“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
The colorized vintage image of vaccination for today’s header is courtesy of MedPage Today and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: AI-generated items in today’s offering will be cited as such. If readers wish to post AI-generated items in today’s discussion thread, they must cite their source. Thank you.
And now, on to the mRNA-1283 (mNEXSPIKE) component of mRNA-1083. Today’s offering is Part One of two:
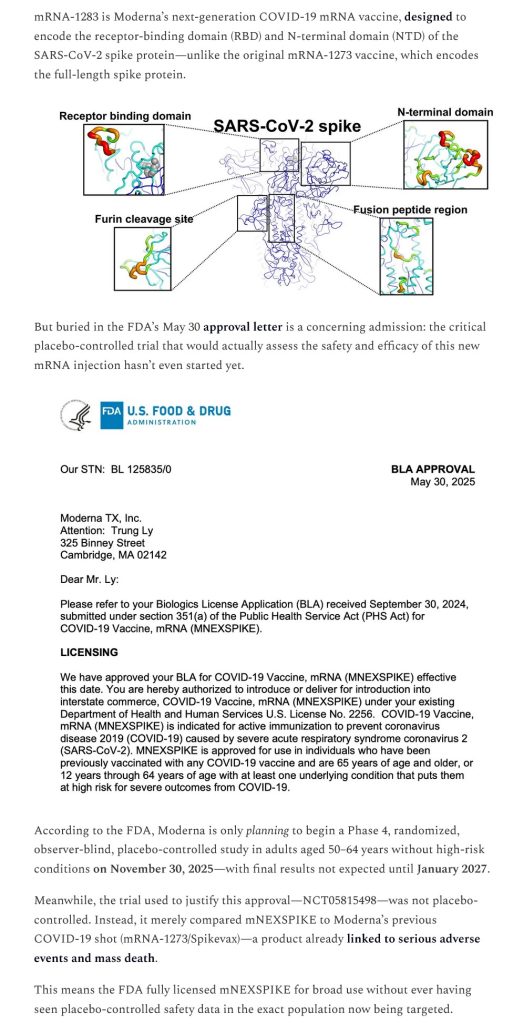
Moderna’s “other” modRNA COVID-19 bioweapon “vaccine”, mRNA-1283 (mNEXSPIKE), was approved for use in the United States on 30 May 2025. The FDA Approval Letter to Moderna is here: https://www.fda.gov/media/186740/download. The Approval Letter for mNEXSPIKE was signed by David C. Kaslow, MD, Director of the Office of Vaccines Research and Review (a subdivision of FDA’s CBER department [Center for Biologics Evaluation and Research]). Dr. Kaslow is a Biden-era “holdover” at the FDA; he has been with CBER since 11 October 2022.
It appears that Dr. Kaslow relied solely on the “data” that was given to the FDA by Moderna regarding the “safety and efficacy” of mRNA-1283, prior to that agency’s granting approval of the BLA (Biologics License Application) that Moderna submitted for the product. In addition, it appears that Dr. Kaslow believed that the “data” that Moderna supplied to the FDA was sufficient enough to warrant a bypass of the review process by the VRBPAC group of the FDA (Vaccines and Related Biological Products Committee.) Please see the screenshot from Dr. Kaslow’s Approval Letter to Moderna for mRNA-1283 (mNEXSPIKE), below:
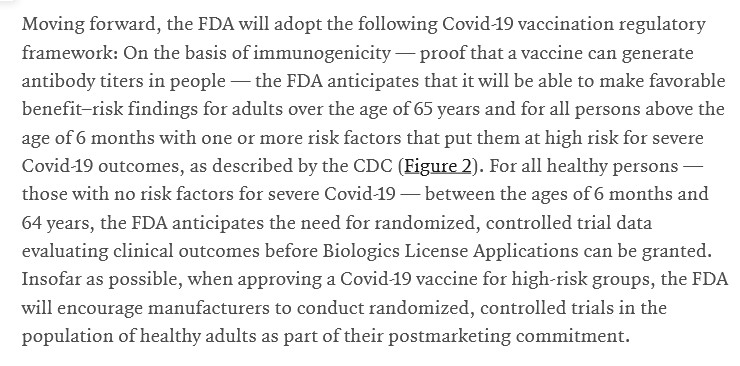
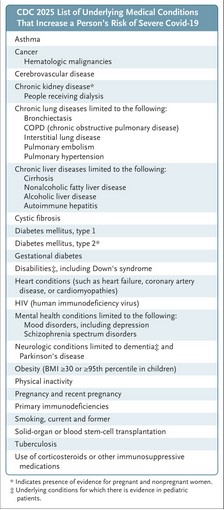
By the way, on 20 May 2025, Dr. Martin Makary (FDA Commissioner) and Dr. Vinay Prasad (Director of the FDA’s CBER division) published an “opinion piece” in the New England Journal of Medicine that purported to be their “opinions” regarding a “new approach” to COVID-19 “vaccination” in the United States. However, this was not really an “opinion piece” — it was implemented as FDA policy. This article by Dr. Prasad and Dr. Makary was published just 10 days before Dr. Kaslow sent the Approval Letter to Moderna for mRNA-1283 (mNEXSPIKE.) Did Dr. Prasad and Dr. Makary know in advance that Dr. Kaslow was going to issue this Approval Letter? Did HHS Secretary Kennedy, Jr., know? The “opinion piece” is here: https://doi.org/10.1056/NEJMsb2506929. “An Evidence-Based Approach to COVID-19 Vaccination.” Vinay Prasad, MD, MPH, and Martin Makary, MD, MPH. 20 May 2025. Below are two screenshots from this article: from the text; and, the Figure 2, which lists the “groups at severe risk from COVID-19.” The persons who would fall under one or more of the categories listed in Figure 2, even if these persons are under age 65, would “qualify” for “vaccination” with mNEXSPIKE:
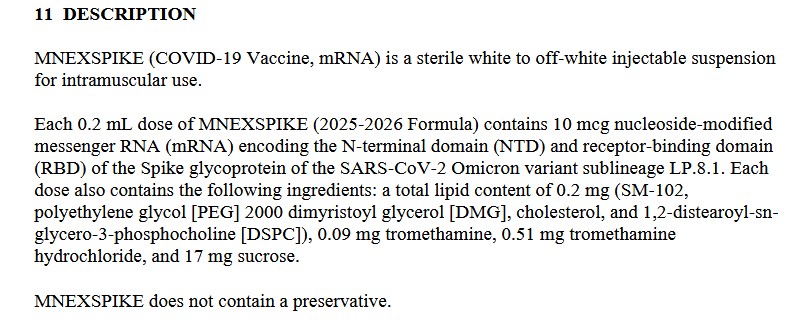
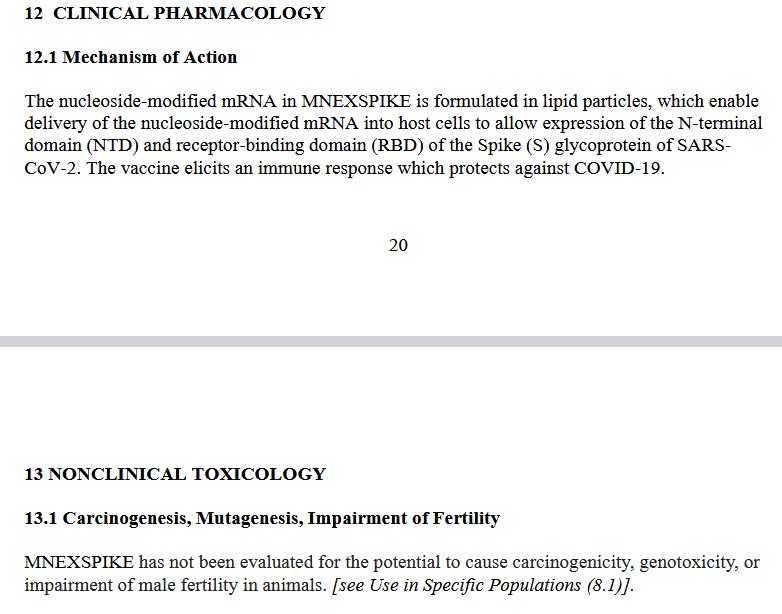
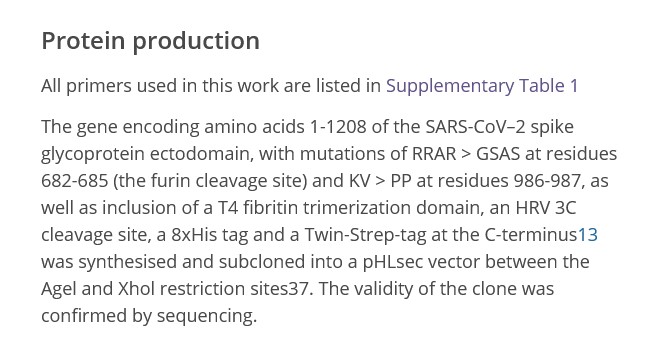
The Package Insert for healthcare professionals for mRNA-1283 (mNEXSPIKE) is here: https://www.fda.gov/media/186738/download. Please see the screenshots of the following sections of this Package Insert, below: first, section 11 Description; then, section 12 Clinical Pharmacology, and section 13 Nonclinical Toxicology:
It would appear that Dr. Kaslow was comfortable in approving an injectable by Moderna (mRNA-1283, also called mNEXSPIKE) that contains the dangerous lipid nanoparticle SM-102; that contains at least PEG-related element (polyethylene glycol); and, that was not tested for carcinogenicity (the potential to cause cancer), for genotoxicity (the potential to damage genes, or to cause changes to genes, either of which can also cause cancer), or for impairment of male fertility.
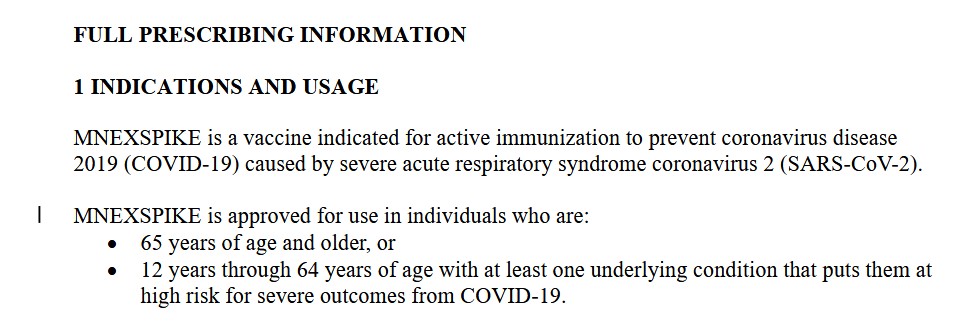
It would also appear that Dr. Kaslow was comfortable with approving this modRNA COVID-19 bioweapon “vaccine” (mRNA-1283, also called mNEXSPIKE), which is purported to “prevent infection of COVID-19” — but, which claim has been proven to be wrong. From the FDA Package Insert for mNEXSPIKE:
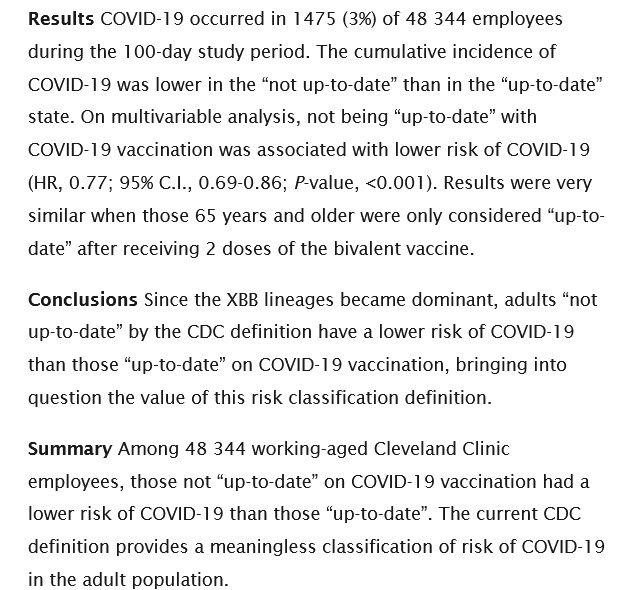
The “prevent coronavirus disease 2019 (COVID-19)” statement is still being used by the FDA on COVID-19 bioweapon “vaccines” Package Inserts, despite the fact that Shrestha, et al., demonstrated in 2023 that “fully up-to-date vaccinated” Cleveland Clinic employees were more likely to become COVID-19 infected than those who were not “fully up-to-date” with COVID-19 “vaccination” (https://doi.org/10.1101/2023.06.09.23290893. “Risk of Coronavirus Disease (COVID-19) Among Those Up-to-Date and Not Up-to-Date on COVID-19 Vaccination.” Nabin K. Shrestha, et al. 13 June 2023.) Please the screenshot from this paper, below:
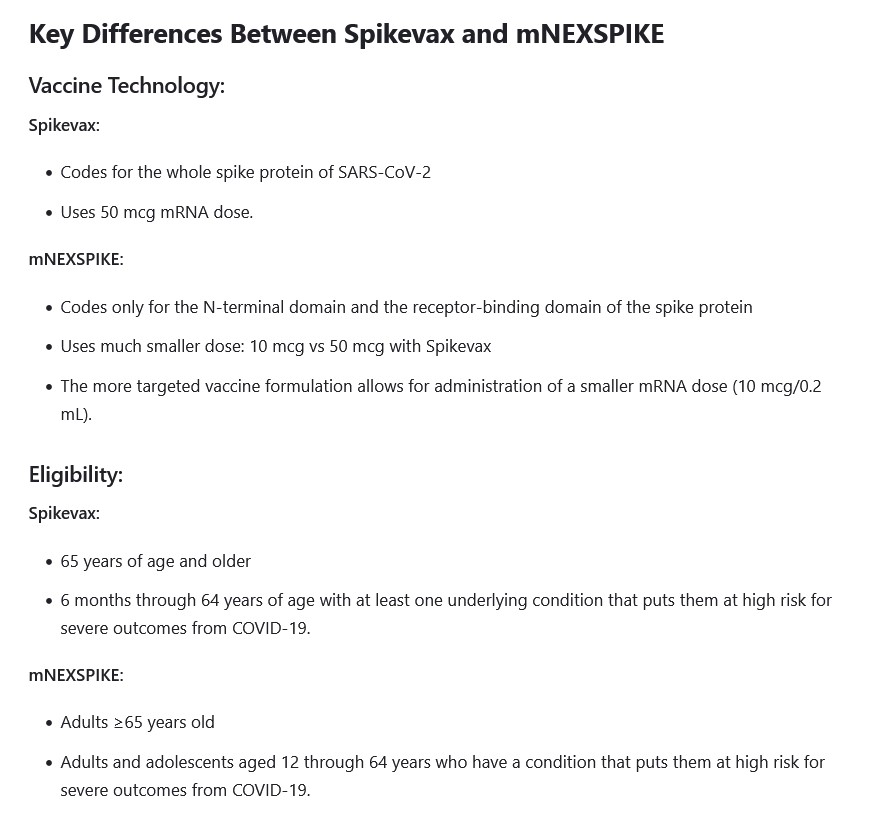
Why aren’t the Moderna “original” modRNA COVID-19 bioweapon “vaccine”, mRNA-1273 (SPIKEVAX), and the Moderna modRNA COVID-19 bioweapon “vaccine”, mRNA-1283 (mNEXSPIKE), the same? Please see the screenshot, below, from this article (https://www.drugs.com/medical-answers/what-difference-between-spikevax-mnexspike-3580787/, “What is the difference between SPIKEVAX and mNEXSPIKE?”, 2 September 2025:
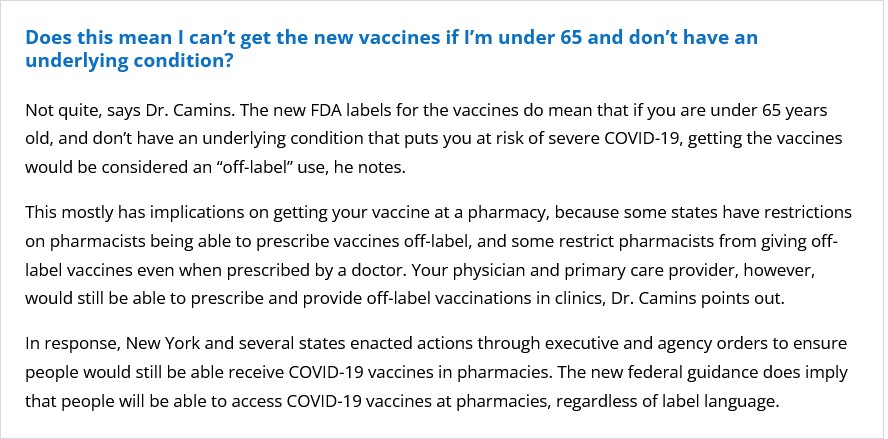
However, regarding mNEXSPIKE, there apparently is a “blurred line” as to the use of it in persons under age 65 who do not have an “underlying medical condition.” Please see the screenshot below, from this article: https://health.mountsinai.org/blog/heres-what-you-need-to-know-about-the-new-covid-19-vaccines/, 23 September 2025; the advice is from Dr. Bernard Camins, MD, MSc, of Mount Sinai Hospital, in the “FAQ” section:
Note the language above, from Dr. Camins, regarding the ability of pharmacists to “prescribe vaccines off-label.”
Why is the N-terminal domain of the SARS-CoV-2 virus so important to Moderna that the company crafted a modRNA COVID-19 bioweapon “vaccine”, mNEXSPIKE, to utilize it? The N-terminal domain area is the “closest” (in terms of placement) to the receptor-binding domain (RCB) on the SARS-CoV-2 virus code. The N-terminal domain is also close to the S1/S2 cleavage site on the virus code. The receptor-binding domain is the part of the virus code that “makes sure” that the “payload” of the “vaccine” binds itself (enters into) the cells of the “vaccinated” person. These, in this writer’s opinion, make the N-terminal domain a “prime target” for the development of modRNA COVID-19 bioweapon “vaccines” that do not need to include the entire virus code, but still can “deliver the payload” through the receptor-binding domain mechanism. Please see: https://doi.org/10.3389/fcimb.2020.587269. “SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development.” Mei-Yue Wang, et al. 24 November 2020. Figure 1.) This is in contrast to the other modRNA COVID-19 bioweapon “vaccines” (by Moderna and by Pfizer-BioNTech) that contain the entire spike protein sequence (S1 and S2 areas.)
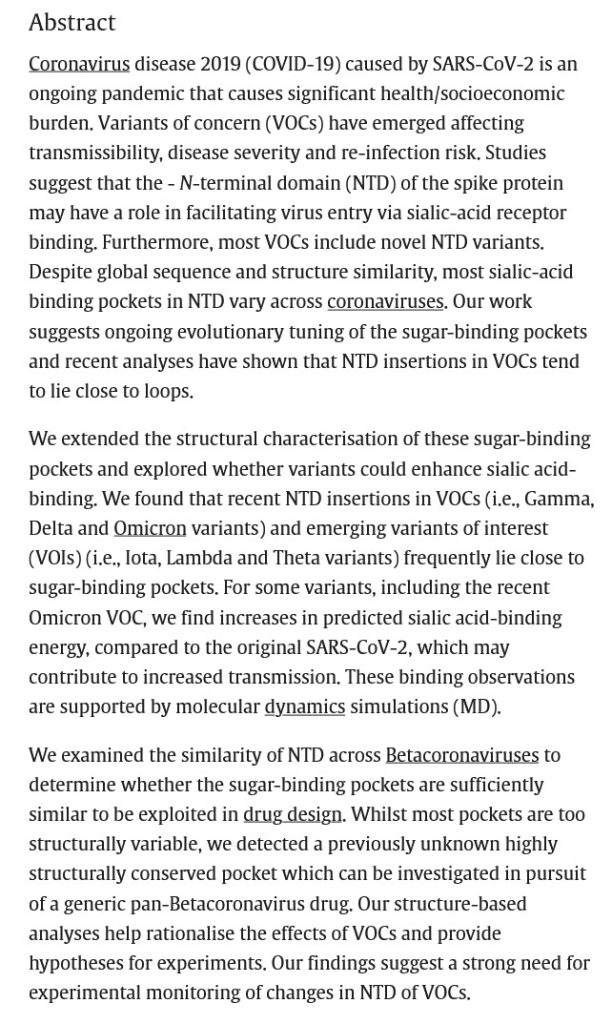
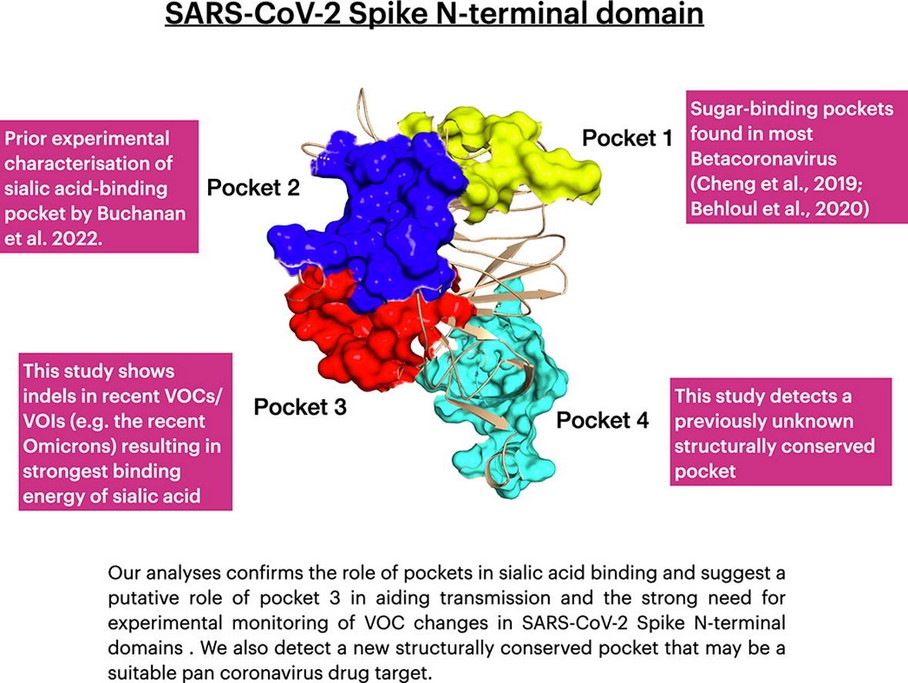
The issue regarding developing a modRNA COVID-19 bioweapon “vaccine” that only utilizes the N-terminal domain and the receptor-binding domain appears to have been determining exactly what “binding pocket” of the N-terminal domain would work. Scientists had been experimenting with the N-terminal domain to find such a “binding pocket”: for example, as described in this paper, from 2022: https://doi.org/10.1016/j.csbj.2022.11.004. “Structural and energetic analyses of SARS-CoV-2 N-terminal domain characterise sugar binding pockets and suggest putative impacts of variants on COVID-19 transmission.” Jonathan Lees, et al. 17 November 2022. Please see the screenshots from this paper, below; first, the Abstract; followed by the Graphical Abstract:
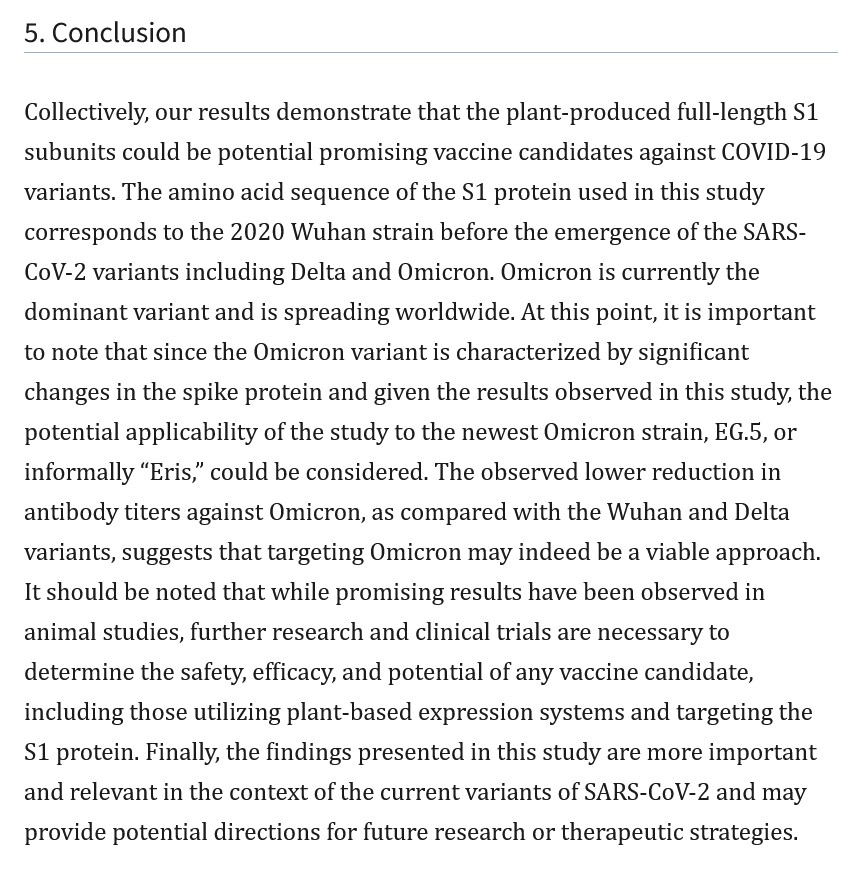
It appears that Moderna did find such an N-terminal “binding pocket” to use for the development of mNEXSPIKE. And, it appears that the company’s decision to “harness” the mechanism to the S1 area of the SARS-CoV-2 spike protein, as opposed to using the entire S1/S2 sequence, is due to the fact that the S1 area is that which appears to be the most “effective” in regards to the Delta and Omicron variants of the virus. Please refer to: https://pubmed.ncbi.nlm.nih.gov/38034565. “SARS-CoV-2 spike protein S1 subunit induces potent neutralizing responses in mice and is effective against Delta and Omicron variants.” Tarlan Mamedov, et al. 14 November 2023. Please see the screenshot, below, of the Conclusion from this paper:
Note that Mamedov, et al., used a tobacco plant to produce the S1 protein from SARS-CoV-2, which they then tested against Delta and Omicron virus variants.
In this writer’s opinion, mRNA-1283 (mNEXSPIKE) cannot be thought of as “mRNA-1273 (SPIKEVAX) Lite.” mNEXSPIKE contains the S1 spike protein of an Omicron variant of SARS-CoV-2. mNEXSPIKE contains the dangerous lipid nanoparticle, SM-102, that mRNA-1273 (SPIKEVAX) also contains. mNEXSPIKE contains N1-Methylpseudouridine (which will destroy the RNA of the “vaccinated” body’s natural Uridine, replacing it with a lab-created chemical compound that has no natural, beneficial mechanism for the body), which mRNA-1273 (SPIKEVAX) also contains. In this writer’s opinion, the only difference between mRNA-1273 (SPIKEVAX) and mNEXSPIKE is that the latter “vaccine” does not contain the S2 area of the spike protein.
To be continued in Part Two.
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA, A modRNA, AN saRNA, OR A taRNA PRODUCT OF ANY KIND, IN ANY FORM. THERE MUST, FIRST, BE MUCH MORE RESEARCH INTO THESE GENE-ALTERING THERAPY PLATFORMS AND PRODUCTS. THERE MUST, SECOND, BE IRREFUTABLE PROOF THAT THESE GENE-ALTERING THERAPY PLATFORMS AND PRODUCTS ARE TRULY “SAFE AND EFFECTIVE.”
Peace, Good Energy, Respect: PAVACA
(Intellectual Disclaimer and Notice: Other than URLs and related items available on the Internet, the ideas and opinions of today’s offering are by PAVACA. Credit must be given to PAVACA if the ideas and opinions of today’s offering are used by other blog writers, by podcasters, or in social or print media.)
The header image for today’s offering of an end run is courtesy of Grammarist and Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for AI-generated items; to the best of her knowledge and belief, there are none. If readers wish to post AI-generated items in today’s discussion thread, they must cite their source. Thank you.
Today’s offering is Part One regarding the current situation with Moderna’s latest entry into the mRNA-based “vaccine” platform: the company’s influenza “vaccine”, mRNA-1010.
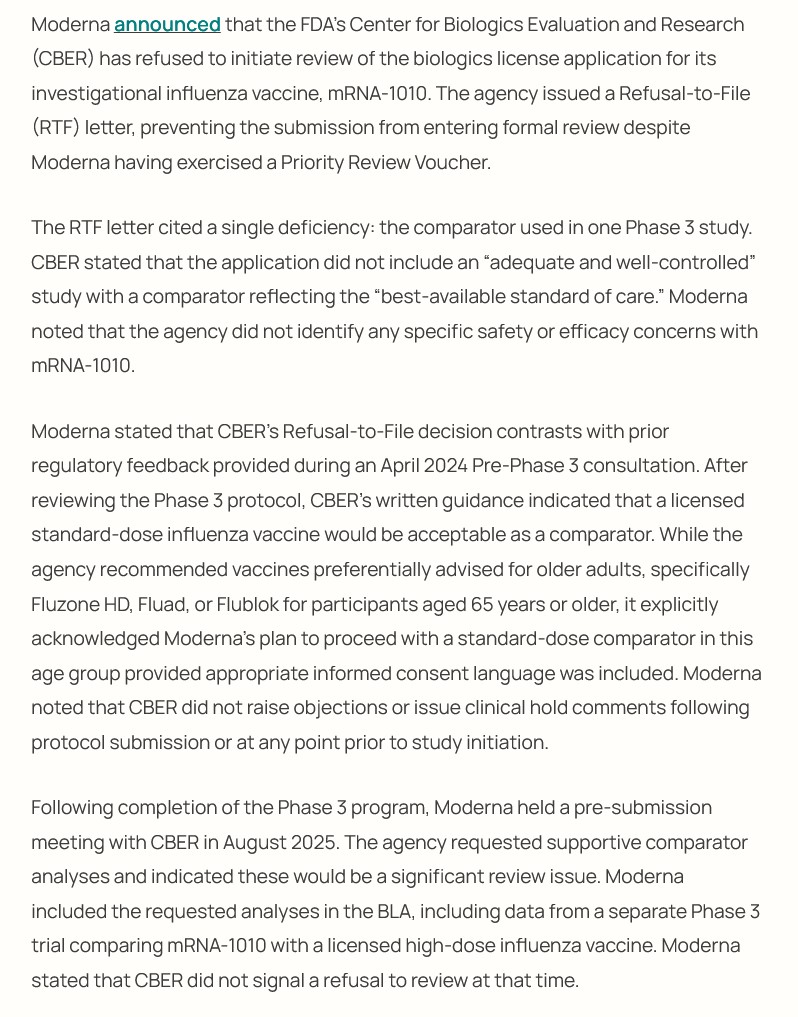
On 11 February 2026, Dr. Vinay Prasad, director the CBER division of the FDA (Center for Biologics Evaluation and Research) sent an RTF letter (Refusal to File letter) to Moderna in response to that company’s BLA application (BIologics License Application) review request for mRNA-1010, a modRNA-based “vaccine” against several strains of influenza. Dr. Prasad cited the lack of a true placebo control group in a study by Moderna using this “vaccine candidate.” Please see the screenshots, below, from https://pharmacally.com/fda-issues-refusal-to-file-letter-for-modernas-mrna-1010-flu-vaccine/, 11 February 2026:
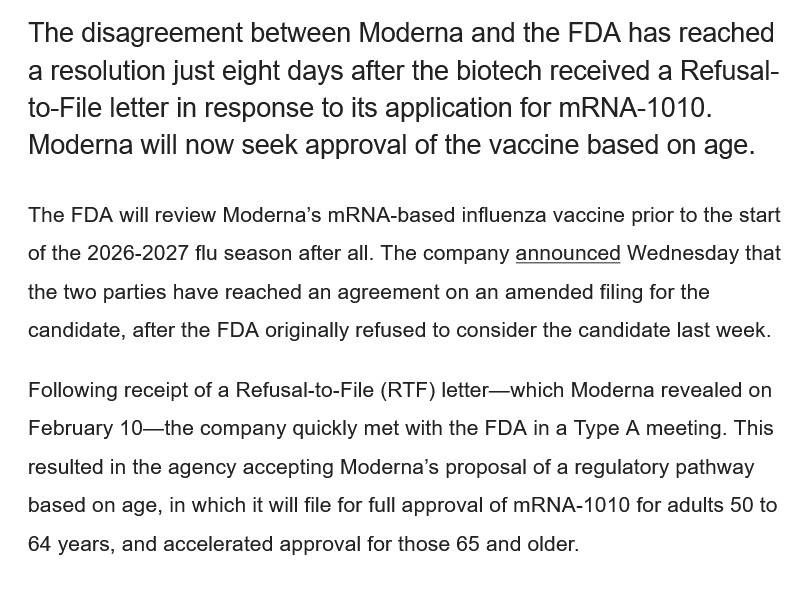
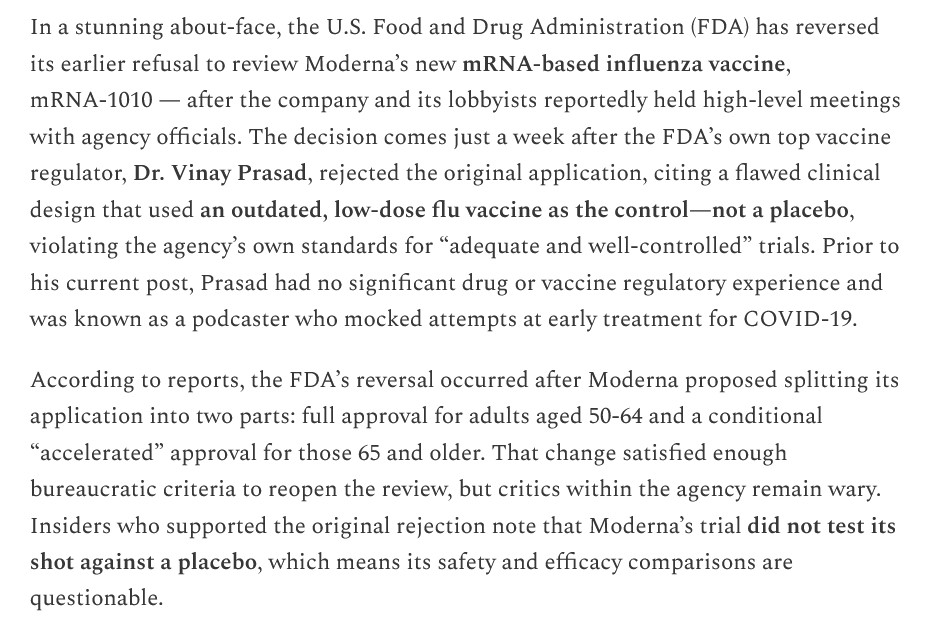
However, by a few days later, the situation had changed completely: the FDA “reversed course”, agreeing to review Moderna’s BLA (amended) application for mRNA-1010.
By 18 February 2026, a “Type A” meeting had been arranged between the FDA and Moderna regarding the RTF letter. Moderna agreed to submit an “amended” BLA application to the FDA for mRNA-1010. The FDA accepted the amended BLA application. The FDA will make a final decision on approving mRNA-1010 by 5 August 2026. Please see the screenshot, below, from https://www.biospace.com/fda/fda-reverses-course-on-modernas-mrna-flu-shot-application-promising-august-decision, Heather McKenzie, 18 February 2026:
Note that last sentence, by Mr. Faroohar. It clarifies three “behind-the-scenes” aspects of mRNA-1010:
**** One: That Moderna will do whatever it takes to get mRNA-1010 approved — including being “more assertive” with the FDA, and arranging it so that the FDA will “work with” Moderna.
**** Two: That Moderna will do a “post-marketing study” on mRNA-1010 AFTER it is FDA-approved — meaning that ANYONE who takes mRNA-1010 AFTER the FDA approves it is being treated as a “human lab rat” by Moderna. This is the same type of situation that occurred when the FDA approved Moderna’s modRNA COVID-19 bioweapon “vaccine”, mRNA-1273.
**** Three: That Moderna considers the FDA approval of mRNA-1010 as the “stepping-stone” to what the company appears to believe is the “Holy Grail” of modRNA-based “vaccines” — the company’s “combo” modRNA-based influenza + modRNA-based COVID-19 “vaccine”, mRNA-1083 (the clinical trials for which have been completed)
There are, in addition, two other aspects to the situation: What appears to be pressure on Dr. Martin Makary, MD (FDA Commissioner) to “knuckle under” to what Moderna wants; and, what appears to be a coordinated campaign to have Dr. Vinay Prasad removed from his position as CBER division director at the FDA. In Yours Truly’s opinion, these relate to the “sudden arrangement” of the FDA “Type A” meeting between Moderna representatives and the FDA almost immediately after the Refusal to File was issued by Dr. Prasad. Please see the screenshots, below, from https://www.biospace.com/fda/makary-prasad-under-fire-as-fda-turmoil-reaches-president-trump, Heather McKenzie, 20 February 2026:
Peter Pitts, by the way, was an FDA employee whose position was that of a “senior communications and policy adviser” of the agency (https://www.centerforbiosimilars.com/authos/peter-pitts.) It appears that Mr. Pitts and CMPI are involved in a campaign to have Dr. Prasad removed from the FDA.
In Yours Truly’s opinion: Dr. Martin Makary is compromised, due to his involvement with BIO.org/, the group that is implementing a campaign to have HHS Sec. Robert F. Kennedy, Jr., removed; and, Dr. Prasad is compromised, due to what appears to be lack of support within FDA, combined with innuendoes regarding his professional behavior at the agency.
In Yours Truly’s opinion, It appears that there is a combination of chaos, mistrust, internecine feuding, and active resistance going on within the FDA; plus, exterior pressure on the agency from companies and other entities to restore the FDA back to the “good old days”, when drugs and other biologics were authorized and approved in what may be called a kind of “rubber-stamp” process. It also appears that HHS Sec. Kennedy, Jr., is either being “kept out of the loop” regarding what is going on with the FDA; or, cannot, for whatever reason, root out personnel within the FDA who are fomenting trouble.
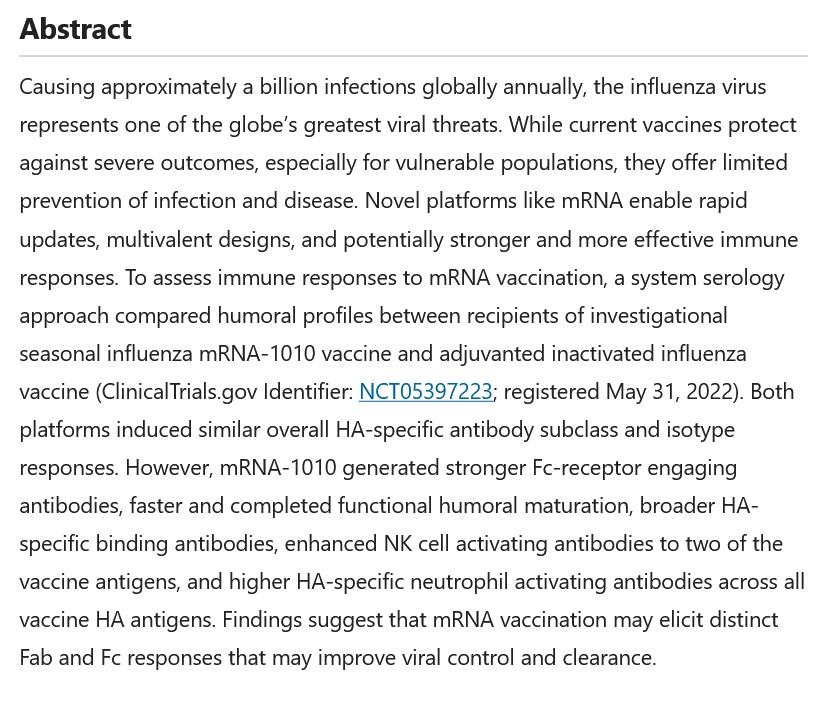
Yours Truly now turns to the Moderna-funded published paper on mRNA-1010, which was cited by Dr. Prasad as the reason for his issuing the Refusal to File letter to the company: https://doi.org/10.1038/s41541-025-01340-5. “mRNA-1010 influenza vaccine elicits distinct and enhanced humoral immunity compared to adjuvanted inactivated vaccines.” Paulina Kaplonek, et al. 15 December 2025. Moderna completely funded this study; all of the paper’s co-authors are either current or former Moderna employees; and, the current Moderna employees who are co-authors of the paper are also stockholders in the company. All of these in and of themselves, in Yours Truly’s opinion, represent massive conflicts of interest that should, under normal circumstances, disqualify the paper from any serious consideration by the FDA for a BLA application review. This is aside from the flaws in the clinical trial NCT05397223, on which the paper was based (more on this below in today’s offering.) Please see the screenshots from this paper, below:
Note the use of the word, “may.” This word is used in several areas of the paper, as in, “may elicit”; “may reflect”; and, “may induce.” In other words, Moderna does not KNOW if mRNA-1010 can actually be helpful against influenza. The company is guessing that it “may.” However, the company is still pursuing the BLA application with the FDA to get the “vaccine” approved — without having provided ANY proof that the “vaccine” actually does what it is “supposed” to do — which is, to prevent influenza infection better than the licensed influenza “vaccines” already on the market.
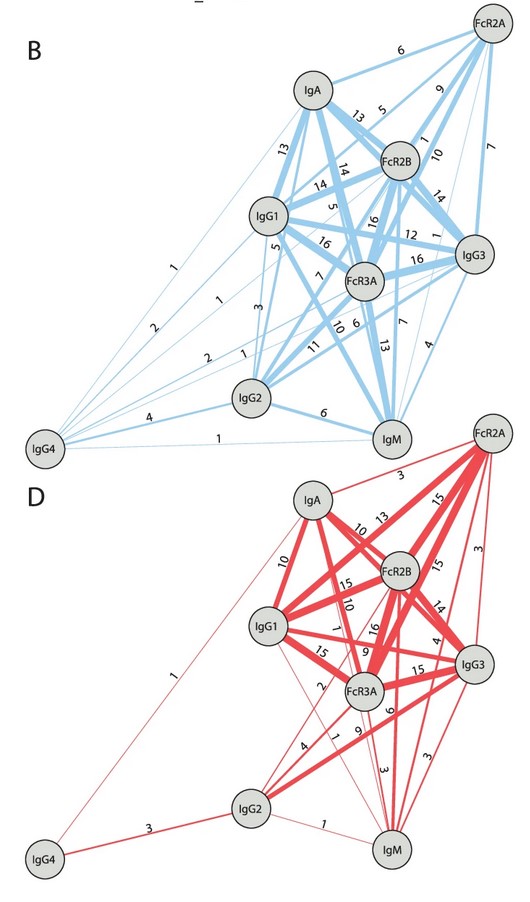
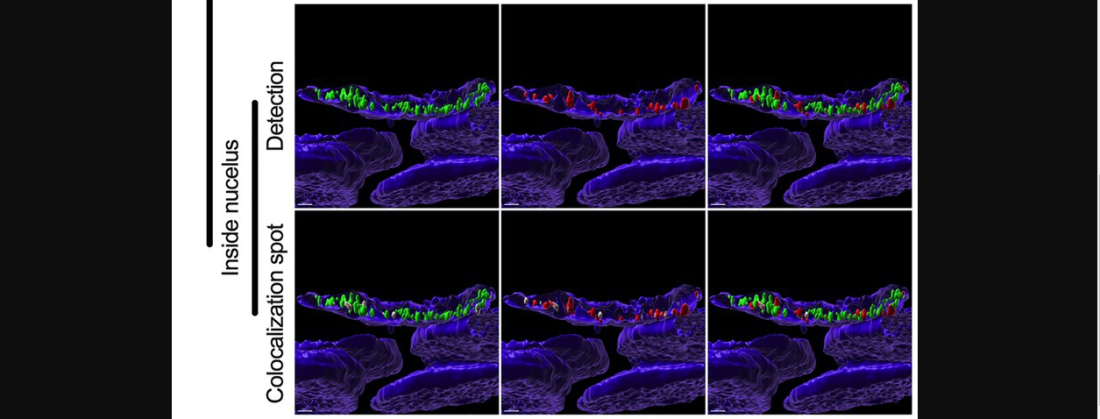
The following screenshots from the paper relate to how mRNA-1010 works, including: Figure 4B and Figure 4D, which show that the “vaccine” minimizes the crucial natural body’s activity of IgM cells (the “recognize an enemy and signal the other cells” immune cells); which show that there is an apparent increase of IgG4 cells (the “tolerate but never clear” cells); and, which appear to hint at mRNA-1010 being used as a kind of “universal influenza vaccine” candidate:
The blue image is the results of the “comparator influenza vaccine”, FLUAD; the red image is the results of mRNA-1010.
Then, from the section that discusses the results of Figure 4B and Figure 4D:
The Moderna paper co-authors did not prove that mRNA-1010 provides mucosal protection from influenza.
Following is a screenshot from the paper regarding the non-involvement of IgM cells induced by mRNA-1010:
Followed by the “hint” that mRNA-1010 may be used as a “universal influenza vaccine” candidate:
Finally, the Acknowledgements section, and the Ethics Declarations section, of the paper:
As shareholders in Moderna, the above employees (and co-authors of the paper on mRNA-1010) stand to make money off the sale and use of this “vaccine.”
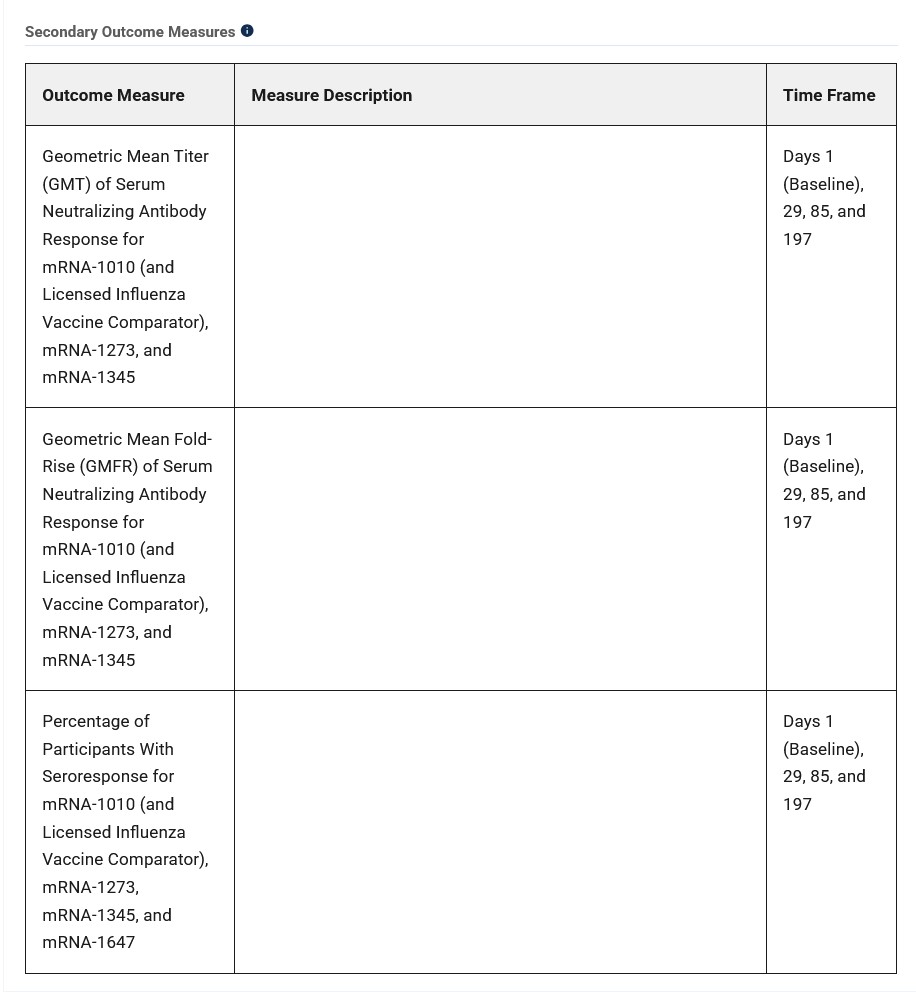
**** Regarding the clinical trial which was the foundation for the Moderna paper that was published on 15 December 2025, NCT05397223, details of which are found here: https://clinicaltrials.org/study/NCT05397223. This clinical trial did NOT have a true saline placebo Control Group. Per the Clinical Trials website, there are TWO separate parts to the study. In Part One, study subjects received injections of: of mRNA-1345 (a modRNA-based “vaccine” against RSV); or, of mRNA-1647 (a modRNA-based “vaccine” against Cytomegalovirus);, or, of mRNA-1273 (the modRNA COVID-19 “vaccine”), all by Moderna. In Part Two, study subjects received injections of either: FLUAD (the “comparator” licensed inactivated influenza vaccine by Seqirus); or, of mRNA-1010. Please see the screenshot, below, from the Clinical Trials website for NCT05397223, the Secondary OutcomesMeasures section:
However,there is not a single word in the Moderna-funded paper cited above in which the outcomes for ANY of the “vaccines” used on the study subjects otherthan FLUAD or mRNA-1010, are found. Nothing for mRNA-1345, for mRNA-1647, or for mRNA-1273. It is unknown if any of these three “vaccines” induced any interactions with either FLUAD or with mRNA-1010. There are “No Results Posted” on the Clinical Trials website for NCT05397223.
Moderna has been in the process of developing and testing mRNA-1010 for the past several years. The company applied pressure, which apparently went all the way up to the Oval Office, in order to force the FDA to reverse course and agree to review the (amended) BLA application for mRNA-1010, despite the flaws of the clinical trial NCT053972723, and despite the Refusal to File letter sent by Dr. Vinay Prasad.
To be continued in Part Two.
THERE IS NO PLACE IN THE HUMAN BODY FOR AN mRNA-BASED, modRNA-BASED, saRNA-BASED, OR taRNA-BASED PRODUCT IN ANY FORM.
Peace, Good Energy, Respect: PAVACA
(intellectual Property Disclaimer and Notice: With the exception of linked items that are found on the internet, the ideas and opinions of today’s offering are by PAVACA. Credit must be given to PAVACA if ideas or opinions in today’s offering are used by other blog writers; by podcasters; or in social or print media.)
The header image for today’s post is courtesy of iStock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering speaks to the disaster of the COVID-19 “vaccines”, Yours Truly dedicates it to all persons, of whatever age or location, who have passed away from the negative effects of the COVID-19 “vaccines” that they had injected into their body.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is one AI-generated image in The Focal Points article, cited below. If readers wish to add any AI-generated content to the discussion thread for today’s offering, they must cite their source. Thank you.
The phrase to keep in mind when reading today’s post is: Follow the money.
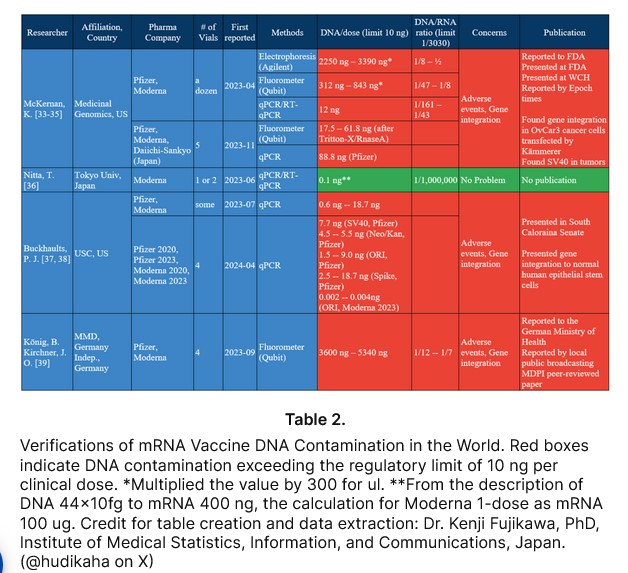
Today’s post begins here: https://www.thefocalpoints.com/p/fda-commits-grave-betrayal-fully, “FDA Commits Grave Betrayal: Fully Approves Deadly Genetic Injections for Infants”, by Nicolas Hulscher, MPH, 11 July 2025. There is an embedded video interview with Mr. Hulscher in this article. This article and interview regard the FDA “full approval” on 10 July 2025 of the Moderna modRNA COVID-19 “vaccine”, SPIKEVAX, to be used on infants and young children from age 6 months to 11 years old. A screenshot of a portion of the Table 2. from this article is below, showing the amounts of “loose” DNA in this “vaccine”:
Yours Truly now turns to a crucial component of the Moderna modRNA COVID-19 “vaccine” situation: the “tied to the hip” relationship that this company has with the NIAID (National Institute of Allergy and Infectious Diseases), part of the NIH (National Institutes of Health.) Both the NIAID and the NIH are institutes of the federal government Department of Health and Human Services (HHS.) Katherine Watt, of Bailiwick News, has studied and written about the “coziness” between Big Pharma entities such as Pfizer-BioNTech and Moderna with federal government agencies, such as the FDA. Please see: https://bailiwicknews.substack.com/p/why-pfizer-and-moderna-and-fda-are, “Why Pfizer and Moderna and FDA are working toward government authorization to inject babies and small children”, 23 March 2022. Ms. Watt includes a statement made by Robert F. Kennedy, Jr. in 2021, on this situation. Please see: https://wsau.com/2021/12/31/robert-f-kennedy-jr-explains-why-fauci-is-going-after-children/, by Meg Ellefson, 31 December 2021. A screenshot from the Bailiwick News article on this is below:
There are SEC filings and “Confidential Agreements” between Moderna, the FDA. and the NIAID, regarding the funding and development of mRNA “vaccines.” There are patent co-ownership and revenue-sharing agreements between Moderna and the NIAID. There is a Moderna – NIH Confidential Agreement that goes back to 2015.
By the way, milestone payments would include payments for items such as, developing the “latest version” of a COVID-19 modRNA “vaccine” — for examples: the Moderna (SPIKEVAX) “2025-2026 COVID-19 Formula Vaccine” that was just “recommended” by the ACIP committee of the CDC; and, the FDA “full approval” of SPIKEVAX being used on infants and young children age 6 months to 11 years old, which “full approval” was granted on 10 July 2025. It appears that Moderna had attempted to “modify” or “avoid” certain types of sharing agreements stipulations, royalty payments to the HHS (via the NIAID), and HHS – Moderna co-owned patents agreements; and, for which, the company was taken to court by the HHS. The decision was rendered against Moderna, with an order to make a multi-million dollar “catch-up payment” to HHS -NIAID.
Now, to the 2015 “Confidential Agreements” between Moderna and the NIH. The document is found here: https://www.documentcloud.org/documents/6935195-NIH-Moderna-Confidential-Agreements/, November 2015. This document has numerous “amendments” and “additions” that go through the year 2018 — and, the last of which appears to “cover” all items related to COVID-19 “vaccines”. On page 16 of the document, with special attention to page 19, start the CRADA stipulations (Cooperative Research and Development Agreement stipulations between Moderna and the NIH.) The language here has numerous Proprietary Information redactions; however, it appears to be broad enough to cover the later co-ownership by Moderna and the NIH of the SPIKEVAX patents and their Expiry Dates (more on these below.)
Here are page 19 and a portion of page 20 of the NIH/NIAID and Moderna CRADA agreement, below:
Recall that the director of the NIAID in 2015 was Dr. Anthony Fauci; and, the director of the NIH in 2015 was Dr. Francis Collins.
Page 41 of this document names the “partners” that will be included in the agreements: DARPA; BARDA; and, the Bill and Melinda Gates Foundation.
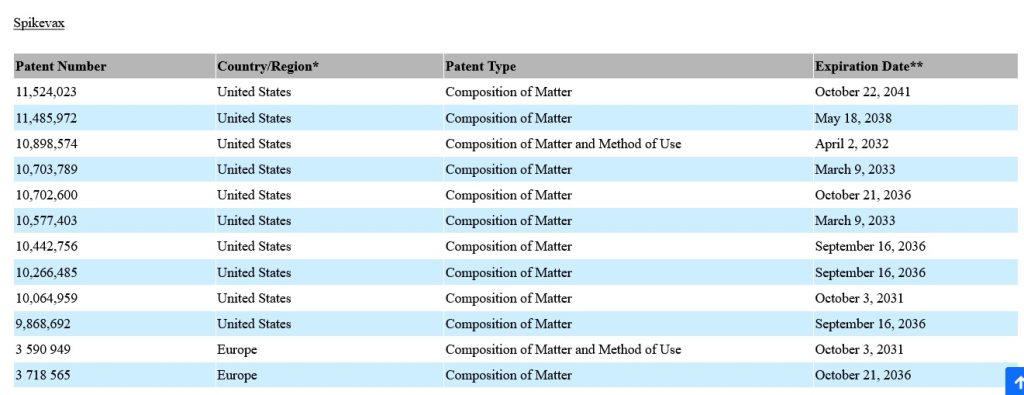
Page 43 of this document details the SPIKEVAX patents and Expiry Dates that will be co-owned by Moderna and the NIH. A screenshot of this page is below:
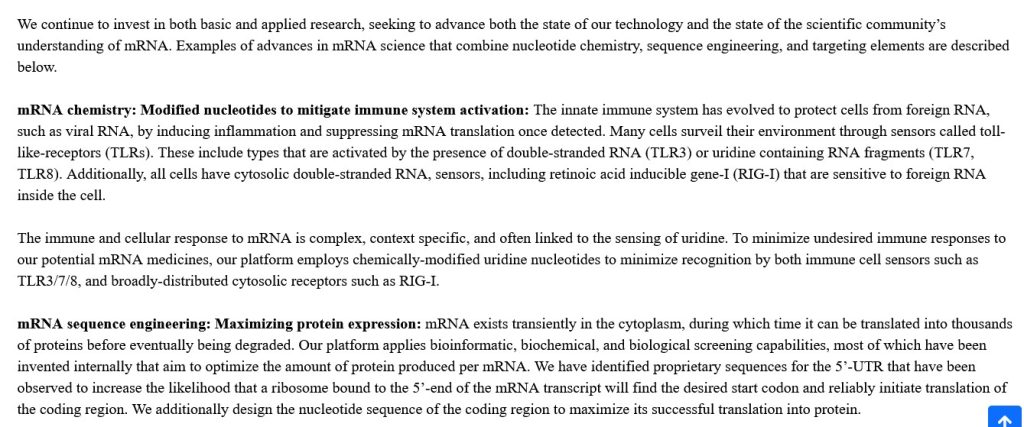
There is also a “vaccine mechanisms” series of sections in this agreement. A screenshot of one of these sections is below:
And, there is a section regarding the “Drug Design Studio” section of the SEC document. Please see the screenshot from this section, below:
On 7 July 2025, HHS Secretary Robert F. Kennedy, Jr., cancelled the 10 July meeting that was scheduled for the USPSTF committee of the HHS (United States Preventive Services Task Force committee.) If Sec. Kennedy, Jr., can do this, why can’t he do something to modify / rescind / cancel the NIH / NIAID – Moderna “Confidential Agreements”, the related royalty-sharing payments agreements, and the 31 December 2022 SEC filing? Is it because of the “SPIKEVAX Patents and Expiry Dates” agreement, the screenshot of which from the SEC filing is above, and which runs, in total, until 22 October 2041? Are his hands tied? “Inquiring minds want to know.”
FLASH ADDENDUM: Our good Gail Combs asked to have the following added to today’s offering, regarding the development of a new BLACK PLAGUE strain variation that was just done by scientist in Israel. Yours Truly is also adding another item related to other work developing BLACK PLAGUE strain variations.
ISRAELI scientists have just developed an mRNA-based BLACK PLAGUE (Yersinia Pestis, or Y. Pestis) vaccine, using a lab-modified gene and adding N1-Methylpseudouridine as the lipid nanoparticle “delivery system.” Please see: https://jonfleetwood.substack.com/cp/168494356, “Israel Engineers Mutant Plague — Puts Its Genes in mRNA Shot That Makes Human Cells Produce Virulence and Immune-Evasion ‘Black Death’ Proteins: Journal ‘Advanced Science'”, 16 July 2025. This is the “BLACK PLAGUE version” of the modRNA + N1-Methylpseudouridine COVID-19 “vaccines” — except that the “payload” is a lab-created genetically altered and more virulent version of the BLACK PLAGUE.
Recall that Yours Truly has written extensively about the mechanism of the N1-Methylpseudouridine used in the Pfizer-BioNTech and in the Moderna modRNA COVID-19 “vaccines” (there’s the connection to Moderna.) This lab-created compound ingredient replaces the natural Uridine in the COVID-19 “vaccinated” person’s body, kicking the door wide open for catastrophic immune system evasion by said “vaccine”: evasion that will occur throughout the body and also the brain. The connection to both Moderna and to Pfizer-BioNTech in regards the use of N1-Methylpseudouridine is that BOTH companies specifically included this lab-created chemical compound in their modRNA COVID-19 “vaccines”, the description of which inclusion IS IN THE PATENT DOCUMENTS THAT WERE FILED BY EACH COMPANY. This begs the question: Did the Israeli scientists pay either Pfizer-BioNTech or Moderna for the “rights” to use this compound IN THEIR BLACK PLAGUE VARIATION “VACCINE” EXPERIMENTS?
The peer-reviewed paper that is referred to in the Jon Fleetwood article is here: https://doi.org/10.1002/advs.202501286, “Novel Bivalent mRNA-LNP Vaccine for Highly Effective Protection Against Pneumonic Plague”, Dan Peer, et al., 25 April 2025. A screenshot from the Fleetwood article is below:
But wait, there’s more! The Fleetwood article links to a paper published in 2024 regarding research by the United States Army Combat Capabilities Development Command Chemical Biological Center in Gunpowder, Maryland, ALSO on lab-creating a variation of the BLACK PLAGUE. This variation was “cultured” in a “bath” of Escherichia coli (E. coli, the same type of “culturing material” that is used by both Pfizer-BioNTech and by Moderna to produce their respective modRNA COVID-19 “vaccines.” The paper is here: https://doi.org/10.1099/acmi.0.000723.v3, “Towards a Yersinia Pestis lipid A recreated in an Escherichia coli scaffold genome”, Nathan D. McDonald, Erin E. Antoshak, 17 July 2024. A screenshot of the Abstract of this paper is below:
In Yours Truly’s opinion: The entire “let’s make a lab-created RNA + lipid nanoparticle vaccine” situation is out of control. The entire “let’s alter a gene or two from a deadly infectious disease and make a variation of this disease” situation is out of control.
The above image of TLR Signalling Pathways is courtesy of BioFinder and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s offering is related to the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created Biological ToxinWeapons.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post any AI-generated content in today’s discussion thread, they must cite their source. Thank you.
And now, to the reader’s Edification Smorgasbord, a “feast of information” regarding just how dangerous and potentially deadly mRNA-1283 (mNEXSPIKE) is, Yours Truly offers the following Menu:
APPETIZER: WHAT IS TLR4?
TLR4 (aka Toll-like receptor 4) is a transmembrane protein that exists across a cell membrane. TLR4 functions as a kind of “sensing device” within the body. It detects foreign bacteria and viruses. When a foreign element is detected by TLR4, it begins to send messages to the natural immune system to activate the immune response. TLR4 is crucial to the correct functioning of the natural immune system. Please see the screenshots below for more information:
FIRST COURSE: THE FDA APPROVES “mNEXSPIKE” IN MAY 2025:
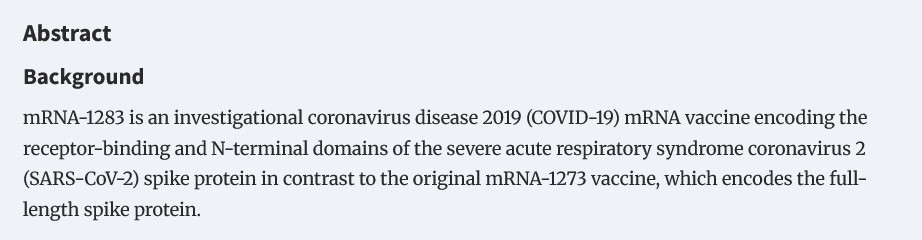
The “newest version” COVID-19 “vaccine”, mRNA-1283 (aka mNEXSPIKE), was “fully approved” by the FDA on 30 May 2025. Yours Truly wrote about this situation here: https://www.theqtree.com/2025/06/01/stop-press-edition-hhs-secretary-robert-f-kennedy-needs-to-resign-now/. This “vaccine” claims to be “more effective” in “preventing” an infection of COVID-19. The claim is based on the fact that mRNA-1283 (aka mNEXSPIKE) uses “only” the S1 protein and the N sector of said S1 protein of the COVID-19 virus spike protein, as opposed to using the entire spike protein (as in mRNA-1273, the original “flagship” modRNA COVID-19 “vaccine” by Moderna.) Please see: https://doi.org/10.1093/infdis/jiaf022, “Safety and Immunogenicity of SARS-CoV-2 Spike Receptor-Binding Domain and N-Terminal Domain mRNA Vaccine”, Spyros Chalkias, et al., 15 April 2025 (most of the authors of this “informational paper” are either affiliated with Moderna, or are employees of Moderna.) A screenshot of the Background section of the Abstract of this paper is below:
At first glance, this “new development” by Moderna may appear to be a “positive” achievement. However, there are other issues that arise:
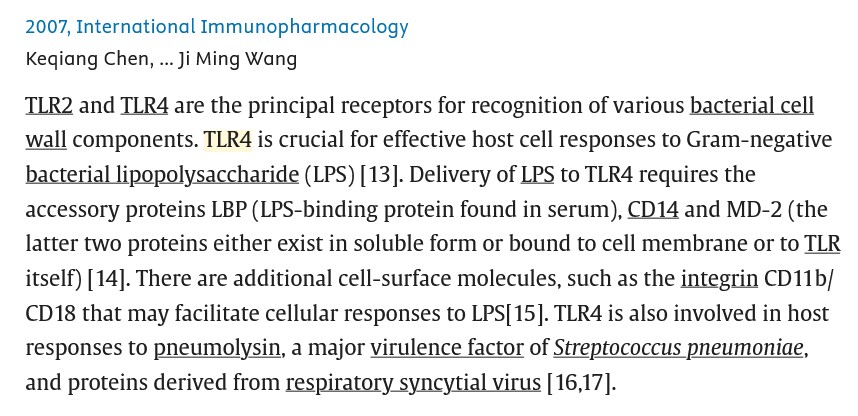
First, there is the fact that the S1 protein of the SARS-CoV-2 virus contains both the RCB (Receptor-Binding Domain) AND the N-terminal domain of the virus. It is the RCB that allows the virus to “attach” itself , or to “dock” itself, to cells in the body — for example, to the ACE2 cell receptors; and, to TLR4 cells. The N-terminal domain is the “end part” of the S1 protein; it is a “free” group at the end of the protein, while, at the same time, it “initiates” a polypeptide chain.
While the above article refers to the Pfizer-BioNTech modRNA COVID-19 “vaccine” BNT162b2, the modRNA COVID-19 “vaccine” from Moderna, mRNA-1273, also targets the RBD, which interacts with TLR4 cells in the “vaccinated” person’s body. In addition, all of the modRNA “descendant clone” COVID-19 “vaccines” by both companies also use the RBD, there interacting with TLR4 cells in the “vaccinated / boosted” person’s body.
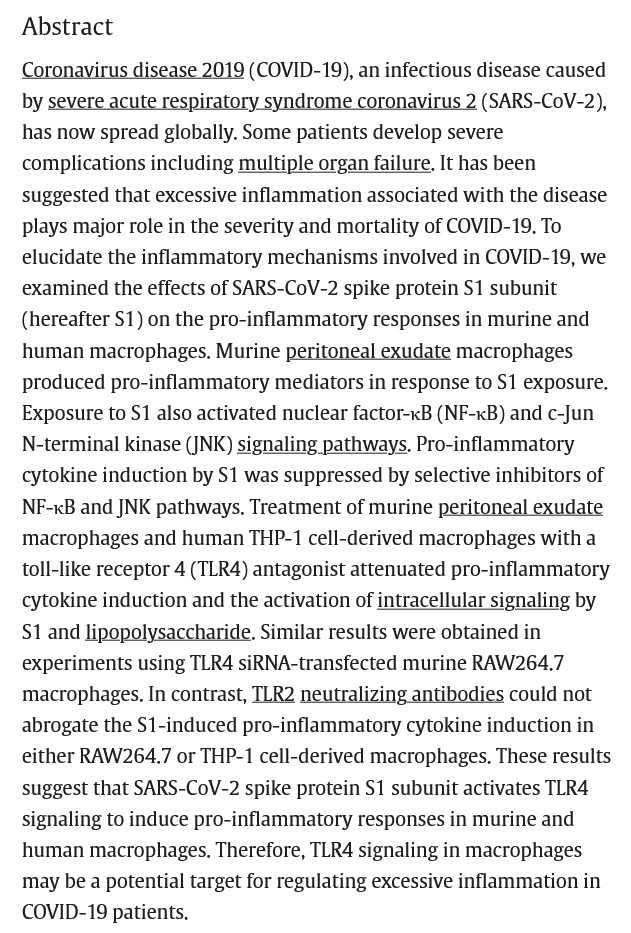
TLR4 cells are also present in multiple areas and organs of the body. The modRNA COVID-19 “vaccines” will interact with these cells. This is due to the fact that the S1 protein of the SARS-CoV-2 virus contains certain amino acids residues (numbers 1-1208) that interact with TLR4 cells. Please see: https://doi.org/10.1016/j.heliyon.2021.306187, “SARS-CoV-2 spike protein S1 subunit induces pro-inflammatory responses via toll-like receptor 4 signaling in murine and human macrophages”, Ken Shirato, Takako Kizaki, February 2021. A screenshot of the Abstract of this paper follows:
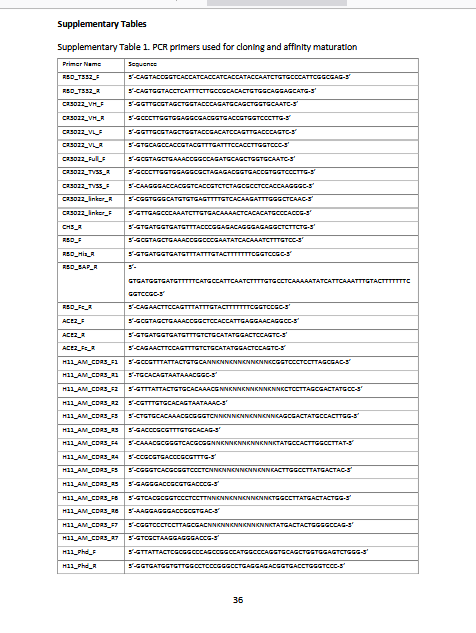
Regarding the S1 amino acids residues 1-1208 and TLR4, please see this paper, from 2020: https://europepmc.org/article/ppr/ppr170060, ” Structural characterization of a nanobody derived from a naive library that neutralizaes SARS-CoV-2″, M Dumoux, et al., 1 June 2020. Below are screenshots from the Methods section and from a portion of the Supplementary Table section of this paper (the Supplementary Table portion shows some of the gene code for the S1 1-1208 residues):
Further information regarding SARS-CoV-2 spike protein and its interaction with TLR4 is found here: https://doi.org/10.3389/fimmu.2024.1368946, “TLR2/4 are novel activating receptors for SARS-CoV-2 spike protein on NK cells”. Nadine Landolina, et al., 30 May 2024. “NK” stands for “Natural Killer” cells in the body. A screenshot from this paper is below:
Then, there is the issue of clinical trial used by the FDA to “justify” the “full approval” of mRNA-1283 (aka mNEXSPIKE), NCT05137236 (https://clinicaltrials.gov/study/NCT05137236.) There was NO Placebo Control Group in this study. The study participants (study subjects) were injected with the following Moderna modRNA COVID-19 “vaccines”: mRNA-1273; OR, mRNA-1283; OR, mRNA-1283.211; OR, mRNA-1283.529. Why was there no Placebo Control Group? Assuming that the study subjects knew, in advance, they would be injected with any one of FOUR different variations of a modRNA COVID-19 “vaccine”, were they fine with that?
And, there is the “opinion piece” by Dr. Martin Makary (FDA Commissioner) and Dr. Vinay Prasad (new head of the FDA’s CBER division), regarding the “new approach” that the FDA will use for COVID-19 “vaccines.” Please see:
SECOND COURSE: WHAT DOES THE modRNA COVID-19 “VACCINE”, mNEXSPIKE, CONTAIN?
Please see the FDA-issued Fact Sheet for Healthcare Providers (aka the Package Insert) for mRNA-1283, mNEXSPIKE: https://www.fda.gov/media/186738/download. Below is a screenshot of section 11 Description, section 12 Clinical Pharmacology, and section 13 Nonclinical Toxicology of this document:
Which plainly states that mNEXSPIKE contains the same types of dangerous, deadly lipid nanoparticle and excipient that all the other modRNA COVID-19 “vaccines” by Moderna contain: SM-102, and PEG2000-DMG. This means that mNEXSPIKE will be rapidly spread into every cell in the “vaccinated” person’s body. It is also clear that mNEXSPIKE has NOT been tested for mutation potential, cancer-inducement potential, or reproductive impairment potential.
Yours Truly then performed a search to ascertain whether or not mNEXSPIKE contains N1-methylpseudouridine. She has written extensively on this board about this lab-created “fake Uridine plus a form of methane”, which completely replaces the natural RNA in the Uridine in the body. Recall that natural Uridine is crucial to multiple body functions and mechanisms: regulation of mood, of learning and memory, and of “gut-brain connection” functions. Lo and behold, the US Patent for mRNA-1283 (aka mNEXSPIKE) does have language describing “various types” of pseudouridine, including N1-methylpseudouridine, are used in all of Moderna’s modRNA COVID-19 “vaccines” — which would also include mNEXSPIKE. The US Patent for mRNA-1283 is found here (US 20240382581A1): https://patents.google.com/patent/US20240382581A1/en?q=(mRNA-1283)&oq=mRNA-1283, “Pan-human coronavirus vaccines”, ModernaTX, published 21 November 2024. Please see sections 0120, 0121, 0122, and 0123 of this document for descriptions of the “various types” of pseudouridine.
Lastly, there is the question as to whether mNEXSPIKE contains any saRNA (self-amplifying RNA) component. Yours Truly searched for information regarding this, since the IM dose (intramuscular injection dose) of this COVID-19 “vaccine” is a very small amount — 0.2mL. She found this, which appears to be a “dancing all around the truth” description of this “vaccine.” Please see: https://synapse.patsnap.com/article/what-is-mrna-1283-used-for?, 28 June 2024. A screenshot from this article is below:
Read the last sentence in the second paragraph above, especially “…a robust and durable immune response, potentially requiring fewer doses and offering longer-lasting immunity compares to other vaccines.” Sounds like a description of the saRNA H5N1 “vaccine”, KOSTAIVE, currently approved for use in the EU / Scandinavia, and in Japan; and, a version of which “vaccine” is to begin clinical trials in the United States (NCT06602531), under the name ARCT-2304.
DESSERT AND BEVERAGES: REACTIONS AND QUESTIONS:
First, this: https://www.thefocalpoints.com/p/maha-movement-flabbergasted-covid, “MAHA Movement Flabbergasted COVID-19 Vaccines Remain on Market”, Peter A. McCullough, MD, MPH, 2 June 2025. There is an embedded interview with Dr. McCullough in this article, along with a linked copy of the “Kabuki Theater performance” regarding “stopping” the COVID-19 “vaccines” in the United States by Dr. Martin Makary (FDA), Dr. Jay Bhattacharya (NIH DIrector), and HHS Secretary Robert F. Kennedy, Jr., on 27 May 2025. A screenshot from the McCullough article is below, giving his views on the current situation:
Second, this tweet, from Dr. William Makis: https://x.com/MakisMD/status/1930296443434348771, 4 June 2024. Two screenshots from his tweet are below: first, a statement from HHS Secretary Kennedy, Jr.; and, second, from Dr. Makis:
Questions, posed by Yours Truly: Why did the FDA “fully approve” a “new”, modRNA COVID-19 “vaccine” that specifically targets person over age 65, and persons who “fit” a detailed list of “persons at risk of severe COVID-19 infection”, as complied by Dr. Martin Makary and Dr. Vinay Prasad? Why was there a “Kabuki Theater performance” on 27 May 2025 by Drs. Makary and Bhattacharya, along with HHS Secretary Kennedy, Jr., when it was obvious by that date that the FDA “full approval” of mNEXSPIKE was “a done deal”? Why did the FDA issue an Approval Letter to Moderna for mNEXSPIKE that has so many “caveats”, “requests for more information”, and an “order” for the company to perform a Phase 4 clinical study on the “vaccine” — a “vaccine” that the FDA had just “fully approved”? Please see: https://www.fda.gov/media/186740/download; and, the screenshot of Page 9 of this document, regarding the “order” for the Phase 4 study, below:
More questions, posed by Yours Truly: How many elderly persons are going to be pressured / cajoled / “mandated” (by the nursing home or care facility where they live), to take mNEXSPIKE? Will they be told that this injectable is “safer” than mRNA-1273, “because the dose is smaller”? What about persons who “fit” into the multiple categories of “persons at high risk for severe COVID-19 infection” according to Drs. Makary and Prasad? What pressure will these persons be subjected to in order to get them to agree to take mNEXSPIKE? Finally, will people be told the truth that mNEXSPIKE, just because it does not contain the S2 portion of the SARS-CoV-2 spike protein, is NOT “mRNA-1273 Lite” — but, rather, it is another version of a dangerous, potentially deadly modRNA COVID-19 ‘”vaccine”?
The above image of a vintage vaccine vial and syringe is courtesy of Google Images.
This post is a STOP PRESS EDITION. It has to do with the FDA BLA (Biologics License Application) approval of the Moderna COVID-19 modRNA “vaccine” mRNA-1283. This “vaccine” was FDA-approved without any clinical trial in which there was a placebo control group. mRNA-1283 contains a “shorter portion” of the COVID-19 virus spike protein. This “vaccine” also contains elements of the H7N9 Avian Influenza strain that was used in Gain-of-Function experiments by Dr. Yoshihira Kawaoka, DVM, PhD, in 2013, along with other scientists, at the University of Wisconsin (Madison.)
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked this post for any AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post any AI-generated content in the discussion thread of today’s offering, they must cite their source. Thank you.
Please see the following breaking news outlets pieces regarding the FDA granting the BLA for the Moderna “newest COVID-19 “vaccine”, mRNA-1283: First, this one: https://www.thefocalpoints.com/cp/164898171, “BREAKING: FDA Goes Rogue — Approves Moderna’s Next-Gen COVID-19 mRNA Injection Without a Placebo-Controlled Trial”, Nicolas Hulscher, May 2025. Please see the screenshots from this article, below:
HOWEVER, there is another aspect to the mRNA-1283 modRNA COVID-19 “vaccine” — this injectable appears to be a combination of BOTH the SARS-CoV-2 virus AND elements of the deadly H7N9 Avian Influenza virus. Please see: https://jonfleetwood.substack.com/cp/164803097, “FDA Approves Moderna COVID Jab Containing GOF Bird Flu Gene Segment That PCR Could Mistake for Infection”, 31 May 2025. The “bird flu gene segment” is from the Gain-of-Function experiments with the H7N9 Avian Influenza virus conducted by Dr. Yoshihiro Kawaoka, Ron Fouchier, and other scientists, under the aegis of the University of Wisconsin (Madison), where Dr. Kawaoka has his lab. These Gain-of-Function experiments were “outed” when serious lab accidents occurred; it appears that the experiments were then stopped. But not before Dr. Fouchier wrote this article: https://www.science.org/doi/10.1126/science.1243325, “Gain-of-Function Experiments on H7N9”, 9 August 2013, in which Dr. Fouchier attempted to justify further Gain-of-Function experimentation.
The archived article regarding the H7N9 experiments at the University of Wisconsin (Madison), is found here: https://archive.ph/LX7MP, “Study: Lab-derived H5N1 virus component binds to human receptors”, Robert Roos, 13 April 2013.
In Yours Truly’s opinion, Robert F. Kennedy, Jr., the Secretary of Health and Human Services, is not doing his job. BOTH the FDA and the CDC have now “gone rogue” — first, with the “sleight-of-hand” regarding the CDC’s “new recommendations” about the COVID-19 “vaccines” (per Dr. Susan Monarez, PhD, the current Acting Director of the CDC, as of 30 May 2025); and, second, with the FDA (Dr. Martin Makary, Commissioner) granting approval of the Moderna modRNA COVID-19 + H7N9 gene pieces combination “vaccine”, mRNA-1283 (as of 31 May 2025.) It is time, in Yours Truly’s opinion, for Secretary Kennedy, Jr., to either get control of the FDA and CDC — after all, these agencies are part of HHS — or, to resign, and allow President Trump47 to find someone who will.
FLASH UPDATES! MORE ON THE “DIRTY BACKSTORY” RELATED TO THE FDA’s APPROVAL OF mRNA-1283 ON 30 MAY 2025:
ONE: The FDA’s Approval Letter to Moderna on 30 May 2025, regarding mRNA-1283: https://www.fda.gov/media/186740/download. Please see the screenshot of page nine of this document, below:
This is the PHASE 4 clinical study that Moderna is requested to perform for mRNA-1283, but which has NOT begun yet, nor has it ENROLLED any subjects yet.
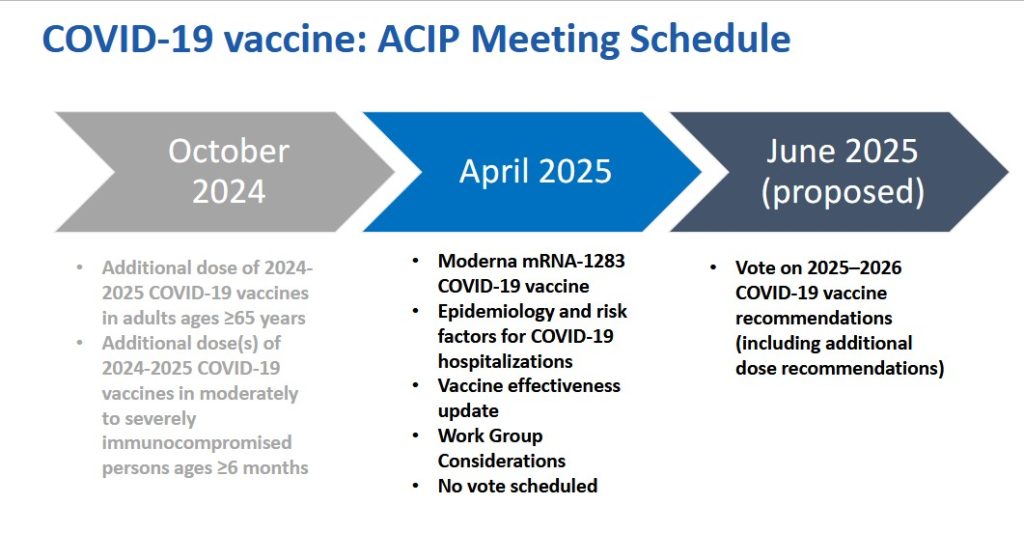
TWO. This is the slide presentation for the CDC’s ACIP committee meeting for April 2025 related to the “2025-2026 COVID-19 Vaccines Formula” selections. Notice that there is NO vote that ACIP planned to take regarding mRNA-1283. Please see: https://www.cdc.gov/acip/downloads/slides-2025-04-15-16/05-Panagiotakopoulos-COVID-508.pdf. Below is a screenshot of the pertinent image from the slide presentation:
The above is a vintage image of mass vaccination. (Courtesy Google Images.)
This series on the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
The origination of today’s post begins here: www.dossier.today/p/double-digits-biden-admin-tells-americans, “Double Digits: Biden Admin tells Americans that it’s soon time for their 10th Covid shot“, by Jordan Schachtel, 13 June 2024. (Mr. Schachtel wrote about the ninth COVID-19 “vaccine” injection here: www.dossier.today/p/dose-number-nine-cdc-panel-green, “Dose number NINE: CDC panel green lights yet another Covid mRNA shot“, 29 February 2024. The CDC recommended that persons over age 65 take another “booster shot” of either the Pfizer-BioNTech or of the Moderna “2023-2024 Formula COVID-19 Vaccine” of these manufacturers.) A person age 65 or older, if that person adhered to every CDC recommendation regarding taking a COVID-19 “vaccine” injection since December 2020 (when the FDA granted first Emergency Use Authorization (EUA) to Pfizer-BioNTech and to Moderna for these companies’ “flagship” modRNA COVID-19 “vaccines” (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), would have taken injection number nine starting on 28 February 2024.
Today’s post is long. There is a large amount of information to “unpack.” Stay with me here.
Note the language regarding the “selection of a specific JN.1 lineage SARS-CoV-2 strain…” More about that later.
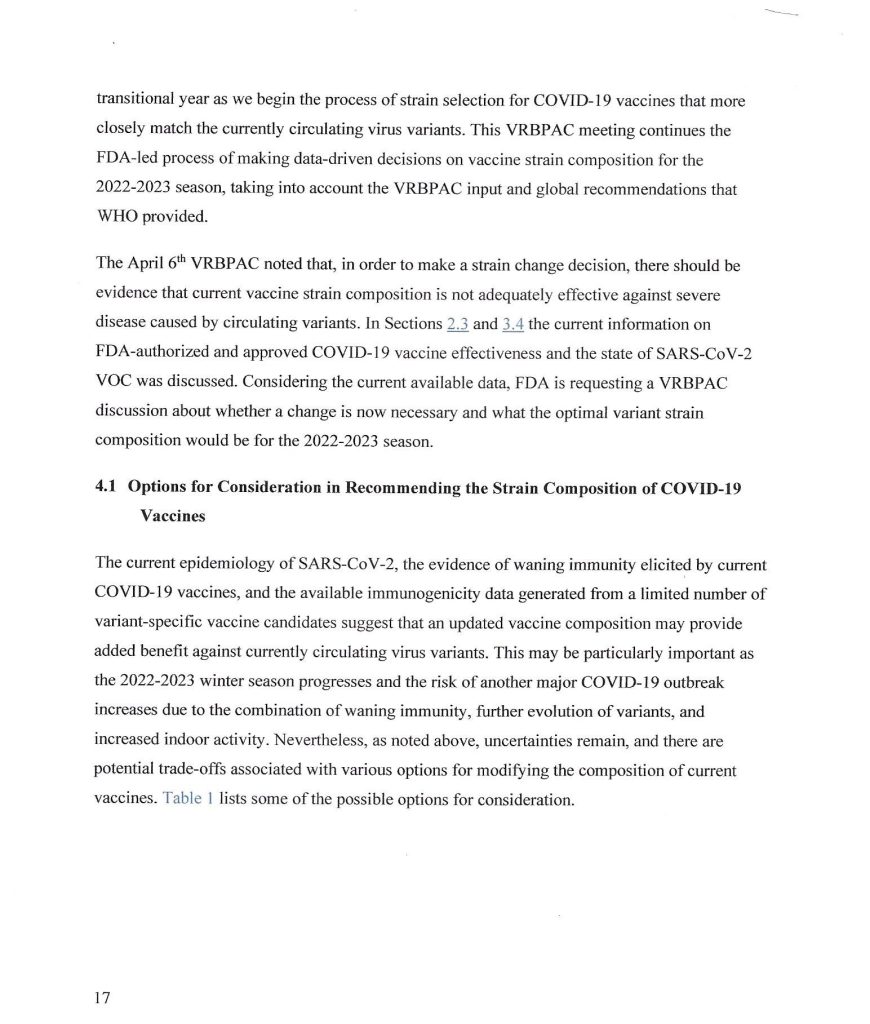
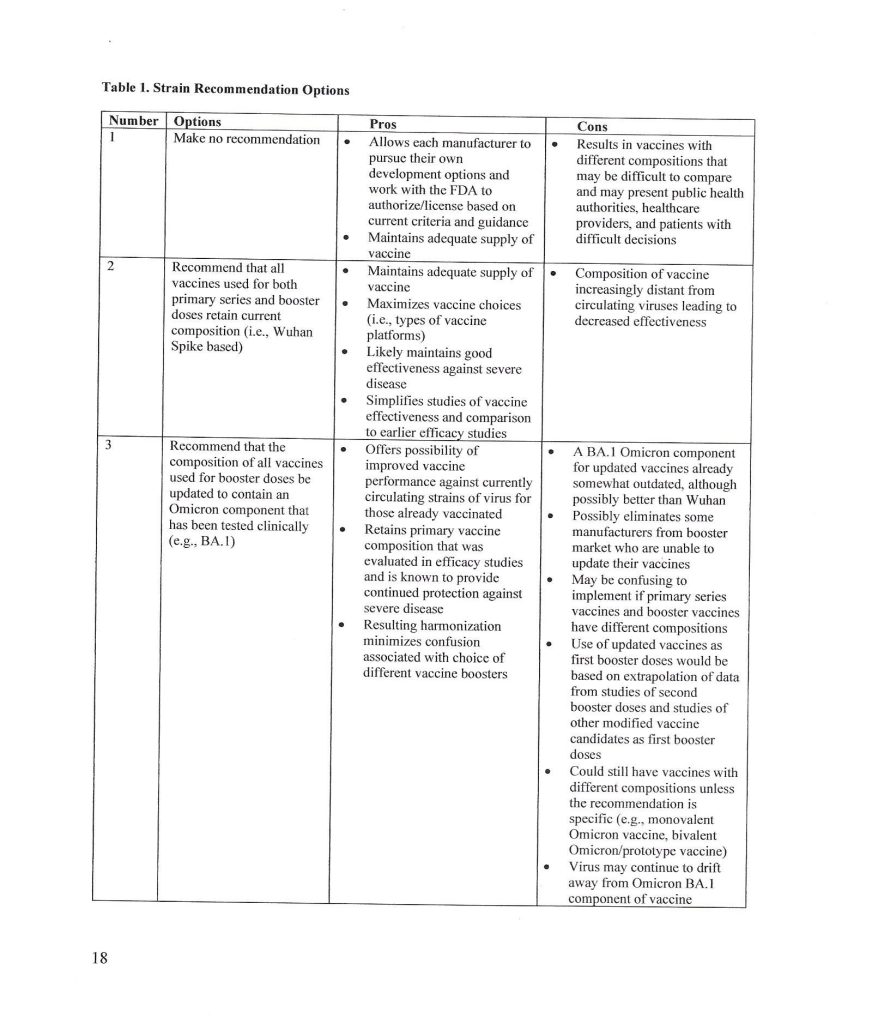
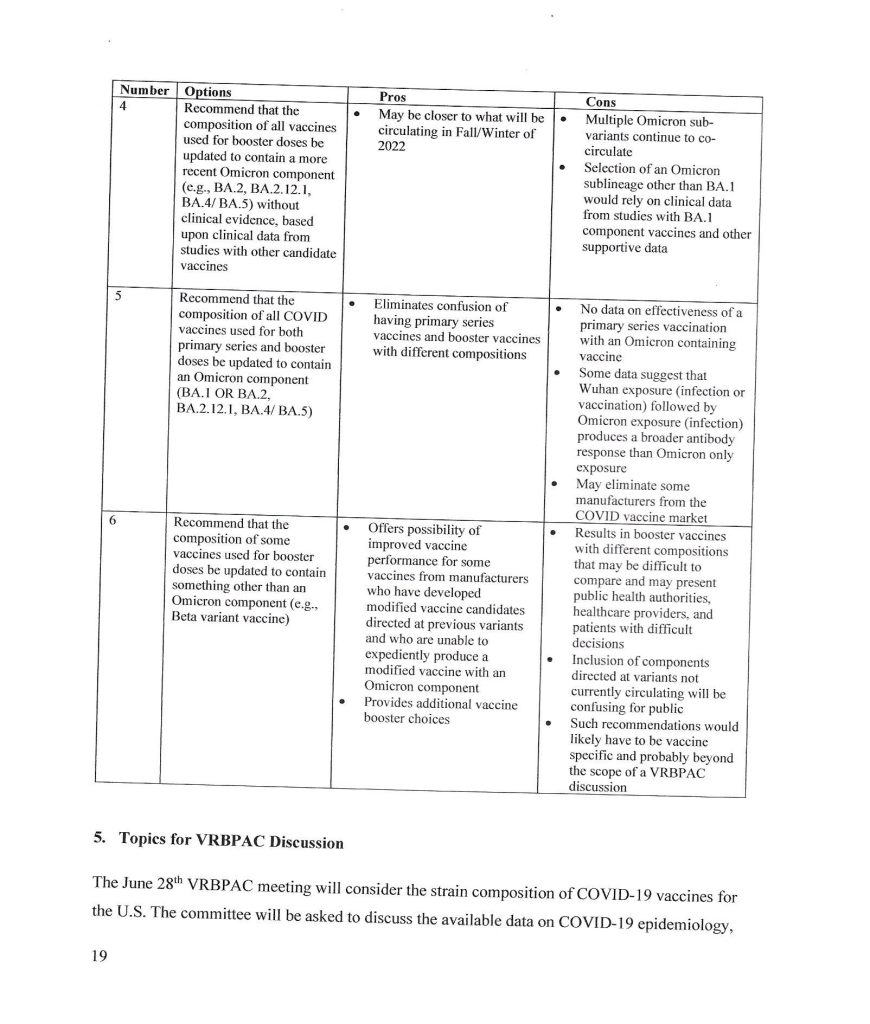
The trail behind the 5 June 2024 FDA announcement begins with the VRBPAC Briefing Document for the meeting held on 28 June 2022: www.fda.gov/media/159452/download, “FDA Briefing Document Vaccines and Related Biological Products Advisory Committee Meeting June 28, 2022.” It was at this meeting that the FDA “codified” the types of “strain composition recommendations” that the agency would use regarding “new versions” of COVID-19 “vaccines.” Yours Truly presents page 17, page 18, and page 19 of this document:
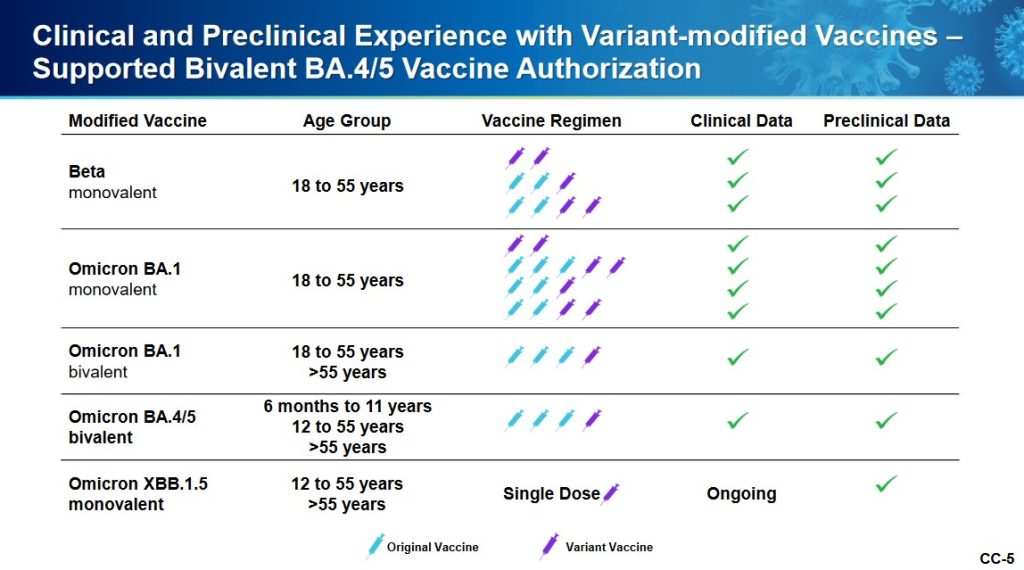
It appears that the FDA simply decided that it would be permissible for the agency to authorize a new COVID-19 “vaccine” strain composition along what, in Yours Truly’s opinion, may be called “very flexible” options. For example, the Pfizer-BioNTech XBB.1.5 COVID-19 “vaccine”, which was FDA authorized in the fall of 2023, had test results only from mouse testing prior to FDA authorization. Following are: The link to the Pfizer-BioNTech slide presentation about this “vaccine” to the CDC’s ACIP committee (Advisory Committee on Immunization Practices) meeting of 12 September 2023; and, an image of slide CC4 from this presentation. First, the presentation: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-09-12/10-COVID-Modjarrad-508.pdf.
Second, slide CC-4 from the above presentation:
The XBB.1.5. Pfizer-BioNTech COVID-19 “vaccine” had only been given as a single injection to humans in the company’s clinical trial; a clinical trial which had only just begun prior to the ACIP meeting. Slide CC-5 of the presentation, the start of the company’s human trial of this “vaccine”, is below:
Slide CC-6 of the presentation has to do with the mouse studies of this “vaccine”, which were of longer duration.
Notwithstanding the above, the FDA authorized the use of the company’s XBB.1.5 COVID-19 “vaccine” on 11 September 2023 (in Yours Truly’s opinion, it appears that the ACIP meeting of 12 September 2023 was a “catch-up” formality.) It also appears (again, in Yours Truly’s opinion), that the FDA used a very loose interpretation of “Option 4” on page 18 of the FDA Briefing Document above in granting the EUA for this “vaccine”.
** Now, on to the latest “new version” of the COVID-19 “vaccines”, the “2024-2025 Formula COVID-19 Vaccines”, that the FDA authorized in June 2024.
The following linked items are important regarding background information related to this situation and to the FDA: First, the FDA document, stating that the agency would “align” its COVID-19 “vaccine” antigen composition to the recommendations of the World Health Organization’s TAG-CO-VAC recommendations: www.fda.gov/media/179139/download (the TAG-CO-VAC recommendation for the “2024-2025 Formula COVID-19 Vaccines” was to use the JN.1 strain); second, the FDA document regarding “considerations and recommendations” for the “2024-2025 Formula COVID-19 Vaccine” composition: www.fda.gov/media/179145/download; third, the FDA announcement of the 5 June meeting of its VRBPAC committee (Vaccines and Related Biological Products Advisory Committee.): www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-june-5-2024-meeting-announcement. From this last link, chick on “Event Materials” to see the slide presentations and other items that were discussed at this meeting.
Two important items from the “Event Materials” list: the FDA Briefing Document; and the VRBPAC roster for this meeting. First, the FDA Briefing Document: www.fda.gov/media/179003/download; and, second, the VRBPAC roster for this meeting: www.fda.gov/media/179225/download. The roster for the 5 June 2024 meeting has some “familiar” members and speakers: Paul Offit, MD; and Peter Marks, MD (director of CBER [Center for Biologics Evaluation the Research of the FDA]); and, among the “Temporary Voting Members”, are: Bruce Gellin, M.D., M. PH., the Chief of Global Public Health Strategy for the Rockefeller Foundation; and, Melinda Wharton, M.D., M. PH., Associate Director of Vaccine Policy of the CDC. (Italics mine)
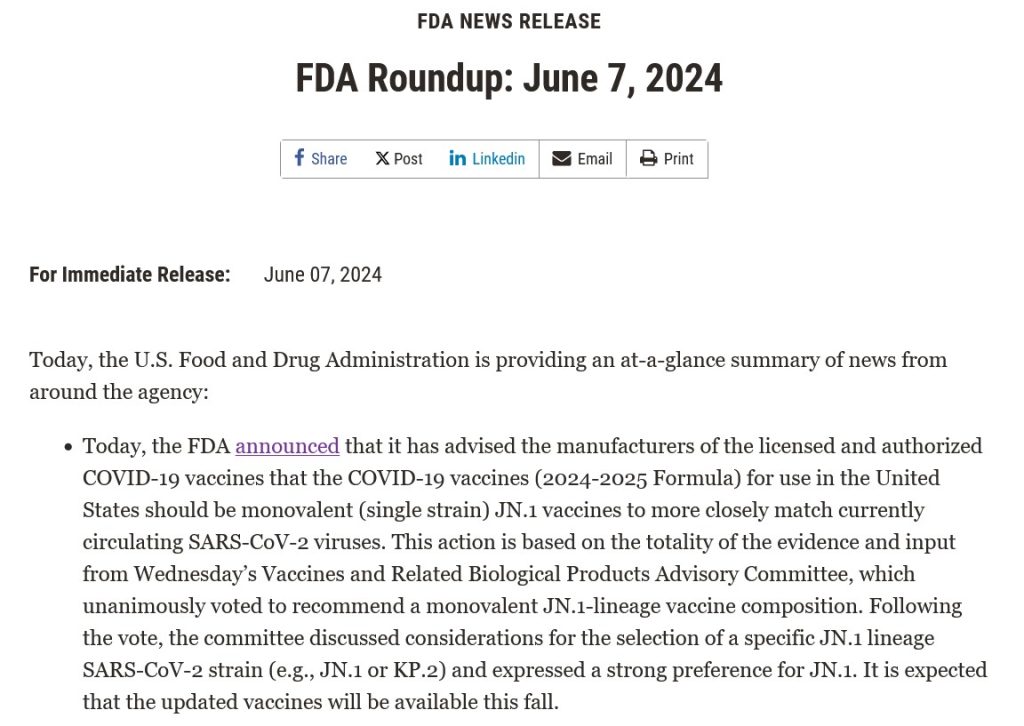
The VRBPAC members voted unanimously to endorse the Pfizer-BioNTech, the Moderna, and the Novavax “2024-2025 Formula COVID-19 Vaccine” by these companies, based on the presentations of these companies’ representatives at the meeting. Yours Truly can find noregistered human clinical trials performed in advance of the 5 June VRBPAC meeting by Pfizer-BioNTech, or by Moderna, or by Novavax, for any “2024-2025 Formula COVID-19 Vaccine”; that would indicate that any “clinical trials” were performed in these companies’ facilities on mice; and that any “human trials” were also performed in these companies’ facilities, prior to the meeting. The FDA then issued the agency’s original announcement of 7 June 2024: www.fda.gov/news-events/press-announcements/fda-roundup-june-7-2024; and, a screenshot from this announcement:
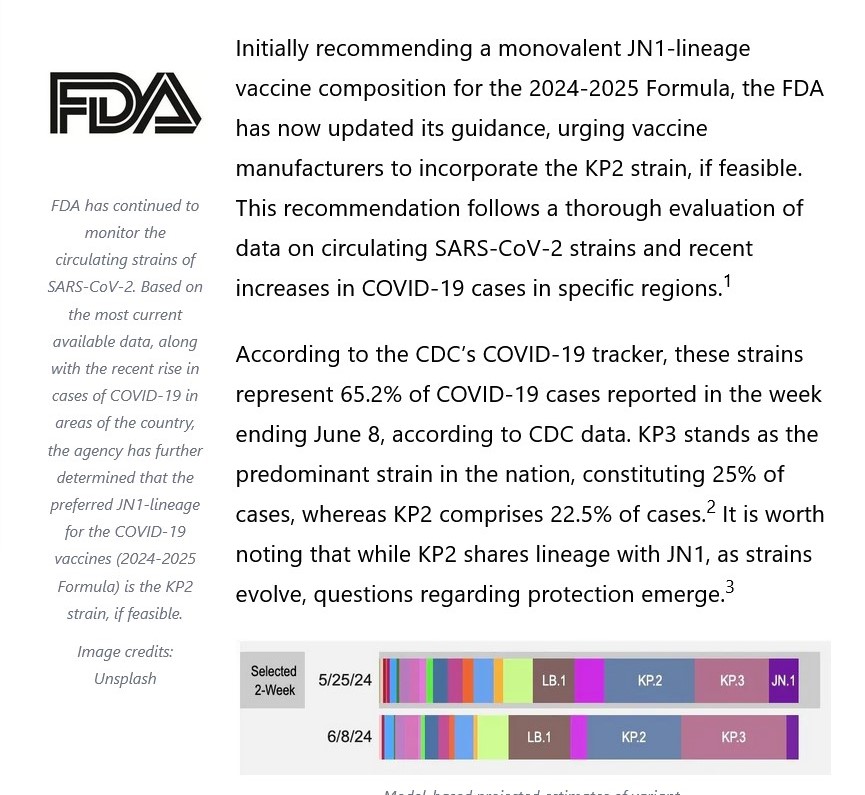
Note in particular “…the selection of a specific JN.1 lineage SARS-CoV-2 strain (e.g., JN.1. or KP.2) and expressed a strong preference for JN.1.” Here’s where it starts to “get interesting.”
What was it that happened? Part of the answer lies in the fact that the NIH and Moderna co-own the patents (and, therefore, share the royalties) for the Moderna “flagship” modRNA COVID-19 “vaccine”, mRNA-1273. This agreement would extend to “descendant clone COVID-19 vaccines” by Moderna. www.citizen.org/article/modernas-mrna-1273-vaccine-patent-landscape/. The NIH’s Dale and Betty Bumpers Vaccine Research Center (part of NIAID — which Dr. Anthony Fauci led from November 1984 until his retirement in December 2022) and Moderna co-developed mRNA-1273. https://covid19.nih.gov/news-and-stories/nih-vaccine-research-center; a screenshot from the article is below:
The other part of the answer is that Moderna was already developing a KP.2 strain COVID-19 “vaccine” for 2024-2025. This, and the FDA’s decision to shift away from the JN.1 strain to the KP.2 strain, are described in this post at Sasha Latypova’s blog: https://sashalatypova.substack.com/p/all-roads-lead-to-resilience, “All Roads lead to Resilience. FDA is removing competitors for the Pentagon & CIA’s baby…Moderna”, 23 June 2024.
However, there’s yet another detail in play here, regarding the FDA’s switch, “based on evaluation of the most recent circulating strains of COVID-19”, from JN.1 to KP.2 — the CIA and the Pentagon. Here is a screenshot from Sasha Latypova’s Substack article:
But wait, there’s more! Resilience lists multiple “partners”, such as the Mayo Clinic. The company also, apparently, has a “partnership” with the United States Army’s Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense https://resilience.com/learn/partnerships. Below is a screenshot from this website:
It appears, then, in Yours Truly’s opinion, that the FDA was perhaps “reminded” of the”details” regarding the NIH-Moderna co-ownership (and royalties – sharing) agreement related to Moderna’s modRNA COVID-19 “vaccines”; and, the role of the CIA-Pentagon-National Resilience (aka Resilience) in manufacturing the mRNA used in the Moderna COVID-19 Omicron “booster vaccines” — and the KP.2. strain is indeed a “descendant strain” in the Omicron lineage (as is the JN.1 strain.) Hence, the FDA’s 2024-2025 COVID-19 “vaccine” strain “sudden switch” announcement of 13 June 2024, only one week after the agency gave the nod to the JN.1 strain.
In Yours Truly’s opinion, it is statistically, medically, and ethically impossible for a new vaccine (let alone any COVID-19 “vaccine”) to be developed; tested (on lab animals, then on human subjects); the test data thoroughly collated and analyzed for “safety and efficacy” on both lab animals and on human subjects; then, which data is presented to the CDC / FDA for consideration; then, these agencies doing their own “due diligence” research; then, and only then, being granted an EUA by the FDA; then, and only then, manufactured for use in humans — in a time span of fewer than three to five years, let alone within a time span of only a few months. It appears, again in Yours Truly’s opinion, that the CDC and the FDA are playing “fast and loose” with the health and safety of the people who choose (or will be “mandated”) to take the “2024-2025 Formula COVID-19 Vaccine.” And, also, that “other entities” are in play here to perhaps “influence” decision making by these agencies.
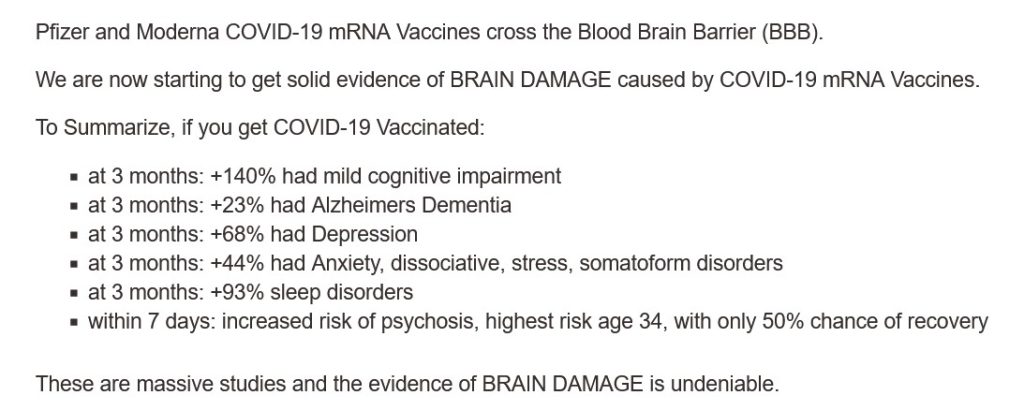
All of above is in addition to the fact that the COVID-19 “vaccines” (actually, gene therapy injections) have caused, are causing, and will cause, multiple health issues, serious adverse reactions, and deaths, in those who are “vaccinated.” Just two of the most recent discoveries: One, the COVID-19 “vaccines” can cause brain damage, an article by Dr. William Makis: www.globalresearch.ca/brain-damage-covid-19-mrna-vaccines/5861012, “Brain Damage Caused by COVID-19 mRNA Vaccines”, 26 June 2024. Below is a screenshot from Dr. Makis’ article:
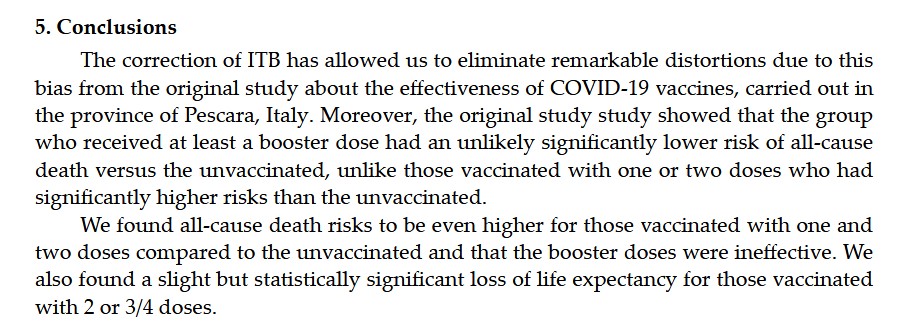
The second most recent discovery, that the COVID-19 “vaccines” reduce life expectancy (even in “all-cause” analysis) among COVID-19 “vaccinated” persons, by Dr. Peter A. McCullough: https://petermcculloughmd.substack.com/p/breaking-publication-a-critical-analysis, “BREAKING Publication — A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, 1 July 2024. The peer-reviewed paper is here: https://doi.org/10.3390/microorganisms12071343, “A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, Marco Alessandria, et al., published 30 June 2024. Below is a screenshot from the Conclusions section of this paper:
In Yours Truly’ opinion, it is apparent at “half a glance” that the COVID-19 “vaccines” (actually, gene therapy injections) must be completely withdrawn for human use until these products have been fully investigated, and then re-designed, before being re-introduced for human use; and, that there is no “co-ownership” or sharing of royalties between a government agency and a COVID-19 “vaccine” manufacturer; and, that there is no involvement of the United States military in the development or manufacture of such products.
This series of posts regarding the ongoing issues of COVID-19 and the COVID-19 “vaccines” is dedicated to the memory of Yours Truly’s cousin Bill, who passed away “suddenly and unexpectedly” in September 2023. Today’s post is addressed to medical professionals who had any COVID-19 “vaccines” (in reality, gene therapy injections) injected into their bodies since 11 December 2020. This post is not “accusatory” in nature: Yours Truly is curious. One will make it clear at the outset that there are vaccines and other injectables that are useful: For examples, the Rabies vaccine and the injectable form of Heparin. One will also make it clear that the following questions regarding the modRNA COVID-19 “vaccines” are not “tin-foil hat” or “conspiracy theory” in nature — all of them are based on the writings and researching of medical doctors and scientists who want to find out the truth about these particular “vaccines.” There are many other questions that must be asked; Yours Truly is presenting a few of the most important ones from a personal point of view in today’s post.
Dear COVID-19 “Vaccinated” Medical Professional:
With all due respect for your education and expertise, there now must be serious questions raised concerning the COVID-19 “vaccines” that were rushed into use in the United States and all over the world. These questions are especially important given the increasing numbers of reports of COVID-19 “vaccine”-induced injuries, illnesses, disabilities, and deaths, among those who have taken, and/or continue to take, these “vaccines.”
The first question that must be raised is: Are you aware that the FDA knew, back on 30 April 2021, that the modRNA COVID-19 “vaccine” by Pfizer-BioNTech, BNT162b2, is involved in the inducement of over 1,200 types of medical diseases and conditions? Here is the document that Pfizer-BioNTech gave to the FDA on that date: https://phmpt.org/document/5-3-6-postmarketing-experience.pdf, 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021. Please see page 30 of this report, APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST. The report is also found here: https://phmpt.org/document/5-3-6-postmarketing-experience.pdf. The document is FDA time-stamped 30 April 2021. Yours Truly will point out that this report covers only between 11 December 2020 (the date of the initial EUA granted by the FDA for BNT162b2 to be used in the United States) and 28 February 2021. The list of Adverse Events of Special Interest begins with 1p36 deletion syndrome; other diseases, disorders, and events mentioned include: Cardiac arrest; Cerebral thrombosis; Demyelination; Guillain-Barre syndrome; hepatic disorders; immune system disorders; pulmonary disorders; Myocarditis; neurological disorders; and, Pericarditis; among many others.
The second question that must be raised is: Are you aware that the modRNA COVID-19 “vaccines” made by Pfizer-BioNTech (these include BNT162b2; this company’s previous “booster” COVID-19 “vaccines”; and this company’s current “2023-2024 Formula COVID-19 Vaccine”) contain two dangerous lipid nanoparticles, ALC-0159 and ALC-0315, both of which are for research use only? Here are the Safety Data Sheets for these lipid nanoparticles: For ALC-0159: https://cdn.caymanchem.com/cdn/msds/34336m.pdf; and, for ALC-0315: https://cdn.caymanchem.com/cdn/msds/34337m.pdf. On page one of each of these Safety Data Sheets, there is the following language: “Application of the substance / the mixture This product is for research use – Not for human or veterinary diagnostic or therapeutic use.” In addition, are you aware that the modRNA COVID-19 “vaccines” made by Moderna (these include mRNA-1273; this company’s previous COVID-19 “booster vaccines”; and this company’s current “2023-2024 Formula COVID-19 Vaccine”) contain the dangerous lipid nanoparticle, SM-102, which is for research purposes only? Here is the Safety Data Sheet for this lipid nanoparticle: https://cdn.caymanchem.com/cdn/msds/33474m.pdf. On page one of this Safety Data Sheet, there is the exact same language in the section “Application of the substance / the mixture” as is listed for ALC-0159 and for ALC-0315 in their respective Safety Data Sheets: “This product is for research use – Not for human or veterinary diagnostic or therapeutic use.” (As an aside, ALC-0149 and ALC-0315 are described only by their chemical component names in the FDA-issued Fact Sheet for the Pfizer-BioNTech “2023-2024 Formula COVID-19 Vaccine”: www.fda.gov/media/167211/download; please see under section 11 DESCRIPTION. However, ALC-0159 and ALC-0315 are called by their proper names in the FDA document, www.fda.gov/media/172019/download, Emergency use Authorization (EUA) for an Unapproved Product Review Memorandum, dated 23 June 2023, section 7.1 Chemistry Manufacturing and Control (CMC) Information.)
The third question that must be raised is: Are you aware that the COVID-19 “vaccines” can, and do, “shed” components of these products from “vaccinated” persons to un-“vaccinated” persons? Dr. Pierre Kory has an extensive series of articles on his blog relating to this phenomenon: https://pierrekorymedicalmusings.com/; please see Part One of this series: https://medicalmusings.com/p/shedding-of-covid-mrna-vaccine-components, published 1 November 2023.
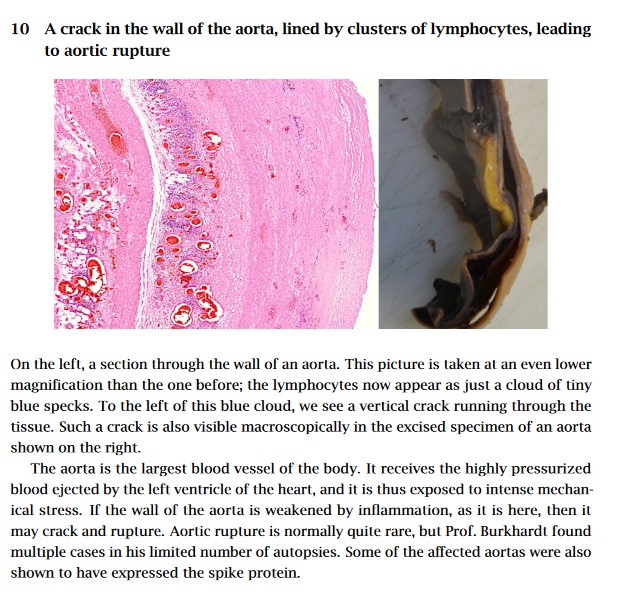
The fourth question that must be asked is: Are you aware that the COVID-19 “vaccines” can, and do, damage the blood vessels, heart tissue, and lung tissue, of persons who have these “vaccines” in their bodies? Please refer to: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, Michael Palmer, MD, and Sucharit Bhakdi, MD. Yours Truly presents page nine of this paper, which is self-explanatory:
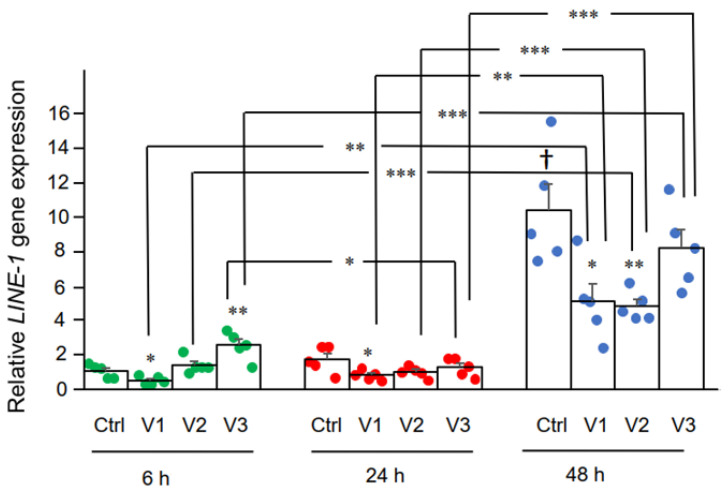
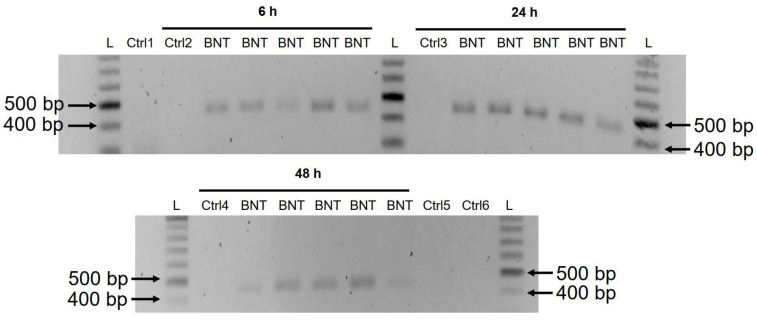
The fifth question that must be asked is: Are you aware that the modRNA Pfizer-BioNTech COVID-19 “vaccine”, BNT162b2, changes the DNA of the LINE-1 Human Liver7 cell line? Please refer to: https://doi.org/10.3390/cimb44030073, “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Yang De Marinis, et al. Yours Truly presents two images from this paper: The first, of DNA expression induced in BNT162b2-treated Human Liver7 cells in LINE-1; the second, of DNA amplicons induced by BNT162b2-treated Human Liver7 cells in LINE-1.
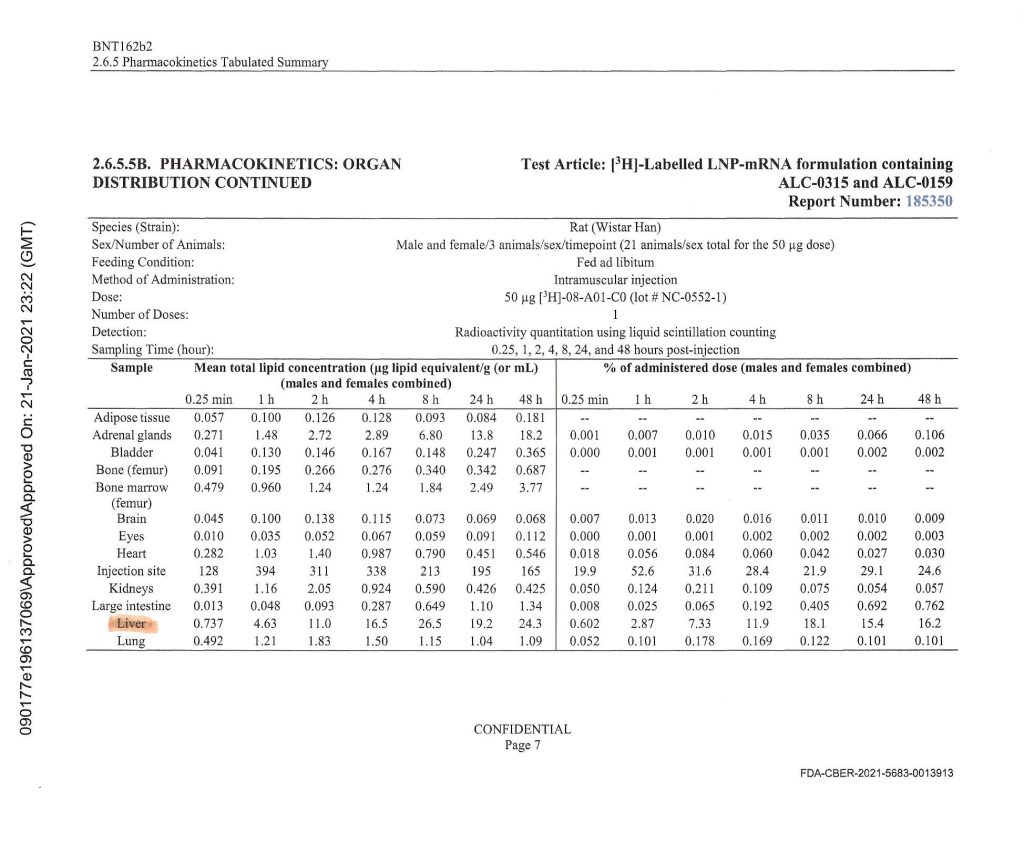
Notice the heavy accumulation of BNT162b2 in the livers of the Wistar lab rats that were used in this experiment conducted by Pfizer-BioNTech. This was the same BNT162b2 Pfizer-BioNTech modRNA COVID-19 “vaccine” that was later injected into human patients (with ingredients amounts calibrated for human use.)
Yours Truly will note that the CDC changed the definitions of “vaccine” and “vaccination” in 2021, after the rollout of the COVID-19 “vaccines” (gene therapy injections.) One suspects that this was done to “shoe-horn in” these products under the aegis of “vaccines.” Please refer to: www.johnlocke.org/the-cdc-changed-its-definitions-of-vaccine-and-vaccination-and-keeps-changing-its-definition-of-fully-vaccinated/. However, the FDA states clearly, on page four of the Fact Sheet for Healthcare Providers for the administration of the “2023-2024 Formula COVID-19 Vaccine” by Pfizer-BioNTech, that this product is to prevent coronavirus disease (COVID-19), not to “protect against serious illness from COVID-19”, as the CDC states. Please refer to: www.fda.gov/media/167211/download, page four, under section 1 EMERGENCY USE AUTHORIZATION; and to www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html under What You Need to Know.
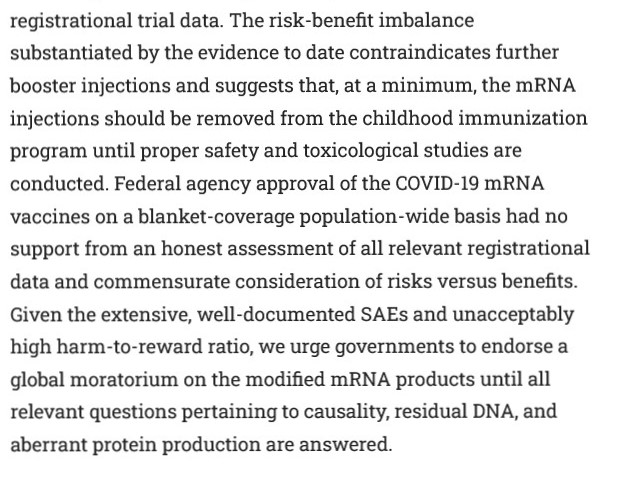
Finally, there is this paper, published on 24 January 2024: https://doi.org/10.7759/cureus.52876, “COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign”, M. Nathaniel Mead, Peter A. McCullough, et al. Yours Truly presents part of the Abstract of this paper:
Sincerely, with Good Energy, Peace, and Respect, PAVACA
PAVACA: BFA (2), Carnegie-Mellon University; MA, Duquesne University. Reading and writing about COVID-19 and the COVID-19 “vaccines” since March 2020. Also interested in Pharmacy and in the impacts of Big Pharma. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 – 2018), First Professor of the Darden School of the University of Virginia, available at www.amazon.com/, www.barnesandnoble.com/, and www.authorhouse.com/.
The bottom line is that I have simply checked the gene sequences of the Pfizer and Moderna vaccines, and verified that they BOTH contain nucleic acid code that translates to the shorter PRRARSV protein code, which is a kind of “hall pass” into the cell nucleus.
Thus, BOTH of these vaccines produce a spike protein which science would predict has the same ability as the virus spike protein, to (1) get into the cell nucleus, and furthermore (2) schlep its own mRNA along with it into the cell nucleus, and finally (3) as proven by experiment on the Pfizer vaccine, integrate the spike protein gene sequence into the human cellular genome.
That’s it. If you want all the gory details, stay tuned. Otherwise, that’s the BLUF (bottom line up front). Have a great day! -Wolf
Introduction
OK – I have an important update to the whole topic of mRNA vaccines messing with people’s genes, and in particular, with a part of the COVID-19 spike protein mRNA sequence called the PRRARSV nuclear translocation signal. This “key” within the whole sequence is like an ID card for the cell nucleus. It was identified in the natural COVID-19 spike protein, and now it appears to remain in both the Pfizer and Moderna vaccines.
I have posted on this topic – the PRRARSV Nuclear Translocation Signal – THREE times before.
First, I posted when I discovered the Mehedi paper, and realized how important it is.
The Mehedi paper explains WHY there is genomic incorporation of the COVID-19 spike protein – specifically, because the spike protein has what is essentially a key to the cell nucleus.
This is SO HUGE. I must explain this to you. TL;DR – The spike protein not only contains a special sequence that allows it into the cell nucleus – it also has an ability to bring its own spike mRNA sequence with it. Both features appear to be unique among coronaviruses. The features explain genomic …
The next time I posted, was the moment that I realized that the murdered American scientist Bing Liu had been directing his research focus to the EXACT SAME SPOT in the SARS-CoV-2 gene sequence – the PRRARSV sequence – when he was conveniently murdered by a crazed acquaintance who was apparently contending with him over a lover.
To me, this murder absolutely REEKED of MKULTRA. Bing Liu had a plausible weakness and it was exploited. Not all people realize how dangerous the science world can be. Not so this cowboy – I’ve been through a lot of weird, evil bullshit in Scienceville, over the years.
Bing apparently recognized that this sequence is found in snake venoms and other, more deadly viruses, and was thus potentially close to realizing that this part of the sequence was behind certain aspects of the pathogenicity of SARS-CoV-2, as well as those other things.
Stated another way – maybe nuclear translocation is WHY those other things are so bad.
Joe Biden didn’t win. This is our Real President: AND our beautiful REALFLOTUS. This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both). …
Finally, at a certain point I realized that any “accidental” explanation of the presence of a working translocation signal which not only violates the central promise of mRNA vaccine technology, but installs the violation itself in the nucleus, was simply too incongruous to be an accident. It’s a BLOODY HACK. There was no way that – on the very first roll-out of a genetic vaccine – the technology which was PRIZED for making the technology safe against genetic incorporation, instead caused genetic incorporation OF the very instructions for genetic incorporation.
I mean, think about it. What are the chances? It’s almost as crazy as the sinking of the “unsinkable” Titanic.
You see what I’m sayin’? This outrageously excellent attack simply cannot be a case of “whoops”. The TRICK is not the “AW SHUCKS, THAT’S LIFE” which sells as stage two to the hubris of the chumps. That’s just the getaway. The TRICK is the LIE – the PROMISE that is actively worked against from the very beginning, and intentionally not delivered.
Ask yourself a simple question. Why should the very first examples of mRNA vaccines for humans violate the most important safety standard of the mRNA platform? Why would the vaccines do exactly what they PROMISED US the vaccines would not do? TL;DR – They didn’t just lie to us about the spike mRNA not going …
I wrote that last post with a certain sense of frustration. NOBODY in COVID Dissident World seemed to understand the importance of this whole “nuclear translocation signal” thing. Either that, or they were utterly afraid to speak of it. Indeed, our RDS is one of the few people who has dared to shine a light on the topic.
I set it aside for a while and basically gave up.
The other side did not give up. During that time, I was seriously shadow-banned on Twitter. Elon’s FEDS are busy little beavers, damming up the truth.
But now, something interesting has happened. On Twitter.
A Tale of Two Acronyms: PRRARSV and SV40
RDS posted a comment that included a tweet of a translated video of the brave Japanese professor who publicly challenged the Japanese Ministry of Health over the crappy vaccines.
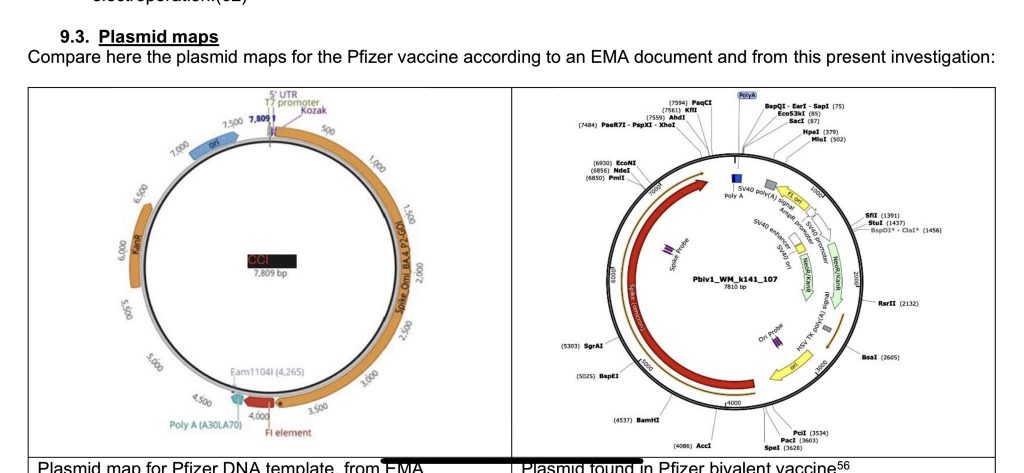
Here, Murakami is discussing contaminating plasmid DNA (little circles of DNA) which were found in very significant quantity in expired vials of the Pfizer vaccine. It’s easier to watch the video on Twitter.
This SV40 stuff also gets into a shocker about nuclear incorporation, but this is not the same shocker as the PRRARSV stuff. This is ANOTHER ANGLE on a different path into the nucleus.
Are you starting to believe me now about intent? Read on.
Japanese professor, Murakami of Tokyo University of Science made an amazing finding.
The Pfizer's vaccine contains the SV40 sequence which is known as a promoter of the cancer virus. The SV40 sequence is completely unnecessary to produce the mRNA vaccine. https://t.co/RtnbCUHAmJpic.twitter.com/gZx5ycf1L9
The translation is as follows. It is a conversation between Professor Murakami (M) and another person (P). I may have gotten a couple of assignments mixed up, when both are talking, but have done my best to attribute statements properly, based on what I can discern.
Commentary by Professor Murakami
(M) It is now possible to read the DNA sequences present in the vaccines. This is the DNA read from the Moderna vaccine.
(P) It may be difficult for the general public to understand, but this sequence is in the form of a ring. Plasmid DNA is in the form of a ring, and the DNA sequence is described in this ring. Spike proteins are encoded in this part of the DNA sequence.
(M) This part of the DNA sequence shows the spike gene. The Moderna’s vaccine has a vector sequence that is often present in Escherichia coli. However, the Pfizer’s vaccine has a staggering problem. I have made an amazing finding. This figure is an enlarged view of Pfizer’s vaccine sequence. As you can see, the Pfizer’s vaccine sequence contains part of the SV40 sequence here. This sequence is known as a promoter. Roughly speaking, the promoter causes increased expression of the gene. The promoter is a sequence that is essential for gene expression. The problem is that the sequence is present in a well-known carcinogenic virus. The question is why such a sequence that is derived from such a cancer virus is present in the Pfizer’s. There should be absolutely no need for such a carcinogenic virus sequence in the vaccine. This sequence is totally unnecessary for producing the mRNA vaccine. It is a problem that such a sequence is solidly contained in the vaccine. This is not the only problem. If a sequence this is present in the DNA, the DNA is easily migrated to the nucleus. So it means that the DNA can easily enter the genome. The problem is that if such a sequence remains intact, the DNA is easily migrated to the nucleus. It means that the DNA can easily enter the nucleus. These are such alarming problems.
(P) Does it mean that the SV40 promoter also contains sequences that can be migrated to the nucleus?
(M) Yes, that’s what I mean.
(P) So you are saying that the DNA can go to the nucleus easily?
(M) It means that the DNA contains sequences that can easily go to the nucleus. This is a well-known fact. This fact has already been documented in a number of scientific literature. It is essential to remove such sequences. The sequences have to be removed. However, Pfizer produced the vaccines without removing the sequences.
(P) This is outrageously malicious.
(M) That’s right. Pfizer retained the SV40 promoter sequence which is completely unrelated to the in vitro synthesis of the messenger.
(P) This issue should be questioned. Why such a promoter sequence is present in the DNA? This kind of promoter sequence is completely unnecessary for the production of the mRNA vaccine. In fact, SV40 is a promoter of cancer viruses.
(M) Yes, SV40 is well known.
(P) The sequence that promotes the cancer virus is present in the DNA for some reasons. As we know, we use this SV40 promoter sequence in various experiments. However, the question is why the promoter sequence is present in this mRNA vaccine.
Do YOU have some questions at this point? I sure as hell do. And the presence of multiple PHARMA TROLLS on Twitter, muddying the water with disingenuous excuses and throw-away coddles, makes things look even more suspicious.
RDS and I discussed this at some length in Saturday’s open. I urge interested readers to follow the above link, repeated here, to see our talk about this video, but it is not necessary for the following discussion.
I then proceeded to Twitter, and got caught up in a variety of arguments between the awesome Jikkyleaks and various “defenders of the narrative”, to put it kindly.
Many of these people (I will avoid calling them “pharma trolls”) shoot from the hip, and – despite sometimes being what should be experts in their fields, seem to have no grasp of basic logic applied to basic principles of biology. They are perfect, however, for defending scientific orthodoxy in a somewhat religious manner.
Meanwhile, sharper people in biotech who understand the basic WTF (like the presence of extraneous DNA in an RNA vaccine being an actual problem) are literally running toward the enemy with the downfall of the original vaccine sales narrative.
I should add, at this point, that SOMEBODY at Twitter is desperately covering all of this up. Twitter uses a stealthy way of “downgrading replies” to hide really important pharma stuff, without overtly banning content. It’s rather ingenious, but it’s VERY frustrating.
First of all, these Twitter IC people are fooling the hell out of Elon Musk – or maybe they aren’t. Either way, some of the most important biology about the vaccines is being hidden, and IMO it sucks big-time.
Thus, it was nearly impossible for me to find the following conversation again. Twitter had hidden my comments so effectively, that I myself could not find them in my own timelines of Tweets and Replies. But with persistence, I did find them.
This conversation and the interspersed commentary explains the how and why of my verifying that the nuclear translocation signal IS in fact in the two main mRNA vaccines – and in my opinion, intentionally so.
Enjoy.
We begin with a Pharm Boy attacking Murakami’s analysis.
Hello, this is false. The plasmid does not contain the entire SV40 gene, just the ori of replication, poly(A) signal, and a promoter. None of these sequences allow for translocation into the nucleus. That sequence is contained in the VP2 region, which is not in this plasmid
The abstract, with the relevant text in BOLD, is here:
ABSTRACT
One of the steps that limit transfection efficiency in non-viral gene delivery is inefficient nuclear import of plasmid DNA, once it has been delivered into the cytoplasm. Recently, via microinjection into the cytoplasm and in situ hybridizations into a few cell types, it was shown that a region of Simian virus 40(SV40), specifically a c. 372-bp fragment of SV40 genomic DNA encompassing the SV40 promoter-enhancer-origin of replication (SV40 DTS), could enable the nuclear import of a plasmid carrying these sequences (Dean D.A. Exp. Cell Res. 230 (1997) 293). In this report, we address the issue of the suitability of the SV40 DTS for cationic lipid-mediated gene delivery, and its capacity to improve the efficiency of the transfection process. For this study, we used transient reporter gene expression assays on various cell types. The gene expression from the plasmid constructs carrying the SV40 DTS varied with cell type and plasmid construct used. Such cell-type and plasmid-construct dependency on gene expression from plasmids containing the SV40 DTS suggests that the gene expression from plasmids is not entirely dependent on its ability to enhance the nuclear import of said plasmids.
The smarmy Taylor responds to this, as follows.
Lmaoooo the plasmid doesn’t contain the enhancer region genius. Just the origin of rep, promoter, and poly(A) signal.
Can you link something saying that using only these three regions that transport into the nucleus is facilitated? Take your time
McKernan does not respond to this, and I don’t know whether Taylor’s point is valid, but assuming that it is correct, the point stands – is the fragment included sufficient to enable nuclear translocation?
This is where I decided to “inject” the fact that there already IS a nuclear translocation signal present (in the lipid nanoparticle) in the spike protein mRNA, so that RNA may be covering for DNA transport as well. But I wanted to make sure that McKernan saw it – I don’t particularly care about Taylor. So I answered directly to McKernan, on the same tweet that Taylor used. I included a link to the Mehedi paper, which is sorely under-exposed.
Is any of this influenced by the simultaneous presence of a translocation signal in the spike protein itself, which does appear to assist translocation of spike mRNA?https://t.co/q2oocDy5eU
I figured that Taylor would respond, and he/she/it did immediately.
[SIDEBAR – I would not be surprised if Twitter insiders are helping these pharma bots by – e.g. – making sure that Taylor Ray and fellow “influencers” can see my input, but that my fellow free scientists, including Kevin McKernan, cannot.]
This paper is about the actual spike protein from the virus, not the spike generated from mRNA vaccines, whose binding site is inactivated.
Taylor’s comment, beginning with “this paper is about something else”, betrays a kind of battered science syndrome that keeps science exactly where the Cabal wants it – defending its own orthodoxy – never questioning by looking off the plantation. It is based on exactly the kind of authority-and-orthodoxy-defending, “teacher’s pet” science that I detest.
Yes, there is a very legitimate question about “virus versus vaccine” – that a VIRUS result is not exactly the same as a VACCINE result. However, if you’re looking at the same or similar things happening for both, and one has a shared culprit, what does logic say?
The entire vaccine paradigm is built on the idea of virus-vaccine symmetry, so if you’re not looking honestly at “virus predicts vaccine” as your FIRST STEP of analysis, you’re never going to predict anything.
Which, by the way, is exactly what the Cabal wants.
This is a perfect example of “unethical skepticism”, as The Ethical Skeptic teaches us.
Taylor at least has the decency of adding a weak and wobbly excuse for a difference – “whose binding site is inactivated”.
This is chaff and countermeasures, as Sundance likes to say. See if you can put that together from my measured, friendly response.
Yes, it's true that Mehedi's work was done on the viral spike mRNA and protein. Likewise, it is true that the full spike pseudo-mRNA in the vaccines has a few seq changes such as prolines to lock conformation, etc. Those don't address whether a functioning NT signal remains.
What I’m saying here implies that the “inactivated binding site” in the vaccine (which itself implies possible changes in the total sequence) does not necessarily affect the presence of a nuclear translocation signal (NTS). These are two different features in the protein. Bringing that up is CHAFF.
Notice that I am not backing down on the idea that data from the virus can and likely is predictive of the vaccines. I am just waiting for Taylor to assert openly that they are not.
Taylor, instead of challenging me, tries a very sneaky deflection.
A quick BLAST search should resolve this as the NLS sequence in the COVID spike is from aa residue 682 to 685.
This gets into bioinformatics. BLAST is a search engine of gene and protein sequences, which allows people to quickly find matching sequences – OR TO MISS THEM.
For sensitive operations, I simply don’t trust BLAST. It’s like Google. It’s a great place to look if you’re willing to throw your cares onto somebody else’s software, but it’s easy to miss things.
The SNEAKY move by Taylor is to MISLEAD me away from PRRARSV into a BAD SEARCH. The suggestion is to use an overly broad search of only 4 amino acids (682-683-684-685). Sorry, Charlie. No dice. I am interested in exactly what I said – PRRARSV – seven amino acids.
Instead, I decided to look for the sequences of the vaccines, and then use simple tools to check for the presence of the PRRARSV signal in them.
To begin with, note that there are TWO kinds of sequences I can potentially get for the vaccines.
the actual sequences, obtained by analyzing the vaccines
the “official” sequences, released by Pfizer and Moderna, the FDA, or somebody else
I tried to get official versions, but simply could not find them. So I found a link in the broader discussion of the results which Murakami was looking at.
The first thing you will note is that this is not likely to contain PRRARSV in it, because it’s all G, T, C, and A, like GATTACA.
This code needs to be translated from DNA/RNA to AMINO ACID, and for that, I need TEXT – not an image. So I looked for a different GitHub upload of the data, with text instead of images, and I found one.
Plugging in the sequences from the paper on GitHub, it’s straightforward. Here are the two vaccines, translated to amino acids, as both images and text.
In each vaccine, there is one and only one instance of the full PRRARSV nuclear translocation signal mentioned by Mehedi, which I have marked in BOLD.
So what does all this mean?
This means that there is no question – the same nuclear translocation signal which gets natural spike protein into the cell nucleus, and natural spike protein messenger RNA into the nucleus, BOTH as demonstrated by Mehedi, is in the vaccine spike proteins.
Do I have to spell it out any more than that? Are the members of the Pfizer Defense Legion so incurious as to what this might mean, that they have to fight the obvious truth every step of the way?
Watch what happens next.
Thank you. You prompted me to do the work. The full nuclear translocation signal (PRRARSV) cited by @masfique appears to be intact in both the actual Pfizer and Moderna sequences. Here is Pfizer.
Taylor’s response was interesting, and I didn’t expect it.
Wonder if the inactivated binding side negates this as it doesn’t allow the vaccine spike to be taken up by the cell. But thank you for doing your due diligence, this is good information
This response actually set me up to explain why the binding site issue is largely irrelevant. First my reply, then the explanation.
Thanks! Even assuming that cell surface binding/entry inactivation reduces direct secondary toxicity of the vaccine-produced spike to new cells, the NTS still means that primary genotoxicity of the Ψ-mRNA+spike may occur for any cell affected by LNP-enabled uptake of Ψ-mRNA.
TRANSLATION: Even if the vaccine-produced spike protein is “inactivated” toward some unspecified binding interaction in some unspecified way [which is contrary to the use of the largely unchanged full spike protein for immunogenic reasons, but let’s just ignore that point], so that the spike does not engage in some alleged “binding” in some way [I provide a plausible example], it doesn’t mean that the spike is not doing exactly what the viral spike has been proven to do, in terms of getting into the cell nucleus, AND bringing in its own mRNA at the same time.
Twitter’s character limits forced me to make that reply too jargon-filled for most, and possibly even for Taylor, who seemed not to have understood the full life cycle of the vaccine.
Allow me to explain in even more detail what I said, which was designed to clarify the issue for Taylor.
Let’s assume that the vaccine spike is somehow “inactivated” in its interaction with cell surface receptors. This would mean that new vaccine spike created by cells, would not interact with new cells in the same way as new disease spike protein, whether that spike was alone or part of a virus particle. I refer to that as “secondary toxicity”.
What I’m pointing out is that this is irrelevant to a “primary” toxicity concern – in fact a “genotoxicity”. This is the risk that spike protein produced in a cell, due to that cell ingesting a lipid nanoparticle of vaccine, might then get into the nucleus, and change the nature of that cell in a more fundamental way.
Now it is understood that the vaccine is “supposed to” lead to the death of infected cells, when those cells produce a bunch of spike protein, and are attacked by the immune system. The problem is that this doesn’t always happen, and indeed may not even be the primary fate of cells which take in the vaccine nanoparticles. What happens if the bell curve of vaccine intake creates a large number of cells which are damaged but not dead – which are not cleaned up by the immune system – and which have injured nuclei? There are lots of ways for things to go wrong.
What I am basically saying is that if the Mehedi results apply to vaccinated cells that are not cleaned up, we have a “bad cell problem”, and the problem isn’t just the spike – it’s in the nucleus. The cell’s problems have just become more “permanent”.
And that’s where things are. That fight is over, but I’m fighting over the De Marinis paper on another part of Twitter. That one is interesting, too.
STAY TUNED FOR MORE.
W
Title: CAREY TREATMENT, THE ¥ Pers: COBURN, JAMES / AUBREY, SKYE ¥ Year: 1972 ¥ Dir: EDWARDS, BLAKE ¥ Ref: CAR019AF ¥ Credit: [ MGM / THE KOBAL COLLECTION ]
RDS in the following comment points out one of the problems we have in waking up the Sheeple. There are highly ‘respected’ doctors and PhDs, who write papers in prestigious journals backing the mRNA vaccines even though they KNOW they are unsafe.
Wolf Moon OMG, this article below is a must-read. Linked from an AMA EdHub email one received today. It’s a JAMA piece written by Dr. Peter Marks — he’s the head of the CBER department of the FDA (Center for Biologics Evaluation and Research). Dr. Marks was in on the ground floor of Operation Warp Speed. Dr. Marks KNOWS EVERY DATA PIECE SUBMITTED TO THE FDA FROM PFIZER-BIONTECH ABOUT THE CLINICAL TRIALS FOR BNT162b2 BACK IN 2020 — AND EVERY DATA PIECE SINCE THEN ALSO. Dr. Marks was in on recommending that the FDA authorize the UNPROVEN, ONLY TESTED ON 8 MICE new “COVID-19 + Omicron BA.4 + Omicron BA.5 booster shot.” His linked article below is a screed for the development of “new” and “different types” of COVID-19 “vaccines” — including ones that specifically target the T-cell response in the body. Dr. Marks KNEW that the “vaccines” developed during Operation Warp Speed and given quick EUAs by the FDA WOULDN’T DO THE JOB: From his article: “One potential model for approaching such development [of a COVID-19 vaccine] was used successfully at the beginning of the pandemic when Operation Warp Speed evaluated numerous global vaccine types and focused on advancing several promising candidates, knowing full well that most would ultimately not be found to meet the criteria set forth for a safe vaccine with adequate efficacy.” (bolding and Italics mine) Dr. Marks represents the “medical establishment” and DeepState. IMO, the “medical establishment” and the DeepState have it as their business to continue to put these dangerous COVID-19 “vaccines” into people — and develop new “vaccines” to keep damaging / destroying the immune systems of those who take them. His article: https://jamanetwork.com/journals/jama/fullarticle/2799600 December 9, 2022 “Urgent Need for Next-Generation COVID-19 Vaccines” Peter Marks, MD, PhD https://www.youtube.com/watch?v=Nat1za4sKjA As an additional note. For those who might wish to watch the documentary it is available to watch free until the end of January. All that is required is your email I think. The link follows. https://therealanthonyfaucimovie.com/trailer/
In addition to censorship and smearing of dissenting voices, hospitals and doctors were getting the carrot and stick treatment – Lose your license OR getbig bucks for pushing bogus PCR tests, ventilators, Remdesivir and killing patients. – For example “A COVID-19 diagnosis provides extra payments to coroners!”
To make sure the Sheeple could not make a solid connection between the Covid Vaccine and death, the shot is a slow ‘poison’ with a variety of adverse reactions.
The CDC has been hiding the Social Security Administration death master file. I got it from a whistleblower. This shows deaths are taking 5 months from the jab to happen. This is why it’s hard to see.
Remember this time factor as we look at the data I found.
Finally we have the DELIBERATELY compromised VAERS system that is SUPPOSED to alert the CDC and FDA to harmful drugs.
There are major problems with the vaccine adverse event reporting system (known as VAERS) which the CDC considers the “front line” of vaccine safety. VAERS was created in 1990 by the CDC and FDA as a means to collect and analyze adverse effects that are associated with vaccines. Unfortunately, the failings of VAERS are “kept from the consciousness” not only of the public, but also from the doctors, pediatricians, and nurses that the public rely on to provide reliable information as to the safety of vaccines. I say “kept from the consciousness” rather than “kept secret” because while these failings are publicly disclosed for all the world to see, they are for all intents and purposes BURIED in documents seldom searched out by the average member of the medical community, much less by the average individual. You could say that the information has been very effectively hidden in plain sight…
In 2000, the 6th Report by the Committee on Government Reform addressed the failings of VAERS in its address of the Vaccine Injury Compensation Program…. [The] Congressional report notes (on page 15), “Former FDA commissioner David A. Kessler has estimated that VAERS reports currently represent only a fraction of the serious adverse events.” (emphasis by author)… That leads us to the interesting case of the CDC and Harvard Pilgrim Healthcare Inc.
The Department of Health and Human Services (HHS) gave Harvard Medical School a $1 million dollar grant to track VAERS reporting at Harvard Pilgrim Healthcare for 3 years and to create an automated reporting system which would revolutionize the VAERS reporting system- transforming it from “passive” to “active.”…
I’ll quote the findings directly from the report,
“Adverse events from drugs and vaccines are common, but underreported. […] Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of ‘problem’ drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed.”
Again, let’s stop and think about this revelation for a moment: fewer than 1% of vaccine adverse events are reported. The CDC’s entire vaccination propaganda campaign rests on their claim that side effects from vaccination are exceedingly rare (and predominantly minor).According to the CDC, in 2016 alone, VAERS received 59,117 vaccine adverse event reports. Among those reports were 432 deaths, 1,091 permanent disabilities, 4,132 hospitalizations, and 10,274 emergency room visits. What if these numbers actually represent less than 1% of the total as this report asserts? Simple multiplication would yield vaccine adverse events reports numbering 5,911,700!…
the United States of America Centers for Disease Control ghosted Harvard Pilgrim Healthcare, Inc.
“the practice of ending a personal relationship by suddenly and without explanation withdrawing from all communication.”
Personally, I would hope that I could hold an organization like the CDC to a higher standard, but… After a one million dollar grant was paid and three years of research conducted on what appeared to be a very successful upgrade to the passive VAERS system, the team’s CDC contacts went MIA
. The ESP:VAERS final report states, “Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.”
So in 2017, the CDC DELIBERATELY left a useless reporting system in place when they had the opportunity to upgrade it.
Since the VAERS data set is compromised as well as next to useless, I decided to see if we could find another way to connect the mRNA vaccines to deaths. There is a nifty site called Dead or Kicking.
there is the graph “United States death comparison by age in 2020“
By changing the date in the URL you get the different years AND if you place your mouse over the graph, it will give you Deaths, Death Rate and Population for each age group.
You can save the graphs for any year – or all of them – as examples, as Wolf did below. Right-clicking on a graph lets you “save image as” or “copy image”.
2019
2020
2021
2022
Note Added By Wolf – CHECK THIS ONE OUT!!!
I originally thought I would see a major drop in the population over 75 but that did not happen since the Baby Boomer cohort is filling the 65+ age groups faster than the orchestrated depopulation can kill them. Notice there are less people in the 45 to 54 age group than in the 55-64 age group. That is a REAL PROBLEM for the Cabal.
…The Social Security Trust Fund should currently have $2.5 trillion in surplus. So how is it that these checks could stop being issued if the debt ceiling isn’t raised? Economics professor Dr. Allen Smith, author of The Looting of Social Security: How The Government is Draining America’s Retirement Account, has been reporting on the theft of Social Security funds for years….
Age / Date
2019
2020
2021
2022
85+
6,604,958
6,628,013
6,673,175
6,715,875
75-84
15,969,872
16,022,410
16,139,651
16,250,631
65-74
31,483,433
31,571,207
31,773,610
31,970,852
55-64
42,448,537
42,643,579
42,929,850
43,208,648
45-54
40,874,902
41,050,404
41,371,452
41,683,591
So I created another table this time of USA Death Rates by age group by year. I included 6 years before covid as a baseline. Then the two years, 2019 & 2020, when Covid hit the USA plus the two years, 2021 and 2022 when the mRNA vaccine was progressively rolled out, starting with adults, then school age children and finally babies.
Also there was the DELIBERATE mis-diagnosis of flu and pneumonia followed by refusal to treat until the person was so sick they needed to be put on a ventilator & remdesivir thus killing up to 88% of those patients.
The result of all of this, is the most vulnerable elderly had already been killed off in 2020 as the much higher death rates for 2020 shows, but by 2021 and 2022 the death rates decrease from that high. Although the elderly were vaccinated, unlike athletes and younger, physically active people, the elderly are going to be a lot more sensitive to what their bodies are telling them and NOT pushing it. They are also more likely to have doctors checking their heart health and be on heart and circulatory medications.
Myocarditis is an important cause of arrhythmias and sudden cardiac death (SCD) in both physically active individuals and athletes.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
RETIREES 65 to 74
The 65 to 74 group is going to be a mixed bag. Compared to the 75+ group they are less likely to be in a nursing home or to have gotten deathly ill in 2020, although a certain percentage will have died. However they are likely to get the vaccine. Thanks to Medicare, they are more likely to be in contact with medical professionals who would try to talk them into the jab. They are also going to be a lot more physically active than older retirees and therefore stressing their hearts more after getting the mRNA vaccine.
You can see the combination of poor health care in 2020 followed by the vaccines and then boosters as the death rate increases year by year from 2019 through 2022.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
FORCED RETIREMENT/SMALL BUSINESS WORKERS 45 to 64
The 45 to 64 are an interesting group. Corporations force retirements and actively discriminate against those 45 years and up because age discrimination laws have no real teeth. Therefore the people 45 and up are most likely NOT working for ‘Corporate America’ and are either small business people or hired by small business people. (BTDT) This group is the most likely to have had a ‘rude awaking’ about the world we live in and are NOT going to be as trusting. Older people are also more likely to tell their boss to go F..K themselves with the darn needle. Like the 65 to 75 group you can see the increase in death rate year to year but it is not as sharp an increase. They are also more likely to be in better health than retirees. If You’re Over 50, Chances Are the Decision to Leave a Job Won’t be Yours Age discrimination in the workplace happening to people as young as 45: study
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
WORKING AGE CORPORATE AMERICA 15 TO 44
The age group 15 to 44 is the group most likely to show PURE UNADULTRATED DATA about Mortality & the mRNA vaccine although there may be some confounding from drug use increasing over the years. Covid-19 virus has little effect on the death rate in 2020. However as the boosters and the 5 month time delay kicks in you can see the death rate almost doubled in 2022 compared to 2019 and earlier.
….Scott Davison, the CEO of OneAmerica, a $100 billion life insurance and retirement company headquartered in Indianapolis.
“The data is consistent across every player in the business.”
Davison said death rates among working age people –
those 18 to 64-years-old – are up 40 percent in the third and fourth quarter of 2021 over pre-pandemic levels.
“Just to give you an idea of how bad that is, a three sigma or 200-year catastrophe would be a 10 percent increase over pre-pandemic levels,” Davison said. “So, 40 percent is just unheard of.”
He blames it on Covid instead of the mRNA vaccine of course. “…the third and fourth quarter of 2021…” would be after Steve Kirsch’s 5 month window. So far I can not find any 2022 insurance data. HMMMmmmm
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
CONTROL GROUP 1 TO 14
The 1 year to 14 can be considered the ‘Control Group’ Covid has little if any effect on the death rate in 2020. They were not vaxed until quite recently (November 2021) and boosters were not approved until May 19, 2022. The death rate so far has been flat but I would expect an uptick after the first of this year as the effects of the boosters kick in.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
BABIES UNDER 1 YEAR
The Under one year of age is interesting since there is actually a slight dip in mortality. Are weaker babies more subject to spontaneous aborting after Mom is vaxed?
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
TIMELINE of Emergency Use Authorization of mRNA VACCINES
The FDA makes it VERY HARD to figure out just when they authorized the use of the mRNA vaccine in youngsters. I gleaned out the following dates. Starting from the FDA Covid Vaccine site.
Turns out it is the CDC who has the final say on vaccination of children so I have also included the CDC news releases.
12/18/2020 – EUA issued for the Moderna COVID-19 Vaccine, December 18, 2020. Emergency Use Authorization (EUA) of the Moderna Inc. COVID-19 Vaccine for the prevention of COVID-19 in individuals 18 years and older.
YEAR 2021
06/10/2021 — Vaccines and Related Biological Products Advisory Committee will meet in open session to discuss, in general, data needed to support authorization and/or licensure of COVID-19 vaccines for use in pediatric populations.
FDA DEFINES: Pediatric use. (A) Pediatric population(s)/pediatric patient(s): For the purposes of paragraphs (c)(9)(iv)(B) through (c)(9)(iv)(H) of this section, the terms pediatric population(s) and pediatric patient(s) are defined as the pediatric age group, from birth to 16 years, including age groups often called neonates, infants, children, and adolescents.
. 09/17/2021 — Application for administration of a third (“booster”) dose of Comirnaty (COVID-19 Vaccine, mRNA) in individuals 16 years of age and older.
10/26/2021 — Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss a request to amend Pfizer-BioNTech’s Emergency Use Authorization (EUA) for administration of their COVID-19 mRNA vaccine to children 5 through 11 years of age.
10/14/2021 – Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss the Emergency Use Authorization (EUA) of the ModernaTX Inc. COVID-19 vaccine and the Janssen Biotech Inc. COVID-19 vaccine for the administration of an additional dose, or “booster” dose, following completion of the primary series, to individuals 18 years of age and older.
Today, CDC Director Rochelle P. Walensky, M.D., M.P.H., endorsed the CDC Advisory Committee on Immunization Practices’ (ACIP) recommendation thatchildren 5 to 11 years oldbe vaccinated against COVID-19 with the Pfizer-BioNTech pediatric vaccine. CDC now expands vaccine recommendations to about 28 million children in the United States in this age group and allows providers to begin vaccinating them as soon as possible.
The Food and Drug Administration today authorized Moderna’s COVID-19 vaccine for children aged 6 months through 17 years old and Pfizer’s COVID-19 vaccine for children aged 6 months through 4 years old, as recommended this week by its vaccine advisory committee. The vaccines previously were authorized for older children.
Before vaccinations can begin, the Centers for Disease Control and Prevention must recommend the vaccines for these age groups. CDC’s Advisory Committee on Immunization Practices is scheduled to vote tomorrow on whether to authorize the vaccines for children age 5 and under.
Children 6 months through 5 years of age who received the original (monovalent) Moderna COVID-19 Vaccine are now eligible to receive a single booster of the updated (bivalent) Moderna COVID-19 Vaccine two months after completing a primary series with the monovalent Moderna COVID-19 Vaccine.
Following today’s meeting of the Advisory Committee on Immunization Practices’ (ACIP), CDC is expanding eligibility of COVID-19 vaccine booster doses to everyone 5 years of age and older. CDC now recommends that children ages 5 through 11 years should receive a booster shot 5 months after their initial Pfizer-BioNTech vaccination series.
Looking around the CDC website, I eventually found what I was looking for. It was off the beaten path, but in a place where journalists were apparently used to looking for goodies on a weekly basis.
This is much like an academic paper. Here is the title information:
Let’s put that into text.
Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems — United States, August 2022
Early Release / August 11, 2022 / 71
Greta M. Massetti, PhD1; Brendan R. Jackson, MD1; John T. Brooks, MD1; Cria G. Perrine, PhD1; Erica Reott, MPH1; Aron J. Hall, DVM1; Debra Lubar, PhD1; Ian T. Williams, PhD1; Matthew D. Ritchey, DPT1; Pragna Patel, MD1; Leandris C. Liburd, PhD1; Barbara E. Mahon, MD1 (View author affiliations)View suggested citation
Summary
What is already known about this topic?
High levels of immunity and availability of effective COVID-19 prevention and management tools have reduced the risk for medically significant illness and death.
What is added by this report?
To prevent medically significant COVID-19 illness and death, persons must understand their risk, take steps to protect themselves and others with vaccines, therapeutics, and nonpharmaceutical interventions when needed, receive testing and wear masks when exposed, receive testing if symptomatic, and isolate for ≥5 days if infected.
What are the implications for public health practice?
Medically significant illness, death, and health care system strain can be reduced through vaccination and therapeutics to prevent severe illness, complemented by use of multiple prevention methods to reduce exposure risk and an emphasis on protecting persons at high risk for severe illness.
Given that NPR is an official party organ, that’s pretty serious. I repeat:
So assuming you’ve read one of the summaries (Fox or CNET) or at least the NPR checklist, what do more critical voices think?
Many people consider it a REVERSAL OF POLICIES in several important ways. Naomi Wolf, who has championed medical freedom from a classical liberal standpoint, is one of them.
Naomi and Steve Take a Tour of WTF Falls
CDC’s sudden reversal on COVID guidance – from obsessively meddling and frequently “backwards” to “almost sane” – is almost certainly political in many ways, including a reaction of the DNC to their dismal prospects in the upcoming election. And yet the new guidance does do some scientific “hand-waving” to justify itself.
Without making enough of a point about natural immunity to admit its superiority to the immunity offered by the “vaccines”, CDC has admitted the fact that natural immunity, along with clot shot immunity, has effectively ended the crisis of the virus.
The crisis of the vaccinated, however, is just beginning.
people don’t want COVID vaccines – Moderna is throwing out 30 million unwanted doses
people don’t want the vaccines for their kids
vaccines don’t affect transmission, and CDC no longer says so
there’s no reason to have mandates, firings, dismissals
now after all the destruction, not even an apology, just ignore vaccination status
“the edifice is crumbling, because so many people have exposed their lies”
the legacy media is not questioning the reversal – just putting it out there
CDC is making up a fantasy about the science having evolved
no evidence is presented, just as no evidence was presented before
no mention is made of the devastation from the policies that went before
So what does the Wolf think of all this?
Light in August
The novel is an exploration of what we think we know vs what we actually know.
Pamela Jean, Goodreads
To dig out the truth, as scientists instead of artists, we have to “think we know” things, and on average, more often than not, what we think we know has to turn into what we actually know.
In addition to simply denying us “things we think we know” by gaslighting and censorship, one of the ways that criminals get away with things, is by throwing enough phony “think we know” at us, to prevent us from ever getting to the point of actually knowing things.
“Chaff and countermeasures“, as Sundance likes to call them.
To me, the very first CHAFF is right in the “title” of the “new guidance”. The PROPAGANDA is LEADING with the “new goal”.
Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems — United States, August 2022
These creeps didn’t just say something short and open-ended like “Summary of Guidance for Management of COVID-19, August 2022” – they added their alleged goal right there.
“Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems“
WAIT A MINUTE.
SO – suddenly THAT MATTERS?
It didn’t matter EARLIER.
These two things are things we actually know.
That title of the new guidance could have been written by Scott Atlas. You know – the SWORN ENEMY OF SCARF WENCH. And yet – we are now in the BIDEN administration – which pushed the FATAL SHOTS.
It has been my contention that Scott Atlas was ABSOLUTELY NOT on #TeamDepopulation, and that Birx refusal to even go to meetings where he was present, was not only a smart tactic of policy engagement, but a tactic of “big plot defense”.
If there was ever anybody who would have seen through to the “virtuous depopulation plan to save the planet from climate change” in real time, it would have been Scott Atlas. Here is a guy who understood motivation in health care, from the inside – but obviously from the “old days” of FIRST, DO NO HARM. He’s old school – just look at his age – obvious in the picture. If Birx would have slipped up somehow in gunning for more control, less treatment, and ultimate reliance on the statistically fatal shots, it would have been clear as day to Atlas. HIS suspicions could have been raised to the proper levels.
This is something we THINK WE KNOW – not something we ACTUALLY KNOW.
At least, NOT YET.
Ideas that can become things we ACTUALLY KNOW have to become CONCEIVABLE first, and to become conceivable TO THE PUBLIC, they have to become public.
This is why ALL THE CENSORSHIP. The “virtuous depopulation plan” was not allowed to become conceivable in the minds of men and women, by not allowing the smaller components of the idea to take shape – to fit together like a jigsaw puzzle, leading to NEW EVIDENCE.
Sure – they love to let people make the BIG assertions, because who would believe them? It’s the smaller things that add up, that allow us to see that 1+2+3+4=10.
Now – Birx is a tricky one. Not only does she admit to sabotaging Trump in terms of her reporting practices and bureaucratic policy documentation, which can be made to look virtuous to the left – she even tried to feed Trump rope to hang himself, which is at best unseemly, and at worst treasonous.
An example of that level of personal duplicity is how Birx gave Trump a “tour of the incredible” in terms of COVID cures, leading Trump to then give the waiting Fake News media exactly what it wanted – “injection of bleach”, “crazy ultraviolet treatments”, and all that noise.
Let’s be very blunt. Birx SET TRUMP UP. KNOWINGLY.
At the time of “infamous injection of bleach”, I was struck by Trump’s demeanor when stating the things he did. It was clear to me that he KNEW this would feed the media with red meat for controversy, but even more, I detected DISDAIN FOR BIRX, as he mentioned VERY BRIEFLY having gotten the tour, and then proceeded to “step into the trap” by stating some of the things they looked at, stripped of anything he MUST have heard, supporting their scientific credibility.
Typical Trump – allowing the Fake News to backhandedly validate him, while not “appearing weak” by making the arguments himself.
He let Scarf Wench crow for the moment, only to “wear the L” later.
Getting back to the point, there has to be a set of reasons WHY CDC is suddenly “normalizing normal again”.
Democrats are no longer pretending. They’re doing the right thing. WHY?
The election is surely one of them. Democrat voters need to come back for their hug after being bitch-beaten to the graveyard.
But there is MORE. This policy is IN MOTION. It has already been allowed to pass the phalanx of school administrators, who had earlier enjoyed their lockdown and mandate powers well beyond the expiration date.
Holly brought us EVIDENCE in that regard. I invite you to enjoy this conversation as much as we did!
Good sign! Utica University’s fall 2022 covid policy no longer requires the vaxx or exemptions for ANYONE. Private and in New York. This is a big deal.
This is now something we ACTUALLY KNOW. Democrats (teachers unions and university administrators) are doing a 180 in terms of feeding the “protesting parents of Democrat-abused children” with any MEDICAL reasons to protest. Even at the CDC level, they are relenting.
WHY? Just for the election?
Democrats are STILL pushing both TRANS and CRT in schools. Indeed, the early assertion that the notorious Tavistock Institute was being shut down not as victory over TRANS, but as a form of TARGET DENIAL, so that TRANS could be disseminated to hospitals and schools, seems to be borne out, as the center of the fight has indeed shifted to a multitude of “woke” hospitals with insane new TRANS policies.
No. There is more. And I may not ACTUALLY KNOW that the depoppers in American medical bureaucracy are strategically retreating, but I certainly THINK I KNOW THIS.
Fauci’s announced retirement at the end of the Biden administration notwithstanding, I suspect that he will exit SOONER – particularly in the event of Republican control of the House. This will have the effect of thwarting public revelation of facts which would lead irrevocably to the realization of what I am certain actually happened – that a shot which damages the hearts of ALMOST ALL RECIPIENTS AFTER REPEATED INJECTION was advanced KNOWINGLY.
I find it interesting that science is now catching up to the plot, and results which should have been obvious earlier, if things were actually innocent, are NOW becoming obvious to scientists who are innocent enough to publish.
Consider the NUMBERS in this very recent Thai study. My comments on Gab, wrapped around comments by Steve Kirsch, who sees the same evidence, but seems to be keeping any recognition of the plot quiet for now. AND YET HE TAUNTS THEM.
What was that they were saying, that had no effect on Republican scientists, but might actually troll up some Democrat scientists to “action”?
“There’s no time.”
Likewise – at the top – people who are intellectually unable to question science from a standpoint of common sense and moral solidity, can easily get out over their skis, when urged by others who they trust. I think I know that Andrew Cuomo is one of them.
I don’t ACTUALLY know who had prior knowledge of the “left-virtuous plan”, but I am gaining pieces of the puzzle every day. Millions of actions which appear to be mistakes, take shape when we consider that thousands of those actions, committed by a small but core cadre of “knowing” participants, created virtue signals that drove the vast remainder of DUPES to participate in a massive folly.
And what is that folly?
Deploying the MOST ADVERSE VACCINE IN HUMAN HISTORY – while simultaneously REFUSING TO EXAMINE OR ADMIT the evidence of its adversity. The actions of the whole PROTECTED THE ADVERSITY.
And remember – that ratio – scientifically studied by the CIA – makes all sorts of things possible.
Motivations in real conspiracies are always complex, interlocking, apparently contradictory, and tend to “shift and flip” in going down from the most knowing top to the less knowing bottom – yet each layer knows the guilt of their own interests and participation. This form of guilty self-motivation locks people – including mostly innocent people – into defending the whole construct.
I do not actually know who the core cadre is, but I’m working on it.
Your suspicions as to WHO THEY ARE – are welcome.
We are an investigatory collective. We are free to postulate – to hypothesize – to be both scientists and detectives.
I know what I think. I ACTUALLY KNOW what I think I know.