“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
TL;DR – Watch this sucker while ignoring the myopic neo-Bolshevik “refugee” propaganda, but instead keeping in mind the current COVID/WEF insanity, to get a grip on the incipient climate-excused holocaust of the depopulationists, which is the fault of SOCIALISM, same as the soon-to-be-dwarfed “Holocaust” of the 1930s and 1940s.
OK – just a bit more detail…..
Don’t watch the Ken Burns Holocaust special for any of the slanted, leftist, socialist messaging stapled onto the historical facts in a DNC-approved and ADL-edited way.
Watch this PBS special while subversively keeping in mind the new socialist, depopulationist, eco-nuttery holocaust which now exceeds 6 million COVID dead and will soon DWARF the old “Holocaust” of so much hypocritical and self-centered angst.
Calmly stroke Suspicious Cat, as the Holocaust is falsely linked to rejection of current “asylum seekers” in a face-palmingly stereotypical and Trump-hating way.
Watch this PBS special while “rebelliously” remembering that RIGHT NOW we are in a DESIGNED CRASH of the world economy, which will kill BILLIONS of innocent people if not stopped – and which is largely driven with the eager participation of globalist and socialist “Jazis” – who are no less evil than the Nazis of old – self-righteous in their “ESG/DEI” zeal, with their vain self-assurance that they and they alone know the answers which must be forced upon the world.
Watch this special remembering Andrew Cuomo, Anthony Fauci, Ralph Baric, Joe Biden, WEF, Klaus Schwab, Pfizer, CCP and Albert Bourla, and keeping close in mind, the NEW holocaust which has already killed over 6 million worldwide by the virus ALONE, and is already creating even-more-massive excesses in mortality in every country, in unacknowledged proportion to acceptance of the “vaccines”.
Watch this PBS propaganda special while remembering how the US and China co-created biological “gain of function” which literally DWARFS the mere chemical nastiness of a bug spray, “Zyklon B”, itself more comparable to Fauci’s murderous remdesivir, or the midazolam they apparently used for “COVID euthanasia” in the UK.
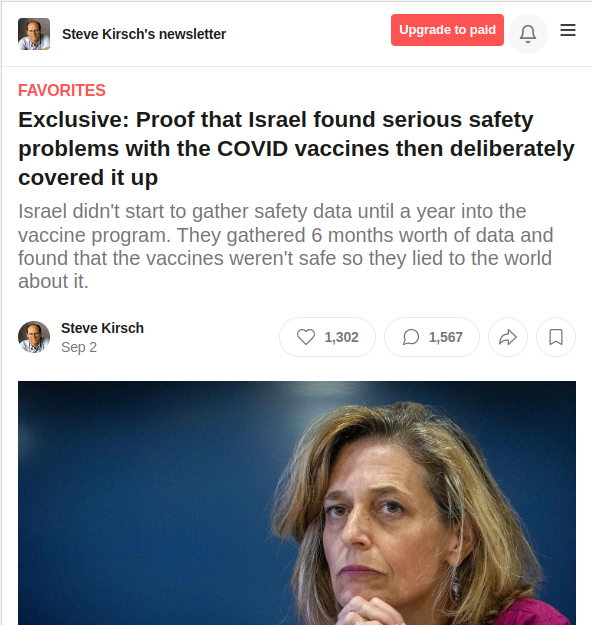
Watch this special while remembering the millions who died around the world from both virus and vaccines, including tens of thousands of Israelis, as secular Jewish leaders condemned their own and didn’t lift a finger, other than to censor Zev Zelenko, and to suppress their own report on the dangers of the vaccines they INVESTED IN.
Watch this special in strict analogy of the THEN unbelievability of the “final solution”, to the NOW unbelievability of “depopulation”.
Realize that the problem isn’t antisemitism or “refugee acceptance” – it’s SOCIALISM.
SOCIALISM KILLS – no matter which brand.
Representative Alexandria Ocasio-Cortez (D-NY) and Senator Ed Markey (D-MA) were joined by Democratic lawmakers from both the House and Senate on February 7, 2019, to introduce Green New Deal legislation.
Oh, hell. I said enough already. Do I really need to explain this?
If so, I’ll do it in the comments.
But the bottom line is that this special has a lot of great facts, which – if you are prepared to see them in the context of current events – are quite convincing that we ARE in the late beginning of yet another socialist holocaust.
Well, they can lock us out of The Q Tree, but they can’t stop the truth from getting out.
Enjoy a post first over on The U Tree and now HERE.
Here is a quickie in my WAR ON REMDESIVIR.
Fellow Treeper barkerjim dropped an interesting document today, from back in July, which showed the NIH mentioning black sheep IVERMECTIN on the same page as REMDESIVIR.
Such a beautiful misdirection. These guys are MAGICIANS.
This is a perfect example of my postulate that fighting FOR ivermectin will not yield results for restoring real science as fast as fighting AGAINST remdesivir.
In fact, I would go so far as to say that the enemy realized that getting us to fight FOR the saving drug would keep us from expending our energy fighting AGAINST the murdering drug that kills us off and gives them money for doing it.
You may recall my previous posts about remdesivir.
My next piece was going to be an expansion on Karl Denninger’s recent post which places remdesivir/ivermectin and remdesivir/hydroxychloroquine in the context of Anthony Fauci and the disturbingly similar case when he was “all about AIDS” – namely, AZT/bactrim.
YES. As Cthulhu has said before, “This is not Fauci’s first rodeo.”
Before there were hydroxychloroquine and ivermectin as innocent victims – good Samaritans accused falsely before the world – there was BACTRIM.
And there was FAUCI on all of them. AZT played the murderous part of remdesivir long before we forgot that “miracle drug”.
However, this new information from barkerjim’s drop right here needs to get out right away. The Q Tree site was brought down YET AGAIN as I started working on this, and again when I resumed, so I know it’s critical stuff. The ChiComs have a huge investment – both financial and military 4GW – in the American-killing drug remdesivir. They WILL protect it.
We know from doctors and scientists quoted in my first two articles, that remdesivir has a horrible track record – shocking, really – of renal toxicity. Studies of the drug against Ebola were TERMINATED because it was killing people in the hospital.
How déjà vu.
But here it comes again.
I read the same study results that the above celebratory announcement was made over. Those results were nothing to cheer about, with shot kidneys just the horrifying icing on the death cake. In my opinion, the results were far WORSE than any prior results for hydroxychloroquine. The results – to me – made HCQ look EXCELLENT in comparison.
Yes – by controlling what is acceptable science and what is not, Fauci was able to force the world to field a BAD, DANGEROUS DRUG that made money for Gilead, over a safe, mildly (but critically) effective drug, that made money only for the generics industry, and a French company.
And to top it off, Fauci USED Trump, who could do absolutely nothing about it, to take a KILLER drug into market as the ONLY way to treat his little pandemic.
So let’s take a look at that page dropped by barkerjim. I have captured it as SIX IMAGES.
As you can see by our comments on The U Tree, most people will look at this table and think they are seeing positive and reasonable behavior by NIH. Adverse events are being discussed, and it appears that things are “even-handed” between different drugs.
And that is EXACTLY the style in which EVIL ABOUNDS IN WASHINGTON, DC (or Atlanta). Good and evil are forced into compromises where GOOD LOSES and EVIL WINS – but the result is called “meeting in the middle”.
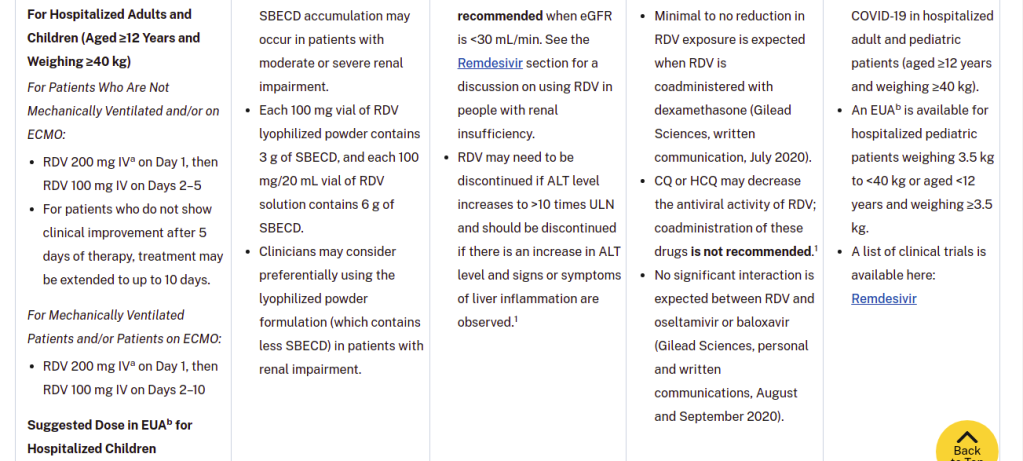
CLOSER INSPECTION of the table gives you this, under Adverse Events for remdesivir.
Nausea
ALT and AST elevations
Hypersensitivity
Increases in prothrombin time
Drug vehicle is SBECD, which has been associated with renal and liver toxicity. SBECD accumulation may occur in patients with moderate or severe renal impairment.
Each 100 mg vial of RDV lyophilized powder contains 3 g of SBECD, and each 100 mg/20 mL vial of RDV solution contains 6 g of SBECD.
Clinicians may consider preferentially using the lyophilized powder formulation (which contains less SBECD) in patients with renal impairment.
This is some of the most remarkable “medical misinformation” I’ve ever seen. It’s truly a work of art.
NIH has HIDDEN – completely hidden – the pronounced renal toxicity of remdesivir. They have hidden it COMPLETELY. It’s GONE. What you are seeing there – the talk about renal and liver toxicity – is a BLAME-SHIFT to a substance that is used WIDELY in intravenous formulations, called sulfobutylether-β-cyclodextrin, or SBECD for short.
This substance is an EXCIPIENT.
An excipient is a substance that is used to MIX with a drug, and take that drug into a form where it can be ADMINISTERED easily. Thus, an excipient may DISSOLVE the drug, or help to dissolve it, into a liquid form. It may help POWDER the drug, so that it can be pressed into tablets or filled into capsules.
Excipients are often considered “inactive ingredients”, even though – YES – they very much can change the effective amount of a drug that the patient gets.
If I had to describe SBECD as something, it would be as a DETERGENT FOR DRUGS. It’s a kind of SOAP made from a cyclodextrin, instead of from some kind of fat or lipid.
Cyclodextrins are rings of sugar molecules that falls somewhere in between being a smaller chain sugar (like sucrose) and a starch. Cyclodextrins have lots of uses, because they form tubes that act like waffle cones for other molecules. Febreze uses cyclodextrins to trap molecules which have unpleasant odors, at the same time that they release more pleasant ones. A genius application, quite frankly.
Thus, if you make a SOAP that has a little waffle cone for drugs, you can EASILY get drugs to dissolve into a concentrated liquid form by using that soap.
See those sidechains hanging off the cyclodextrin ring? Those are the “SBE” part of SBECD. They are typical of DETERGENTS.
This SBECD stuff and things like it are VERY useful for delivery of drugs. AND they’re relatively safe, too. They are rapidly excreted through the kidneys. Yeah, you don’t want a SOAP piling up in your blood if your kidneys are not working, and THAT is the fact that is being TWISTED by NIH when they say:
Drug vehicle is SBECD, which has been associated with renal and liver toxicity. SBECD accumulation may occur in patients with moderate or severe renal impairment.
Did you catch that sleight of hand? I’m gonna show it to you.
What exactly is causing the renal problems in the FIRST PLACE that you MAY have to be careful about, so that you don’t build up the excipient FOR IT, which MAY constitute a FURTHER risk?
REMDESIVIR.
It’s a crafty little lie. If you have good kidneys, you don’t have anything to worry about with this SBECD crap. But if you have bad kidneys, the LEAST of your problems is SBECD buildup. It’s the remdesivir IN the SBECD that’s gonna kill you.
Weakened kidneys do NOT need to be hit with remdesivir.
Which doesn’t even work ANYWAY. Except to keep people LONGER in the hospital.
Now what you SHOULD be getting, when they administer remdesivir, at the point where the VIRUS is basically gone, and you’re dealing with spike protein damage, cytokine storm, and all that nasty crap, are antiinflammatory, antithrombotic, and immunomodulatory drugs. Even HCQ (a known antirheumatic) at reasonable doses had some antiinflammatory effect in late-stage hospitalized COVID cases, although steroids and other things work better.
When the virus is basically gone, and a bunch of its CRAP is left behind, there is no point administering a toxic antiviral like remdesivir, other than to send money to Gilead Pharmaceuticals and their Deep State friends.
Now, let me stop here and validate this stuff.
HERE is a link that explains how SBECD can be filtered out of blood ANYWAY if a patient has renal impairment.
Do you see what that means? SBECD is a nothingburger. It’s a DEFLECTION.
The renal problems of remdesivir are never mentioned, by quickly bringing up the risks of the excipient due to the unmentioned damage BY remdesivir.
What NIH did here was to quickly point their finger at THE OTHER GUY and said “HE DID IT!”
This is pure politicized science, where the politics is to defend the drugs and vaccines that enable the shared profits of both the Deep State and the companies that NIH, CDC, and NIAID are in bed with.
Let’s go back to that link I just gave you. THIS part of the conclusions comports very nicely with the reality of SBECD as a widely used excipient.
The finding that SBECD can be effectively removed by CVVH is clinically important, because some cyclodextrins have been associated with hepatotoxicity or nephrotoxicity due to vacuolation [3]. Although our study was small, no evidence to suggest SBECD as a cause of hepatotoxicity or nephrotoxicity was demonstrated in our study patients. This finding is consistent with other SBECD safety studies in humans [3,18]. Additionally, animal studies have only been able to demonstrate cyclodextrin toxicities when dosages more than 50-fold greater (3,000 mg/kg) than those used in humans were administered [3,19,20]. Unlike other cyclodextrins used in these animal studies, SBECD undergoes only minimal tubular reabsorption and limits concentrations within the intracellular tissues of the kidney, potentially reducing the risk of nephrotoxicity. Nevertheless, the FDA labeling for voriconazole recommends that IV therapy be avoided, if possible, in patients with a CrCl <50 ml/min [5]. Our data suggest that IV voriconazole can be safely administered in this population if the patient is concurrently undergoing CVVH.
Delafloxacin, a fluoroquinolone, has activity against Gram-positive organisms including methicillin-resistant S aureus and fluoroquinolone-susceptible and -resistant Gram-negative organisms. The intravenous formulation of delafloxacin contains the excipient sulfobutylether-β-cyclodextrin (SBECD), which is eliminated by renal filtration. This study examined the pharmacokinetics and safety of SBECD after single intravenous (IV) infusions in subjects with renal impairment. The study was an open-label, parallel-group, crossover study in subjects with normal renal function or mild, moderate, or severe renal impairment, and those with end-stage renal disease undergoing hemodialysis. Subjects received 300 mg delafloxacin IV or placebo IV, containing 2400 mg SBECD, in 2 periods separated by ≥14-day washouts. SBECD total clearance decreased with decreasing renal function, with a corresponding increase in area under the concentration-time curve (AUC0-∞ ). After IV delafloxacin 300 mg administration, SBECD mean total clearance was 6.28 and 1.24 L/h, mean AUC0-∞ was 387 and 2130 h·μg/mL, and mean renal clearance was 5.36 and 1.14 L/h in normal and severe renal subjects, respectively. Similar values were obtained after IV placebo administration. In subjects with end-stage renal disease, delafloxacin 300 mg IV produced mean SBECD AUC0-48 values of 2715 and 7861 h·μg/mL when dosed before and after hemodialysis, respectively. Total SBECD clearance exhibited linear relationships to estimated glomerular filtration rate and creatinine clearance. Single doses of IV delafloxacin 300 mg and IV placebo were well tolerated in all groups. In conclusion, decreasing renal function causes reduced SBECD clearance and increased exposures, but SBECD continues to exhibit a good safety and tolerability profile in IV formulations.
“In conclusion, decreasing renal function causes reduced SBECD clearance and increased exposures, but SBECD continues to exhibit a good safety and tolerability profile in IV formulations.“
Now, the above is not the only “New York Times” style trick that NIH plays here.
Let me list, without going into long-winded explanations, my additional favorites.
The table authors note that clinical drug-drug interaction studies have not been done, but nonetheless, they say “CQ or HCQ may decrease the antiviral activity of RDV; coadministration of these drugs is not recommended.1” – with a hanging reference.
For three OTHER potential drug interactions, communications from Gilead are cited as sufficiently exonerating. One is a non-competing generic steroid (dexamethasone) and the other two are patented big pharma antivirals from corporate “frenemy” Genentech. The interaction and “C-level mind-melding” between these two companies is very interesting. Look who just went from one to the other. Interesting times.
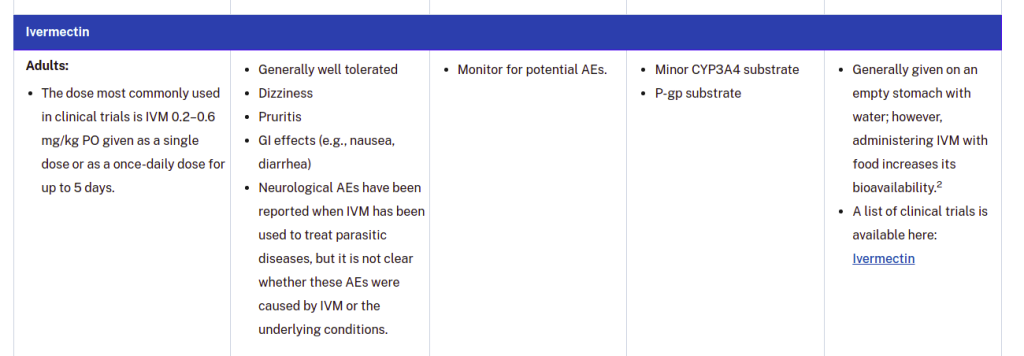
Some crafty shade is thrown at ivermectin by citing a possible adverse event risk and then retracting it, lawyer-style: “Neurological AEs have been reported when IVM has been used to treat parasitic diseases, but it is not clear whether these AEs were caused by IVM or the underlying conditions.” Meanwhile, the DEMONSTRATED risks of remdesivir are not even mentioned.
Bottom line – NIH is protecting Gilead on the toxicity of remdesivir, and they used FAKE NEWS tricks to do it. I keep telling people – science journalism is bad, and science governance is WORSE. It’s been CHINATIZED and OBAMATIZED.
And until there IS justice, we will drag the CRIMES of Anthony Fauci and Gilead “Pharmaceuticals” and their SLEAZY ASSOCIATES thorough the headlines, over and over, until people SPIT IN THEIR PATH as they walk down the streets.
So where do we begin?
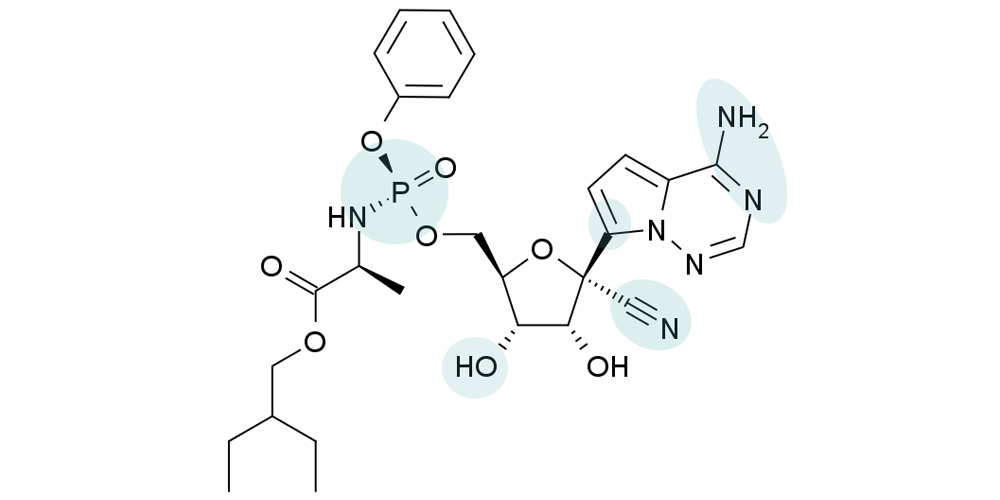
Let’s take a brief look at ZYKLON D.
This is the molecule of remdesivir, a.k.a. Zyklon D (as in DEMOCRAT). This is the drug that is killing Americans – primarily “Deplorables”, in the hospital.
The shading of parts of the molecule is significant, and I’ll get to that in a future article. The shading is more significant in a NEW way, than it was in the original way.
If you remember NOTHING ELSE from this article, remember this.
Hydroxychloroquine, chloroquine, and ivermectin TOGETHER over their entire histories have not killed as many people as remdesivir kills in a SINGLE DAY.
In fact, I’m sure it’s significantly less, but I leave the exact numbers as an exercise.
What’s really nasty there, is that OUR tax dollars are being used to PAY HOSPITALS to murder us with remdesivir. As long as hospitals use this WRONG drug at the WRONG TIME (which I will explain) to kill OLD TRUMP VOTERS, they get money from the federal government.
But if hospitals use the RIGHT drug at the RIGHT time, they don’t get the cash.
So what do HOSPITAL ADMINISTRATORS – who more and more are NOT DOCTORS – do? They do what you EXPECT them to do. They do NOT do the right thing for patients.
(H/T Gudthots and GAB)
This has been a part of the general phenomenon of the “lawyering of science”. Has it made science better?
I don’t think so.
It’s beyond evil, but hey – when you have a mafiosa in charge of not only the purse strings, but the “quiver”, these sorts of things happen.
Impeachahontas Now Wearing Two Diapers Nobody expected Chris Wray to play Mafia Nan’s queen of diapers face-up on January 6, but that is exactly what appears to have happened. The only question now is WHY. To quote a friend from a former life, “AYE-YI-YI!” OK – let me back up a bit. First, I want …
And then there’s the “medical mafia”.
Do you see Trump with his hands tied over there? He had to let that jackass on the left declare that a terrible drug recruited to MURDER old Republicans was “the new gold standard of care”, because the murderer is a member of “SES”, and can’t be fired. The medical mafioso can tell whatever lie he wants, and nobody can do anything about it.
Of course, maybe it IS the “GOLD STANDARD” for DEMOCRATS and HOSPITALS.
Yes, the EVIL in charge of this nation is fairly impressive. Moscow has NOTHING on Washington.
But back to the new “secret euthanasia drug”, remdesivir.
“When you go to a hospital, even if you don’t have COVID-19, you’d be construed that way,” says Renz during his program “Lawfare with Tom Renz” on Brighteon.TV. “They get hundreds of thousands of dollars for putting you on remdesivir, putting you on ventilator and letting you die. And if you don’t follow, they’ll just intimidate you and coerce you.”
His guest on the program, Nancy Ross, has experienced that firsthand. Ross has been given the power of attorney to act on behalf of Veronica Wolski, a known patriot from Chicago who recently died from COVID-19 at AMITA Health Resurrection Medical Center.
Ross says the hospital wanted to intubate Wolski and put her on ventilator, and the doctors kept telling that every time they see the patient. “They kept reminding her of that instead of talking about other possible treatment,” says Ross, referring to the ventilator. “I just couldn’t get it.” (Related: Overreliance on ventilators led to coronavirus deaths, study shows.)
According to Ross, Wolski had been asking the hospital to give her ivermectin but her requests had been repeatedly denied.
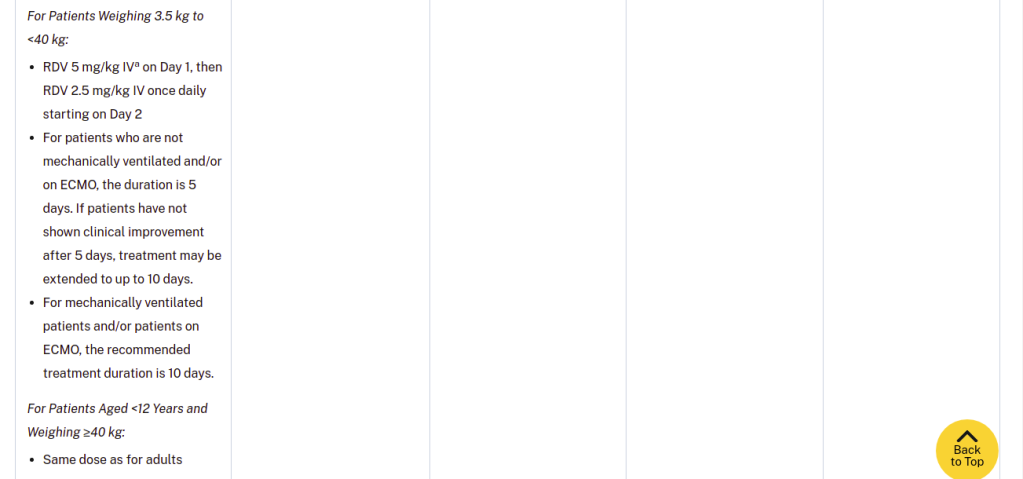
For the uninitiated, the only treatment for the disease approved by the Food and Drug Administration (FDA) involves remdesivir. It is approved for use in adults and children at least 12 years old who weigh at least 88 pounds (40 kilograms).
Remdesivir is an antiviral medication that targets a range of viruses. It was originally developed over a decade ago to treat hepatitis C and a cold-like virus called respiratory syncytial virus (RSV). Remdesivir is not an effective treatment for either disease, but it has shown promise against other viruses.
It works by interrupting the production of the virus. Coronaviruses have genomes made up of ribonucleic acid (RNA). Remdesivir interferes with one of the key enzymes the virus needs to replicate RNA, preventing the virus from multiplying.
However, up to 31 percent of patients who received remdesivir have developed multiple organ failure and/or acute kidney failure. “Remdesivir was pulled from clinical trials because it’s too dangerous. It’s just a disastrous drug,” says Renz.
Doctor admits 99 percent of intubated patients die
Renz also shares a message he has just received about a recording from a doctor admitting that 99 percent of the patients they intubate have ended up dying. “These are just bad treatments. They just kill people,” he says.
Many hospitals are also giving COVID-19 patients with midazolam, which is questionable at best as it depresses a person’s ability to breathe. It is most frequently used before surgeries or procedures to decrease anxiety, cause drowsiness, and help with anesthesia in patients who need tubes or machines to help them breathe.
Midazolam has an FDA black box warning, which notes that the medication has been associated with respiratory depression and arrest because it can slow or stop breathing.
Ross says they also requested to give Wolski the budesonide treatment, but the hospital instead gave the patient a generic brand, which is not the best thing to have under that circumstance.
Wife dodges ventilator, survives COVID-19 with budesonide treatment
A husband from Georgia has had a better success in forcing a hospital to give his wife the budesonide treatment.
The husband named Mick tells Clay Clark during “Thrive Time Show” on Brighteon.TV that his wife has made it out of the intensive care unit two days after getting the budesonide treatment and has been able to go home in a week.
Mick says his wife is in really bad shape after a week of battling symptoms of COVID-19.
“She’s 57, has a partially collapsed lung and has preexisting conditions. Her blood oxygen was 50 and her blood pressure was 100/50,” said Mick. The normal blood oxygen level is between 94 to 99 percent. Anything below 90 is considered to be low blood oxygen.
“I went on battle mode immediately. I thought ‘this is it,’” said Mick, fearing that his wife would be put on a ventilator in which very few patients had survived.
After talking with Bartlett, Mick sends the hospital a fax message asking to put his wife under the budesonide protocol – which is 1 milligram of budesonide every eight hours. He also sends a copy to the doctor treating his wife, as well as a lawyer.
Mick cites several studies and a magazine article about the budesonide protocol, but he thinks that what catches the hospital and the doctor’s attention is his threat of escalating the matter to the ethics committee if they don’t grant his request.
Budesonide reduces COVID-19 hospitalization
Researchers at the University of Oxford has found that early treatment of inhaled budesonide reduced the need for urgent care and hospitalization in people with COVID-19 by as much as 90 percent. The study has also found that inhaled budesonide given to patients with COVID-19 within seven days of symptoms reduces recovery time.
Participants allocated the budesonide inhaler has had a quicker resolution of fever, symptoms and fewer persistent symptoms after 28 days. The study has also demonstrated that there’s a reduction in persistent symptoms in those who received budesonide.
Doctors have prescribed budesonide for more than 20 years as preventive medicine for asthmatics. Bartlett has written a paper with case reports describing favorable outcomes for two of his patients with the regimen. A lab study in the U.S. has also shown that budesonide inhibited the ability of a coronavirus to replicate and inflame the airways.
[Back to Wolf]
If, after reading all that, you’re STILL not suspicious that maybe remdesivir is problematic, then please read my previous article.
I have been a poor and rotten servant of the Lord during my too long and too miserable life. I have made innocent women cry. I have led others astray. I have turned away from those in need in their time of need, and I have lied to myself and to God about why I …
In the prior article, there is a VIDEO that explains how remdesivir WORSENS pneumonia by shutting down the kidneys. The people who killed Veronica with remdesivir are NOT telling you that. They are HIDING the fact that Veronica Wolski was KILLED BY REMDESIVIR, but the effects of kidney-failure-induced pulmonary edema LOOKS like bacterial pneumonia.
It LOOKS like the disease did it, but it’s really the DRUG. Fauci gets away with what he CAN get away with.
He’s not a doctor. He’s an administrator. As his CLASSMATES have said many times.
But let’s say that Veronica Wolski actually DID have real pneumonia – AGGRAVATED by remdesivir kidney shutdown. THAT is exactly why Didier Raoult used AZT along with hydroxychloroquine – as a rapid attack on ANY bacterial pneumonia that might develop. So AGAIN – had Veronica gotten the RIGHT DRUGS right away, she would not have died.
In fact, AZT plus even OTC antihistamines (which prevent pulmonary inflammation) will prevent death by COVID-19, as long as the patients DON’T get remdesivir.
In that previous article I did a very fast proof that hydroxychloroquine (HCQ) works, demonstrated at a national and international statistical level (the “Lancetgate effect”), but I just glossed over Prof. Didier Raoult’s first communication on the efficacy of a combination of hydroxychloroquine and azithromycin (HCQ + AZT) to prevent DEATH by COVID-19.
Here is Raoult’s comment on the uncovering of the Lancetgate fraud. Note that Raoult’s work was never attacked directly (which would have been scientifically suicidal), other than to say that his sample size was “too small” (not in my opinion) when he first communicated his findings.
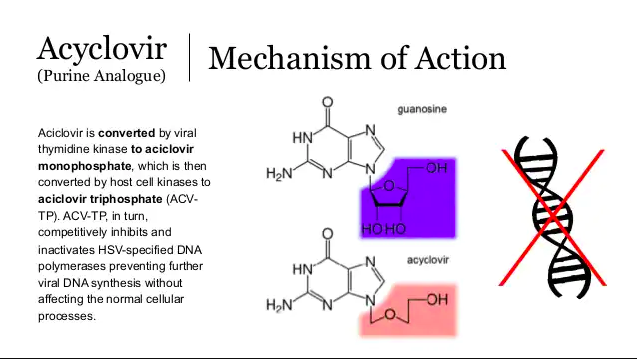
Hydroxychloroquine is NOT a standard antiviral like acyclovir, remdesivir, and most of the other “vir” drugs, which are all based on what can best be described as “ringer” nucleotides, nucleosides, and nucleic acid bases.
Here is acyclovir, which as a “fake nucleoside” is very easy to understand. You can see where the name comes from – it’s an “acyclic” version of guanosine, where part of the ribose ring has been REMOVED.
Now the part they say about “without affecting the normal cellular processes” is NOT actually true. There are plenty of papers on the side effects of acyclovir. Those side effects are not USUALLY all that bad, but they are VERY REAL because acyclovir DOES impact normal cellular processes.
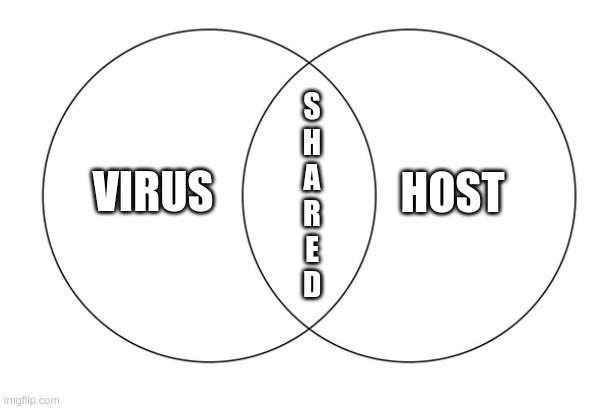
There are VERY FEW drugs which impact ONLY the processes of viruses, cancers, bacteria, fungi, protozoa, trypanosomes, flukes, helminths, ticks, fleas, lice, and other parasites, and do NOT at all impact host (that means US) cellular processes.
In fact, it’s not easy to say WHICH processes are purely HOST processes, and which OTHER processes are parasite processes. Host processes turn into viral processes by their ABUSE, and one of the BEST ways to stop viruses, is to simply stop the HOST processes that help the virus, until IMMUNE PROCESSES have time to identify, target, and DEFEAT the virus.
Under these tactics, the larger organism can WIN by not giving the virus what it needs.
VIRAL DENIAL IS A VALID TACTIC.
I hope that’s clear. Targeting ANY host process which helps the virus, and doesn’t hurt the host too badly when sabotaged, is a VALID way to stop a virus and beat a disease.
Most antivirals work by disrupting viral GENETIC processes, by serving as bogus pieces in RNA or DNA construction. They are like styrofoam or rubber links that create weaknesses in steel chain.
It doesn’t really matter exactly WHEN and exactly WHERE the “vir” type antivirals cause things to fail. They are simply SABOTAGE LINKS in the nucleic acid chains that viral construction depends upon.
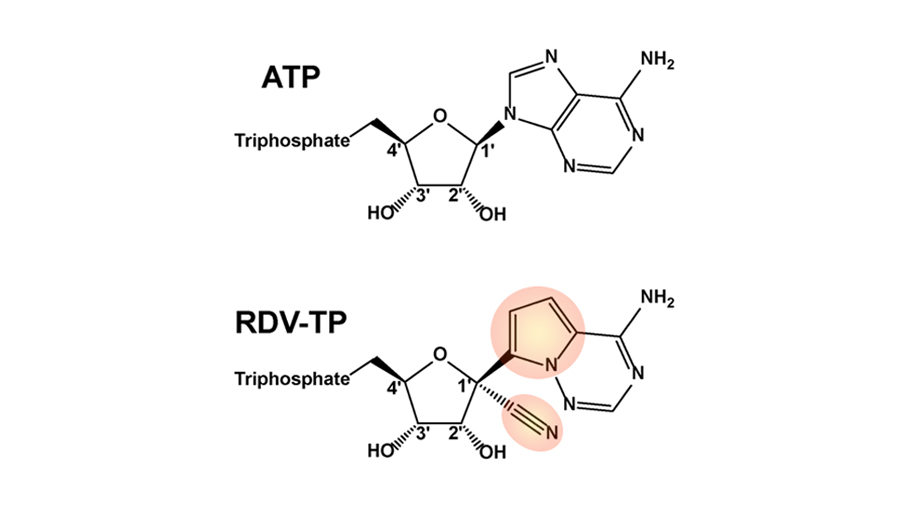
Here is remdesivir’s sabotage molecule:
ATP is adenosine triphosphate – a critical molecule for both genetic construction AND energy transfer.
Remdesivir leads to the construction of a FAKE version of ATP (called RDV-TP above) which has two points of sabotage. One is an added cyano group – the other is an altered ring structure that cannot hydrogen bond properly, because one nitrogen has been removed, and another has been relocated.
It’s too bad that remdesivir is so toxic, but that’s the sad reality of drug discovery. MOST potential drugs have a lot of side effects, and are not all that safe.
Hydroxychloroquine and ivermectin are not all that good as antivirals, in my opinion, BUT they have the GLORIOUS property of being VERY safe. That is part of why they’re considered essential medicines for their normal uses against LARGER parasites (trypanosomes, flukes, helminths, and mites).
BOTH of those drugs have good postulated NON-STANDARD mechanisms of antiviral action – meaning these drug molecules are not bogus genetic building blocks – they disrupt something else. There is some debate on exactly how these drugs work, but it doesn’t really matter, as long as they work.
There are reasonable explanations of how they may work, there is empirical evidence that they DO work, and they are known to be safe at effective doses.
These drugs are SAFE TO USE.
Now – this is where TIME comes into play.
The main problem with remdesivir is that it is used TOO LATE in the viral process. It SHOULD be administered early in the process, on an outpatient basis, like hydroxychloroquine or ivermectin. The reason is fairly obvious. If you attack a virus after it has already multiplied, you can’t stop the damage it ALREADY DID.
REMDESIVIR BOMBS A VILLAGE OF SURVIVORS AFTER THE TALIBAN CAME AND LEFT.
Hydroxychloroquine and ivermectin, administered early, are like sending in a platoon of commandos right after the Taliban shows up.
Which strategy is going to give the most survivors?
This is a no-brainer. You don’t need a Ph.D. to see this. And yet, literally, THOUSANDS of American Ph.D.s cannot SAY this because they’re afraid of losing their jobs, their reputations, or their potential for advancement.
Thankfully, I’m retired, so I can speak the truth.
Now, as a scientist who GETS relative importances, I can see how to FIX remdesivir. I TOLD them how to fix remdesivir in spring of 2020. Let me explain this YET AGAIN.
I take note especially of the horrible record of side effects (especially total kidney failure requiring dialysis and transplant) of remdesivir in hospitalized patients – who get high doses of remdesivir because they have high levels of virus (or low POST-INFECTIVE levels, but again – the people behind remdesivir are not being logical if we take them at face value).
The fact of the matter is that remdesivir has to be given I.V. – it cannot be given orally. That is the EXCUSE for giving it so late.
But IF it was given earlier, remdesivir could be given in lower doses that would probably work just as well as HCQ or ivermectin.
That is all that is needed. Protect people from death. Less drug because less virus. Less side effects because less drug. And it’s not like a doctor’s office can’t administer a lower, safer, yet STILL intravenous dose of remdesivir on an outpatient basis. EARLY.
They never did this.
Why not?
Now, I believe it’s because curing people with remdesivir was NEVER the intent of the primary conspirators.
Profit, obviously, for many participants, is the “legitimate” motivation. But there is more.
Secret euthanasia of “useless eaters” with remdesivir WAS their intent. And that “authority” to inject people (either literally or practically) against their will requires a hospital setting. The hospital setting creates the EXPECTATION OF DEATH – and that is how they get away with it.
The people who COULD have changed things to administer remdesivir when it would have been safer did NOT, because they were either cowardly, brainwashed, politically impeded, monetarily motivated, or part of the actual conspiracy.
SO – bottom line – if you feel that you have to go to a hospital, DO NOT go unless you are assured that your doctor can treat you with drugs that YOUR DOCTOR wants to treat you with, including ivermectin, hydroxychloroquine, budesonide, and antibody cocktails.
These are the things that ACTUALLY WORK. And are ACTUALLY SAFE.