“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
The above free image of an 1867 vaccination certificate is courtesy of iStock and Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics. As today’s post speaks to the disaster of the COVID-19 “vaccines”, Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created bioweapon toxin injections.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s post for any AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post any AI-generated content in the discussion thread for today’s post, they must cite their source. Thank you.
Today’s Health Friday offering is one of a “mini-series” devoted to one topic and to one important news item related to that topic (although there may be other items related to the topic presented as supporting and/or clarifying information. The topic for today is what the COVID-19 “vaccines” do to damage and/or destroy the crucial IgG3 immune system cells in the “vaccinated” person’s body.
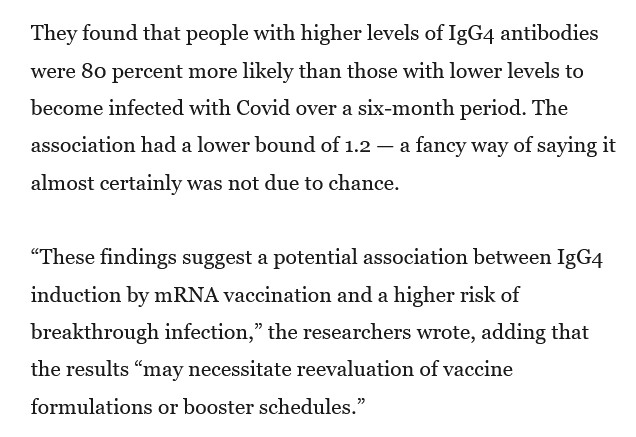
This 80% higher risk was found in persons who had had multiple injections of COVID-19 “vaccines.”
The COVID-19 “vaccines”, especially via repeated injections, damage and destroy the crucial IgG3 (“fight it off”) immune system cells in the “vaccinated” person’s body; while, at the same time, fostering the increase of the IgG4 (the “tolerate but never clear”) immune system cells.Another screenshot from the Berenson article is below:
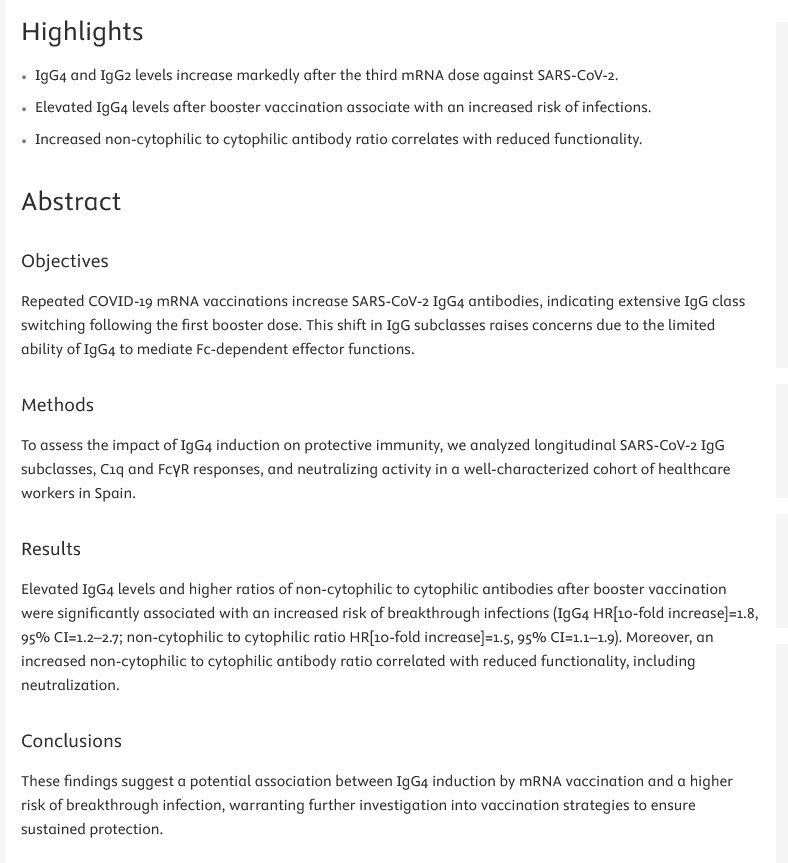
The paper referred to in the Berenson article is here: https://doi.org/10.1016/j.jinf.2025.106473, “Post-Vaccination IgG4 and IgG2 class switch associates with increased risk of SARS-CoV-2 infections”, Gemma Monocunill, et al., 18 March 2025. Below is a screenshot from this paper:
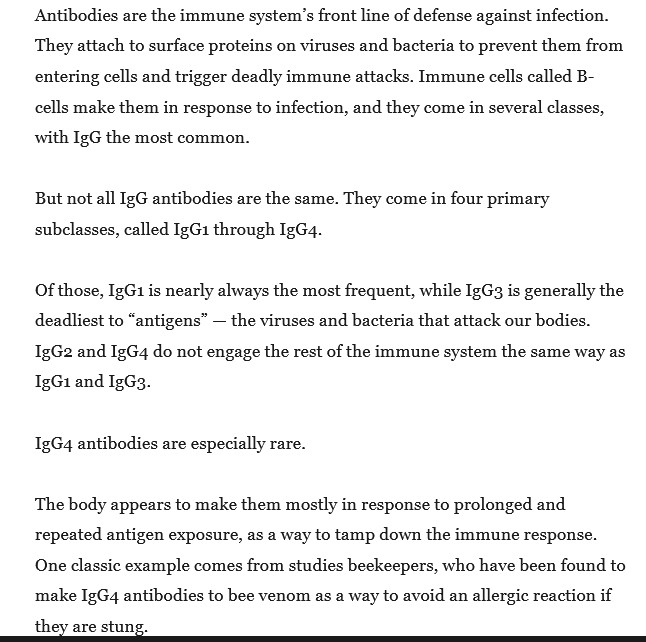
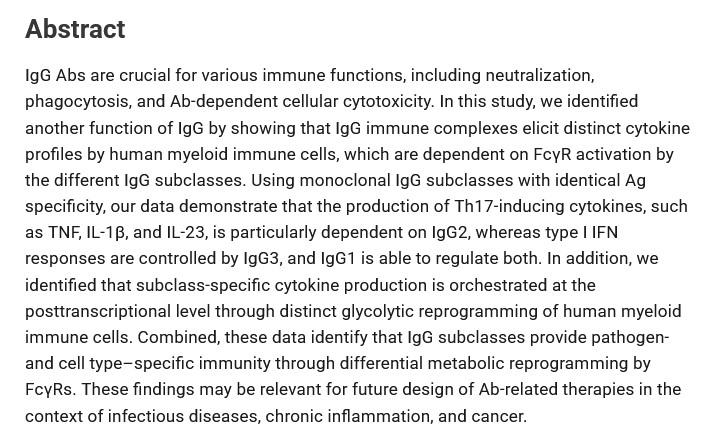
An important paper regarding descriptions and functions of the IgG immune system cell class in the human body is here: https://journals.aai.org/jimmunol/aticle/205/12/3400/107683/IgG-Subclasses-Shape-Cytokine-Responses-by-Human, “IgG Subclasses Shape Cytokine Responses by Human Myeloid Immune Cells through Differential Metabolic Reprogramming”, Willianne Hoepel, et al., 15 December 2020. A screenshot of the Abstract of this paper is below:
Note that this paper was published after the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna were granted their initial EUAs in the United States by the FDA (this occurred on 11 December 2020), but before these bioweapon toxin injections entered widespread use.
Back to the Monocunill, et al., paper. There is mention in the paper regarding the involvement of the T17 cells in the “vaccinated” person’s body in the IgG subclass switching. Yours Truly wrote about the importance of the T17 cells (also called Th17 cells or T17 Helper Cells), and the role of the N1-Methylpseudouridine in the modRNA COVID-19 “vaccines” in “turning off” these cells in the “vaccinated” person’s body (thus paving the way for continuous inflammation of many types) here: https://www.theqtree.com/2025/03/21/health-friday-3-21-2025-open-thread-more-on-the-n1-methylpseudouridine-in-the-modrna-covid-19-vaccines/.
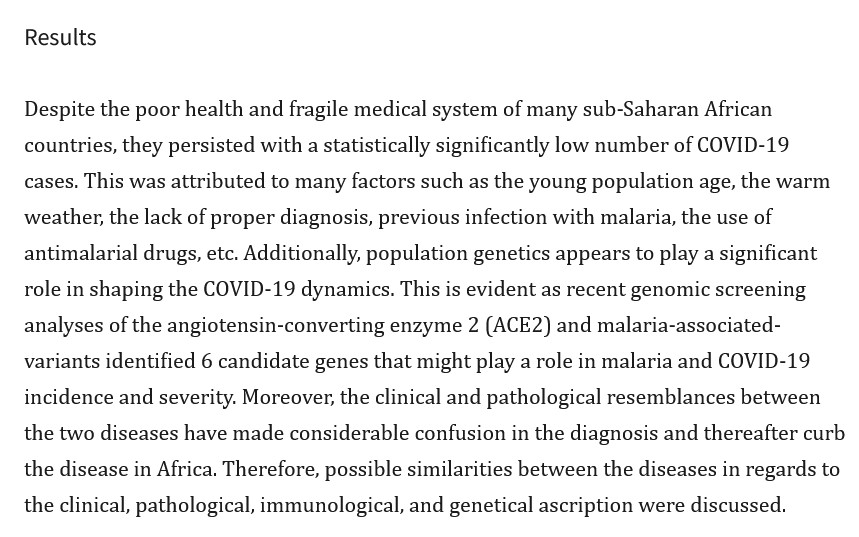
However, there is another aspect of the situation discussed in the Monocunill, et al., paper that is of huge importance: The similarities between malaria, COVID-19 infection, and the class switch to IgG4 that the COVID-19 “vaccines” induce. Below is a screenshot from the Discussion section of the paper regarding this:
Yours Truly will now blow something out of the water regarding the FDA’s and the CDC’s official opposition to, and prohibition of, using Ivermectin or Hydroxychloroquine to prevent or to treat COVID-19 infection.
And, Hydroxycholoquine (and also Chloroquine) can be used to treat malariaAND COVID-19. Please see this paper from September 2020: https://pmc.ncbi.nlm.nih.gov/articles/PMC7476892/, “Chloroquine and hydroxychloroquine in the treatment of malaria and repurposing in treating COVID-19”, Zi-Ning Lei, et al. (USA and CCP), 8 September 2020.
In Yours Truly’s opinion, it is inconceivable that the NIH / NIAID / FDA / CDC did not know about the existence of these papers. Instead, by September 2020, these entities were hell-bent in pushing through the unproven modRNA “technology” for the Pfizer-BioNTech and the Moderna modRNA COVID-19 “vaccines” then in development. This meant that the FDA / CDC accepted the manipulated / incorrect “data” that were given to them from the truncated “clinical trials” for these “vaccines” by Pfizer-BioNTech and by Moderna. This meant that the FDA / CDC did not question the sudden “vaccine”-manufacturing switch from the original “Process 1” method to the “Process 2 method” that occurred in August 2020, that is still in use by both companies in the production of their respective “new formula” COVID-19 “vaccine booster shots”, and is based on “culturing” the modRNA of the said “vaccines” in a “bath” of E. coli.
Further confirmation that malaria and COVID-19 infect the lungs in similar ways is here:https://pmc.ncbi.nlm.nih.gov/articles/PMC9445119/, “The striking mimics between COVID-19 and malaria: A review”, Emadeldin Hassan E Konozy, et al. A screenshot from this paper is below:
Note the mention of the ACE2 receptorsas regards malaria infection. These cells are also attacked by the COVID-19 virus itself (and, therefore, since they are based on the virus, so do the COVID-19 “vaccines” attack the ACE2 receptors of the “vaccinated” person’s body.)
In short: the FDA / CDC pushed, and continue to push, COVID-19 “vaccines” to “prevent” COVID-19 infections, while knowing that Ivermectin and Hydroxychloroquine also prevent — and treat — COVID-19 infections. Why is this still going on? How about ASKING BILL GATES. UNDER OATH.
This is aside from the fact that those who lab-created the bioweapon of the COVID-19 virus itself, and those who lab-created-and-enhanced the bioweapons of the COVID-19 “vaccines” — knew that malaria and COVID-19 would attack the lungs in similar ways. They knew what would “turn off” the T17 cells that are so important for the immune system and for Uridine in the human body. They knew what would damage or destroy the crucial IgG3 cells of the natural immune system of the human body, while fostering the increase of the IgG4 cells that allow illness and medical conditions to take hold and thrive. These things they incorporated into the creation of the COVID-19 virus itself, and into the creation of the COVID-19 “vaccines.”
I wrote this almost 2 decades ago. Most of the reference documents have been removed, archived or changed. However the basics remain the same.
Raw milk is a product whose safety CAN be assured by means other than pasteurization. The first is herd isolation and constant testing of the herd for diseases such as tuberculosis and brucellosis. The second is a very high standard of cleanliness during milking, the third is the testing of the milk itself. If you wish to drink raw milk, as some do then you KNOW the seller and check his facilities and testing procedures.
Unfortunately this type of program would uncover a whole can of worms the USDA/FDA and more importantly the International Corporate Cartel wants buried very DEEP. It is for that same reason the USDA and the Bush Admin. squashed the attempts of Creekstone to do its own BSE testing for Mad Cow disease.
Here is a bit about the BSE cover-up most people are unaware of and why the USDA/FDA want NO TESTING.
…Before the BSE crisis about 350,000 tons of MBM feed was sold in Britain a year, and relatively little was exported. After the ban the UK government did inform the EU, but there was a surge in exports to Europe. Then, as European states – informed of the danger – banned British feed, exporters opened up new markets, including North America, the Middle East and Asia.
Dr Stephen Dealler, a microbiologist and BSE expert, said: “It was a terrible mistake… Look at the controls they are now trying to apply to stop BSE in France and other EU countries. It is going to be much harder in African and Middle Eastern countries.”
Evidence to the British BSE inquiry headed by Lord Phillips shows that British officials washed their hands of moral responsibility over the dangers of MBM spreading BSE to infection-free countries, the approach was to inform international bodies, leaving it to member states to decide whether to import UK feed and prevent it being fed to cattle.…
… It took the United States 10 years to follow Britain’s lead and ban the feeding of cattle-derived meat and bone meal (MBM) back to cattle. But the U.S. allows – indeed, actively promotes – the export of MBM to other countries. The Food and Drug Administration (FDA) makes no requirement that warning labels against feeding it to cattle be placed on the product.
One country that exports over a million cattle a year to the United States – Mexico – is just now adopting the ban on MBM as cattle feed. And the enforcement of that ban is suspect.
The FDA has allowed hundreds of meat-processing facilities to fudge on its MBM rules, handing out a handful of warning letters and taking little action to force compliance…
There is a small chance that mad cow disease.. (BSE), is already in this country, according to a risk assessment released today by Harvard University. The risk assessment concluded that even if BSE had entered this country, it wouldn’t become a major public health problem, although human illnesses could occur”.Harvard Risk Assessment 12/3/2001 http://www.organicconsumers.org/madcow/danger6102.cfm
Quantitative assessment of the BSE risk from meat and bone meal in MBM export, pet food, etc. non-ruminant feed mill mixed feed mill non-ruminant: http://www.svepm.org.uk/posters/2007/De%20Vos.pdf — Page not archived
After disease detectives in Great Britain determined that mad cow (BSE), was spread by feeding cattle infected meal, British officials banned the practice. But they didn’t ban the export of feed, spreading BSE to continental Europe and Japan…At the height of the BSE epidemic, the UK exported 500,000 tons, including 168,000 metric tons of MBM (meat and bone meal) between 1990 and 1996. It also exported 3.2 million cattle to 36 countries. A Harvard study said that the exact amount sent to the U.S. was unknown, but it noted that at least 69 tons of “mammalian meal and flour” and 334 cattle were shipped here during the period. https://web.archive.org/web/20020813043834/http://www.organicconsumers.org/madcow/danger6102.cfm
….is raw milk safe to drink even? The FDA and food safety experts caution against consuming unpasteurized dairy but that doesn’t stop A-list celebs, like Gwyneth Paltrow from adding raw cream to her coffee every morning.
She lives in California, where the sale of raw milk is legal, provided it has a warning label. (FYI: Her purveyor for raw milk has been linked to at least 165 salmonella cases, the largest outbreak in the U.S. in over a decade.) [So why in hades has it not been shut down? – GC]
…And talk about politics making strange bedfellows: Former presidential candidate Robert F. Kennedy Jr.said, “I only drink raw milk,” in a video clip that made rounds on Twitter/X. Pesky government food regulations be damned!….
Here are some of the pros (notice the fight has been a very long one)
Pasteurization’s great claim to popularity is the widespread belief, fostered by its supporters, that tuberculosis in children is caused by the harmful germs found in raw milk. Scientists have examined and tested thousands of milk samples, and experiments have been carried out on hundreds of animals in regard to this problem of disease-carrying by milk. But the one vital fact that seems to have been completely missed is that it is CLEAN, raw milk that is wanted. If this can be guaranteed, no other form of food for children can, or should, be allowed to take its place.
Dirty milk, of course, is like any other form of impure food — a definite menace. But Certified Grade A Milk, produced under Government supervision and guaranteed absolutely clean, is available practically all over the country and is the dairy-farmer’s answer to the pasteurization zealots.
Recent figures published regarding the spread of tuberculosis by milk show, among other facts, that over a period of five years, during which time 70 children belonging to a special organization received a pint of raw milk daily. One case only of the disease occurred. During a similar period when pasteurized milk had been given, 14 cases were reported.
Besides destroying part of the vitamin C contained in raw milk and encouraging growth of harmful bacteria, pasteurization turns the sugar of milk, known as lactose, into beta-lactose — which is far more soluble and therefore more rapidly absorbed in the system, with the result that the child soon becomes hungry again.
Probably pasteurization’s worst offence is that it makes insoluable the major part of the calcium contained in raw milk. This frequently leads to rickets, bad teeth, and nervous troubles, for sufficient calcium content is vital to children; and with the loss of phosphorus also associated with calcium, bone and breain formation suffer serious setbacks.
Pasteurization also destroys 20 percent of the iodine present in raw milk, causes constipation and generally takes from the milk its most vital qualities
Looks like pasteurized milk is great news for Big Pharma and the supplement manufacturers.
My testimony was framed to respond to objections to raw milk raised by the state health department and to document the benefits of raw milk. To quote from that testimony:
“The state epidemiologist writes that ‘It has yet to be demonstrated that raw milk has any beneficial health effects. . . ‘ He cites articles attached to his letter. In one article, ‘Unpasteurized Milk, The Hazards of a Health Fetish’ (Journal of the American Medical Association, 10/19/84), the authors make a series of misstatements about the research of Francis Pottenger before concluding that raw milk has no health benefits. I detail these charges as follows in the paper I’ve given the members of the Committee.
“Now what Pottenger actually did in some of his experiments is this. He used four groups of cats. All received for one-third of the diet raw meat. The other two-thirds of the diet consisted in either raw milk or various heat-treated milks. The raw milk/raw meat diet produced many generations of healthy cats. Those fed pasteurized milk showed skeletal changes, decreased reproductive capacity and infectious and degenerative diseases.
“Now just who was Francis Pottenger? He was the son of the physician who founded the once famous Pottenger Sanatorium for treatment of tuberculosis in Monrovia, California. He completed his residency at Los Angeles County Hospital in 1930 and became a full-time assistant at the Sanatorium. From 1932 to 1942, he also conducted what became known as the Pottenger Cat Study.
“In 1940, he founded the Francis M Pottenger, Jr. Hospital at Monrovia. Until closing in 1960, the hospital specialized in treating non-tubercular diseases of the lung, especially asthma.
“Dr. Pottenger was a regular and prolific contributor to the medical and scientific literature. He served as president of several professional organizations, including the Los Angeles County Medical Association, the American Academy of Applied Nutrition and the American Therapeutic Society. He was a member of a long list of other professional organizations.
“Pottenger’s experiments met the most rigorous scientific standards. His outstanding credentials earned him the support of prominent physicians. Alvin Foord, MD, Professor of Pathology at the University of Southern California and pathologist at the Huntington Memorial Hospital in Pasadena, co-supervised with Pottenger all pathological and chemical findings of the study.
“One particular question that Pottenger addressed in his study is one that modern science has largely ignored. It has to do with the nutritive value of heat-labile elements-nutrients destroyed by heat and available only in raw foods.
“In his article ‘Clinical Evidences of the Value of Raw Milk,’ Pottenger writes: ‘Some of the factors transmitted by milk are thermo-labile [sensitive to heat]. Though their destruction may not produce death, their deficiency may prevent proper development of the child. This may show in the development of an inadequate skeleton or a decrease in resistance. . . . delay in development of osseous centers is noted more frequently in those children. . . receiving heat treated milk. It is particularly absent from the raw milk fed children. . . . I am basing this discussion on analysis of 150 children whose parents have consulted me because of respiratory allergies. Many other workers. . . have also shown that treating milk by heating interferes with its proper assimilation and nutritional qualities. . . . The best milk from a nutritional standpoint is raw milk. . . . Heat-treating milk interferes with calcium metabolism causing. . . delay in bone age and small bones. . . . The interference with calcium metabolism as shown in the bones is only a physiological index of disturbed metabolism throughout the body.’
“I have prescribed raw milk from grass-fed animals to my patients for nearly fifteen years. Time and again I have seen allergies clear up and dramatically improved health. Particularly in children, middle ear infections usually disappear and do not recur on raw milk. Both children and adults unable to drink pasteurized milk without problems have thrived on raw milk. In hundreds-perhaps thousands-of my patients using raw milk, not one has ever developed a salmonella, campylobacter, or other raw-milk-related infection.
“In the letter cited above, the state epidemiologist states that ‘The processes of certification and/or inspection do not guarantee that raw milk will not be contaminated with pathogenic organisms.’ He also lists a host of microorganisms that are alleged to be transmitted by raw milk, not mentioning that, as the literature accompanying his letter makes clear, the only organisms even potentially associated with the consumption of certified raw milk are salmonella and campylobacter. And in one of the articles he cites, ‘The Hazard in Consuming Raw Milk’ (in The Western Journal of Medicine), the authors actually state that ‘Salmonella and campylobacter diseases in humans are generally not serious. But in persons with compromised health (particularly those with malignant conditions and immunosuppressed by disease or therapy), these infections may be serious.’
“So, the gist of the state’s argument against certified raw milk is that it might possibly on isolated occasions cause serious disease in some people whose immune systems have been compromised by the toxic effects of chemotherapy. And because of this very slight risk, those of us who might choose to drink certified raw milk for the benefits I have catalogued should be denied that right.”
Here is the REASON the FDA went on the attack.
Please read the whole thing because it is really eye opening what has been done to the actual safety of our food.
“…While I believe a meaningful, uniform, universal ID system for all livestock with adequate tracking will evolve, as a state animal health official, I would be less than responsible if I did not encourage industry and government to move quickly to get a handle on our ability to traceback animals today for diseases such as brucellosis, tuberculosis, and others that present risks of exacerbation and the extreme costs associated with such…” Dr. Sam Holland, State Veterinarian, South Dakota from REPORT OF THE COMMITTEE ON LIVESTOCK IDENTIFICATION – 2005
Why the sudden need to stampede the USA into a track back system?
This is an example of the USDA’s response to one disease over the last decade. The chart shows how USDA cut back testing after WTO was created and the VP of Cargill wrote the WTO Agreement on Agriculture 1995.
Summary of Tuberculosis Surveillance in California Cattle
Number of Cattle Tested……..1995…..1996…..1997…….1998…….1999……2000…..2001 By Animal Health Officials…10,576…5,100 ….2,861 …..3,530…..1,425 ….1,967…..2,500 By Private Veterinarians …15,921…17,100…19,930…18,189…22,863…19,930…19,587 Submissions at Slaughter……….39……….58 ………64………..39………..58……….64………385
What about the danger of Bovine Tuberculosis in the USA since the passage of WTO and the lifting of tariffs and quarrantine mandated by WTO?
Bovine TB was confirmed in three dairy herds during 2002-2003.[California] ….Although the source of the infections was not confirmed, the investigations indicate TB was most likely imported in infected cattle…. http://www.cdfa.ca.gov/ahfss/Animal_Health/pdfs/Tb_in_California_2006.pdf — archived page removed
…
“The high prevalence of bovine tuberculosis in Mexican cattle was discussed. A multiagency investigation in New York city identified 35 cases of human M. bovis infection. Fresh cheese from Mexico was identified as the likely source of infection” (Winters et al., 2005). http://www.nzfsa.govt.nz/science/riskprofiles/FW0320_Mbovis_in_meat_final_May_2006.pdf — archived page removed
What was the USDA’s response to “The high prevalence of bovine tuberculosis in Mexican cattle”
Texas imports a million cattle a year from Mexico. The cattle port-of-entry at Santa Teresa, NM is the largest entry.
Cattle crossing facilities on the U.S. side of the border are operated primarily by private firms… at Santa Teresa, NM, Chihuahuan cattle producers [Mexican] operate both sides of the cattle port-of-entry… https://web.archive.org/web/20011117084712/http://www.ers.usda.gov/publications/Agoutlook/june2001/AO282d.pdf
SO what happened after the waivers of whole herd testing was granted”
For Mexican Feeder Cattle in Effect April 1, 2002… Dr. Logan… said, the disease is extremely rare in U.S. herds. However, more TB-lesioned cattle are being detected at slaughter, and ear tags indicate that many of these animals are of Mexican origin. https://web.archive.org/web/20030413013230/http://www.tahc.state.tx.us/news/pr/2002/302TBMx.pdf
Oklahoma On May 1, 2007, the Oklahoma Department of Agriculture reported a case of bovine tuberculosis (TB) discovered as a result of slaughter surveillance…. Subsequent testing of the index herd identified a TB- positive cow with a Colorado ID tag… The herd has been depopulated…Bovine TB was last reported in Oklahoma in 1982, and Oklahoma has been classified by the USDA as tuberculosis-free since 1984.
New Mexico On June 14, 2007, the State of New Mexico confirmed that a dairy herd in Curry County was infected with bovine tuberculosis…Two infected herds were confirmed with TB in late 2002, .
Additionally, it is anticipated that both New Mexico and California will lose their TB “free” status in 2008, from AGENCY STRATEGIC PLAN: FOR THE FISCAL YEARS 2009-2013 BY TEXAS ANIMAL HEALTH COMMISSION
What is the USDA/FDA position on testing by non-government (or non corporate cartel) entities???
The USDA is abandoning a known effective method of disease prevention, the first-point testing program, where the live cows in a herd are tested, in favor of a method that allows the disease more time to spread since the cows are at the end of their life before testing is done. Also Texas complains of the USDA shutting down disease testing labs by withdrawing funding. This is in line with the USDA’s refusal to allow Creekstone to test 100% of their slaughtered cattle for BSE and Japan’s response of increasing their cattle herds. See: http://www.cornucopia.org/2008/09/appeals-court-prevents-company-from-testing-for-mad-cow-disease/
Government targeting of independents.
The Henshaws were not allowed to test their animals or to even SEE the government test results.
….The claim is that the USDA did this because of Pseudorabies, yet the government did not follow it’s own standard operating procedures of testing as outlined in the USDA’s own documents. The USDA spilled bodily fluids from the slaughtered pigs all over the road where any disease could be transmitted to other farms and other animals. Slaughter is not required for testing for Pseudorabies. These issues seriously puts into question the validity of the disease claim and/or the competence of the government officials involved…. https://web.archive.org/web/20080922034213/http://nonais.org/2006/09/29/henshaw-incident/
The Faillice family had similar treatment from the USDA. When the standard test results were all negative and the animals had all been slaughtered, an experimental testing procedure was used and then the samples “lost” and “Destroyed” Of interest was the fact the Faillice family lived in England and were Experts on Mad Cow disease. (sorry about no direct link you would have to read the book Mad Sheep
There is a darn good reason to bury this report because it gives very good evidence that the USDA and FDA are intentionally allowing disease into this country and ALLOWING it to go unchecked by shutting down testing labs and NOT testing at farms.
Without the increase in food borne disease and the media’s propaganda spreading fear, there would be not reason to implement the new “Food Safety” law passed Congress during the December 2010 lameduck session. Senator Burr, after promising NC farmers he would not vote for the bill, was a co-sponsor. The new Law is specifically designed to wipe out independent farmers as similar laws have done in the European Union. The FDA has already stated it will “harmonize” with EU and other international laws per an agreement signed by Bush and the WTO AoA treaty.
Those treaties and the NEW Law are NOT designed to do a blasted thing about actual food safety. They are only there to help the International Cartels remove “barriers” to trade…. and to remove the independent farmer competition.
From the original before it was modified under the same date of course
The surveillance element or function is the most intensive of the six functions with respect to resources and personnel. Surveillance includes all activities designed and implemented to identify and locate any possible focus of infection or exposure to diseases of animal/poultry health significance in the livestock, poultry and exotic animal population. TAHC surveys animal populations for possible disease problems by collecting blood samples at livestock markets, on farms or ranches, and at slaughter plants…. Additionally, TAHC foreign animal disease diagnosticians investigate all reports of potential foreign animal diseases in order to achieve early diagnosis of a foreign animal disease, should it be introduced into the state.
USDA is moving toward supporting fewer labs nationwide, with the remaining labs serving as regional labs and supporting larger geographic areas….. If this funding is not maintained, this lab will be closed and the out-of-state samples will not be processed by remaining TAHC laboratories….
The first-point testing program is the “early warning system” for the brucellosis program, enabling detection of infection prior to sale of cattle within the state. With the discontinuation of first-point testing, slaughter testing will become the primary method for brucellosis surveillance. There is a key difference between first-point testing and slaughter testing. An animal identified through first-point testing as possibly infected is alive. This allows the agency to collect additional samples (blood, milk and tissue) and conduct additional diagnostic serologic and culture tests to determine if the animal is in fact infected with Brucella abortus. An animal identified through slaughter testing as possibly infected is no longer living and therefore additional testing of that animal is not possible. As a result, the process to be followed requires the identification of the herd the animal came from and conducting a whole herd test to determine whether or not infection is present in the herd. The traceability back to the original owner or farm of origin is also much higher in a first-point test positive versus a slaughter positive, because the animals are individually identified with permanent identification devices, are identified to an owner at the time of testing and market records improve traceability of the animals. …
..All states are expected to collaboratively participate in cooperative disease control and eradication programs or face significant animal movement restrictions from USDA and other states. Movement restrictions would significantly reduce the marketability of Texas animals and increase the cost of market access.
[NAFTA and WTO trade agreements impact] …New national disease control programs, emergency management responsibilities, and trade agreements with foreign countries have a significant impact on TAHC. These new or expanded programs continue to stretch TAHC’s already stressed resources to their limits.
[foreign diseases imported due to trade agreements and the Agreement on the Application of Sanitary and Phytosanitary Measures]
…The responsibilities of TAHC have significantly increased as programs for disease control and surveillance have expanded, animal and premises identification systems have been initiated, and participation in emergency planning and response activities impacting animal health require more agency resources. Additionally, new disease challenges are emerging. Some are domestic diseases that are increasing in significance. Others are foreign diseases that may be imported as result of the exponential increases in international importations of animals and animal products. Our industries and our economy are threatened by diseases and pests that heretofore we only read about in disease text books or heard about in lectures….
Since 1999, there have been seven foreign animal diseases diagnosed within the United States (West Nile Virus, Exotic Newcastle Disease, High Pathogenic Avian Influenza, Hemorrhagic Disease of Rabbits, Monkey Pox, Bovine Spongiform Encephalopathy, and Wildebeest Associated Malignant Catarrhal Fever). Unfortunately, there does not appear to be an end in sight for outbreaks of foreign or domestic diseases and these diverse activities related to disease control and eradication….
As usual the situation is not nearly as cut and dried as the government and its propaganda arm, the Mass Media would paint it.
Analysis of the real problems with US food safety:
The above free vintage image of a scientist at work is courtesy of StockCake and Google Images.
As Gail Combs is apparently still in “locked out” mode for publishing posts (via WordPress, or **some other entity**), our host, Wolf Moon, gave the go-ahead for Yours Truly to do a Placeholder Open Thread for today. I am indebted to our host for this opportunity, as further information has surfaced regarding the role of the pangolin-CoV MP789 virus in the lab-creation of the SARS-CoV-2 (COVID-19) virus itself. Since today’s post concerns the COVID-19 virus itself, and the COVID-19 “vaccines”, it is dedicated to the memory of Yours Truly’s COVID-19 “vaccinated” brother Sam, and to her cousin Bill; and to all persons, of whatever age and location, who have passed away from the negative effects of the COVID-19 “vaccines” that they had in their bodies. However, the discussion is not limited to what is presented here: It is an Open Thread. Bear with me: there are a couple of surprising details coming up. There is a General Summary at the end of the post.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
To Begin: What will be called the “Part 1 Presentation” of the role of the PRRARSV genome code of the pangolin-CoV MP789 in the lab-creation of the SARS-CoV-2 virus itself is here: www.theqtree.com/2024/11/22/health-friday-11-22-2024-open-thread-lets-talk-about-prrarsv-the-backdoor-key/. Yours Truly presented evidence that: One: the pangolin-CoV MP789 virus genome code has “an uncanny similarity” to the PRRARSV genome code that was inserted into the genome code of the SARS-CoV-2 virus itself; Two: that this insertion occurred during the lab-creation process for the genome code of the SARS-CoV-2 virus itself; Three: that this insertion is at or very near the S1-S2 furin cleavage site in the genome code of the SARS-CoV-2 virus itself; Four: that the bat-coronavirus RaTG13 coronavirus also has a role to play in the lab-creation of the genome code of the SARS-CoV-2 virus itself, although the pangolin-CoV MP789 coronavirus genome code has more “areas of similarity” to the SARS-CoV-2 virus genomecode; and, Five: that taxpayer-funded Gain-of-Function experiments were {most likely] used to perform all of the above, and most likely, at the Wuhan Institute of Virology.
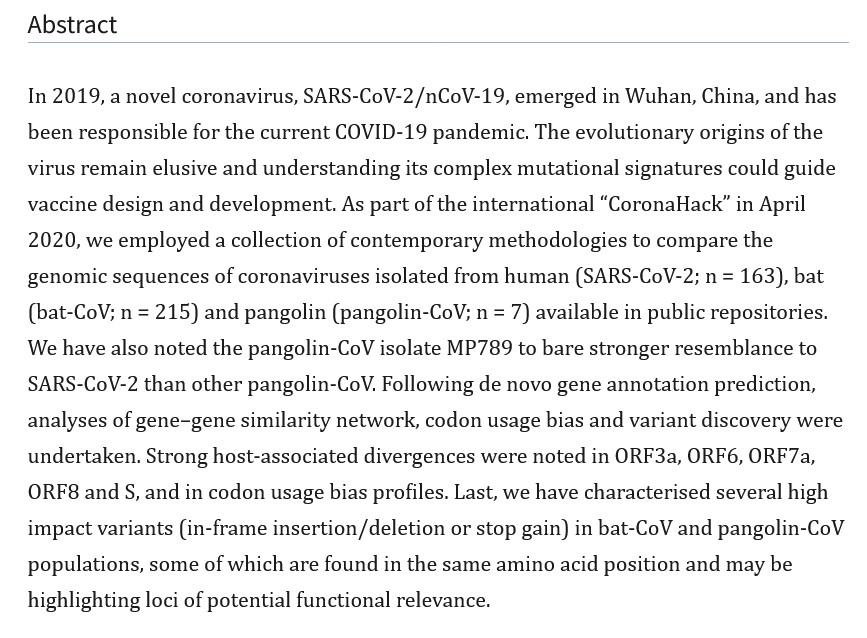
In 2020, the year after the SARS-CoV-2 virus itself was beginning to ravage the world, and when COVID-19 “vaccines” had not yet been granted Emergency Use Authorizations by the FDA in the United States, by the EMA (European Medicines Agency), or by other agencies, a plethora of scientific papers and articles were written and published: papers and articles in which the researchers attempted to pinpoint exactly how the SARS-CoV-2 virus itself came into being. Many of these papers and articles examined the role(s) that various animal coronaviruses may have played in the emergence of the SARS-CoV-2 virus itself: for examples, by “natural evolution”; or, by “recombination” of coronavirus genomes among animals via cross-infection; or, by a “sudden appearance.” These investigations and their published results pre-date the confirmation within the past 18 months that Gain-of-Function experiments at lab facilities, most notably the Wuhan Institute of Virology, were the foundation of the lab-created disaster called the SARS-CoV-2 virus itself (links to Congressional reports on this situation are in the “Part 1 Presentation” Health Friday post, see above.) One such year 2020 scientific paper is the “Dimonaco, et al.” paper: https://pmc.ncbi.nlm.nih.gov/articles/PMC7823979/, “Computational Analysis of SARS-CoV-2 and SARS-Like Coronavirus Diversity in Human, Bat and Pangolin Populations”, Nicholas J. Dimonaco, et al., 30 December 2020. A screenshot of the Abstract of this paper is below:
The Health Friday post cited above discusses Yours Truly’s hypothesis that the pangolin-CoV MP789 coronavirus genome code was chosen, along with the important but actually less-similar bat coronavirus RaTG13 genome code, as the main virus genome that were used to create the SARS-CoV-2 virus itself genome. Today’s post, in Yours Truly’s opinion, presents evidence that “clinches the deal” on the choice of the pangolin-CoV MP789 genome code as the primary one for insertion into the SARS-CoV-2 virus itself genome code — however, the evidence comes from a surprising source.
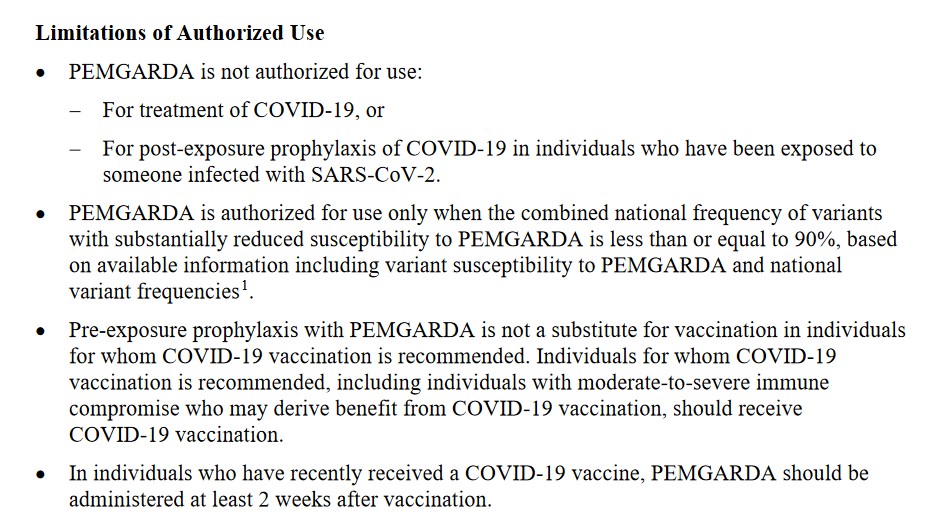
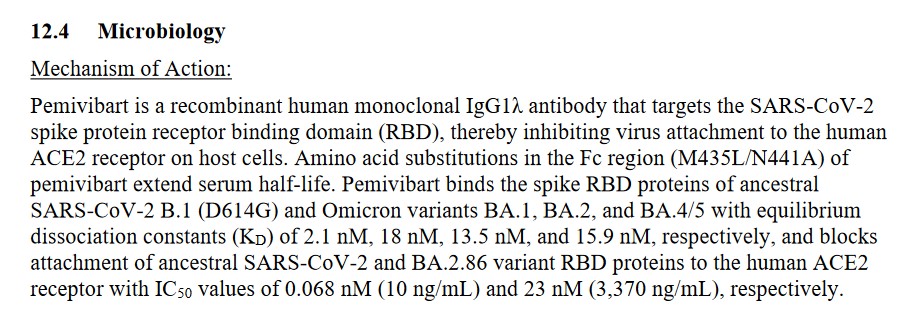
This is the link to the FDA-issued document for healthcare professionals for PEMGARDA: www.fda.gov/media/177067/download (note: PEMGARDA is also called Pemivibart in this document.) There have been no studies performed for PEMGARDA regarding carcinogenicity, mutagenicity, or impairment of fertility (section 13 Nonclinical Toxicology of the FDA document.) Persons who have been prescribed PEMGARDA need to take the infusion (IV) of the drug every 3 months (page 15 of the FDA document.) Also, PEMGARDA is not to be used as a “substitute” for COVID-19 “vaccination” (page 15 of the FDA document.) More details from the section Limitations of Authorized Use of the FDA document are below:
There is a slew of other warnings (including Black Box warnings), cautions, and restrictions regarding PEMGARDA in the FDA document.
Here is a screenshot of section 12.4Mechanism of Action of the FDA document on PEMGARDA (aka Pemivibart):
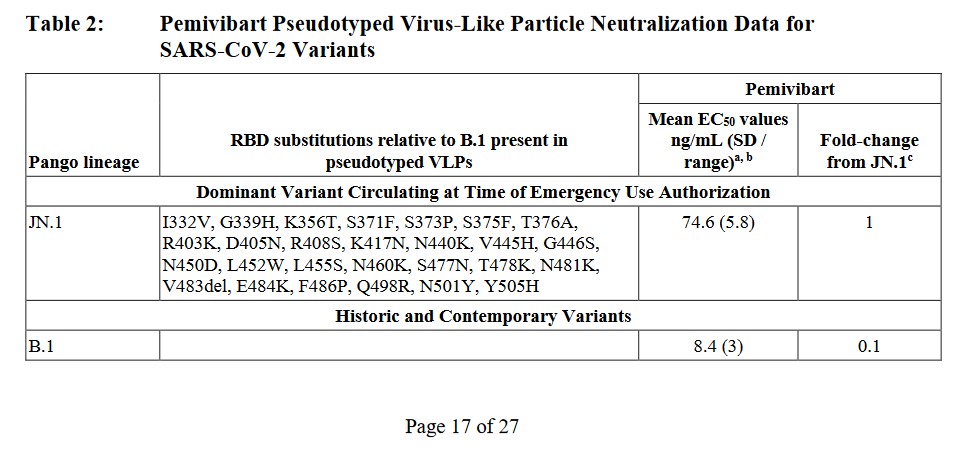
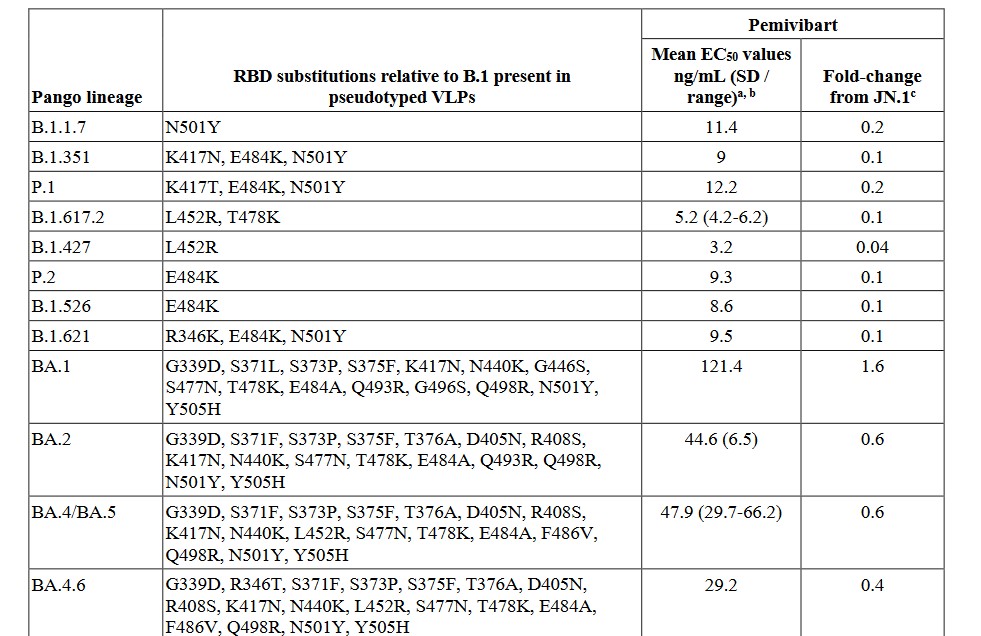
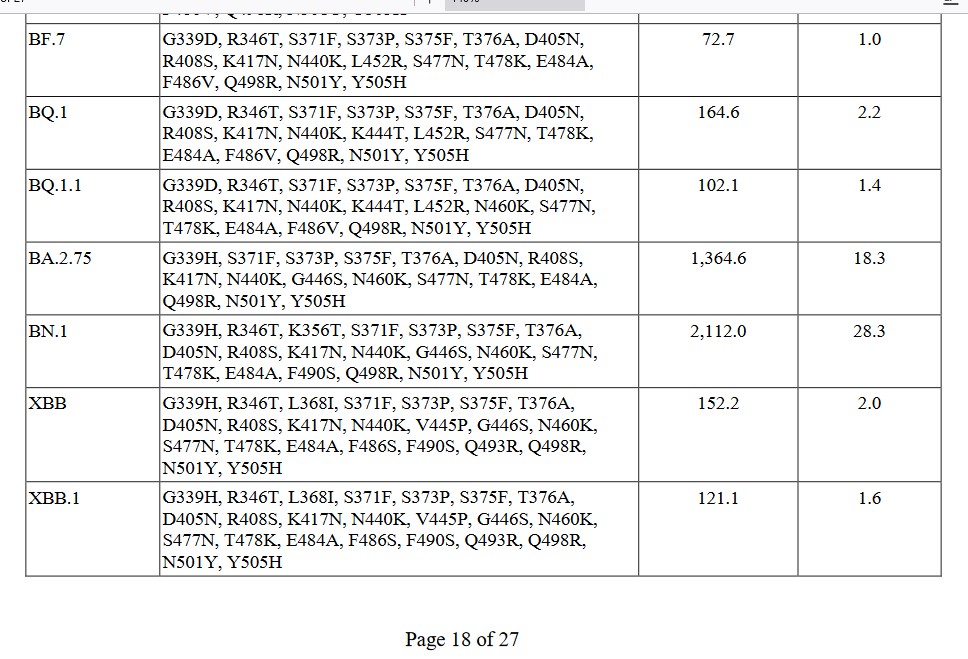
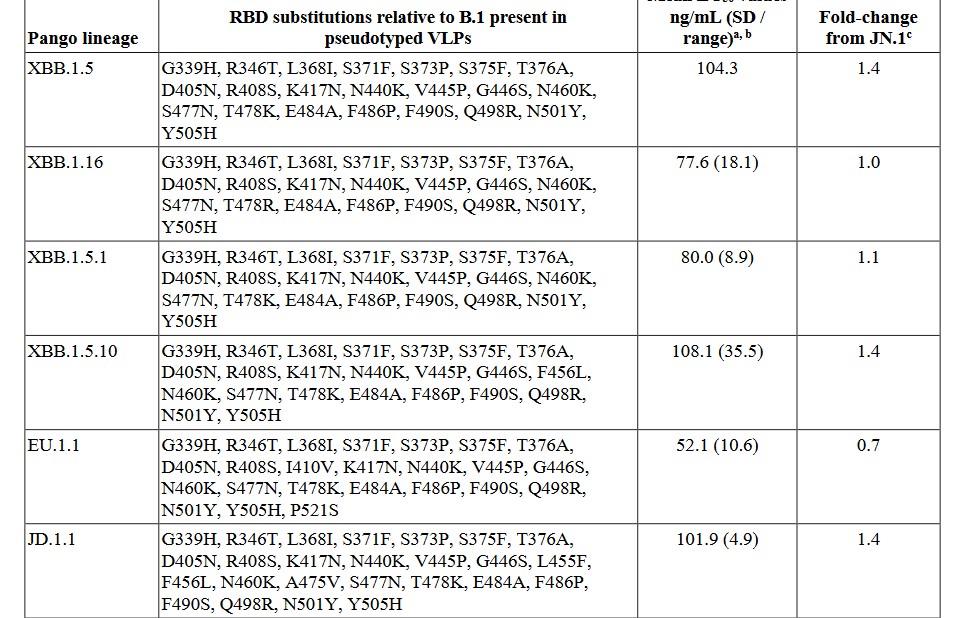
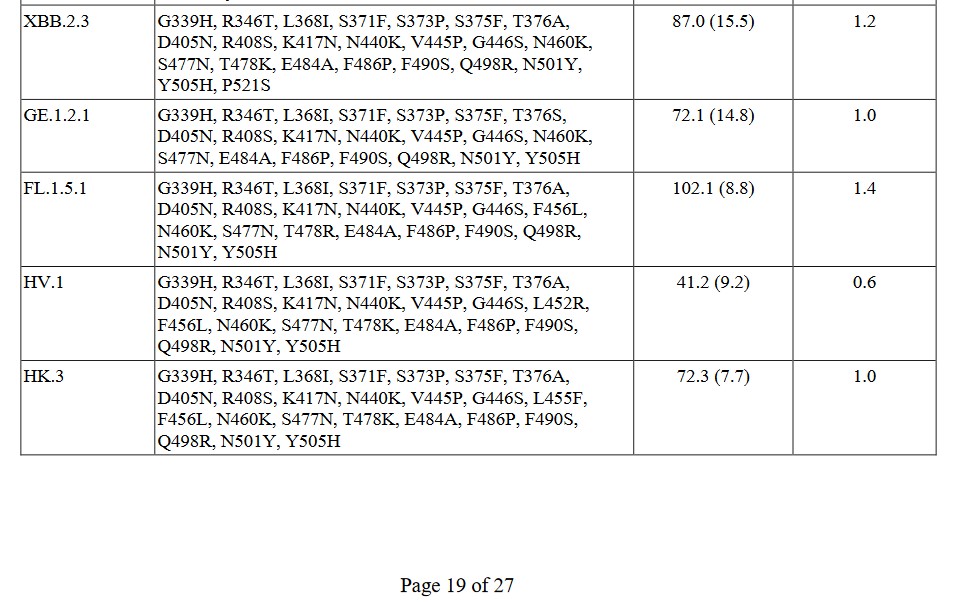
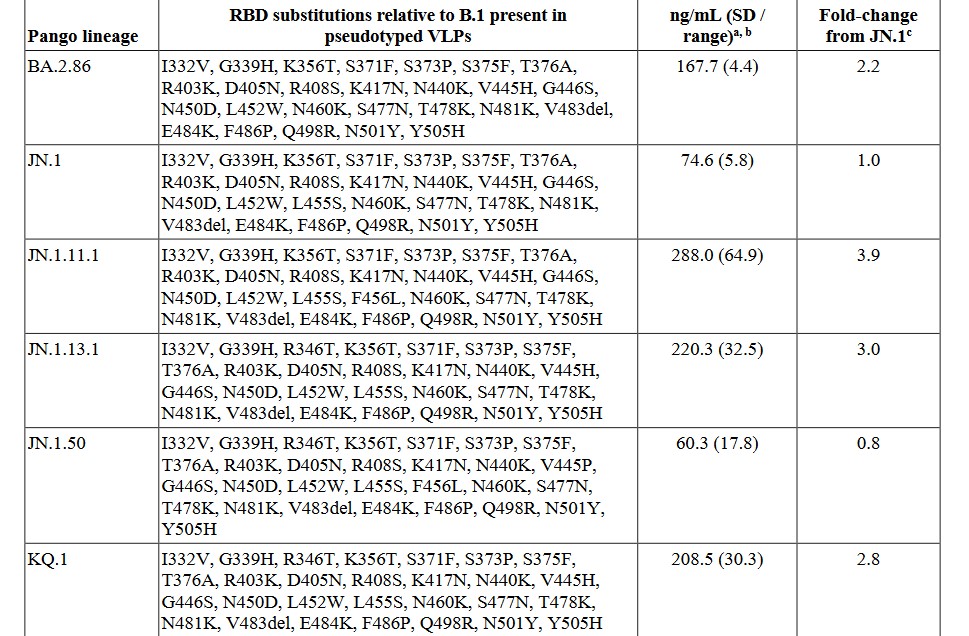
****And now, for the pangolin-CoV connection: This is found in the FDA document on PEMGARDA, Table 2. Yours Truly is including screenshots of Table 2., below. Please look at the screenshots carefully. There are seven screenshots. This is the list of SARS-CoV-2 variants that PEMGARDA is ** allegedly ** supposed to help “guard against.” The bottom line here is: Virtually every SARS-CoV-2 variant is derived from a pangolin-CoV genome code (most likely that of pangolin-CoV MP789) that was “blended in” along with the bat-CoV RaTG13 genome code in the lab-creation of the original SARS-CoV-virus itself. The giveaway is “Pango lineage” at the top of the variants columns. (Note: due to screenshot size constraints, some of the variant lists are broken up: however, EVERY variant column clearly states Pango lineage at the top left.)
The question that comes to mind is: Why is PEMGARDA being promoted as a “pre-exposure prophylaxis” against a COVID-19 infection in immunocompromised persons; or, for that matter, for any person, COVID-19 “vaccinated” or not? The answer is that the FDA still does not recognize, authorize, or recommend, the use of Ivermectin, Hydroxycholorquine, Zinc, Quercetin, Vitamin D, or other “non-FDA-authorized or approved” drugs or treatments for prophylaxis for COVID-19 infection; or for COVID-19 infection treatment. While there may be need for PEMGARDA to be used for certain patients in narrow circumstances, it is Yours Truly’s opinion that it is vastly less expensive and effective to use Ivermectin, Hydroxycholorquine, Zinc, Quercetin, and Vitamin D in the large majority of situations to prevent infection by COVID-19.
Then, there is the issue of what Yours Truly will call “Universal Immune System Compromise from COVID-19 Vaccination.” It is her firm opinion that any person who has ever taken a COVID-19 “vaccine” has a compromised immune system. This is due to the ingredients and the mechanisms of the COVID-19 “vaccines” themselves; in which the critical IgG3 “fight it off” immune system cells of the “vaccinated” person are damaged and/or destroyed, and the growth of IgG4 “tolerate but never clear” cells is increased. This process increases with each successive COVID-19 “vaccine booster” injection (which would include injections of the “latest version” of said “vaccines.”) Please see: https://jessicar.substack.com/p/igg4-cd4s-and-why-the-lnpmrna-platform, “IgG4, CD4s and why the LNP/mRNA platform should be prohibited”, by Jessica Rose, Ph.D., 14 August 2023.
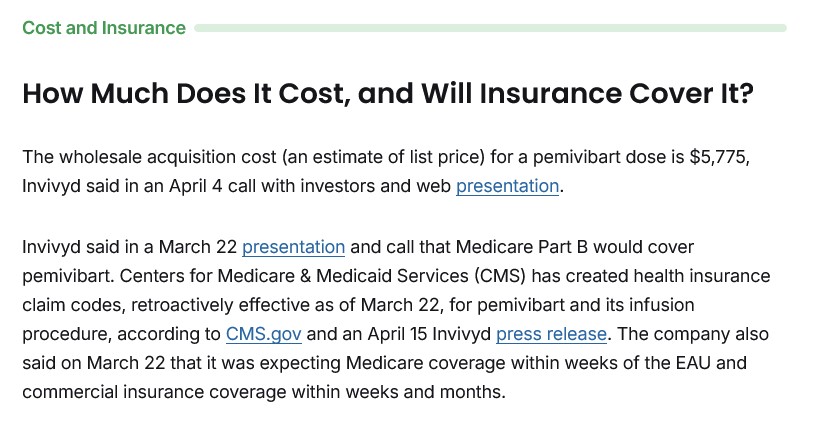
PEMGARDA (aka Pemivibart) is an expensive drug. For example, below is a screenshot from www.patientpower.info/ regarding the cost per treatment for PEMGARDA. This is the non-insurance covered cost:
Recall that the FDA document on PEMGARDA cited above states that persons who are prescribed to take this drug need to repeat the treatment every 3 months.
General Summary: One: Yours Truly presented the first of the hypothesis regarding the use of the pangolin-CoV MP789 in the lab-creation of the original SARS-CoV-2 virus itself (the original Wuhan Hu1 COVID-19 virus itself) in the Health Friday post of 15 November 2024. Two: there is a large amount of scientific papers and articles published in 2020, with researchers investigating various hypotheses regarding a “combination” of animal coronaviruses in nature that produced the original SARS-CoV-2 virus itself. This research was performed prior to the confirmation that the SARS-CoV-2 virus itself was the product of Gain-of-Function lab-creation, most likely at the Wuhan Institute of Virology, using coronaviruses from various animals, including the bat-CoV RaTG13 and the pangolin-CoV MP789. Four: the pangolin-CoV MP789 virus genome has the “closest overall match similarity” to the genome of the SARS-CoV-2 virus itself. Five: there is a new FDA “pre-exposure prophylaxis and antiviral” drug, PEMGARDA, that is administered by infusion (IV) only, and only for certain types of immunocompromised persons. Six: the FDA-issued Fact Sheet for PEMGARDA clearly shows, in Table 2. of the document, that the SARS-CoV-2 variants that PEMGARDA is to “guard against” are virtually all derived from what the document states is “Pango lineage.” Seven: the FDA still does not recognize, authorize, or approve, of the use of Ivermectin, Hydroxycholorquine, and other effective alternatives for COVID-19 infection prevention or treatment.
A Simple but Nagging Question Brought to Us by RFK Jr., “Sudden Death”, Unnaturally Red Salmon, and My Dearly Beloved Cheese Balls
I must begin this discussion by admitting that I’m very pro-freedom – and that includes the freedom to conduct honest business without government intervention – which intervention would include taxes. In fact, I have tended, over my lifetime, to scoff at people who want to restrict business over what I generally regard as unfounded allegations of harm.
Thus, I approached the following video, and its enclosing article, with some skepticism. Please read and watch, if you have not already.
Cory Booker? Do they mean, lying, hoaxing, finger-wagging Marxist Cory Booker?
Cory Booker, ally of the Maoist Obama minion Kamala Harris, and assisting perpetrator of the Jussie Smollett lynching hoax?
(No, Michelle Obama and Jussie Smollett didn’t really say that when they were laughing. This is called a “meme”. It’s a form of propaganda and satire. In this case, it is responding to propaganda, fraud, and deception perpetrated by Jussie Smollett, Kamala Harris, and Cory Booker.)
THAT Cory Booker?
So what video would HE promote? More hoaxes and lies?
Let’s take a look. But color me skeptical.
OK – there is a lot to unpack here. This will take a while.
Some background. I am both a scientist, and a lover of the history of science. Far too many scientists are NOT lovers of the history of science, because if they were, they would realize how bad scientists are at spotting the wrongness of contemporaneous science. Which is ALL THE TIME.
And, that would include me. Thankfully, I have often discovered my own wrongness in science within my own lifetime. We’ll get to that, as we move along here.
Now the first thing that irritated me about this video, is the way coal tar is used as a lead-in to attack a food dye called tartrazine, a.k.a. Yellow Number Five.
It almost sounds like Robert F. Kennedy Jr. (RFKJ hereafter) is saying that tartrazine is obtained by draining it out of coal – or if not that, out of “coal tar”, which is somehow gotten out of coal.
Just a side point. Coal tar is a very useful substance, which is actually used as a medicine for treating skin problems.
So – just from the start, it’s not totally justified to demonize coal tar. Yet on the other hand, YES, thank you – hold the coal tar on my deli sandwich, please. It IS medicine, and can even cause cancer.
But FULL STOP. Back to the point. Tartrazine is not exactly “made from coal tar”. It is made from “organic” (carbon-containing) chemicals – basic organic chemicals – that can be made in a variety of ways, from a variety of things, including coal, petroleum, natural gas, biowaste, corn, soybeans, CO2 in the air, apples, healthy fruit – WHATEVER.
See what I’m saying? Tartrazine is being demonized by association. I was ready to bitchslap RFKJ here. Bear in mind that, years ago – before the COVID nightmare and revelations after that – I considered him a NUT – and would often say as much.
AND YET. If you know the history of science and organic chemistry, RFKJ has a point. A very valid point – in that association.
RJKJ clarifies in the video (3 min 6 sec) that tartrazine is now made almost entirely from chemicals which now come from petroleum – not coal tar. However, that original time period – the coal tar days – has something to teach us.
The discovery of synthetic dyes like tartrazine was back when mankind was in a state of “chemical hubris” not unlike the “biological hubris” of current times.
In the same way that we now look back and face-palm at the “irrational exuberance” of early organic and medicinal chemistry, which gave us the hormonal poison diethylstilbestrol (DES), injected into millions of pregnant women before we realized that it damaged their daughters, so we will one day look back at the “clot shot” – marveling at the combination of ignorance (most people), hubris (most scientists), and – behind layers of global governmental denial – malevolent or warped benevolent depopulation do-gooderism (top-secret scientists and psychopathic power players), that pushed bad experimental vaccines on an almost unsuspecting but increasingly skeptical public.
Once I was in the state of seeing the historical analogy, I was ready to realize that there is almost no excuse for allowing anything into food that is not food or a known nutrient.
If one asks WHY Yellow Number Five is in those wonderful-tasting but unnaturally yellow cheese balls, it is obvious – the chemical makes the cheese balls look “cheesier” in a weird but highly unnatural way. It’s psychological. It’s an “allowed psy-op” by makers of food.
Or take salmon. The last time I looked at a really good deal on salmon in the grocery store, I noticed that it was just a bit too strangely orange. Reading the label, there was an admission that the salmon “might” be treated with some dyes to keep it looking attractive.
Suddenly, the salmon didn’t look quite as good to me. It still looked reasonable, and I toyed with the idea of buying it. But I didn’t. In this post-mRNA world, I elected to put off a buy until I could do more research.
So now, after watching this video, I realize that RFKJ is correct. Dyes make foods more appealing, but they do so in a very deceptive way. To me, if dyes have ANY risks, putting them in food makes almost no sense, other than we are allowing “deception in the quality of food” as a kind of freedom. Well, murdering people, stealing their things, and doing other bad things to them are “freedoms” we used to have as humans – and we did away with those freedoms, while keeping most of the rest.
And yet, the enjoyment of food is right there in the Declaration of Independence.
Because I believe in freedom, including the pursuit of happiness in cheese balls and salmon, I don’t want to tell you what to believe, but I will tell you what I believe.
Some people may want vaccines with side effects and risks. I personally don’t, but I want those people to be free to have their vaccines – but not force them on me or my children. And I want the TRUTH about those vaccines to be KNOWN. Not just a little known – A LOT KNOWN.
Some people may want unnaturally yellow cheese balls. I certainly don’t – not any more. I would like some nice, corn-and-cheese-looking cheese balls that I know are healthy for me. But other people may want the yellow cheese balls with strange dyes. Is there a way that we BOTH can be happy? As the founding fathers wanted?
I would like to see more foods without risky, unnatural additives. I would like to see TRUTH IN FOOD and TRUTH IN DRUGS.
I think there is a way forward that will make America HEALTHIER, FREER, and TRUER.
But we have to be honest, if we want to get there.
And what do you know – there are now some people who believe in honesty! And they’re going to be in office, if we continue to support them!
The above is a vintage image of Dr. Edward Jenner administering the first smallpox vaccination (inoculation) to James Phipps, 14 May 1796. Courtesy of www.sciencemuseum.org.uk/.
Today’s post, as it relates to the disaster of COVID-19 and the COVID-19 “vaccines”, is dedicated by Yours Truly in memory of her cousin Bill, who died “suddenly and unexpectedly” in September 2023. However, the discussion is not limited to what is presented here: it is an Open Thread.
There are two separate, although connected (Big Pharma), parts to today’s offering. Each part is of itself an expose’. This post is a long one, but important. Please, take a cup of coffee or tea; or, if it’s an appropriate time of the day, perhaps a “wee dram” of something like chilled D.O.M. Benedictine with a twist of lemon peel, and settle in for reading.
Readers already know the caveats regarding civil discussion on this board; of the alternate sites in case the main board is not accessible (here and here); and, that what Yours Truly presents on Health Friday is not medical advice, but opinions and/or hypotheses from ongoing research on COVID-19, Big Pharma, and other health topics.
“Quick, down-and-dirty summary” of today’s post:
One: Pfizer-BioNTech has begun a new enterprise, PfrizerForAllTM, which apparently seeks to completely circumvent / marginalize, in-person consumer contact with pharmacies; to “funnel” in-person consumer contact with healthcare practitioners to “Pfizer-affiliated” professionals; and, to “redirect” the dissemination of information about the COVID-19 “vaccines” to that provided by Pfizer-BioNTech.
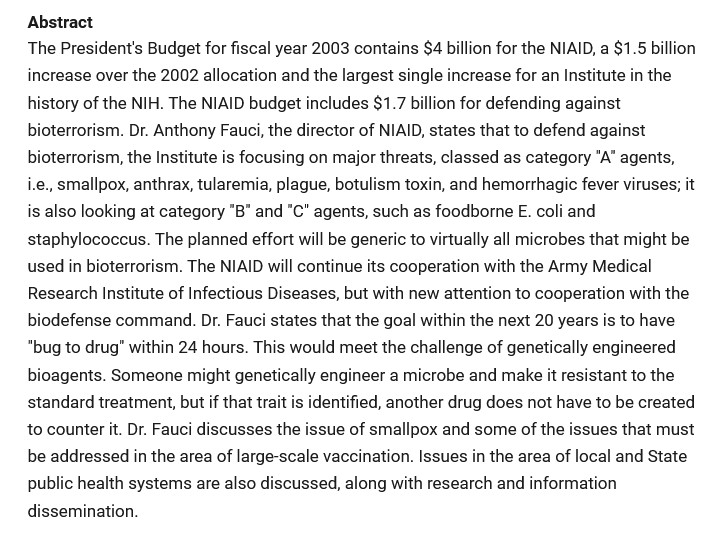
Two: That the FDA approval of the very dangerous and deadly Smallpox “vaccine”, ACAM2000, for use also as a “prevention” for Mpox, is the result of a complex mixture of Big Pharma influence + FDA review of the Biologics License Applicaion for this use of ACAM2000 that is, in Yours Truly’s opinion, “a foregone conclusion despite serious reservations”, to say the least + Gain-of-Function experiments on the Mpox virus. There is also a potential tie-in to “an expanded biodefense role.”
Yours Truly has tried to avoid making today’s post read like a scientific paper; however, there is a lot of information that is relevant to each Expose’. Note: Mpox is now the “official” name for monkeypox.
Expose’ One: It appears that Pfizer-BioNTech is creating new ways to increase the company’s consumer operations (and, therefore, potential profit lines.) Pfizer-BioNTech has just launched PfizerForAllTM — a direct sell-to-consumer business that will provide online access to healthcare providers (online [virtual], or affiliated healthcare providers encounters [for example, to get a COVID-19 “vaccination”]); plus, “delivered to your door” prescription drugs and “easier access” to other company products, such as their COVID-19 “test kits.”
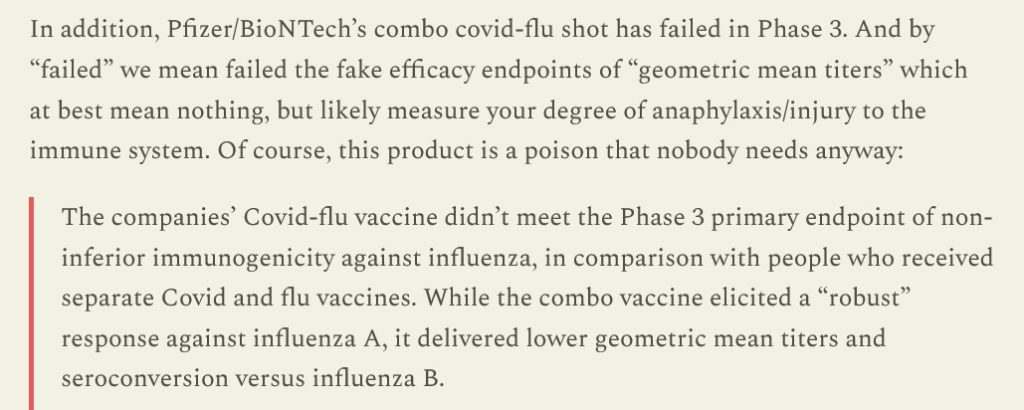
In other words, in Yours Truly’s opinion, Pfizer-BioNTech, not happy with the company’s portfolio loss due to falling consumer acceptance of the modRNA COVID-19 “vaccines” offered, and due to the failure of the company’s clinical trial of its “combo” modRNA COVID-19 “vaccine” + influenza “vaccine”, a corporate decision was made to find a way to go straight to the consumer and make it “so easy” to get access to the “vaccines”, plus other Pfizer products. Translation: banish “vaccine” hesitancy / “vaccine” refusal, by doing what may be called “straight to the consumer medical psy-op.” Again, from the Latypova article:
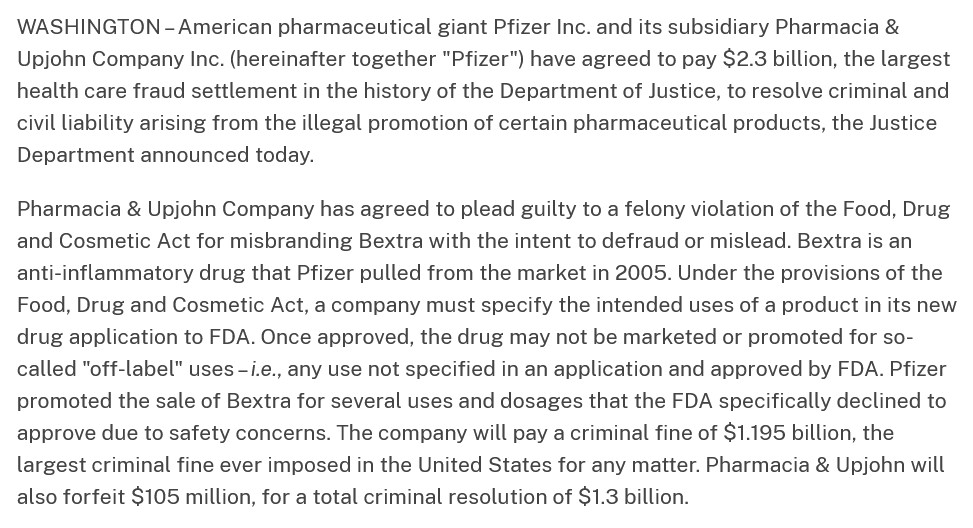
The lawsuit that Pfizer-BioNTech settled in 2009 was over the use of the company’s drug, Bextra, in “off-label” situations. The scope of the settlement is described here: www.justice.gov/, “Justice Department Announces Largest Health Care Fraud Settlement in Its History”, 1 November 2023. A portion of the announcement is below:
This lawsuit was the starting point for FDA changes to its “regulations” regarding the use of prescription drugs in “off-label” situations. The latest FDA changes are summarized here: www.sidley.com/en/insights/newsupdates/2023/11/fda-s-latest-off-label-guidance, 1 November 2023. It appears, in a nutshell, that drug manufacturers can be held responsible (liable) for “off-label” use of their products, even if they already comply with the “new” FDA “regulations.” (Think of this in light of the use of, for example, Ivermectin or Hydroxychloroquine to prevent or to treat COVID-19 — these uses, arguably, are “off-label” for these drugs.)
By the way, PfizerForAllTM is working with UpScript Health and Alto Pharmacy regarding access to healthcare services and filling prescriptions. Guess what? UpScript Health lists Pfizer as a “partner” on the company’s “About” page of their website: www.upscripthealth.com/about/. And, there’s more — Alto Pharmacy, the online prescription drug company, has a couple of interesting members on their Board of Advisors: Alex Azar (HHS head under then-President Trump); and, Dr. Ezekiel Emanuel (he who helped to write the “ObamaCare” bill; he who advocated for people to take their own lives at age 75 “to make room for the younger generation”, and more): www.alto.com/our-company. Dr. Emanuel is also involved with the Center for American Progress (Soros-connected: www.americanprogress.org/c3-our-supporters/); The Aspen Institute; and, he is Co-Director of the Healthcare Transformation Institute (HTI) at the University of Pennsylvania. Below is the Mission statement of HTI (https://hti.upenn.edu/mission/):
Note 1: the “objective” to transform the behavior of physicians and other healthcare providers. (Italics, mine.) Note 2: the “imagifashion” hyperlink, apparently, after getting past the “fake Latin language” on the main page, takes one to a clothing/accessories company in California: https://nilah.la-studioweb.com/contact-us/. (??)
This statement really frosts Yours Truly. My late father was a Registered Pharmacist for 57 years, who: kept his pharmacy very clean and neat (one was part of the crew that swept the floors and cleaned the display shelves starting when she was 10 years old); made it a point to know about all of his patients and to TALK with with then they came to have prescriptions filled or refilled; worked out deals with his suppliers to get extra samples of OTC products to give to his patients who had lost their steel mill jobs when the mills left Pittsburgh in the late 1970s-early 1980s, and, who paid for their prescriptions with his own money at times, etc., — finds the language, “…brick-and-mortar terrible experience…” in the above statement not only to be personally insulting to the memory of her father: but, also, degrading to those “brick-and-mortar” pharmacists who do their job to keep their stores clean and organized.
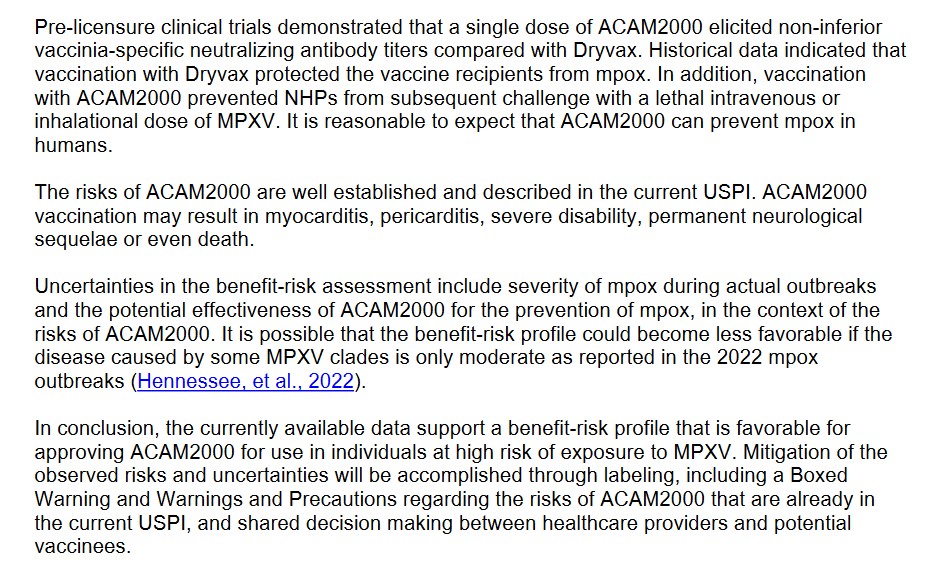
Expose’ Two: This regards the FDA just “approving” the “expanded use” of the dangerousand deadly Smallpox “vaccine”, ACAM2000, for the “prevention” of Monkeypox (now called “Mpox.”) The FDA issued this “approval” on 29 August 2024. The trail on this begins here: https://mole.substack.com/p/acam2000-package-insert-warning-death, 14 September 2024.
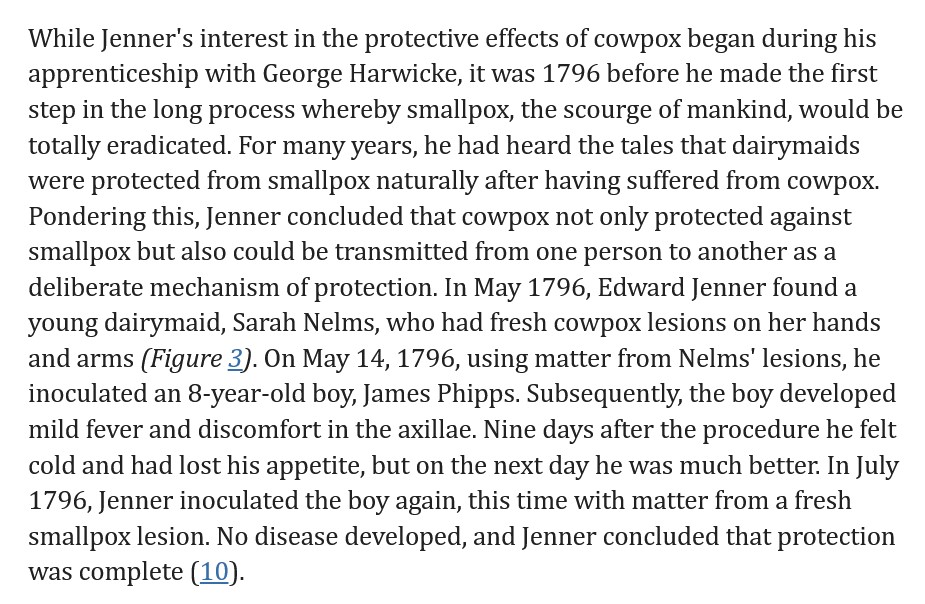
To gain more understanding of Smallpox and inoculation / vaccination against Smallpox, please see: www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination. Both Smallpox (variola) and Mpox (mpox virus) are members of the genus Orthopoxvirus. Whereas, a disease condition that would equate to Smallpox goes at least as far back as to China around 3000BC, Mpox was first discovered in 1958 (all, per Wikipedia search.) Dr. Edward Jenner, an English physician, noticed that milkmaids were immune from Smallpox infection; he deduced that the Cowpox infections that they sustained had made them immune to the other type of infection. Dr. Jenner administered the first “inoculation” of Cowpox virus (to prevent Smallpox) to a child, James Phipps, on 14 May 1796. Another source of information is here: wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/smallpox-and-other-orthopoxvirus-associated-infections. Further details are found here, in the article, Edward Jenner and the history of smallpox and vaccination, January 2005. A screenshot of a portion of this article is below:
About ACAM2000: it is manufactured by Emergent BioSolutions, headquartered in Gaithersburg, MD. The FDA approved ACAM2000 for use for the prevention of Smallpox in August, 2007. It contains vaccinia, a live virus ingredient used in modern Smallpox vaccines. The vaccinia used in ACAM2000 is a replicating version. The vaccine is cultured in a mixture of African Green Monkey kidney cells (sound familiar? — as in, perhaps, SV40 African Green Monkey cancer promoter gene splice that was found in the Pfizer-BioNTech modRNA COVID-19 “vaccine” by Dr. Kevin McKernan?). ACAM2000 was originally only intended for use to prevent Smallpox — until its use was “suddenly expanded” on 29 August 2024 by the FDA to include prevention of Mpox (more on that later in the post.) Since then, articles such as this one have appeared (https://childrenshealthdefense.org/defender/fda-acam2000-mpox-vaccine-warning-death-unvaccinated/, 17 September 2024, by Suzanne Burdick, Ph.D.; and, social media has been posting items like this one: https://x.com/toastontheside/status/1835921932841062412. This tweet references the FDA-issued handout for patients and/or caregivers regarding ACAM2000. The FDA handout is found here: www.fda.gov/media/75800/download. FDA handout documents for patients and/or caregivers are likely to have, in Yours Truly’s opinion, “sanitized” information and “pablum-like” assurances regarding the “safety and efficacy” of the drug or injectable. The FDA handout for ACAM2000, however, is different: when one reads the handout, one gets a distinct impression that this “vaccine” is highly dangerous. Below is a screenshot portion of the FDA patient/caregiver handout for ACAM2000:
Note that there is NO MENTION of the other FDA-approved Mpox vaccine, JYNNEOS, which is arguably “safer” for the patient (see further down in the presentation regarding JYNNEOS.)
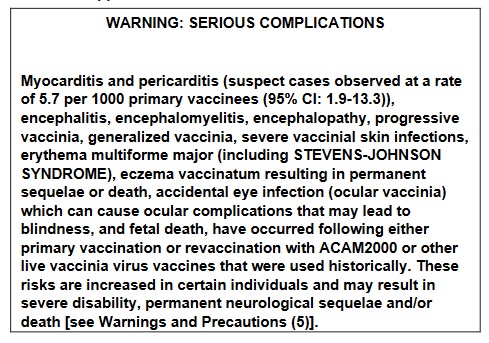
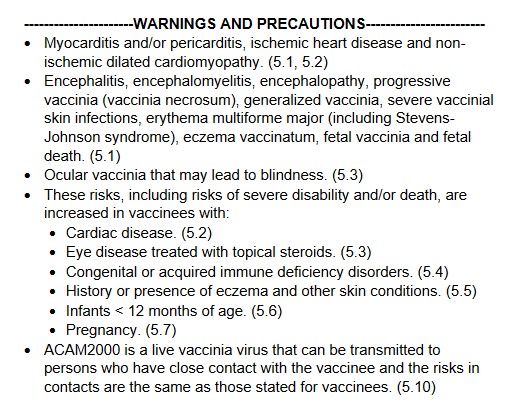
The Fact Sheet for Healthcare Providers for ACAM2000 is here: www.fda.gov/media/75792/download. The document gives a much more comprehensive picture of the dangers of this “vaccine.” Yours Truly will highlight a few of the items in this document which show how dangerous and deadly this vaccine is, beginning with two images from page 1 of the Fact Sheet: the Black Box Warning; and, the Warnings and Precautions:
Remember, this dangerous and deadly “vaccine” is now approved for persons “at risk for Mpox”, in addition to persons at risk for Smallpox (this disease was eradicated in 1980.)
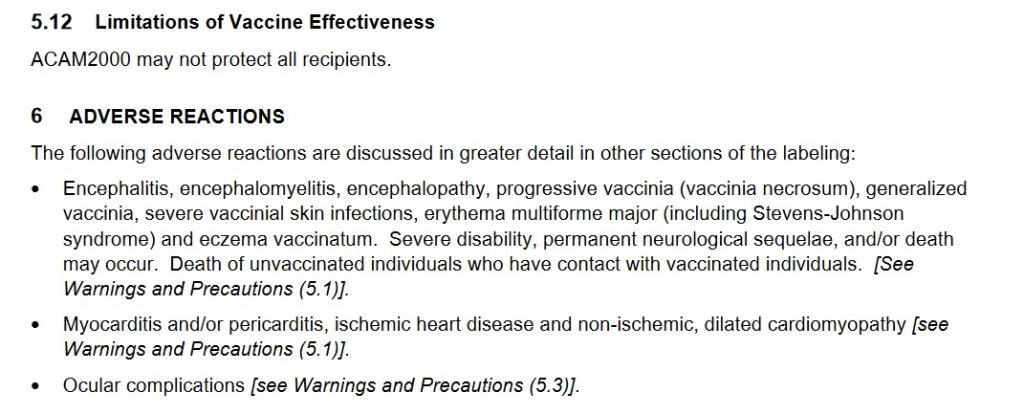
And, from Section 6 Adverse Reactions portion of the Fact Sheet for ACAM2000:
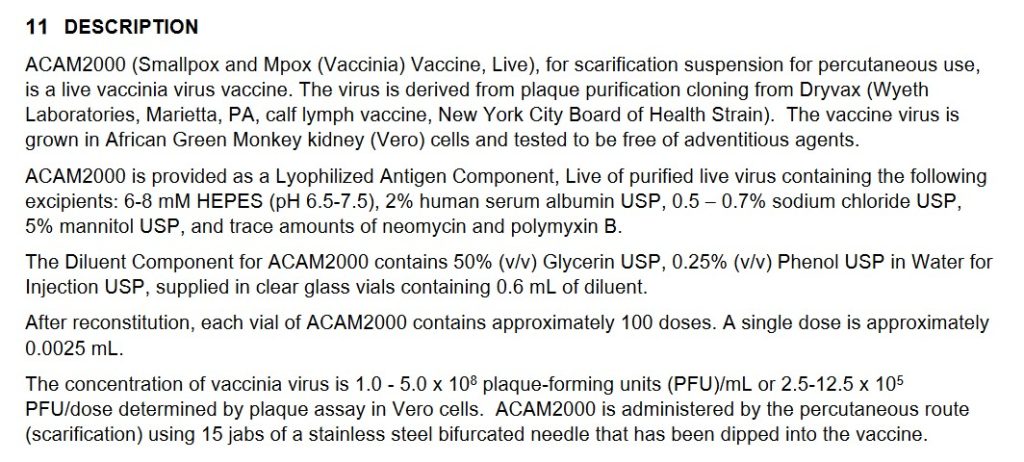
Continuing with Section 11 Description from the Fact Sheet for ACAM2000:
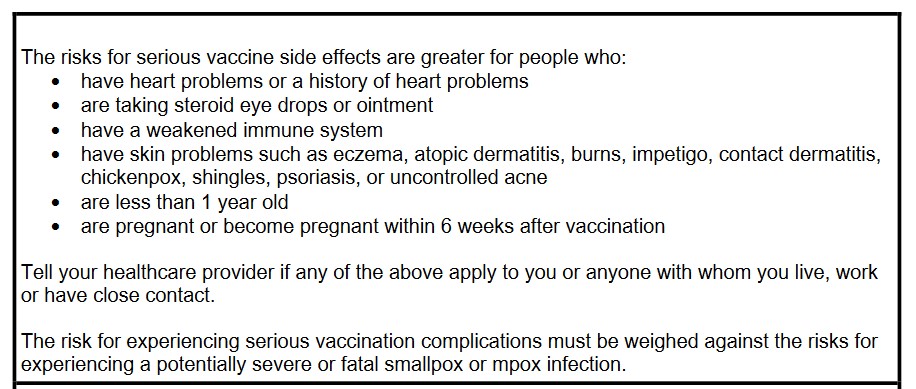
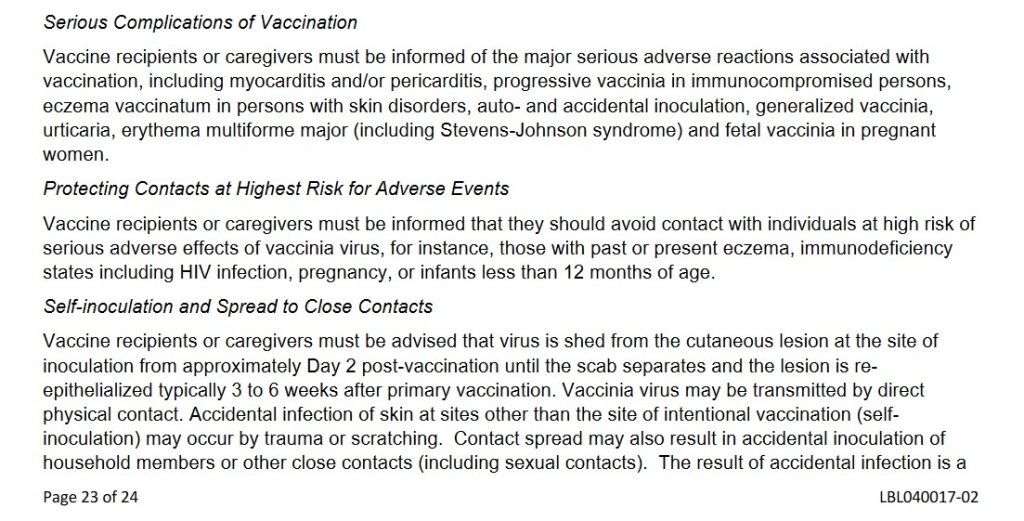
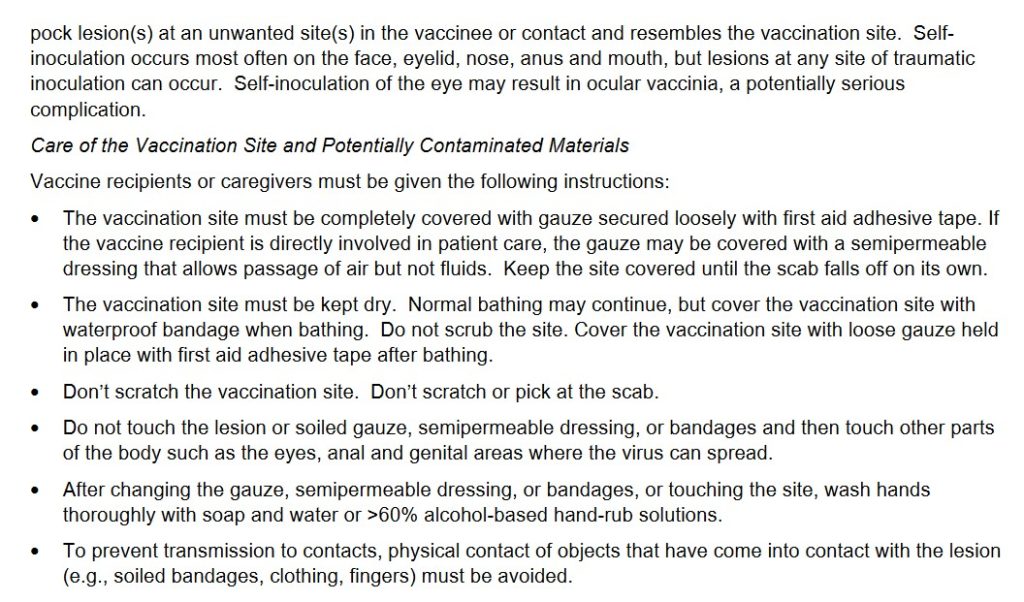
And, from Section 17 Patient Counseling Information of the Fact Sheet for ACAM2000, two portions:
Note several items from the above screenshots: One, that the “vaccine” must be given to the recipient via 15 separate jabs with a bifurcated needle; Two, there are MULTIPLE adverse reactions potential for persons taking this “vaccine”; Three, that persons who contract a Smallpox infection from a person “vaccinated” with ACAM2000 can die of the infection they contract; Four, that the ACAM2000-“vaccinated” person must stay away from pregnant women, household members, persons with eczema, etc., for a period of time after “vaccination”; among many other issues.
Yours Truly will again recall to the reader’s mind that ACAM2000 is now FDA-approved for PREVENTIVE USE among persons who are at risk for Mpox. From what Yours Truly has read about it, Mpox is, for all intents and purposes, likely to be a LESS-DANGEROUS form of Orthopoxvirus, compared to another form of the same Genus, variola (Smallpox virus.) [HOWEVER, see the presentation answering Question Two, further below in the post.] There is a vaccine that was previously FDA-APPROVED for the prevention of Mpox — JYNNEOS, manufactured by Bavarian-Nordic. This vaccine also uses the vaccinia virus as the foundation; but, JYNNEOS is cultured in a mixture of chicken embryo cells; and, although it also has live vaccinia, it is a NON-replicatingversion. JYNNEOS was also originally FDA-approved for the prevention of Smallpox. In Yours Truly’s opinion, even though JYNNEOS does indeed have potential for serious adverse reactions (for example, cardiac issues), this vaccine appears to be much less dangerous and deadly compared to ACAM2000. The FDA Fact Sheet for Healthcare Providers for JYNNEOS is here:www.fda.gov/131078/download.
Two questions arise immediately: First, what is about ACAM2000 that makes it so dangerous?; and, Second, why did the FDA suddenly approve the use of ACAM2000 for the prevention of Mpox in August 2024?
As to the first question: ACAM2000 is the “descendant Smallpox vaccine” from the older Dryvax Smallpox vaccine, which was manufactured by Wyeth. ACAM2000 replaced Dryvax in August 2007, after FDA approval. The Package Insert (archived version) for Dryvax is here: https://biotech.law.lsu.edu/blaw/bt/smallpox/dryvax_label.htm. Below are two screenshots from the Package Insert for Dryvax:
Note that the inoculation process for Dryvax consisted of 2 or 3 punctures for the initial (primary) vaccination; and that 15 punctures were used for revaccination. However, ACAM2000 requires 15 punctures for the initial vaccination. Why 15 punctures for the initial vaccination? It would appear, in Yours Truly’s opinion, that requiring 15 punctures for the initial vaccination with ACAM2000 exposes the patient to more of the ingredients of the vaccine (think the Moderna COVID-19 modRNA “vaccines”all having more than 3 times the “mcg payload” of lab-enhanced SARS-CoV-2 spike protein PER INJECTION, as compared to the “mcg payload” of the Pfizer-BioNTech modRNA COVID-19 “vaccines.” [Which is NOT to say that the Pfizer-BioNTech modRNA “vaccines” are somehow “safer” than those of Moderna. THEY ARE NOT.])
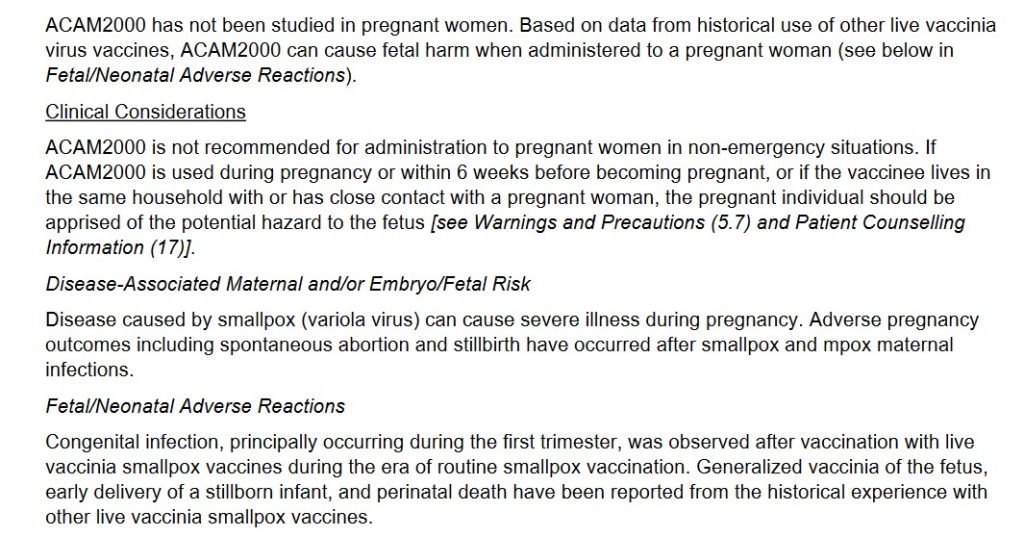
Yours Truly turns to section 8.1 of the FDA Fact Sheet for Healthcare Providers for ACAM2000 (link above.) This “vaccine” is particularly dangerous to pregnant women, to women who wish to become pregnant, and to a fetus carried by a pregnant woman (whether or not she is “vaccinated” with ACAM2000, since persons “vaccinated” with this product will “shed” ingredients [from the forming / formed pustule, or the scab from the pustule, etc.], onto other persons who come into contact with the “vaccinated” person.) Below is section 8.1:
It would also appear that there is inherent danger due to the fact that ACAM2000 uses a live, replicating vaccinia (another Orthopoxvirus that is “weaker” than variola [the Smallpox virus], and which is used to make modern-day Smallpox / Mpox vaccines), as compared to the live, NON-replicating vaccinia that is used the JYNNEOS Smallpox / Mpox vaccine. Once inoculated (vaccinated) with ACAM2000, the vaccinia produces a kind of “mini-infection” in the patient, affecting the area around the inoculation site, along with the lymph nodes in the same area. Vaccinia may also appear in the blood of the patient. There is also the issue of “self-inoculation” by the ACAM2000-“vaccinated” patient (from scratching or “picking at” the scab that forms after the “mini-infection” pustule forms on the skin, and also when this pustule begins to clear); and for other reasons — the FDA Fact Sheet section 17 Patient Counseling Information for ACAM2000 discusses this. In addition, there is the varying amount of vaccinia concentration that is produced in the patient after ACAM2000 inoculation; see below from section 11 Description of the FDA Fact Sheet for Healthcare Providers:
In other words, there are many areas about the ingredients and mechanisms of ACAM2000 that raise the risk of complications, including death, for the patient who takes this “vaccine”, for pregnant women and their fetuses, for women who wish to become pregnant, for persons who are immunocompromised, and for persons who are NOT “vaccinated” with ACAM2000, during the multiple “danger zone” weeks after ACAM2000 inoculation.
Turning to the second question, concerning the FDA approval in August 2024 for ACAM2000 to be used as an Mpox “vaccine”: this situation is complex. It involves Big Pharma, the WHO, and, what to Yours Truly “smells like” Gain-of-Function research, among other items.
Yours Truly will begin with Emergent BioSolutions, the company that produces ACAM2000. Emergent BioSolutions, a “global enterprise” with headquarters in Gaithersburg, MD, was established in 1998. Its first project was to partner with the United States Defense Department to supply the Anthrax vaccine that was administered to members of the military (www.emergentbiosolutions.com/about-us/.) The current CEO of the company is Joseph C. Papa. Mr. Papa’s most-recent position was CEO of Bausch + Lomb, another large Big Pharma company. Mr. Papa, apparently, is a “mover and shaker” in the pharmaceutical industry. However, it is also apparent that Baush + Lomb was in financial trouble when he left it to become CEO of Emergent BioSolutions. In fact, Bausch + Lomb is “exploring” selling off some of its pharmaceutical assets, due to “significant debt load” (https://finance.yahoo.com/news/bausch-lomb-explores-sale-amid-112230409.html.) Perhaps, the company’s Post-IPO debt funding was not enough: www.crunchbase.com/organization/bausch-lomb/company_financials; scroll down to “Investors.” Mr. Papa has Bachelor’s and Doctorate degrees in Pharmacy; his career includes working with many Big Pharma companies (Novartis, Cardinal Health, and Watson Pharmaceuticals, among others.) Please see his entry in Wikipedia; and, here: https://waterstreet.com/people/papa-joseph. Water Street (Water Street Healthcare Partners) is an investment company that has a portfolio worth approximately $6Billion spread across healthcare services companies, medical diagnostics companies, and pharmaceutical/life sciences companies (https://waterstreet.com/companies.)
Mr. Papa was hired on 21 February 2024 by Emergent BioSolutions to facilitate the financial turnaround of the company. Below is a screenshot of the company’s financials from September 2023 to September 2024, via Crunchbase. It appears that Mr. Papa, a “mover and shaker” in the Big Pharma world, is working hard:
Also, via Crunchbase, a snapshot of Emergent BioSolution’s funders:
It appears that now, Mpox is being “re-classified” as another, although serious, sexually-transmitted disease that can infect any sexually-active person; and, that Mpox has apparently “made the leap” from monkeys to other animals (rodents and even to domesticated dogs), and to between animals and humans. This leads to another aspect of the situation: Yours Truly’s suspicion that there have been / are ongoing, Gain-of-Function experiments on Mpox.
Here is the “fast and dirty” summary on Gain-of-Function experiments with Mpox:
One: Up until 22 August 2024, the FDA had only ONE approved “vaccine” for Mpox: JYNNEOS. However, on that same day, the FDA conducted a “review” of the BLA Application (Biologics License Application) for ACAM2000 to have approval as a “vaccine” for Mpox. This application was approved on 29 August 2024 (www.fda.gov/news-events/press-announcements/fda-roundup-august-30-2024.) Please see: www.fda.gov/media/181552/download for the BLA review. The FDA reviewers, apparently, had some “reservations” about ACAM2000 — see the screenshot below:
Despite the multiple reviewer comments regarding the BLA for ACAM2000, the FDA approved it anyway for Mpox “prevention.” In fact, look at THIS, from section 11.2 of the ACAM2000 BLA document, below:
Two, the Gain-of-Function issue regarding Mpox: First, the CDC connection:
The CDC has an updated report on the incidence of Clade II infections of Mpox, an outbreak that originated in Central Africa (more on Clade II of Mpox further down in today’s post): www.cdc.gov/, “Clade II Mpox Outbreak Originating in Central Africa”, 13 September 2024. Per this article, there are no Clade I Mpox infections in the United States at this time; however, there are 2466 reported cases of Clade II Mpox infections, with 7 deaths. There are also, per the CDC report, cases of Clade II of Mpox literally all over the world at this time.
Here is an example of Gain-of-Function experiments with the Clade II of Mpox. This paper is about a study conducted at Kansas State University in which pigs were exposed to the Clade II of Mpox to see if they would get sick, and then take various blood and biological samples and test them. Sure enough, the pigs contracted Mpox. Please see: www.ncbi.nlm.nih.gov/pmc/articles/PMC11168330/, “Experimental inoculation of pigs with monkeypox virus results in productive infection and transmission to sentinels”, Emily Mantlo, et al., 7 May 2024. “Sentinels” were the pigs who were not injected with the Clade II Mpox, but were put in the same cages as those pigs who were. The “sentinel” pigs also came down with Mpox (in other words, animal-to-animal transmission of the virus.) Below are the Ethics Statement and the Funding Statement for this study:
Note that the study was conducted in BSL-3 labs at KSU; that tissue-processing was performed at CDC BSL-2 facilities; and, that, apparently, college students were working in the BSL-3 labs in the study. This indicates that Gain-of-Function experiments with the Clade II of Mpox were being performed; that lower-level biosafety labs were used; and, that college students were involved (how much close supervision was provided by KSU?)
So, Gain-of-Function experiments are being performed using the Mpox virus; experiments funded by the NIH. A very dangerous, deadly Smallpox “vaccine”, ACAM2000, was suddenly FDA-approved for the “prevention” of Mpox. The “definition” of who is “at risk” for an Mpox infection has been “expanded” to include all persons who are sexually active. The Clade II of Mpox (the one that is the subject of the Gain-of-Function experiments) is now infecting people all over the planet, including in the United States. And more. Cui bono? How many of the general public will line up for an injection of ACAM2000 because the CDC / FDA / AMA / Establishment Medicine, will issue a warning due to “increasing numbers of infections being reported of Mpox?” How many healthcare professionals will be “mandated” into taking ACAM2000 “to protect themselves and the patients they care for?” (Again, JYNNEOS was already approved for Mpox “vaccination”, and it is ** potentially ** a “safer” alternative “vaccine.”) How many more Gain-of-Function experiments will be conducted, not in facilities like the Wuhan Institute of Virology or the Baric Lab at UNC Chapel Hill — but at places like the BSL-3 Ag Lab at Kansas State University (a facility where, arguably, one would expect research on, say, equine viruses, not Clade II Mpox experiments on pigs)? How much more Gain-of-Function experimentation will be hidden and/or “obscured” from public knowledge, let alone from Congress?
The above is a vintage image of mass vaccination. (Courtesy Google Images.)
This series on the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
The origination of today’s post begins here: www.dossier.today/p/double-digits-biden-admin-tells-americans, “Double Digits: Biden Admin tells Americans that it’s soon time for their 10th Covid shot“, by Jordan Schachtel, 13 June 2024. (Mr. Schachtel wrote about the ninth COVID-19 “vaccine” injection here: www.dossier.today/p/dose-number-nine-cdc-panel-green, “Dose number NINE: CDC panel green lights yet another Covid mRNA shot“, 29 February 2024. The CDC recommended that persons over age 65 take another “booster shot” of either the Pfizer-BioNTech or of the Moderna “2023-2024 Formula COVID-19 Vaccine” of these manufacturers.) A person age 65 or older, if that person adhered to every CDC recommendation regarding taking a COVID-19 “vaccine” injection since December 2020 (when the FDA granted first Emergency Use Authorization (EUA) to Pfizer-BioNTech and to Moderna for these companies’ “flagship” modRNA COVID-19 “vaccines” (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), would have taken injection number nine starting on 28 February 2024.
Today’s post is long. There is a large amount of information to “unpack.” Stay with me here.
Note the language regarding the “selection of a specific JN.1 lineage SARS-CoV-2 strain…” More about that later.
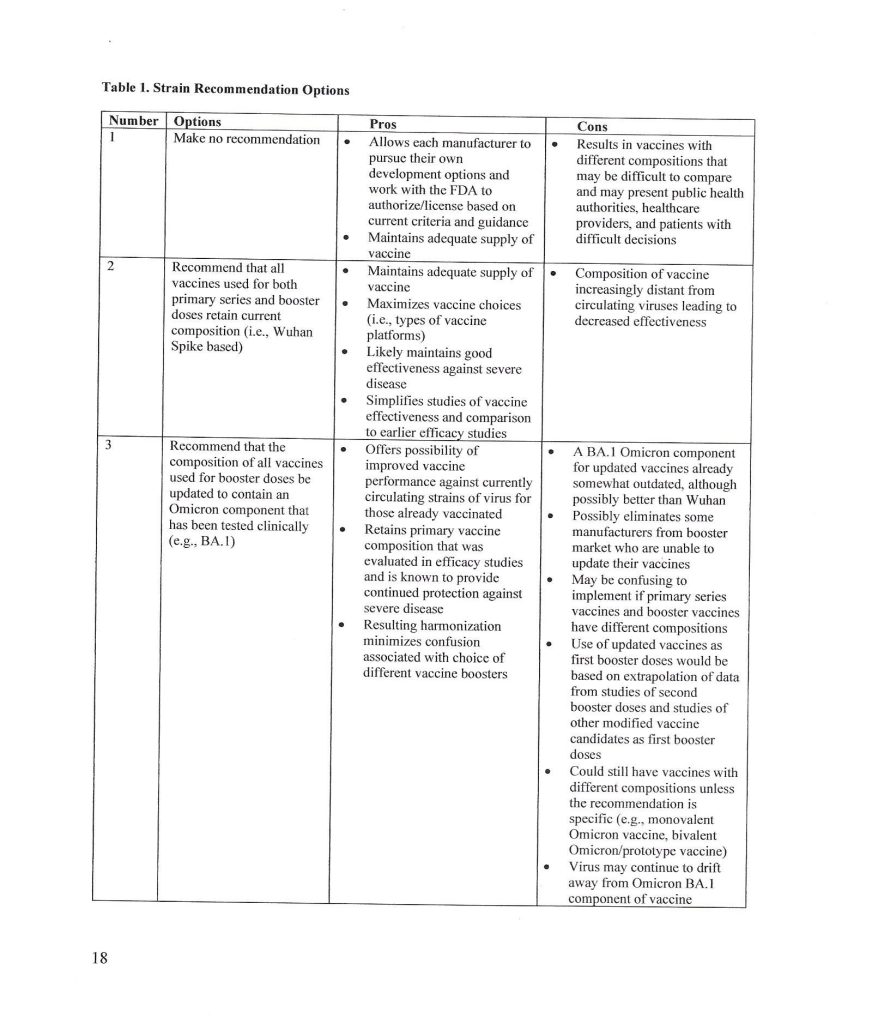
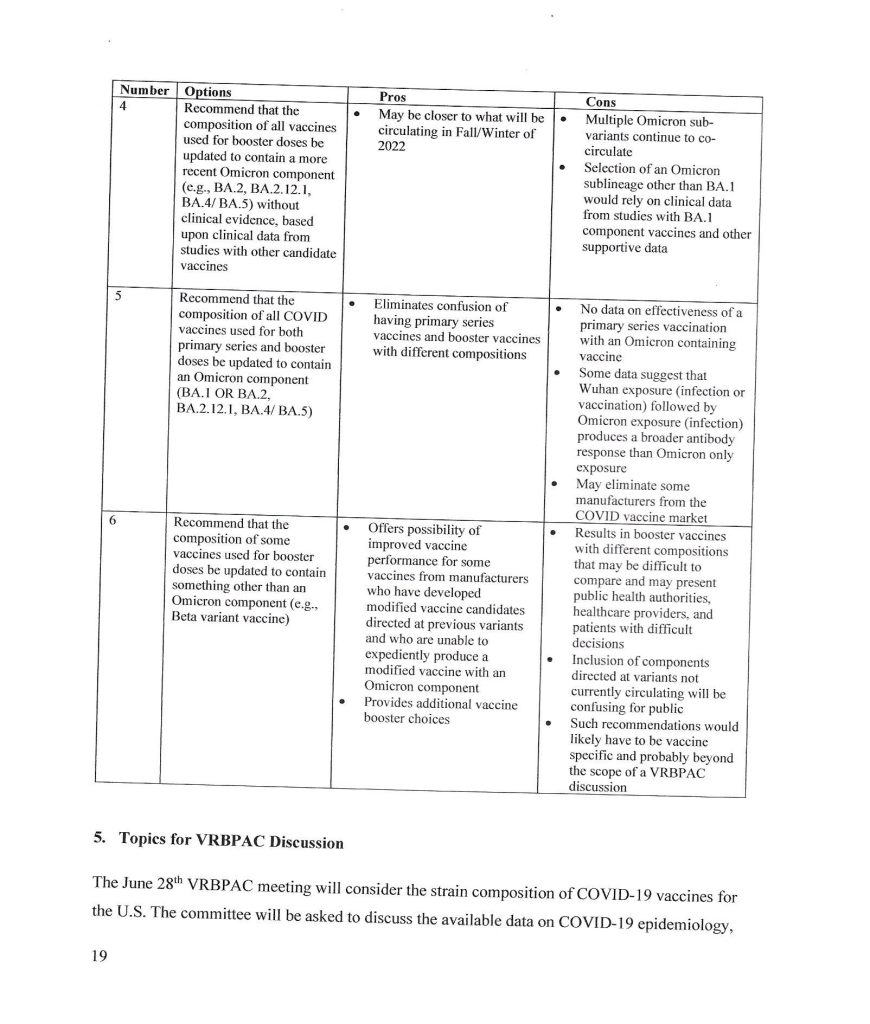
The trail behind the 5 June 2024 FDA announcement begins with the VRBPAC Briefing Document for the meeting held on 28 June 2022: www.fda.gov/media/159452/download, “FDA Briefing Document Vaccines and Related Biological Products Advisory Committee Meeting June 28, 2022.” It was at this meeting that the FDA “codified” the types of “strain composition recommendations” that the agency would use regarding “new versions” of COVID-19 “vaccines.” Yours Truly presents page 17, page 18, and page 19 of this document:
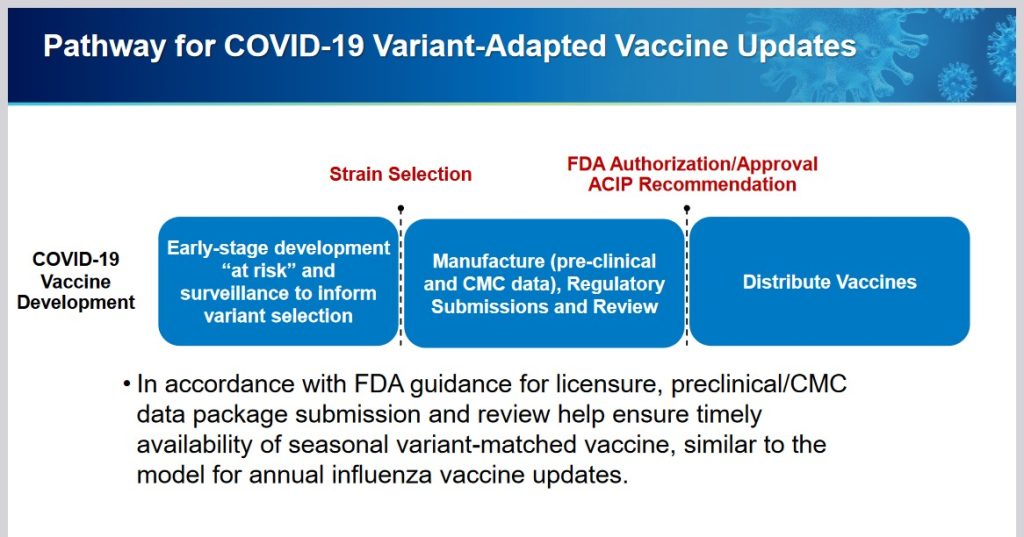
It appears that the FDA simply decided that it would be permissible for the agency to authorize a new COVID-19 “vaccine” strain composition along what, in Yours Truly’s opinion, may be called “very flexible” options. For example, the Pfizer-BioNTech XBB.1.5 COVID-19 “vaccine”, which was FDA authorized in the fall of 2023, had test results only from mouse testing prior to FDA authorization. Following are: The link to the Pfizer-BioNTech slide presentation about this “vaccine” to the CDC’s ACIP committee (Advisory Committee on Immunization Practices) meeting of 12 September 2023; and, an image of slide CC4 from this presentation. First, the presentation: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-09-12/10-COVID-Modjarrad-508.pdf.
Second, slide CC-4 from the above presentation:
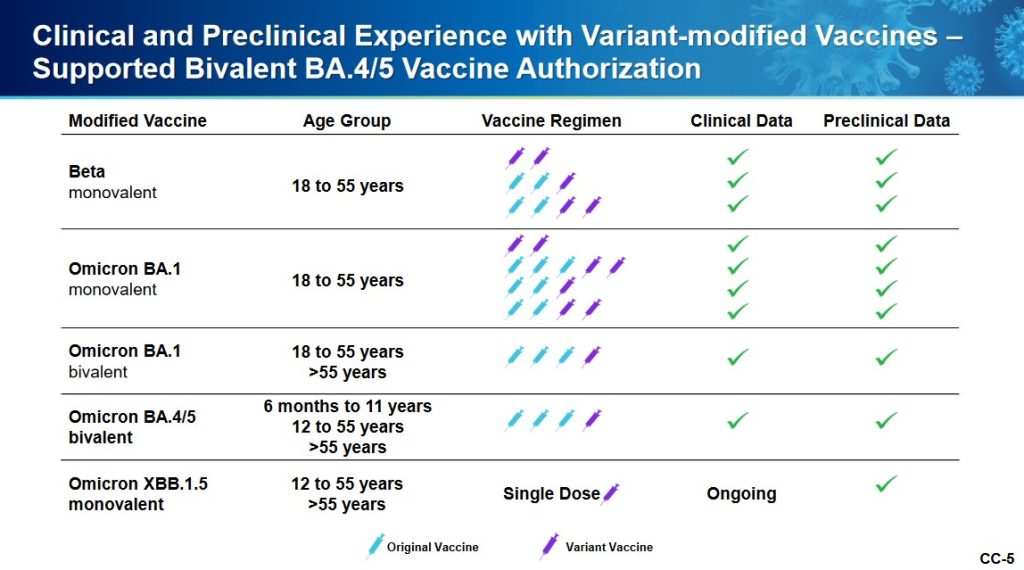
The XBB.1.5. Pfizer-BioNTech COVID-19 “vaccine” had only been given as a single injection to humans in the company’s clinical trial; a clinical trial which had only just begun prior to the ACIP meeting. Slide CC-5 of the presentation, the start of the company’s human trial of this “vaccine”, is below:
Slide CC-6 of the presentation has to do with the mouse studies of this “vaccine”, which were of longer duration.
Notwithstanding the above, the FDA authorized the use of the company’s XBB.1.5 COVID-19 “vaccine” on 11 September 2023 (in Yours Truly’s opinion, it appears that the ACIP meeting of 12 September 2023 was a “catch-up” formality.) It also appears (again, in Yours Truly’s opinion), that the FDA used a very loose interpretation of “Option 4” on page 18 of the FDA Briefing Document above in granting the EUA for this “vaccine”.
** Now, on to the latest “new version” of the COVID-19 “vaccines”, the “2024-2025 Formula COVID-19 Vaccines”, that the FDA authorized in June 2024.
The following linked items are important regarding background information related to this situation and to the FDA: First, the FDA document, stating that the agency would “align” its COVID-19 “vaccine” antigen composition to the recommendations of the World Health Organization’s TAG-CO-VAC recommendations: www.fda.gov/media/179139/download (the TAG-CO-VAC recommendation for the “2024-2025 Formula COVID-19 Vaccines” was to use the JN.1 strain); second, the FDA document regarding “considerations and recommendations” for the “2024-2025 Formula COVID-19 Vaccine” composition: www.fda.gov/media/179145/download; third, the FDA announcement of the 5 June meeting of its VRBPAC committee (Vaccines and Related Biological Products Advisory Committee.): www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-june-5-2024-meeting-announcement. From this last link, chick on “Event Materials” to see the slide presentations and other items that were discussed at this meeting.
Two important items from the “Event Materials” list: the FDA Briefing Document; and the VRBPAC roster for this meeting. First, the FDA Briefing Document: www.fda.gov/media/179003/download; and, second, the VRBPAC roster for this meeting: www.fda.gov/media/179225/download. The roster for the 5 June 2024 meeting has some “familiar” members and speakers: Paul Offit, MD; and Peter Marks, MD (director of CBER [Center for Biologics Evaluation the Research of the FDA]); and, among the “Temporary Voting Members”, are: Bruce Gellin, M.D., M. PH., the Chief of Global Public Health Strategy for the Rockefeller Foundation; and, Melinda Wharton, M.D., M. PH., Associate Director of Vaccine Policy of the CDC. (Italics mine)
The VRBPAC members voted unanimously to endorse the Pfizer-BioNTech, the Moderna, and the Novavax “2024-2025 Formula COVID-19 Vaccine” by these companies, based on the presentations of these companies’ representatives at the meeting. Yours Truly can find noregistered human clinical trials performed in advance of the 5 June VRBPAC meeting by Pfizer-BioNTech, or by Moderna, or by Novavax, for any “2024-2025 Formula COVID-19 Vaccine”; that would indicate that any “clinical trials” were performed in these companies’ facilities on mice; and that any “human trials” were also performed in these companies’ facilities, prior to the meeting. The FDA then issued the agency’s original announcement of 7 June 2024: www.fda.gov/news-events/press-announcements/fda-roundup-june-7-2024; and, a screenshot from this announcement:
Note in particular “…the selection of a specific JN.1 lineage SARS-CoV-2 strain (e.g., JN.1. or KP.2) and expressed a strong preference for JN.1.” Here’s where it starts to “get interesting.”
What was it that happened? Part of the answer lies in the fact that the NIH and Moderna co-own the patents (and, therefore, share the royalties) for the Moderna “flagship” modRNA COVID-19 “vaccine”, mRNA-1273. This agreement would extend to “descendant clone COVID-19 vaccines” by Moderna. www.citizen.org/article/modernas-mrna-1273-vaccine-patent-landscape/. The NIH’s Dale and Betty Bumpers Vaccine Research Center (part of NIAID — which Dr. Anthony Fauci led from November 1984 until his retirement in December 2022) and Moderna co-developed mRNA-1273. https://covid19.nih.gov/news-and-stories/nih-vaccine-research-center; a screenshot from the article is below:
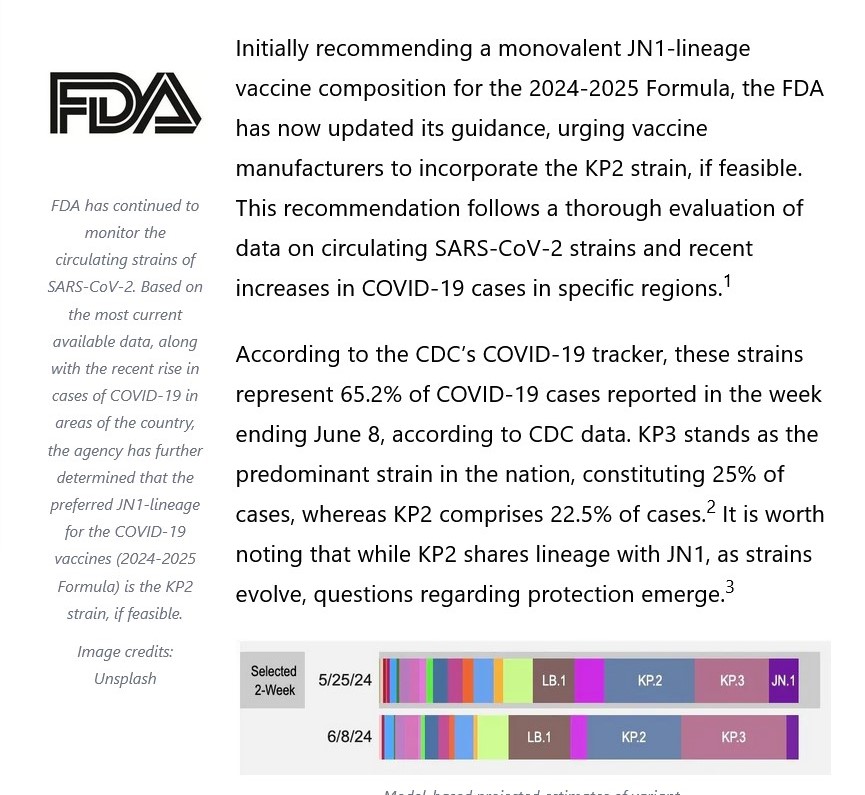
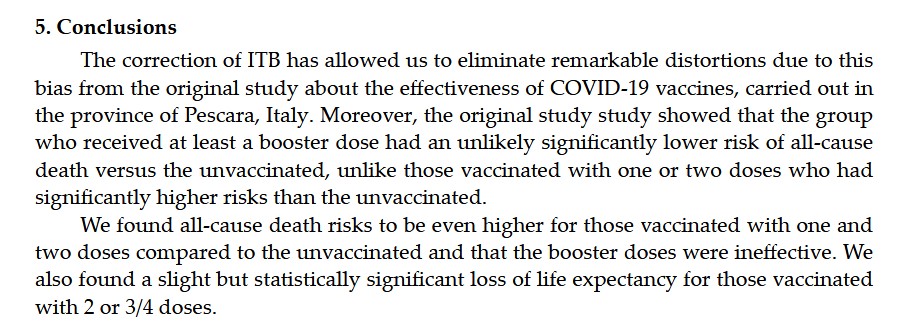
The other part of the answer is that Moderna was already developing a KP.2 strain COVID-19 “vaccine” for 2024-2025. This, and the FDA’s decision to shift away from the JN.1 strain to the KP.2 strain, are described in this post at Sasha Latypova’s blog: https://sashalatypova.substack.com/p/all-roads-lead-to-resilience, “All Roads lead to Resilience. FDA is removing competitors for the Pentagon & CIA’s baby…Moderna”, 23 June 2024.
However, there’s yet another detail in play here, regarding the FDA’s switch, “based on evaluation of the most recent circulating strains of COVID-19”, from JN.1 to KP.2 — the CIA and the Pentagon. Here is a screenshot from Sasha Latypova’s Substack article:
But wait, there’s more! Resilience lists multiple “partners”, such as the Mayo Clinic. The company also, apparently, has a “partnership” with the United States Army’s Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense https://resilience.com/learn/partnerships. Below is a screenshot from this website:
It appears, then, in Yours Truly’s opinion, that the FDA was perhaps “reminded” of the”details” regarding the NIH-Moderna co-ownership (and royalties – sharing) agreement related to Moderna’s modRNA COVID-19 “vaccines”; and, the role of the CIA-Pentagon-National Resilience (aka Resilience) in manufacturing the mRNA used in the Moderna COVID-19 Omicron “booster vaccines” — and the KP.2. strain is indeed a “descendant strain” in the Omicron lineage (as is the JN.1 strain.) Hence, the FDA’s 2024-2025 COVID-19 “vaccine” strain “sudden switch” announcement of 13 June 2024, only one week after the agency gave the nod to the JN.1 strain.
In Yours Truly’s opinion, it is statistically, medically, and ethically impossible for a new vaccine (let alone any COVID-19 “vaccine”) to be developed; tested (on lab animals, then on human subjects); the test data thoroughly collated and analyzed for “safety and efficacy” on both lab animals and on human subjects; then, which data is presented to the CDC / FDA for consideration; then, these agencies doing their own “due diligence” research; then, and only then, being granted an EUA by the FDA; then, and only then, manufactured for use in humans — in a time span of fewer than three to five years, let alone within a time span of only a few months. It appears, again in Yours Truly’s opinion, that the CDC and the FDA are playing “fast and loose” with the health and safety of the people who choose (or will be “mandated”) to take the “2024-2025 Formula COVID-19 Vaccine.” And, also, that “other entities” are in play here to perhaps “influence” decision making by these agencies.
All of above is in addition to the fact that the COVID-19 “vaccines” (actually, gene therapy injections) have caused, are causing, and will cause, multiple health issues, serious adverse reactions, and deaths, in those who are “vaccinated.” Just two of the most recent discoveries: One, the COVID-19 “vaccines” can cause brain damage, an article by Dr. William Makis: www.globalresearch.ca/brain-damage-covid-19-mrna-vaccines/5861012, “Brain Damage Caused by COVID-19 mRNA Vaccines”, 26 June 2024. Below is a screenshot from Dr. Makis’ article:
The second most recent discovery, that the COVID-19 “vaccines” reduce life expectancy (even in “all-cause” analysis) among COVID-19 “vaccinated” persons, by Dr. Peter A. McCullough: https://petermcculloughmd.substack.com/p/breaking-publication-a-critical-analysis, “BREAKING Publication — A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, 1 July 2024. The peer-reviewed paper is here: https://doi.org/10.3390/microorganisms12071343, “A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, Marco Alessandria, et al., published 30 June 2024. Below is a screenshot from the Conclusions section of this paper:
In Yours Truly’ opinion, it is apparent at “half a glance” that the COVID-19 “vaccines” (actually, gene therapy injections) must be completely withdrawn for human use until these products have been fully investigated, and then re-designed, before being re-introduced for human use; and, that there is no “co-ownership” or sharing of royalties between a government agency and a COVID-19 “vaccine” manufacturer; and, that there is no involvement of the United States military in the development or manufacture of such products.
The above is an image of Father Christmas from a vintage postcard.
The following may be a bit “heavy” — please regard it as a kind of rich “Christmas Pudding” of COVID-19 “vaccine” knowledge base. Not a “lump of coal!”
Just in time for Christmas, Yours Truly presents a list of what she considers to be the “Top 12” types of damage that the COVID-19 “vaccines” can do to the body of the “vaccine” recipient. This list has been gathered from the 1600+ hours of investigating “all things COVID-19” that Yours Truly has done since March 2020. Therefore, it is only her opinion. People who read through the report that Pfizer-BioNTech gave to the FDA on 30 April 2021, regarding the over 1,000 serious adverse events medical conditions that the company’s COVID-19 “vaccine”, BNT162b2, caused in persons who took this “vaccine” IN FEWER THAN THREE MONTHS after the FDA granted the initial EUA for this “vaccine” in December 2020 for its use in the United States, may come up with “Top Lists” of their own. The report can be found here: https://phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Events Reports. The APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST, found at the end of the report, lists these serious adverse events conditions reports that BNT162b2 caused in “vaccinated” persons.
However, what is NOT opinion is that the FDA then knew, on 30 April 2021, that the Pfizer-BioNTech “flagship” COVID-19 “vaccine” BNT162b2 (actually, an untried gene therapy injection), was capable of damaging the body of the “vaccine” recipient in over 1,000 different ways, including the ways on Yours Truly’s “Top 12 List..” However, instead of performing its regulatory (and moral and ethical) obligations to immediately pull BNT162b2 off the market and out of use until the situation could be further investigated, the FDA chose to CONTINUE the EUA that it granted in December 2020 for BNT162b2. Not only that, but the FDA went ahead and granted “full approval” for the use of the European version of BNT162b2, called COMIRNATY, in the United States. Not only that, but the FDA granted EUA’s for the Pfizer-BioNTech COVID-19 “bivalent vaccine” to be used in the United States. Finally, in the spring of 2023, the FDA quietly stopped all use of BNT162b2 in the United States — in Yours Truly’s opinion, after mounting reports of serious adverse events, including deaths, being caused by this “vaccine” were beginning to circulate widely and to be confirmed by professional researchers and by doctors — and substituted the use of the Pfizer-BioNTech (and the Moderna) “booster vaccines” for the Omicron variant. In the summer of 2023, the FDA granted EUA’s for both the Pfizer-BioNTech and for the Moderna “2023-2024 Formula COVID-19 Vaccine”, which had only been tested on mice.
Here is Yours Truly’s “Top 12 List”: The first nine, from the APPENDIX 1. cited above:
Death: neonatal and Sudden unexplained death in epilepsy (page 3 and page 8); Myocarditis and Pericarditis (page 6 and page 7); Stroke (Cerebral artery embolism page 2; Cerebral thrombosis, page 2); Thrombotic Stroke (page 9), among other types; THIRTY different types of Autoimmune disorders (page 2); FORTY different types of Herpes disorders (page 4 and page 5); THIRTY-PLUS different types of Liver disorders (page 4); TWENTY-FIVE different types of Immune System disorders (page 5); SIXTEEN different types of Neurological (brain and/or central nervous system) disorders (page 6); and, COVID-19 and COVID-19 Pneumonia (page 3).
As an example, here is a handy-dandy image of page 4 of the APPENDIX 1., with Yours Truly’s notes:
To round out the “Top 12 List” of COVID-19 “vaccine” damage to the body of the recipient, there are these three:
One: Heart tissue and lung tissue damage / destruction: Please refer to: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, by Michael Palmer, MD, and Sucharit Bhakdi, MD; Two: Fetal / Neonatal disorders, including 1p36 deletion syndrome (also listed on page 1 of the APPENDIX 1.): Please refer to the following regarding 1p36 deletion syndrome: https://medlineplus.gov/genetics/condition/1p36-deletion-syndrome/ (more on this condition below); and, Three: Cancer induced with the assistance of the SV40 cancer promoter DNA that has been recently discovered in the Pfizer-BioNTech COVID-19 “vaccines” (more on this below): Please refer to the following: https://osf.io/preprints/osf/mjc97, “DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events”, David Speicher, Jessica Rose, Kevin McKernan, et al. From lines 94-95 of this paper: “McKernan, et al., found SV40 promoter-enhancer-ori [DNA], and SV40 polyA signal sequences in the Pfizer vaccines.” The SV40 promoter-enhancer DNA is also in the Pfizer-BioNTech COVID-19 “vaccines” that were used in the United States: https://rumble.com/v3r1pqf-vaccine-adulteration-wkevin-mckernan-byram-bridle-chris-martenson-steve-kir.html, beginning at 3:32 in the video. Please also refer to the letter of December 2023 from Florida Surgeon General, Dr. Joseph Ladapo, to the directors of the FDA and the CDC: www.floridahealth.gov/about/_documents/12-06-2023-DOH-Letter-to-FDA-RFI-on-COVID-19-Vaccines.pdf. Yours Truly will posit that, since the modRNA + its spike protein and the “Process 2” manufacturing method for the current “2023-2024 Formula COVID-19 Vaccine” by this company in use in the United States are both based on its original “vaccine” formulations (BNT162b2 and the “booster and bivalent vaccines”), it appears that this opens up the possibility that the SV40 promoter-enhancer DNA is present in this “vaccine” also. Important: The SV40 promoter-enhancer DNA in the Pfizer-BioNTech COVID-19 “vaccines” is not the entire code, only a part of it. In and of itself, this “partial code” likely would not cause cancer; however, it can be involved in the general damage / destruction that the COVID-19 “vaccines” do to the “vaccine” recipient’s body, which can, in turn, be involved in the onset of cancer, or the re-emergence of cancer already in remission, in that person’s body. In addition, Pfizer-BioNTech DID NOT TELL the Canadian health authorities, nor, apparently, the FDA in the United States, about the SV40 issue.
About the 1p36 deletion syndrome caused by the modRNA COVID-19 “vaccines”: This is particularly troubling, since it effects UNBORN children and THE SPERM AND THE EGGS OF THE “VACCINATED” PARENTS. 1p36 deletion syndrome is a multi-faceted condition that negatively affects fetal development. Infants born with this condition have severe intellectual difficulties; weak muscle tone; have vision, hearing, and heart issues; and either do not speak, or can only speak a limited vocabulary; among other things. Please refer to the MedlinePlus link, above, for further information. It has been proven that large amounts of the dangerous lipid nanoparticles AND the enhanced spike protein + its modRNA in the Pfizer-BioNTech COVID-19 “vaccine” migrate to, and lodge in, two important areas of the recipient’s body — the OVARIES and the TESTES. Please refer to the image below, directly from Pfizer-BioNTech, on page 8 of a document that the company gave to the FDA on 21 January 2021. The document is called BNT162b2 2.6.5 Pharmacokinetics Tabulated Summary. It is available through https://phmpt.org/.
Please also refer to this graphic, which shows what the modRNA COVID-19 “vaccines” do in the pregnant mother’s body and in the body her unborn child or her nursling child (this is from a CDC presentation):
1p36 deletion syndrome is “...caused by a deletion of genetic material from a specific region in the short (p) arm of chromosome 1…Most cases of 1p36 deletion syndrome are not inherited.” (per the MedlinePlus link, above.) Think about that.
A final note on the current “2023-2024 Formula COVID-19 Vaccines” by both Pfizer-BioNTech and by Moderna: These apparently do include the ingredients (although in smaller amounts) of the original modRNA COVID-19 “vaccines” made by each company (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), with additional elements of the Omicron XBB 1.5 variant lineage. Please refer to the following: www.fda.gov/media/167211/download, page 39 (Pfizer-BioNTech); www.fda.gov/media/167208/download, page 34 (Moderna); and, https://covid19.nih.gov/covid-19-vaccines.
As an aside, in case readers hear someone “congratulating themselves” for their taking either the Novavax or the Johnson & Johnson (Janssen) COVID-19 “vaccines”, because they believed that somehow these “vaccines” are “safer” than those of Pfizer-BioNTech or of Moderna: The Novavax COVID-19 “vaccine” uses the same modRNA + its spike protein as in the Pfizer-BioNTech and the Moderna COVID-19 “vaccines.” The difference with the Novavax COVID-19 “vaccine” is that the SARS-CoV-2 virus is “marinated” in an insect culture, with the resulting modRNA “harvested” and mixed with “adjuvants” made from soap tree bark; this “vaccine” also uses lipid nanoparticles (LNPs.). The Johnson & Johnson (Janssen) COVID-19 “vaccine” was removed from use (revoked) in the United States by the FDA in May 2023. However, persons who took this “vaccine” prior to May 2023, are at risk for Thrombosis and Thrombocytopenia, as listed on the “black letter warning” area on the (revoked) FDA Fact Sheet for Healthcare Providers for this “vaccine.” Please refer to the following: for the Novavax COVID-19 “vaccine”: www.fda.gov/media/159897/download, page 33; www.hackensackmeridianhealth.org/en/healthu/2022/08/09/novavax-vaccine-how-its-different-and-how-it-works; and, for the Johnson & Johnson (Janssen) revoked COVID-19 “vaccine”: www.fda.gov/media/146304/download, page 1.
Yours Truly will make it clear she believes that COVID-19, in its variants forms, is still a threat to health. Since one is a concerned citizen, not a healthcare practitioner, one can only offer the following thoughts:
First: it is of primary importance that all people have, and maintain, the best level of personal health and immunity that is possible; “un-vaccinated” people have a primary responsibility here to themselves. Second: It is of primary importance that all “un-vaccinated” people follow a protocol for prophylaxis against COVID-19, such as those outlined at https://covid19criticalcare.com/, and including judicious exposure to sunlight and daily mild to moderate exercise. Third: It is of primary importance that all people follow “common sense” approaches, such as washing the hands, and staying away from sick people if possible. Fourth: It is of importance that “vaccinated” people know about various protocols to try and mitigate the dangerous effects of the COVID-19 “vaccines” at work in their bodies; https://covid19criticalcare.com/treatment-protocols/. Fifth: It is of great importance to have and keep a positive connection with a Supreme Being.
“Then will you know the truth, and the truth shall set you free.” John 8:32
It is past time, in Yours Truly’s opinion, to bring to justice those who were/are involved in the development and manufacture of the COVID-19 “vaccines”; and those in the FDA / CDC / AMA, and other medical agencies and organizations, who either know, should have known, or knew of, the dangers of these “vaccines” — but still continue to push them. Some examples: Albert Bourla, DVM (CEO of Pfizer Inc.); Stephane Bancel (CEO of Moderna); Alex Gorsky (CEO of Johnson & Johnson until 2022); Anthony Fauci, MD (former head of the NIAID); Francis Collins, MD (former head of the NIH); Janet Woodcock, MD (former Acting Commissioner of the FDA); Rochelle Walensky, MD (former Director of the CDC); Peter Daszak, CEO of EcoHealth Alliance; Robert Califf, MD (current Commissioner of the FDA); Mandy Cohen, MD (current Director of the CDC); Jesse M. Ehrenfeld, MD, (current head of the AMA); and, Ralph Baric, PhD, of the Baric Lab at the University of North Carolina, Chapel Hill.
RDS in the following comment points out one of the problems we have in waking up the Sheeple. There are highly ‘respected’ doctors and PhDs, who write papers in prestigious journals backing the mRNA vaccines even though they KNOW they are unsafe.
Wolf Moon OMG, this article below is a must-read. Linked from an AMA EdHub email one received today. It’s a JAMA piece written by Dr. Peter Marks — he’s the head of the CBER department of the FDA (Center for Biologics Evaluation and Research). Dr. Marks was in on the ground floor of Operation Warp Speed. Dr. Marks KNOWS EVERY DATA PIECE SUBMITTED TO THE FDA FROM PFIZER-BIONTECH ABOUT THE CLINICAL TRIALS FOR BNT162b2 BACK IN 2020 — AND EVERY DATA PIECE SINCE THEN ALSO. Dr. Marks was in on recommending that the FDA authorize the UNPROVEN, ONLY TESTED ON 8 MICE new “COVID-19 + Omicron BA.4 + Omicron BA.5 booster shot.” His linked article below is a screed for the development of “new” and “different types” of COVID-19 “vaccines” — including ones that specifically target the T-cell response in the body. Dr. Marks KNEW that the “vaccines” developed during Operation Warp Speed and given quick EUAs by the FDA WOULDN’T DO THE JOB: From his article: “One potential model for approaching such development [of a COVID-19 vaccine] was used successfully at the beginning of the pandemic when Operation Warp Speed evaluated numerous global vaccine types and focused on advancing several promising candidates, knowing full well that most would ultimately not be found to meet the criteria set forth for a safe vaccine with adequate efficacy.” (bolding and Italics mine) Dr. Marks represents the “medical establishment” and DeepState. IMO, the “medical establishment” and the DeepState have it as their business to continue to put these dangerous COVID-19 “vaccines” into people — and develop new “vaccines” to keep damaging / destroying the immune systems of those who take them. His article: https://jamanetwork.com/journals/jama/fullarticle/2799600 December 9, 2022 “Urgent Need for Next-Generation COVID-19 Vaccines” Peter Marks, MD, PhD https://www.youtube.com/watch?v=Nat1za4sKjA As an additional note. For those who might wish to watch the documentary it is available to watch free until the end of January. All that is required is your email I think. The link follows. https://therealanthonyfaucimovie.com/trailer/
In addition to censorship and smearing of dissenting voices, hospitals and doctors were getting the carrot and stick treatment – Lose your license OR getbig bucks for pushing bogus PCR tests, ventilators, Remdesivir and killing patients. – For example “A COVID-19 diagnosis provides extra payments to coroners!”
To make sure the Sheeple could not make a solid connection between the Covid Vaccine and death, the shot is a slow ‘poison’ with a variety of adverse reactions.
The CDC has been hiding the Social Security Administration death master file. I got it from a whistleblower. This shows deaths are taking 5 months from the jab to happen. This is why it’s hard to see.
Remember this time factor as we look at the data I found.
Finally we have the DELIBERATELY compromised VAERS system that is SUPPOSED to alert the CDC and FDA to harmful drugs.
There are major problems with the vaccine adverse event reporting system (known as VAERS) which the CDC considers the “front line” of vaccine safety. VAERS was created in 1990 by the CDC and FDA as a means to collect and analyze adverse effects that are associated with vaccines. Unfortunately, the failings of VAERS are “kept from the consciousness” not only of the public, but also from the doctors, pediatricians, and nurses that the public rely on to provide reliable information as to the safety of vaccines. I say “kept from the consciousness” rather than “kept secret” because while these failings are publicly disclosed for all the world to see, they are for all intents and purposes BURIED in documents seldom searched out by the average member of the medical community, much less by the average individual. You could say that the information has been very effectively hidden in plain sight…
In 2000, the 6th Report by the Committee on Government Reform addressed the failings of VAERS in its address of the Vaccine Injury Compensation Program…. [The] Congressional report notes (on page 15), “Former FDA commissioner David A. Kessler has estimated that VAERS reports currently represent only a fraction of the serious adverse events.” (emphasis by author)… That leads us to the interesting case of the CDC and Harvard Pilgrim Healthcare Inc.
The Department of Health and Human Services (HHS) gave Harvard Medical School a $1 million dollar grant to track VAERS reporting at Harvard Pilgrim Healthcare for 3 years and to create an automated reporting system which would revolutionize the VAERS reporting system- transforming it from “passive” to “active.”…
I’ll quote the findings directly from the report,
“Adverse events from drugs and vaccines are common, but underreported. […] Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of ‘problem’ drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed.”
Again, let’s stop and think about this revelation for a moment: fewer than 1% of vaccine adverse events are reported. The CDC’s entire vaccination propaganda campaign rests on their claim that side effects from vaccination are exceedingly rare (and predominantly minor).According to the CDC, in 2016 alone, VAERS received 59,117 vaccine adverse event reports. Among those reports were 432 deaths, 1,091 permanent disabilities, 4,132 hospitalizations, and 10,274 emergency room visits. What if these numbers actually represent less than 1% of the total as this report asserts? Simple multiplication would yield vaccine adverse events reports numbering 5,911,700!…
the United States of America Centers for Disease Control ghosted Harvard Pilgrim Healthcare, Inc.
“the practice of ending a personal relationship by suddenly and without explanation withdrawing from all communication.”
Personally, I would hope that I could hold an organization like the CDC to a higher standard, but… After a one million dollar grant was paid and three years of research conducted on what appeared to be a very successful upgrade to the passive VAERS system, the team’s CDC contacts went MIA
. The ESP:VAERS final report states, “Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.”
So in 2017, the CDC DELIBERATELY left a useless reporting system in place when they had the opportunity to upgrade it.
Since the VAERS data set is compromised as well as next to useless, I decided to see if we could find another way to connect the mRNA vaccines to deaths. There is a nifty site called Dead or Kicking.
there is the graph “United States death comparison by age in 2020“
By changing the date in the URL you get the different years AND if you place your mouse over the graph, it will give you Deaths, Death Rate and Population for each age group.
You can save the graphs for any year – or all of them – as examples, as Wolf did below. Right-clicking on a graph lets you “save image as” or “copy image”.
2019
2020
2021
2022
Note Added By Wolf – CHECK THIS ONE OUT!!!
I originally thought I would see a major drop in the population over 75 but that did not happen since the Baby Boomer cohort is filling the 65+ age groups faster than the orchestrated depopulation can kill them. Notice there are less people in the 45 to 54 age group than in the 55-64 age group. That is a REAL PROBLEM for the Cabal.
…The Social Security Trust Fund should currently have $2.5 trillion in surplus. So how is it that these checks could stop being issued if the debt ceiling isn’t raised? Economics professor Dr. Allen Smith, author of The Looting of Social Security: How The Government is Draining America’s Retirement Account, has been reporting on the theft of Social Security funds for years….
Age / Date
2019
2020
2021
2022
85+
6,604,958
6,628,013
6,673,175
6,715,875
75-84
15,969,872
16,022,410
16,139,651
16,250,631
65-74
31,483,433
31,571,207
31,773,610
31,970,852
55-64
42,448,537
42,643,579
42,929,850
43,208,648
45-54
40,874,902
41,050,404
41,371,452
41,683,591
So I created another table this time of USA Death Rates by age group by year. I included 6 years before covid as a baseline. Then the two years, 2019 & 2020, when Covid hit the USA plus the two years, 2021 and 2022 when the mRNA vaccine was progressively rolled out, starting with adults, then school age children and finally babies.
Also there was the DELIBERATE mis-diagnosis of flu and pneumonia followed by refusal to treat until the person was so sick they needed to be put on a ventilator & remdesivir thus killing up to 88% of those patients.
The result of all of this, is the most vulnerable elderly had already been killed off in 2020 as the much higher death rates for 2020 shows, but by 2021 and 2022 the death rates decrease from that high. Although the elderly were vaccinated, unlike athletes and younger, physically active people, the elderly are going to be a lot more sensitive to what their bodies are telling them and NOT pushing it. They are also more likely to have doctors checking their heart health and be on heart and circulatory medications.
Myocarditis is an important cause of arrhythmias and sudden cardiac death (SCD) in both physically active individuals and athletes.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
RETIREES 65 to 74
The 65 to 74 group is going to be a mixed bag. Compared to the 75+ group they are less likely to be in a nursing home or to have gotten deathly ill in 2020, although a certain percentage will have died. However they are likely to get the vaccine. Thanks to Medicare, they are more likely to be in contact with medical professionals who would try to talk them into the jab. They are also going to be a lot more physically active than older retirees and therefore stressing their hearts more after getting the mRNA vaccine.
You can see the combination of poor health care in 2020 followed by the vaccines and then boosters as the death rate increases year by year from 2019 through 2022.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
FORCED RETIREMENT/SMALL BUSINESS WORKERS 45 to 64
The 45 to 64 are an interesting group. Corporations force retirements and actively discriminate against those 45 years and up because age discrimination laws have no real teeth. Therefore the people 45 and up are most likely NOT working for ‘Corporate America’ and are either small business people or hired by small business people. (BTDT) This group is the most likely to have had a ‘rude awaking’ about the world we live in and are NOT going to be as trusting. Older people are also more likely to tell their boss to go F..K themselves with the darn needle. Like the 65 to 75 group you can see the increase in death rate year to year but it is not as sharp an increase. They are also more likely to be in better health than retirees. If You’re Over 50, Chances Are the Decision to Leave a Job Won’t be Yours Age discrimination in the workplace happening to people as young as 45: study
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
WORKING AGE CORPORATE AMERICA 15 TO 44
The age group 15 to 44 is the group most likely to show PURE UNADULTRATED DATA about Mortality & the mRNA vaccine although there may be some confounding from drug use increasing over the years. Covid-19 virus has little effect on the death rate in 2020. However as the boosters and the 5 month time delay kicks in you can see the death rate almost doubled in 2022 compared to 2019 and earlier.
….Scott Davison, the CEO of OneAmerica, a $100 billion life insurance and retirement company headquartered in Indianapolis.
“The data is consistent across every player in the business.”
Davison said death rates among working age people –
those 18 to 64-years-old – are up 40 percent in the third and fourth quarter of 2021 over pre-pandemic levels.
“Just to give you an idea of how bad that is, a three sigma or 200-year catastrophe would be a 10 percent increase over pre-pandemic levels,” Davison said. “So, 40 percent is just unheard of.”
He blames it on Covid instead of the mRNA vaccine of course. “…the third and fourth quarter of 2021…” would be after Steve Kirsch’s 5 month window. So far I can not find any 2022 insurance data. HMMMmmmm
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
CONTROL GROUP 1 TO 14
The 1 year to 14 can be considered the ‘Control Group’ Covid has little if any effect on the death rate in 2020. They were not vaxed until quite recently (November 2021) and boosters were not approved until May 19, 2022. The death rate so far has been flat but I would expect an uptick after the first of this year as the effects of the boosters kick in.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
BABIES UNDER 1 YEAR
The Under one year of age is interesting since there is actually a slight dip in mortality. Are weaker babies more subject to spontaneous aborting after Mom is vaxed?
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
TIMELINE of Emergency Use Authorization of mRNA VACCINES
The FDA makes it VERY HARD to figure out just when they authorized the use of the mRNA vaccine in youngsters. I gleaned out the following dates. Starting from the FDA Covid Vaccine site.
Turns out it is the CDC who has the final say on vaccination of children so I have also included the CDC news releases.
12/18/2020 – EUA issued for the Moderna COVID-19 Vaccine, December 18, 2020. Emergency Use Authorization (EUA) of the Moderna Inc. COVID-19 Vaccine for the prevention of COVID-19 in individuals 18 years and older.
YEAR 2021
06/10/2021 — Vaccines and Related Biological Products Advisory Committee will meet in open session to discuss, in general, data needed to support authorization and/or licensure of COVID-19 vaccines for use in pediatric populations.
FDA DEFINES: Pediatric use. (A) Pediatric population(s)/pediatric patient(s): For the purposes of paragraphs (c)(9)(iv)(B) through (c)(9)(iv)(H) of this section, the terms pediatric population(s) and pediatric patient(s) are defined as the pediatric age group, from birth to 16 years, including age groups often called neonates, infants, children, and adolescents.
. 09/17/2021 — Application for administration of a third (“booster”) dose of Comirnaty (COVID-19 Vaccine, mRNA) in individuals 16 years of age and older.
10/26/2021 — Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss a request to amend Pfizer-BioNTech’s Emergency Use Authorization (EUA) for administration of their COVID-19 mRNA vaccine to children 5 through 11 years of age.
10/14/2021 – Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss the Emergency Use Authorization (EUA) of the ModernaTX Inc. COVID-19 vaccine and the Janssen Biotech Inc. COVID-19 vaccine for the administration of an additional dose, or “booster” dose, following completion of the primary series, to individuals 18 years of age and older.
Today, CDC Director Rochelle P. Walensky, M.D., M.P.H., endorsed the CDC Advisory Committee on Immunization Practices’ (ACIP) recommendation thatchildren 5 to 11 years oldbe vaccinated against COVID-19 with the Pfizer-BioNTech pediatric vaccine. CDC now expands vaccine recommendations to about 28 million children in the United States in this age group and allows providers to begin vaccinating them as soon as possible.
The Food and Drug Administration today authorized Moderna’s COVID-19 vaccine for children aged 6 months through 17 years old and Pfizer’s COVID-19 vaccine for children aged 6 months through 4 years old, as recommended this week by its vaccine advisory committee. The vaccines previously were authorized for older children.
Before vaccinations can begin, the Centers for Disease Control and Prevention must recommend the vaccines for these age groups. CDC’s Advisory Committee on Immunization Practices is scheduled to vote tomorrow on whether to authorize the vaccines for children age 5 and under.
Children 6 months through 5 years of age who received the original (monovalent) Moderna COVID-19 Vaccine are now eligible to receive a single booster of the updated (bivalent) Moderna COVID-19 Vaccine two months after completing a primary series with the monovalent Moderna COVID-19 Vaccine.
Following today’s meeting of the Advisory Committee on Immunization Practices’ (ACIP), CDC is expanding eligibility of COVID-19 vaccine booster doses to everyone 5 years of age and older. CDC now recommends that children ages 5 through 11 years should receive a booster shot 5 months after their initial Pfizer-BioNTech vaccination series.
I had already seen the video I’m about to show you, when I watched the press conference in which Florida Governor Ron DeSantis powerfully chastised the media for mischaracterizing his administration’s position of OPPOSING the mRNA vaccines for kids, as PROHIBITING the vaccines for kids – something which DeSantis reminded the idiot media that he cannot do.
However, DeSantis didn’t “hide” his opposition in the least. He still seemed to be doing everything in his power to get parents to look at Pfizer’s clinical trial data (or lack thereof) allegedly justifying this needless – if not counterproductive – if not downright dangerous vaccine.
Thus, when I saw how STRONGLY DeSantis held his ground, I thanked God that somebody in his administration surely saw the same video that I had seen.
YOU NEED TO SEE IT, TOO.
Just watch this. It’s short and to the point.
BOMBSHELL: Dr. Clare Craig Exposes How Pfizer Twisted Their Clinical Trial Data for Young Children
Gov. Ron DeSantis clarifies Florida's position on COVID shots for children, saying he's not surprised that the White House would lie and legacy media amplify it.
He adds countries with similar approaches to Florida "have been right on COVID way more than Fauci and his crew." pic.twitter.com/biRQf9Es2z
— The Post Millennial (@TPostMillennial) June 20, 2022
Twitter will try to remove this tweet from the historical record, so let’s just make a copy.
In my opinion, this Pfizer clinical trial is nearly 100% BAD SCIENCE.
That such bad science is not merely allowed to pass without comment by America’s major scientific organizations, such as the AMA and the ACS, but was in fact used by the FDA to approve utterly needless vaccines – this kind of failure of American science is SOUL-DEADENING.
It’s not just one person here or a research group there. This is multiplicity of large-group institutional failure.
Personally, I blame this shocking failure on the triumph of Chinese ethics over traditional Western ethics.
Pfizer, with its global HQ for clinical trial data in Wuhan (SURPRISE, SURPRISE, SURPRISE!) is now allowing China and the CCP to effectively run all its clinical trials. This horrible, shoddy trial just REEKS of a sick combination of malignant Chinese battered anarcho-capitalism and corrupt Chinese communism. This is typical “top down” forcing of mistakes due to POLITICS and GREED.
I have been telling people that I will NEVER take another drug from Pfizer.
In my opinion, the approval of a “likely safer” coronavirus vaccine is – in the long game – a big win for popular science – here’s why.
The approaching approval (or not) of a competing EUA for the NON-mRNANON-viral-vectorNON-geneticNovavax coronavirus vaccine is going to tell us a LOT about how much power Pfizer and China still hold over FDA and CDC.
As you may have read two days ago, I regarded the conveniently timed FDA public statement about the myocarditis risks of the Novavax vaccine as a cynical “pot-vs.-kettle” attempt to sway approval and prevent the entirety of future Novavax data from getting into VAERS, where such data would very likely highlight every possible problem with the mRNA vaccine technology of the Pfizer and Moderna vaccines.
TL;DR – “I believe that mRNA vaccines have serious risks that would be REVEALED by approval of the Novavax vaccine.” -Wolf Moon I’m actually surprised that FDA and Pfizer/China allowed Novavax to get this close to approval, but they clearly have the upcoming vote RIGGED, just like the 2020 election. The trusty “board mules” that …
Well, it looks like the VRBPAC bunch did the smart – or at least consistent thing, and recommended approval.
The 21-0 vote with one abstention is telling, IMO. A vote AGAINST would cause an uproar on both sides, and put VRBPAC in the hot seat. Are they shuffling the murder of Novavax off to “the Roach” for a kill? We will see.
Here is a comment I added to my prior post, regarding an article in the Federalist, which takes the “no more approvals of any vaccine” approach – which I believe is well-intended but short-sighted. This comment explain my strategic reasons for supporting approval.
Here is a great example of somebody who sees the vaccines much the same as me, but strategically comes to the exact opposite point of view on approval of Novavax.
Reading his point of view may help people to see mine – or maybe not. Worth a read.
Dr. Gortler basically wants to begin playing fair and correctly on Novavax – making it jump through the hoops that Pfizer and Moderna didn’t have to jump through, but (IN MY OPINION, NOT HIS) thus denying what is likely a SAFER vaccine (in many respects – not all) to people who are going to take a vaccine, one way or another.
In my opinion, admitting the Novavax vaccine will shed necessary light on mRNA technology, as this “shingles-style” (recombinant protein) vaccine will help to highlight the flaws of the mRNA tech in the long run.
This is where I take a “Trumpian” and “they have to be shown” position. I regard a denial here as the kind of “purism” that has been deadly to conservatives, and was responsible for “NeverTrump” as an effective weapon of the left.
We have what is likely a “saf-ER” vaccine. Do we approve it or not?
YMMV.
Wolf Moon, June 9, 2022
Note that there is still plenty of time for FDA and/or CDC to snake Novavax and help Pfizer and China. Will they do it? Let’s wait and see. Either way, we win.
If Rochelle Alinsky and Anthony Fauci knife Novavax in the back to protect mRNA, I will have one of my greatest arguments yet that they need to be removed and prosecuted. The blatant hypocrisy will win more and more Democrats to our side. All of my neighbors are perfect recipients of the message. They will be screaming for Fauci to hang.
If they allow Novavax the opportunity to prove itself [to any degree] safer than mRNA vaccines, they fight another day – but they have to fight a battle we are destined to win.
Like I say, every day is a fight – but we are winning more and more fights, sooner and sooner.