Why would we mass treat a virus with a drug which forces the virus to mutate, when mutation is how the virus creates new variants that reinfect the vaccinated?
Before I explain the title contradiction, let me start with an admission.
Most of my life, I have been very friendly with the pharmaceutical industry. I have eloquently defended Big Pharma, the FDA, “government and corporate medical science”, and all those things that the Biden administration so earnestly defends now.
I even got an award sponsored by one of those Big Pharma companies – which is not to say much, because they give out a LOT of them. In fact, the grooming of young scientists to revere Big Pharma, is no different from the grooming of doctors (and now medical bureaucrats, who know less “talk-back” science) to promote and prescribe their products.
If you go back and look through my posts here, you will see that my thinking about Big Pharma has only evolved slowly from starry-eyed hope and blissful faith. I was quite earnest in my wishes that some of their new products might be better than doctor-discovered, repurposed, off-label drugs like hydroxychloroquine and ivermectin.
What I would NOT do, was deny the obvious effectiveness of those cheap, plentiful, and SAFE doctor-discovered drugs.
If the world was against HCQ, then “Lupus contra mundum” (Wolf against the world).
Why so? Because the DATA on these two drugs killing virus and preventing death was so alarmingly GOOD. You just have to be HONEST and INDEPENDENT to see it. Then, you just ask WHY. And the answers came.
It was BEAUTIFUL. It was SCIENCE.
Even when it was ugly. Like the Lancetgate Effect.


I’m a DATA GUY. I know WHICH data matters and WHICH data doesn’t. I can SEE THROUGH CURVES like a horny guy next to a woman in bed in the dark, seeing her under the sheets. With DATA, I can see through walls. I can see around corners. I have escaped death many times by seeing what nobody else saw.
It’s a gift from GOD, and I don’t waste it.
I really WANTED remdesivir to work, but then I saw the numbers. I could not unsee them. I was forced to admit that the drug DID not work, and COULD not work, in large part because it was being administered too late.
Antivirals work best EARLY, when they have an overwhelming numerical advantage – which is very hard to obtain over an EXPONENTIAL ENEMY. But if you administer early, even ATYPICAL antivirals like hydroxychloroquine and ivermectin, in proper ANTIVIRAL doses, have a chance.
Remdesivir is fairly toxic stuff, and when administered too late, when the virus is long gone, it kills its victims in a way surprisingly similar to what late-stage COVID does, by kidney failure, and then pulmonary dysfunction which looks like pneumonia. So if you administer remdesivir to dying COVID patients, it may not do THEM any good, but it will make YOU a whole lot of money on their deaths, which are thus ENSURED. And YOU won’t get caught doing it, because it all looks like COVID.
SLICK.
And WE have covered remdesivir before.
Remdesivir Is How We Bring Down The Temple of Faucism
NIH and Gilead Blamecasting Remdesivir Renal Toxicity to an Excipient
OAN Hosts Amazing Anonymous Documentary on Discovery and Suppression of Ivermectin for COVID, and How Gilead and Fauci Gamed a Remdesivir Study
And last but not least:
The Murder of Veronica Wolski by Fauci and Gilead’s Zyklon D
There will be justice for Veronica Wolski, because we will DEMAND IT. And until there IS justice, we will drag the CRIMES of Anthony Fauci and Gilead “Pharmaceuticals” and their SLEAZY ASSOCIATES thorough the headlines, over and over, until people SPIT IN THEIR PATH as they walk down the streets. So where do we begin? …
Remdesivir goes really well with murderous vents and no prior therapeutics, and NO, NO, NO ivermectin allowed, which – DO TELL – is exactly how the Stalinist Biden-Obama-Harris administration and its CHINAZI allies kill off us pesky American seniors.
But that’s getting a little ahead of things. We’ll come back to remdesivir.
First – molnupiravir.
Molnupiravir was once called EIDD-2801, back when it was more of a hope and a dream.
I had high hopes for molnupiravir back then. I had hoped it would be a significantly better antiviral than hydroxychloroquine and ivermectin, both of which are antiparasitics first, and antivirals second – and at that, only by a bit of luck. But that LUCK can SAVE YOUR LIFE.
That was back when I didn’t realize how diabolical the people who CONTROL Big Pharma really are – that they would SHIT on a lucky, life-saving break, just for money.
As it turns out, molnupiravir is roughly as good as the cheaper drugs, but definitely not as safe.
Nevertheless, molnupiravir is NEW, it’s PATENTABLE, and it’s a MONEYMAKER. The system is RIGGED, and thus we are DENIED the cheaper, safer drugs, so that our money will fund expensive drug research.
Whatever. That is just the way things are. I didn’t know that, when I was a student. I didn’t realize that the system was actually corrupt. Although the system probably wasn’t as bad back then, either.
Chinese communist ethics have filtered into America, and they have not done Big Pharma any good.


Would I take molnupiravir? Maybe. If I had to pick ONE, it would probably be ivermectin. Second choice, hydroxychloroquine. Third, molnupiravir. I don’t think I would take remdesivir next – I’d probably try acyclovir. That stuff really WORKED for my shingles – TWICE. It might not work on a coronavirus, but at least it wouldn’t kill my kidneys.
Now that you know how I feel about the drugs, let’s talk about WHY I feel that way. But in a roundabout and very telling manner.
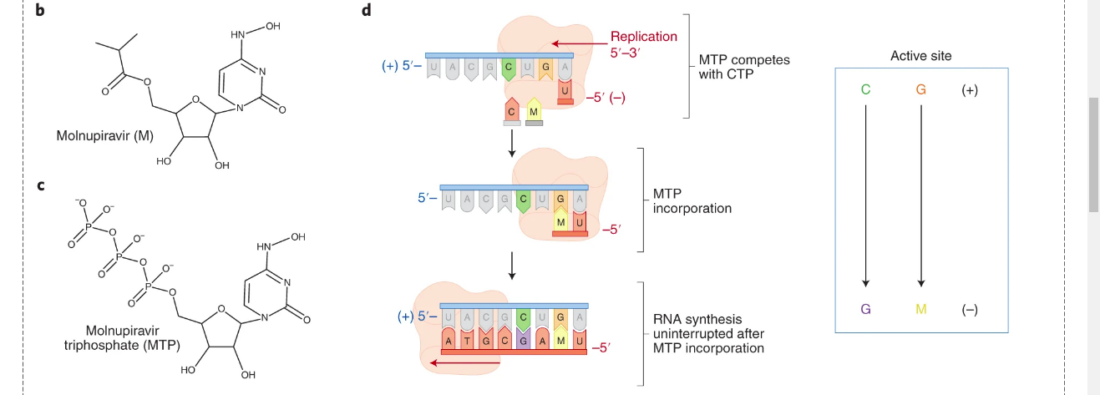
Here is a synthesis of molnupiravir from cytidine – the molecule that it mimics in order to kill RNA viruses, including SARS-CoV-2.
If you look at the molecular structure of molnupiravir above, on the right, you will see two rings. The pentagonal ring with an “O” (oxygen) is a SUGAR ring, and the hexagonal ring with two “N” (nitrogen) atoms is a BASE ring.
Together, those two rings are ALMOST a nucleoside – a component of RNA – called cytidine, shown above on the LEFT, or below.
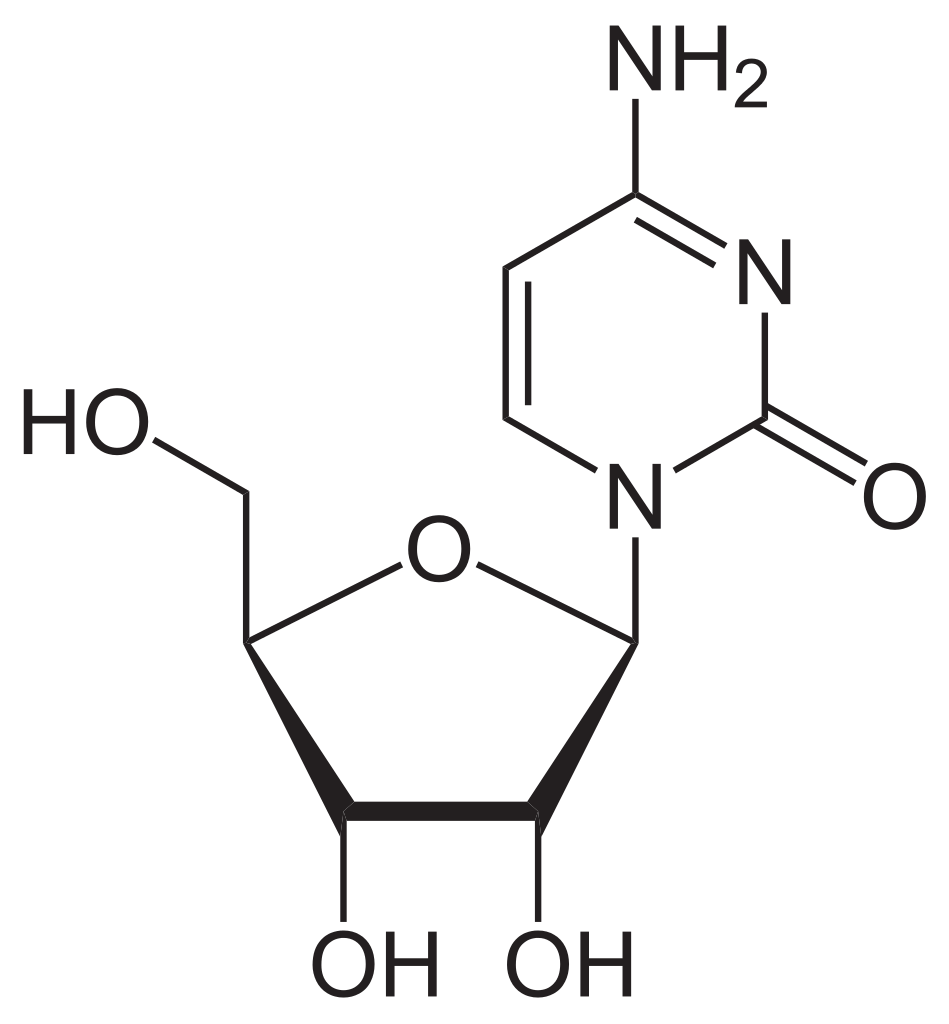
The only real differences between molnupiravir and cytidine, as shown, are the tail on the left of molnupiravir, hanging off the left-hand O group (and which really only helps the delivery of the drug), and more importantly, that extra “OH” group, hanging off the right-hand NH group of the molnupiravir molecule, in the diagram above.
Add that OH group to cytidine, and you have N4-hydroxycytidine (NHC) – the “real” drug being administered, also known as EIDD-1931. Add that little ester tail on the left, to make a nice orally active and bioavailable “prodrug” of NHC, and you have molnupiravir, or EIDD-2801.
That OH group totally screws things up. It’s absolutely AMAZING what that does to the genetic machinery of the virus, inside YOU.
FAKE cytidine, like FAKE NEWS, kills.
There is a great but still fairly technical explanation of how molnupiravir works that was published in Nature, called “Molnupiravir: Coding for Catastrophe“. You can download a PDF of the article HERE.
The abstract is very useful:
Molnupiravir, a wide-spectrum antiviral that is currently in phase 2/3 clinical trials for the treatment of COVID-19, is proposed to inhibit viral replication by a mechanism known as ‘lethal mutagenesis’. Two recently published studies reveal the biochemical and structural bases of how molnupiravir disrupts the fidelity of SARS-CoV-2 genome replication and prevents viral propagation by fostering error accumulation in a process referred to as ‘error catastrophe’.
https://www.nature.com/articles/s41594-021-00657-8
I used part of one graphic from the paper for the feature image of this article. That graphic shows crude, flattened structures of both molnupiravir, and the fully phosphorylated fake nucleotide that gets incorporated into the virus RNA, which is called molnupiravir triphosphate, or MTP.
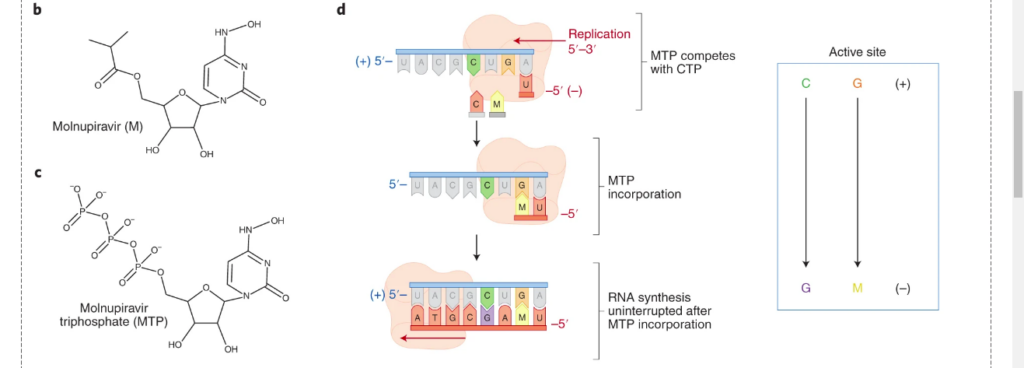
Technically, it’s really not molnupiravir any more, after that prodrug ester gets replaced by a triphosphate unit – it should really be called N4-hydroxycytidine triphosphate. But that pickiness is confusing – MTP is still very true in spirit, and that’s FINE with us big picture types.
Now – THIS is where it all happens. This is where THINGS GO WRONG, and the drug starts to work.
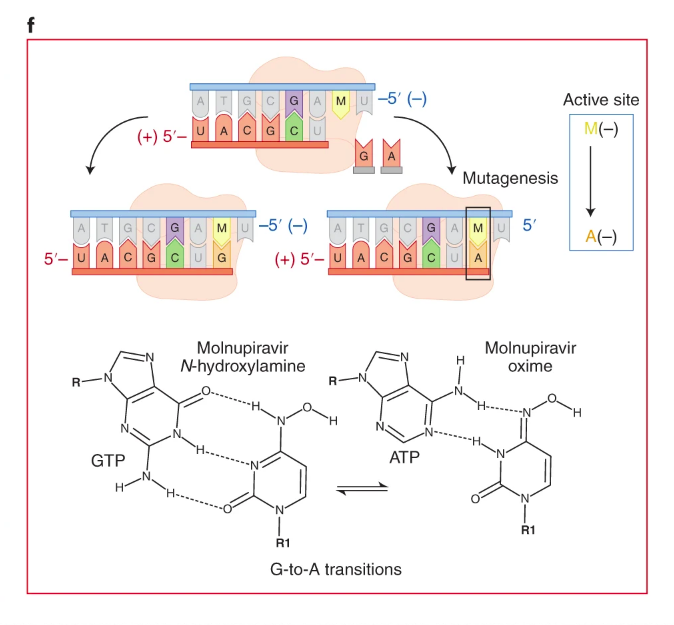
That OH group hanging off the NH of molnupiravir CHANGES the nature of the nitrogen atom to which it is attached, and in a BIG way. Suddenly, the little hydrogen atom that is attached to that nitrogen, would almost rather be located on the OTHER nitrogen in the ring, instead of staying where it is, on the sideshain nitrogen, next to OH. In fact, that hydrogen atom almost stops caring which place it stays. This is a phenomenon called tautomerism. It’s a molecule that can exist in two forms.
One little proton. It’s now happy either way.
But RNA? It ain’t happy.
So what happens, is MTP goes into RNA where CTP should go. And once M is in there where C should be, M can’t make up its mind where that little proton should go. If the machinery sees M with the hydrogen where C would keep it, the machinery does the right thing, and M just gets treated like C. No mutation. But if the hydrogen is in the other place, the machinery thinks M is actually U, and a mutation occurs.
You can see that in this next diagram, where the “hydroxylamine” (-NHOH) form binds correctly with GTP, but the “oxime” form (=NOH) binds INCORRECTLY with ATP.
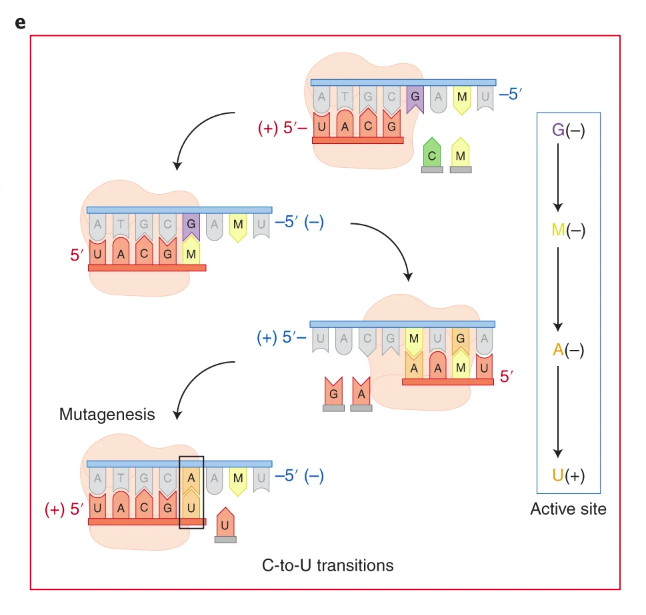
In the next graphic, you can see how M gets incorporated for C, and starts to cause problems by leading to U instead of C. The events shown in the graphic follow a sequence I’ll try to describe.
If you can’t follow it, don’t worry. This stuff is always confusing when you track the changes.
Starting from the top, below……
- one ringer M is already present (top strand), while M competes with C to match the next G (two choices shown waiting)
- the second ringer M goes in on the bottom strand, to match the G, where C should have gone
- the second ringer M (now on top, follow UACGM from left) is then matched with a new A (WRONG) on the bottom, instead of a G (two choices shown). You can also see (and this is very complicated) that the first ringer M was matched with a G (now shown on top), and that G has already matched up to ANOTHER (third) ringer M, now on the bottom strand in the third subgraphic.
- the strand with incorrect A (follow UMAA from right to left on bottom, now on TOP, right to left) is then matched with a U on the second A, completing the screw-up from C to U
- the net effect, bottom strand, is that UACG[C] (top of diagram, what should have happened) became UACG[U] (bottom of diagram, what did happen)
One can look at this whole process as N4-Hydroxycytidine (M) cutting in line where C was supposed to go, and then handing things off to the WRONG base, so that C gets replaced by U.
Complicated, isn’t it? But THAT is how mutations are PROMOTED by this drug, and they are KEY to how it works. There is an AVALANCHE of mutations that kills the virus. The whole idea is that the DRUG makes the virus mutate too much, too fast, into non-viable forms, and it just dies – or at least enough for your immune system to take over and WIN the fight. The virus CRASHES because of the drug. Meanwhile, the body mounts a defense.
You can read the rest of the article if you want, and get some sense of the complexity of considerations as to whether this makes a good drug or not for the individual.
There IS a legitimate question of whether screwing up the RNA of the virus, might also lead to screw ups in the host – either in RNA or DNA, leading to things like birth defects, cancer, adverse events during therapy, etc.
That concern is nicely summarized in a Zero Hedge article:
“Proceed With Caution At Your Own Peril” – Merck’s COVID ‘Super Drug’ Poses Serious Health Risks, Scientists Warn
BY TYLER DURDEN
SATURDAY, OCT 09, 2021 – 05:22 AM
Now, I’m not really interested – for the purposes of this article – in the question of whether or not there are INDIVIDUAL dangers posed by molnupiravir, due to either mutations of the host, OR the forcing of mutation of the virus in that host.
There are excellent reasons to believe, that just like vaccines don’t really pose INDIVIDUAL risks through mutation of the virus in any particular victim, there is no significant individual risk from mutations of the virus due to a mutagenic drug.
HOWEVER, that’s not my concern.
My concern is related to Dr. Geert Vanden Bossche’s concern about mass vaccination during a pandemic. He differentiates between the idea of a vaccine being good for an individual, and that vaccine being good public policy for humanity as a whole, ultimately including that individual.
Geert’s concern is that a virus AS A WHOLE – as a global population – as almost an ecosystem – will evolve due to pressure from a non-sterilizing vaccine, to create new strains that will resist the vaccine. Thus, while the vaccine may benefit an individual in the short term, it ultimately does NOT benefit the sum of all individuals, who will ALL suffer from the mutated virus, which would not have happened, absent the specific evolutionary pressure of the vaccine.
If Geert is right, it’s not just stupid to “vaccinate ourselves into trouble” – it’s downright EVIL.
We have already seen Geert’s prediction apparently (wait for it) fulfilled with the delta strain of SARS-CoV-2, which basically ignores vaccines against “wild type” Wuhan coronavirus.
But again, that is not STRICTLY my concern.
Then what IS my concern?
Original predictions, based on the mutation of the original Wuhan coronavirus, were that the virus was genetically contained – that it was not mutating into significantly different forms requiring changes in the vaccine. And yet, something seems to have CHANGED that. The early predictions could have been WRONG, but they could also have been UNDERMINED. And they could have been undermined by the same terrible logic of “we have to pass it to see what’s in it”, or “we have to try to MAKE the virus catch in human cells, to see if it CAN catch in human cells”.
You see what I mean? There could be “dishonest science” and other such “skulduggery” here, just like we have seen with LIARS like Fauci, Baric, Tedros, and China.
My concern is that in Geert Vanden Bossche’s scenario, which I have described as “coronavirus variant whack-a-mole”, it will only be made WORSE by drugs which encourage the mutation of the virus.
In other words, mass vaccination into a pandemic with “leaky” vaccines is bad, but to do so while chemically promoting the mutation of the virus is even worse.
Thus, not only is it CONTRADICTORY to vaccinate in such a scenario – it is EVEN MORE contradictory to promote mutation in such a scenario.
And – worse than THAT – it appears that we have ALREADY BEEN DOING IT – with remdesivir.

Remdesivir is notable as being an antiviral which is generally being given to patients, with no hope of it actually working, long after the SARS-CoV-2 virus has done its dirty work, and those patients are ACTUALLY dying of a cytokine storm. These patients may still be producing and shedding some virus, but the sum of all studies is rather definitive at this point – remdesivir does little except LENGTHEN the stay of patients in the hospital.
Well, what are those patients doing there, staying too long in the hospital?
One strong possibility is that these dying patients are creating mutants and variants. The following paper shows what happens to SARS-CoV-2 virus when confronted in vitro with remdesivir – and it is basically what I am predicting will happen with molnupiravir.
In vitro evolution of Remdesivir resistance reveals genome plasticity of SARS-CoV-2
https://www.biorxiv.org/content/10.1101/2021.02.01.429199v1.full
ABSTRACT
Remdesivir (RDV) is used widely for COVID-19 patients despite varying results in recent clinical trials. Here, we show how serially passaging SARS-CoV-2 in vitro in the presence of RDV selected for drug-resistant viral populations. We determined that the E802D mutation in the RNA-dependent RNA polymerase was sufficient to confer decreased RDV sensitivity without affecting viral fitness. Analysis of more than 200,000 sequences of globally circulating SARS-CoV-2 variants show no evidence of widespread transmission of RDV-resistant mutants. Surprisingly, we also observed changes in the Spike (i.e., H69 E484, N501, H655) corresponding to mutations identified in emerging SARS-CoV-2 variants indicating that they can arise in vitro in the absence of immune selection. This study illustrates SARS-CoV-2 genome plasticity and offers new perspectives on surveillance of viral variants.
Now this is moderately straightforward, but the big picture is not apparent, because the authors know they are playing with dynamite, so I’m going to restate what they found in more direct language.
Bottom line up front, they basically found evidence that remdesivir does exactly what I’m thinking molnupiravir will do – which is to promote mutation per se, including into “variants of concern”, independently of drug resistance evolutionary considerations, which makes tons of sense.
A mutagenic drug (or rather a drug which works on the principle of mutagenesis) creates mutations with high frequency on a large scale, without the need for evolution to strongly amplify rare beneficial mutations. But at the same time we don’t see – in the wild – any evolution of resistance to remdesivir (RDV). The paper spells this out.
So let’s look at what the study found:
“in vitro with omnipresent RDV” – we see both appearance of variants of concern AND resistance to RDV
“in vivo with late-stage RDV” – we see appearance of variants of concern but NO resistance to RDV
[ The second is a bit of a joke – I’m talking about what we see in the wild globally – no RDV resistance. ]
How can this be rationalized?
In the in vitro case, resistance to RDV is a NECESSITY forced upon the virus. All mutations must persist under omnipresent high concentrations of RDV, so this is a pressure that cannot be worked around or escaped from. Yes, RDV benefits the virus by assisting mutation, despite doing it “too much”, which forces resistance to occur. And what IS the resistance? It is for the virus to continue propagating, both unhindered by RDV yet also assisted by RDV. So, essentially, SARS-CoV-2 and RDV negotiate to the point where the “benefits” of RDV to speed up mutation don’t diminish the viability of the virus. The virus learns to USE the ringer nucleoside M to mutate faster, without dying from it. Thus, we see evolution of traits that have benefited SARS-CoV-2 in the wild, plus evolution of a trait of adaptation to RDV.
In the in vivo case, in a Petri dish called “planet Earth”, resistance to RDV is NOT a necessity. The virus has plenty of hosts who are not using it, so it negotiates more strongly to a better deal. It takes all the mutations it can get from RDV, but it does NOT accept the need to mutate to adapt to RDV. THAT particular mutation is unnecessary for most of the virus, so it is not forced to cut that deal.
Bottom line question: Does RDV in the wild speed up mutation?
My answer: I would bet money on it. It appears to do so in the lab.
And if I’m right, enhancement of mutation should happen even more strongly for molnupiravir, which has a more clearly mutagenic mechanism of action than remdesivir.
The authors simply refer to the plasticity of the VIRUS, because woe unto them if they talked about a Big Pharma drug being a promoter of viral plasticity-COUGH-mutation. But that is exactly what the in vitro results mean here. They were able to generate the “variants of concern” in the lab, using exposure to remdesivir.
They went looking for mutations for resistance to remdesivir, and they not only found one of those – they found MORE mutations, including ones matching “variants of concern”.
WHY?
Well, let’s go back to the original point:
Why would we mass treat a virus with a drug which forces the virus to mutate, when mutation is how the virus creates new variants that reinfect the vaccinated?
In my opinion, it is REASONABLE to expect that any drug which operates as a “ringer” nucleoside – as BOTH remdesivir AND molnupiravir do – is going to cause SOME level of genetic errors – a.k.a. mutations – as a consequence. You can dress up pro and con arguments in fancy language, but scientific common sense points one to the likelihood that a fake nucleoside will operate to some extent, if not to its main extent, as BAD DATA in the tape of life. And THAT means MUTATIONS.
And if remdesivir was doing it, then molnupiravir should do it on STEROIDS.
And I am NOT going to let Fauci explain his way out of this one by any kind of hand-waving, or Shifty-Schiff experiments like Lancetgate.
So where does this go?
I was having a lot of trouble figuring out why the push for remdesivir made sense to a particular PART of the corrupt forces behind the Plandemic.
Remember – AND logic.
In any rally of a giant societal “conspiracy”, which can be as big as:
- “Let’s all go to the New World for each of our own reasons! It’s OURS!”
- “The Islamic world attacked our towers! Let’s DO SOMETHING!”
- “The other people are INSURRECTIONISTS! Arrest them!”
- “White supremacists! Take away their rights!”
- “It’s airborne Ebola! Civil rights out the window! We’re all gonna die!”
…..there is always a REASON for every aspect and for every beneficiary, but they’re usually quite different reasons, specific to the individual or group, and thus profoundly motivating.
In other words, these are “conspiracies of fortune”, in which MOST buy in not in an illegal way, but in either an immoral, amoral, or self-deceiving way. Some truly guilty ones secretly initiate the money-grab, and everybody else goes along, making true justice impossible.
It’s a great scam. It happens for ALL of the reasons – not just any one of them.
Still, in that context, things tend to make sense, but generally after the fact.
The advancement of remdesivir just didn’t make SENSE. More than that, its whole terrible history was wrapped up with the liar Anthony Fauci.
But if you back up even further – a useful tactic when things don’t make sense – one comes to the realization that many things about antivirals just don’t make sense.
- we have good safe ones that “they” seem to hate now, upon their “discovery”
- those drugs were never promoted or studied properly, IMO
- the excuses for not vigorously pursuing the class of drugs BEFORE, ring VERY hollow NOW
- the main class of “allowed” antivirals (ringer nucleosides) seems fundamentally flawed
- the fundamental flaw (that we are using genetic error as a “cure”) is never acknowledged
- the fact that we have to cure diseases that never had to exist, like SARS-CoV-2, fails to outrage any of the people in charge, who pushed these Frankenstein gain-of-function experiments to begin with
- there is a bizarre fixation of vaccines as the only allowed solution to viral disease
- genetic vaccines are pushed, when antigen vaccines are obviously fundamentally safer
- genetic antivirals are pushed, when other categories are obviously both safer AND more effective
The LAST points seem to show some commonality, both in leading toward the massive money pit of gene therapy, and in relating to Anthony Fauci.
And THAT is where things start to make sense. The POLITICAL aspects of this. The installation of World Government, their holy grail.
Fauci, Baric, Daszak, Rick Bright, and Hillary Clinton all know what is actually going on – I am convinced of that. They are all knowledgeable, more than others, in the true agenda and schedule of the “Plandemic”, including the POLITICAL GOALS. They understand both the SCAM and the NOBLE (lying) PURPOSE.
I am convinced that VARIANTS are a key construct in the giant grift of COVID. The whole plan has to keep going, by ginning up more COVID as needed, but it also has to look NATURAL, so that nobody finally decides to send about 100 cruise missiles into Wuhan and a spare 20 into various Swiss cities, which would end this entire Globonazi / Chinazi farce once and for all.
OK. Save some for North Carolina and Canada, too. It’s complicated.
They COULD make more variants and release them, but nobody wants to screw up and get caught, like they already have been caught, time and time again, to the point that the whole Globonazi plan might finally get run down like a rabid dog in the middle of the road.
The fact of the matter, however, is that even with DRASTIC homing in on Baric, Daszak and Wuhan from the left, with Fauci finally treed by BEAGLES, of all things, and the rest of us bearing down on them from the right and center, they keep pushing on. They are NOT going to stop.

Variants have now died down due to the mechanics of immunity, largely due to refusal of so many people to take the immunosuppressing phony vaccines. But THAT can be worked around. Don’t think that variants are gone. They’re TOO DAMNED USEFUL.
So how do you get MORE of them, without a ChiCom release operation, to convince all the CHUMPS in science, who will swear on their various manuals and codexes that it’s all real?
Just give a CURE that makes sure there are MORE variants.
Remdesivir doesn’t WORK well enough. It makes money, because ALL modern operations have to make their own money, but it doesn’t promote mutation fast enough. Nor is it administered during the viral maximum, when maximum mutation is possible.
Enter molnupiravir.
Move variants needed? Sure! And in time for their NEXT political operation, a.k.a. the 2022 election!
The way this scam of vaccines and drugs works is really smart.
The narrow vaccines NARROW humanity’s pool of immunity coverage of the spike protein, while decreasing overall immunity, both broad-based immunity to COVID and to other diseases. Meanwhile, the drugs WIDEN the shotgun pattern of the spike to find new variants that evade the vaccines.
This is such an incredibly slick grift, I almost have to applaud it. BRAVO! Satan himself has to be IMPRESSED. New diseases hidden in cures for old ones. And all of it helping to achieve the socialist goal of transforming mankind PER SE.
Before this is over, as they begin to move the increasingly narrow coverage genetically, even the original Wuhan strain will become a “variant of concern” for vaxxies! Ah, what a beautiful SCAM. The irony!
Note that this explains why HCQ and ivermectin cannot be used. They dead-end the scam. One has to have something that completes the “scam cycle” of increasing the problem while pretending to fix it.
This is their modus operandi. They find something that looks like solving a problem, that actually perpetuates the problem, or creates a new and similar one.
Just like “pursue gain of function to prevent gain of function” – which scam was revealed by Judy Mikovits.
If you find Democrats like Fauci anywhere NEAR one of these cyclic grifts, you know you’ve identified a scam correctly.
You have found something communist.
And now you break it.
W
LINK: https://popularrationalism.substack.com/p/the-extraordinary-hypocrisy-of-molnupiravir