“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
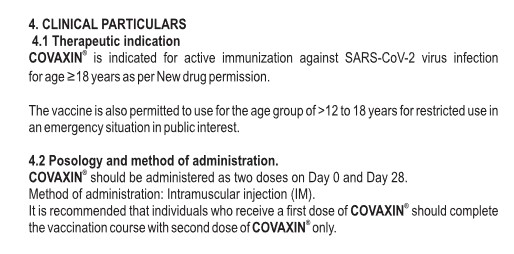
This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both).
Our various sister sites, listed in the Blogroll in the sidebar
Our beloved country is still under Occupation by hostile forces, but we are evicting those forces!
Daily outrage and epic phuckery still abound.
We can give in to despair…or we can be defiant and fight back in any way that we can.
Joe Biden didn’t win.
And we will keep saying Joe Biden didn’t win, long after we got His Fraudulency out of our White House.
Wolfie’s Wheatie’s Word of the Week:
damoiseau
noun
male form of damsel
a young man not yet dubbed a knight
a young gentleman who was not yet a knight but aspired to be one
a young nobleman accompanying his lord or lady to hunt, walk, travel, etc.
a young nobleman or squire
Used in a sentence
The word damoiseau appears to be related to the word mademoiselle.
Shown in a picture by Gab’s Watercolor AI
Video of a rum distillery named Damoiseau.
MUSIC!
What kind of music do you get back when you search on “damoiseau”? Well, somewhere down the page you get one of cthulhu’s favorite bands – “Pample Moose” or whatever. So let’s just go with it!
THE STUFF
In honor of my former colleague, who was SEMPER FIDELIS in all matters of Q, it is my plan to make sure that certain touches of what she regarded as important are not forgotten.
Trump world problems! Almost as bad as too much winning!
Susie Q is right. Something is going on here. And it’s good!
Remember Kary Mullis? Establishment popularization science remembers him, and while Veritasium keeps the expected diss of this gnarly dissident fairly gentle, their coverage fills in a lot of blanks, and is appreciated by this more lupine dissident. Don’t worry – you’ll still like Kary – maybe even a little more after watching this.
A toast to Kary! And today, we’ll skip the LSD, but maybe rum is appropriate.
The above image of a Mental Health word graphic is courtesy of Google Images.
Health Friday is a series about Big Pharma, vaccines, general health, and associated topics. Since today’s post speaks to the COVID-19 disaster, it is dedicated to Yours Truly’s COVID-19 “fully vaccinated and boosted” late brother, Sam; to her late cousin, Bill; and to all others who have died, or have become injured or disabled, directly or indirectly, due to the negative effects of the COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”) they had put into their bodies.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats by Yours Truly, of which readers should be aware. They are linked here. The discussion is not limited to what is presented today: It is an Open Thread.
This post is an Opinion Piece. Yours Truly will be making statements that, hopefully, can start a dialogue on what one believes is an important topic.
To Begin: There are approximately eight billion human beings on Earth at this time. Approximately five billion of these human beings have taken at least one dose of a COVID-19 BTI (aka the “vaccines.”)This means that approximately 61% of the entire population of the Earth has been COVID-19 “vaccinated.” Approximately one billion of these COVID-19 “vaccinated” human beings are already dead, or “vaccine”-injured, or “vaccine”-disabled. Please refer to this tweet, which contains a video clip from a recent interview between Ed Dowd and Brett Weinstein: https://x.com/_BlakeHabyan/status/1872735868709941748, which discusses this situation. This number will increase as time goes on, and as more COVID-19 “vaccinated” persons succumb to “vaccine”-induced injuries, “vaccine”-induced disabilities, or die from the negative effects of these injections. In addition, Yours Truly believes it can be fairly argued that what may be called the “ripple effects” among all persons in the world from the COVID-19 BTI (aka the “vaccines”), including among persons who are not “vaccinated”, will eventually be felt by every person on the planet.
Yours Truly will state at the outset that she is neither a medical professional, nor a mental-health professional. However, she has taken psychology and sociology courses in the process of earning two BFA degrees and an MA degree. She has also researched into the effects of the COVID-19 BTI (Bioweapon Toxin Injections, aka “vaccines”) on the body and brain of the “vaccinated” since March 2020. One will use terms “COVID-19 BTI” and “COVID-19 vaccines” interchangeably.
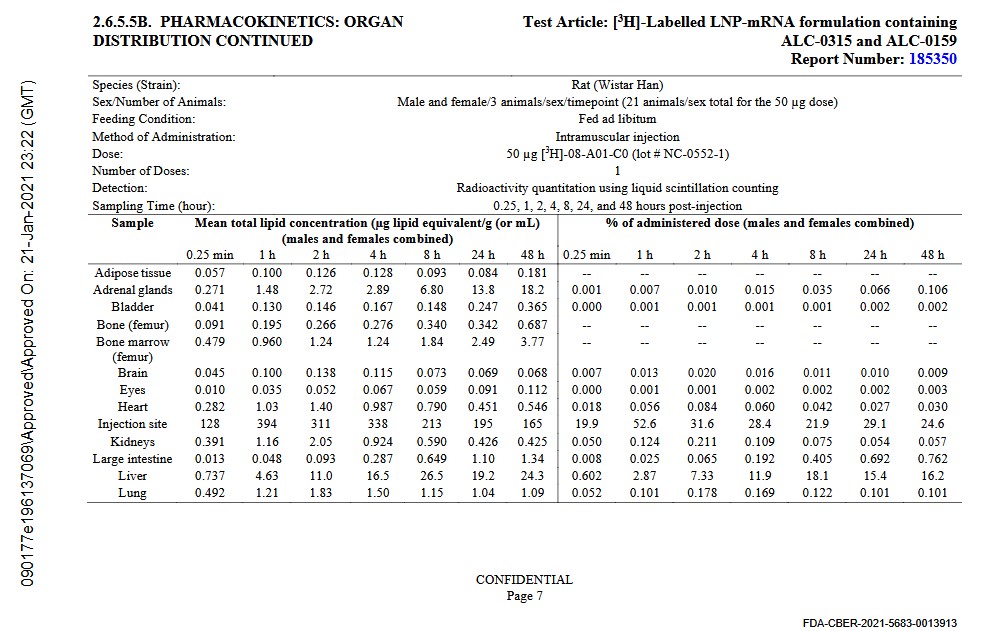
Note the accumulations of BNT162b2 in the Brain, the Adrenal Glands, and in the Pituitary Gland. Note especially the accumulations in the Liver. The Liver is where the body produces Uridine, which is crucial for all kinds of body functions, including the regulation of mood. This is all part of what is called the “Brain-Gut Connection.” The human gut (stomach, intestines, liver, etc.), and, importantly, Uridine, sends “signals” to the brain, which processes these signals and “translates” them into body functions, emotional reactions, mood states, cognitive processes, and more. The N-1 Methylpseudouridine in the modRNA COVID-19 “vaccines” literally replaces the RNA of the body’s natural Uridine with a combination of “fake Uridine” (which evades the body’s “are you a friend or a foe” recognition and elimination mechanisms), plus a form of methane.
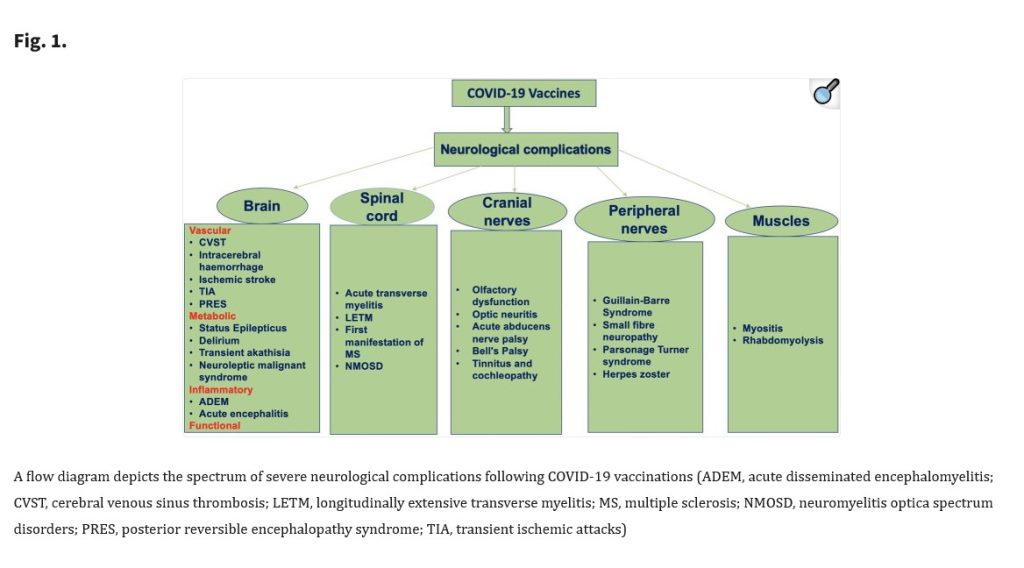
There is an increasing number of scientific papers, articles, and editorial pieces regarding the negative effects on the brain, its components and mechanisms, and on its emotional-psychological functions, after COVID-19 “vaccination.” These negative effects range from inducement of “autism-like” behavior, to inducement of psychosis, to reports of suicide attempts and depression, and more. Examples of such writings include: https://doi.org/10.1007/s11064-023-04089-2. “Prenatal Exposure to COVID-19 mRNA Vaccine BNT162b2 Induces Autism-Like Behaviors in Male Neonatal Rats: Insight into WNT and BDNF Signaling Perturbations”, Mumin Alper Erdogan, et al., Epub 10 January 2024; www.psychiatrist.com/pcc/psychosis-associated-covid-19-vaccination/, Abdulsamad A. Aljeshi, MBBS, FRCPC, et al., 17 February 2022; https://pmc.ncbi.nlm.nih.gov/articles/PMC8716269/, “P.0707 Suicide attempt and depression after COVID-19 vaccination: a case report”, IA Gencan, et al., 30 December 2021; and, https://doi.org/10.1007/s10072-021-05662-9, “Spectrum of neurological complications following COVID-19 vaccination”, Ravinda K Garg, Vimal K Paliwal, 31 October 2021. Below is Figure 1. from the Garg and Paliwal paper:
Note that the neurological issues induced by COVID-19 “vaccination” are not confined to “vaccination” by the modRNA COVID-19 BTI; they also occur after “vaccination” with the adenovirus DNA COVID-19 BTI by AstraZeneca.
There are also studies that have been conducted regarding the mental health of persons who have what is called Long COVID; for example: https://scholarcommons.towerhealth.org/t-med/vol3/iss2/2/ “Examining the Mental Health Impact: Investigating the Association between Suicide and Long Covid Syndrome”, Nicole Ann E. Villa, et al., June 2024 (click on the article title at the URL link and the PDF will load.)
However, there is also a myriad of other mental-health issues that arise regarding COVID-19. For example: What about a person who is COVID-19 “fully vaccinated and boosted” who then passes away from “died suddenly”? What mental-health effects does this produce in the deceased’s survivors? — such as, grief — shock — denial — anger — and more? For example: What about a COVID-19 “fully vaccinated and boosted” person, who has previously-diagnosed mental-health issues that were under control, but then after “vaccination” presents with symptoms of aggravation of these issues? — such as, onset of new psychosis — loss of interest in daily activities — anxiety — and more? For example: What about a COVID-19 “fully vaccinated and boosted” person who then presents with a disability? — the mental-health issues that can arise from this, and the issues that can arise among the affected person’s family members? — such as, anxiety — grief (over lost abilities and opportunities) — anger — depression — and more? For example: What about non-COVID-19 “vaccinated” persons who have friends and family who are “vaccinated”, and who are starting to see the negative effects of these “vaccines” present in their loved ones? — such as, “anticipatory grief” — anger — sadness (especially if the non-“vaccinated” person tried to warn them)?
There are, in addition, the hormones that the body will release when under stress, in danger, in grief, and similar situations, among them cortisol and adrenaline. These hormones, once released into the body, interact with the Gut-Brain connection organs, and with the Vagus Nerve, which is an important component of the whole. For some further information on the Vagus Nerve, and its importance in good health please see: https://marica1776.com/2023/03/17/53289, “The Glass Wall Part 3 — The Body Needs a Healthy Vagus Nerve.”
Refer back to the images of page 7 and page 8 of the Appendix 1. in the BNT162b2 report above, regarding accumulations of BNT162b2 in the organs of the “vaccinated” lab rats in the study performed. The Brain, the Adrenal Glands, the Pituitary Gland, and the Liver all perform immensely important functions and regulation processes for the entire body — including in cognitive and emotional/psychological processes and regulation. It is clear that the modRNA COVID-19 BTI accumulate in, and attack, these very important areas of the “vaccinated” person’s body. **** And there is also this: Researchers at Yale University have found out that the spike protein from the COVID-19 BTI remain the body of the “vaccinated” person for as long as 700 days post-injection — https://alexberenson.substack.com/p/urgent-yale-researchers-have-found, “URGENT: Yale researchers have found Covid spike protein in the blood of people never infected with Covid — years after they got mRNA jabs”, 19 December 2024. This as-yet-unpublished study, called the “LISTEN study”, was headed by Dr. Akiko Iwasaki, a COVID-19 “vaccine” proponent. The findings are shocking. In addition to the COVID-19 spike protein being found in the blood of “vaccinated” persons for as long as 700 days post-injection (and that these “vaccinated” persons had never tested positive for COVID-19 infection), it was found that their CD4 immune system cells were compromised; also, that the DNA in the plasmids of the “vaccine” can indeed integrate into the genome of the “vaccinated” person’s body.
The implications of this the LISTEN study results are profound. It appears that the COVID-19 “vaccinated” person’s body literally manufactures spike protein for a very long time post-“vaccine” injection. However, at the same time, it is also known that whatever “immunity” that is “conferred” by COVID-19 “vaccination” dissipates after a matter of weeks or months. Thus, it is possible that, while the “immunity” conferred by these “vaccines” is short-lived, the body’s manufacturing of continuous amounts of spike protein from these “vaccines” is ongoing. The implications of the negative impacts of these “vaccines” on the mechanisms and processes of the Brain, the Adrenal Glands, the Pituitary Gland, and the Liver, especially with repeated “vaccine” injections, are likely incalculable.
Meanwhile, what can COVID-19 “vaccinated” persons (and, also, non-COVID-19 “vaccinated” persons) do to support their personal mental health in the era of COVID? The answer is unique to each individual. Some may have psychological counseling. Some will decide to make healthy changes to their diet, or to incorporate daily exercise. Others may consult their personal physician. Still others may craft a program of their own. Yet others will turn to meditation, and/or to a spiritual Force or Supreme Being to guide them. Some will consult with alternative medicine practitioners. And so on. However, what will not work is to turn to drug or alcohol abuse. What will not work is unhealthy or harming behavior to the self or to others. Here are two online resources, among many others, that provide helpful information: www.helpguide.org/mental-health/grief/coping-with-grief-and-loss. by Melinda Smith, M.A., et al.; and, www.anxietycentre.com/, which has many free articles, videos, and other resources.
The issue of mental health in the era of COVID is one that is an unfolding situation. It deserves deep and ongoing investigation. Today’s Opinion Piece can hopefully be part of the conversation about this issue.
A Complete Description of an Alternative Chemotherapeutic Approach Which Quickly Led to 100% Cancer Freedom
Foreword by WOLF MOON
Most of the regular denizens of The Q Tree are familiar with Linda’s journey through the terrifying uncertainty of a cancer diagnosis and treatment during the last year. That story, spread out over many daily threads here on the website, is incredibly hard to stitch together, if you have not been following along.
Just a few days ago, we were blessed with amazing news. While all of us were thrilled by the good news, I had to admit that I had already forgotten very important details of the original diagnosis. Some of it may have been mixing things up with my wife’s case, or that of a friend’s wife, but still – it wasn’t a great moment in the history of my memory.
Rather than asking Linda a million questions, and surely having others do the same, I had an atypically inspired idea – why not ask Linda to re-tell the whole story as one coherent statement, and better still, tell us with her current perspective? Wonderfully, Linda agreed to do just that.
That’s all I’m saying. Here is Linda, in her own words. I have not changed a thing.
MY CANCER JOURNEY
As many of you know, I was diagnosed with breast cancer last August. Looking back, it was only by the hand of God that it was found at all. For a good part of my adult life, I’ve avoided going to doctors for anything but what I can’t find a way to treat myself. I found out a long time ago in dealing with my hypothyroidism that most doctors are not going to deviate from their strict standard of care, which means Big Pharma drugs, whether they really help or not. And I try to avoid Big Pharma drugs if at all possible.
So I wouldn’t have gone to the doctor at all except I had a pre-cancerous lesion that I wanted to get zapped. I get my health care from the VA and they actually now have a primary care clinic in Salem. They assigned me a primary care NP and gave me an appointment. She wasn’t about to just zap the lesion but also gave me a complete physical along with labs and insisted I get a mammogram.
I drug my feet for a couple of weeks, but finally made the appointment and thankfully got it done. They found a small mass in my left breast and then did a needle biopsy using ultrasound a week later. They found that I had ER+ PR+ HER2- breast cancer. ER+ and PR+ mean that my cancer has estrogen and progesterone receptors. HER2- is a less aggressive cancer than HER2+, so I caught a break there.
At that point, I started reading everything I could find on fenbendazole. I heard it mentioned here several times on the Q Tree as a cancer treatment, but didn’t know where to get it, how much to take, or what to take it with. I finally found the Fenbendazole Cancer Support Group on Facebook that gave me most of the answers that I was looking for, a protocol I could use and adjust for my own situation, and a lot of support from others fighting cancer. This is the group:
It’s a private group. But anyone who has cancer or is the care giver of someone with cancer can join. There are a lot of health care professionals in the group who are very knowledgeable. They have a suggested protocol that anyone can download and use. Most people take that protocol and adjust it for their own needs. I doubt that any 2 people in that group are using the exact same protocol. One thing to keep in mind is that the protocol doesn’t mention Ivermectin. During COVID, Facebook was closing down groups and banning people for even mentioning Ivermectin, so they didn’t include it or allow people to talk about it until about the last year when that changed. But most people in the group are taking 24 mg of Ivermectin a day as part of their protocol.
Ivermectin is super important because it actually kills cancer stem cells in addition to all the different ways it fights cancer. Chemotherapy and radiation therapy don’t kill cancer stem cells, which is one reason why cancers come out of remission.
The whole point of having a cocktail of supplements taken at different times of the day is that you need anti-cancer compounds circulating in your body 24/7. It’s really amazing to me how many foods and supplements actually have anti-cancer qualities. And that’s important because cancer has a lot of different pathways to get fuel for growth and different signalling mechanisms to spread and metastasize. Some supplements attack one or two of those pathways, but you need different ones to attack other pathways. Jane McClelland wrote a book called “How to Starve Cancer” in which she identified all the pathways cancer uses to grow and to spread and then found old drugs that could be used to block all those pathways. She cured her own cancer that way. The problem for most of us, though, is getting a doctor to prescribe all those old, out-of-patent drugs! Using supplements that do much the same thing instead of Big Pharma drugs is the answer.
When I first started, I bought most of what was on their protocol. I also tried a lot of different supplements that people suggested and found worked well for them. Many people swear by soursop tea and Esiac tea. I’m not much of a tea drinker, but I do drink soursop tea once in awhile. Another was frankincense (Boswellia). It has anti-inflammatory properties and anti-cancer properties as well. I was really excited about trying it, so I bought a couple of bottles only to find out after a week that it caused unbearable itching all over my body. Needless to say, I dropped that one! The point is to use what works best for you and also to make sure there are no interactions with any drugs you may be taking.
This is the protocol I finally settled on:
1 Hour Before Breakfast: Hi-Dose Serrapeptase – 120,000 spu
2 Hours After Dinner: D3 – 5,000 mg (I drop that to 2,000 in the summer) Magnesium – 400 mg Melatonin – 400 mg
Before Bed: Hi-Dose Serrapeptase – 120,000 spu
That probably sounds like a lot of supplements. It did to me, even though I already took a lot of vitamins and supplements. And fenbendazole, ivermectin, and supplements can be expensive to buy month after month after month. But I managed it on my social security check. A number of people in my cancer group who had undergone more traditional treatments ended up paying thousands of dollars their health insurance didn’t cover. So maybe I actually took the cheaper route.
But for someone on a really limited budget, I think they would still do really well just starting with Fenben, Ivermectin, Tudca (or milk thistle), and Serrapeptase (or pectasol). Fenben and Ivermectin are the big guns that each fight cancer in a half dozen different ways. Tudca or milk thistle is for liver support. Serrapeptase (or pectasol) is used to get the dead cancer cells out of your system so the cancer doesn’t use them as fuel.
With fenbendazole, you can’t immediately start with a high dose or you’re going to have a Herxheimer reaction – a lot of flu-like symptoms. Taking it slowly helps a lot. What was stressed in my cancer group was to work your way up to the higher doses and monitor your liver numbers as you go. I started at 222 mg for a week, then 444 mg the next week, then kept increasing at that pace until I got up to 1500. I reached 1500 mg about 2 weeks before my lumpectomy surgery. I could have gone up to the 2000, but at that point I found out that my tumor had shrunk by half so I just stayed at that dose. I knew it was working and would continue to work at that point. It’s really important to take fenben AFTER eating a meal that contains fat for absorption. Or as an alternative, you can mix the powder with a little bit of DMSO. This also helps fenben penetrate the blood brain barrier for those who have a brain cancer.
Anyone researching Fenben is going to hear about Joe Tippens. He had small cell lung cancer and used Fenben and a few other supplements in his protocol. He never took more than 222 mg 4 days a week. Unfortunately, this protocol has gone all over the internet and people think that’s all they need. They try it and find it doesn’t work for them. The problem is that 222 mg is the dose you would give a 10 pound dog, not a human. Most people are going to need 1,000-2,000 mg per day, especially if they have a late stage or aggressive cancer. Joe Tippens was on an immunotherapy trial at the same time he was taking Fenben, so that is undoubtedly why it worked for him. In my cancer group, there are many people who had stage 4 cancers who ended up cancer free on this protocol. They all took close to 2,000 mg per day of Fenben.
Protecting your liver during this protocol is really important. Fenbendazole will cause a lot of cancer cell die-off and start to stress your liver. Tudca or milk thistle will add protection. Dandelion root and burdock root also protect the liver. If you have a hormonal cancer like mine, or you have a lot of other health issues, you shouldn’t take milk thistle or dandelion root. Tudca is recommended for those in that situation. Tudca is simply a bile salt and very safe. Most people start with 500 mg twice a day. However, once I got to 750 mg of Fenben, my liver numbers started rising out of range. Raising my tudca dosage to 1,000 mg twice a day brought them back down.
My cancer group recommends you get liver labs every 2-3 months. Most doctors aren’t going to order them for you. They would probably discourage you from using fenben or ivermectin to start with. Many people don’t know that you can order your own lab tests online, print out the requisition, and then take it down to your local lab and get your blood drawn. I order my labs from Ulta Lab Tests. Their Liver Function Panel is $19.95 and can be ordered here:
You also need to take high dose serrapeptase twice a day to get the dead cells out of your system after fenben and ivermectin kills them. Otherwise, your cancer will actually “eat” those dead cells as fuel. Plus, your liver will have to work a lot harder. You need to take 120,000 spu twice a day. It must be taken at least 2 hours after eating and at least 1/2 hour before eating. I always took mine before bed and an hour before breakfast. Then 1/2 hour before breakfast and dinner I would take my tudca and a couple other supplements that need to be taken on an empty stomach. Amazon or iherb both have high dose serrapeptase. The one I use is the Drs. Best brand.
Anyone on blood thinners shouldn’t take serrapeptase, but substitute Pectasol (modified citrus pectin) instead. You need 15 grams daily for the best anti-cancer benefits. 1 scoop of powder is 5 grams. So you can take 1 scoop 3 times daily or 1.5 scoops twice daily. It’s taken the same way as serrapeptase – 2 hours after eating and at least 1/2 hour before eating.
Those 4 items – Fenben, Ivermectin, Tudca (or milk thistle), and Serrapeptase (or Pectasol) – are a great place to start and can form the basis of any protocol. You can add more supplements as you go along. But those 4 are critical.
You may be wondering about that super high dose of melatonin I take – 1,000 mg per day. Many people take 3-5 mg before bed to help with sleep. 1,000 mg sounds like it would put you in a coma all day. Actually, you don’t feel the effects at all until it gets dark and that seems to trigger the sleepiness. Melatonin is really great for cancer. It fights cancer 6 different ways, particularly at higher doses. The cancer group recommends taking 300 mg an hour before any scan that involves radiation to protect from some of the effects. If you want to learn more, “Doris Loh Talks” is a private Facebook group about the healing benefits of high dose Melatonin based on scientific research.
I buy melatonin powder because it is a lot cheaper than pills. 1/16 teaspoon is 200 mg. Amazon has tiny measuring spoons that go down to 1/64 teaspoon that are really handy. Here is where I buy melatonin:
I starred two items in my protocol – iodine and DIM – because they’re very specific to breast cancer. The two places in the body that use over 95% of the iodine the body needs are breasts and the thyroid. Iodine at 50-100 mg per day has also been shown to very effectively fight breast cancer. Like Fenben, you shouldn’t just start at 50 mg or you’ll end up with a Herxheimer reaction. I started with just 1 drop of 5% Lugols in a glass of water then added another drop each week until I reached 8. One nice effect I saw once I reached 50 mg was that I could lower my dosage of thyroid meds. 5% Lugols is really hard to find. Most places only have 2%. But I found a good supplier here:
DIM helps the body to get rid of excess estrogen. My oncologist tried really hard to get me on hormone blockers, but after researching the side effects – osteoporosis and heart issues – I said no and started taking DIM instead.
I get almost all my supplements from either iherb.com or Amazon. The only place I buy Fenben from is the Happy Healing Store:
The group sent a bunch of different samples of Fenben from different suppliers to a testing lab a couple of years ago and the only ones that tested pure fenbendazole were the Happy Healing Fenben and Merck’s Panacur-C and Safeguard. The one from Fenben Labs that you see recommended everywhere was only 5% fenben. A lot of people (including me at first) bought that brand and didn’t think fenben worked. Some guy in Lithuania owns it and the lab he supposedly uses to test his fenben is located at the same address. Buyer beware!
I’ve always bought my ivermectin from an Indian seller because it’s about half the price of the websites based here. And most of the ivermectin is made in India to start with. I bought from India Mart back during COVID. I think Kalbo mentioned them as a source. You just go on the site and post what you want and how you want to pay and vendors will contact you. There are now a lot of Indian sellers that have their own websites to sell ivermectin. The list below are from sites I’ve collected from mentions in the cancer group and from here. I haven’t used anywhere near all of them. The first 2 are the ones I’ve used most recently. You really have to check them out for yourself because some change their payment methods without notice. I prefer using Pay Pal myself. I generally buy 200 12 mg pills at a time because this protocol is long-term and I’ll definitely use them. Shipping from India is generally $30 whether you order a small or large amount.
I was on this protocol a little over 3 months before I had my surgery. I kept dragging my feet because I wanted to see how well the protocol worked. A week or two before surgery they did another ultrasound and I found that my tumor had shrunk by half. I seriously considered not doing surgery at all and just letting the protocol finish the job. But I finally decided that I just wanted to get the tumor out. A lumpectomy is nowhere near as invasive as a lot of surgeries. And they do a lymph node biopsy at the same time. They found that my sentinel node, the closest one to that breast had a micro tumor in it. So the cancer was just starting to metastasize. It could be that micro tumor was actually a lot bigger and had shrunk from the protocol.
As I mentioned last week, that surgery was over a year ago and I just had a mammogram that was completely clear of cancer. This protocol has definitely helped me get there and stay there. I’m now moving to a maintenance protocol to make sure it doesn’t come back.
I really appreciate all the prayers from the people here and people outside this site. I know that in the final analysis, God healed me. He just used the protocol and the good surgeons and nurses at the VA Hospital to do the work. God bless all of you!
Addendum: Notes by Wolf
I want to start by thanking Linda for sharing this information. As you can see, this is enough for almost anybody to get started using fenbendazole to treat cancer. Praise God! This is phenomenal information, and again, thank you to Linda for sharing it. I absolutely feel confident that I could being taking the steps needed to use fenbendazole, based on this article.
Now, a point for the chemically curious.
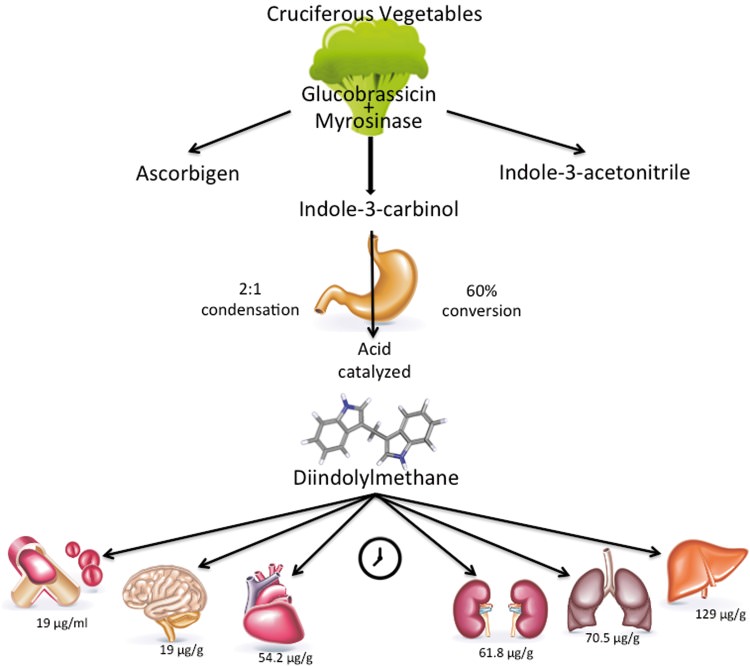
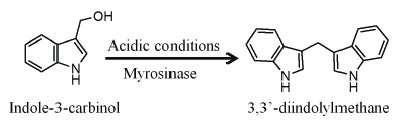
DIM is 3,3′-diindolylmethane, a natural product which is formed by stomach action on another compound found in cruciferous vegetables. The reaction is shown below.
DIM has proven antihormonal effects that are useful for treating breast cancer. See the following medical study.
3,3-Diindolylmethane (DIM): a nutritional intervention and its impact on breast density in healthy BRCA carriers. A prospective clinical trial
Please feel free to ask Linda any questions you might have. I will say right now that she does not have to answer any questions she would prefer not to answer. She can just say “Wolf says next question!” and that’s that! OK? Good! *WINK*
A Simple but Nagging Question Brought to Us by RFK Jr., “Sudden Death”, Unnaturally Red Salmon, and My Dearly Beloved Cheese Balls
I must begin this discussion by admitting that I’m very pro-freedom – and that includes the freedom to conduct honest business without government intervention – which intervention would include taxes. In fact, I have tended, over my lifetime, to scoff at people who want to restrict business over what I generally regard as unfounded allegations of harm.
Thus, I approached the following video, and its enclosing article, with some skepticism. Please read and watch, if you have not already.
Cory Booker? Do they mean, lying, hoaxing, finger-wagging Marxist Cory Booker?
Cory Booker, ally of the Maoist Obama minion Kamala Harris, and assisting perpetrator of the Jussie Smollett lynching hoax?
(No, Michelle Obama and Jussie Smollett didn’t really say that when they were laughing. This is called a “meme”. It’s a form of propaganda and satire. In this case, it is responding to propaganda, fraud, and deception perpetrated by Jussie Smollett, Kamala Harris, and Cory Booker.)
THAT Cory Booker?
So what video would HE promote? More hoaxes and lies?
Let’s take a look. But color me skeptical.
OK – there is a lot to unpack here. This will take a while.
Some background. I am both a scientist, and a lover of the history of science. Far too many scientists are NOT lovers of the history of science, because if they were, they would realize how bad scientists are at spotting the wrongness of contemporaneous science. Which is ALL THE TIME.
And, that would include me. Thankfully, I have often discovered my own wrongness in science within my own lifetime. We’ll get to that, as we move along here.
Now the first thing that irritated me about this video, is the way coal tar is used as a lead-in to attack a food dye called tartrazine, a.k.a. Yellow Number Five.
It almost sounds like Robert F. Kennedy Jr. (RFKJ hereafter) is saying that tartrazine is obtained by draining it out of coal – or if not that, out of “coal tar”, which is somehow gotten out of coal.
Just a side point. Coal tar is a very useful substance, which is actually used as a medicine for treating skin problems.
So – just from the start, it’s not totally justified to demonize coal tar. Yet on the other hand, YES, thank you – hold the coal tar on my deli sandwich, please. It IS medicine, and can even cause cancer.
But FULL STOP. Back to the point. Tartrazine is not exactly “made from coal tar”. It is made from “organic” (carbon-containing) chemicals – basic organic chemicals – that can be made in a variety of ways, from a variety of things, including coal, petroleum, natural gas, biowaste, corn, soybeans, CO2 in the air, apples, healthy fruit – WHATEVER.
See what I’m saying? Tartrazine is being demonized by association. I was ready to bitchslap RFKJ here. Bear in mind that, years ago – before the COVID nightmare and revelations after that – I considered him a NUT – and would often say as much.
AND YET. If you know the history of science and organic chemistry, RFKJ has a point. A very valid point – in that association.
RJKJ clarifies in the video (3 min 6 sec) that tartrazine is now made almost entirely from chemicals which now come from petroleum – not coal tar. However, that original time period – the coal tar days – has something to teach us.
The discovery of synthetic dyes like tartrazine was back when mankind was in a state of “chemical hubris” not unlike the “biological hubris” of current times.
In the same way that we now look back and face-palm at the “irrational exuberance” of early organic and medicinal chemistry, which gave us the hormonal poison diethylstilbestrol (DES), injected into millions of pregnant women before we realized that it damaged their daughters, so we will one day look back at the “clot shot” – marveling at the combination of ignorance (most people), hubris (most scientists), and – behind layers of global governmental denial – malevolent or warped benevolent depopulation do-gooderism (top-secret scientists and psychopathic power players), that pushed bad experimental vaccines on an almost unsuspecting but increasingly skeptical public.
Once I was in the state of seeing the historical analogy, I was ready to realize that there is almost no excuse for allowing anything into food that is not food or a known nutrient.
If one asks WHY Yellow Number Five is in those wonderful-tasting but unnaturally yellow cheese balls, it is obvious – the chemical makes the cheese balls look “cheesier” in a weird but highly unnatural way. It’s psychological. It’s an “allowed psy-op” by makers of food.
Or take salmon. The last time I looked at a really good deal on salmon in the grocery store, I noticed that it was just a bit too strangely orange. Reading the label, there was an admission that the salmon “might” be treated with some dyes to keep it looking attractive.
Suddenly, the salmon didn’t look quite as good to me. It still looked reasonable, and I toyed with the idea of buying it. But I didn’t. In this post-mRNA world, I elected to put off a buy until I could do more research.
So now, after watching this video, I realize that RFKJ is correct. Dyes make foods more appealing, but they do so in a very deceptive way. To me, if dyes have ANY risks, putting them in food makes almost no sense, other than we are allowing “deception in the quality of food” as a kind of freedom. Well, murdering people, stealing their things, and doing other bad things to them are “freedoms” we used to have as humans – and we did away with those freedoms, while keeping most of the rest.
And yet, the enjoyment of food is right there in the Declaration of Independence.
Because I believe in freedom, including the pursuit of happiness in cheese balls and salmon, I don’t want to tell you what to believe, but I will tell you what I believe.
Some people may want vaccines with side effects and risks. I personally don’t, but I want those people to be free to have their vaccines – but not force them on me or my children. And I want the TRUTH about those vaccines to be KNOWN. Not just a little known – A LOT KNOWN.
Some people may want unnaturally yellow cheese balls. I certainly don’t – not any more. I would like some nice, corn-and-cheese-looking cheese balls that I know are healthy for me. But other people may want the yellow cheese balls with strange dyes. Is there a way that we BOTH can be happy? As the founding fathers wanted?
I would like to see more foods without risky, unnatural additives. I would like to see TRUTH IN FOOD and TRUTH IN DRUGS.
I think there is a way forward that will make America HEALTHIER, FREER, and TRUER.
But we have to be honest, if we want to get there.
And what do you know – there are now some people who believe in honesty! And they’re going to be in office, if we continue to support them!
The above vintage image of a Rolodex is courtesy of CSA Images via Google Images.
Today’s Health Friday is a very Special Edition.
God Bless You, my brother Sam — 24 November 1948 – 29 October 2024.
Requiescat in pace aeterna, et Lux Perpetua luceat tibi. You are now with your beloved wife in the next world. Have a wonderful new life together there. “Till we all meet again.”
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and caveat items from Yours Truly, all linked here, of which readers should be aware. The discussion today is not limited to what is presented below — it is an Open Thread.
Health Friday today is a list of links to various scientific papers and articles, blog posts, and other items, regarding the COVID-19 “vaccines” injections (gene therapy injections.) Today’s list is not exhaustive; it is part of an ongoing project. The discoveries that reveal more of the truth about these dangerous and deadly injections, and the items that are published about these discoveries, are increasing by the month. Readers may know some of the information presented below already; other items may be new. And, while the fact is that the COVID-19 “vaccines” have been, and are, inducing injuries, illnesses, disabilities, and deaths in “vaccinated” people all over the planet — there are things that they can do to mitigate, reduce, or perhaps even eliminate, the damage that these “vaccines” have done, and are doing, to their bodies (these links are at the end of The List, Part One.) In addition, in Yours Truly’s opinion, there is one important item that COVID-19 “vaccinated” persons need to at least consider: Do not take any more COVID-19 “vaccine” injections; and, Do not allow these injections to be given to minor children.
The list, Part One:
Three books,: Two, by Naomi Wolf, Ph.D., and Amy Kelly: The Pfizer Papers: Pfizer’s Crimes Against Humanity; and, The Moderna Papers: Moderna’s Crimes Against Humanity. Search by title at https://books.google.com/; and, the third, by Dr. Pierre Kory, MD: The War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the Pandemic; available at www.amazon.com/.
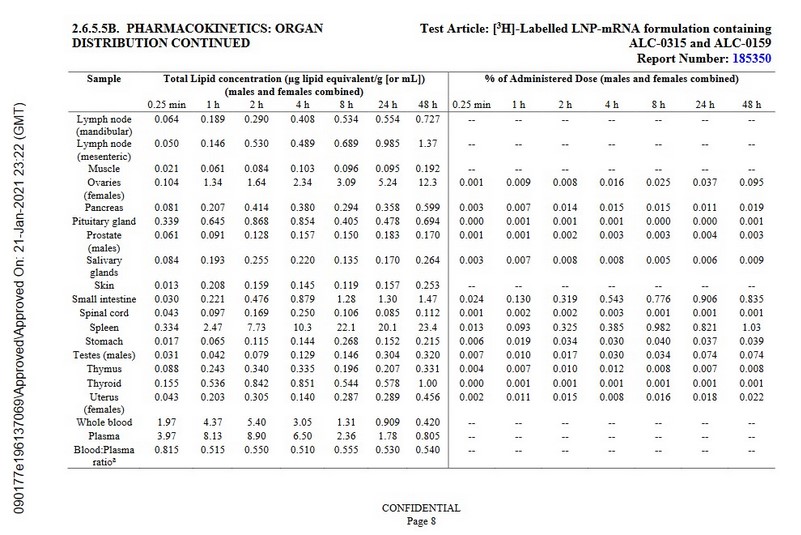
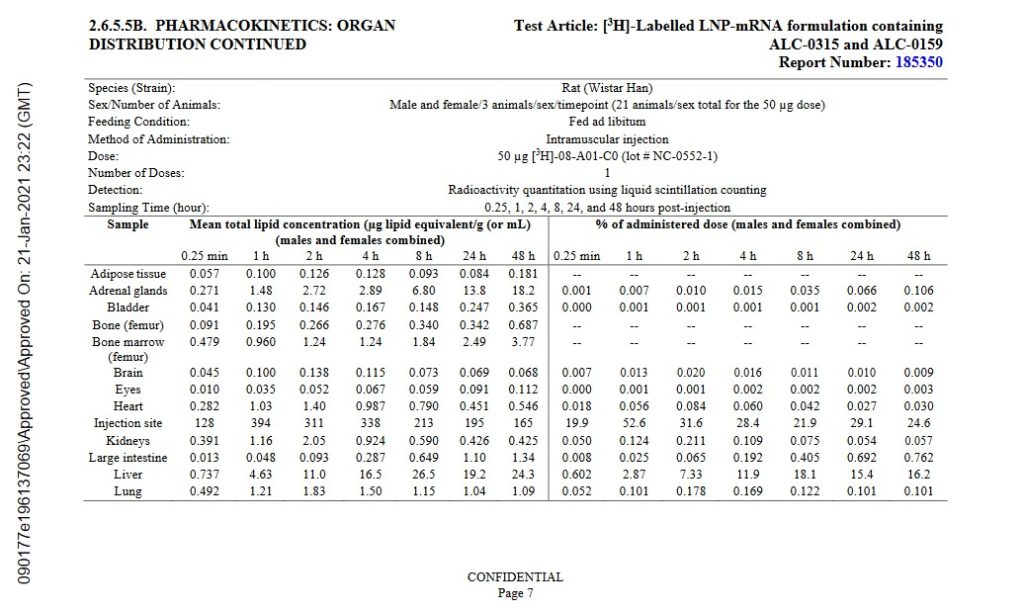
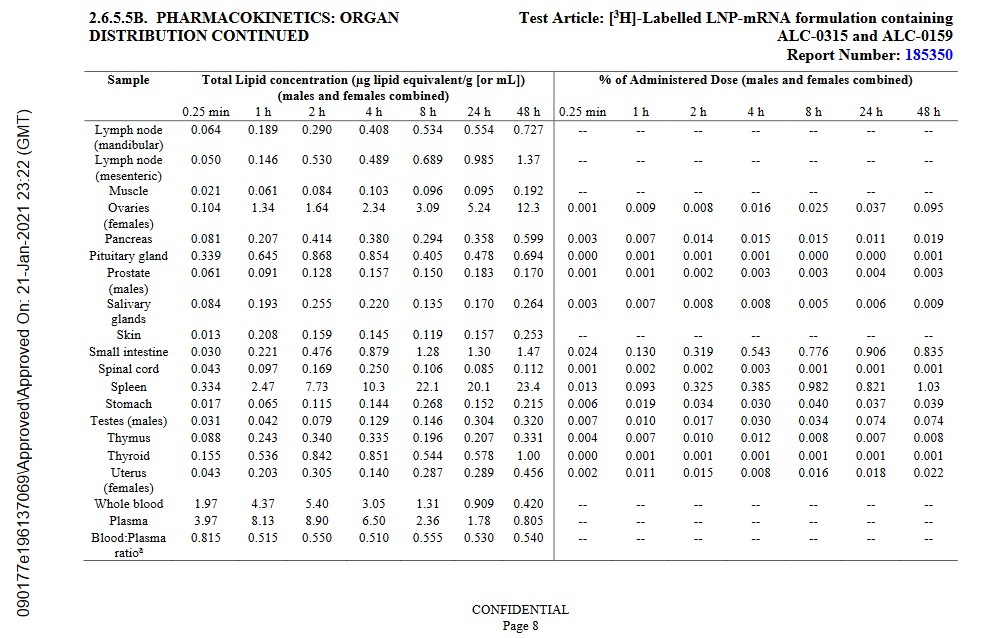
https://icandecide.org/wp-content/uploads/2022/03/125742_S1_M2_26_pharmkin-tabulated-summary.pdf, BNT162b2 Module 2.6.5. Pharmacokinetics Tabulated Summary, FDA time-stamped 21 January 2021. The agency knew, as of this date, that the Pfizer-BioNTech modRNA COVID-19 “vaccine”, BNT162b2, spreads throughout the body of the “vaccinated” person. However, the agency had already granted the initial EUA for this injectable to be used in the United States. This report should have been the signal to the FDA that all use of BNT162b2 needed to be suspended, pending further investigation and testing. The FDA did nothing of the kind: in fact, the agency granted “full approval” of BNT162b2, under the name COMIRNATY. Please see Page 7 and Page 8 of this report, below, which shows the whole-body biodistribution of BNT162b2:
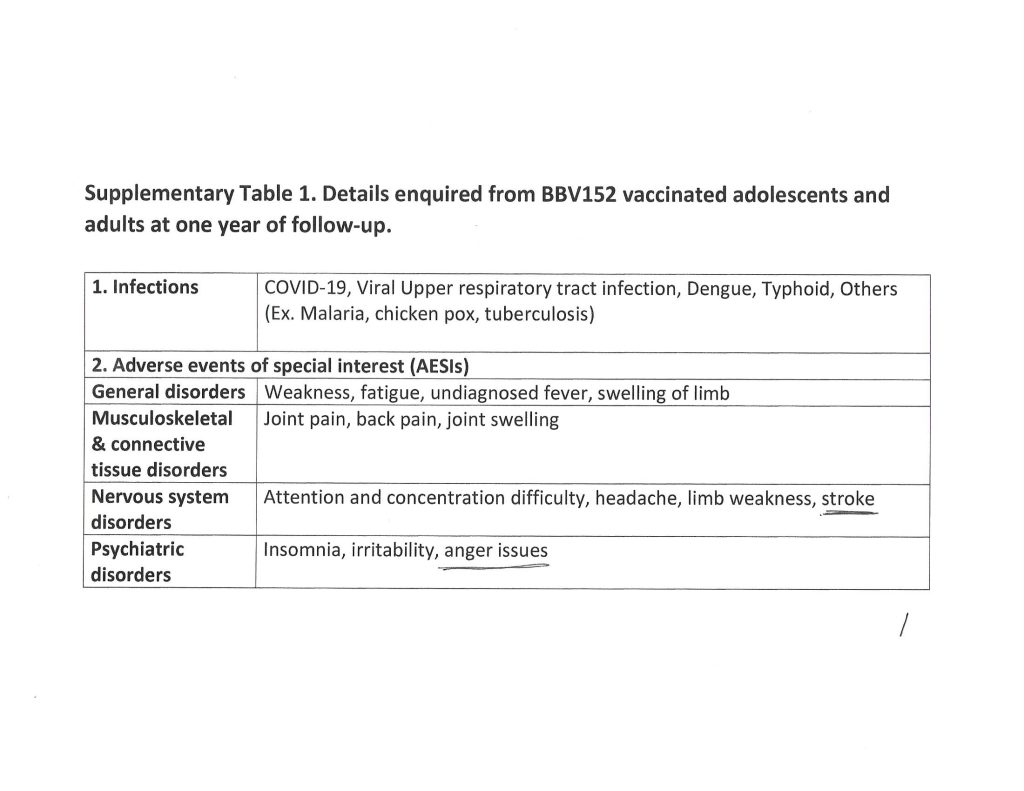
www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports, FDA time-stamped 30 April 2021. This report, given by Pfizer-BioNTech to the agency, contains an Appendix 1. List of Adverse Events of Special Interest at the end of the report. The Appendix 1. lists over 1,200 different types of adverse events medical conditions and illnesses, including death, resulting in persons who took BNT162b2 between 11 December 2020 (the date on which this “vaccine” was granted the initial EUA by the FDA for use in the United States) and 28 February 2021. The FDA knew about this on 30 April 2021. This report should have been another signal for the agency to suspend all use of BNT162b2 pending further investigation and testing, but the FDA did nothing to stop the continuing rollout of this injectable.
Scientific papers and/or articles:
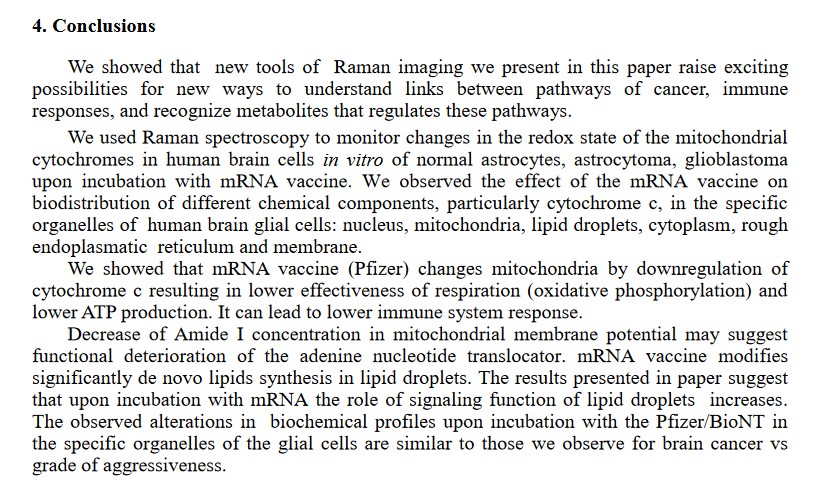
The Pfizer-BioNTech modRNA COVID-19 “vaccines” cross the Blood-Brain Barrierand negatively affect the cells of the “vaccinated” person’s brain. Below is section 4. Conclusions of the paper by H. Abramczyk, et al. (https://doi.org/10.1101/2022.03.02.482639, “Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System: human brain normal glial and glioma cells by Raman imaging”, 2022):
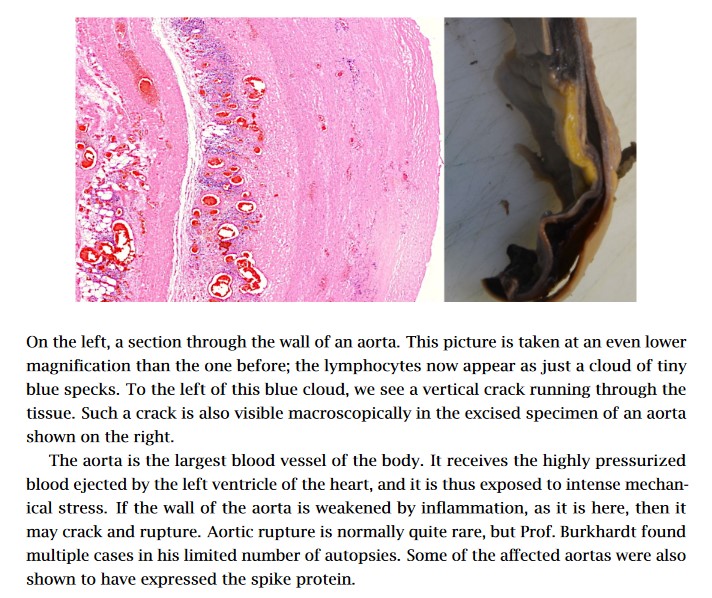
The COVID-19 “vaccines”damage the lungs, the cardiovascular system, and the heart of the personwho takes these “vaccines.” Please see the slides in this 2022 article: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, by Michael Palmer, MD, and Sucharit Bhakdi, MD. Below, for example, is Slide 10 from the article, showing lymphocytes lining the aorta prior to aortic rupture in a COVID-19 “vaccinated” person (from the autopsy):
ThePfizer-BioNTech modRNA COVID-19 “vaccines” change the DNA of the person who takes these injectables. This is the “Markus Alden, et al” 2022 paper (https://doi.org/10.3390/cimb44030073, “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Markus Alden, et al., February 2022.) The DNA that is reverse transcribed is the LINE-1 of the human liver cell line Huh7.
The Pfizer-BioNTech modRNA COVID-19 “vaccines” replace the RNA in Uridine, an important component produced by the liver, in persons who take these injectables. This is done by the mechanism of the N-1 Methylpseudouridine that is added to these “vaccines.” (https://pubmed.ncbi.nlm.nih.gov/32090264, “N1-Methylpseudouridine substitution enhances the performance of synthetic mRNA switches in cells”, Callum JC Parr, et al., April 2020.) Uridine helps to regulate mood, among other functions. In addition to the Parr, et al., paper above, there is also this, regarding negative neurological effects induced by the COVID-19 “vaccines”: www.theqtree.com/2024/10/18/health-friday-10-18-2024-special-edition-neurological-effects-of-the-covid-19-vaccines-physical-and-psychological/.
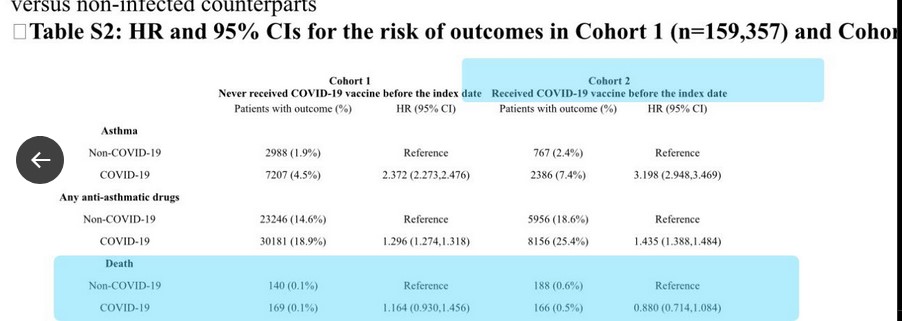
The paper referred to: https://doi.org/10.1007/s15010-024-02329-3. “The association between COVID-19 vaccine/infection and new-onset asthma in children–based on the global TriNetX database”, Chia-Chi Lung, et al., (June 2024.) This study is actually a “two-fer”: First, the COVID-19 “vaccines” induce new-onset asthma in children; and, second, children are at risk of dying from the COVID-19 “vaccines.”
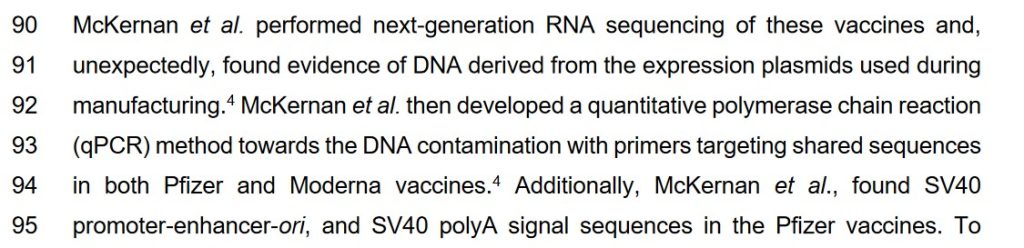
There are DNA “fragments” in the COVID-19 “vaccines”; and, there is a piece from the gene code of the SV40 cancer promoter from the African Green Monkey in the Pfizer-BioNTech modRNA COVID-19 “vaccines.“ The “McKernan, et al. paper” describes both of these negative effects. Below is a screenshot of a portion of the Introduction of this paper:
The “McKernan, et al.” paper: www.researchgate.net/publication/374870815, “DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events.”, Kevin McKernan, David Jeremiah Speicher, et al. (2023.)
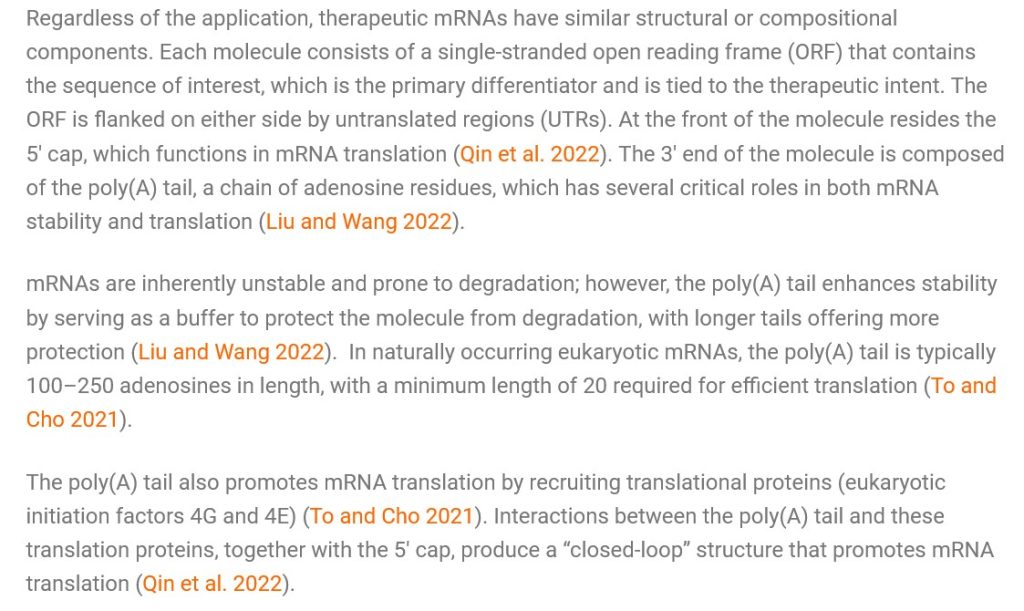
**** The “placement” of the SV40 cancer promoter gene piece in the polyA tail of the modRNA COVID-19 “vaccines”, in Yours Truly’s opinion, was deliberate. The following quotation is from an article by Marwan Alsarraj in August 2023: “In mRNA therapeutics, the poly(A) tail drives the efficacy of the mRNA molecules…” The article: www.bioradiations.com/polya-tails-in-mrna-based-therapeutics-823/, “Poly(A) Tails: A Critical Quality Attribute in mRNA-based Therapeutics”, 8 August 2023. Below is a screenshot from this article:
**** In Yours Truly’s opinion, the “closed loop” produced by the interactions of the poly(A) tail and the “translation proteins” means that the changes that the COVID-19 “vaccines” make to the DNA (via the SV40 cancer promoter gene piece in these “vaccines”) and to the RNA (via the N-1 Methylpseudouridine in these “vaccines”) of COVID-19 “vaccinated” persons can likely be permanent.
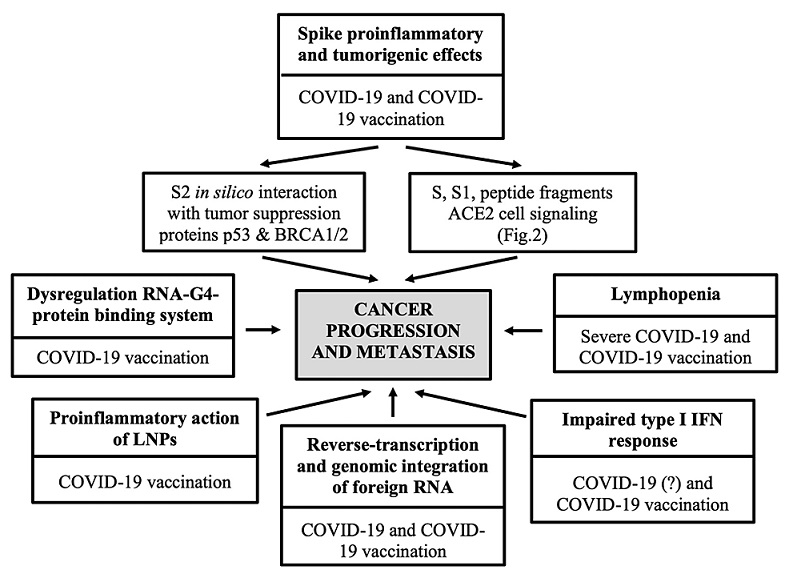
The COVID-19 “vaccines” can induce cancer, including what is called “turbo-cancer” in “vaccinated” persons; they can also induce “re-establishment” of previously under control or even previously cured cancers in “vaccinated” persons. The “vaccines” do this, among other ways, via the mechanisms of the SV40 cancer promoter gene (see above); and, the damage the “vaccines” do to the p53 cancer tumor suppressor protein in the body. Please see: www.theqtree.com/2023/11/29/the-covid-19-vaccines-pave-the-way-for-turbo-cancers-and-a-note-on-the-virus-itself/. Please also see: https://doi.org/10.7759/cureus.50703, “SARS-CoV-2 Vaccination and the Multi-Hit Hypothesis of Oncogenesis”, Raquel Valdes Angues and Yolanda Perea Bustos, (2023.) Below is a screenshot from the Review section of this paper:
In addition, please watch the video linked to this tweet (a presentation by British surgeon Dr. James Royle): https://x.com/SaiKate108/status/1851199741276602449. At 1:42 in the video, Dr. Royle describes what he sees in COVID-19 “vaccinated” patients who present with cancer: “…out of the blue, [the] liver [is] filled with large, round tumor masses.” Please refer up in today’s post at the Pfizer-BioNTech biodistribution amounts of BNT162b2 (Page 7 of the company’s Pharmacokinetics Tabulated Summary report): the accumulation of the dangerous lipid nanoparticles carrying the modRNA of this “vaccine” is 24.3mcg per gram (or mL) in the livers of the lab rats 48 hours after BNT162b2 was injected into them.Notice that the amount had steadily increased post-injection before it was measured at 48 hours post-injection. Also, note that BNT162b2 is the basis for all other modRNA COVID-19 “vaccines” manufactured by this company. **** In Yours Truly’s opinion, the liver was “targeted” as a major accumulation area for the lipid nanoparticles and for the other ingredients of BNT162b2, due to the number of body mechanisms and functions it regulates or assists in regulating. Please the Introduction, below, of the NIH StatPearls book, Physiology, Liver, by Arjun Kalra, et al. (StatPearls Publishing, January 2024):
COVID-19 virus and COVID-19 “vaccine” detox / mitigation protocols:https://covid19criticalcare.com/ (FLCCC Alliance); https://americasfrontlinedoctors.org/ (AFLDS); www.mercola.com/ (Dr. Joseph Mercola, MD; must sign up to access); www.americaoutloud.shop (Dr. Peter McCullough’s Wellness Company site.) Note: this is not an exhaustive list, and does not include herbal medicine, natural medicine, or other allopathic / osteopathic / homeopathic medicine sites.
Yours Truly has been researching, reading, and writing about the COVID-19 virus and the COVID-19 “vaccines” since March 2020. What readers find in the Health Friday posts are opinions and hypotheses based on this research and reading: it is not medical advice.
The uncovering of the truth about the dangerous, deadly COVID-19 “vaccines” is an ongoing, evolving issue. It is Yours Truly’s considered opinion that, with some exceptions, any person who has taken any COVID-19 “vaccine” since 11 December 2020 is at risk for adverse events, including COVID-19 “vaccine”-induced illness, injury, disability, or even death from these injectables. The COVID-19 “vaccines” have proven to not be “safe and effective.” Those who developed these injectables, knowing (or even suspecting) that they were not, and are not, “safe and effective”; and those who “mandated” their use, who coerced people into getting them, and who continue to push them, must be held accountable.
The above word-cloud image about memory loss is courtesy of Google Images.
This post is part of Health Friday, a series devoted to Big Pharma, vaccines, general health, and associated topics. Today’s offering, a Special Edition, is in honor of Yours Truly’s “fully vaccinated and boosted” brother, who was just diagnosed with “sudden-onset dementia.” Yours Truly will make it clear that one is not a medical doctor; one is not treating my brother; and, this post is a “narrative primer” on negative neurological effects from the COVID-19 “vaccines”, the Pfizer-BioNTech COMIRNATY (BNT162b2) modRNA COVID-19 “vaccine” in particular.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and, certain extra items that readers should be familiar with. They are all linked here.
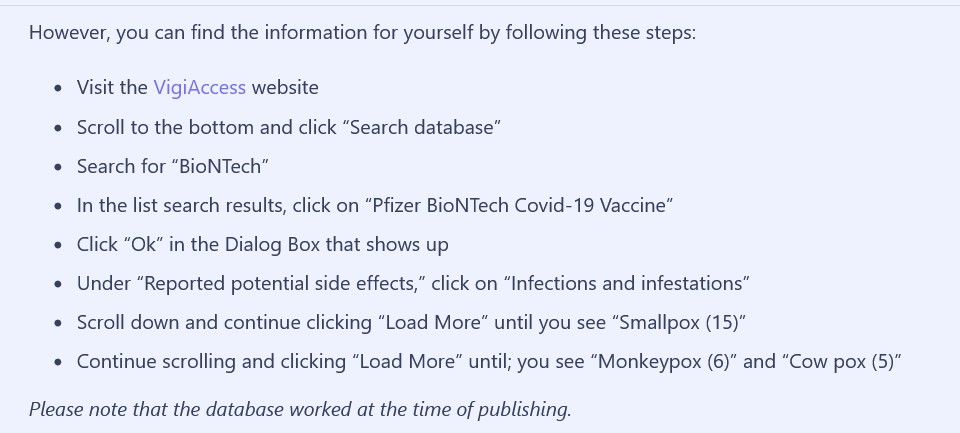
The World Health Organization (WHO) has a website, www.vigiaccess.org/, that lists “side effects” reported in persons who took COVID-19 “vaccines.” The Mole article describes how the VigiAccess search was performed to find “Monkeypox” as a “side effect” of the Pfizer-BioNTech COVID-19 “vaccine”, BNT162b2. A screenshot of the search protocol is below:
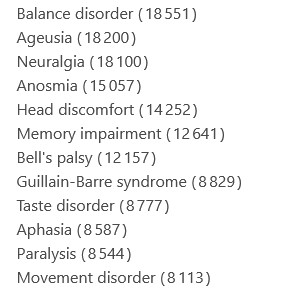
Yours Truly performed a VigiAccess search for reported memory problems (dementia is considered to be a form of “memory impairment.”) This is what I did:
Clicked on “Pfizer BioNTech COVID-19 Vaccine” on the list that came up
Clicked “OK” on the “Dialog” box
Under “Reported potential side effects”, I clicked on “Nervous system disorders” — and found a long list. A screenshot of a portion of this list shows “Memory impairment”:
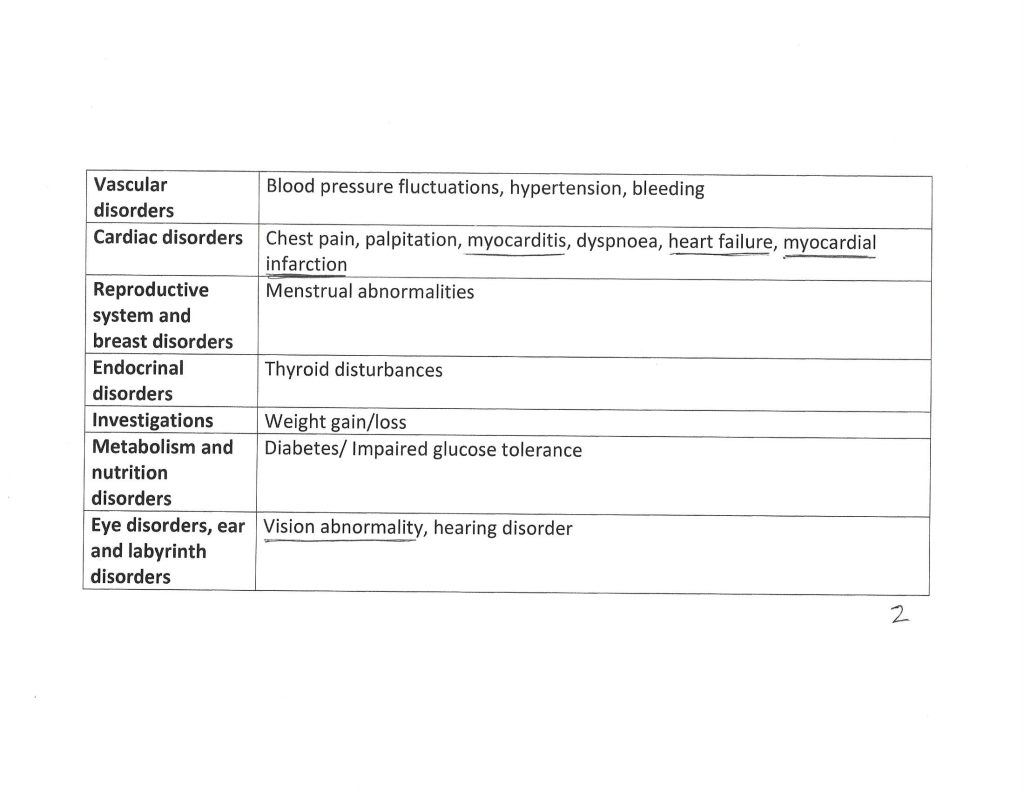
These are only the reported cases of conditions that are considered to be “side effects” of BNT162b2. It can be argued that there are many multiples more “side effects” cases from BNT162b2 that are not reported for some reason. Yours Truly also performed searches on the VigiAccess list under “Psychiatric disorders”, and under “Metabolism and nutrition disorders”, as certain other details were given to one in phone conversations related to the situation which raised interest.
The balance of today’s post will be presented in a “quasi-scientific paper” form. With the exceptions of some in-line references, scientific paper, blog and/or article citations will be numbered in the text with [“number”], and listed at the end of the post. Hypotheses and opinions of Yours Truly (H/O) will be delineated by Bold text with Italics. A General Summary will be included at the end of the post.
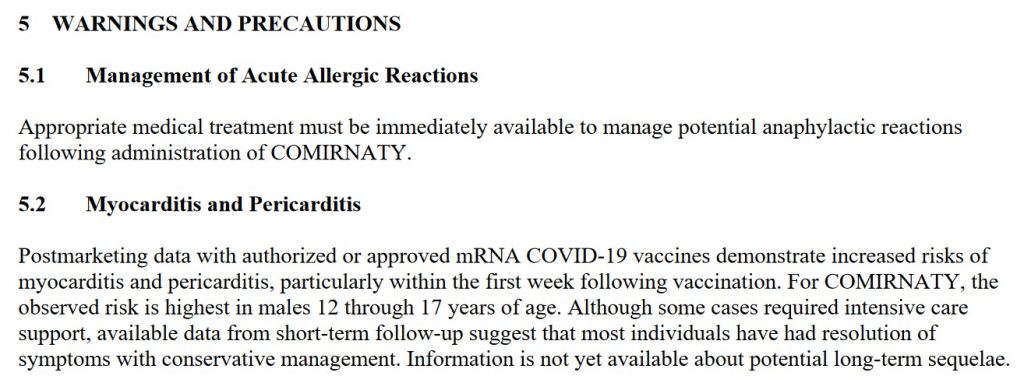
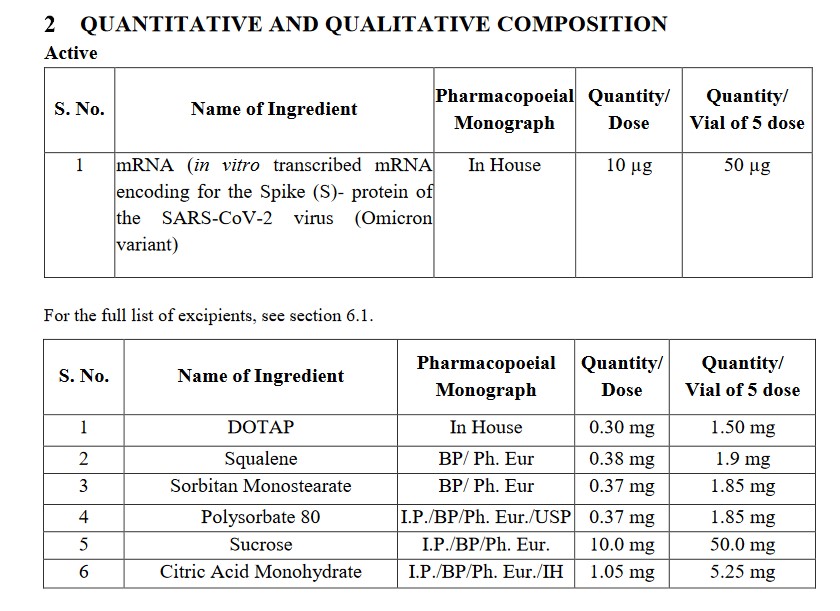
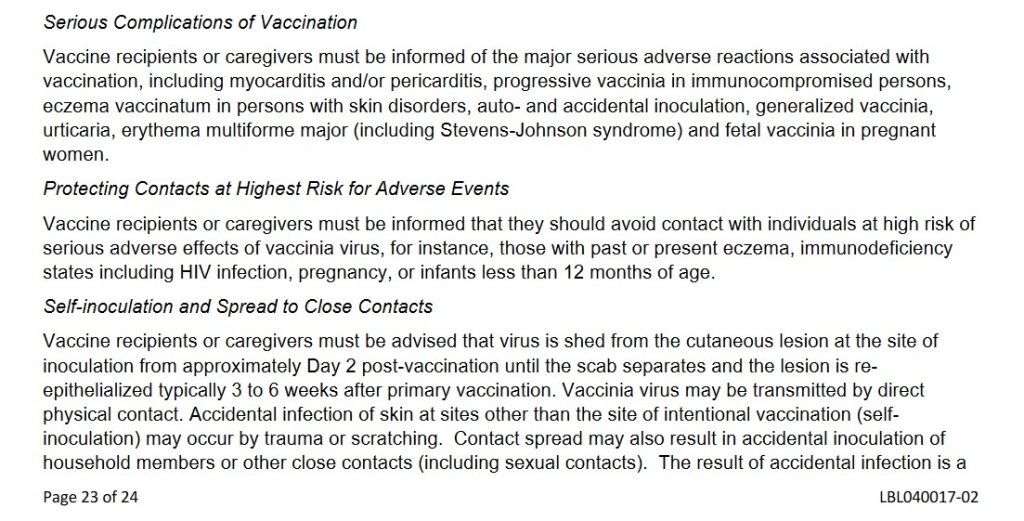
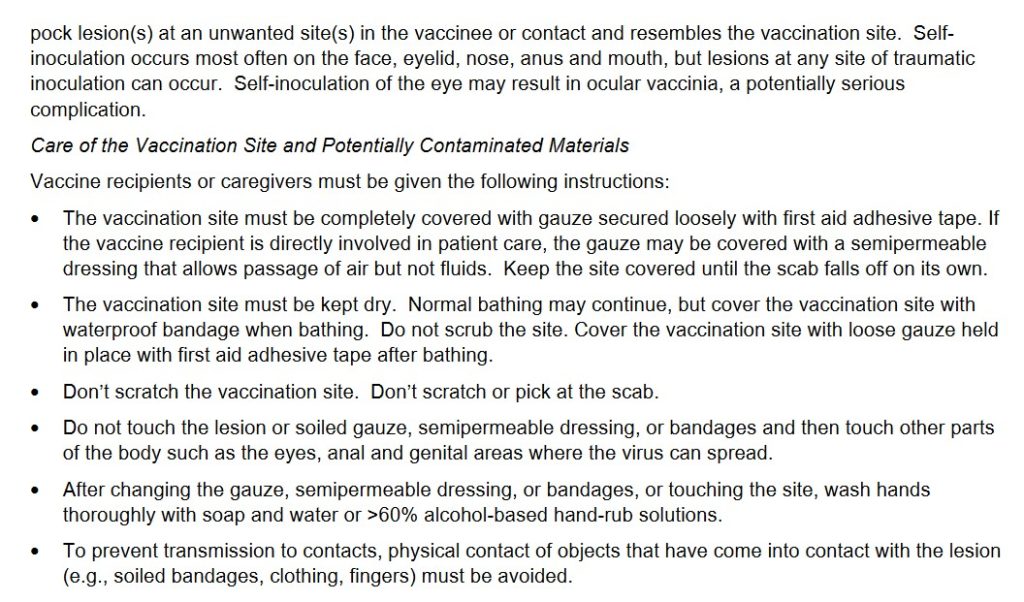
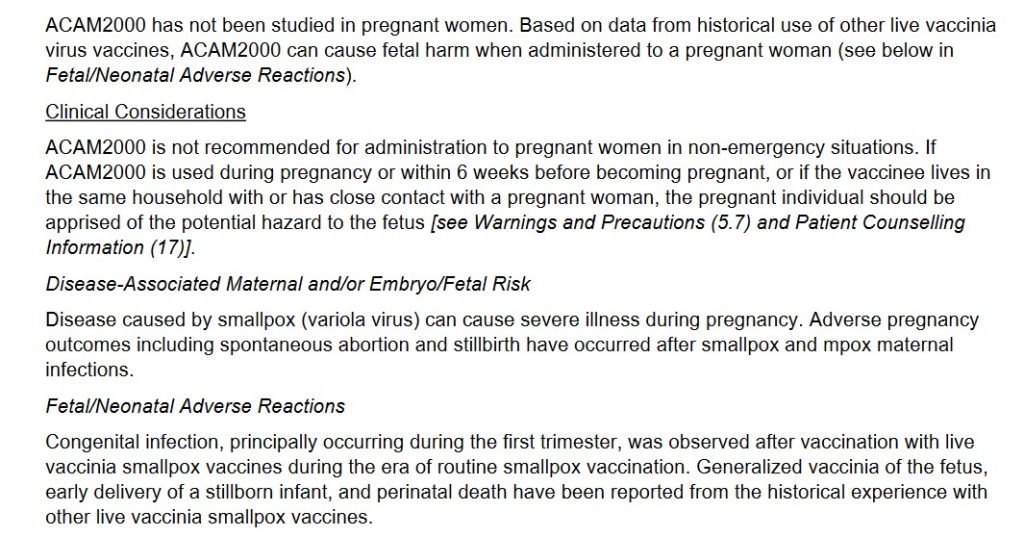
First: A Short Narrative Summary of What Occurs When a Person is Injected with the Pfizer-BioNTech modRNA “Vaccine” COMIRNATY: The “vaccine” here is the 2024-2025 Formula COMIRNATY COVID-19 “vaccine” (which, by the way, contains elements of BNT162b2, the original Pfizer-BioNTech modRNA COVID-19 “vaccine.”) Each “vaccine” dose is either supplied in a single-dose vial, with the dose to be administered withdrawn for injection; or, is in a pre-filled syringe ready for administration. (H/O)Upon “vaccination”, the person’s body immediately sends an “enemy detected” signal to the brain. The person’s body may react from fainting to chills to nausea, among other physical responses: see Sections 5.1 and 5.2 of the COMIRNATY 2024-2025 Fact Sheet, below [1]:
The lipid nanoparticles in the “vaccine” quickly begin to spread the contents of the injection throughout the “vaccinated” person’s body. This process is called biodistribution. Images of page 7 and page 8 of the January 2021 Pfizer-BioNTech Pharmacokinetics Tabulated Summary of the company’s modRNA COVID-19 “vaccine”, BNT162b2, are below [2]. Yours Truly will again emphasize that BNT162b2 is the basis for all of the Pfizer-BioNTech modRNA COVID-19 “vaccines”, including the COMIRNATY 2024-2025 Formula.
Note the accumulations in the Brain, the Liver, and the Large Intestine.
Note the accumulations in the Pituitary Gland, the Thymus Gland, and the Small Intestine. The intestines produce 90% of the body’s Serotonin. Serotonin is a neurotransmitter that is involved in the emotional / psychological / cognitive processes of the brain (per Wikipedia.)
Why is there accumulation of BNT162b2 in the Pituitary Gland? This small organ, called the “master gland” of the body, produces or directs many important hormones. Together with the hypothalamus, the pituitary gland work together to serve as the “brain’s central command center to control vital bodily functions”, according to Yours Truly’s online search at the Cleveland Clinic. These functions include breathing, stress response, reproduction, blood pressure, and more. (H/O): BNT162b2 and/or COMIRNATY is a “vaccine” to supposedly “prevent” a COVID-19 virus infection, not to work like a sort of pituitary gland treatment vehicle.
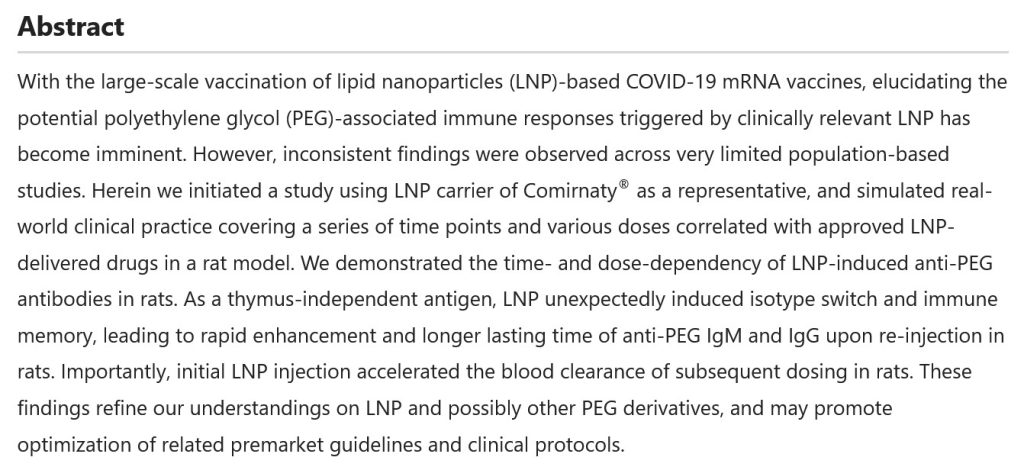
At least one of the lipid nanoparticles (LNPs) in COMIRNATY, ALC-0159 (but listed under its chemical component name), affects the thymus gland of the “vaccinated” person’s body. The thymus gland is “the primary lymphoid organ of the immune system” (per Wikipedia). The Abstract of a paper [3] that explains how ALC-0159 and other PEG-based LNPs work in the body is below:
While the lipid nanoparticles (LNPs) in COMIRNATY are spreading the ingredients of this “vaccine” throughout the “vaccinated” person’s body, the “vaccine” is using the PRRARSV “backdoor key” (an element which is only in the SARS-CoV-2 virus; and therefore, by extension, the modRNA COVID-19 “vaccines”) to facilitate entry of the “vaccine” ingredients into every cell in the “vaccinated” person’s body [4},[5]. (H/O)At the same time, the ingredients and mechanisms of COMIRNATY (BNT162b2) are beginning to work on inducing accelerated aging in the “vaccinated” person’s body, all the way down to the mitochondrial level [6]. Dao-Fu Dai, et al., wrote a paper in 2014 on how oxidative stress affects the mitochondria and the aging process [7].
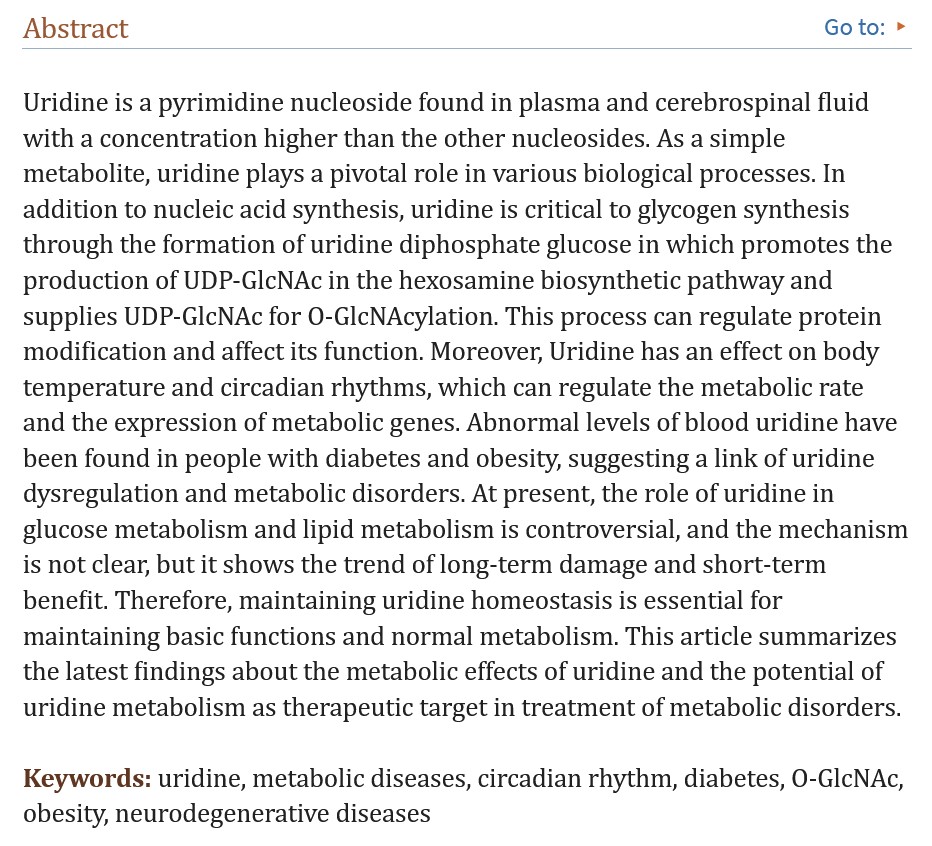
N1-Methylpseudouridine is present in all versions of COMIRNATY (BNT162b2), starting with the “original version” of this “vaccine”, BNT162b2. N1-Methylpseudouridine is a synthetic form of Uridine. Uridine is an important nucleoside for neurological processes, for the central nervous system, and other body processes. It is found only in RNA. Below is the Abstract of the Yueyuan Yang, et al., paper that the mechanism of Uridine in the body [8]:
The importance of Uridine cannot be minimized. This RNA element is produced in the Liver. Uridine helps to regulate mood; it also assists in the release of dopamine in the brain. Dopamine is a neurotransmitter that “affects emotions, behavior, and movement” (per WebMD.)
The purpose of N1-Methylpseudouridine in COMIRNATY is twofold: One, to “supersede” / “overwrite” the mechanisms of the natural Uridine in the “vaccinated” person’s body; and, Two, to enhance the mechanism of COMIRNATY in “mRNA switches in cells” of the “vaccinated” person’s body (Callum JC Parr, et al.) [9]. Below is the Abstract of this paper:
Yours Truly will blow the lid off the deliberate inclusion of N1-Methylpseudouridine in BNT162b2 (COMIRNATY.) This chemical was specifically added to the “vaccine” to replace the processes of natural Uridine; and, to evade the body’s natural immune system’s “enemy detection and elimination” elements and mechanisms. Below are screenshots from the Global Patent for BNT162b2, 28 October 2021 [10}:
Note that this appears to be a tacit admission that Gain-of-Function experiments were performed to create the modRNA in BNT162b2.
Note that this appears to be an admission that self-amplifying RNA (saRNA) can be used in Pfizer-BioNTech COVID-19 “vaccines.”
In addition to the “replacing” of uridine with N1-Methylspeudouridine in the body of the person “vaccinated” with COMIRNATY, the DNA of that person’s body is also being changed; please see Slide 14 of this article for a graphic of how the modRNA COVID-19 “vaccines” change the DNA.
Meanwhile, the newly-COMIRNATY-“vaccinated” person’s body, having “detected” an “enemy within the gates” (the “vaccine”), is sending out “all-out effort” signals to the body’s natural immune system to manufacture large amounts of cells to “fight off” the “detected enemy.” These natural immune system cells include CD4 cells, CD8 cells, IgG3 cells, and lymphocytes. However, the ingredients and mechanisms of the “vaccine” hamper, damage, and/literally destroy these natural immune system cells, via the “class switch” [11]; while, at the same time, inducing oxidative stress and cell death at the mitochondrial level all over within the “vaccinated” person’s body; and, also, inducing a state (of a still-unknown timeframe) of “faux SARS-CoV-2 infection” in the “vaccinated” person’s body [12]. A screenshot from this University of Maryland Medical System is below; note the last sentence:
The “rationale” behind the development and use of the modRNA COVID-19 “vaccines” is that the human body is not capable, of itself, to detect and “fight off” an infection by the SARS-CoV-2 virus; the body must have “assistance” in the form of the modRNA COVID-19 “vaccines” and their mechanisms. (H/O)However, it can be fairly argued that, given the multiple Adverse Events reports regarding COMIRNATY to VAERS and to VigiAccess, that this “vaccines” needs much more thorough R&D processes, testing on lab animals and then on humans, and extensive data collection and analyses, before this “rationale” can be fully proven. Pfizer-BioNTech rushed BNT162b2 into production, into securing the initial Emergency Use Authorization from the FDA in December 2020, and into this modRNA COVID-19 “vaccine” being used on the general public, before any of the above were fully undertaken. Pfizer-BioNTech and the FDA knew, back in April 2021, that BNT62b2 could, and did, cause hundreds of serious Adverse Events [13].
Second: Physical Neurological Effects of the COVID-19 “Vaccines”: These negative effects are somewhat “easier” to identify, as they can present with unmistakable symptoms. From the Appendix 1. List of Adverse Events of Special Interest in the 5.3.6 Cumulative Analysis document on BNT162b2 that was cited above, some examples: Page 2: Brain stem embolism; Brain stem mycoplasmal (encephalitis); Central nervous system lupus; Cerebellar artery thrombosis; Cerebral venous thrombosis. Page 3: Demyelination; Embolic stroke; Encephalitis autoimmune; Encephalitis post-immunisation. Page 4: Epilepsy; Epileptic psychosis; Grey matter heterotopia; Guillain-Barre syndrome. Page 5: IIIrd nerve paralysis; Immune-mediated encephalitis; IVth nerve paresis. Page 6: Meningitis; Multiple sclerosis; Neuritis; Neuromyelitis optica spectrum disorder; Neuropsychiatric lupus. Page 9: Thrombotic stroke; XIth nerve paralysis.
Bell’s Palsy is also reported after BNT162b2 “vaccination” [14].
In other words, COMIRNATY (and BNT162b2) damage multiple mechanisms and processes of the brain that result in physical medical conditions and/or illnesses. This “vaccine” damages the sheath coverings of the nerves, including of the spinal cord (Demyelination.) This “vaccine” causes brain inflammations of various types (Encephalitis.) This “vaccine” causes stroke. This “vaccine” causes nerve paralysis. And more. (H/O) This “vaccine” can also potentially aggravate existing physical neurological conditions and/or illnesses, including ones that were under control before the patient was COVID-19 vaccinated.”
There is also what may be considered a “hybrid” condition, since it involves both physical and psychological symptoms, and since can be brought on by either an infection by the COVID-19 virus itself, or by COVID-19 “vaccination”: Long COVID (also called Long Vax.) Long COVID appears to be an “overraction of the immune system” [15]. Physical symptoms include blood pressure swings, fatigue, and “brain fog.” Psychological symptoms include depression, anxiety, and even PTSD [16]. The FLCCC Alliance has articles on Long COVID / Long Vax.
Third: Psychological Effects of the COVID-19 “Vaccines”: The Blood-Brain Barrier (BBB) consists of “closely-spaced cells” that act as a protective barrier to keep many substances from reaching the brain. Below is the National Cancer Institute definition of the Blood-Brain Barrier [17]:
However, COMIRNATY (and the BNT162b2 before it) were specifically developed to cross the Blood-Brain Barrier and to damage glial cells of the brain, down to the mitochondrial level [18]. A screenshot of section 4. Conclusions of this paper is below:
Recall that COMIRNATY (and the BNT162b2 before it) contain the lipid nanoparticle, ALC-0159. This lipid nanoparticle, one of the four within the “vaccine”, assists in the spread of the “vaccine” to all areas of the “vaccinated” person’s body, including into the brain.
Does the crossing of the Blood-Brain Barrier by COMIRNATY (and the BNT162b2 before it) also affect the psychological processes of the brain? The answer is, Yes: and, most likely, via the use of the N1-Methylpseudouridine in this “vaccine.” Recall that natural uridine, (which is one of the nucleosides that make up the RNA of the body) is produced by the liver. Uridine influences the brain by assisting in regulating mood, behavior, movement, and more. N1-Methylpseudouridine was deliberately included in COMIRNATY (and the BNT162b2 before it) to replace the natural uridine in the “vaccinated” person’s body with a created “faux uridine” (see the screenshots from the BNT162b2 Global Patent document, above in the post.) This chemical was chosen because it was “more effective” than the other two chemicals listed in the Global Patent documentation screenshot above in the post.
The Roh, et al., paper of 28 May 2024 traced a potential association between COVID-19 “vaccination” and the onset of Alzheimer’s disease(AD)and also of Mild Cognitive Impairment(MCI)[19]. A screenshot from this paper is below:
While there is not yet a proven association between MCI and the onset of dementia, the potential is higher for onset of dementia in persons who have MCI [20].
At the same time, there is documented proof that COVID-19 “vaccination” can cause psychosis. Examples of papers published on this topic are: the “Aljeshi paper” [21]; the “Borodina, et al., paper” [22];, the “Lazarevna, et al.” paper [23]; the “Morz paper” [24]; and, the “Laxmi and Grover paper” (psychosis diagnosed months after COVID-19 “vaccination”[25].
Yours Truly will again emphasize that one is not a medical doctor; nor am I treating my brother. (H/O) However, I believe there is sufficient evidence to at least consider the possibility that COMIRNATY (BNT162b2) modRNA COVID-19 “vaccinated” persons are at risk of numerous negative effects to the brain, both physical and psychological, induced by this “vaccine”; AND, since it is unknown exactly how long the elements and mechanisms of COMIRNATY (BNT162b2) work in the “vaccinated” person’s body, the possibility also exists that the potential for any physical or psychological neurological negative effects from this “vaccine” may actually increase with additional injections of COMIRNATY (BNT162b2.)
General Summary: One: The Pfizer-BioNTech modRNA COVID-19 “vaccine” COMIRNATY (and, the company’s modRNA COVID-19 “vaccine” BNT162b2 before it) can induce multiple negative physical and psychological neurological side effects and/or Adverse Events conditions in persons who take these “vaccines.”Two: COMIRNATY (and BNT162b2) contain dangerous lipid nanoparticles, among them, ALC-0159, which quickly spread the ingredients of this “vaccine” throughout the “vaccinated” person’s body, including to the brain, the intestines, and the pituitary gland. Three: COMIRNATY (and BNT162b2) contain the lab-created chemical, N1-Methylpseudouridine, which replaces the natural Uridine in the “vaccinated” person’s RNA. Four: Pfizer-BioNTech included N1-Methylpseudouridine in the formulation COMIRNATY (and BNT162b2) and stated this in the company’s Global Patent documentation for this “vaccine.” Five: Pfizer-BioNTech tacitly admitted that Gain-of-Function experiments were performed in the development of BNT162b2, per the Global Patent documentation for this “vaccine.” Six: Pfizer-BioNTech admitted that self-amplifying RNA (saRNA) can be used in COVID-19 “vaccines”, per the Global Patent documentation for this “vaccine.”
In addition, the following may be of interest: One: A blog article by Alex Swanson, M.S., on uridine, 30 November 2020; and, Two: The FLCCC protocol on recovering from COVID-19 “vaccination.”
The list of citations follows. Peace, Good Energy, Respect: PAVACA
[1]www.fda.gov/media/151707/download, Full Prescribing Information for COMIRNATYR (COVID-19 Vaccine, mRNA) suspension for injection, for intramuscular use 2024-2025 Formula
[5]https://doi.org/10.1101/2022.09.27.509633, Nuclear translocation of spike mRNA and protein is a novel pathogenic feature of SARS-CoV-2, Sarah Sattar, et al., 27 Sept. 2022
[9]https://pubmed.ncbi.nlm.nih.gov/32090264/, N1-Methylpseudouridine substitution enhances the performance of synthetic mRNA switches in cells, Callum JC Parr, et al., 6 Apr. 2020
[14]https://doi.org/10.1016/S1473-3099(21)00451-5, Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: a case series and nested case-control study, Eric Yuk Fai Wan, PhD, et al. 16 Aug. 2021
[18]https://doi.org/10.1101/2022.03.02.482639, Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System: human brain normal glial and glioma cells by Raman imaging, H. Abramczyk, et al., 2 Mar. 2022
[19]https://doi.org/10.1093/qjmed/hcae103, A potential association between COVID-19 vaccination and development of alzheimer’s disease, Jee Hoon Roh, et al., 28 May 2024
[22]https://doi.org/10.24869/psyd.2022.377, First Episode of Psychosis Following the COVID-19 Vaccination – A Case Series, Tonka Borodina, et al., 18 May 2022
[24]https://doi.org/10.3390/vaccines10101651, A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19, Michael Morz, 1 Oct. 2022
The above blurred image of persons attending a conference is courtesy of Google Images and Vecteezy.
Today’s Health Friday offering is one a of a series devoted to Big Pharma, vaccines, general health, and associated topics. The discussion is not limited to what is presented in today’s post: it is an Open Thread.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and other items that readers should be familiar with. They are all linked here.
This post will be diving into some “interesting” rabbit-holes. Stay with Yours Truly — I believe they are all interconnected. There is a General Summary at the end of the post.
Note: the scientific paper referred to by Dr. Nevradakis is here: www.preprints.org/manuscript/202406.0060/v1, “Proximal Origin of Epidemic Highly Pathogenic Avian Influenza H5N1 Clade 2.3.4.4b and Spread by Migratory Waterfowl”, Nicolas Hulscher, John Leake, Peter McCullough, 3 June 2024; click on “Download PDF” to read or save the paper. The authors suspect Gain-of-Function to be in play. Below is the Abstract of the paper:
Since this paper is a preprint; and, that it may be a target for Retraction; Withdrawal; or, Reissue with “new conclusions” that would reflect pressure on the paper’s authors and/or the publisher, Yours Truly suggests that interested readers download or make a hard copy of the preprint version.
The International Bird Flu Summit was held in Fairfax, Virginia, on 2 – 4 October 2024. This is the website for the “summit”: https://birdflusummit.com/. Here is the Brochure for the “summit”: https://birdflusummit.com/Bird Flu Summit Brochure.pdf. Reading through these “summit” websites, one gets the distinct impression of a general tone that “a Bird Flu pandemic” is about to occur; and, that various “interventions”, “command and control” methods, and “monitoring and dismantling” of “misinformation” detected on social media platforms, etc., will be “necessary” as part of a “coordinated response.”
Taking a look at the Brochure for the “Bird Flu Summit”, here is a portion of one of the “overview” pages:
Seems innocuous enough. However, moving on in the Brochure, one finds this:
And, further along in the Brochure, there is this:
Military involvement? “Inter-agency Communication and Resource Allocation”? What is “Seamless Response”?
John Leake, who works with Dr. Peter McCullough, attended this “summit.” Here is his take: https://petermcculloughmd.substack.com/p/at-the-bird-flu-summit, 2 October 2024. Yours Truly agrees with his impression that the speakers at the “summit” were “middle-of-the-road, rather than barn-burning experts” (my phrase.) One also agrees with the impression that the “summit” was all about “a Bird Flu pandemic being just around the corner.” However, this is NOT to minimize the potential for something like a “bird flu epidemic / pandemic” occurring — either from a “natural cause”: or, by another “lab leak.” Here is another view on the situation: www.theburningplatform.com/2024/09/22/could-bird-flu-be-the-october-surprise/, by Clayton J. Baker, MD.
FLASH! — The McCullough Foundation just got a demand from one of the speakers at the “Bird Flu Summit”, Syra Madad, PhD, to delete a video that John Leake and Nicolas Hulscher (another McCullough Foundation member) made of a Question-and-Answer session between Mr. Leake and herself at the “summit.” Dr. Madad is the coordinator of the upcoming New York City “Bird Flu Response Conference.” Please see here: https://petermcculloughmd.substack.com/p/mccullough-foundation-receives-bird, “McCullough Foundation Receives Bird Flu Summit Censorship Demand”, 9 October 2024. Below is a portion of the article:
The transcript of the video follows in the article (the video was deleted.) Below is a portion of the transcript, followed by an assessment by Mr. Leake:
Turning to the entity that “presented” the event (Ginkgo Biosecurity), and the entity that “produced” the event (SyllabusX): this is where the “rabbit holes” emerge; and, something that Yours Truly will call the Big Pharma-Government-Medical Complex (BPGMCTM) comes into the situation. Yours Truly defines BPGMC as an “interwoven cooperation” among Big Pharma, Federal government agencies regarding development / funding / support (including the Department of Defense), institutional investors, private investors, and “Establishment Medicine” (CDC, FDA, AMA, etc.)
First, the “producer” of the “Bird Flu Summit”, SyllabusX. The company’s address and phone number: 1900 Campus Commons Dr., Suite 100, Reston, VA 20191; phone number: 703.466.0011. The company was founded in 2017. SyllabusX has its “fingers in many pies” regarding producing conferences and other events on student safety and security, on technology for educators, on health and biosecurity, and more (https://syllabusx.com/home-2; and, https://syllabusx.com/about-us.) (Note: it is not easy to find information online about this company, especially as regards financials. A couple of sources that Yours Truly found: https://pitchbook.com/profiles/company/520513-39#overview; and, www.zoominfo.com/c/syllabusx-inc/480230653.) It appears that SyllabusX is a “privately-held company.”
The Chief Research Officer of SyllabusX is Ahmed Al Faraj (www.linkedin.com/in/ahmed-al-faraj; Note: this link may not work, unless the reader first joins LinkedIn.) And here’s where the issue gets, IMO, interesting. It appears that Mr. Faraj graduated with a B.S. in Economics from the University of Kansas School of Business in 2006. His languages are listed as, “Native or bilingual proficiency” in Arabic.
Before starting SyllabusX, Mr. Faraj previously worked for a company called New-Fields Exhibitions, headquartered in Dubai (https://inf.ae/.) While at New-Fields Exhibitions, Mr. Faraj held positions as Program Manager, Education & Public Health Group; and. as Program Manager, Defense Business Group. Below are two screenshots from the type of work he performed while at New-Fields Exhibitions:
Mr. Faraj also previously worked for a company called AdvanFort. He was the Chief Operating Officer of this company. AdvanFort is owned by a person called Samir Farajallah. His son, the then-Chief Operating Officer, was called Ahmed Farahjallah. AdvanFort is “a US private maritime security company”, per Wikipedia. The company was founded in 2007, and its headquarters office is in Herndon, VA (www.advanfort.com/.) A vessel owned by AdvanFort was involved in an international maritime incident in 2014. One of the stories that covers this incident is here: www,bbc.com/news/uk-england-34095843, 7 September 2015, “AdvanFort accused of abandoning British men facing India trial.” As a result of this incident, AdvanFort withdrew from membership in SAMI (the Security Association for the Maritime Industry): https://gcaptain.com/sami-responds-accusations-from-advanfort/, 2 April 2014. (Interested readers may want to compare the photo of Ahmed Faraj on the SyllabusX LinkedIn site, to the photo of Samir Farajallah and Ahmed Farajallah that is in the BBC article linked above. In one’s opinion, the “Ahmed” in these photos is the same person, with a perhaps 10-year gap between the photos. One has no objection to people wishing to change their names — this is simply an interesting item.)
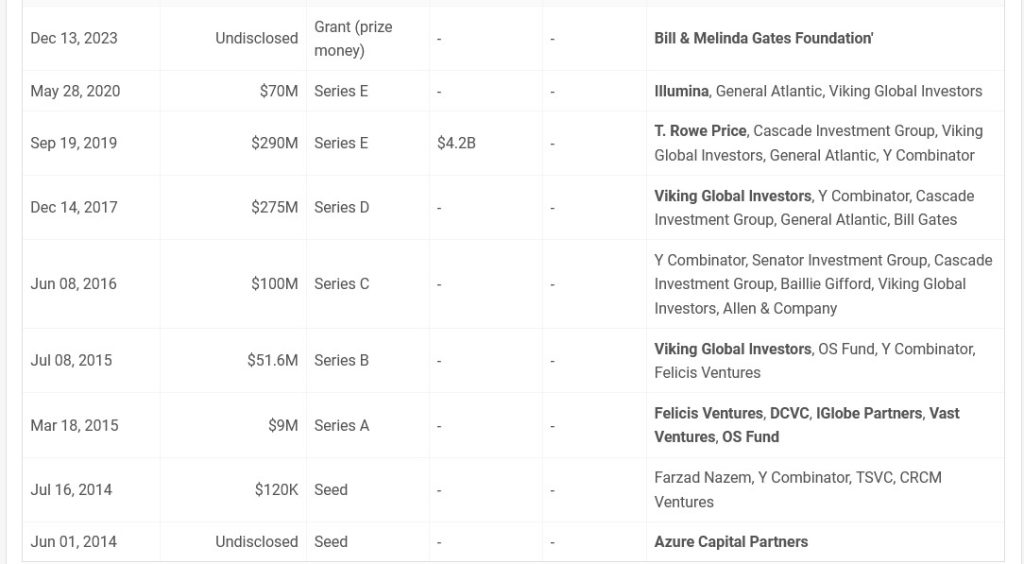
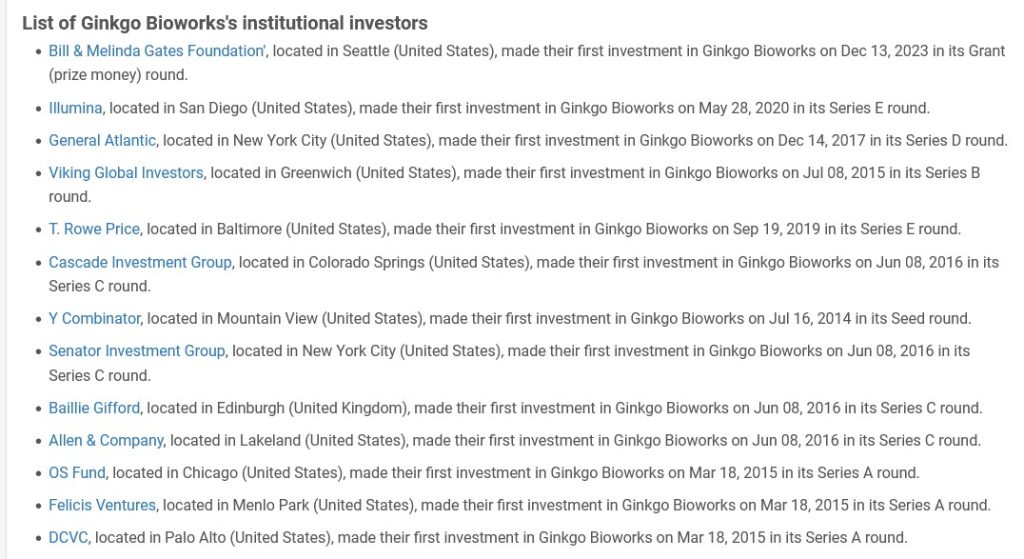
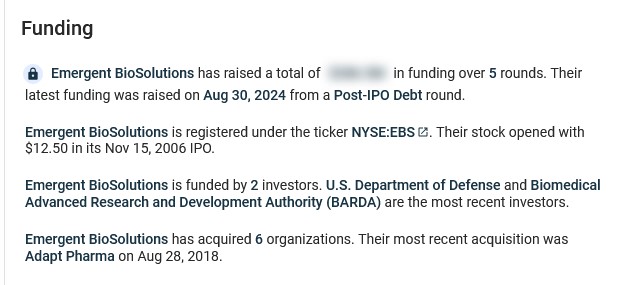
It appears that Ginkgo BioWorks has quite a bit of funding. Below are screenshots from https://tracxn.com/:
And, some institutional funders:
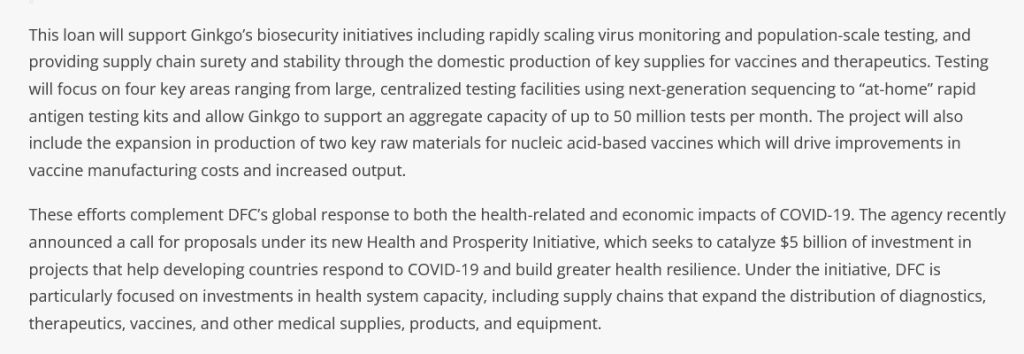
The United States government is also funding the biosecurity arm of Ginkgo BioWorks:www.dfc.gov/media/press-releases/dfc-approves-11-billion-loan-ginkgo-bioworks-expand-its-commercial-biosecurity, “DFC Approves $1.1 Billion Loan to Ginkgo BioWorks to Expand its Commercial Biosecurity Business to Combat COVID-19 on a Global Scale”, 25 November 2020. DFC is the U.S. International Finance Development Corporation. Below is a screenshot from the article:
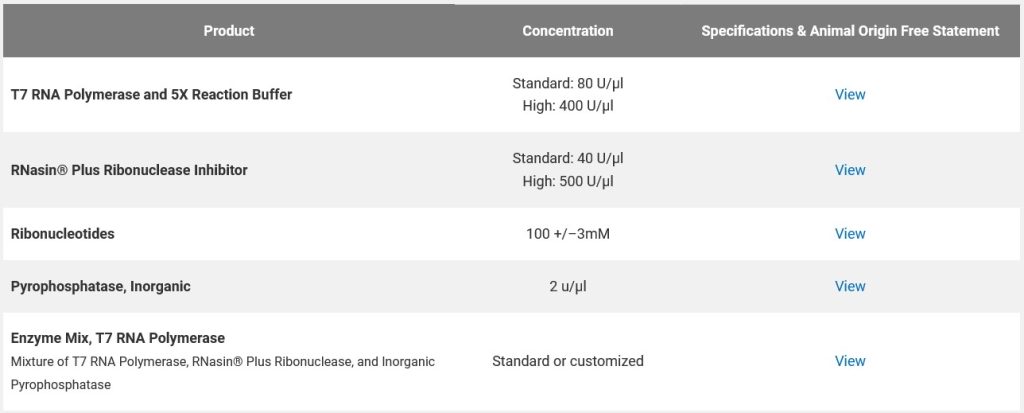
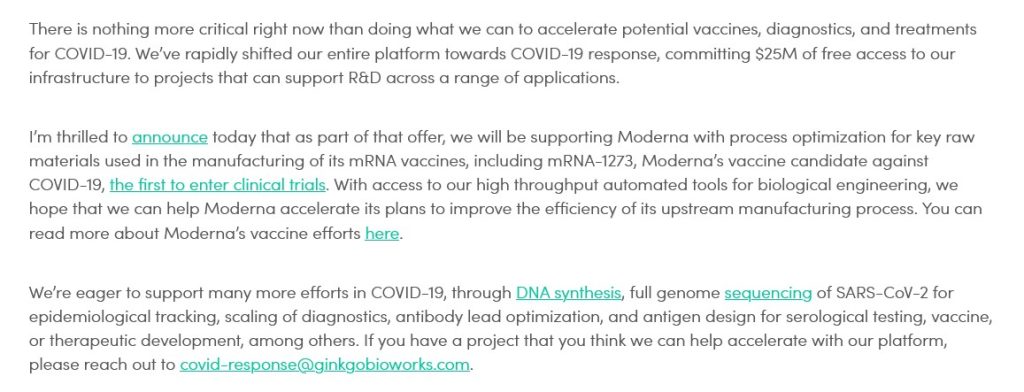
It would appear that Ginkgo BioWorks was involved in the “rapid deployment” of those PCR tests and antigen tests for COVID-19 at the start of the pandemic; and, also in the production of “two key raw materials for nucleic acid-based vaccines” (the modRNA COVID-19 “vaccines”.) Below is a blog post from April 2020 by Jason Kelly, another Ginkgo BioWorks co-founder, regarding the company’s partnership with Moderna in the production of the modRNA COVID-19 “vaccine”, mRNA-1273, along with other of that company’s mRNA “vaccines”:
Yours Truly has not, to date, found information as to the exact “raw materials” that Mr. Kelly is referring to.
Recall that the NIH/NIAID and Moderna co-developed mRNA-1273, co-own the patents of this modRNA COVID-19 “vaccine”, and share in the “royalty payments” for the sales and administration of this “vaccine” (and its “descendant clone” modRNA COVID-19 “vaccines.”)
Ginkgo BioWorks also “has its fingers in many pies”, including the bio-engineering of elements for gene therapy: www.ginkgobioworks.com/offerings/gene-therapy-services/. One such “service” is the bio-engineering of bacteria for treatment of diseases, such as cancer: www.ginkgobioworks.com/2023/01/09/engineering-bacteria-for-cancer-patient-treatment-with-prokarium/ (Prokarium is another “partner” with Ginkgo BioWorks.) The bacteria to be bio-engineered is a type of Salmonella bacteria, which will be used for “delivery of RNA payloads to treat cancer patients.” (Salmonella is “the most common form of food poisoning the in the U.S.”, according to the Cleveland Clinic. This brings up two questions: One, “Why is a bacteria related to food poisoning going to be used to treat cancer patients?”; and, Two, “How is this Salmonella bacteria going to be bio-engineered — is it going to be “sanitized” to be a beneficial element?”)
In Yours Truly’s opinion, Ginkgo BioWorks is a company to keep “on the radar.” It is acquiring other “partner companies” at a rapid rate. It is expanding its “services” into the gene-therapy sector. It is a “partner” with Moderna (and, therefore, by extension the NIH / NIAID.) In general, one has no objection to a company wishing to increase its profit margin and/or the number of its partner companies; at issue here are the following factors: the bio-engineering of DNA; the use of “automated tools” for engineering / manufacturing “raw materials” for gene-therapy treatments and/or “vaccines”; and the tie-in with the federal government.
General Summary: One: The International Bird Flu Summit was held in Fairfax, Virginia, earlier this month. The general tone of the “summit” was that a “bird flu epidemic / pandemic outbreak” is likely to occur, and soon. Two: The “summit” covered many topics related to epidemic / pandemic response, “command and control” methods, and how “seamlessly” federal, state and local governments and the military can “work together” in the response. Three: the “producer” of the “summit” was SyllabusX, a company that manages events ranging from student security to biosecurity to health education. SyllabusX is based in Virginia. Its Chief Research Officer is Ahmed Al-Faraj, who had previously (apparently) worked for his father’s company, AdvanFort, and (actually) for several other companies. Four: The “presenter” of the “summit” was Ginkgo Biosecurity (Ginkgo BioWorks), a company that offers “services” ranging from commercial biosecurity to bio-engineering to gene therapy research. This company, based in Massachusetts, has “deep funding” from many sources, including from the U.S. government. It has multiple “partners” in R&D, including Moderna. Ginko BioWorks was founded by students and scientists from MIT, including Tom Knight, the “godfather” of “DNA hacking” and of “synthetic biology.” Five: It appears that Ginkgo BioWorks, and, possibly, SyllabusX, are part of what may be called the Big Pharma-Government-Medical Complex (BPGMCTM), the “reach” of which runs far and wide.
Yours Truly will again emphasize the importance of having, and maintaining, the highest degree of health possible of the body’s natural immune system.
The above image of lab equipment is courtesy of Google Images and Public Domain Pictures.
Today’s offering for Health Friday concerns what is called self-amplifying RNA (saRNA.) As the presentation includes discussion of saRNA COVID-19 “vaccines”, this post is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
Readers already know about the Important Wolf Moon Notifications, the importance of Civil Discussion, the Rules of our late, good Wheatie, and the caveats regarding Health Friday posts by Yours Truly. Links to these items can be found here. NOTE: Since this post is detailed and there are multiple areas to cover, Yours Truly has added Summaries of certain sections, and a General Summary at the end.
Before one begins: It is well known that the modRNA and the viral vector COVID-19 “vaccines” currently in use have been, and are, a disaster on multiple fronts. Not only do they induce literally thousands of negative medical and psychological effects in the bodies of those who took them and who take them now; these “vaccines” also cause death. The numbers of COVID-19 “vaccinated” persons presenting with COVID-19 “vaccine”-induced illnesses, injuries, disabilities, or “died suddenly and unexpectedly” are increasing by the month. Nobody knows exactly how long, or in what amount, the elements and mechanisms of the COVID-19 “vaccines” work in the “vaccinated” person’s body: what IS known, is that whatever “protection” is conferred by these “vaccines” is short-lived, while, at the same time, the “vaccine” mechanisms linger on in the body for an indeterminate period of time. Yours Truly has written extensively for this board regarding this situation. For further information, please see websites such as these: https://kirschsubstack.com/ (Steve Kirsch); https://petermcculloughmd.substack.com/ (Peter McCullough, MD); and, https://phinancetechnologies.com/HumanityProjects/Projects.htm#Nav_ExcessDeaths (Ed Dowd, statistician.)
At the same time, the development of new types of COVID-19 “vaccines”, as well as new types of “vaccine delivery” (intranasal, oral, and aerosol, for examples) goes on apace. One of the “newest” types of COVID-19 “vaccines” uses what is called self-amplifying RNA, or saRNA.
The concept of saRNA is the use of a small amount of RNA (or mRNA) in an injectable. Once introduced into the body of the patient, the saRNA theoretically goes to work, “re-creating itself.” (Think RNA or mRNA being turned into a “Xerox copier” inside the “vaccinated” person’s body.) The “goal” of saRNA is for the agent to “re-create itself” inside the “vaccinated” person’s body for a certain amount of time and in some amount. The patient’s body is “instructed” by the saRNA to “recognize” and produce antibodies against certain “enemies”, such as viruses. The theory is that a smaller amount of saRNA initially introduced into the body, followed by the “Xerox copier effect”, then followed by “instructing” the body to “recognize” and fight off certain “enemies”, will make saRNA a “more effective use” of mRNA in injectables.
Basically,saRNA COVID-19 “vaccines” turn the “vaccinated” person’s body into a “Xerox copier” (which, apparently, the “vaccinated” person’s body CANNOT stop, slow down, or mitigate) for the ingredients (and, by extension, the mechanisms) of the saRNA “vaccine.” Today’s post is a primer about saRNA COVID-19 “vaccines.”
****** Summary: In other words, saRNA injectables **may**, at some point down the road, have **some** benefits. In the meantime — NONE of these types of injectables (GEMCOVAC, Kostaive) have been SUFFICIENTLY AND THOROUGHLY INVESTIGATED AND TESTED FOR USE ON HUMANS. But they are being approved ANYWAY, and are being injected into the bodies of unsuspecting persons who buy into the “Look, this shot has less mRNA than the ones you took before, and it’ll work better!” hype.
****** Look closely at the above graphic. It appears that the basic schema of saRNA is a “double-layer” of saRNA “replicons” that create a “subgenomic RNA.” This, in turn, creates the “Xerox copier” response which forces the body of the saRNA “vaccinated” person to endlessly produce immune system response— and for “at least” as long as 28 days after such “vaccination.”
Please see this paper regarding a discussion of saRNA “vaccine” design: https://doi.org/10.1016/j.tibtech.2023.05.007, “Rise of the RNA machines — self-amplification in RNA vaccine design”, Jerome D.G. Comes, et al., 14 June 2023. Below is the Abstract of this paper:
Note the language about “,…at least in theory” advantage of saRNA “vaccines.” Also note the last sentence — saRNA can “persist for a month.” In fact,nobody really knows how long saRNA elements will “persist” in the body of the person who takes this type of “vaccine” — NO long-term clinical trial or study has been performed using this technology.
On 28 November 2023, the Japanese Government approved the use of the saRNA COVID-19 “vaccine”, ARCT-154 (also called LUNAR-COVID-19 and Kostaive) for “active immunization” (translation: “prevention”) against COVID-19 for persons age 18 and older. Kostaive was developed by CSL / Arcturus (remember this company? Yours Truly took the lid off it here: www.theqtree.com/2024/08/02/the-hhs-gave-the-go-ahead-to-use-an-h5n1-vaccine-but-the-ama-just-issued-new-cpt-codes-for-an-h5n8-vaccine/.) This “vaccine” was to have supplies ready for administration by physicians or hospitals by mid-December 2023.
CSL / Arcturus, the Japanese government, and media outlets were quick to herald this “first-ever saRNA COVID-19 “vaccine.” Except — there already was an saRNA COVID-19 “vaccine” approved and in use, since 2022, in India: GEMCOVAC. Perhaps what CSL / Arcturus, the Japanese government, and media outlets should have mentioned the fact that Kostaive is modRNA-based from the J.1. Omicron SARS-CoV-2 variant (along with other “familiar” manufacturing methods, see below in today’s post); whereas GEMCOVAC based on an “ancestral variant” (in other words, the Beta variant) of the original Wuhan Hu1 SARS-CoV-2 virus.
Before Yours Truly presents information on Kostaive, she will first discuss GEMOCOVAC. This is in order to present further background information on saRNA technology as applied in COVID-19 “vaccines.” Stay with me — this is all germane to the situation:
Looking at GEMCOVAC, one can get the beginning of a picture of how saRNA COVID-19 “vaccines” work. The “latest version” of this “vaccine” is called GEMCOVAC-OM. Below is a portion of the SmPC pdf for this product (https://gemcovac.com; scroll down the page to GEMCOVAC-OM SmPC (pdf) and click “Download”):
The BA.1. Omicron variant of SARS-Co-V-2 is the basis for this “vaccine.” It is not strictly modRNA (however, recall that ALL of the “descendant variants” of the original Wuhan Hu1 SARS-CoV-2 virus contain elements of that original lab-created virus).
Of the excipients (in other words, the adjuvants): per Wikipedia, DOTAP (1,2-Dioleoyl-3-trimethylammonium propane) is a chemical used in fabric softeners, but also is used as a lipid nanoparticle in vaccines. Squalene: below is Page 1 of the FisherScientific MSDS Safety Data Sheet for this chemical (www.fishersci.com/):
Continuing: for polysorbate 80, again from Fisher Scientific, Page 1 of the MSDS Safety Data Sheet:
And, here is the Mechanism of Action for GEMCOVAC-OM, from the Package Insert (see the link above):
Note the language, “…which is reported to interact with host cells receptors (ACE-2.)” (Italics mine.) The developer and manufacturer (GENNOVA) of this “vaccine” can’t exactly quantify how the product works.
Yours Truly now turns to Kostaive, (ARCT-154) the saRNA COVID-19 “vaccine” that was approved by the Japanese government in November 2023.
Note the language in the above regarding “…the potential for extended duration of protection while using lower doses of mRNA compared to existing mRNA vaccines.” (Italics mine) Again, nobody knows exactly how long this “extended duration” period is; nobody knows exactly how much “Xerox copying” of the altered mRNA in Kostaive occurs during this period in the “vaccinated” person’s body; and, nobody knows exactly what effects this “Xerox copying” of the altered mRNA in Kostaive will have in the “vaccinated” person’s body. In other words, anyone who takes Kostaive, or any saRNA “vaccine”, in Yours Truly’s opinion, is being used a “human lab rat” — just as people were used / are still being used, as “human lab rats” for the modRNA COVID-19 “vaccines.”
And, here is the Report of the Deliberation Results (which contains the information about Kostaive that led to its approval) from the Japanese Ministry of Health, Labour, and Welfare: www.pmda.go.jp/files/000269813.pdf. This report is an interesting read. There are numerous “blacked-out” areas, reminding one of the blacked-out areas in certain publicly-released Pfizer-BioNTech reports that the company gave to the FDA regarding that company’s modRNA COVID-19 “vaccine” BNT162b2. HOWEVER, section 2.1 Active Substance for Kostaive states that this saRNA “vaccine” contains elements from the original Wuhan Hu1 SARS-CoV-2 virus, plus elements from the Omicron variant strain. More information on this is found on Page 4 of the document. Below is a portion of this page:
Looking at the above, starting with the D614G mutation, the Abstract from the Zhang, et al. paper on this (https://doi.org/10.1038/s41467-020-19808-4, “SARS-CoV-2 spike-protein D614G mutation increases virion spike density and infectivity”, Lizhou Zhang, et al., 26 November 2020. The paper was researched and published before any COVID-19 “vaccine” was authorized for use):
In other words, the D614G element causes the SARS-CoV-2 virus to be more infective.
Looking at V987P, part of the section Full-Length S Glycoprotein Vaccines from this paper: https://doi.org/10.3389/fimmu.2021/701501, “SARs-CoV-2 Vaccines Based on the Spike Glycoprotein and Implications of New Viral Variants”, Daniel Martinez-Flores, et al., 11 July 2021):
In other words, if V987P was “good enough” for Pfizer-BioNTech and for Moderna to use in their modRNA COVID-19 “vaccines”, it apparently was “good enough” to be used in Kostaive.
The K986P protein used in Kostaive: please see here: www.rcsb.org/structure/6zp1. This viral protein, along with V987P above, are BOTH on the Arg S1/S2 cleavage site on the SARS-CoV-2 virus genome. (FURIN CLEAVAGE SITE, anyone?)
The R682G, R683S, and R685S proteins used in Kostaive: please see here: https://doi.org/10.1038/s41467-022-32665-7, “Omicron SARS-CoV-2 mutations stabilize spike-up RBD conformation and lead to a non-RBM-binding monoclonal antibody escape”, Zhennan Zhao, et al., 24 August 2022. If appears that these proteins help to create a “one-RBD-up conformation.” Below is a portion of the Abstract of this paper:
In other words, these proteins increase the immune system attack from the Omicron SARS-CoV-2 variants by making Omicron “stick better” to the ACE2 receptor cells in the human body.
****** Summary: It appears, then, that Kostaive contains one protein from the original Wuhan Hu1 SARS-CoV-2 virus genome (D614G); two proteins from the “ancestral line” of the SARS-CoV-2 virus (K986P and V987P); and three proteins of the Omicron SARS-CoV-2 variant (R682G, R683S, and R685S.) See below in the post for more information on these items.
One more ingredient of Kostaive, mRNA-2105: This ingredient is derived from the Venezuelan Equine Encephalitis virus (VEEV.) Below is section 4.R.1. of the Deliberations Results document discussing this:
The question that immediately occurs regarding the above: How can Arcturus (the manufacturer of Kostaive) state that mRNA-2105 cannot be “incorporated into host cell DNA”? How is Arcturus absolutely sure that there is zero reverse transcription potential or ability in Kostaive? This is similar to the same statements from Pfizer-BioNTech about BNT162b2 “cannot change the DNA of the vaccinated individual” — which has been proven to be false (please see: here, Slide 14.)
****** Summary of the above: What Yours Truly is getting at here is that Kostaive appears to be the end-product of: ONE: a lab-created mixture of the dangerous D614G element from the original Wuhan Hu1 SARS-CoV-2 virus, plus, various elements of earlier SARS-CoV-2 mutations; TWO: NO long-term clinical trials, NO safety studies for Toxicity, use on pregnant women, etc.; THREE: the “Process 2”-type manufacturing method (“culturing” the lab-enhanced mRNA for the “vaccine” in a “bath” of E. coli); FOUR: using lipid nanoparticles, one of which (ATX-126) has never been used before in an injectable); FIVE: what appears to be a “pro-forma” Deliberation Results document on Kostaive that raises more questions than it answers; and, SIX: approval by the Japanese government for use on humans without a thorough investigation of the above. Related to point SIX: below is the list of Approval Conditions that were imposed along the approval of Kostaive for use in Japan, from the Deliberations Results document:
By the way, these Approval Conditions read very much like the ones that the FDA imposed on Pfizer-BioNTech along with that agency’s EUA for BNT162b2.
Regarding Kostaive itself, more particulars:
The ingredients of Kostaive are listed in section 2.2 Vaccine Product of the report. A screenshot of this section is below:
Kostaive contains at least three separate types of LNPs (lipid nanoparticles): ATX-126; DSPC; and, PEG2000-DMG. Below is a portion of the MSDS Safety Data Sheet for ATX-126:
Section 2.2.3 of the Deliberation Results document for Kostaive discusses the manufacturing process for Kostaive. It appears that Kostaive ALSO “switched” from a “Process A” manufacturing method over to a “Process B” manufacturing method. (Recall that the Pfizer-BioNTech BNT162b2 was “switched” from its “Process 1” manufacturing method over to a “Process 2” manufacturing method):
One more item from the Deliberation Results document for Kostaive, again on the ATX-126 lipid nanoparticle used in this “vaccine.” It confirms that this “novel excipient” (adjuvant) has not been used before in a “vaccine.”
Yours Truly will again emphasize that other sections of the DeliberationResults document on Kostaive make it clear that NO studies were performed for numerous items, such as Toxicity, potential for impairment of reproduction, and so on. By the way, buried in the document is a “passing reference mention” that the “Process B” manufacturing method for this “vaccine” uses E. coli as the “culturing medium” for the “enhanced” mRNA in the product. (The “Process 2” manufacturing method for BNT162b2 and its “descendant” COVID-19 “vaccines” also uses E. coli.) It also appears that the use of Kostaive on pregnant women in clinical trials was “inconclusive”; this “vaccine” should be taken by pregnant women only if the situation so warrants.
Also: Kostaive is to be taken as a “primary series” of two separate injections, 28 days apart; with a “booster” taken about three months later. The question that arises is: If it is true that the saRNA in Kostaive is active, including installing numberless “Xerox copiers” of itself in the “vaccinated” person’s body for AT LEAST 28 days AFTER the initial injection, WHY is there a need for ANOTHER injection around Day 28? And a “booster” after that?
******BUT — AND THIS IS A HUGE BUT — TAKE ANOTHER LOOK AT SECTION 2.2.1 OF THE DELIBERATION RESULTS DOCUMENT FOR KOSTAIVE:
Look at the “active ingredient” item, “zapomeran.” What is zapomeran? It is a “drug” that contains the RNA of the Venezuelan Equine Encephalitis Virus (VEEV or VEE) in an saRNA form. It is ALSO manufactured by ARCTURUS (CSL.) It is unclear if it is being used in other types of COVID-19 “vaccines” other than Kostaive. Please see: https://synapse.patsnap.com/drug/510bcf7ef75649278b284a94663c69f6. Scroll down the page to R&D Status to see that zapomeran has already been approved in the EU; Norway; Iceland; and Liechtenstein; but in what final form it is used, is also unclear. NOTE 1: It has been impossible to find a complete list of ingredients for zapomeran. One would not be surprised to learn that the names Kostaive and zapomeran may, in some respects, be “interchangeable.” NOTE 2: It is not easy to find information on zapomeran. Yours Truly has encountered “504 Bad Gateway” error messages when going back to recheck a couple of the links to zapomeran in this post.
Looking further into VEEV (or VEE), there is this article: https://ceh.vetmed.ucdavis.edu/health-topics/venezuelan-equine-encephalitis-vee, by Amy Young, 28 August 2020. This virus can affect horses, donkeys, or zebras. VEEV is transmitted to these animals by infected mosquitos that bite them. It can cause severe disease or death by infecting the brain and the central nervous system. Humans who contract VEEV can also become severely ill and can also die from it. Another paper, discussing the RNA of VEEV (VEE),by Sarah E. Hickson and Jennifer L. Hyde, is here.
****** VERY IMPORTANT:The SARS-CoV-2 spike proteins in zapomeran are the same ones that are in Kostaive. These were discussed above in the post. Turning to the nsP proteins (non-structural proteins) in zapomeran (hyperlinks to papers are embedded), as these elements are also apparently contained in Kostaive:
****** SUMMARY:IT APPEARS, THEN, THAT KOSTAIVE CONTAINS ZAPOMERAN, WHICH INCLUDES THE VENEZUELAN EQUINE ENCEPHALITIS RNA; PLUS, SIX LAB-ENHANCED/LAB-ISOLATED GENOME CODES OF SARS-CoV-2; AND, FOUR NON-STRUCTURAL PROTEINS, ONE OF WHICH IS A ROTAVIRUS TOXIN. KOSTAIVE ALSO CONTAINS DANGEROUS LIPID NANOPARTICLES (SUCH AS ATX-126.) THESE ARE ALL PRESENT IN THIS saRNA COVID-19 “VACCINE” PRODUCT. RECALL THAT LIPID NANOPARTICLES WILL HELP TO SPREAD A “VACCINE” THROUGHOUT THE ‘VACCINATED” PERSON’S BODY, INCLUDING CROSSING THE BLOOD-BRAIN BARRIER.
Why on Earth is a COVID-19 “vaccine” that contains the RNA of an equine brain inflammation virus (a virus that comes from infected mosquitos that bite equine animals) being used on humans? A “vaccine” that is engineered to create an unknown number of “Xerox copiers” of the “vaccine” elements into the body of the “vaccinated” person? A “vaccine” that contains six apparently lab-enhanced/lab-isolated genome codes from the SARS-CoV-2 virus or its variants? What does an equine brain inflammation virus have in common with SARS-CoV-2? What if a person who has already taken, say, five or six injections of a modRNA COVID-19 “vaccine” decides to take Kostaive? Could an saRNA COVID-19 “vaccine” somehow “interact” with the modRNA COVID-19 “vaccine” elements already in that person’s body?
****** GENERAL SUMMARY: saRNA “vaccines” for COVID-19 are already being used (GEMCOVAC in India); and are being approved for use (Kostaive in Japan.) The technology for saRNA is not fully developed and not fully tested; the COVID-19 “vaccines” that use saRNA contain “lab-enhanced”/”lab-isolated” genome codes of the SARS-CoV-2 virus or its variants; saRNA COVID-19 “vaccines” contain lipid nanoparticles — and, in the case of Kostaive, an LNP (ATX-126) that has never been used before in an injectable; that no studies have been performed on saRNA COVID-19 “vaccines” regarding Toxicity, the effects on reproductive potential, and so on; and, that Kostaive contains the RNA of the Venezuelan Equine Encephalitis Virus. And yet, these products are being hailed as “the vaccines of the future.” And, the people taking them are again being used as “human lab rats.”
The above image from an old medical-scientific journal is from PeopleImages, via Google Images.
This post is part of Health Friday, a series of offerings related to Big Pharma, vaccines, general health, and associated topics. The discussion is not limited to what is presented today; it is an Open Thread. However, since this presentation is about a COVID-19 “vaccine”, the post is dedicated to the memory of Yours Truly’s cousin Bill, who died “suddenly and unexpectedly” in September 2023.
To begin, there are Important Wolf Moon Notifications, with a couple of extra items:
Free Speech is practiced here: “Use it or lose it.”
The following are alternate Q Tree sites for certain circumstances:
The U Tree is for “argue it out” interactions. There is a “Featured” article at this site for use as a “Rescue Thread.”
The “third site”, in case the above two are inaccessible.
Civil discussion is practiced here. The excellent and timely Rules of our late, good Wheatie prevail:
One: No food fights.
Two: No running with scissors.
Three: If you bring snacks, bring enough for everyone.
Please follow the added Guidelines from Wolf Moon. Please do not give the modern-day version of Cato the Elder the opportunity to show “enmity” to the board.
The extra items: What Yours Truly presents in this series, as in her other blog posts to this board, is not medical advice — the are opinions and hypotheses based on her over 4 1/2 years (and continuing) of reading about, researching out, and writing about “all things COVID”, Big Pharma, and other health topics. Readers are encouraged to consult a healthcare practitioner regarding health concerns or conditions.
The Health Friday post today concerns the impending Retraction of a peer-reviewed and published paper that details long-term COVID-19 “vaccine”-induced injuries in North India. The paper was submitted to Springer for review and publishing on 9 January 2024; it was accepted (it had passed the peer-review process); and it was published on 13 May 2024. Here is a free-access version (to read the entire paper on Springer, one has to either access through an institution, or to pay for a copy): www.qeios.com/read/JK7IBA/pdf, “Long-Term Safety Analysis of the BBV152 Coronavirus Vaccine in Adolescents and Adults: Findings from a 1-Year Prospective Study in North India”, Upinder Kaur, et al., 13 May 2024. The study was conducted at Banaras Hindu University in India. BBV152 is another name for the COVAXIN COVID-19 “vaccine”, developed by Bharat BIotech of India in cooperation with Indian Council on Medical Research (ICMR) – National Institute of Virology. ICMR receives “royalty payments” for each dose of COVAXIN that is administered, as does Bharat Biotech (Sound familiar? — as in, the co-development, co-ownership of patents, and sharing of “royalty payments” between the NIAID and Moderna for the modRNA COVID-19, mRNA-1273?)
The Kaur, et al., paper referenced above was published by Springer on 13 May 2024. Almost immediately, the attacks began on the paper, the authors, and the publisher — with articles like this one: https://timesofindia.indiatimes.com/india/1-in-3-covaxin-recipients-hit-by-adverse-events-study/articleshow/110187284.cms, “1 in 3 Covaxin recipients hit by adverse events: Study”, 17 May 2024. On 18 May 2024, the ICMR demanded that Springer retract the paper (Yours Truly: nothing like causing panic in a government agency when the truth is published about a “vaccine” that the agency is pushing as “safe and effective,” especially when that agency is also getting “royalty payments” for the use of the “vaccine”, is there?). But, the attack on Springer and the authors didn’t end there. In July 2024, Bharat Biotech filed a lawsuit against Springer and the authors (some of the authors are students), demanding retraction of the paper and the payment of damages to Bharat Biotech of $600,000 US dollars (50 million Indian rupees.) In addition, the lawsuit accused the paper’s authors of defamation against the company, included with a demand for separate damages to be paid to the company for defamation. Despite sworn statements from the authors that no defamation was intended or written into the paper; and, despite the fact that Nitin Joshi, the editor of the Springer journal (Drug Safety) in which the study appeared, was one of the reviewers who approved the study for publishing, it was Joshi who notified the authors on 28 August 2024 that he was going to have the paper retracted. He confirmed this decision in an email to the authors on 17 September. However, as the defamation lawsuit is now in court, the study is still available on the internet.
What is BBV152/COVAXIN? It is an “inactivated whole virion vaccine” (whole virus vaccine) for “active immunization” against COVID-19. It is not an mRNA-based/modRNA-based COVID-19 “vaccine”, although it does use an “ancestral wave strain” of the original Wuhan Hu1 SARS-CoV-2 virus (in other words, a strain from the Wuhan Hu1 virus that occurred before the Beta, Delta, or Omicron strains.) The Package Insert for COVAXIN is here: www.bharatbiotech.com/images/covaxin/covaxin-pack-insert.pdf. Below is an image from the Package Insert:
Per Wikipedia, 363,774,435 persons in India had been “vaccinated” with at least one dose of COVAXIN as of 4 March 2023.
However, the COVAXIN Package Insertdoes not actually describe how the “vaccine” works (the “Mechanism of Action.”) Yours Truly found something along the lines of the necessary information here: www.clinicaltrialsarena.com/projects/covaxin-bbv152-for-the-treatment-of-covid-19/?cf-view&cf-closed, “COVAXIN (BBV152) for the Treatment of Covid-19, India”, 28 June 2022. Below is a screenshot from this article:
But, COVAXIN has been hailed by the Indian government about being “the first indigenous COVID-19 vaccine in India” (www.bharatbiotech.com/covaxin.html.) Why is ViroVax involved? (More on this later in the post.) Back to the Package Insert for COVAXIN. Below is a screenshot of the ingredients used in this “vaccine”:
Looking further into the ingredients list, starting with the NIV-2020-770 strain of SARS-CoV-2: please refer to this paper: www.ncbi.nlm.nih.gov/pmc/articles/PMC7825810/, “Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: a double-blind, randomised Phase 1 trial”, Krishna Mohan Vadrevu, et al., May 2021. It appears that NIV-2020-770 (the “inactivated whole virion”) is part of the Asp614Gly variant chain of the SARS-CoV-2 virus. The Asp614Gly variant itself is apparently part of the “ancestral wave” of the original Wuhan Hu1 SARS-CoV-2 virus; and, it is “not as serious” as the Beta or the Delta waves of the virus. Please refer to this article: www.thelancet.com/pdfs/journals/langlo/PIIS2214-109X(22)00199-1.pdf, Vol.10, July 2022, a Comment “Decoding the next SARS-CoV-2 variant”, by Jeremy Nel and WD Francois Venter. Below is a screenshot of a portion from the Comment:
Thus, BBV152/COVAXIN cannot be considered to be one of the “most recent” types of COVID-19 “vaccines”, as it does not include any elements before the Beta, Delta, or Omicron variants.
The Aluminium Hydroxide Gel in the ingredients (it is an “excipient” [“adjuvant]”): this is also called “Algel-IMDG” and “Alhydroxiqium-II” — in other words, it is a hydrogel. It was invented by ViroVax LLC of Lawrence, Kansas, under the aegis of the EpscoR Idea Foundation (part of the National Science Foundation in the United States), and with funding by the NIAID. This is the ViroVax / United States government connection. Here is a screenshot from an article by the EpscoR Idea Foundation on this “success story” (www.epscorideafoundation.org/success-stories/kansas-adjuvant-developed-with-nih-funding-enhances-efficacy-of-indias-covid-19-vaccine):
Note that Alhydroxiqium-II targets the lymph nodes of the person who takes COVAXIN. So, while this excipient is not exactly a lipid nanoparticle (LNP), it, in Yours Truly’s opinion, basically functions like an LNP in targeting the lymph nodes for delivery of the “vaccine payload” of COVAXIN; and, by “stimulating” the “vaccinated” person’s natural immune system to go and “search” for invading pathogens. By the way, Aluminium Hydroxide Gel is not to be used in foods, drugs pesticides, or “biocidal” products — see the screenshot below, from the search on Fisher Scientific (ThermoFisher) about this chemical, Page 1:
HOWEVER, it appears that FisherScientific had a “change of heart” since December 2021 regarding the “Uses advised against” for Aluminium Hydroxide — below is their MSDS Safety Sheet as of February 2024, Page 1:
Here is another source for an MSDS Safety Sheet, this one specifically for Aluminium Hydroxide Gel:www.oxfordlabfinechem.com/msds/ALUMINIUMHYDROXIDEGEL.pdf. Please see section 3Hazards Identification; and section 11Toxicological Information Special Remarks on Other Toxic Effects on Humans. Below is part of the Special Remarks portion of section 11:
The TLR7/8 excipient (adjuvant) in COVAXIN: This one is used in immunotherapy, including in the treatment of HIV-1. Please see: https://doi.org/10.3389/fmicb.2023.1033448, “Novel TLR7/8 agonists promote activation of HIV-1 latent reservoirs and human T and NK cells”, Yangyang Li, et al., 26 January 2023. This begs the question, Why is an HIV-1 immunotherapy treatment element being used in a COVID-19 “vaccine?” This also, in Yours Truly’s opinion, removes any consideration of COVAXIN to be labeled a “vaccine” — it is actually a gene therapy/immunotherapy injectable.
And, the 2-Phenoxyethanol excipient (adjuvant) in COVAXIN. Below is a screenshot portion of the Fisher Scientific (ThermoFisher) MSDS Safety Sheet for this chemical, Page 1:
The Kaur, et al., paper, goes into detail regarding the types of reported serious adverse events that affected the study subject pool who took COVAXIN. Three pages of the Supplementary Table 1. from the paper are below. Note that these are details from subjects one year after “vaccination” with COVAXIN. Note also that another paper from December 2020 (by different authors) shows that the S1 protein of the SARS-CoV-2 virus itself crosses the Blood-Brain Barrier.
If Yours Truly is reading about this situation correctly, it appears that one of the “problems” with the Kaur, et al., paper, is that the subject pool of COVAXIN-“vaccinated” persons in North India who reported serious adverse events following “vaccination” to the study authors was “small.” One has to ask: How many COVAXIN-“vaccine”-induced serious adverse events would need to be reported before they would be considered “relevant” by the Indian government and by Bharat BioTech? — say, a “minimum” of 3 million adverse events reports? Is it “within acceptable limits” that COVAXIN-“vaccinated” persons in North India suffer a stroke or a heart attack after “vaccination” with this product? Is this another situation of “the known and potential benefits outweigh the known and potential risks” of taking a COVID-19 “vaccine”, which is the “official” position of the CDC and the FDA in the United States?
Yours Truly has gone into detail regarding the situation with BBV152/COVAXIN for several reasons: First, to enumerate the multiple potentials for “vaccine”-induced serious adverse effects from this COVID-19 “vaccine” product; Second, to highlight the persecution of the authors of a paper who sought to study and write about these potentials; Third, to highlight the persecution of the journal that peer-reviewed, approved, and published the paper;Fourth, to bring to light the involvement of the United States government (via the NSF and the NIAID) in the funding and development of an ingredient (excipient/adjuvant) in this “vaccine” intended for use in a foreign country; and, Fifth, to again emphasize how important it is that consumers “do their own due diligence” regarding information on drugs and/or injectables that they put into their bodies.
The above is a vintage image of Dr. Edward Jenner administering the first smallpox vaccination (inoculation) to James Phipps, 14 May 1796. Courtesy of www.sciencemuseum.org.uk/.
Today’s post, as it relates to the disaster of COVID-19 and the COVID-19 “vaccines”, is dedicated by Yours Truly in memory of her cousin Bill, who died “suddenly and unexpectedly” in September 2023. However, the discussion is not limited to what is presented here: it is an Open Thread.
There are two separate, although connected (Big Pharma), parts to today’s offering. Each part is of itself an expose’. This post is a long one, but important. Please, take a cup of coffee or tea; or, if it’s an appropriate time of the day, perhaps a “wee dram” of something like chilled D.O.M. Benedictine with a twist of lemon peel, and settle in for reading.
Readers already know the caveats regarding civil discussion on this board; of the alternate sites in case the main board is not accessible (here and here); and, that what Yours Truly presents on Health Friday is not medical advice, but opinions and/or hypotheses from ongoing research on COVID-19, Big Pharma, and other health topics.
“Quick, down-and-dirty summary” of today’s post:
One: Pfizer-BioNTech has begun a new enterprise, PfrizerForAllTM, which apparently seeks to completely circumvent / marginalize, in-person consumer contact with pharmacies; to “funnel” in-person consumer contact with healthcare practitioners to “Pfizer-affiliated” professionals; and, to “redirect” the dissemination of information about the COVID-19 “vaccines” to that provided by Pfizer-BioNTech.
Two: That the FDA approval of the very dangerous and deadly Smallpox “vaccine”, ACAM2000, for use also as a “prevention” for Mpox, is the result of a complex mixture of Big Pharma influence + FDA review of the Biologics License Applicaion for this use of ACAM2000 that is, in Yours Truly’s opinion, “a foregone conclusion despite serious reservations”, to say the least + Gain-of-Function experiments on the Mpox virus. There is also a potential tie-in to “an expanded biodefense role.”
Yours Truly has tried to avoid making today’s post read like a scientific paper; however, there is a lot of information that is relevant to each Expose’. Note: Mpox is now the “official” name for monkeypox.
Expose’ One: It appears that Pfizer-BioNTech is creating new ways to increase the company’s consumer operations (and, therefore, potential profit lines.) Pfizer-BioNTech has just launched PfizerForAllTM — a direct sell-to-consumer business that will provide online access to healthcare providers (online [virtual], or affiliated healthcare providers encounters [for example, to get a COVID-19 “vaccination”]); plus, “delivered to your door” prescription drugs and “easier access” to other company products, such as their COVID-19 “test kits.”
In other words, in Yours Truly’s opinion, Pfizer-BioNTech, not happy with the company’s portfolio loss due to falling consumer acceptance of the modRNA COVID-19 “vaccines” offered, and due to the failure of the company’s clinical trial of its “combo” modRNA COVID-19 “vaccine” + influenza “vaccine”, a corporate decision was made to find a way to go straight to the consumer and make it “so easy” to get access to the “vaccines”, plus other Pfizer products. Translation: banish “vaccine” hesitancy / “vaccine” refusal, by doing what may be called “straight to the consumer medical psy-op.” Again, from the Latypova article:
The lawsuit that Pfizer-BioNTech settled in 2009 was over the use of the company’s drug, Bextra, in “off-label” situations. The scope of the settlement is described here: www.justice.gov/, “Justice Department Announces Largest Health Care Fraud Settlement in Its History”, 1 November 2023. A portion of the announcement is below:
This lawsuit was the starting point for FDA changes to its “regulations” regarding the use of prescription drugs in “off-label” situations. The latest FDA changes are summarized here: www.sidley.com/en/insights/newsupdates/2023/11/fda-s-latest-off-label-guidance, 1 November 2023. It appears, in a nutshell, that drug manufacturers can be held responsible (liable) for “off-label” use of their products, even if they already comply with the “new” FDA “regulations.” (Think of this in light of the use of, for example, Ivermectin or Hydroxychloroquine to prevent or to treat COVID-19 — these uses, arguably, are “off-label” for these drugs.)
By the way, PfizerForAllTM is working with UpScript Health and Alto Pharmacy regarding access to healthcare services and filling prescriptions. Guess what? UpScript Health lists Pfizer as a “partner” on the company’s “About” page of their website: www.upscripthealth.com/about/. And, there’s more — Alto Pharmacy, the online prescription drug company, has a couple of interesting members on their Board of Advisors: Alex Azar (HHS head under then-President Trump); and, Dr. Ezekiel Emanuel (he who helped to write the “ObamaCare” bill; he who advocated for people to take their own lives at age 75 “to make room for the younger generation”, and more): www.alto.com/our-company. Dr. Emanuel is also involved with the Center for American Progress (Soros-connected: www.americanprogress.org/c3-our-supporters/); The Aspen Institute; and, he is Co-Director of the Healthcare Transformation Institute (HTI) at the University of Pennsylvania. Below is the Mission statement of HTI (https://hti.upenn.edu/mission/):
Note 1: the “objective” to transform the behavior of physicians and other healthcare providers. (Italics, mine.) Note 2: the “imagifashion” hyperlink, apparently, after getting past the “fake Latin language” on the main page, takes one to a clothing/accessories company in California: https://nilah.la-studioweb.com/contact-us/. (??)
This statement really frosts Yours Truly. My late father was a Registered Pharmacist for 57 years, who: kept his pharmacy very clean and neat (one was part of the crew that swept the floors and cleaned the display shelves starting when she was 10 years old); made it a point to know about all of his patients and to TALK with with then they came to have prescriptions filled or refilled; worked out deals with his suppliers to get extra samples of OTC products to give to his patients who had lost their steel mill jobs when the mills left Pittsburgh in the late 1970s-early 1980s, and, who paid for their prescriptions with his own money at times, etc., — finds the language, “…brick-and-mortar terrible experience…” in the above statement not only to be personally insulting to the memory of her father: but, also, degrading to those “brick-and-mortar” pharmacists who do their job to keep their stores clean and organized.
Expose’ Two: This regards the FDA just “approving” the “expanded use” of the dangerousand deadly Smallpox “vaccine”, ACAM2000, for the “prevention” of Monkeypox (now called “Mpox.”) The FDA issued this “approval” on 29 August 2024. The trail on this begins here: https://mole.substack.com/p/acam2000-package-insert-warning-death, 14 September 2024.
To gain more understanding of Smallpox and inoculation / vaccination against Smallpox, please see: www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination. Both Smallpox (variola) and Mpox (mpox virus) are members of the genus Orthopoxvirus. Whereas, a disease condition that would equate to Smallpox goes at least as far back as to China around 3000BC, Mpox was first discovered in 1958 (all, per Wikipedia search.) Dr. Edward Jenner, an English physician, noticed that milkmaids were immune from Smallpox infection; he deduced that the Cowpox infections that they sustained had made them immune to the other type of infection. Dr. Jenner administered the first “inoculation” of Cowpox virus (to prevent Smallpox) to a child, James Phipps, on 14 May 1796. Another source of information is here: wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/smallpox-and-other-orthopoxvirus-associated-infections. Further details are found here, in the article, Edward Jenner and the history of smallpox and vaccination, January 2005. A screenshot of a portion of this article is below:
About ACAM2000: it is manufactured by Emergent BioSolutions, headquartered in Gaithersburg, MD. The FDA approved ACAM2000 for use for the prevention of Smallpox in August, 2007. It contains vaccinia, a live virus ingredient used in modern Smallpox vaccines. The vaccinia used in ACAM2000 is a replicating version. The vaccine is cultured in a mixture of African Green Monkey kidney cells (sound familiar? — as in, perhaps, SV40 African Green Monkey cancer promoter gene splice that was found in the Pfizer-BioNTech modRNA COVID-19 “vaccine” by Dr. Kevin McKernan?). ACAM2000 was originally only intended for use to prevent Smallpox — until its use was “suddenly expanded” on 29 August 2024 by the FDA to include prevention of Mpox (more on that later in the post.) Since then, articles such as this one have appeared (https://childrenshealthdefense.org/defender/fda-acam2000-mpox-vaccine-warning-death-unvaccinated/, 17 September 2024, by Suzanne Burdick, Ph.D.; and, social media has been posting items like this one: https://x.com/toastontheside/status/1835921932841062412. This tweet references the FDA-issued handout for patients and/or caregivers regarding ACAM2000. The FDA handout is found here: www.fda.gov/media/75800/download. FDA handout documents for patients and/or caregivers are likely to have, in Yours Truly’s opinion, “sanitized” information and “pablum-like” assurances regarding the “safety and efficacy” of the drug or injectable. The FDA handout for ACAM2000, however, is different: when one reads the handout, one gets a distinct impression that this “vaccine” is highly dangerous. Below is a screenshot portion of the FDA patient/caregiver handout for ACAM2000:
Note that there is NO MENTION of the other FDA-approved Mpox vaccine, JYNNEOS, which is arguably “safer” for the patient (see further down in the presentation regarding JYNNEOS.)
The Fact Sheet for Healthcare Providers for ACAM2000 is here: www.fda.gov/media/75792/download. The document gives a much more comprehensive picture of the dangers of this “vaccine.” Yours Truly will highlight a few of the items in this document which show how dangerous and deadly this vaccine is, beginning with two images from page 1 of the Fact Sheet: the Black Box Warning; and, the Warnings and Precautions:
Remember, this dangerous and deadly “vaccine” is now approved for persons “at risk for Mpox”, in addition to persons at risk for Smallpox (this disease was eradicated in 1980.)
And, from Section 6 Adverse Reactions portion of the Fact Sheet for ACAM2000:
Continuing with Section 11 Description from the Fact Sheet for ACAM2000:
And, from Section 17 Patient Counseling Information of the Fact Sheet for ACAM2000, two portions:
Note several items from the above screenshots: One, that the “vaccine” must be given to the recipient via 15 separate jabs with a bifurcated needle; Two, there are MULTIPLE adverse reactions potential for persons taking this “vaccine”; Three, that persons who contract a Smallpox infection from a person “vaccinated” with ACAM2000 can die of the infection they contract; Four, that the ACAM2000-“vaccinated” person must stay away from pregnant women, household members, persons with eczema, etc., for a period of time after “vaccination”; among many other issues.
Yours Truly will again recall to the reader’s mind that ACAM2000 is now FDA-approved for PREVENTIVE USE among persons who are at risk for Mpox. From what Yours Truly has read about it, Mpox is, for all intents and purposes, likely to be a LESS-DANGEROUS form of Orthopoxvirus, compared to another form of the same Genus, variola (Smallpox virus.) [HOWEVER, see the presentation answering Question Two, further below in the post.] There is a vaccine that was previously FDA-APPROVED for the prevention of Mpox — JYNNEOS, manufactured by Bavarian-Nordic. This vaccine also uses the vaccinia virus as the foundation; but, JYNNEOS is cultured in a mixture of chicken embryo cells; and, although it also has live vaccinia, it is a NON-replicatingversion. JYNNEOS was also originally FDA-approved for the prevention of Smallpox. In Yours Truly’s opinion, even though JYNNEOS does indeed have potential for serious adverse reactions (for example, cardiac issues), this vaccine appears to be much less dangerous and deadly compared to ACAM2000. The FDA Fact Sheet for Healthcare Providers for JYNNEOS is here:www.fda.gov/131078/download.
Two questions arise immediately: First, what is about ACAM2000 that makes it so dangerous?; and, Second, why did the FDA suddenly approve the use of ACAM2000 for the prevention of Mpox in August 2024?
As to the first question: ACAM2000 is the “descendant Smallpox vaccine” from the older Dryvax Smallpox vaccine, which was manufactured by Wyeth. ACAM2000 replaced Dryvax in August 2007, after FDA approval. The Package Insert (archived version) for Dryvax is here: https://biotech.law.lsu.edu/blaw/bt/smallpox/dryvax_label.htm. Below are two screenshots from the Package Insert for Dryvax:
Note that the inoculation process for Dryvax consisted of 2 or 3 punctures for the initial (primary) vaccination; and that 15 punctures were used for revaccination. However, ACAM2000 requires 15 punctures for the initial vaccination. Why 15 punctures for the initial vaccination? It would appear, in Yours Truly’s opinion, that requiring 15 punctures for the initial vaccination with ACAM2000 exposes the patient to more of the ingredients of the vaccine (think the Moderna COVID-19 modRNA “vaccines”all having more than 3 times the “mcg payload” of lab-enhanced SARS-CoV-2 spike protein PER INJECTION, as compared to the “mcg payload” of the Pfizer-BioNTech modRNA COVID-19 “vaccines.” [Which is NOT to say that the Pfizer-BioNTech modRNA “vaccines” are somehow “safer” than those of Moderna. THEY ARE NOT.])
Yours Truly turns to section 8.1 of the FDA Fact Sheet for Healthcare Providers for ACAM2000 (link above.) This “vaccine” is particularly dangerous to pregnant women, to women who wish to become pregnant, and to a fetus carried by a pregnant woman (whether or not she is “vaccinated” with ACAM2000, since persons “vaccinated” with this product will “shed” ingredients [from the forming / formed pustule, or the scab from the pustule, etc.], onto other persons who come into contact with the “vaccinated” person.) Below is section 8.1:
It would also appear that there is inherent danger due to the fact that ACAM2000 uses a live, replicating vaccinia (another Orthopoxvirus that is “weaker” than variola [the Smallpox virus], and which is used to make modern-day Smallpox / Mpox vaccines), as compared to the live, NON-replicating vaccinia that is used the JYNNEOS Smallpox / Mpox vaccine. Once inoculated (vaccinated) with ACAM2000, the vaccinia produces a kind of “mini-infection” in the patient, affecting the area around the inoculation site, along with the lymph nodes in the same area. Vaccinia may also appear in the blood of the patient. There is also the issue of “self-inoculation” by the ACAM2000-“vaccinated” patient (from scratching or “picking at” the scab that forms after the “mini-infection” pustule forms on the skin, and also when this pustule begins to clear); and for other reasons — the FDA Fact Sheet section 17 Patient Counseling Information for ACAM2000 discusses this. In addition, there is the varying amount of vaccinia concentration that is produced in the patient after ACAM2000 inoculation; see below from section 11 Description of the FDA Fact Sheet for Healthcare Providers:
In other words, there are many areas about the ingredients and mechanisms of ACAM2000 that raise the risk of complications, including death, for the patient who takes this “vaccine”, for pregnant women and their fetuses, for women who wish to become pregnant, for persons who are immunocompromised, and for persons who are NOT “vaccinated” with ACAM2000, during the multiple “danger zone” weeks after ACAM2000 inoculation.
Turning to the second question, concerning the FDA approval in August 2024 for ACAM2000 to be used as an Mpox “vaccine”: this situation is complex. It involves Big Pharma, the WHO, and, what to Yours Truly “smells like” Gain-of-Function research, among other items.
Yours Truly will begin with Emergent BioSolutions, the company that produces ACAM2000. Emergent BioSolutions, a “global enterprise” with headquarters in Gaithersburg, MD, was established in 1998. Its first project was to partner with the United States Defense Department to supply the Anthrax vaccine that was administered to members of the military (www.emergentbiosolutions.com/about-us/.) The current CEO of the company is Joseph C. Papa. Mr. Papa’s most-recent position was CEO of Bausch + Lomb, another large Big Pharma company. Mr. Papa, apparently, is a “mover and shaker” in the pharmaceutical industry. However, it is also apparent that Baush + Lomb was in financial trouble when he left it to become CEO of Emergent BioSolutions. In fact, Bausch + Lomb is “exploring” selling off some of its pharmaceutical assets, due to “significant debt load” (https://finance.yahoo.com/news/bausch-lomb-explores-sale-amid-112230409.html.) Perhaps, the company’s Post-IPO debt funding was not enough: www.crunchbase.com/organization/bausch-lomb/company_financials; scroll down to “Investors.” Mr. Papa has Bachelor’s and Doctorate degrees in Pharmacy; his career includes working with many Big Pharma companies (Novartis, Cardinal Health, and Watson Pharmaceuticals, among others.) Please see his entry in Wikipedia; and, here: https://waterstreet.com/people/papa-joseph. Water Street (Water Street Healthcare Partners) is an investment company that has a portfolio worth approximately $6Billion spread across healthcare services companies, medical diagnostics companies, and pharmaceutical/life sciences companies (https://waterstreet.com/companies.)
Mr. Papa was hired on 21 February 2024 by Emergent BioSolutions to facilitate the financial turnaround of the company. Below is a screenshot of the company’s financials from September 2023 to September 2024, via Crunchbase. It appears that Mr. Papa, a “mover and shaker” in the Big Pharma world, is working hard:
Also, via Crunchbase, a snapshot of Emergent BioSolution’s funders:
It appears that now, Mpox is being “re-classified” as another, although serious, sexually-transmitted disease that can infect any sexually-active person; and, that Mpox has apparently “made the leap” from monkeys to other animals (rodents and even to domesticated dogs), and to between animals and humans. This leads to another aspect of the situation: Yours Truly’s suspicion that there have been / are ongoing, Gain-of-Function experiments on Mpox.
Here is the “fast and dirty” summary on Gain-of-Function experiments with Mpox:
One: Up until 22 August 2024, the FDA had only ONE approved “vaccine” for Mpox: JYNNEOS. However, on that same day, the FDA conducted a “review” of the BLA Application (Biologics License Application) for ACAM2000 to have approval as a “vaccine” for Mpox. This application was approved on 29 August 2024 (www.fda.gov/news-events/press-announcements/fda-roundup-august-30-2024.) Please see: www.fda.gov/media/181552/download for the BLA review. The FDA reviewers, apparently, had some “reservations” about ACAM2000 — see the screenshot below:
Despite the multiple reviewer comments regarding the BLA for ACAM2000, the FDA approved it anyway for Mpox “prevention.” In fact, look at THIS, from section 11.2 of the ACAM2000 BLA document, below:
Two, the Gain-of-Function issue regarding Mpox: First, the CDC connection:
The CDC has an updated report on the incidence of Clade II infections of Mpox, an outbreak that originated in Central Africa (more on Clade II of Mpox further down in today’s post): www.cdc.gov/, “Clade II Mpox Outbreak Originating in Central Africa”, 13 September 2024. Per this article, there are no Clade I Mpox infections in the United States at this time; however, there are 2466 reported cases of Clade II Mpox infections, with 7 deaths. There are also, per the CDC report, cases of Clade II of Mpox literally all over the world at this time.
Here is an example of Gain-of-Function experiments with the Clade II of Mpox. This paper is about a study conducted at Kansas State University in which pigs were exposed to the Clade II of Mpox to see if they would get sick, and then take various blood and biological samples and test them. Sure enough, the pigs contracted Mpox. Please see: www.ncbi.nlm.nih.gov/pmc/articles/PMC11168330/, “Experimental inoculation of pigs with monkeypox virus results in productive infection and transmission to sentinels”, Emily Mantlo, et al., 7 May 2024. “Sentinels” were the pigs who were not injected with the Clade II Mpox, but were put in the same cages as those pigs who were. The “sentinel” pigs also came down with Mpox (in other words, animal-to-animal transmission of the virus.) Below are the Ethics Statement and the Funding Statement for this study:
Note that the study was conducted in BSL-3 labs at KSU; that tissue-processing was performed at CDC BSL-2 facilities; and, that, apparently, college students were working in the BSL-3 labs in the study. This indicates that Gain-of-Function experiments with the Clade II of Mpox were being performed; that lower-level biosafety labs were used; and, that college students were involved (how much close supervision was provided by KSU?)
So, Gain-of-Function experiments are being performed using the Mpox virus; experiments funded by the NIH. A very dangerous, deadly Smallpox “vaccine”, ACAM2000, was suddenly FDA-approved for the “prevention” of Mpox. The “definition” of who is “at risk” for an Mpox infection has been “expanded” to include all persons who are sexually active. The Clade II of Mpox (the one that is the subject of the Gain-of-Function experiments) is now infecting people all over the planet, including in the United States. And more. Cui bono? How many of the general public will line up for an injection of ACAM2000 because the CDC / FDA / AMA / Establishment Medicine, will issue a warning due to “increasing numbers of infections being reported of Mpox?” How many healthcare professionals will be “mandated” into taking ACAM2000 “to protect themselves and the patients they care for?” (Again, JYNNEOS was already approved for Mpox “vaccination”, and it is ** potentially ** a “safer” alternative “vaccine.”) How many more Gain-of-Function experiments will be conducted, not in facilities like the Wuhan Institute of Virology or the Baric Lab at UNC Chapel Hill — but at places like the BSL-3 Ag Lab at Kansas State University (a facility where, arguably, one would expect research on, say, equine viruses, not Clade II Mpox experiments on pigs)? How much more Gain-of-Function experimentation will be hidden and/or “obscured” from public knowledge, let alone from Congress?