“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
The above vintage image of the United States Congress in session is courtesy of the Library of Congress and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As today’s post speaks of the disaster of the lab-created bioweapons called COVID-19 — the COVID-19 virus itself; and, the COVID-19 “vaccines” — Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these bioweapons.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. NOTE: Yours Truly has checked today’s offering for AI-generated content. To the best of her knowledge and belief, there is none. If anyone wishes to post AI-generated content to today’s discussion thread, they must cite their source. Thank you.
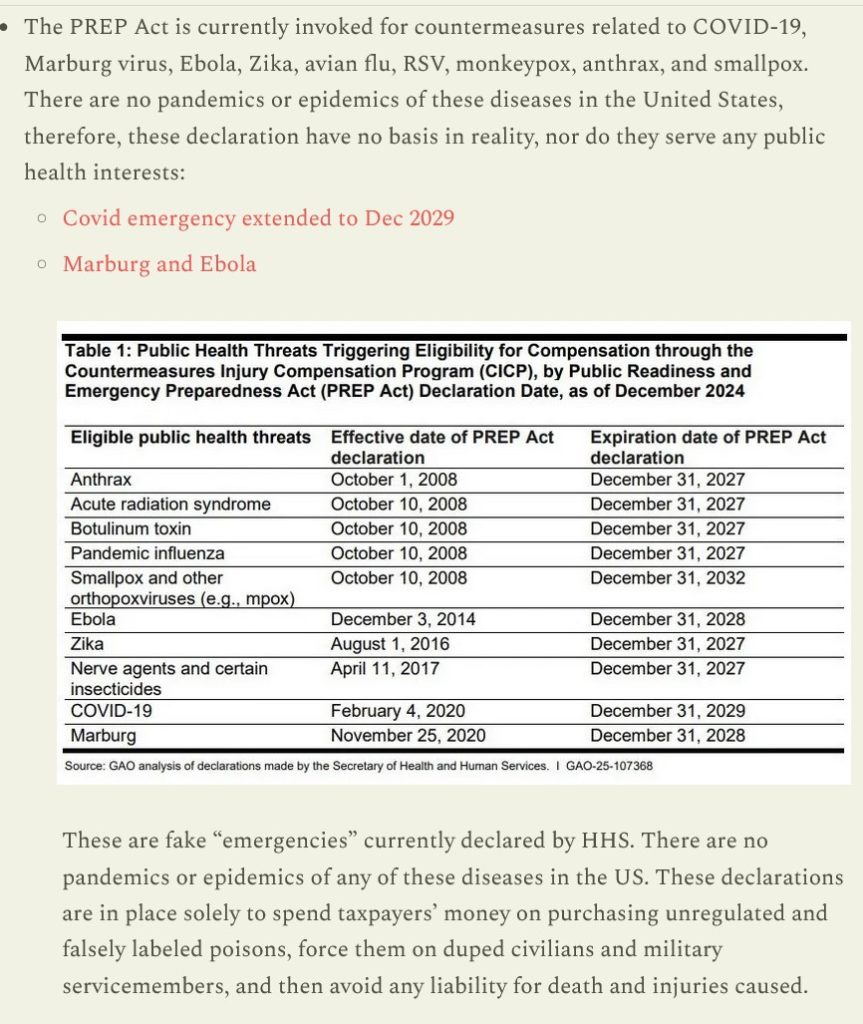
The PREP Act (also called PREPA) is a “License to Kill“, in the words of Sasha Latypova (https://sashalatypova.substack.com/.) The PREP Act removes accountability, liability, and transparency from the activities of the Health and Human Services Department of the United States Federal Government under the provisions of the Act. The PREP Act allows: unlimited research, development, and use of COVID-19 “countermeasures”, including, but not limited to, “vaccine” development and use; “respiratory devices” development and use (think ventilators); prescription drugs use (think Paxlovid and Remdesivir); “mandated” uses of masking, of “social distancing”, and even of “lockdowns”; the “mandated” administration of COVID-19 “vaccines”, including to newborn babies, to persons under the age of 18, to persons who wish to attend school or to work; and much more. The PREP Act allows the United States Federal government and its associated departments (including Health and Human Services and the United States Defense Department) to literally use American citizens as “human lab rats” in the administration and use of dangerous, deadly, COVID-19 “countermeasures” which are not “safe and effective”; but which, instead, damage and/or destroy the bodies and minds of the persons who take the COVID-19 “vaccines” and/or drugs such as Remdesivir. The PREP Act uses taxpayer monies, private research grants, collaboration with scientific labs all across the United States (think the Baric Lab at UNC, Chapel Hill), and with foreign labs (think the Wuhan Institute of Virology) to pursue the provisions of the PREP Act.
Yours Truly begins here: https://www.federalregister.gov/documents/2024/12/11/2024-29108/12th-amendment-to-declaration-under-the-public-readiness-and-emergency-preparedness-act-for-medical, “12th Amendment to Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID-19”, signed by then-Health and Human Services Secretary Xavier Becerra, 11 December 2024. This 12th Amendment extends the PREP Act (also called PREPA) “emergency status” of COVID-19, along with all medical countermeasures used against COVID-19 (including development and use of “vaccines”, “respiratory devices”, and so on) — until 31 December 2029 (in other words, until after the 2028 General Election and into the Presidential administration that takes over on 20 January 2029.) It also means that, even though the “official” COVID-19 “state of emergency” ended in May 2023, the “virus emergency status” has not been ended. It also means that legal liability for any person, any medical professional, any drug manufacturer, any hospital / clinic / care facility, and supplier, and so on, that fall under the provisions of the 12th Amendment — are legally exempt from any and all liability. It also means that, while the current Health and Human Services Secretary can sign a document that rescinds and/or modifies the 12th Amendment, it must take an act of Congress to repeal the PREP Act.
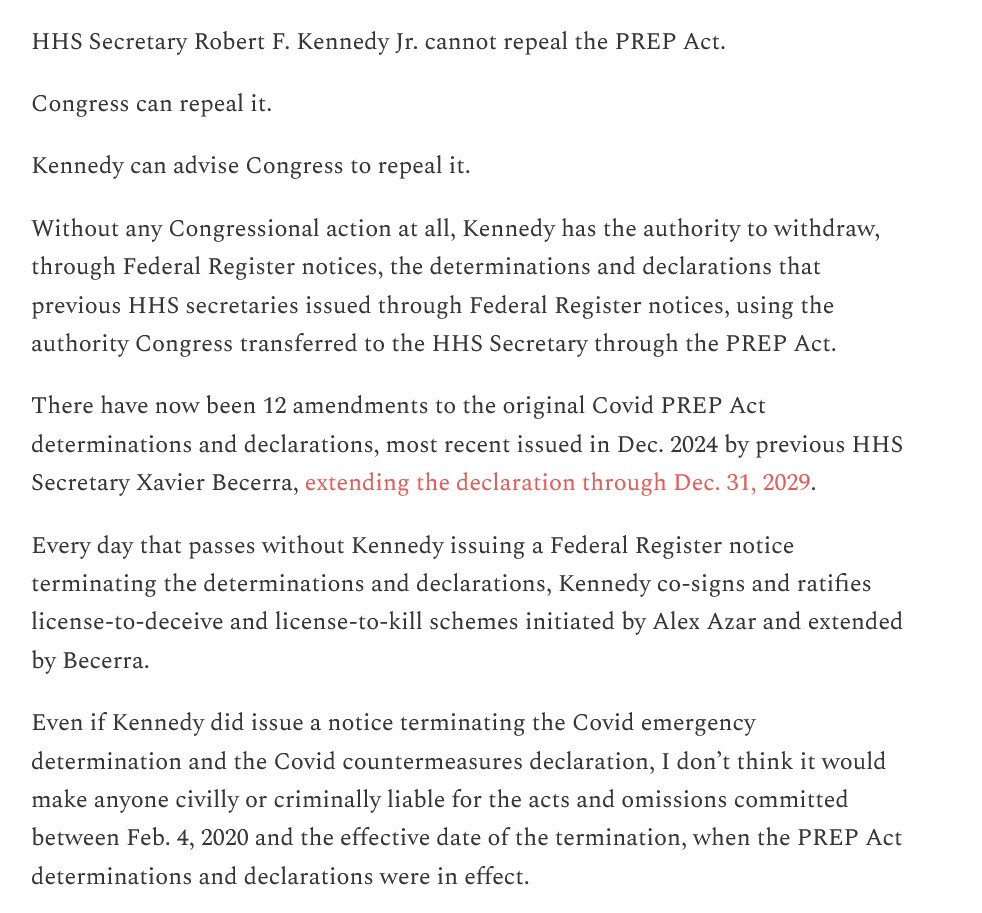
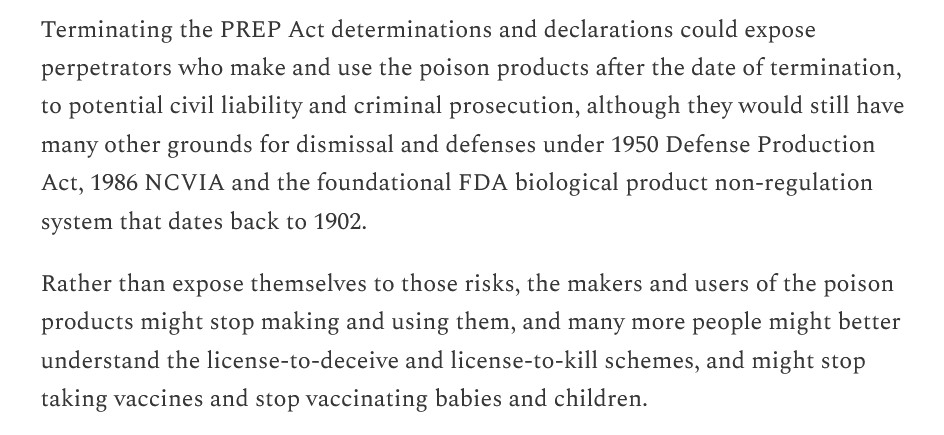
Per Katherine Watt (paralegal and professional researcher), the two separate actions mentioned above are discussed here: https://bailiwicknews.substack.com/p/repealing-prep-act-and-terminating, “Repealing PREP Act and terminating HHS Secretary determinations and declarations issued under PREP Act are two different things.”, 4 April 2025. Please see the screenshots from her article, below:
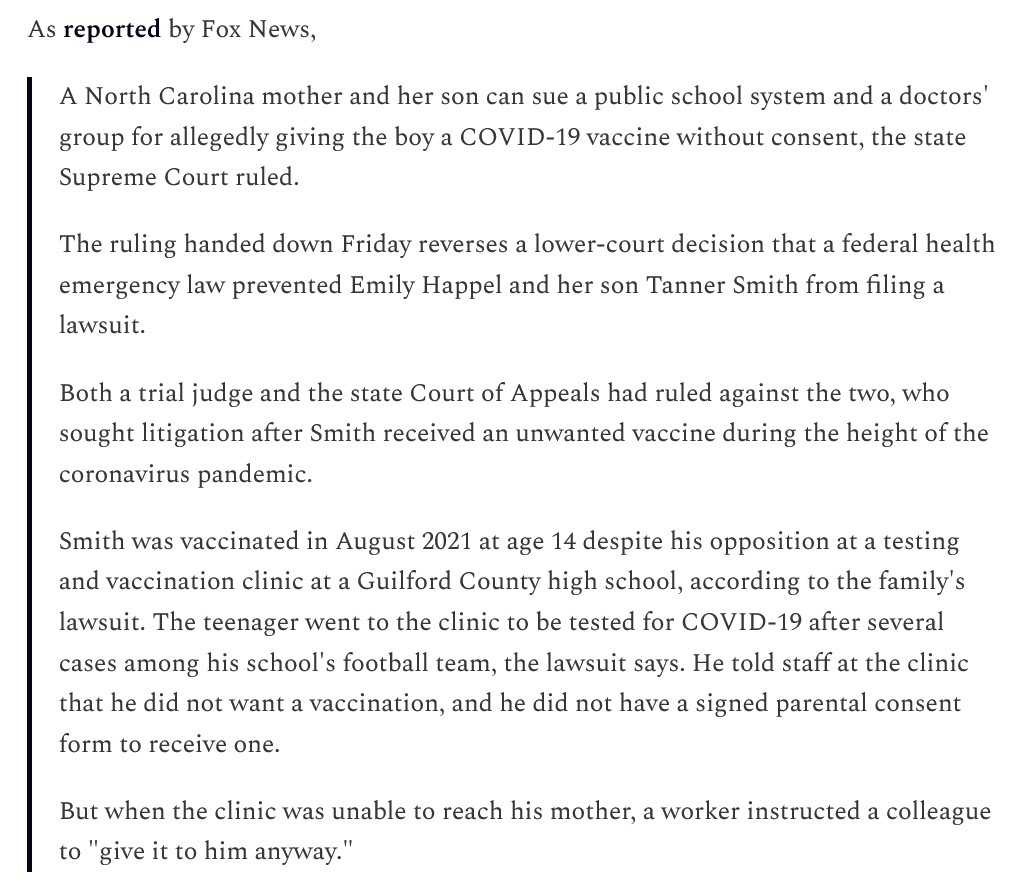
It appears that the various States of the United States have little room to challenge the provisions of the PREP Act. However, a recent case before the North Carolina Supreme Court, regarding a person under age 18 who was given a COVID-19 “vaccine” without consent, was decided in favor of the plaintiff: https://thefocalpoints.com/p/give-it-to-him-anyway-teen-given, “Give It to Him Anyway”: Teen Given COVID-19 mRNA Shot Without Consent — State Supreme Court Says Family Can Sue”, by Nicolas Hulscher, MPH, 24 March 2025. Please see the screenshot from the Hulscher article, below:
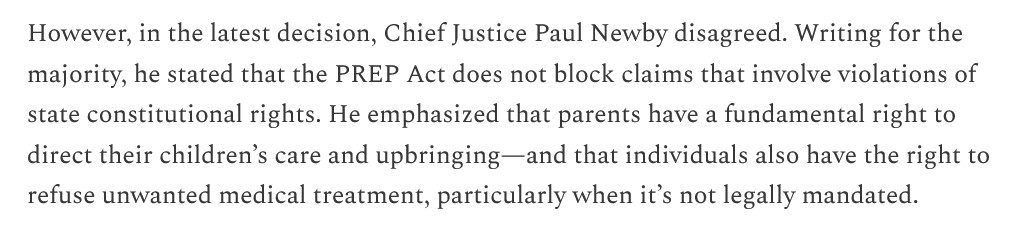
A lower court in North Carolina ruled that the family could not sue the school system, due to the “liability provisions” of the PREP Act. However, the North Carolina Supreme Court overruled the lower court, stating that the family can indeed sue:
Before turning to the final aspect of today’s offering, Yours Truly will expand the mention of Sasha Latypova above in the post. Ms. Latypova, a native of Ukraine, was trained in medical and pharmaceutical technology. She owned and ran several companies in this area. She worked with Pfizer-BioNTech and other drug manufacturers in medical technology. She is therefore a person with deep experience, in Yours Truly’s opinion, regarding the workings of these industries. After moving to the United States and subsequently retiring from these endeavors, Ms. Latypova began to research and write on how the medical technology and the pharmaceutical industries have now become entities that serve their shareholders and the government, not the patients they claim to serve. Regarding the PREP Act, here is one of her blog posts: https://sashalatypova.substack.com/p/prep-act-license-to-kill-must, “PREP Act Brief: “License to Kill” must be repealed.”, 21 April 2025. This article is densely-written and detailed. Below are a couple of screenshots from her post. Note: There are numerous hyperlinked information sources embedded in the article:
Please also see this post, an interview between Ms. Latypova and Ms. Watt (Bailiwick News) regarding the PREP Act: https://sashalatypova.substack.com/p/interview-with-the-former-feds-foundation, “Interview with the Former Feds Foundation: Katherine Watt and I discuss PREP Act as an act of treason.”, 25 April 2025.
Finally, there is this blog article from “Spartacus”: https://iceni.substack.com/cp/162062988, “Declaration of Sovereignty Pt. 1”, 24 April 2025 (this is a cross-post from the Mole substack website.) This post is long and intense; it traces the “Profane Myth of COVID-19.” A screenshot of part of this post is below:
It is the PREP Act which, in significant amounts, has placed the United States in the position where the country is today: just under 70% of the population has taken at least one injection of a dangerous, deadly COVID-19 “vaccine” (these injectables are NOT “safe and effective”, and mounting evidence proves this); the country is just beginning to emerge from the economic devastation and chaos of the “COVID lockdowns” period; and, the Medical Tsunami of COVID-19 “vaccine”-induced injuries, illnesses, disabilities, and deaths, which is starting to present among the “vaccinated.” There are many persons involved in the above who must now be held accountable; not the least of which are those who knew how dangerous and potentially deadly the COVID-19 “vaccines” are while working with “Operation Warp Speed”, and who withheld this information from then-President Donald Trump.
The free vintage image above of children being vaccinated is courtesy of iStock and Getty Images, via Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics. As today’s post speaks to the disaster of the COVID-19 “vaccines” (Bioweapon Toxin Injections), Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created bioweapons.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. NOTE: Yours Truly has checked today’s offering for any AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post anything in the discussion thread for today’s post that is AI-generated, they must cite their source. Thank you.
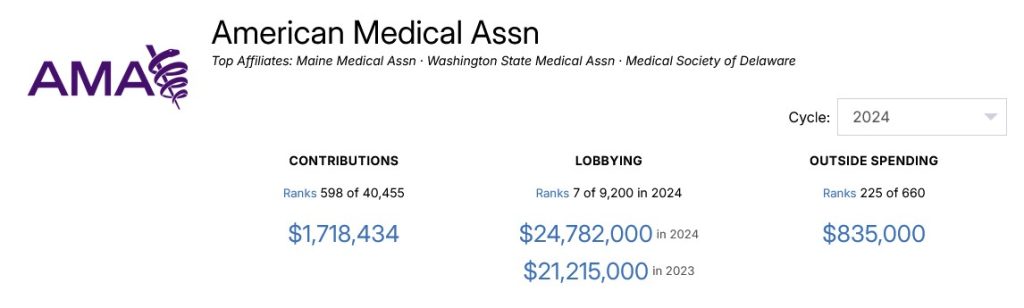
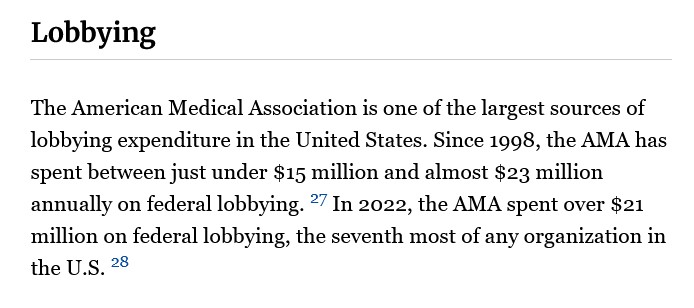
Yours Truly has written about the American Medical Association (the AMA) on previous occasions. The AMA is one of the most powerful professional organizations for physicians in the United States. The organization, which does not provide a list of its members to the general public, is also one of the most powerful lobbying agents in Congress. In addition, the AMA owns the rights to use the CPT codes, which are the codes for medical procedures, examinations, tests, for ordering medical equipment, and much more. The CPT codes are used to bill CMS (Medicare / Medicaid), and to bill private insurers. Please see below for screenshots from, first, https://www.opensecrets.org/orgs/american-medical-association-summary; and, second, https://www.influencewatch.org/non-profit/american-medical-association/, regarding AMA spending on lobbying:
And, not surprisingly, the CPT code royalties paid to the AMA for use of these codes appear to generate the bulk of income for the organization — no wonder the AMA can spend over $21 million on lobbying efforts. Please see: https://paddockpost.com/2024/12/16/how-revenue-is-spent-at-the-ama-2022/.
The AMA has multiple “sub-units” within the organization. These “sub-units” range from DEI (Diversity, Equity, and Inclusion), to “health equity”, and to LGBTQ++ “health inclusion”, among others. The organization offers numerous CME (Continuing Medical Education) online courses and webinars for AMA members, to assist them in accumulating the yearly CME credits they must earn in order to maintain their License to Practice Medicine. It also publishes numerous medical papers, articles, and other media; among them, JAMA (the Journal of the American Medical Association.) Please see: https://www.theqtree.com/2024/04/24/the-ama-edhub-window-to-establishment-medicine/.
An example of an AMA-published article regarding “physician strategies to combat vaccine hesitancy among patients” is here: https://www.ama-assn.org/delivering-care/public-health/covid-19-vaccine-hesitancy-10-tips-talking-patients#, “COVID-19 vaccine hesitancy: 10 tips for talking with patients”, by Tanya Albert Henry, 15 December 2023. Here are the “10 tips”: “Know you are the most trusted information source”; “Tell patients they need to get the vaccine”; Understand your patients’ concerns”; “Ask why a patient is hesitant”; Counter any misinformation”; “Tailor your message”; “Address patients’ fear about side effects”; “Prepare our staff to answer questions”; “Show your vaccination pride”; “Tell stories to make impact”.
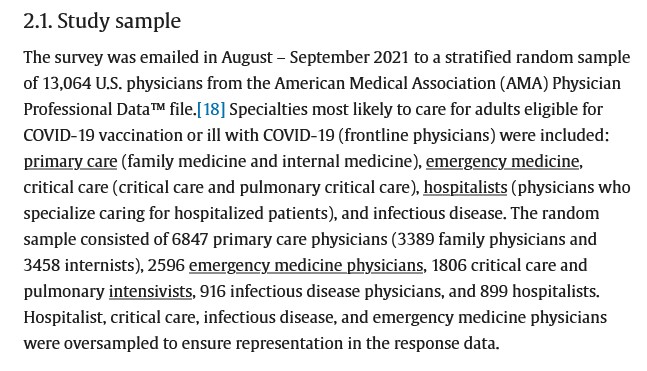
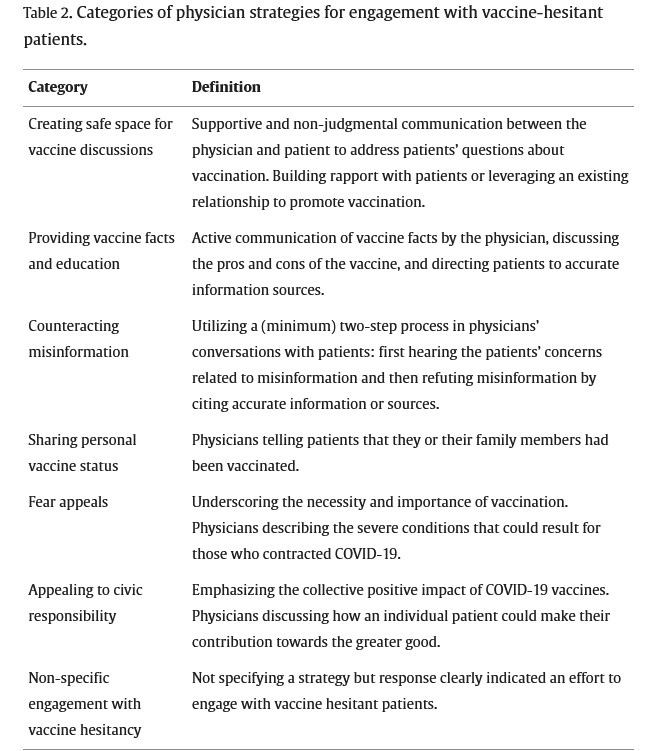
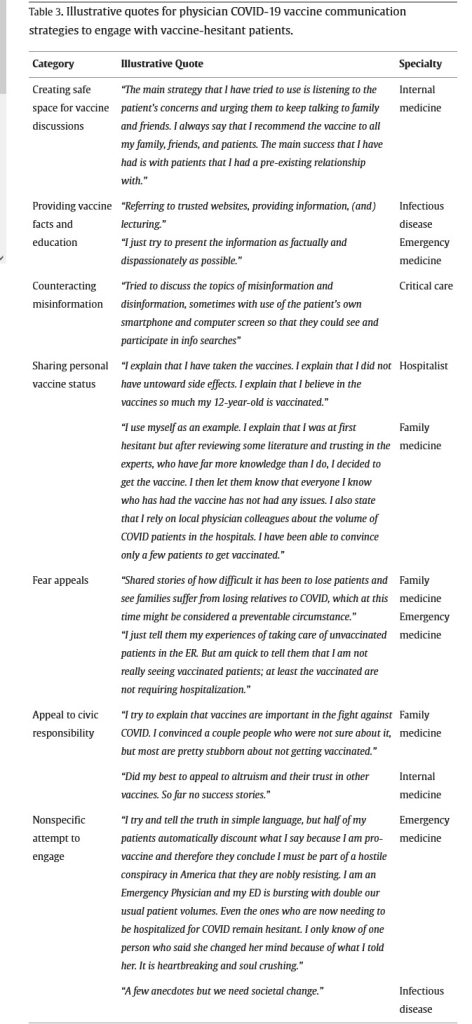
But, what are physicians supposed to say to the patient in order to “convince” them to take a COVID-19 “vaccine”? Again, the AMA has answers: for example, the “templates” in this published study: https://www.sciencedirect.com/science/article/pii/S0264410X24004377, “Patient concerns and physician strategies for addressing COVID-19 vaccine hesitancy”, Joy Melnikow, et al., 22 May 2024. Below are three screenshots from this paper: section 2.1 Study sample; followed by Table 2, then Table 3:
All of above is to get a patient to agree to having a COVID-19 Bioweapon Toxin Injection (aka a COVID-19 “vaccine”) injected into their body. In Yours Truly’ opinion, if a physician follows the above “templates”, they are functioning not as physicians who swore to “Do No Harm”; in fact, they may be considered as “government representatives” under the current “extension” of the PREP Act for COVID-19 Countermeasures” that was signed by then-HHS Secretary Xavier Becerra in December 2024. Notice also the use of various aspects of direct psychological manipulation and of gaslighting in the “templates” for the physicians to follow. One wonders: What would these physicians say in response to a “vaccine-hesitant” patient who gives them a hard copy of a published study that clearly shows what the COVID-19 “vaccines” actually do to damage a “vaccinated” person’s body?
And now, to the most recent AMA “strategies for physicians to use on patients with vaccine hesitancy” effort, from the AMA EdHub series: https://doi.org/10.1001/jama.2025.4882, “Strategies for Communicating with Parents About Vaccines”, Sean T. O’Leary, MD, MPH, 9 April 2025. This article is full-access for AMA members; through an institution; or, via renting it through DeepDyve. Yours Truly went to DeepDyve and was able to get the following screenshot from the first page of Dr. O’Leary’s article, below:
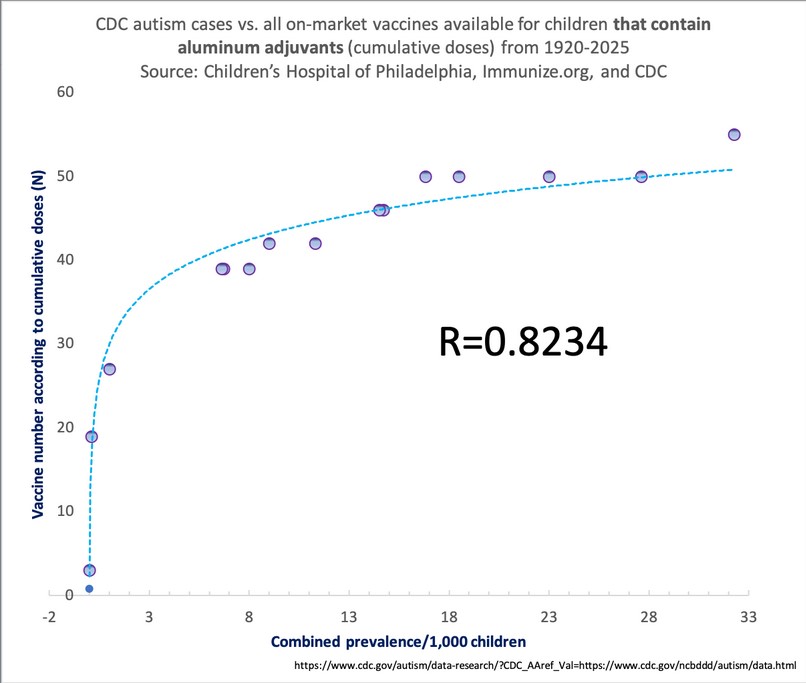
Note the “strategies” that are to be used by the physician, listed in the Table above. Again, it appears to be yet another mixture of “your physician is the most trusted source of information”; plus, “It’s the responsible thing to do for your child”; plus, something new, “Prebunking“, which appears to be a type of psychological manipulation of / gaslighting of, the parent regarding any information they may find online from other physicians (say, Dr. Peter A. McCullough) regarding the dangers of taking the COVID-19 “vaccines”; or, other researchers (say, Steve Kirsch, about how childhood vaccination can induce autism [via the aluminum in the vaccines], and who cites medical statistics to support his contention.) Please see: https://kirschsubstack.com/p/two-pieces-of-evidence-that-together, “Two pieces of evidence that together show that vaccines cause autism”, 21 April 2025. Please also see: https://jessicar.substack.com/p/aluminum-exposure-and-autism-prevalence, 19 April 2025. Dr. Rose cites the following image, from data collected by the CDC:
Why is the AMA still pushing psychological manipulation / gaslighting “strategies” for physicians to use to “convince” patients to take a COVID-19 “vaccine”, or to allow their child (children) to be COVID-19 “vaccinated”, or to allow their child (children) to be “vaccinated” with injectables that contain substances such as Aluminum? Why does the CDC have dozens of “vaccines” listed on the agency’s Child and Adolescent Immunization Schedule (https://www.cdc.gov/vaccines/hcp/imz-schedules/downloads/child/0-18yrs-child-combined-schedule.pdf)? With “vaccines” that are to be administered to newborns immediately after birth? Why do almost all public school systems “require” certain “vaccines” to be given to a child in order to attend public school? Why do state legislatures give the force of law to the CDC Child and Adolescent Immunization Schedule through legislative fiat for public school attendance — given that the CDC states on the schedule that the injectables are “Recommended”, not “Required”? Why do the AMA, the CDC, and the FDA refuse to acknowledge that the COVID-19 “vaccines” are dangerous and deadly, given the mountain of evidence currently in print which proves this to be the case?
The above free image of an 1867 vaccination certificate is courtesy of iStock and Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics. As today’s post speaks to the disaster of the COVID-19 “vaccines”, Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created bioweapon toxin injections.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. Note: Yours Truly has checked today’s post for any AI-generated content. To the best of her knowledge and belief, there is none. If readers wish to post any AI-generated content in the discussion thread for today’s post, they must cite their source. Thank you.
Today’s Health Friday offering is one of a “mini-series” devoted to one topic and to one important news item related to that topic (although there may be other items related to the topic presented as supporting and/or clarifying information. The topic for today is what the COVID-19 “vaccines” do to damage and/or destroy the crucial IgG3 immune system cells in the “vaccinated” person’s body.
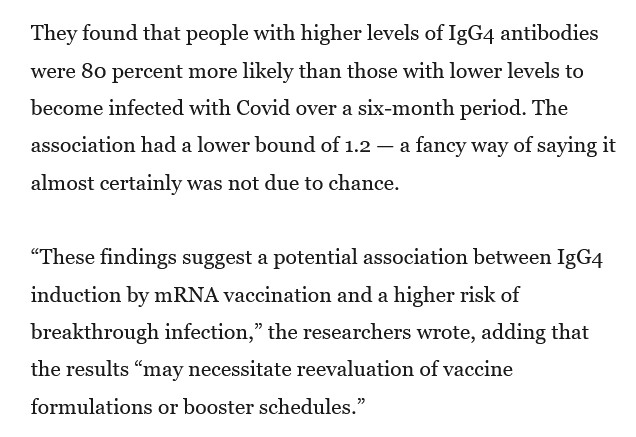
This 80% higher risk was found in persons who had had multiple injections of COVID-19 “vaccines.”
The COVID-19 “vaccines”, especially via repeated injections, damage and destroy the crucial IgG3 (“fight it off”) immune system cells in the “vaccinated” person’s body; while, at the same time, fostering the increase of the IgG4 (the “tolerate but never clear”) immune system cells.Another screenshot from the Berenson article is below:
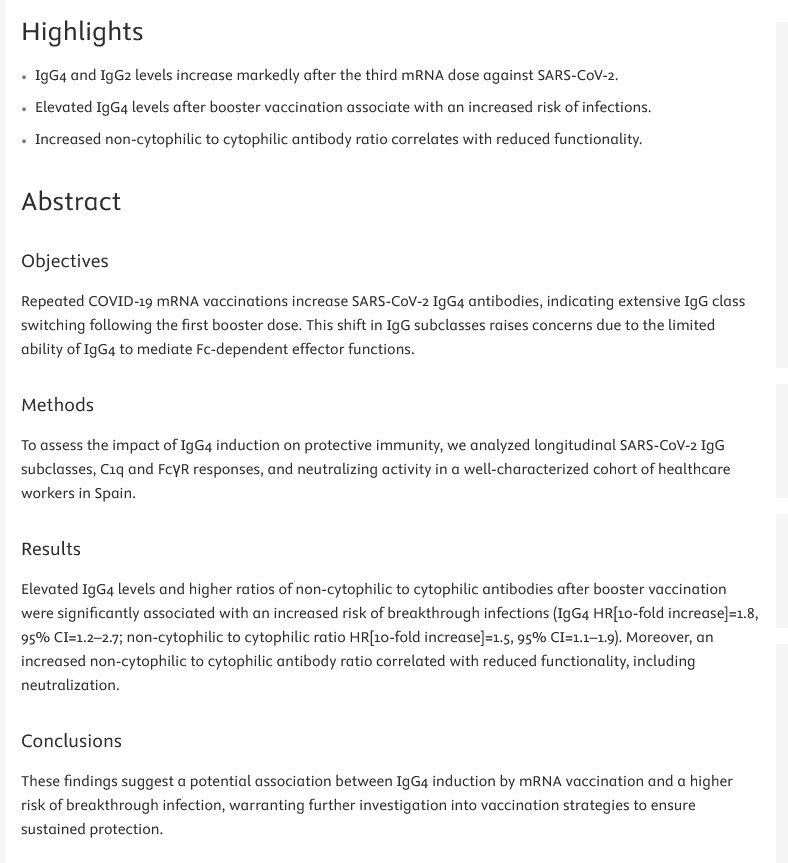
The paper referred to in the Berenson article is here: https://doi.org/10.1016/j.jinf.2025.106473, “Post-Vaccination IgG4 and IgG2 class switch associates with increased risk of SARS-CoV-2 infections”, Gemma Monocunill, et al., 18 March 2025. Below is a screenshot from this paper:
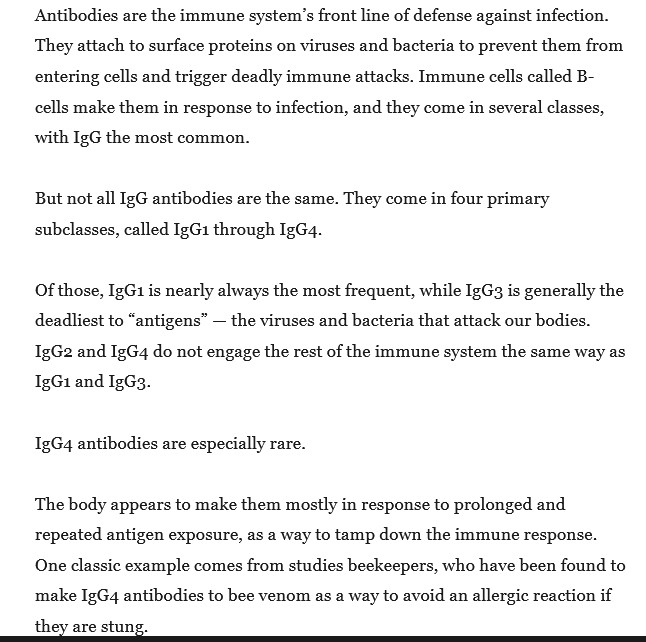
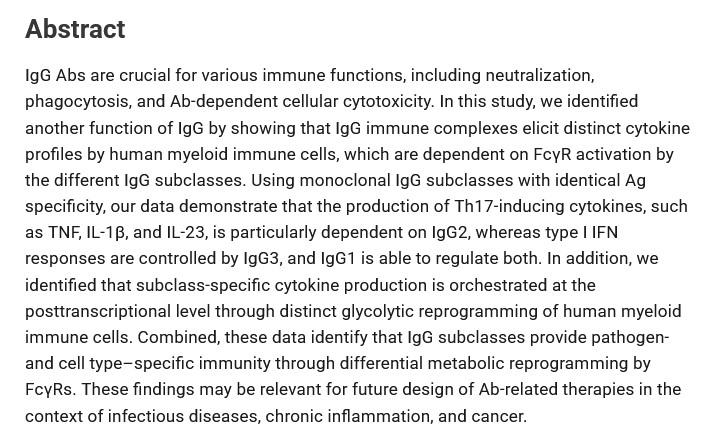
An important paper regarding descriptions and functions of the IgG immune system cell class in the human body is here: https://journals.aai.org/jimmunol/aticle/205/12/3400/107683/IgG-Subclasses-Shape-Cytokine-Responses-by-Human, “IgG Subclasses Shape Cytokine Responses by Human Myeloid Immune Cells through Differential Metabolic Reprogramming”, Willianne Hoepel, et al., 15 December 2020. A screenshot of the Abstract of this paper is below:
Note that this paper was published after the modRNA COVID-19 “vaccines” by Pfizer-BioNTech and by Moderna were granted their initial EUAs in the United States by the FDA (this occurred on 11 December 2020), but before these bioweapon toxin injections entered widespread use.
Back to the Monocunill, et al., paper. There is mention in the paper regarding the involvement of the T17 cells in the “vaccinated” person’s body in the IgG subclass switching. Yours Truly wrote about the importance of the T17 cells (also called Th17 cells or T17 Helper Cells), and the role of the N1-Methylpseudouridine in the modRNA COVID-19 “vaccines” in “turning off” these cells in the “vaccinated” person’s body (thus paving the way for continuous inflammation of many types) here: https://www.theqtree.com/2025/03/21/health-friday-3-21-2025-open-thread-more-on-the-n1-methylpseudouridine-in-the-modrna-covid-19-vaccines/.
However, there is another aspect of the situation discussed in the Monocunill, et al., paper that is of huge importance: The similarities between malaria, COVID-19 infection, and the class switch to IgG4 that the COVID-19 “vaccines” induce. Below is a screenshot from the Discussion section of the paper regarding this:
Yours Truly will now blow something out of the water regarding the FDA’s and the CDC’s official opposition to, and prohibition of, using Ivermectin or Hydroxychloroquine to prevent or to treat COVID-19 infection.
And, Hydroxycholoquine (and also Chloroquine) can be used to treat malariaAND COVID-19. Please see this paper from September 2020: https://pmc.ncbi.nlm.nih.gov/articles/PMC7476892/, “Chloroquine and hydroxychloroquine in the treatment of malaria and repurposing in treating COVID-19”, Zi-Ning Lei, et al. (USA and CCP), 8 September 2020.
In Yours Truly’s opinion, it is inconceivable that the NIH / NIAID / FDA / CDC did not know about the existence of these papers. Instead, by September 2020, these entities were hell-bent in pushing through the unproven modRNA “technology” for the Pfizer-BioNTech and the Moderna modRNA COVID-19 “vaccines” then in development. This meant that the FDA / CDC accepted the manipulated / incorrect “data” that were given to them from the truncated “clinical trials” for these “vaccines” by Pfizer-BioNTech and by Moderna. This meant that the FDA / CDC did not question the sudden “vaccine”-manufacturing switch from the original “Process 1” method to the “Process 2 method” that occurred in August 2020, that is still in use by both companies in the production of their respective “new formula” COVID-19 “vaccine booster shots”, and is based on “culturing” the modRNA of the said “vaccines” in a “bath” of E. coli.
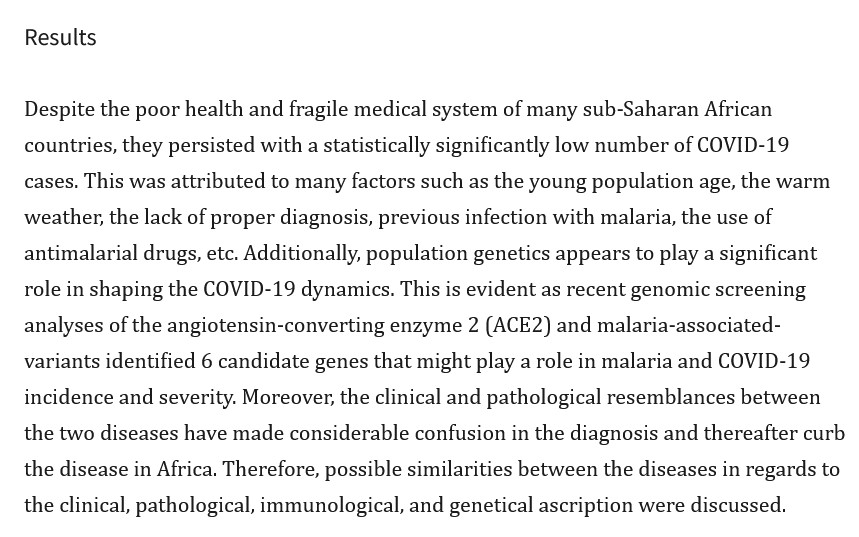
Further confirmation that malaria and COVID-19 infect the lungs in similar ways is here:https://pmc.ncbi.nlm.nih.gov/articles/PMC9445119/, “The striking mimics between COVID-19 and malaria: A review”, Emadeldin Hassan E Konozy, et al. A screenshot from this paper is below:
Note the mention of the ACE2 receptorsas regards malaria infection. These cells are also attacked by the COVID-19 virus itself (and, therefore, since they are based on the virus, so do the COVID-19 “vaccines” attack the ACE2 receptors of the “vaccinated” person’s body.)
In short: the FDA / CDC pushed, and continue to push, COVID-19 “vaccines” to “prevent” COVID-19 infections, while knowing that Ivermectin and Hydroxychloroquine also prevent — and treat — COVID-19 infections. Why is this still going on? How about ASKING BILL GATES. UNDER OATH.
This is aside from the fact that those who lab-created the bioweapon of the COVID-19 virus itself, and those who lab-created-and-enhanced the bioweapons of the COVID-19 “vaccines” — knew that malaria and COVID-19 would attack the lungs in similar ways. They knew what would “turn off” the T17 cells that are so important for the immune system and for Uridine in the human body. They knew what would damage or destroy the crucial IgG3 cells of the natural immune system of the human body, while fostering the increase of the IgG4 cells that allow illness and medical conditions to take hold and thrive. These things they incorporated into the creation of the COVID-19 virus itself, and into the creation of the COVID-19 “vaccines.”
The above free image of memoir writing is courtesy of iStock and Google Images.
Health Friday is a series devoted to information regarding Big Pharma, vaccines, general health, and associated topics. As today’s post speaks about the disaster of COVID-19 (the COVID-1 p9 virus itself, and the COVID-19 “vaccines”), Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created bioweapons.
There are Important Notifications from our host, Wolf Moon; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are found here. NOTE: Yours Truly has checked today’s offering for any AI-generated content. To the best of my knowledge and belief, there is none. Also: If readers wish to post anything in the discussion thread for today’s offering that is AI-generated, they must cite their source.
Today’s post is a COVID-19 Memoir, with this post as the inspiration: https://www.theburningplatform.com/2025/03/17/a-covid-contrarian-speaks-out-about-all-she-has-lost/, a guest post by Alex Berenson. This post describes the memoir statement of Jennifer Sey, who lost her job, her friends, family ties, and more, because she refused to bow to the demands of the organized psy-op that was the “command and control method” used over literally billions of human beings during the COVID-19 pandemic — and which organized psy-op is still being used today. Readers are welcome to post their own COVID-19 memoirs on today’s discussion thread, leaving out or referring to in an “oblique” manner, those details they wish to keep private.
Others on the board here have shared their COVID-19 Memoirs. Some of these postings have detailed dealing with an infection of the COVID-19 virus itself. Other postings have described the experiences of watching “vaccinated” family or friends becoming ill from the negative effects of the “vaccines” that they had taken. Still others have described their own issues after being “shed upon” by COVID-19 “vaccinated” persons. Sadly, our own Deplorable Patriot (Susie Sampson) passed away from the combined effects of the COVID-19 infection she very likely caught in November 2024 from a recently COVID-19-“boosted” choir member.
Yours Truly now adds her own COVID-19 Memoir. It began in December 2019, with the first media reports of a “mystery illness” that was infecting and killing people in Communist China, which “mystery illness” then making its way to the United States. This “illness” was variously called “Wuhan coronavirus”, “coronavirus”, or “novel coronavirus” (among other names), finally settling on the name “COVID-19” or “SARS-CoV-2” in early 2020. The issue became more “personal” in mid-February 2020, when Yours Truly contracted an illness that had all the hallmarks of an infection by the COVID-19 virus itself, most likely via exposure either at a restaurant in Chapel Hill, or at a local discount store in Durham. One was very sick for almost a month, subsisting on hot tea with honey and lemon, vitamins, scrambled eggs and toast, Tylenol(R), DayQuil(R), and guaifenesin cough syrup; after that, it was another month before the fatigue began to lift, the coughing to lessen and stop, and taste and smell to fully return. I was literally sequestered to my house for over six weeks. At the same time that I was sick, I was also taking care of my little Yorkie, Sona, who was entering the end stage of the kidney disease that resulted in his being put to sleep in my arms in mid-August of 2020.
It was during this period that I began to research about, read about, think about, and to eventually write about, this virus. My first decision was that I would never permit the deep-nasal probe PCR “test” to be administered to me. I began to order in groceries; to wear disposable gloves whenever I had to leave the house to do absolutely necessary things like getting gasoline for the car; to change clothes and bathe after I returned from being out of the house; and so on. Amazon became my source for many items. The United States went into “lockdown” on almost all aspects of the economy, and of life in general, by mid-March of 2020. The fear was palpable.
By the summer of 2020, there was speculation regarding the development and use of COVID-19 “vaccines.” There was speculation regarding the development and use of monoclonal antibody therapy for COVID-19 virus infected persons. Persons hospitalized for COVID-19 infection were being put on Remdesivir and ventilators, killing many. Antigen tests to determine whether or not a person had been infected with the COVID-19 virus were being used by September 2020. Then, the Pfizer-BioNTech and the Moderna modRNA COVID-19 “vaccines” were granted their initial Emergency Use Authorizations for use in the United States on 11 December 2020. Starting in January 2021, all of the members of my family, with the exception of Yours Truly, were getting COVID-19 “vaccinated”; in many cases, this was “mandated” or “required” in order for them to keep their jobs, for travel, and so on. In the spring of 2021, I began to shift much of my focus to researching about the COVID-19 “vaccines” — and came to the conclusion that a “vaccine” that had been developed and put on the market as quickly as these products were, was likely not a good thing. I made a decision to never allow myself to be COVID-19 “vaccinated.” This was the beginning of strained relationships with “vaccinated” family and friends, once Yours Truly informed them that these “vaccines” were not for her. I contacted a physician through AFLDS (America’s Frontline Doctors), and started taking prescribed Hydroxychloroquine and Zinc. Afterwards, I contacted the then-FLCCC Alliance (now the Independent Medical Alliance) and began taking prescribed Ivermectin. Yours Truly is still not COVID-19 “vaccinated.”
It is now, in March 2025, five years from the first COVID-19 “lockdowns.” Yours Truly lost a cousin in September 2023 due to the negative effects of the COVID-19 “vaccines” he had taken. Yours Truly lost her brother in October 2024 due to the negative effects of the COVID-19 “vaccines” he had taken. Yours Truly is now concerned about the other “vaccinated” members of her family. She had tried to warn some of them, based on my research, of the dangers and uncertainties of these bioweapon toxin injections, but was met with “We follow the science” or “I trust my doctor.” I hope the ongoing strained relationships between certain “vaccinated” family members and Yours Truly will heal. I have made certain decisions regarding how I interact with people and situations outside the family circle when encountering them in public places.
Life as it was before November 2019 will never be the same. COVID-19 is the perfect example of an “equal-opportunity” bioweapon. The COVID-19 virus itself, if a person is infected with it, can have lingering, or even permanent, issues that remain after the person recovers. The COVID-19 “vaccines”, since they contain the virus, plus “enhancements” such as N1-Methylpseudouridine, permanently and negatively affect “vaccinated” persons throughout the body, including the brain. “Long COVID”, resulting either from an infection of the COVID-19 virus itself, or from being COVID-19 “vaccinated”, is now recognized medical condition. There is also the emerging issue of COVID-19 “vaccine shedding” from “vaccinated” persons onto other persons, including onto the non-“vaccinated.”
Those adults who are not COVID-19 “vaccinated” (the percentage of people in this category is anywhere between 15% – 25% of the entire population of the Earth) have, in a sense, “defeated COVID-19” — even if they contracted an infection of the virus and recovered. This has nothing to do with the “Joe X is not COVID-19 “vaccinated”, so he is a pureblood” depiction; or with the “Joe X is not COVID-19 “vaccinated”, so he is somehow morally superior to those who are “vaccinated”” allegation — this has everything to do with personal decision making. Those adults who are not COVID-19 “vaccinated” have resisted the gaslighting, the “mandates” and the “recommendations” to get COVID-19 “vaccinated”; the urging from “vaccinated” family and friends; the loss of employment, of schooling, of opportunities, of relationships. They have grieved and mourned for “vaccinated” family members and/or friends who have passed away from the negative effects of the COVID-19 “vaccines” that they had taken. They have, in many instances, done their own research into the “vaccines” and vowed never to take them. They have, in many instances, decided to never allow their children to be COVID-19 “vaccinated.” They have learned that “safe and effective”, as applied to these bioweapon toxin injections, was — and is — a lie. They are stronger than they knew. They are stronger than they know. They will need this strength in the future.
Yours Truly believes that, in order for society to heal from the COVID-19 disaster, to have trust in the medical profession, to have trust in the government, the perpetrators of the COVID-19 disaster must be brought to justice; and that the unsafe, ineffective, dangerous and deadly COVID-19 “vaccines” must be withdrawn from the market worldwide. The “establishment medicine” entities (the American Medical Association; the American Academy of Pediatrics; the American College of Obstetricians and Gynecologists; and many more); the government agencies (the CDC; the FDA; the Department of Health and Human Services; and many more) — who are still “recommending” these injectables, who still have them on the Immunization Schedules — must stop these activities. All mRNA-based “vaccine” funding and development must be stopped until the entire issue of the safety and efficiency of these injectables is thoroughly investigated and analyzed. Medical freedom of choice must be returned to the general public — for example, Ivermectin and Hydroxychloroquine must be made readily available at a low cost. Physicians must be permitted to prescribe these safe and effective prophylactic / treatment drugs for COVID-19 infection without fear of being “disciplined” or “restricted” by the their state medical licensing board; let along having their License to Practice Medicine revoked. Hospitalized COVID-19 patients mustbe allowed freedom of choice to be treated inpatient with Ivermectin or Hydroxychloroquine, Vitamin D, and other effective treatments that are, even now, being denied because the FDA does not “authorize” or “approve” them.
There are many persons who must be held accountable for their actions during the entire COVID-19 disaster. Among them:The first person, in Yours Truly’s opinion, who must be held accountable for his actions during the entire COVID-19 disaster is Dr. Anthony Fauci. Now in “retirement”, he commands $100,000 per “motivational talk”, like the one he is scheduled to give on 14 April in Sarasota, Florida. Please see: https://rescue.substack.com/p/serious-questions-for-fauci, by Matt Walsh, 23 March 2025.
The next two persons, in Yours Truly’s opinion, who must be held accountable for their actions during the entire COVID-19 disaster are: Dr. Francis Collins (Dr. Fauci’s superior at the NIH; now retired); and, Peter Daszak, PhD, of EcoHealth Alliance (funneling Gain-of-Function funds to the Wuhan Institute of Virology, among other research facilities, for the lab-creation of the COVID-19 virus, and coordinating the “official” government communications to the media; Dr. Daszak has recently been fired from EcoHealth Alliance. )
The above image of a vintage Rolodex is courtesy of CSA Images via Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s post speaks to the disaster of COVID-19 (the COVID-19 virus itself, and the COVID-19 “vaccines”), Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created bioweapons.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here.
And now, Part Two of the COVID-19 Information File:
BOOKS: One: Cancer Care, Second Edition. By Dr. Paul E. Marik, MD, FCCM, FCCP (Dr. Marik is a co-founder of the FLCCC Alliance). This book is found on https://www.amazon.com/.
Two: The Doctors Book of Home Remedies, by the editors of Prevention Health Magazine Books, 1990 edition. This book is available online as used copies.
WEBSITE NAME CHANGES:
The FLCCC Alliance (formerly https://covid19criticalcare.com, also called FLCCC Alliance) is now Independent Medical Alliance: https://imahealth.org/.
COVID-19 VIRUS and COVID-19 “VACCINES” DETOX / MITIGATION PROTOCOLS:
https://imahealth.org/ (Independent Medical Alliance, formerly FLCCC); https://americasfrontlinedoctors.org/ (AFLDS); https://www.mercola.com/ (Dr. Joseph Mercola, MD; must sign up to access); https://www.americaoutloud.com/ (Dr. Peter McCullough, MD’s, Wellness Company site.) Note: this is not an exhaustive list, and does not include herbal medicine, naturopathic medicine, homeopathic medicine, Ayurvedic medicine, Traditional Chinese Medicine, or other allopathic / osteopathic websites.
THE YALE “LISTEN” STUDY PAPER:
Yours Truly has written on the main discussion thread several times regarding this groundbreaking paper (the “Iwasaki et al. paper”) about COVID-19 “vaccine”-induced injuries presenting as long as 709 days after “vaccination.” Here is Steve Kirsch’s take on the paper: https://kirschsubstack.com/p/covid-vaccine-injury-study-published, “COVID vaccine injury study published on preprint server because the mainstream medical journals refused to publish it”, 19 February 2025. HOWEVER, Yours Truly has found that the original preprint paper has already been reissued in a “new” preprint version. The original version is found here: https://www.medrxiv.org/content/10.1101/2025.02.18.25322379v1, “Immunological and Antigenic Signatures Associated with Chronic Illnesses after COVID-19 Vaccination”, Akiko Iwasaki, et al., dated 18 February 2025. The “new” preprint version is found here: https://www.medrxiv.org/content/10.1101/2025.02.18.25322379v2.full, same title, Akiko Iwasaki, et al., dated 25 February 2025. Meanwhile, Dr. Pierre Kory, MD, has written a blog post regarding how the LISTEN study may be used as legal support for persons with COVID-19 “vaccine”-induced issues in lawsuits: https://pierrekorymedicalmusings.com/p/new-study-provides-legal-support, “New Study Provides Legal Support For The Vaccine Injured”, 21 February 2025. Dr. Kory has coined the term, “Post Covid Vaccination Syndrome”, or PVS, to describe the conditions and issues that COVID-19 “vaccinated” patients in his practice present.
MORE INFORMATION ON HOW THE COVID-19 “VACCINES” INCREASE THE IgG4 “TOLERATE BUT NEVER CLEAR” IMMUNE SYSTEM CELLS IN THE “VACCINATED” PERSON’S BODY:
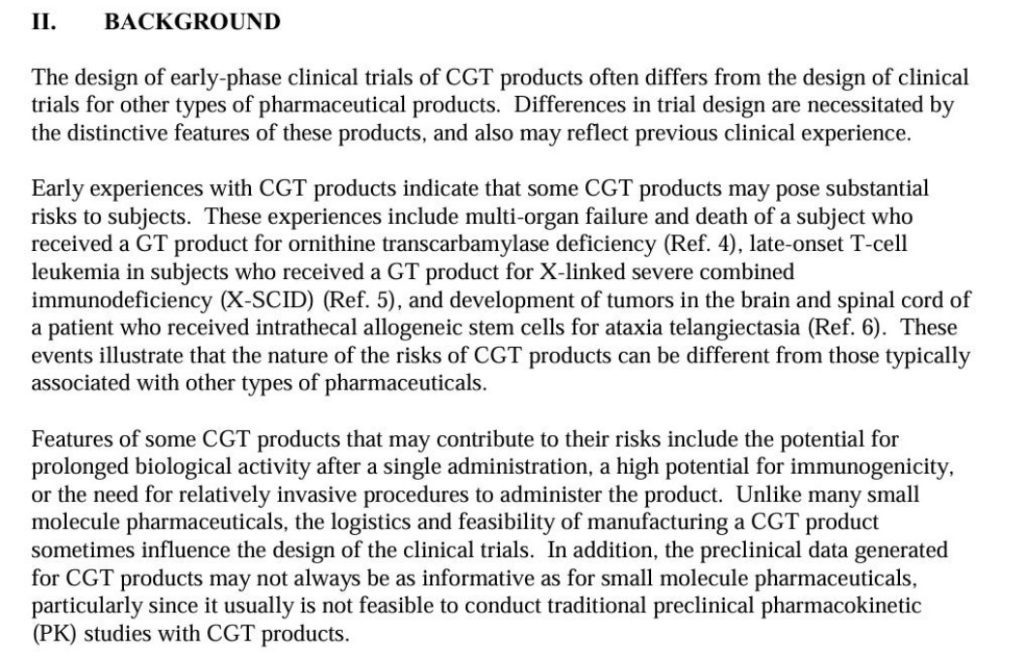
The following screenshot is from the 2015 FDA guidance document on gene therapies:
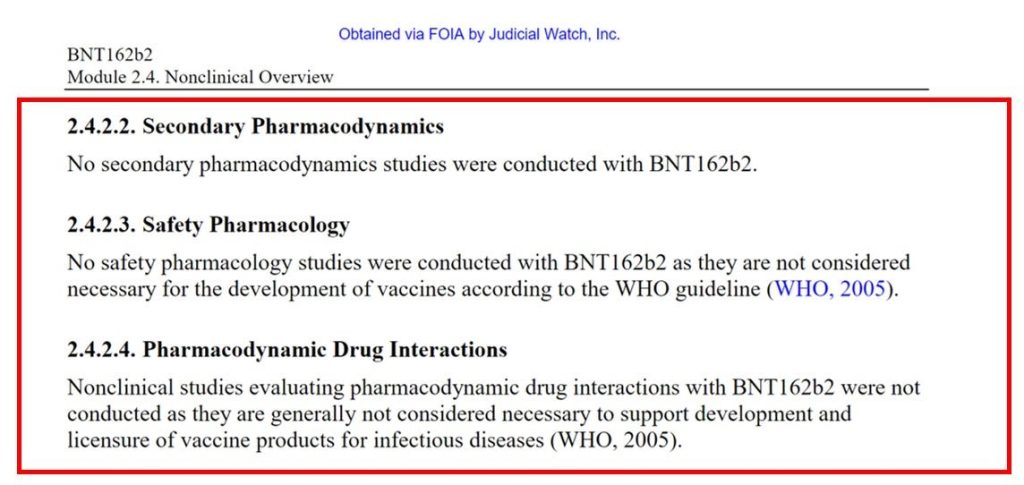
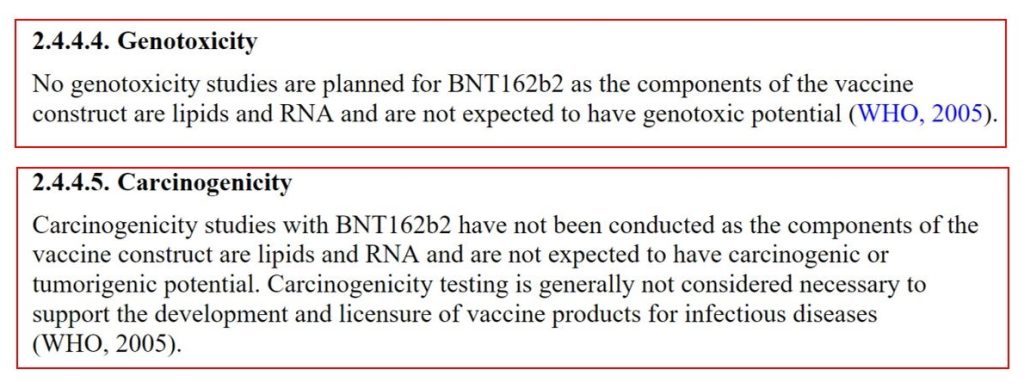
The following screenshots are via FOIA information that Judicial Watch sued the FDA for and won regarding the Pfizer-BioNTech “flagship” modRNA COVID-19 “vaccine”, BNT162b2:
COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”) AND ORAL COVID-19 “VACCINE” NEWS:
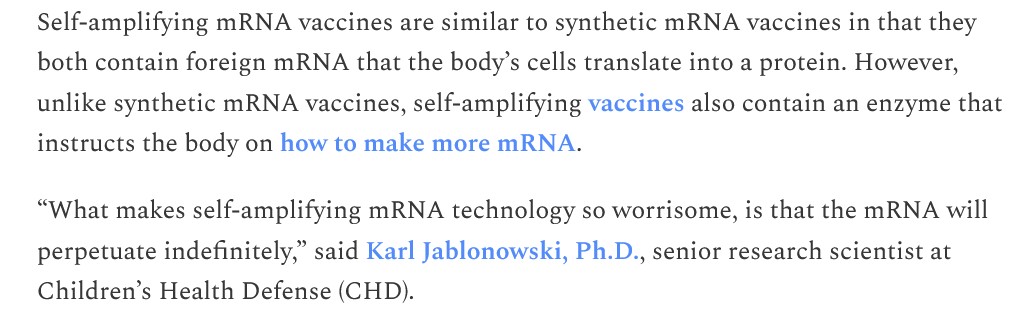
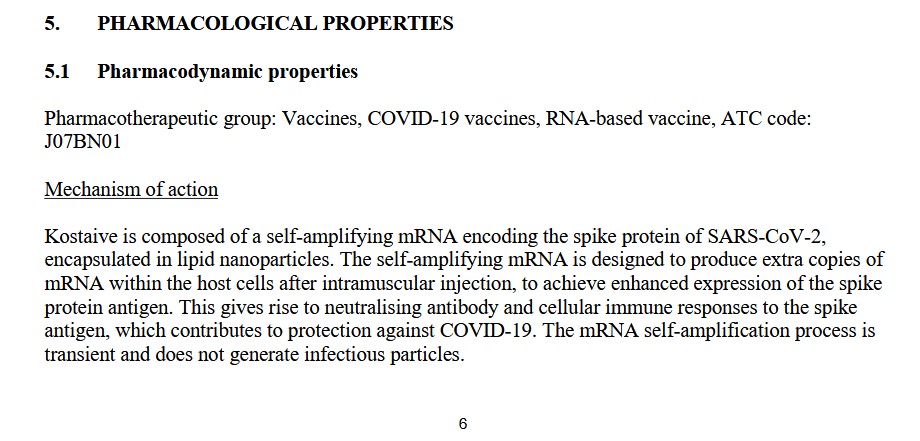
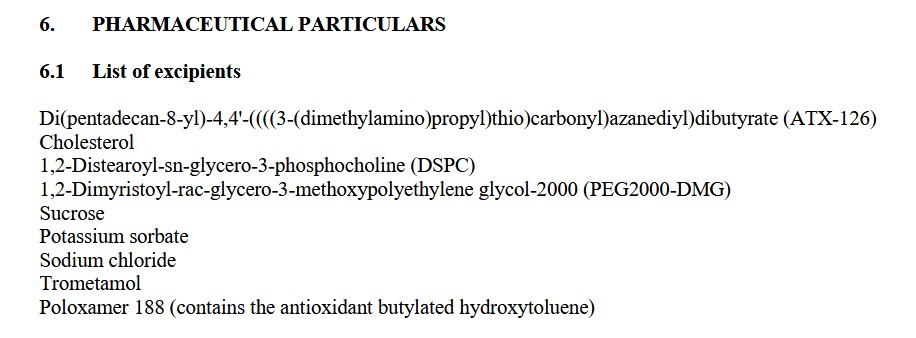
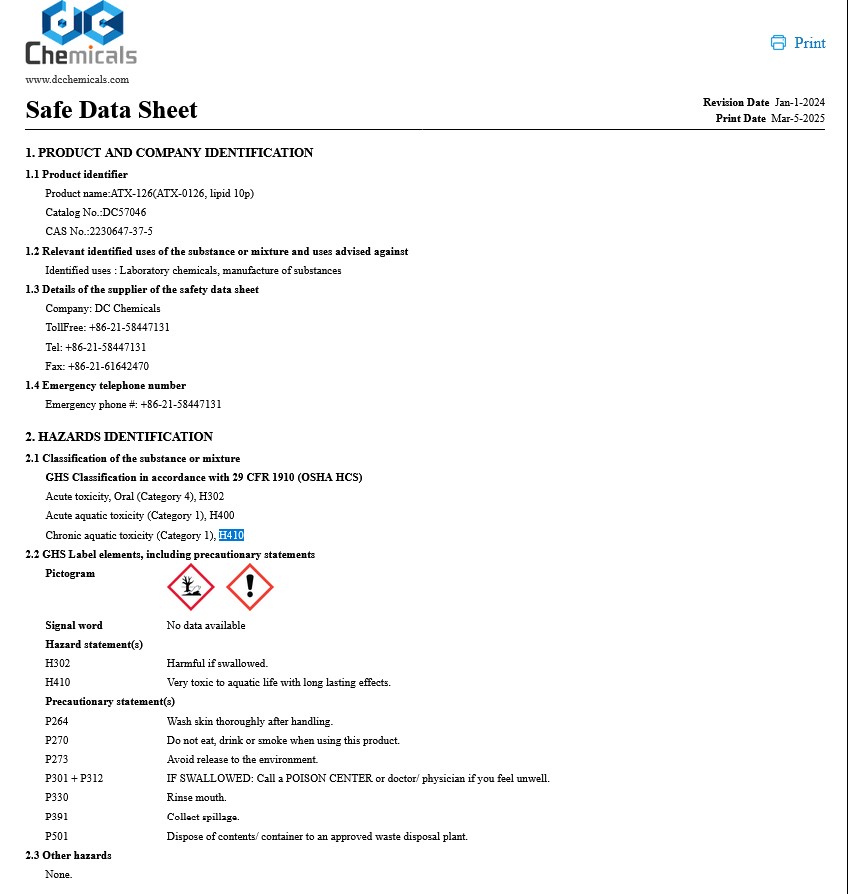
One: The European Commission has just approved the use of the self-amplifying RNA (saRNA) COVID-19 “vaccine”, KOSTAIVE, for use in the European Union / Scandinavia. Please see: https://defender.substack.com/p/europe-approval-self-amplifying-covid-mrna-vaccine-no-long-term-safety-data, “Inhumane, Reckless: Critics Weigh in on Europe’s Approval of Self-Amplifying COVID mRNA Vaccines”, by Suzanne Burdick, PhD, 23 February 2025. KOSTAIVE is the brand name of the injectable called ARCT-154, by Arcturus Therapeutics. This product was approved in Japan in November 2024 and is in use there. Below are two screenshots from the Defender article:
Please re-read the sentence above from Dr. Jablonowski regarding how an saRNA COVID-19 “vaccine” is “like being vaccinated every day for the rest of your life.” (Italics mine)
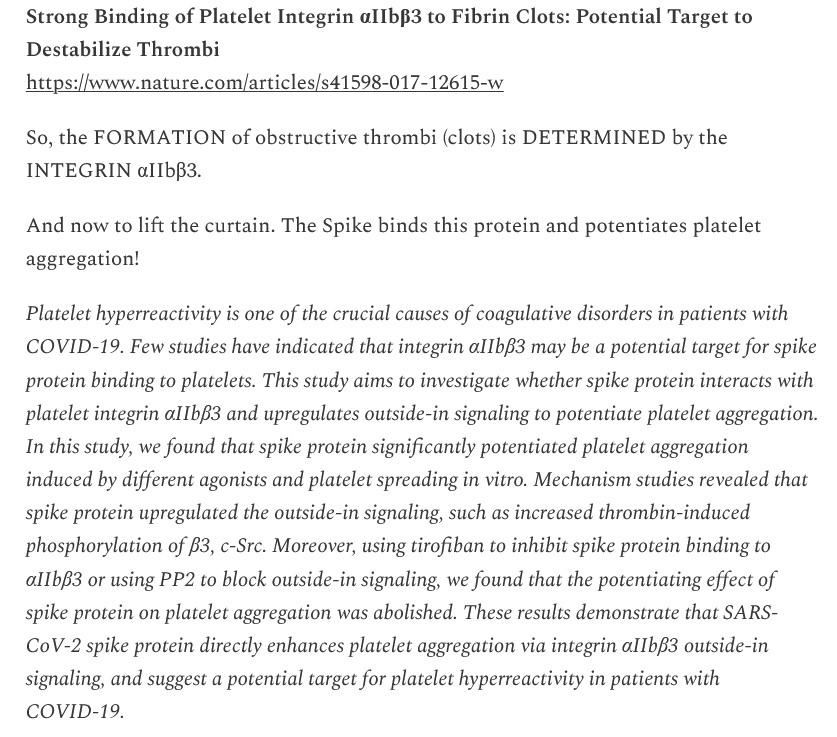
One of the blogs that Yours Truly reads regularly is that of Walter M Chesnut: https://wmcresearch.substack.com/. Mr. Chesnut has been performing solid research into the mechanisms of the spike protein of the SARS-CoV-2 (COVID-19) virus itself for over 3 years. While it is not known for absolute certainty the actual ingredients of the lab-created bioweapon called the SARS-CoV-2 virus, Mr. Chesnut continues to find possible pieces of this puzzle. Here are two recent such blog articles of his. The first: https://wmcresearch.substack.com/p/turbocancers-a-secondary-manifestation, “Turbocancers: A Secondary Manifestation of the Extracellular Matrix (ECM)?” The second: https://wmcresearch.substack.com/p/the-spike-protein-and-iib3-understanding, “The Spike Protein and [alpha]IIb[beta]3: Understanding the Fibrous Clots from an Integrin-Mediated Perspective”, 24 February 2025. A screenshot from this article is below:
The point here is that the COVID-19 virus itself it NOT “just another virus.” It is a lab-created bioweapon that, in and of itself, can damage the infected person’s body. Combined with the “enhanced” ingredients found in the COVID-19 “vaccines” (lipid nanoparticles and N1-methylpseudouridine), this “foundational” bioweapon virus becomes extremely dangerous or even deadly. (NOTE: Yours Truly apologizes for the [alpha] and the [beta] in the title of the Chesnut article cited above. She is still in the WP “learning curve.”)
FLASH! UPDATE 6 MARCH: REGARDING THE “DISCOVERY” OF THE “NEW” BAT CORONAVIRUS, HKU5-CoV-2:
This “new” bat coronavirus was supposedly “discovered” by the Wuhan Institute of Virology. The first question this raises is: How many OTHER bat (or other) coronaviruses are in the “storage vaults” of the WIV to be “discovered” at some point? There is speculation all over the internet regarding HKU5-CoV-2 and if / when, it could infect humans. This “new” coronavirus apparently can use the same types of entry methods into the human body that SARS-CoV-2 and MERS do.
Two: But wait, there’s more! Another question is raised: What did / does, Pfizer-BioNTech know about HKU5-CoV-2? Because this company has been Phase 1 testing an “experimental” modRNA “Pandemic Influenza vaccine” since December 2023. The study is NCT06179446 (https://clinicaltrials.gov/study/NCT06179446), begun on 13 December 2023 and scheduled to finish the Phase 1 clinical trial on 26 August 2025. This “experimental” modRNA prophylactic “Pandemic Influenza vaccine” is called pdmFlu. The Pfizer-BioNTech product identifier number is PF-07985819, and the Study Identifier number is C5561001. According to the “Researcher View” of the Clinical Trials entry, as many as eight different formulas and/or dosage amounts will be given to the study participants (there are 160 registered study participants.) NCT06179446 has two separate “control groups”: One “control group” will receive injections of a “licensed influenza vaccine”; the other “control group” will receive a placebo.
WHAT DID / DOES, PFIZER-BIONTECH KNOW ABOUT HKU5-CoV-2?
Three: And, by the way — RALPH BARIC has been experimenting with HKU5-CoV-2 SINCE AT LEAST 2014, funded by the NIH. One of his papers is here: https://pmc.ncbi.nlm.nih.gov.articles/PMC7022341/, “Trypsin Treatment Unlocks Barrier for Zoonotic Bat Coronavirus Infection”, Ralph S. Baric, et al., 14 February 2020.
WHAT DOES / DID RALPH BARIC KNOW ABOUT HKU5-CoV-2?
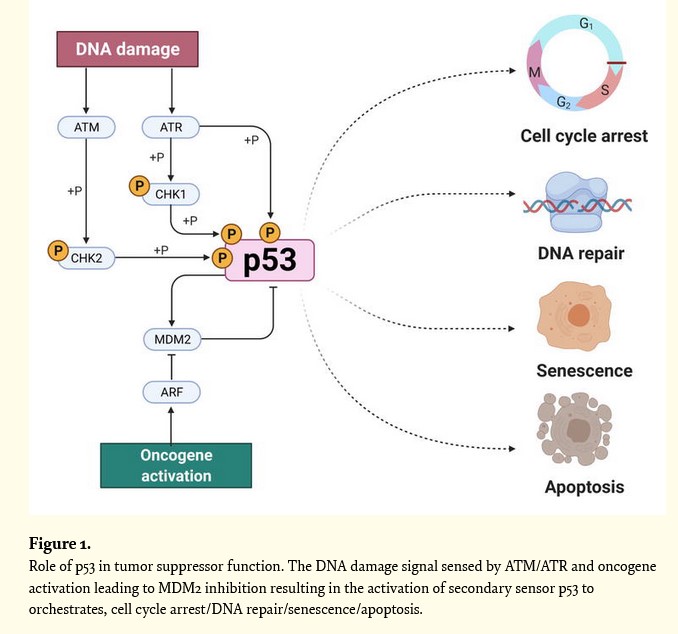
The above graphic is courtesy of the Farooq, et al., 2022 paper on the functions of the p53 protein in the human body. The paper is found here: https://doi.org/10.5772/intechopen.105029, “p53 Tumor Suppressor: Functional Regulation and Role in Gene Therapy”, Zeenat Farooq, et al., 1 August 2022.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. Since today’s offering is related to the disaster of COVID-19, Yours Truly dedicates it to all persons, of whatever age or location, who have suffered COVID-19 “vaccine”-induced injuries, illnesses, disabilities, or have passed away from, the negative effects of these injectables that they had put into their bodies. However, the discussion is not limited to what is presented today; It is an Open Thread.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
Readers may recall that Yours Truly posted regarding her discovery of the death of a former opera singer with whom she worked, who will be called “D.M.” D.M., as a professional operatic bass-baritone, had an international career, in which one of his “signature roles” was that of Horace Tabor in the Douglas Moore opera, The Ballad of Baby Doe. He had an enormous voice with an unusual “upward extension” that could cover dramatic tenor repertoire. In fact, D.M. was commuting to New York City to study with a voice instructor at the Mannes School of Music to become a Heldentenor (Wagnerian tenor.) However, D.M. eventually left opera performing and taught voice for some years; he then worked as an insurance sales professional. He had had successful MOHS surgery to remove a basal cell carcinoma over a decade ago. There is no doubt in Yours Truly’s mind that D.M. took the COVID-19 “vaccines” in order to keep his job in insurance. In early 2022, he was diagnosed with colon cancer. He passed away in January 2024. I do know that D.M. had at least one potential co-morbidity: he was tall and very big, built almost like a Sumo wrestler, with an extra-large ribcage (this type of body build is important for being a Heldentenor.) May he rest in eternal Peace.
And this is where the p53 protein of the human body comes in.
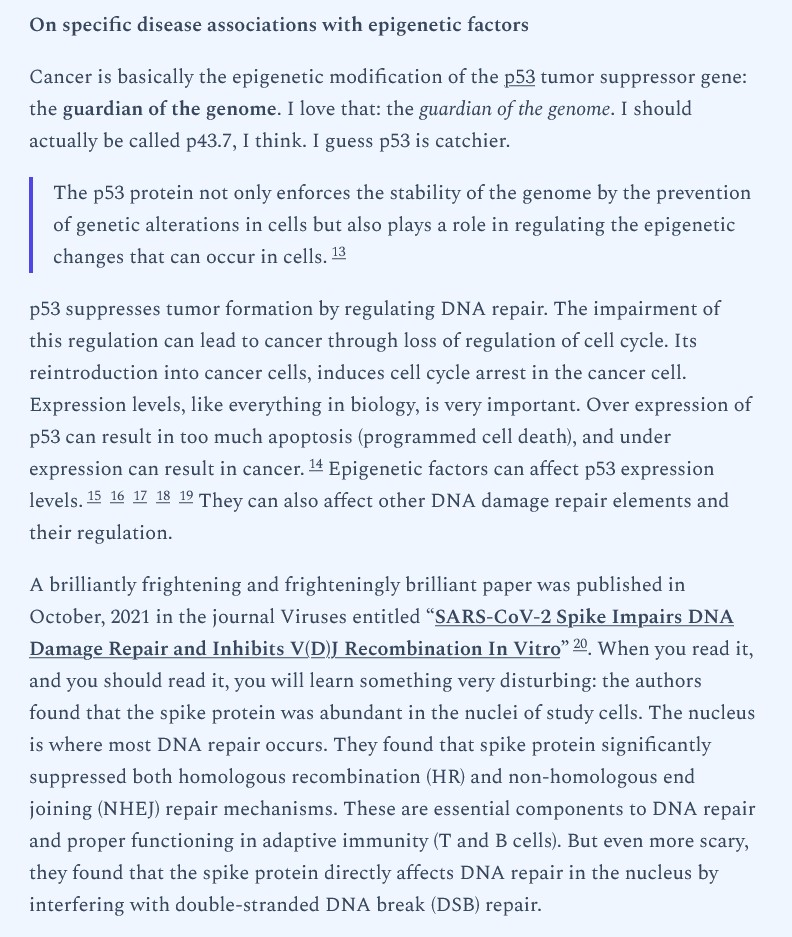
And, yes, this paper was ordered to be Retracted. It is still available to be read, but the word “RETRACTED” is on every page: https://www.mdpi.com/1999-4915/13/10/2056.
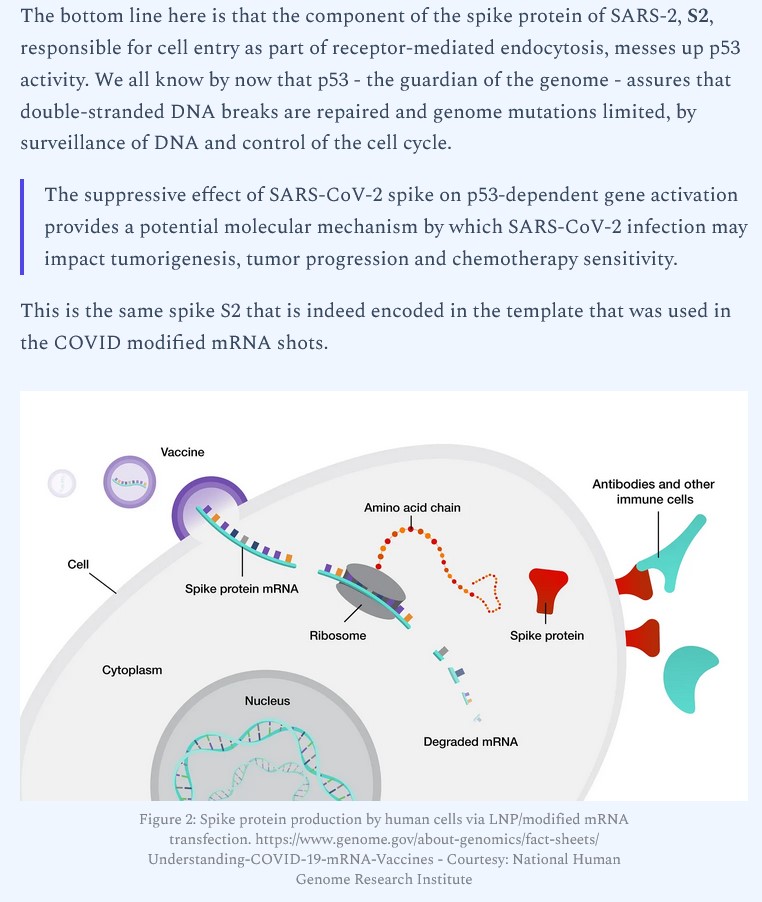
Yours Truly turns to another blog post by Dr. Rose: https://jessicar.substack.com/p/s2-of-spike-protein-buggers-up-p53, 16 April 2024. Dr. Rose discusses the “El-Deiry” paper regarding what the S2 protein of the SARS-CoV-2 virus (the COVID-19 virus; this protein is also in the COVID-19 “vaccines”) does to interfere with the p53 protein in the “vaccinated” person’s body. The paper is found here: https://doi.org/10.1101/2024.12.589252, “SARS-CoV-2 spike S2 subunit inhibits p53 activation of p21(WAF1), TRAIL Death Receptor DR5 and MDM2 proteins in cancer cells”, Wafik El-Deiry, et al., 15 April 2024. Below is a screenshot from this paper:
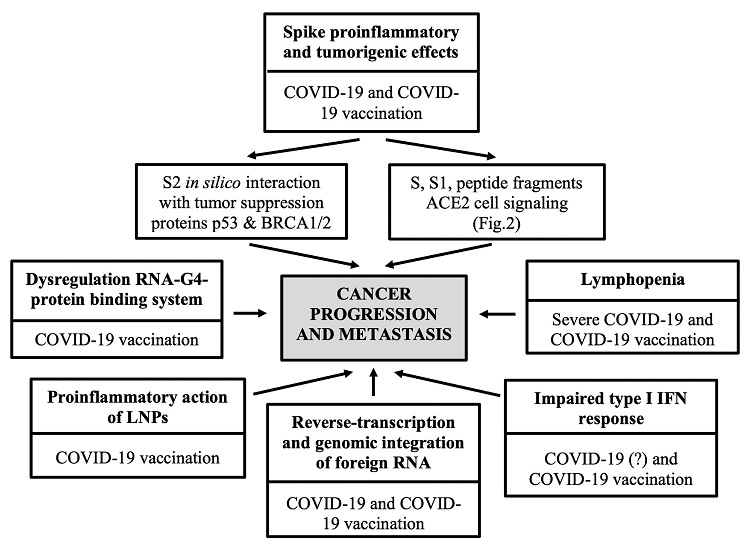
Yours Truly will again reference the “Angues and Bustos” paper regarding cancer genesis from both the COVID-19 virus itself, and from the COVID-19 “vaccines” (which contain the virus’ spike protein and other “enhancements”): https://doi.org/10/7759/cureus.50703, “SARS-CoV-2 Vaccination and the Multi-Hit Hypothesis of Oncogenesis”, R.V. Angues, Y.P. Bustos, 17 December 2023. Below is the salient Figure 1 from the paper:
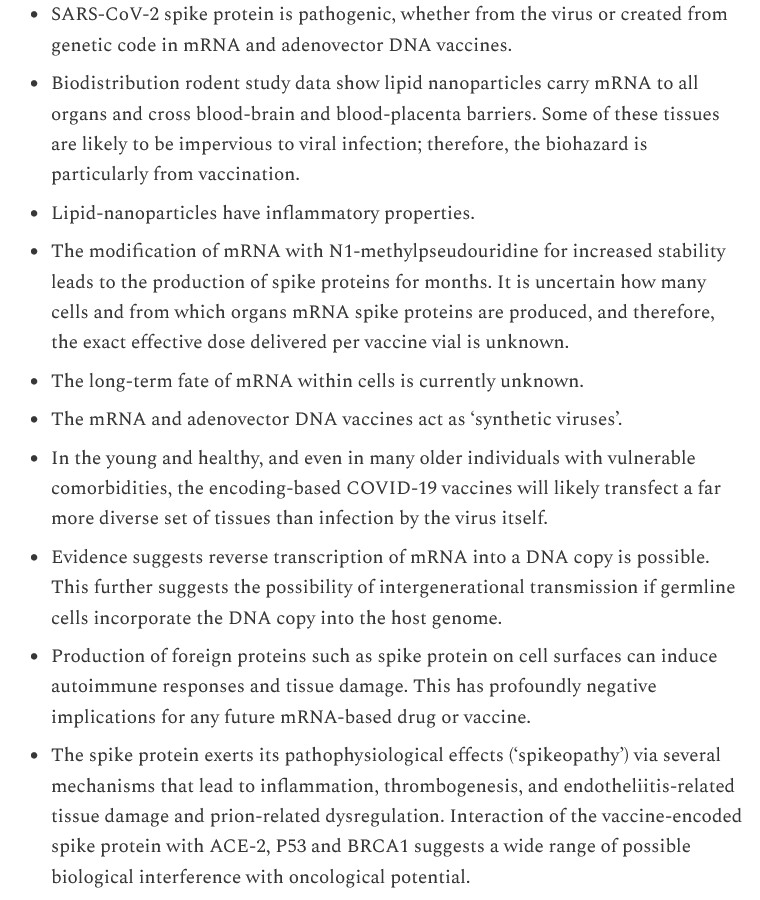
Another discussion of how the spike protein from the COVID-19 virus itself, and the COVID-19 “vaccines”, induce negative effects in the body of the “vaccinated” person: https://www.thefocalpoints.com/p/spikeopathy-covid-19-spike-protein, “Spikeopathy: COVID-19 Spike Protein Is Pathogenic from Both Virus and Vaccine mRNA”, Peter A. McCullough, MD, 25 October 2023. Below is a screenshot of some of the topics discussed in the paper:
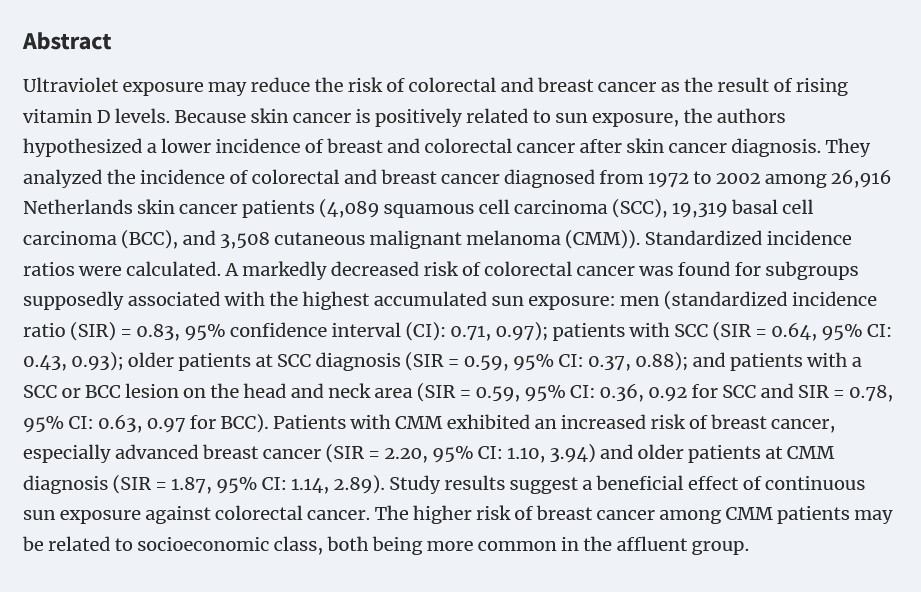
Back to the situation regarding D.M.: There is evidence that skin cancer treatment can actually reduce the risk of colon cancer. Please see: https://doi.org/10.1038/sj.bjc.6604842, “Second primary cancers in patients with skin cancer: a population-based study in Northern Ireland”, MM Cantwell, et al., 6 January 2009. The Cantwell, et al., paper has a reference to a 2008 scientific article on the reduction of colon cancer risk in patients who were treated for basal cell cancer. Please see: https://doi.org/10.1093/aje/kwn077, “Are patients with skin cancer at lower risk of developing colorectal or breast cancer?”, E. de Vries, et al., 15 June 2008. The Abstract from this paper is below:
Note the importance of Vitamin D from sun exposure in the lowering of risk. In Yours Truly’s opinion, as it is not always possible to have sun exposure on a daily basis to obtain Vitamin D, judicious supplementation of Vitamin D may help to “fill in the gap.” (NOTE: the link to the de Vries paper may, or may not, work: however, interested readers can access this paper via the in-line hyperlink reference to the same in the Cantwell paper.)
Yours Truly is not an “armchair Coroner”, nor does she “play one on TV.” On the other hand, I got to know D.M. fairly well in working with him as accompanist/coach; I very strongly suspect that he was “mandated” to take the COVID-19 “vaccines” in order to keep his insurance job; and I know a fair amount about the negative effects of these Bioweapon Toxin Injections. My personal opinion is that the successfully-treated basal cell cancer that D.M. had years ago was “re-established” as colon cancer after he took the COVID-19 “vaccines.”
Regarding support for the p53 protein, the most potent food source is from Cruciferous vegetables. Please see: https://doi.org/10.3389/fnut.2022.951935, “Cruciferous vegetables as a treasure of functional foods bioactive compounds: Targeting p53 family in gastrointestinal tract and associated cancers”, Saikat Mitra, et al., 3 August 2022. A partial list from this paper of Cruciferous vegetables: cabbages; broccoli; Brussels sprouts; kale; cauliflower; and, turnips.
How many other successfully-treated and/or in remission cancers among COVID-19 “vaccinated” people have been “re-established” as new cancers, or brought out of remission as “aggravated” forms of the original cancers?
The above vintage image of vaccine vials and vaccine syringes is courtesy of Shutterstock and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As today’s post speaks to the disaster of the COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”), Yours Truly dedicates it to the memory of all persons, or whatever age or location, who have passed away from the negative effects (direct or indirect) of the the COVID-19 “vaccines”, no matter whether the deceased were COVID-19 “vaccinated” or not.
A special note for today’s post: Of your charity, please pray for the repose of the soul of our good DePat (Deplorable Patriot), Susan P. Sampson. Her Funeral Mass is to be held tomorrow, Saturday 8 February, at the St. Roch Roman Catholic Church in St. Louis, Missouri, at 10AM Central Standard Time. Of your charity, please pray for the repose of the soul of Yours Truly’s “fully vaccinated and boosted” brother, Sam. His Memorial Service is to be held tomorrow, Saturday 8 February, at the Peeples Valley Baptist Church in Cartersville, Georgia, at 2PM Eastern Standard Time. Thank you.
Requiem aeterna dona eis, Domine; et Lux Perpetua luceat eis. Requiescant in pace. Amen.
However, the discussion is not limited to what is presented today: It is an Open Thread.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
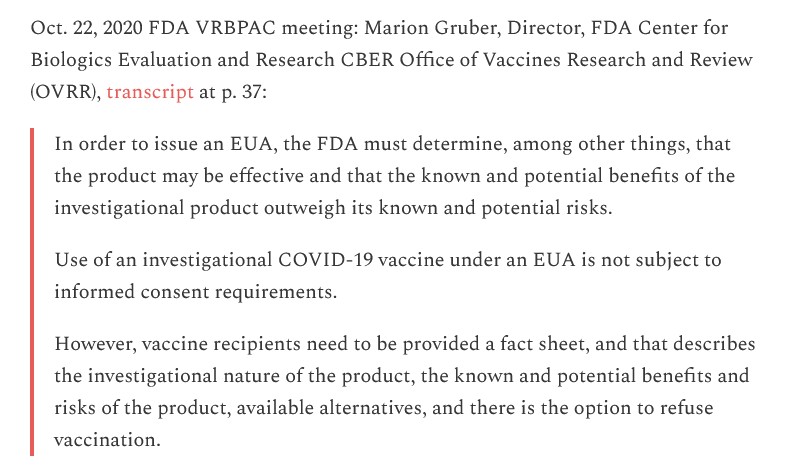
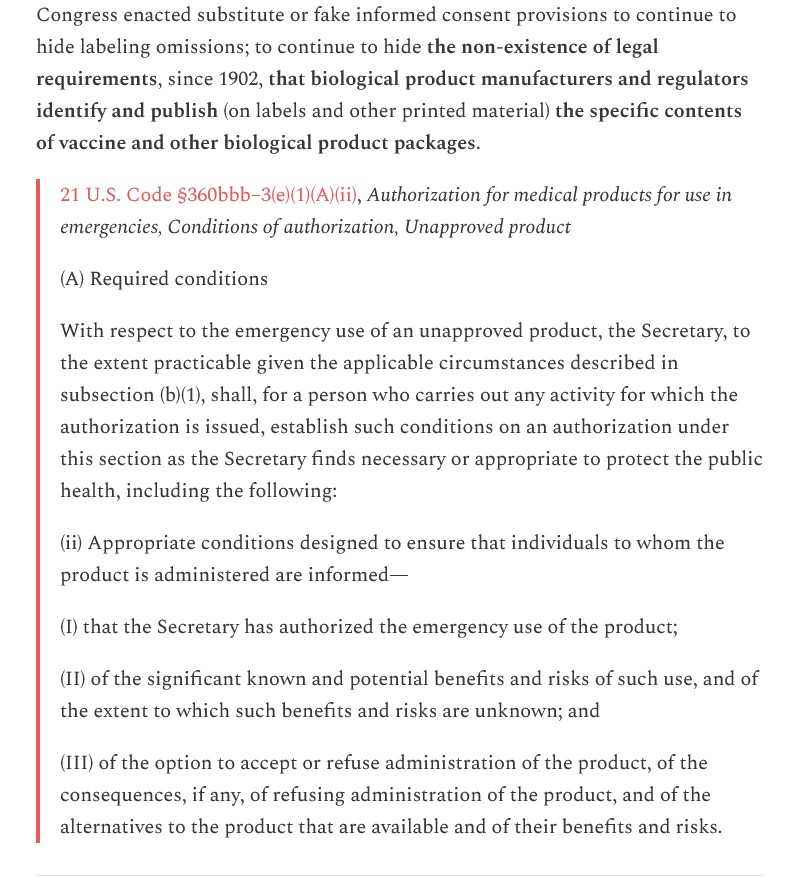
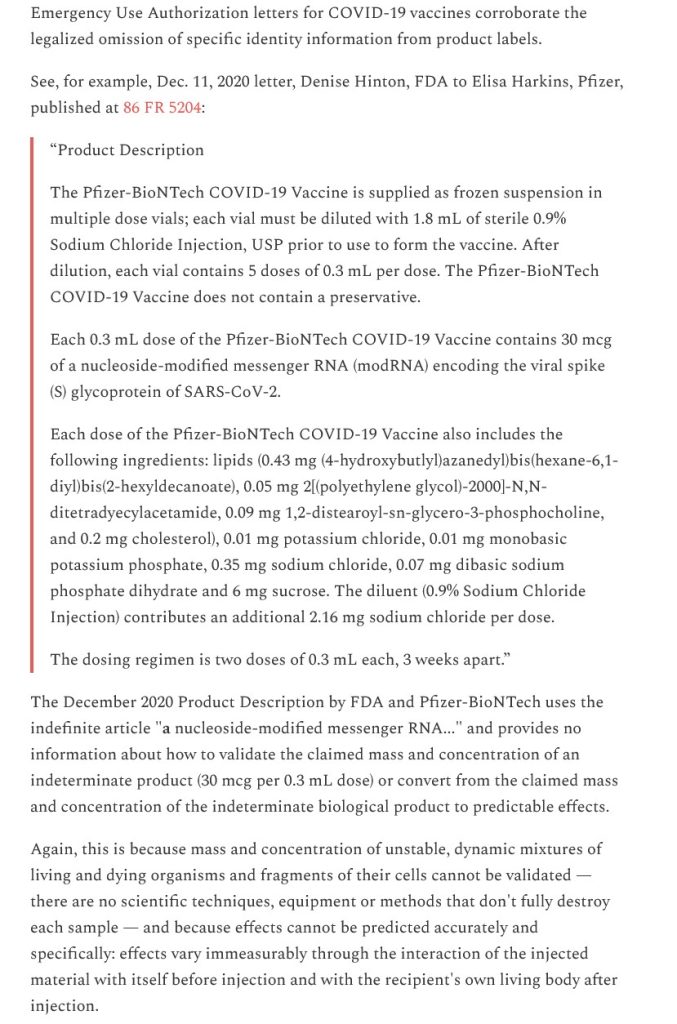
Today’s post begins here: https://bailiwicknews.substack.com/p/labeling-deceits-and-omissions-and, “Labeling deceits and omissions, and fake informed consent for vaccines and other legalized biological and chemical weapons.”, by Katherine Watt, 29 January 2025. In this post, Ms. Watt describes the lack of transparency and honesty in several areas of these topics, among them: One, in the labeling of the modRNA COVID-19 “vaccines”; and, Two, in the lack of detailed informed consent documents for people who want to take (or are “mandated” to take) injections of the COVID-19 modRNA “vaccines.” Ms. Watt traces this trail of lies and deceit back at least 1902. Below are some screenshots from her article related to the COVID-19 “vaccines”:
Ms. Watt makes it clear that “our betters” do NOT want the people who took / who continue to take, the COVID-19 “vaccines” to really know what is in the “modRNA” of the injections.
There is another issue regarding the lack of true informed consent regarding the COVID-19 “vaccines” — the fact that the FDA has made it virtually impossible for COVID-19 “vaccinated” people who become “vaccine”-injured, acquire an illness after being “vaccinated”, or even die from the negative effects of these bioweapon injectables, to be able to sue the “vaccines” manufacturers, those who administer these “vaccines”, entities who “require” or “mandate” the taking of these ‘vaccines”, or agencies of the Federal government who push these “vaccines.” The FDA has done this by making BOTH the Emergency Use Authorization AND “full approval” applicable to the COVID-19 “vaccines” in use, thereby “insulating” the above entities and persons from liability.
The FDA approved the use of COMIRNATY (Pfizer-BioNTech) in people OVER 11 YEARS OF AGE. The FDA also authorized the use of “Pfizer-BioNTech COVID-19 Vaccine (2024-2025 Formula” to be used in people FROM 6 MONTHS THROUGH 11 YEARS OF AGE. Also — notice that the COMIRNATY approval was granted to the GERMAN partner of PfizerUSA (BioNTech Manufacturing GmbH); and that the “Pfizer-BioNTech COVID-19 Vaccine (2024-2025 Formula” authorization was granted to Pfizer Inc.
But wait, there’s more! Under the “magic” of legalese and bureaucratic obfuscation, here are the links to the websites that the FDA and Xavier Becerra (then-head of HHS) used to perform the “sleight of hand” to grant EXEMPTION FROM LIABILITY to the makers of the “2024-2025 Formula COVID-19 Vaccines” for BOTH the “approved” AND the “authorized” formulations of these injectables. It’s all under the PREP Act:
Regarding a current “Informed Consent” document for the general public, Yours Truly found the following from a search that began here: https://www.cdc.gov/vaccines/hcp/vis/index.html, which eventually (via being “redirected” from other CDC websites that are now shut down with the “The page you are looking for doesn’t exist”-type error messages) led to this: https://www.cdc.gov/vaccines/hcp/current-vis/covid-19.htmlCDC_AAref_Val=https://www.cdc.gov/vaccines/hcp/vis/vis-statements/covid-19.html. It turns out that the “Informed Consent” handouts for patients / caregivers appear to be basically a “Pablum” version of government and/or “vaccine” manufacturer misinformation, disinformation, and downright lies, about the COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”) that the patient is going to have injected into their body (or that parents / guardians are going to have injected into the body of a minor child.)
Let’s look at some screenshots of this FDA-issued Fact Sheet for recipients and caregivers for the EUA-granted “Pfizer-BioNTech 2024-2025 Formula COVID-19 Vaccine” for children 6 months of age to 11 years of age, as an example. The FDA document is found here: https://www.fda.gov/media/167212/download.
The COVID-19 “vaccines” do not “prevent” an infection of COVID-19. In fact, COVID-19 “vaccinated” persons have a much higher chance of coming down with COVID-19. Please see: https://petermcculloughmd.substack.com/p/breaking-sixth-study-confirms-negative, “BREAKING — Sixth Study Confirms Negative Efficacy of COVID-19 mRNA Injections”, by Nicolas Hulscher, MPH, 4 February 2025. The only items, in Yours Truly’s opinion, in the screenshot above that might prompt a medical professional to stop and question whether or not the child should take a COVID-19 “vaccine” would be: an allergy to PEG-2000DMG (one of the lipid nanoparticles in the “vaccine”) or to any of the ingredients of the “vaccine”; a history of myocarditis and/or pericarditis; or has a bleeding disorder. On the other hand, in fact, pregnant women are “encouraged” to take a COVID-19 “vaccine”; and, that immunocompromised persons are “permitted” to take an “extra dose” of a COVID-19 “vaccine.”
Screenshot Three:
So much important information and disclosures regarding the ACTUAL “safety record” of the COVID-19 “vaccines” (for example, the data at https://www.openvaers.com/covid-data); the ACTUAL “clinical trials” data that, for example, Pfizer-BioNTech gave to the FDA regarding the serious Adverse Events reports on BNT162b2; and other items, are missing. The OpenVAERS link takes one to the “Red Boxes” Adverse Events reports and statistics for the COVID-19 “vaccines.” Recall that VAERS receives fewer than 10% of reports of Adverse Events.
How many parents / guardians would go through with having their child (children) COVID-19 “vaccinated” if they knew, for example, that the ingredients and mechanisms of these bioweapon toxin injections change the DNA in their body? Please see: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, Slide 14.
Screenshot Four:
Which, again, mention nothing of the ACTUAL data as reported at OpenVAERS. Instead, there appears to be a strong effort to minimize the ACTUAL potential for serious Adverse Events to occur after taking a COVID-19 “vaccine.”
Yours Truly was able to find a “Consent Document” for persons over age 18 to read and to sign prior to taking a COVID-19 “vaccine”: https://www.gannon.edu/media/gannon-university/content-assets/documents/health-center/GannonUniversity-ScreeningAndConsentForCovid-19Vaccine.pdf. But, even here, there is no presentation of the ACTUAL data from, for example, OpenVAERS regarding serious Adverse Events reports about the COVID-19 “vaccines.” How many persons over age 18 would take a COVID-19 “vaccine” if they were told in advance that these bioweapon toxin injections cross the Blood-Brain Barrier and can induce multiple types of neurological damage? Below are images of the “Consent Document”:
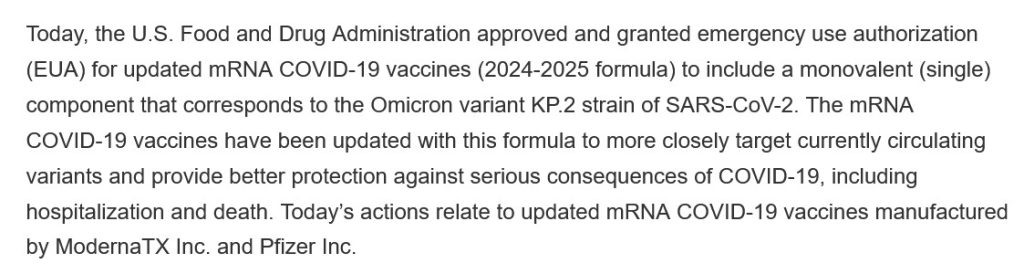
How many persons would take a “2024-2025 Formula COVID-19 Vaccine”, or have such a “vaccine” injected into their child (children), under ANY circumstances, if they knew in advance that these bioweapon toxin injections were either ONLY “tested” on lab mice; or, were “approved” and/or “authorized” based on “manufacturing and nonclinical data”? For this last is exactly what happened with the “2024-2025 Formula COVID-19 Vaccines.” Please refer back to the FDA announcement of 22 August 2024 further up in this post. Here is the salient portion of this announcement as it regards this “2024-2025 Formula”:
The above still image of Charles Boyer and Ingrid Bergman from the 1944 film, Gaslight, is courtesy of Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As today’s post speaks to the disaster of the COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”), Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects (direct or indirect) of the COVID-19 “vaccines”, no matter whether the deceased were COVID-19 “vaccinated” or not. However, the discussion is not limited to what is presented here: It is an Open Thread.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
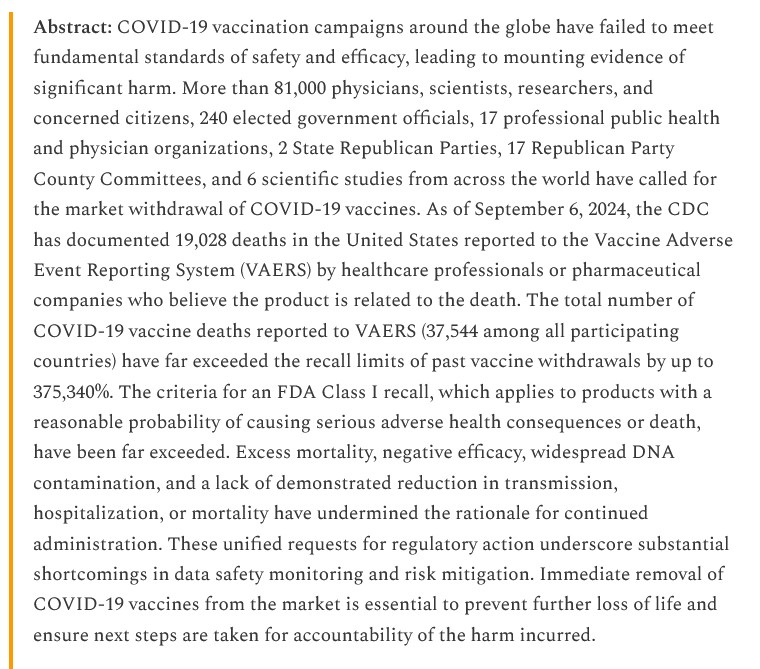
Yours Truly begins here: https://petermcculloughmd.substack.com/p/the-evidence-is-clear-its-time-to, “The Evidence Is Clear: It’s Time to Permanently Ban the COVID-19 mRNA Injections”, by Nicolas Hulscher, MPH, Epidemiologist, and Administrator of the McCullough Foundation, 18 January 2025. There is a video of an interview with Mr. Hulscher by Luiza Asyamova, along with links and graphics from numerous scientific papers, in this article. One of these linked papers is this: https://doi.org/10.5281/zenodo.14269255, “COVID-19 spike protein pathogenicity research library”, Dr. Martin Wulcher, Erik Sass, et al., 3 December 2024 (also found here: https://zenodo.org/records/14269255). There are over four hundred papers listed in this particular compilation.
Yours Truly will focus on one other linked item in the Nicolas Hulscher article cited above, regarding the activities of the United States Department of Health and Human Services to increase uptake of the COVID-19 “vaccines.” The first example is here: https://petermcculloughmd.substack.com/p/the-us-hhs-risk-less-do-more-propaganda, “The U.S. HHS “Risk Less. Do More.” Vaccine Propaganda Campaign”, by Nicolas Hulscher, 19 December 2024. Below are two screenshots regarding the HHS campaign:
HHS launched this propaganda campaign a few months ago, under then-Secretary of Health and Human Services, Xavier Becerra. The agency has already released over 80 videos on its You Tube channels, among many other gaslighting / propaganda items, to “convince” Americans to get the COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”); the influenza virus “vaccines”; and the RSV (Respiratory Syncytial Virus) “vaccines.”
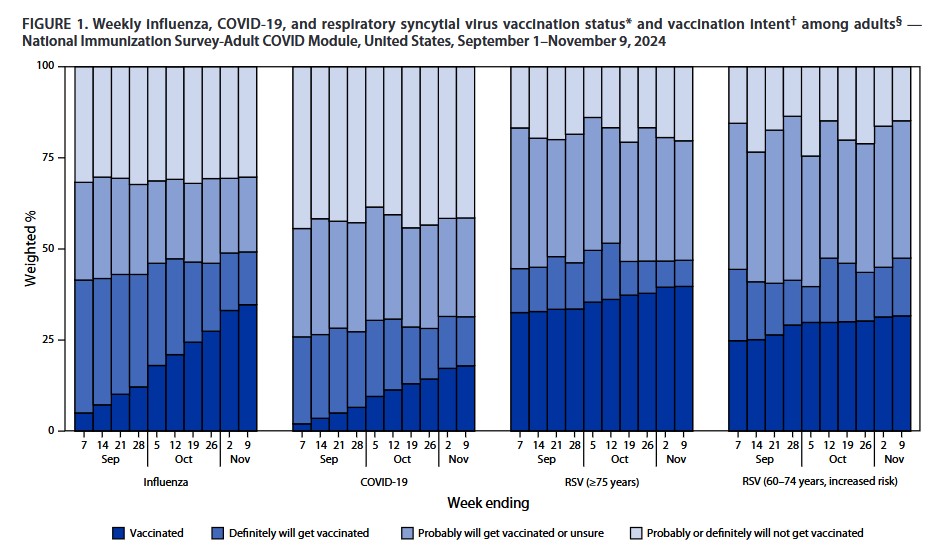
The agency, apparently, was already “alarmed” over the “lack of vaccine uptake” among Americans. Please see here: https://petermcculloughmd.substack.com/p/americas-compliance-with-federal, “America’s Compliance with Federal Vaccine Recommendations as Collapsed”, by Nicolas Hulscher, MPH, 24 November 2024. The CDC’s MMWR (Morbidity and Mortality Weekly Report) article regarding this issue is here: https://dx.doi.org/10.15585/mmwr.mm7346a1, “Influenza, COVID-19, and Respiratory Syncytial Virus Vaccination Coverage Among Adults — United States, Fall 2024”, Jennifer L. Kriss, et al., 21 November 2024. The salient graphic from this article is below:
Which is filled with, in YoursTruly’s opinion, misinformation, disinformation, and outright falsehoods (for example, not mentioning and even dismissing the increasing cases of serious adverse reactions from taking a COVID-19 BTI (the “vaccines”).)
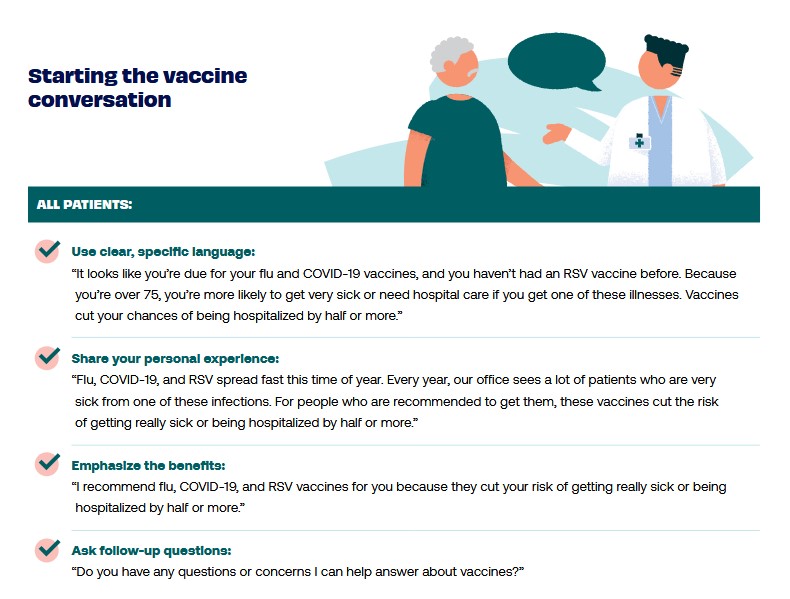
But wait, there’s more! Here is the portion of the HHS gaslighting / propaganda website for medical professionals: https://www.hhs.gov/risk-less-do-more/for-health-care-providers/index.html. In this part of the HHS gaslighting / propaganda effort, one can read through the various “Use these on your “vaccine-hesitant” patients” techniques to “convince” them to agree to having one of the above “vaccines” injected into them. Below are examples from the “Discussion Guides” section of https://www.hhs.gov/sites/default/files/talking-your-patients.pdf, “Talking to Your Patients About Flu, COVID-19, and RSV Vaccines” from the HHS gaslighting / propaganda website. Below are examples culled from this section: the first, how the physician is to “initiate” the gaslighting / propaganda discussion with a patient: and, the second, how the physician can “steer” the conversation if the patient is “vaccine-hesitant”:
Note that the image of the “patient” is that of an elderly male. There are similar “Discussion Guides” for the flu “vaccines” and for the RSV “vaccines.”
Yours Truly will also note the following regarding the above HHS gaslighting / propaganda campaign materials: One: The use of an “elderly male patient” in the example “discussion” with the physician. The CMS (Center for Medicare/Medicaid Services) is involved up their eyeballs in the campaign, due to the payments that CMS receives from every injection of a COVID-19 “vaccine”, an influenza “vaccine”, and/or an RSV “vaccine.” Please see here: https://www.cms.gov/medicare/payment/covid-19/coding-covid-19-vaccine-shots, updated 2 January 2025. And, Two: The AMA gets a “royalty payment” from every CPT code that is used for medical procedures or treatment billing, including injections of “vaccines” such as the ones listed above. This is because the AMA owns the rights to use the CPT codes. Please see here: https://www.ama-assn.org/practice-management/cpt/big-changes-will-streamline-cpt-coding-immunization, 5 January 2024. The “new, all-inclusive” CPT code for any “vaccine” injection administration is 90480.
So far, all of the above has applied to persons over age 18. What about persons under age 18? For this, Yours Truly turns to the American Academy of Pediatrics (AAP) “Redbook” post of 20 November 2024, found here: https://publications.aap.org/redbook/pages/Immunization-Schedules. “Immunization Schedules for 2025” PDF, subtitled “Child and Adolescent Immunization Schedule by Age.” These mirror the CDC Child and Adolescent Immunization Schedule, found here: https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-age.html, 21 November 2024. These are CDC recommended immunization schedules; they are not the law. However, many state legislatures in the United States have adopted this recommended immunization schedule and turned it into state law for children who wish to attend school (public, but in some areas, also private or even home-school situations) within their state. For example, here is the link to the required “vaccines” schedule that children must take if they wish to got to public school in North Carolina: https://immunization.dph.ncdhhs.gov/schools/k-12.htm, “K-12 School Requirements – NC Immunization Branch”, 23 August 2024.
So, it would appear that the Department of Health and Human Services is engaged in a full-on gaslighting / propaganda campaign to “convince” American adults to take the COVID-19 “vaccines”; while, at the same time, the CDC immunization schedule for children and adolescents (which clearly indicates that the COVID-19 “vaccines”, along with the other “vaccines” on the schedule, are NOT law, but arerecommended), have been added into state public school “vaccination schedules” statutes, thus making these recommendations the law of the state. Adults are free to refuse and and all recommended “vaccines”, but persons under age 18 are, in effect, required to take them if they wish to attend public school.
Then, there is the phenomenon of potential COVID-19 “vaccine” shedding. If adults who take a COVID-19 “vaccine” can potentially shed the ingredients of these injectables onto other persons, it would follow that children and adolescents who take these injectables can potentially shed the ingredients. And what about persons under age 18 who are immunocompromised? It is now known that the COVID-19 “vaccines” damage or destroy the natural immune system of the “vaccinated” person. The immune systems of the immunocompromised are already at risk; it can be fairly argued that taking a COVID-19 “vaccine” could put the already-at-risk natural immune system of these persons at further risk.
However, the other links above in today’s post are still active (at least until today 30 January 2025); it appears that the Trump administration order is not retroactive to 20 January 2025. Therefore, the “Discussion Guides”, the handouts, the billing / coding information, and so on, listed in today’s post, are likely still being used.
THERE. MUST. BE. JUSTICE. Yours Truly believes that the confirmation of Robert F. Kennedy, Jr., as the new Secretary of Health and Human Services needs to happen as soon as possible: so he can end the HHS gaslighting/propaganda efforts, to start.
With that settled, I jump to the second item on the agenda.
A call for weekly open-thread authors on Tuesday and Thursday.
I know this seems abrupt, but DePat’s obituary has already published, and I’m already going to talk about even more sensitive topics now – by request – so I don’t feel too much guilt in making sure that DePat’s MISSION of keeping this site running is fully taken care of.
The best thing that we can do, in my opinion, to maintain Susie’s legacy in the MAGA world, is to keep all of her posts here (just under 1000 of them) online and searchable. SO – we need new authors for Tuesday and Thursday, to keep this site running.
Gudthots is thinking about taking over Thursday.
Do we have anybody else, who would like to do Tuesday? Which means that the post goes up Monday night, scheduled for one minute after midnight (I can help with this).
Just to be clear to potential authors, these daily threads are YOUR BABIES – meaning they don’t have to be anything like the way that DePat did them. In fact, it’s probably better not to. I invite new authors to come up with their own new styles.
We do have a very thin guideline post of basics in the sidebar, shown here:
We were actually more rigorous about format then, but it does help that daily open posts publish on the day listed in the title, and that the titles have a searchable format.
Anyway, if you are interested, just leave a comment.
If you are shy about saying something, you can always do “PMTW” (see “Contact”), commenting on this post, and then I can respond anonymously in public, although I recommend just being open.
Looking forward to somebody picking up DePat’s second sword.
And now for the big item.
A discussion of various pathological possibilities, including some new ones, and an explanation of why I lean toward particular theories.
I begin by citing relevant portions of FG&C’s report on the “sudden and unexpected” passing of Susie, which he communicated to me privately.
7-8 weeks ago Susie attended a choir rehearsal, during which she had stood right next to a fellow choir member who she learned afterwards had been Covid vax-boosted for the 4th time that day. Perhaps she mentioned at some point in these pages that in the time since that night she believed she had contracted “long Covid”, experiencing physical weakness, insomnia, a persistent cough, and low appetite. She believed she had inhaled “spike proteins” shedding from the woman she stood next to that night at rehearsal, stating that had she known the woman had been so recently vaxxed she would never have gotten so close to her.
Recently, she had stated she was feeling better, the cough all but gone, and in the past week felt she had gotten over the insomnia hump and was getting good rest. I was optimistic. However, on Monday AM….inauguration day….her brother discovered her in her bedroom, unresponsive, after becoming concerned he had not heard her moving about and she had not come downstairs. Paramedics were subsequently unable to resuscitate her, and it is currently believed she suffered a heart attack and passed away in her sleep. After many attempts to reach her (we texted daily), her brother called me this afternoon with the news. I knew you would want to know as well.
I am going to tease this apart very gently, so that you can see all the possibilities that we’re actually dealing with.
Point 1 – “Shedding”
Now, if you were following along with DePat’s posts in recent weeks, then you realize that she was very convinced that she had been subject to shedding of [COVID-19 vaccine-created] spike protein.
The first problem there, is that very near the end, DePat realized that the vaccine-originated shedding would more likely have been the spike mRNA, not the spike protein.
Here is her comment, which was in fact her third-to-last, made on January 17, 2025.
This one is particularly scary as it claims the shedding is due to mRNA and not the spike protein. Drat.
Does anyone have further evidence on this or a rebuttal? I always thought it was just the spike protein. So far, no heart issues or unexplained pain, true brain fog (I’m sleepy today as the insomnia is FINALLY subsiding. I slept a LOT in the last 24 hours.), or any of the other hard core stuff. A LOT of stiffness keeping warm, and the return of some relatively normal complaints for me in winter.
Fortunately, we haven’t given away the bulk of my mother’s tools she used for the last so many years of her life after the hip replacement, and subsequent ailments. They’ve come in handy. I have another friend who is helping me out in a lot of ways. The next week will be a challenge temperature wise and then I can at least sit in the front door and soak up radiant heat as the sun comes out. Less than a half hour is recommended.
I’ve decided to use this experience as part of writing about an elderly or disabled person. There’s too much challenge at this point to really articulate it, but this is for the birds even if the worst of it is fatigue.
And, yes, stay away from crowds and people you know who get boosters.
So – let me just spell this out. DePat realized that vaccine shedding could be the spike protein, but that it’s more likely (and more dangerously) to be the spike protein mRNA enclosed in lipid nanoparticles that can get into cells. It is by this mechanism that much more spike protein could be created in the body of the shedding recipient.
Not a pleasant thought.
Now – just a side note. DePat and I had discussed all this, many times, WAY BACK in late spring of 2021, so she knew this stuff years ago. Thus, I really believe that she had some brain fog recently. And we know from her comments – DePat understood that she had brain fog, too, despite the fact that it was interfering with her memory.
Years ago, she and I had speculated on the shedding of spike protein, to explain things which were being observed in people close to vaccine recipients. Unlike DePat, I was not a believer in “shedding”, but when Naomi Wolf started reporting observations consistent with some kind of shedding phenomenon, I came up with a scientifically solid explanation of how shed spike protein could actually cause such symptoms, if the spike protein had highly potent, oxytoxin-like pharmacological activities.
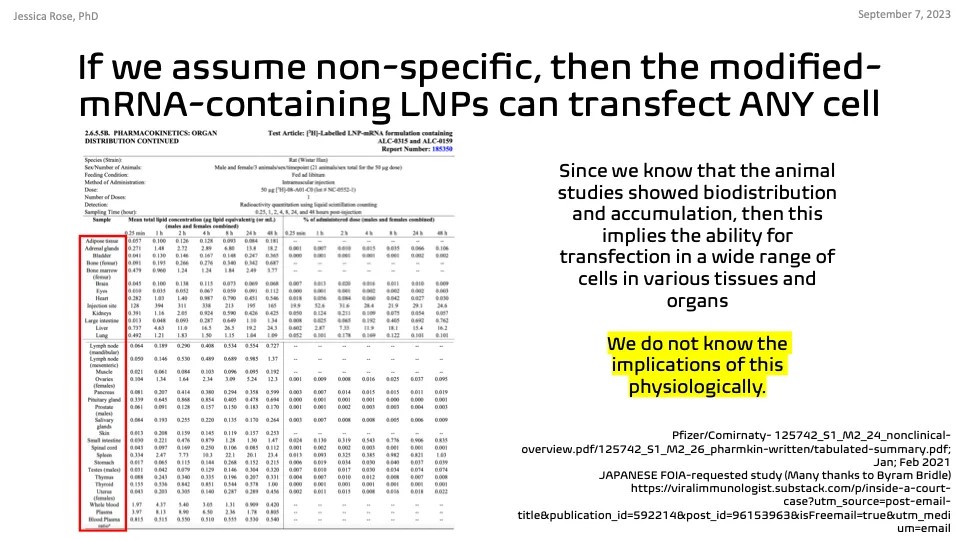
The idea of spike protein shedding seemed plausible AS IS, but when Pfizer’s own data, released to vaccine skeptics by the Japanese government, showed the vaccine itself persisting and migrating in test animals, it became clear that shedding of the VACCINE would be an even better explanation.
The point about snake venoms and spike protein is an ANALOGY – it’s not direct – but it’s very useful in understanding both potencies and pharmacological and pathological actions.
I want people to understand this. EVEN if it was just the spike protein being shed, if that protein is even slightly like snake venom in pathogenicity, then it behooves us to look at how snake venoms are dealt with in real life.
Specifically, when cages of venomous snakes are being cleaned, those present have to actually wear respirators. Not just masks – respirators. That is because the dust from dried snake venom in venomous snake cages can literally cause dangerous symptoms in people cleaning the cages.
SO – I want people to understand that DePat had a good theory here – namely, the theory that she got many lung-fulls of either spike protein, or (more dangerously) vaccine nanoparticles, from that vaccine-injected choirmate of hers.
According to this theory, not only did the “shed” vaccine cause typical vaccine-related symptoms – it potentially caused myocarditis, aortal embolism, blood clots, or any one of the many serious cardiovascular events that the vaccines are capable of causing.
This is actually a really reasonable theory.
However, it’s not the only one.
Point 2 – Nicotine
DePat’s last post indicates that she was continuing to use nicotine patches as an off-label way to “inhibit spike protein”. Here is that post.
I’m trying, be sure of that.
Others in my family aren’t. They think this will all go away just with ivermectin. I’m not done with the nicotine protocol yet.
OK – so what is this “nicotine protocol”?
The TL;DR is that one of the alternative medical treatments for “spike protein” / “long COVID” – and particularly “brain fog” – is medicinal nicotine, either as chewing gum, patches, or sublingual.
But before I get into this treatment, it’s helpful to see when and where DePat began investigating nicotine as a solution to her ailment. The entire conversation is very instructive, and begins here, where DePat began asking all of us for suggestions about treatment of her condition.
After talking over symptoms with a friend who is in the same boat as many of us are with the COVID shots – she didn’t take them, but her husband did and she’s now suffering with the side effects despite all sorts of alternative treatment – I think whatever this is that I have is related to a choir member getting a booster last month and exposing me. The fatigue symptoms pretty much match what she had. Just unloading and loading the dishwasher is a challenge. Forget actual housework which desperately needs to be done. (When the kids get here on Saturday, I’m using them to deck the halls.) This crap is for real.
Other than making a run for Tennessee, which really isn’t that bad of a drive from here, for Ivermectin, any ideas? My friend ordered me a nebulizer and is willing to help me use it to break up biofilm, etc., but is there anything in anyone’s arsenal of natural remedies that may help? I had a talk with our Lord and Savior at Eucharistic Adoration today, and I’m hoping my Novena for wellness is doing some good, but, really, I have a lot to do and no energy to do it. Just about every old injury has flared up – especially in my torso which are pretty much all from singing – and some other things.
I just want and need this to go away.
Any ideas?
Thanks.
P.S. please pray for a cousin, A, and her husband, K, who are suddenly expecting identical twins over the summer. it’s a CLASSIC case of you make plans, God laughs. They are in their late thirties, and their toddler was born via c-section due to pre-eclampsia. Fortunately, her OB services are through a Vanderbilt extension, so we’re all hoping for the best.
P.P.S. Next week, we are going to have a house full of people, so the posts will be placeholders of a sort. I’m going to resurrect an old one and draft something new for the day after Christmas. Just a head’s up.
Now, at that time, all of us came in with a wide variety of suggestions, but one late response came from a hitherto lurking account, I Hate Acronyms, now registered as Sigma.
Very long time lurker here from the great Q purge OT. Please consider nicotine patches. The highest strength, cut into fourths. Apply one of the fourths to your skin, replacing with a fresh one daily. Do a search on Rumble for “nicotine and spike proteins”. “Nicotine vs nanotech” If they are going to work, you should see results within days, if not hours. Non-addictive.
As I felt this was earnest and helpful advice, and that the nicotine method had solid science behind it, I approved the comment immediately, hoping it might help DePat.
I am sure that DePat thoroughly investigated this, and found all the same information that I did. If you dig deep enough and far enough on this, you will find all of the following.
there are valid scientific reasons to think nicotine might work as a treatment for “long COVID” / “long vax” / “spike protein”
there is a wide range of voices supporting treatment with nicotine
those voices include more “controversial” ones like Dr. Bryan Ardis and Dr. Tau Braun
they also include more widely respected ones like Dr. Peter McCullough
there are also discrediting connections to “nanomachines” and the like, which I ignore
for some people with long COVID, nicotine has helped when nothing else has worked
I advise just doing the recommended Rumble searches, to learn more.
For example, this video shows a variety of scientific papers which not only explain why nicotine affects spike protein-based symptoms, but also show demonstrated clinical benefit in actual patients.
I do NOT suspect that nicotine poisoning was involved in DePat’s death. Toxic levels of nicotine result in very obvious symptoms (nausea, vomiting, tremors, vertigo, flushing, palpitations, etc.) that quickly make people back off on whatever means by which they were ingesting nicotine. I know, because the first cigar I ever smoked sent me into nicotine poisoning. People learn very quickly how to dose nicotine correctly.
DePat was actually getting some positive results with this method. More specifically, it was making her feel better. I personally think her efforts would have been more successful under a doctor’s supervision (preferably one connected to FLCCC or the like), but when I suggested “doctors and tests” to DePat, she was not a fan.
DEPAT:I’m wondering if some of this fatigue is coming from trying to stay warm in a drafty house.
Hmmm….
ME:That sounds very likely to me.
Your body basically sends your periphery into overdrive to stay warm. Long johns / thick leggings and a sweater indoors can be very helpful. Feeling warm indoors can stabilize you.
Also wondering if your doctor is running a yearly thyroid check (TSH) If the numbers are odd or marginal, you may have something going on there.
DEPAT:Doctor? I learned my lesson with conventional medicine a long time ago.
ME:Sounds a lot like COVID. Have you tested yourself at any point?
DEPAT:No. But I was exposed to two people who had their boosters over a month ago. The coughing fits started on the 17th last month. True weakness and needing to sit down for tasks the three days before Thanksgiving. I think I’m just about at the end.
In my opinion, DePat really needed a complete physical checkup, if only because it might have picked up any underlying conditions. But even more than that, there was a need for better diagnosis of what was ailing her. Simply assuming that it was vaccine shedding was risky, IMO.
Point 3 – COVID-19
Notice that I had asked DePat about COVID. The symptoms of being a “shedding recipient” should be almost the same as “long vax” – which should be very similar to the disease itself. Even more to the point, it is extremely easy to pick up COVID in a place like a choir. In fact, it only takes a much smaller dose of an infectious organism, than it does of a “shed vaccine”, to cause the exact same kind of problems that DePat was having.
DePat seemed very resistant to the idea that she might have had COVID or a similar ILI (influenza-like illness). However, to rule out an actual disease takes some effort. And to PREVENT disease takes even more.
Was she taking her temperature daily or twice daily? As far as I know, NO. Was she taking ivermectin AT ALL, much less regularly? NO. Was she taking vitamin D? Had she ever tested her levels of vitamin D? NO. Was she taking enough zinc? I don’t think she was taking ANY zinc.
DePat’s situation was a lot like Wheatie’s. She KNEW – more or less – what sorts of things might be useful if she ever got COVID, but she had NOT prepared by having those things purchased, fully understood, and on hand, ready for trouble. Even more, she was not ready to DIAGNOSE COVID.
I KNOW that I have had COVID three times, because I’ve done the testing and clinical work to make absolutely firm diagnosis. I know that what I have right now is most certainly influenza, and NOT COVID.
And that brings me to my next point.
Point 4 – Influenza
I think it is VERY likely that DePat had the very nasty influenza that is going around right now, which singingsoul1 suffered from greatly, at almost the same time as DePat, and which I am suffering from at this very moment. As is my wife – so I am studying TWO cases, almost identical.
“feel bad”
aches and pains
persistent cough
no appetite
insomnia
chills
fatigue
sense of smell OK
stuffy sinuses and phlegm – mostly upper respiratory
“forget doing housework”
need a nebulizer (I use saline spray, myself)
Everything DePat was saying about what she was suffering, sounds like what I’m suffering right now. And, in fact, what MANY people are suffering right now.
And here’s the kicker. Influenza is a PRIME candidate for setting up a heart attack afterwards.
I know that many of you (like me) might suspect that this angle is pure post-clot-shot “explain away the vaccine heart attacks” bullshit, BUT the fact is, influenza has ALWAYS been notorious for killing old people, and heart attacks is one of the ways that it does it. Viral diseases – colds and flu – are also notorious as initiators of pericarditis and myocarditis. They didn’t have to make this shit up, to use it to deflect from their horrible vaccines.
As I love to say, there’s no cover like the truth.
Now – one might think DePat would have known if she had the flu, but this thing my wife and I have, has proven to be surprisingly low-fever – especially for my wife. Even after the fever has subsided, we still feel very ill. Were I not monitoring our temperatures every day, getting actual numbers, and signal over noise, it would have been easy to dismiss this thing as something other than influenza.
At numerous times during the last week, I have thought that maybe this was something other than influenza. But the reality keeps coming back, as I read more and more solid information about influenza and its treatment. What I have – what my wife has – what singingsoul had – and what DePat likely had – was a long, slow case of influenza, with a long recovery time.
Bear in mind that viral diseases often leave patients stuffy and suffering many symptoms for 60 days (2 months), long after the virus is gone. That fits perfectly with the timescale that DePat reported.
I think it is very critical to make a correct diagnosis, and to beware of reflexive “it’s the vaccine” thinking, when DISEASE never went away as a significant threat. Maybe even a MORE significant threat.
It’s entirely possible that DePat was exposed to “shed vaccine” – but I would argue that it’s more possible she was exposed to a nasty flu, didn’t have the right tools to diagnose or treat it, and damage by this flu ultimately led to a heart attack or stroke.
Either way, I now urge everybody – investigate treatments ahead of time. Don’t wait for being sick, because you won’t make it to the store – you won’t make that long trip to Tennessee – you won’t figure out which drug, where to get it, and how to take it.
Do all that ahead of time, if you want to live.
With that, I invite people to give me THEIR opinions. Feel free to disagree with me! After all, we have free speech back. THANK GOD!!!
Finally, this. Say a prayer for DePat and her family – grieve as you need, and you WILL need – but trust that God knows what God is doing, and seek comfort in that knowledge.
Trust in God. He is with us, and DePat is with Him.
The above free image of a handwritten letter from 1889 is courtesy of Colourbox and Google Images.
Health Friday is a series devoted to Big Pharma, vaccines, general health, and associated topics. As this post speaks of the disasters of COVID-19 and of the COVID-19 BTI (Bioweapon Toxin Injections, aka the “vaccines”), it is dedicated to the memory of Yours Truly’s “fully vaccinated and boosted” late brother, Sam; to her late cousin, Bill; and to all persons, of whatever age or location, who have passed away from the negative effects (direct or indirect) of the COVID-19 “vaccines” they had in the their bodies. However, the discussion is not limited to what is presented today: It is an Open Thread.
There are Important Wolf Moon Notifications, the Rules of our late, good Wheatie, and certain caveats from Yours Truly, of which readers should be aware. They are linked here.
Herewith, the letter:
Dear Incoming President Donald J. Trump and Incoming Secretary of Health and Human Services Robert F. Kennedy, Jr.:
Greetings. This letter is from an independent researcher who has been writing about the COVID-19 virus and the COVID-19 “vaccines” for over four years.
The COVID-19 virus is, by now, a part of human life on this planet. It will continue to mutate and infect humans. The failed COVID-19 “vaccines” were developed and mandated for use on humans to “prevent” infection by this virus. The COVID-19 “vaccines” are not “safe and effective” as they are claimed to be by the CDC, the FDA, and many medical organizations. In fact, these injectables induce thousands of types of medical conditions; can aggravate existing medical conditions; re-establish previously-controlled medical conditions; induce COVID-19 infection; and more, among those who have COVID-19 “vaccines” in their bodies. For further information, please see the Appendix 1. List of Adverse Events of Special Interest section of the following document, given to the FDA by Pfizer-BioNTech on 30 April 2021, regarding the company’s modRNA COVID-19 “vaccine” BNT162b2: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf, “5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162B2) Received Through 28-Feb-2021.”
It is now known that the COVID-19 virus was a lab-created biological weapon (bioweapon); and that the COVID-19 “vaccines”are lab-created and -enhanced biological weapons (bioweapons.) There were, and are, numerous entities and persons involved in the creation of this virus and these “vaccines” that must now be brought to justice for their activities. Among these activities was the deliberate withholding of vital information from you, President Trump, as then-President of United States, during “Operation Warp Speed”, which was part of the White House Coronavirus Task Force in your first administration. Please refer to: https://oversight.house.gov/wp-content/uploads/2024/12/2024.12.04-SSCP-FINAL-REPORT-ANS.pdf, “After Action Review of the COVID-19 Pandemic: The Lessons Learned and a Path Forward”, by the Select Subcommittee on the Coronavirus Pandemic, Chairman Brad Wenstrup, for more information regarding the development of the COVID-19 virus and of the COVID-19 “vaccines.”
To gain more knowledge regarding the disaster of the COVID-19 virus and the COVID-19 “vaccines”, please refer to: https://kirschsubstack.com/p/game-over-medicare-data-shows-the, “GAME OVER: Medicare data shows the COVID vaccines increase your risk of dying”, by Steve Kirsch, 2 February 2023; and, also:
The following website lists links to contracts between the United States government and Pfizer-BioNTech related to the COVID-19 issue: www.keionline.org/covid-contracts, “COVID-19 Contracts.” These contracts involve the Department of Defense; the Department of Health and Human Services; the Administration for Strategic Preparedness and Response (ASPR); the Biomedical Advanced Research and Development Authority (BARDA); the National Institutes of Health (NIH); and the National Institute for Allergies and Infectious Diseases (NIAID.) There are also links to contracts between the United States government and other companies related to COVID-19. These include companies such as, Glaxo-Smith-Kline; Johnson & Johnson; Moderna; and Novavax, among many others.
The following paper details how the dangerous lipid nanoparticles in the modRNA COVID-19 “vaccines” spread the ingredients of these “vaccines” throughout the body, inducing changes body-wide, particularly in the heart: https://doi.org/10.1038/s41587-024-02528-1, “Nanocarrier imaging at single-cell resolution across entire mouse bodies with deep learning”, Hendrik Dietz, et al., 14 January 2025. Please see the image of the Abstract from this paper, below:
Please also see the image below, from the blog post by Dr. Jessica Rose, PhD, which discusses the above paper (https://jessicar.substack.com/p/lnp-spike-mrna-induction-of-changes, “LNP spike mRNA induction of changes in proteins related to vasculature formation and maintenance (collagen) in the heart”, 15 January 2025):
President Trump and Mr. Kennedy, Jr.: The double disaster of the lab-created bioweapon called the COVID-19 virus, and the disaster of the lab-created and -enhanced bioweapons called the COVID-19 “vaccines”, must not ever be allowed to occur again. The entities and persons involved in the creation of this double disaster must be held accountable. In addition: The use of the COVID-19 “vaccines” must be stopped immediately, for all age groups, until complete, detailed, and proper clinical trials are held regarding these products, with all data fully collected, analyzed, and published for the public to see.And,President Trump: Mr. President, it is also incredibly important that those who deliberately withheld from you, or minimized to you, information that you needed to know during “Operation Warp Speed” in your previous administration, be held accountable.
It is also imperative that all medical professional organizations, state medical licensing boards, and specialty medical certification granting organizations, which currently require their applicants, licensees, and certification holders, to be COVID-19 “vaccinated”, to use only FDA-approved prophylactics and/or treatments for COVID-19, and to urge these products on their patients, be enjoined to end these requirements. Furthermore, access to, and use of, prophylactic and/or treatment options for COVID-19 that are safe and effective, such as, Ivermectin, Hydroxychloroquine, Quercetin, Zinc, and Vitamin D, must become available to all persons, including to persons with COVID-19 infection, whether they are hospitalized or not. In addition, medical professionals who choose to treat patients with the products listed above must not become subject to “professional discipline” protocols, or to have their License to Practice Medicine and/or their specialty medicine certifications restricted or revoked.
With Peace, Good Energy, and great Respect, from an independent COVID-19 researcher,