injected, self-assembly inside the body” approach has profound implications. Please see below, again from the Fleetwood article:
The paper that was published on this issue is here: https://www.nature.com/articles/s44286-025-00194-x, “Self-aggregating long-lasting injectable microcrystals”, Vivian K. Feig, et al., 24 March 2025. Note how “self-assembling” has magically become “self-aggregating” — in some attempt to hide the fact that the microcrystals really do “self-assemble?”
The SLIM “delivery system” for the contraceptive levonorgestrel (called “LNG” in the paper above) uses a solvent called Benzyl Benzoate (called “BB” in the paper above.) The paper describes the experiments performed to find the “right combination” of levonorgestrel + Benzyl Benzoate to create the SLIM delivery system — the “winning delivery system candidate” was named “LNG-BB.” Benzyl Benzoate is clearly dangerous. Part of Section 4 FIRST AID MEASURES from the MSDS Safety Sheet on Benzyl Benzoate from Spectrum Chemical (https://www.spectrumchemical.com/) is below:
And this is the “long-lasting solvent” that is used in the SLIM microneedle “self-aggregating” delivery system for levonorgestrel. Which means that this solvent will be acting in the body of the female who uses this delivery system for this drug for an (undetermined) amount of time.
Now, on to a recent GoF experiment, this one funded by NIH / NIAID, at the University of Pittsburgh. This GoF experiment resulted in the lab-creation of a chimeric H5N1 Avian Influenza virus strain that could infect dairy cattle. Jon Fleetwood wrote about this situation, here: https://jonfleetwood.substack.com/p/nih-funded-pennsylvania-researchers, “NIH-Funded Pennsylvania Researchers Build New Frankenstein Bird Flu Virus: ‘Journal of Virology'”, 26 August 2025. Vesicular stomatitis virus (VSV) is a virus that infects horses and cattle. In humans, Stomatitis infection can result in HSV-1 (the “cold sore” virus: per https://my.clevelandclinic.org/health/diseases/stomatitis-oral-mucositis.) However, the researchers at the University of Pittsburgh concentrated on “splicing” an element of VSV with H5N1. The paper that was published from this experiment is here: https://doi.org/10.1128/jvi.00621-25, “Dairy cattle herds mount a characteristic antibody response to highly pathogenic H5N1 avian influenza viruses”, Kevin R. McCarthy, et al., 25 August 2025. Please see the screenshots from the Fleetwood article on this issue, below:
Isn’t it “convenient timing” that this “new, chimeric VSV + H5N1 virus” comes on the heels of the announcement by the White House on 5 May 2025, that Gain-of-Function research would be stopped — but it appears that “certain contracts” would be permitted to “finish out”? And, that one of those “certain contracts” is with Arcturus Therapeutics for its self-amplifying RNA (saRNA) Avian Influenza “vaccine”, ARCT-2304? The White House announcement is here: https://www.whitehouse.gov/presidential-actions/2025/05/improving-the-safety-and-security-of-biological-research/. The news release related to the second quarter 2025 financial update and “pipeline progress” for Arcturus Therapeutics in which ARCT-2304 is mentioned, is here: https://www.biospace.com/press-releases/arcturus-therapeutics-announces-second-quarter-2025-financial-update-and-pipeline-progress, 12 August 2025. The clinical trial for ARCT-2304 is registered here: https://clinicaltrials.gov/study/NCT06602531; which, by the way, has NO saline-only Placebo control group; the only “control groups” in the study will be injected with a “control vaccine” or a “placebo vaccine” (which last, in and of itself, is not a true Placebo.)
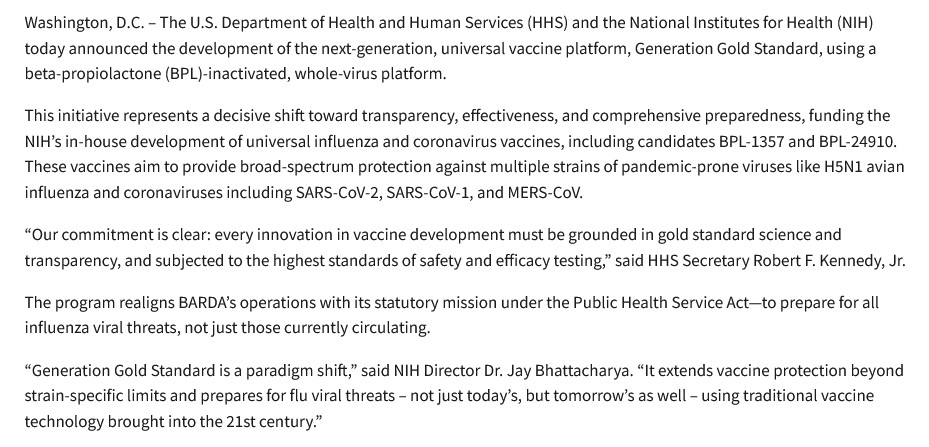
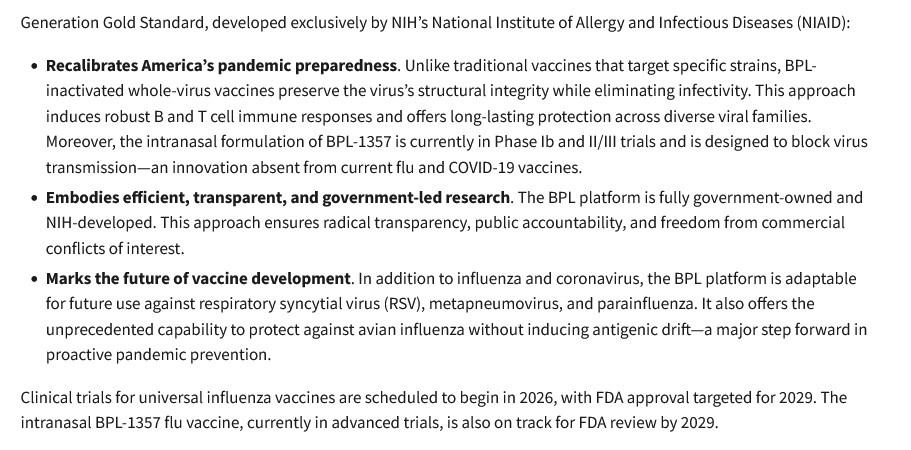
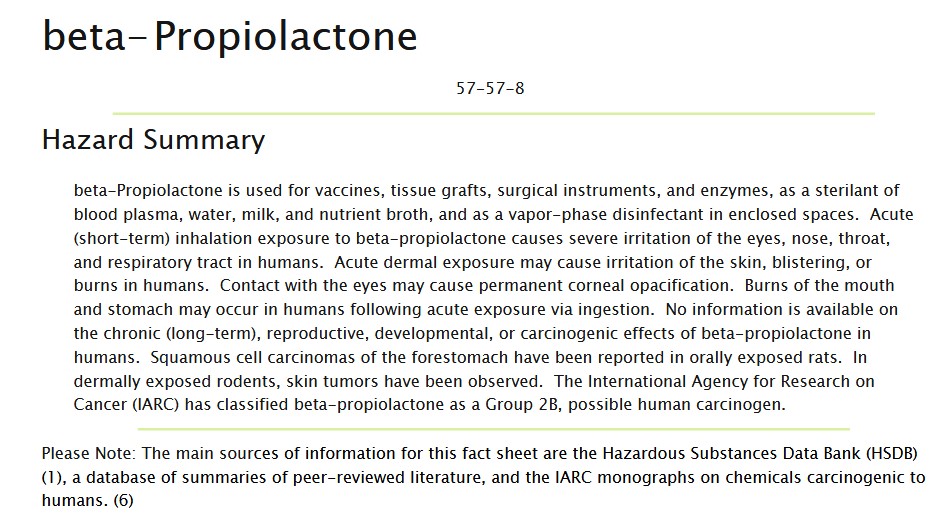
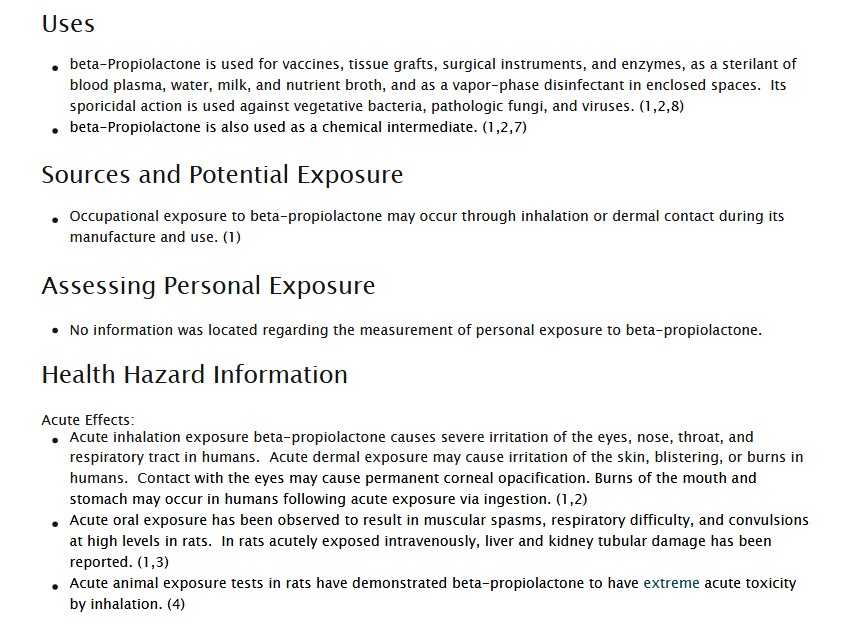
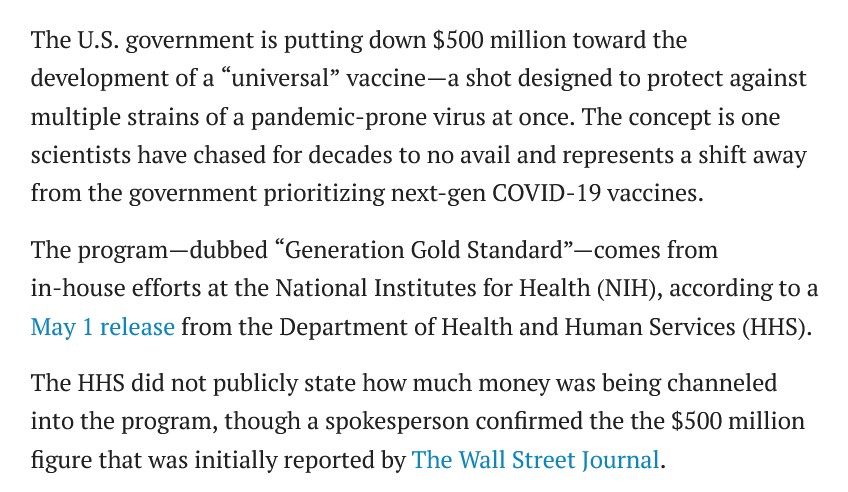
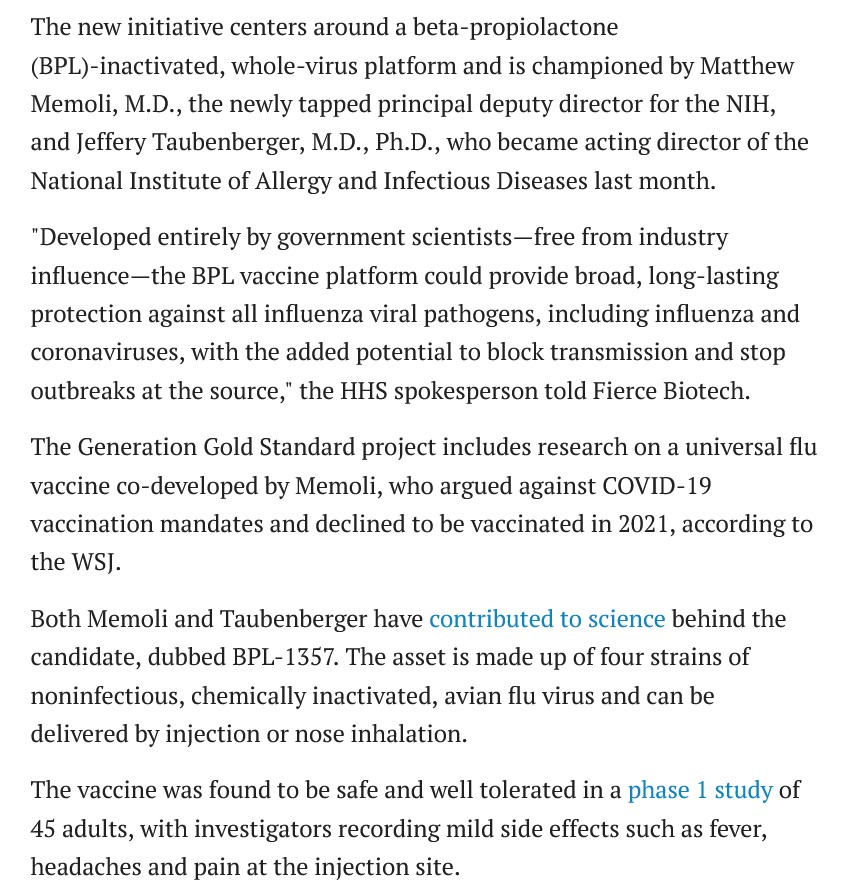
And now, regarding something else: the GoF experiments that resulted in the lab-creation of an Avian Influenza “vaccine” which is a “Cocktail of Inactivated Avian Influenza Viruses”, a patent owned by Dr. Jeffery Taubenberger, a “career medical employee” of HHS and the federal government, and who is also the current Acting Director of the NIAID (National Institute of Allergy and Infectious Diseases, previously headed by Dr. Anthony Fauci), and who now is in control of the $500 Million dollars that was pulled from mRNA research activities in May 2025. This “bird flu vaccine cocktail” contains BPL (Beta-propiolactone), a known carcinogen.
The NIH TechTransfer information on this “cocktail” invention by Dr. Taubenberger is here: https://www.techtransfer.nih.gov/tech/tab-3388, “Broadly Protective Influenza Vaccine Compromising a Cocktail of Inactivated Avian Influenza Viruses”. Sounds “benign,” yes? Until one starts reading the actual Patent document itself, found here: https://image-ppubs.uspto.gov/dirsearch-public/print/downloadPdf/11369675, filed 21 July 2020. The following are screenshots from the Patent document:

Note it appears that Dr. Taubenberger was experimenting with as many as sixteen different strains of Avian Influenza to lab-create his “cocktail vaccine.”

Note it appears that Dr. Taubenberger is perfectly all right with “vaginal” and “rectal” administration of his “cocktail vaccine.”
Note that the Patent was registered in July 2020 — which can only mean that work on the experiments to lab-create this “Avian Influenza cocktail vaccine” must have begun at least nine months earlier. This would place the commencement of the experiments around October 2019 — just before the COVID-19 original virus was unleashed on on the world.
Here are two screenshots from the MSDS Safety Sheet for Beta-propiolactone from Sigma Aldritch (https://www.sigmaaldritch.com/US/en/sds/sigma/p5648):
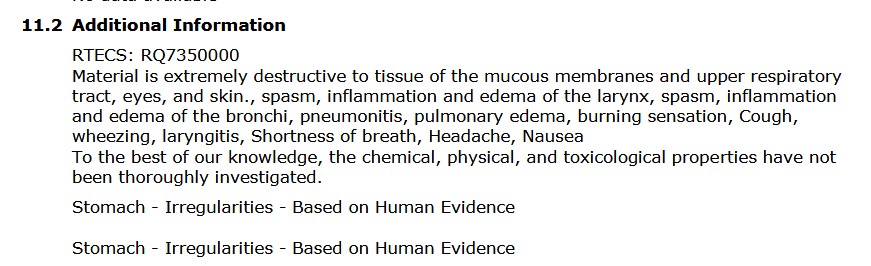
And THIS ingredient is part of the “Avian Influenza Cocktail Vaccine” of Dr. Jeffery Taubenberger, two possible methods of administration of which are INTRANASAL or INHALED, per the Patent document images above?

It is not enough that HHS Secretary Robert F. Kennedy, Jr., terminated 22 contracts for mRNA research in May of this year, but allowed “certain contracts” for mRNA (and saRNA) research to “finish out.” It is not enough that the White House announced a ban on Gain-of-Function research, since this type of research is still going on — funded by “private Big Money”, and/or by the NIH / NIAID (in other words, the United States government). The entire Gain-of-Function situation must be stopped, from all funding sources and on all levels of research and experimentation — until there are clear, firm, and enforceable regulations and restrictions on who can perform this type of research; that such research can only be permitted under strict circumstances; that such research must be under tight supervision; and, that such research can only be performed where there is a clear need in the area of public health — not what amounts to a “chimeric fishing expedition” to lab-create viruses. It is time for any and all “go-along-to-get-along” activities to stop — such as, bowing to the “demand” by Sen. Dr. Bill Cassidy for his “cooperation” in “working with” HHS as regards hiring, or anything else. By the way — Sen. Dr. Cassidy has received donations from multiple pharmaceutical entities (United Health, AstraZeneca, Pediatrix Medical Group, and so on: per Open Secrets (https://opensecrets.org/.) And — that the further development of the above-discussed “Avian Influenza Cocktail Vaccine” must be stopped.
HHS Secretary Kennedy, Jr.: Please understand that the “career medical bureaucrats” in the CDC, the FDA, and the other divisions of the HHS, are not inclined to your views. They want “the good old days” of these divisions brought back. They are working “behind the scenes” in some instances, and in other instances, out in the open, to obstruct, delay, and thwart your efforts to clean up HHS and “re-tool” the department to reflect Make American Healthy Again. There is even what may be called “soft interference” by persons not employed by HHS such as, Sen. Dr. Cassidy.
THERE. MUST. BE. ACCOUNTABILITY.
THERE. MUST. BE. JUSTICE.
THERE. MUST. BE. TRUTH.
Peace, Good Energy, Respect: PAVACA