“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
The brown recluse is related to several other recluses, and a couple of other families of spiders, that all have a similar venom – a protein called sphingomyelinase D. This is an enzyme that degrades animal tissues, and is responsible for the very distinctive giant-pock-mark-wound-forming symptoms of recluse bites. The brown recluse does not have as much of this protein in its venom as do some other recluses. The worst recluse, distributed over several countries in South America, has roughly ten times as much sphingomyelinase D as the North American brown recluse. Bites by THAT recluse not only result in deep wounds – they result in SYSTEMIC effects much more often than do bites of the “mere” brown recluse. Fatalities are much more common.
But just stop and think – THAT is how potent protein venoms can be. The tiny bite of a spider with a tiny bit of a protein in it – mere micrograms – can leave a 10-inch hole in the leg, with life-threatening systemic effects.
Snake venoms use different proteins from spiders in their venoms. Some spiders like the black widow have neurotoxic venoms, which affect nervous function, and some snakes like cobras have DIFFERENT neurotoxic venoms.
The honey badger is, weirdly, somewhat immune to the paralyzing neurotoxic cobra venom (jump to near the end of the video).
Many snakes have hemotoxic venoms, and THOSE venoms tend to cause cardiovascular problems. Interestingly, one of those problems is a somewhat rare clotting disorder called thrombocytopenia.
Thus, when I heard that this uncommon symptom was sometimes occurring as a coronavirus vaccine adverse effect, I suspected that there might be a protein cause – the spike protein – acting similarly to proteins in those hemotoxic snake venoms.
If that were the case, we should expect the same effect to be caused by COVID-19 itself, sometimes.
Should we just jump on such an analogy? One that is based on the ASSUMPTION that the spike protein is causing thrombocytopenia? Or at least similarly involved in the two cases?
Let’s think about this.
One of the things which is most fascinating about the BRANCH COVIDIANS – including the high clergy in government and media – is just how STRONGLY they tend to discourage alternative perspectives on COVID-19 – doing so in a way which is alarming even by the normal standards of narrative-setting and enforcement.
For example, at the very beginning, social media gatekeepers were needlessly hostile to Dr. Cameron Kyle-Sidell’s “high-altitude sickness” perspective on COVID-19 hypoxia, despite the fact that this led to a very beneficial new policy on keeping patients OFF vents, probably saving millions of lives, as well as giving us all a better understanding of HOW COVID-19 is and (more importantly) is NOT damaging lungs of patients.
Millions of lives. Think about it. Not a bad save – unless you want a guy named Trump GONE by any means necessary.
Now, some of these “different” perspectives can and do lead to non-working or just plain wrong theories at a micro-level, but so can ANY perspective. Dr. Kyle-Sidell’s ideas led to a variety of hemoglobin-related and malaria-related theories of COVID-19 which were neither fundamentally true nor useful, and which theories died on their own, without any need for censorship, but which were part of a questioning movement which also led to increased recognition of the endothelial nature of the coronavirus attack on patients’ lungs and other organs.
A CHANGE in perspective which WAS and IS fruitful.
Whether we are talking about damage to capillaries in the lungs, vein occlusions in the retina, or organ damage, particularly in the heart or kidneys, it appears that the cardiovascular endothelium is where COVID-19 does the most damage.
Comorbidities which already involve damage or potential damage to blood vessels – particularly diabetes and endocrine or cardiovascular diseases – are thus particularly dangerous, as SARS-CoV-2 and (presumably) its spike protein – which is what attacks cells – would be attacking an already weak point of failure.
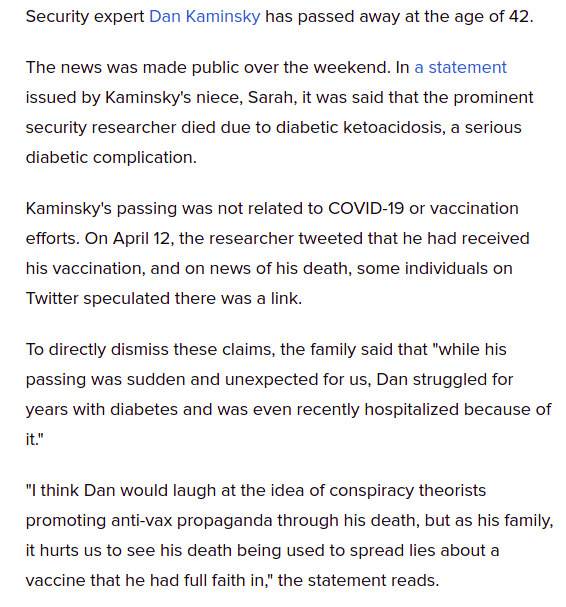
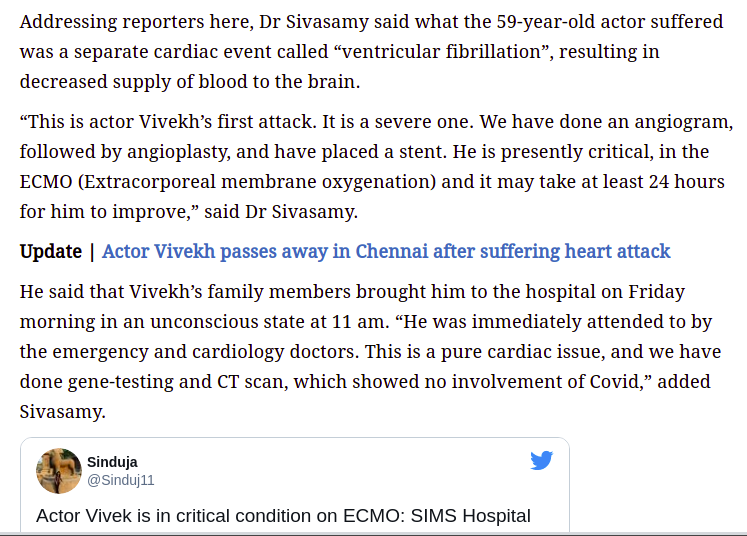
I want to thank GrandmaInTexas for those two most recent examples of COVID vaccinations precipitating fatal outcomes in people with both diagnosed and undiagnosed comorbidities. For the record, Dan Kaminsky’s vaccine was undoubtedly either Pfizer, Moderna, or Johnson+Johnson, while Actor Vivekh’s vaccine was Covaxin. The former 3 are all genetic vaccines – the latter is inactivated whole virus. All of them use the WHOLE spike protein in some form or another to trigger immunity.
Here is a handy principle which I call “spike protein equivalence”, as a special case of “vaccine immunological equivalence”.
If some affliction, condition, or mere FACTOR happens to be BAD for a potential victim of COVID-19 itself, then it’s also going to be bad for recipients of the vaccine. The difference is only that – most likely – in MOST cases – the vaccine constitutes a far lighter assault on the patient, than the disease itself.
THAT is the basic logic of vaccination. REDUCE THE RISK. But nonetheless, ACCEPT A RISK.
Do not kid yourself. The WHOLE POINT of vaccines is to entertain a lesser risk – a risk that is not as bad as the disease. The only question is “how less bad” does any particular vaccine happen to be. Based upon that information, one has INFORMED CONSENT.
People need to understand risks clearly in order to take those risks smartly.
Or NOT take them. Where the lyric“If you choose not to decide, you still have made a choice” operates against the circling helicopters of COVID-19 and any successor viruses.
When we do not honestly face the risks and benefits of vaccines, we end up with the psychotic disconnect we now see, where people who SHOULD be voices of reason and trust – like the CDC – are LYING and losing half or more of the nation as trusting followers.
Rather than re-hash here how the CDC has lied to us already, or why the handy principles of “spike protein equivalence” and “snake protein analogy” work so well in understanding COVID disease and vaccine risks, let me give you links to my most recent discussions of the relevant thought.
The FIRST ONE is probably the most comprehensive, and helps to understand the rest.
PREFACE I thought that I might withhold this post on Easter Sunday, and then I changed my mind, thanks to Deplorable Patriot, Trump, Gab and Jesus. If anybody ever FOUGHT on Easter Sunday, it was Christ. It’s time to FOLLOW POINT. The Branch Covidians have taken a toll, but the WAR is turning, and – …
Alternate Title: Is Persistent Reverse Transcription a Hidden Virus/Vaccine Objective? Gloating Pre-Preface There are few feelings of satisfaction like opening up the NEWS and knowing one’s theories and understandings are WORKING even better than one thought. Let’s see if they use this one for damage control, and get the “new science” out before the STORY …
Every coronavirus vaccine so far has shown us SOME defect upon mass release, which was NOT evident in EVEN phase III clinical trials. Look HERE for a searchable PDF document of adverse effects from the Pfizer vaccine: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/977005/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print.pdf Check out these videos on the low-platelet clotting problem from the Oxford/Astrazeneca vaccine. Here is a fantastic …
I saw an excellent explanation of the clotting problem with the AstraZeneca vaccine against SARS-CoV-2 / COVID-19 here: The doctor, Dr. ZDogg, MD, offers an exceptionally clear explanation of both what is going on with the AstraZeneca vaccine, and why its distribution was halted or limited in some places for some age groups of patients. …
I am not the only person who is seeing that the SPIKE PROTEIN and variants are interesting beasts. Cthulhu tipped me off to THESE TWO GEMS by Karl Denninger, which are extraordinarily worthwhile:
Even though these deal primarily with spike protein equivalence rather than the snake protein analogy, the latter of which Cthulhu mentioned in his tip (he knew I would like these), there is some even more shocking perspective in the second link, in which Denninger simply asks – why did we use the WHOLE sequence of the spike protein which we received from China?
Beyond simple blame games, in which I could postulate that “whole spike protein vaccines” may have resulted from dumb psychology, or even malicious treachery by one or more parties, I can ALSO place Denninger’s question in the context of both failing to ask “Stoecker questions” about “should we base vaccines on the WHOLE spike protein?”, AND the idea that – intentionally or unintentionally – by whoever – we essentially fell into China’s version of the plot of Species…..
OR – if we don’t want to be all negative about things, try the Earth-saving genetic sequence reconstruction sub-plot of The Fifth Element, with a few more plot devices about process-skipping on the internal growth code, also a bit of a lesson.
Is such “gain of function” good or bad? One could view horsepox-based smallpox vaccine adoption as “gain of function” – a low-level example of the intelligent acceleration of evolution as a “natural” part of evolution itself.
As an aside, IMO the reason they use women for these scenes is ultimately the same reason the spike protein seems to target women’s physiology more than men’s, and that men are actually the first utilitarian sex robots, but – well – it’s so simple, it’s complicated. Patriarchy is both overrated and overstated, shall we just say.
ANYWAY, back to snakebite. “Cleopatra meets spike protein” – only worse.
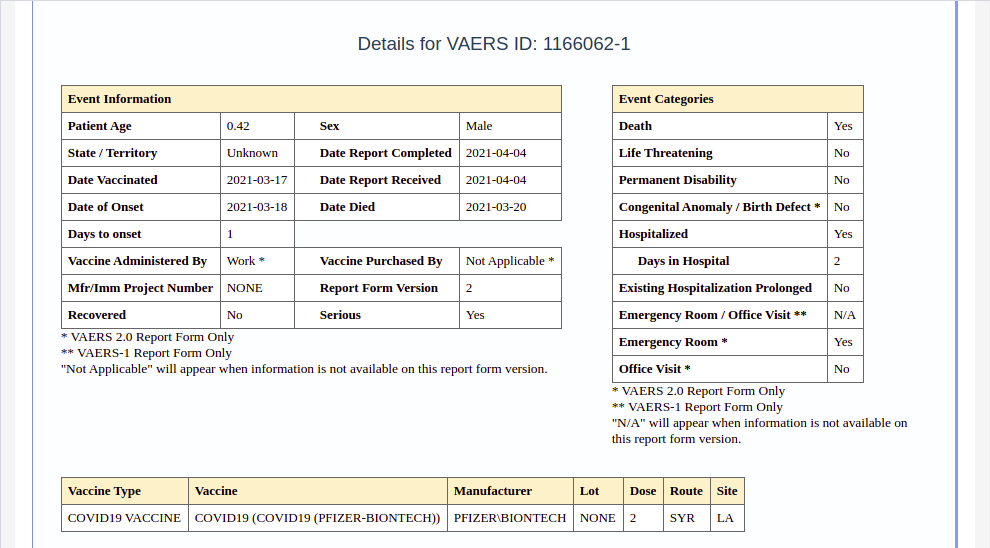
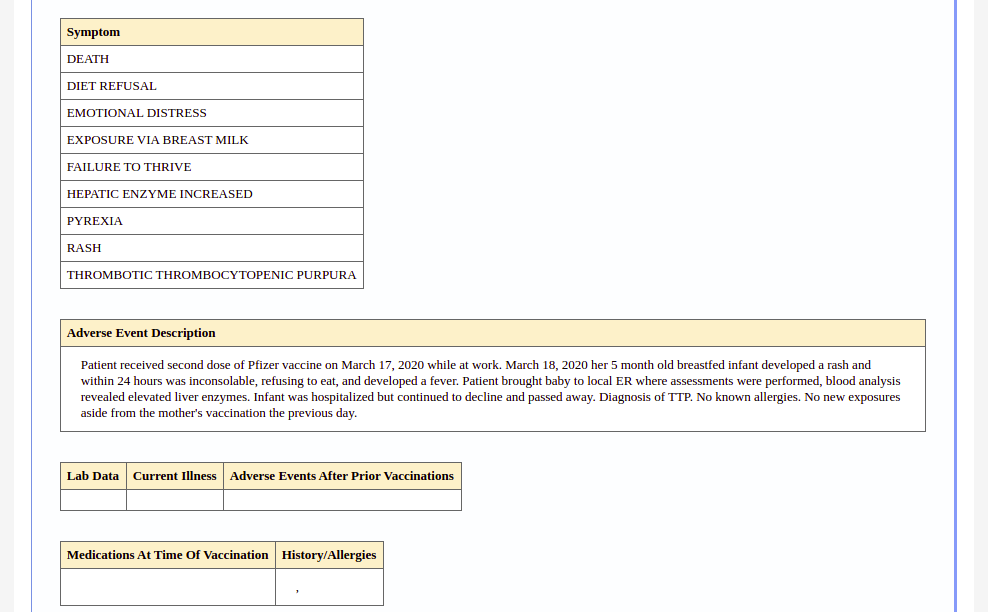
VAERS reports a breastfeeding five-month old infant has died of TTP – a rare clotting disorder linked to, yes, low platelets. He became ill one day after his mother received her second @pfizer shot.
I actually saved that whole report, which is not easily linked, as a series of images:
Before I go on, let me just say that immunology strikes me as a lot like quantum mechanics. If anybody says they truly understand it, it’s almost a sign that they don’t. Nevertheless, basic suspicions work like crazy in either field, which is, again, interesting. In either field, it doesn’t take a genius to see that – 99% of the time – a snake in the grass IS a snake in the grass.
Already, the entire Snopesian Empire is fired up over this case.
SEEK anything related, and you will FIND – both WHEAT and CHAFF.
READ, and you will FIND – both INTERESTING and HOLLOW.
No matter how many guns they get working and belt-fed, cross-firing with their diversionary strawman arguments on this one case, the fact of the matter is that TTP is intimately linked to immune disorders, immune responses, and vaccination, so if it shows up, vaccines are and will remain the likeliest suspect NO MATTER WHAT. All Fauci’s horses and all Pfizer’s men are not going to get rid of the NOTABLY MANY cases of TTP , other thrombocytopenic clotting disorders, and clotting disorders in general, which are showing up in (1) COVID cases, (2) COVID recoverees, (3) vaccination adverse events, and (4) vaccination of recoverees in particular.
The relationship of TTP to vaccines and “malappropriate antibodies” in particular is UNDERSTOOD SCIENCE. This is not going away, despite the near-dogmatic narrative that “COVID vaccines do no harm” at the public level, reinforced by the narrative that “fighting vaccine hesitancy is worth LYING about adverse effects”.
No, it’s not.
Skip the following scientific review unless you feel nerdy. I recommend just skimming in either case. But I promise – the deeper you dig here, the more WHEAT you will find.
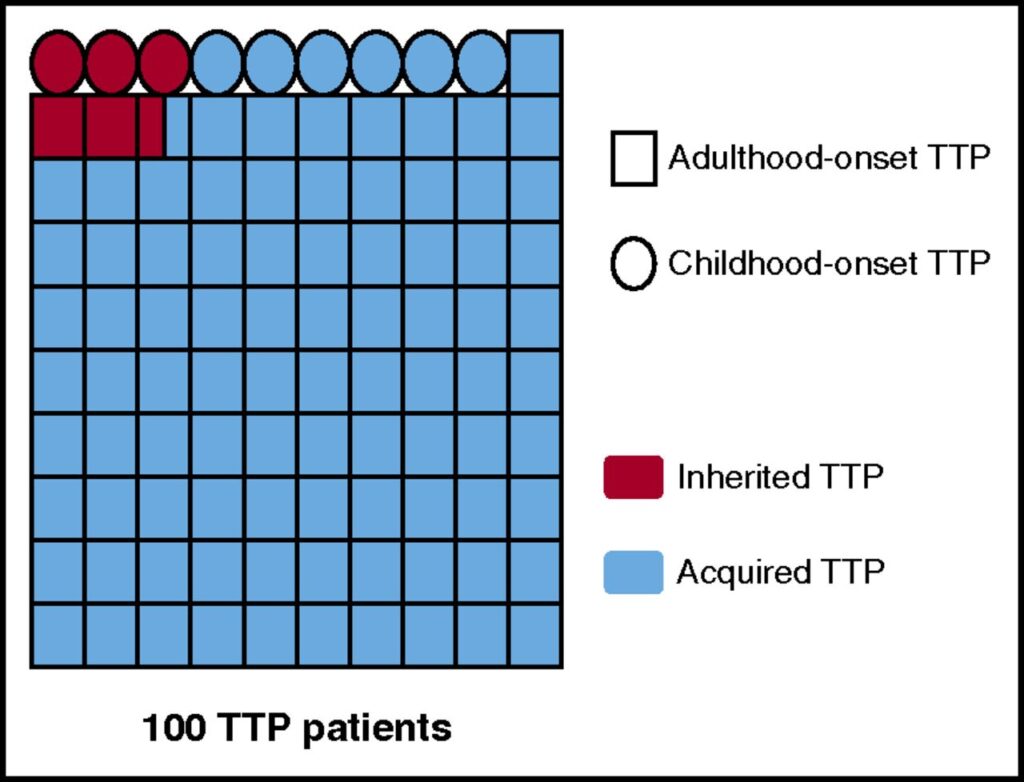
TTP as a function of age of onset and mechanism for ADAMTS13 deficiency. The proportions of adulthood-/childhood-onset TTP and acquired/inherited TTP, respectively, presented in this figure were calculated from the data of the French Registry for TTP (840 patients).10,13 These data are in agreement with miscellaneous demographic data reported in the literature by other teams.3,5-9 The diagram shows 100 patients with TTP, each patient being represented by a symbol, either a square for patients with adulthood-onset TTP (91%) or a circle for patients with childhood-onset TTP (9%). Acquired TTP is presented in blue (94.5%), and inherited TTP (USS) in red (5.5%). Interestingly, the proportion of USS is very low (2.5%) in adulthood-onset TTP, whereas it is as high as 33% in childhood-onset USS.
Abstract
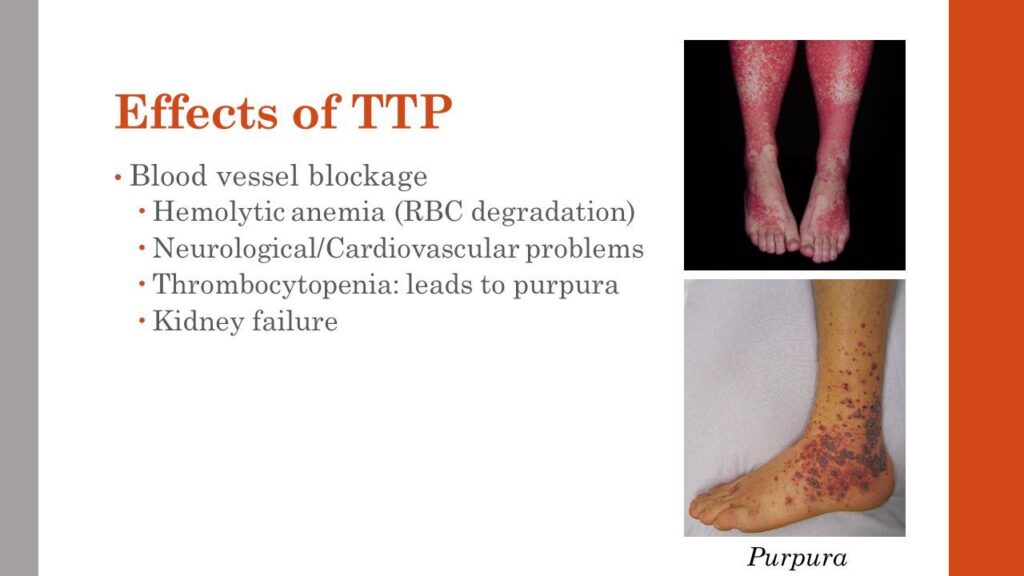
Thrombotic thrombocytopenic purpura (TTP) is a rare and life-threatening thrombotic microangiopathy characterized by microangiopathic hemolytic anemia, severe thrombocytopenia, and organ ischemia linked to disseminated microvascular platelet rich-thrombi. TTP is specifically related to a severe deficiency in ADAMTS13 (a disintegrin and metalloprotease with thrombospondin type 1 repeats, member 13), the specific von Willebrand factor-cleaving protease. ADAMTS13 deficiency is most frequently acquired via ADAMTS13 autoantibodies, but rarely, it is inherited via mutations of the ADAMTS13 gene. The first acute episode of TTP usually occurs during adulthood, with a predominant anti-ADAMTS13 autoimmune etiology. In rare cases, however, TTP begins as soon as childhood, with frequent inherited forms. TTP is ∼2-fold more frequent in women, and its outcome is characterized by a relapsing tendency. Rapid recognition of TTP is crucial to initiate appropriate treatment. The first-line therapy for acute TTP is based on daily therapeutic plasma exchange supplying deficient ADAMTS13, with or without steroids. Additional immune modulators targeting ADAMTS13 autoantibodies are mainly based on steroids and the humanized anti-CD20 monoclonal antibody rituximab. In refractory or unresponsive TTP, more intensive therapies including twice-daily plasma exchange; pulses of cyclophosphamide, vincristine, or cyclosporine A; or salvage splenectomy are considered. New drugs including N-acetylcysteine, bortezomib, recombinant ADAMTS13, and caplacizumab show promise in the management of TTP. Also, long-term follow-up of patients with TTP is crucial to identify the occurrence of other autoimmune diseases, to control relapses, and to evaluate psychophysical sequelae. Further development of both patients’ registries worldwide and innovative drugs is still needed to improve TTP management.
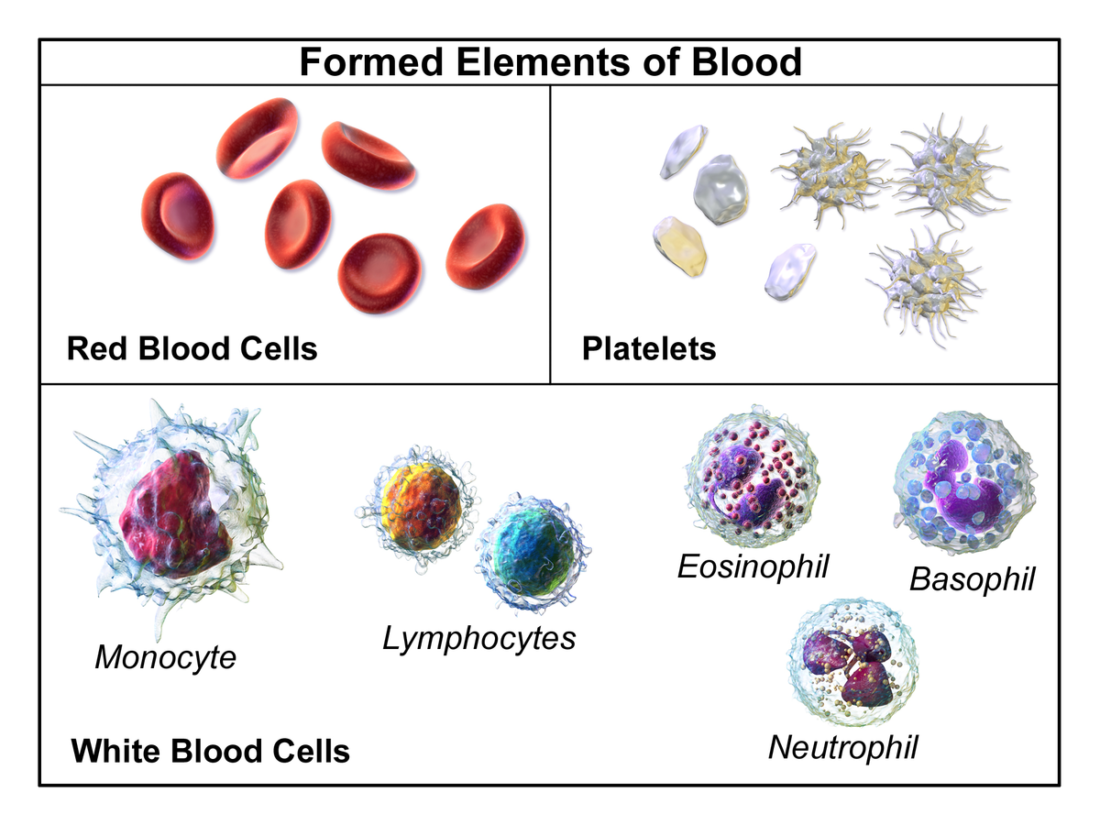
So what does TTP look like?
See those pictures? You may want to THINK TWICE about the coronavirus vaccine if you ALREADY have this risky potential outcome of either the disease or the vaccine. I have a link showing that TTP is a high risk in COVID recoverees who get any of the vaccines – I just can’t find it now.
We ARE seeing some public recognition of adverse effects now:
However, as is visible in this article, we are not seeing ANY contraindications to vaccination being admitted publicly. The advice tends to be “get vaccinated, and if you don’t die, but have bad symptoms, see your doctor.
“Sure, Dr. Stalin. Sure. Say – you don’t have any recommendations to PREVENT THIS from happening again to somebody else now, do you? Those would be called ‘contraindications’. Most drugs have them.”
However, I think some recognition is coming. And why is that? Well…..
“When the people have any power to object to a socialist solution, a deniable 5% fait accompli is always more desirable to socialists than a negotiated 50% solution, because they can always negotiate on the remaining 95%.” -Wolf Moon When I first heard about a case of a miscarriage by a pregnant doctor, due to …
…..we discussed other disorders – affecting reproductive health, you might say – that MAY or MAY NOT be mediated through the SAME or DIFFERENT activities of the spike protein.
THAT is an interesting question, actually. How economic is spike protein activity? How MUCH strategic information is carried, and at what density? How efficient ARE proteins at carrying smaller-molecular strategies into “genetic warfare”? We may not have those answers yet – and certainly not in PUBLIC SCIENCE – for some time.
Still, I think these questions will eventually be asked and answered, because the menstrual/gestational and clotting effects of the vaccines are so startling, that people are going to ask questions and get answers, whether the “mainstream” (meaning government/corporate) media wants to ask them or not, or to see them answered.
In that regard, we will carry on, asking questions and getting answers, carrying the principle of SPIKE PROTEIN EQUIVALENCE with us, as a handy and useful physiological tool.
The idea of SNAKE PROTEIN ANALOGY will become less of a medical utility, and more of a METAPHOR.
There is a refreshing honesty and innocence in this guy’s work. But more than that, he just has a way of catching small details that everybody else misses, and making them beautifully prominent. His portraits of famous figures are quite wonderful in this way. He will completely drop many of the features of those people that I love and see prominently as part of my personal recognition algos, and yet childishly play up awesome things I never noticed.
And with that, let’s talk about Eve.
Our next installment is going to go BACK IN TIME, and show you something very startling about WHEN all this COVID vaccine technology was actually invented.
A lot earlier than anybody wants to admit publicly. Here is a hint.
I saw an excellent explanation of the clotting problem with the AstraZeneca vaccine against SARS-CoV-2 / COVID-19 here:
The doctor, Dr. ZDogg, MD, offers an exceptionally clear explanation of both what is going on with the AstraZeneca vaccine, and why its distribution was halted or limited in some places for some age groups of patients. He has a REALLY GOOD explanation of relative risks, so you can understand why the decision was made to limit, at least temporarily, distribution of the AstraZeneca vaccine, in various countries.
One important thing that Dr. ZDogg notes, is that – because the Johnson+Johnson vaccine is similar to the AstraZeneca vaccine, both being DNA vaccines and both being adenovirus vector vaccines, it is possible that the J+J vaccine might also have the same rare side effect as the AstraZeneca vaccine. This possibility is now being scrutinized carefully.
I mentioned the above video in my previous post on the Johnson+Johnson vaccine:
Every coronavirus vaccine so far has shown us SOME defect upon mass release, which was NOT evident in EVEN phase III clinical trials. Look HERE for a searchable PDF document of adverse effects from the Pfizer vaccine: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/977005/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print.pdf Check out these videos on the low-platelet clotting problem from the Oxford/Astrazeneca vaccine. Here is a fantastic …
In that post, I noted that one critical difference between the AstraZeneca vaccine, which uses DNA and viral vectors, and the Johnson+Johnson vaccine which uses the same, is that the AstraZeneca vaccine also does NOT use the “2P mutation” in the spike protein, which almost everybody else among the early players (Pfizer, Moderna, J+J, Novavax) does use it.
That would seem to potentially suggest that the problem of vaccine-induced thrombotic disorders could be limited to the AstraZeneca vaccine.
Well, first of all, it looks like the J+J vaccine also has the clotting problems.
…..suggests that there MAY be something LIKE the AstraZeneca problem, known as vaccine-induced prothrombotic immune thrombocytopenia (VIPIT), going on with BOTH Pfizer and Moderna.
This case was actually covered by the Daily Mail in blaring headlines on January 6 and 7, 2021. Kind of obvious NOW why this got memory-holed!
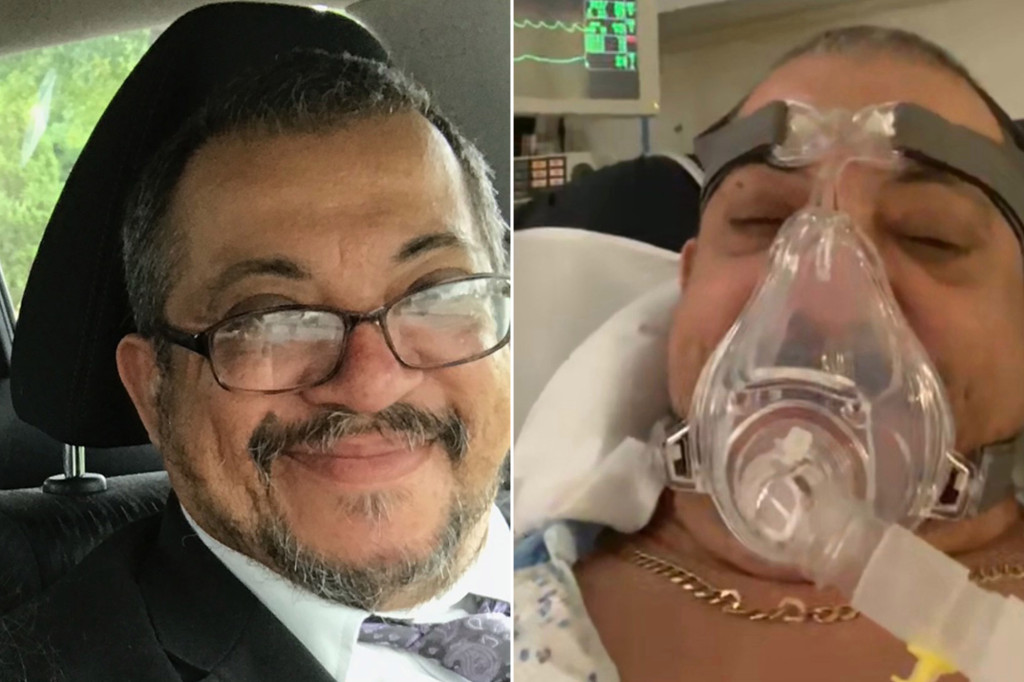
EXCLUSIVE: Wife of ‘perfectly healthy’ Miami doctor, 56, who died of a blood disorder 16 days after getting Pfizer Covid-19 vaccine is certain it was triggered by the jab, as drug giant investigates first death with a suspected link to shot
Beloved Miami obstetrician Gregory Michael, 56, died following a suspected catastrophic reaction to the Pfizer Covid-19 vaccine, DailyMail.com can reveal
Heidi Neckelmann says her husband was completely healthy until he had the jab on December 18 at Mount Sinai Medical Center
He succumbed this week to a stroke brought on by acute IDP – Idiopathic thrombocytopenic purpura – a blood disorder caused by a lack of platelets
IDP can be acute or chronic, lasting six months or more, striking on its own or in conjunction with other autoimmune conditions or certain cancers
Heidi insists, however, that her husband did not have an immune disorder or any similar condition that could have caused ITP
The mother-of-one said: ‘In my mind his death was 100 percent linked to the vaccine. There is no other explanation’
She said: ‘My husband had conversations with the doctors who said it was highly probable that the vaccine was the cause’
If his death is linked directly to the vaccine, Michael would be the first known case in the world of a person dying after the injection
A spokesman for Pfizer told DailyMail.com the firm was looking into Gregory’s death but they did not believe it had any link to the vaccine
PUBLISHED: 18:54 EDT, 6 January 2021 | UPDATED: 12:16 EDT, 7 January 2021
Despite the bad timing earlier, it’s getting a lot more attention now.
There may also be other problems with the Pfizer vaccine that are being lost simply due to the ages of the patients.
CNA Nursing Home Whistleblower: Seniors Are DYING LIKE FLIES After COVID Injections! SPEAK OUT!!!
HealthImpactNewsPublished January 26, 2021 303,563 Views SUBSCRIBE SHARE
It’s definitely time to look at the data in hand, very carefully.
This is going to help us all look at relative risks properly now, IMO.
John Fink and James Coburn discuss case in a scene from the film ‘The Carey Treatment’, 1972. (Photo by Metro-Goldwyn-Mayer/Getty Images)
It’s going to help us understand what’s really going on.
Title: CAREY TREATMENT, THE ¥ Pers: COBURN, JAMES / AUBREY, SKYE ¥ Year: 1972 ¥ Dir: EDWARDS, BLAKE ¥ Ref: CAR019AF ¥ Credit: [ MGM / THE KOBAL COLLECTION ]
And that’s a good thing.
W
John Fink, James Coburn, and Jennifer O’Neill having a meal in a scene from the film ‘The Carey Treatment’, 1972. (Photo by Metro-Goldwyn-Mayer/Getty Images)
Check out these videos on the low-platelet clotting problem from the Oxford/Astrazeneca vaccine.
Here is a fantastic explanation of the AstraZeneca problem and what people are doing about it.
You will note that Dr. ZDogg, MD points the J+J vaccine being at risk of having the same clotting problem as the AstraZeneca vaccine, due to them BOTH using DNA (as opposed to mRNA) and viral vector (as opposed to liposome) delivery technologies.
I just learned something today from C&EN that may impact this.
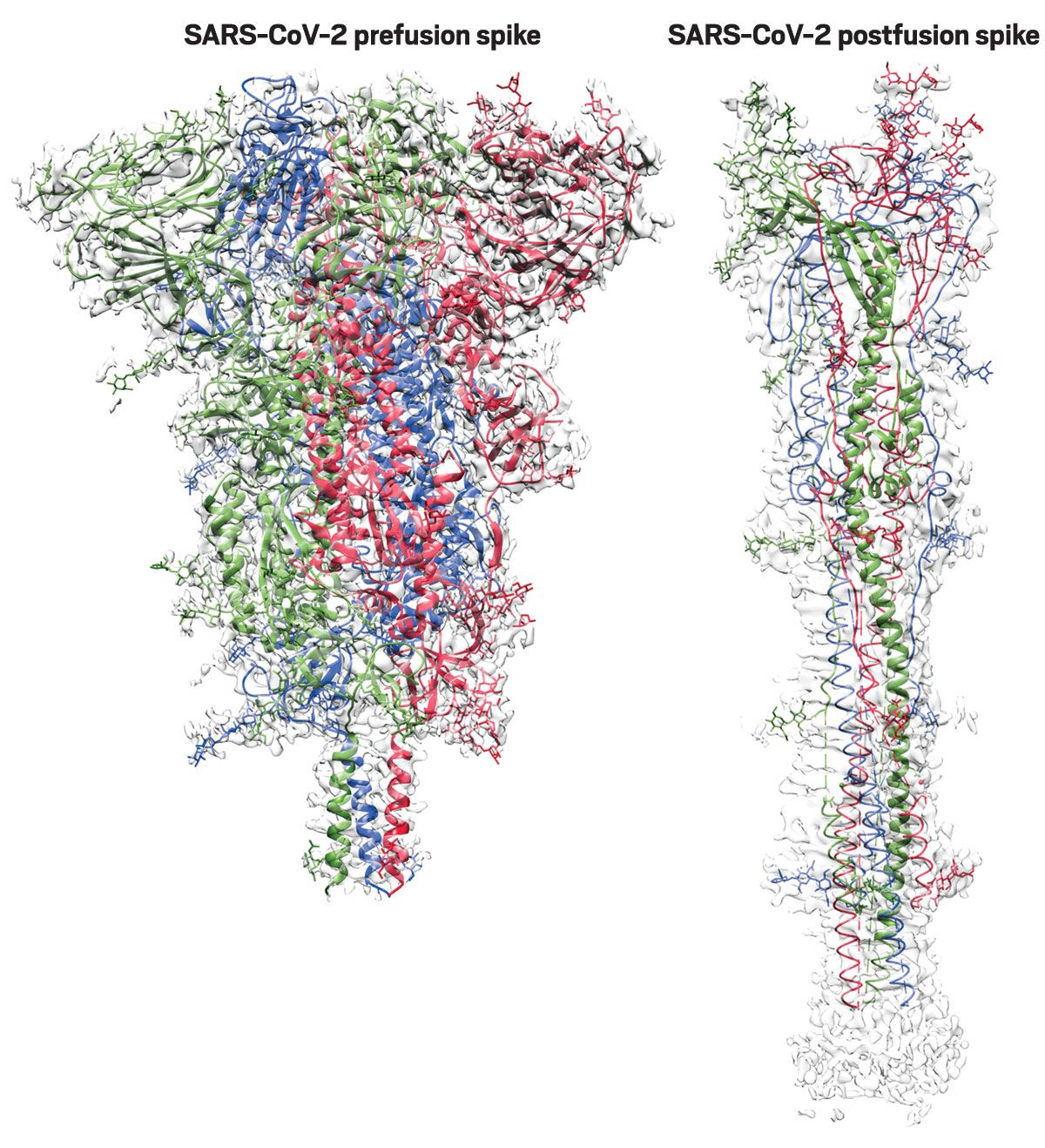
It turns out that Pfizer, Moderna and J+J are ALL using the “2P mutation” of the spike protein, but AstraZeneca is not. This mutation significantly CHANGES the spike protein, preventing it from leaving the “pre-attack” molecular shape.
Is THAT the difference? Does the 2P mutation prevent the spike protein from causing problems? Stay tuned! The J+J vaccine will get intense scrutiny going forward.
Now – J+J has had a problem of being WEAK from the very beginning, but STATISTICALLY it has still shifted people AWAY from being hospitalized or dying. People may have still caught the disease after vaccination, but they were never going to the hospital or dying – a LOT like hydroxychloroquine administered early, or better still, the Zelenko protocol.
A short while back, one gal in New York got COVID about a month after getting J&J.
She was not hospitalized. This was a living example of the admitted weakness of the J+J vaccine. NOW, however, somebody who got J+J DID get COVID and DID go to the hospital, so the “promise” you will not go to the hospital with the J+J vaccine just got a bit weaker.
Is Persistent Reverse Transcription a Hidden Virus/Vaccine Objective?
Gloating Pre-Preface
There are few feelings of satisfaction like opening up the NEWS and knowing one’s theories and understandings are WORKING even better than one thought.
Let’s see if they use this one for damage control, and get the “new science” out before the STORY OF THE SCAM gets ahead of them. CDC is lying to us so badly. SO badly.
It’s all good, people. I’m on these bastards like BLACK on TAR.
Notice that the governor’s WIFE also tested positive later. But most importantly, notice how the news never asks the RIGHT QUESTIONS connecting the vaccine to the positive test. Instead, we get LIES.
The FAKE NEWS is going along with this crap. They are so deep in this.
Yes, we are now in peak MITHRIDATISM that they wanted to turn into the MIDAS TOUCH of SPIKE PROTEIN.
Such a SCAM.
In my opinion, the CDC should be CLOSED as a CRIME SCENE.
Thank you, Greg. You are a SCIENTIST, and when you felt SYMPTOMS you forced them into coughing up the DATA that reveals how badly they SCAMMED us, and how badly they continue to scam us.
I think Fauci knows exactly what I know. He could tell you EXACTLY why this happened. And once Rand Paul reads this, he’ll know, too. Somebody needs to start cornering Fauci on all this crap.
It ALL goes somewhere.
LOOSE SCIENCE that you know and everybody else doesn’t is a MAGIC ACT. BAD FAUCI!
I’m seeing into the psy-op, people. I’m seeing so deeply.
THE SPIKE MUST FLOW. AND FLOW AND FLOW AND FLOW. It’s the KEY to the SCAM.
Once you see the spike protein CORRECTLY, you see why they do everything they do.
How much you want to bet Bill Gates is wise to this stuff?
Real Preface
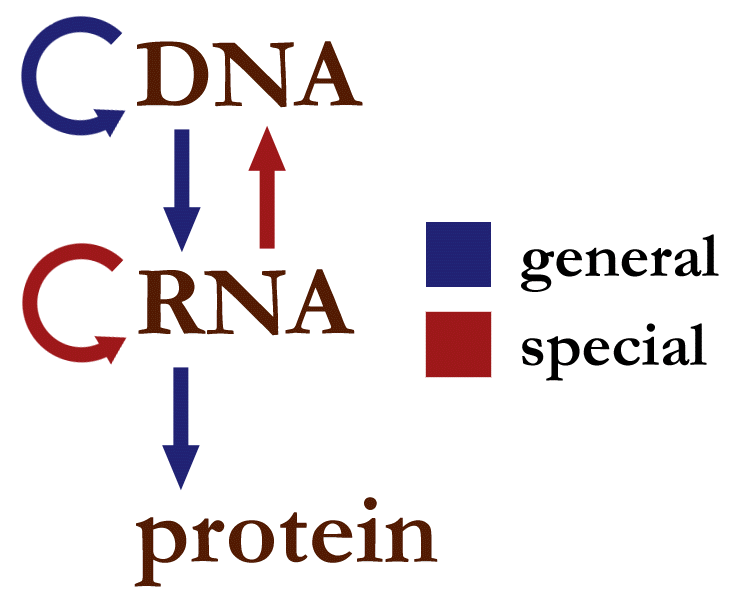
I have come to the conclusion that something is very wrong with COVID-19 and the vaccines thereof, and I think I’ve finally put my finger on the scientific macguffin that ties all the skeevy, sketchy stuff together – reverse transcription.
That would be that little red arrow back to DNA from RNA.
It turns out that reverse transcription, and vaccines for diseases that might code for it, are very “Fauci”.
Learn to code. It’s KEY.
Too many things “political, organizational, governmental, and media” have not added up about the phony “plague”. Going beyond that, too much SCIENCE about the “novel coronavirus” and vaccines being offered for them, simply did not add up.
At least, not until now.
It’s not my inner conspiracy theorist which is finding a problem here – it’s my inner scientist. I am having great difficulties rationalizing certain seemingly careless choices which have resulted in some of the most problematic and badly framed medical offerings since “eye of newt” and “really large leeches for anemia“.
I am having a scientific problem with TESTING that is so bad – so intentionally bad – that it borders on the freaking Ouija Board.
And FAUCI KNEW.
It’s all the result of DISHONEST SCIENCE.
Background: “Science Is Real”
I’m not exactly anti-science, having worked in science all my life. I’m not even opposed to “transhumanism”, which I don’t think is inherently and necessarily BAD. The idea of expanding my memory without putting Google or Facebook or anybody else in charge of it? Talk to me. I’m listening.
I’ve ALWAYS gotten the flu vaccine – ALWAYS. I NEVER miss it. That’s not exactly transhumanism, but it shows that, for most of my life, I had great TRUST in medical science. In fact, I would even say I still do. Generally speaking.
I’ve had vaccines for everything I could get – even the RABIES vaccine, when I was bitten by a bat. The rabies vaccine is, in fact, one of the STRONGEST defenses of vaccination in medical history. No vaccine opponent WILL or SHOULD turn down the rabies vaccine – it is a HUGE success story in medicine. If you get bitten by a rabid animal, the rabies vaccine promptly administered against that SLOW virus will SAVE YOUR LIFE. Some vaccines are of arguable worth, but the rabies vaccine is not one of them.
Indeed, I consider myself to be something of a gourmet, or at the very least a connoisseur of vaccines. Previous “reviews” of vaccines on this site have featured my lovely assistant, Miss Direction, néeRetroculture, who helps me convince people that vaccines weren’t always questionable, and might even be good for people.
Hey, it’s not every day that I get to post something that’s not only about the unspeakable issue of vaccines, but is both PRO-VAX and ANTI-VAX at the same time. I mean, what’s the use of FREE SPEECH if we can’t use it to troll EVERYBODY – including PENCILNECK? Whoops – WRONG PENCILNECK. Let’s try …
Perhaps you recall my PREVIOUS correspondence and “review” of the new, two-shot shingles vaccine, Shingrix – or more specifically, my review of the FIRST SHOT. Wolf’s Hot Date With Retrosynthetic Dinopox Hey, it’s not every day that I get to post something that’s not only about the unspeakable issue of vaccines, but is both PRO-VAX and …
I was anticipating getting one of the new coronavirus vaccines – and was holding out for the first one PROVEN to be safe for recoverees from COVID-19, one of whom I happen to be.
My lungs aren’t that good anymore – not after COVID-19 seared them like some kind of biological chlorine gassing on the front lines in France. I have to be very careful. Another case of COVID, or pulmonary / vascular coronavirus vaccine side effects of comparable severity, might actually “finish me off”.
So – I’m SHOPPING. And I mean SMART SHOPPING. I’ve been paying a LOT of attention to the new vaccines, and trying to understand their technologies, their benefits, their risks, and the science behind them. I simply can’t afford to make a mistake on side effects. Not if I want to enjoy the retirement for which I worked LONG and HARD.
I already knew quite a bit of the science behind COVID and the new vaccines – enough that it has been easy for me to follow the scientific news about these things. I’m not a virologist, an epidemiologist, a vaccine expert, or a molecular biologist, but I’ve worked with such people for much of my life. I picked up a few key ideas in the process. I’ve also come up with a few scientific ideas and principles of my own, but that is largely because I’m a devotee of the history of science, which gives perspective on science.
If you don’t think science can be WRONG, and that large numbers – HERDS – of scientists therein, can go OVER A CLIFF, just take a look at Planet Vulcan, Lysenkoism, The Great Leap Forward, and science in the Third Reich – a seminar on the latter having been quite instructive in my youth. It was not simple how the scientific masses in Germany were led astray, once socialist politics DRAGGED, PUSHED, and SCARED them away from “Jewish Science”. The top echelons of German science, filled with Jews and their friends and spouses, were forced into horrible choices, as some of the best science and scientists were politically rejected over a real social stupidity which fractured and destroyed what was arguably the leading scientific nation on the planet.
None of that had to happen – but it did.
Don’t think we’re immune from scientific debacle. We’re not. Socialism is the greatest “hold my beer” knucklehead that science ever green-lighted into a dysfunctional relationship. He’s always coming back on Saturday night with roses and cherry vodka, after the “last” last time he wrecked Science’s cute little sports car.
Science normally checks itself for errors – and it is my contention that the checking needs to be extensive – all the way out to society as a whole – including stakeholder scientists, non-stakeholder scientists, and even the non-scientific public at large. Sure, you can skip the non-stakeholders and the public, but is it wise? Hardly, in my opinion. The smaller the group needing to be fooled, the easier it is to accomplish things which society simply does not want, or which have vast intended or unintended consequences.
Yuri Geller proved that scientists are easy to fool. James Randi made that point even more strongly. And I have my own take on it, which adds pushy and manipulative politics of any kind as a RISK to science. The same “sale by urgency” which works for salesmen at the appliance store, works in science. Many of us – particularly those of us with historical perspective – saw this problem in climate science. Now, we see it in COVID and vaccines. We are being rushed into something, for some reason. The questions are WHAT and WHY.
I’m going to assume that most people reading this, have started to grasp enough of the basics of viruses and vaccines, and particularly the new mRNA and DNA vaccines, that they don’t need “the way things are supposed to work” explained to them. Indeed, if you go out, and absorb all the “mainstream” journalism on COVID – science sites – mainstream media – cable networks – your favorite non-conspiratorial “science guys” – fact checkers – explaining the way things are SUPPOSED TO WORK, you will be thoroughly and smartly educated by excellent science.
If you want, try this great link courtesy of Ethical Skeptic, one of my favorite “dissident scientists” out there, pulling us back from the current “woke Lysenkoism” we seem to be in.
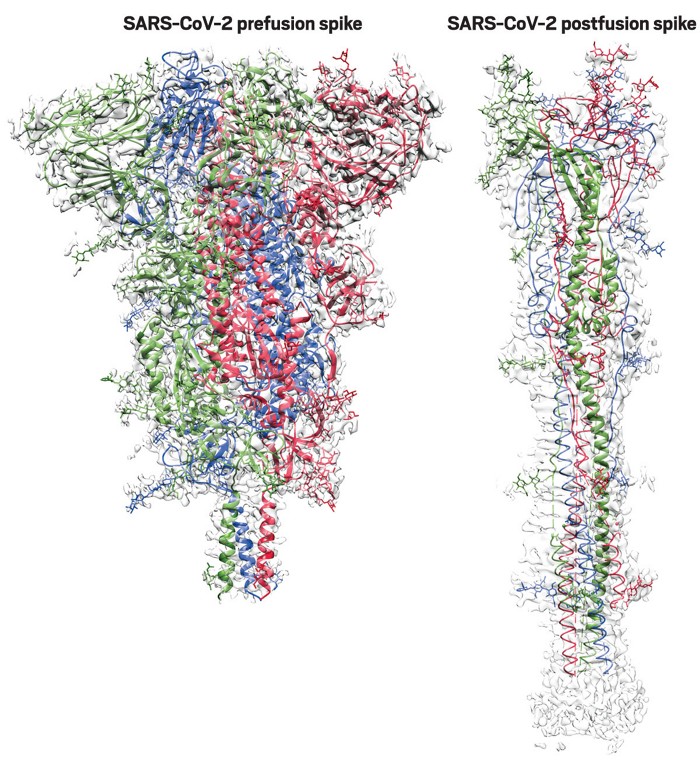
Good summary of the unique structure of the Spike Protein mRNA vaccine and how it differs from the Coronavirus' Spike Protein RNA in pseudouridylyl Ψ and synonymous codon stealth.
See? Yeah, I’m a grade-A conspiracy theorist, because I told you to look at Snopes, and not some clickbait site saying these vaccines are injecting nanobots into you to turn you into something non-human.
The PROBLEM with the conspiracy theories on vaccination isn’t so much DIRECTION as it is MAGNITUDE. It’s all over-reach. Silly, perhaps well-intended, but self-discrediting overreach. Much of it is clickbait or psy-op. A lot of it is actually true – at some small level – often orders of magnitude less dramatic than the headline claims. I can talk to the consumers of such in terms they will understand, and I’m generally talking them DOWN and BACK to what are more scientifically grounded problems with the new vaccines. And there are some. Which is the POINT of this entire piece.
In this essay, I am now talking primarily to what might be called “vaccination normies”, who are – like me – normally rather trusting of vaccines, but perhaps feel like there’s something not quite right about the current situation. These are people who have SOME vaccine hesitancy, but are likewise leery of TRULY baseless skepticism of science.
I’m talking about the people who put “SCIENCE IS REAL” yard signs out in front of their houses. There is a side of me that likes that. However, there is a side of me that wants to put out a sign that drops LOVE IS LOVE (Pedo? No way!) and all the rest, and sticks to what I know about science from the inside:
SCIENCE IS REAL
SCIENTIFIC FRAUD IS REAL
SCIENTIFIC GREED IS REAL
SCIENTIFIC BIAS IS REAL
SCIENTIFIC ERROR IS REAL
SCIENTIFIC DECEPTION IS REAL
SCIENTIFIC SELF-DECEPTION IS REAL
SCIENCE IS REALLY MESSED UP
SCIENCE IS STILL BEAUTIFUL
You see what I’m sayin’? You want SCIENCE, you get the whole, lovely, crazy, smart, dumb, dysfunctional bimbo who thinks she can handle SOCIALISM, and ends up on some frat party lawn in a lab coat and a mini-skirt, throwing her shoes at strangers, demanding somebody take her home, and SHE’S NOT DRUNK.
Yeah. I knew that crazy, wonderful bitch.
Wolf’s Take on Coronavirus Vaccines
You can check out my posting history here to follow the chronology of my thinking on coronavirus vaccines, but I’ll try to recap toward my current thinking, and what seems to be wrong with them. I am going to lead you up to my last post on the vaccines, where I almost saw what I’m seeing now, plus a whole bunch of other stuff.
PREFACE I thought that I might withhold this post on Easter Sunday, and then I changed my mind, thanks to Deplorable Patriot, Trump, Gab and Jesus. If anybody ever FOUGHT on Easter Sunday, it was Christ. It’s time to FOLLOW POINT. The Branch Covidians have taken a toll, but the WAR is turning, and – …
The first news that really grabbed me was about Inovio – a DNA vaccine – a “Bill Gates” vaccine (almost all are, TBH) – and thus one of what I will refer to as genetic vaccines. Such vaccines are not supposed to work by modifying one’s genes or genome, despite the word genetic. They simply exploit cellular biochemical processes CLOSER to the genes, using the known biology of genetic expression. They dump DNA or messenger RNA (or a close facsimile thereof, to be more precise) into existing cellular processes, to “fool” the processes into creating – in the case of the current coronavirus vaccines – a stabilized form of the spike protein of the virus.
At the time, I noticed that these would be THE FIRST genetic vaccines being tested in or deployed successfully in humans. And this is where things get “iffy”. Just a little bit.
The next vaccine to get into the news in a big way was Moderna – an mRNA vaccine, again using a full and slightly stabilized spike protein as the antigen, but created in vivo via the mRNA genetic instructions thereof. While Moderna seemed to be successful in its first clinical trials, the side effects were noteworthy, frequent, and fairly significant – even compared to the notoriously “spicy”, arm-reddening-and-bicep-swelling, shingles vaccine, Shingrix. As one respected “pro-vax” scientist of my old acquaintance put it, they would have to kill him to give him the Moderna vaccine. He was definitely thinking the same thing I was thinking. Rush job, problems, keep looking.
My initial hopes quickly moved toward Novavax. Novavax is NOT an mRNA or DNA vaccine. It uses the same full stabilized spike protein strategy as the others, but it provides the spike protein AS spike protein, using a nifty little nanochemical “pincushion” to hold the spikes in an outwardly facing array, thus to engage receptors properly and at LOW DOSAGE. This is an excellent strategy that AVOIDS the unknowns of mRNA vaccines like Moderna, or DNA vaccines like Inovio or Russia’s Sputnik V.
The most significant risks of spike protein vaccines like Novavax are the risks of the spike protein itself, NOT of abusing the genetic processes to CREATE the spike protein in vivo, like Moderna. Indeed, Moderna scientists admitted in one of their first papers on their vaccine, that there ARE unknown potentials for long-term side effects with mRNA vaccines. Go find the paper – it’s there. They couch the admission in gentle and somewhat obscuring language, but the disclaimer is there. It has to be. They’re being honest.
mRNA vaccines in animals have not been uniformly free of side effects, to put it VERY kindly. We can argue about the severity of those side effects, and whether they extrapolate to humans, but I suppose we will find out now. The risks are there, and they tend to be long-term. So – in full disclosure – there are RISKS to mRNA vaccines. The older you are, the less the long-term risks matter, and conveniently, the higher the risks of COVID-19 itself. That’s a good thing. It means we only have to take the risks with those patients who can most likely afford them.
On the flip side, why the hell we want to take huge, unnecessary risks to vaccinate children is beyond me, but I’ll save those arguments for another essay. Or look at my LAST essay. Those arguments are, in part, subtle “history of vaccination” propositions that would bog us down right now.
In contrast, Novavax doesn’t take those risks. It’s a more conservative vaccine. This is why it jumped to the top of my list. An entire class of risks – the genetic processing ones – were automatically removed. As a “nothing can go wrong or I’m likely DEAD” vaccine recipient, I appreciated my better chances with Novavax.
BUT as a “real” scientist, I am not just swayed by THEORY – I love the results of EXPERIMENT. Thus, when Pfizer’s clinical trial results came out, I was IMPRESSED by the excellent antibody levels and the almost minimal side-effects. Far from being an arm-burner like Moderna, Pfizer was looking to be much milder on short-term side-effects, with stronger adverse effects being downright RARE. The large population of test subjects also implied that a recoveree LIKE ME was likely in the study by accident – and NO deaths or severe reactions occurred – definitely a GOOD SIGN for my case.
This not only bode well for lower likelihood of some kind of lethal short-term reaction due to my recoveree status – the smart scientific position would be that lower short-term risk very likely reflects lower long-term risk – and this supposition is completely absent ANY “knowing” causative reason to connect them.
Thus, Novavax and Pfizer were at the top of my list. Things were looking GOOD to take a vaccine, even if I didn’t get an explicit study on safety in recoverees.
And THEN reality started to hit.
Yes – when millions of doses of a vaccine go out, there are going to be deaths and injuries. We have a system in place – let’s be honest – which tries to HIDE the minority reports on vaccine adverse events, in order to keep buy-in on vaccine compliance. That doesn’t mean people should stop getting vaccines, any more than reports on horrible vehicle accidents OR the “hiding” of such accidents on the back pages of newspapers, mean that we should stop driving.
Nevertheless, my scientific curiosity was piqued. We DO have COVID vaccine problems now, and MORE than seemed to have been revealed by the vaccine trials.
WHY NOT DO SOMETHING ABOUT THEM?
I repeat. Differently. THERE IS NOTHING WRONG WITH BETTER VACCINES.
Taking stock of the many positives and negatives associated with THREE VACCINES which gained the most initial experience – Moderna, Pfizer, and Oxford/AstraZeneca – I noted three things, one from each.
Moderna – side effects sometimes REMARKABLY resembled COVID-19 itself – even up to SEVERITY.
Pfizer – nursing home patients were testing positive AFTER vaccination – some dying of COVID symptoms
AstraZeneca – hematological problems reminded me of another protein hemotoxin – snake venoms
I could go into deep details about these observations, but in TWO of the cases, it was VIDEOS where the “light-bulb” finally went on. So let’s look at some videos.
Moderna: Ben Stein’s vaccination experience
As I was listening to Ben, I was stunned. He was describing COVID-19 – at least from my perspective. This was not coincidence – this was SPIKE PROTEIN.
WHOA, NELLY!!!
Note that Ben is still “pro-vax” here – he’s just CAUTIONING people about REALITY.
Pfizer: Nursing Home CNA describes correlation of vaccination to later positive diagnosis and death
This man, a CNA in a nursing home, reported online what he had observed, amidst great personal anguish about “whistle-blowing”. He observed that he had protected his elderly patients for all of 2020, but when they finally got the Pfizer vaccine, many of them just started “testing positive” and DYING. He was NOT buying the management line that there was a super-spreader – if you listen to him, he’s fully contemptuous of the idea. He was CERTAIN it was the vaccine.
I agreed with this guy – a TRUSTED SCIENTIFIC REPORTER, in my opinion. His GUT was telling him that the chronology was one of correlation. He was very likely seeing in his mind a pattern in a delay over TIME, integrated over cases, that could only be explained by the vaccine itself. He was NOT accepting the management excuse of a “super-spreader” fortuitously infecting the vaccinated, to give that same result. THIS GUY is my kind of scientist. SKEPTICAL of ad hoc, contrived, politically correct explanations that don’t explain all the facts and observations in a clean, natural fashion.
AstraZeneca: Rare but serious clotting reactions are enough to evoke CONCERN from medical professionals
I think THESE DOCTORS in the following video represent my position extremely well – the problems with the AstraZeneca vaccine are RARE, but we KNOW there is a correlation, and it is our DUTY to stop and fix the problems, weighing in particular the relatively lower risks of COVID-19 itself in younger patients, where these events are occurring.
The difference between IGNORING the rare thrombocytopenia incidences and FIGURING THEM OUT is the difference between Stalinism and responsible popular government.
I truly admire these front line doctors for their SCIENTIFIC BALANCE. Frankly, I consider front line doctors to be scientists of the highest order, just like that CNA in the video above. PRACTICE is what matters – not DEGREES.
Now in this latter case, the AstraZeneca vaccine, I dragged in what I consider a very useful analogy to hemotoxic snake venoms, but I didn’t really see WHY this would be happening – until I found something that explains ALL of these problems.
I just didn’t realize I was holding an ACE.
The Macguffin – Reverse Transcription
In March of 2021, I reacquainted myself with a paper that I had noted when it came out, in December of 2020, but had not fully grasped the significance. The authors clearly knew that what they had found was a big deal, and worded the title appropriately, but even then, I don’t think they dared consider the possible deeper significance of their finding.
Nobody can FIRE ME from retirement, so I’m quite willing to say what needs to be said. Could it be wrong? Maybe. But if it’s RIGHT, there are issues that need to be dealt with. So let’s go there.
SARS-CoV-2 RNA reverse-transcribed and integrated into the human genome
Liguo Zhang, Alexsia Richards, Andrew Khalil, Emile Wogram, Haiting Ma, Richard A. Young, Rudolf Jaenisch doi: https://doi.org/10.1101/2020.12.12.422516
I will refer to this paper at “the Jaenisch paper” – after the main author to whom correspondence is written – not because I don’t want to credit the fortunate and likely excellent first co-author Zhang in this instance, but because there is another paper I talk about all the time, dealing with masks, that I call “the Zhang paper“.
THAT one – the mask paper – in an embarrassingly good journal – is a piece of crap – some of the worst “political science” ever – designed to virtue signal to the CCP-DNC narrative of election-fraud-assisting masks, in utter contradiction to the very data presented by the authors.
The Jaenisch paper, in contrast, opens up a barn door that I am sure both industry and “in bed” government wants closed, Closed, CLOSED.
Stated very bluntly, the paper says that the virus behind COVID-19 actually “changes the genome” of victims – similarly to, though not exactly like, HIV.
You know – that OTHER disease for which Fauci was so interested in creating a vaccine.
And not only that – the COVID-19 virus does it enough to throw off those damn PCR tests that Kary Mullis warned us about for the exact same reason. In fact, the solution of that aspect of testing – the way “test-triggering fragments” just hung on and on and on in recoverees – is one of the BEAUTIES of the Jaenisch paper. The conclusions of the paper explain very neatly certain OBSERVATIONS and scientific conundrums that were first found by Korean scientists, who were very very persistent in proving that their COVID patients were NOT getting reinfected, as the fear-mongering American media “wanted”, but were still testing POSITIVE while being NON-INFECTIOUS.
Now we have a wonderful explanation. Excellent scientific work. THIS is why I signed up for science!
The THREE-TRILLION DOLLAR QUESTION that nobody wants to ask, however, is whether the genetic vaccines based on mRNA or DNA of the viral spike protein do the same thing – meaning get incorporated into the genomes of recipients. Well, do they?
Ever? Sometimes? Always? Or even just enough to make a difference?
It’s a great question! That deserves a CLOSE LOOK with MUCH SIDE-EYE.
I will say this. Even if these vaccines only get incorporated sometimes, that would make the “crazy people” yelling “OMG THESE CORONAVIRUS VACCINES ARE GENETIC MODIFICATION!” become suddenly – oddly – scandalously – CORRECT.
I find that incredibly ironic.
BUT WAIT – THERE’S MOAR. And then, there is EVEN MOAR STILL.
The Spike Must Flow
I had set the Jaenish paper aside in my mind in January 2021, as I was busy being pursued by the FBI as an “insurrectionist”, having wanted to see “fellow dissident scientist” Dr. Simone Gold speak at the Capitol Building on January 6, 2021. Rather luckily, I never found her, or realized where she was. Had I found her, I would have likely been arrested and all that nonsense, since she wandered, far too trustingly, into the interior of the Capitol building.
This old wolf, too wary to go into buildings – too old to play tug-of-war games – too injured to stand up to direct pepper spray – settled for singing the Star Spangled Banner at over 100 decibels with tens of thousands of patriots outside – which was an absolutely surreal experience.
But back to the story.
When I began seeing more and more vaccine problems by March of 2021, some of the possible answers seemed to point to the WHOLE SPIKE PROTEIN being the BAD ACTOR. The trouble was, I needed disease-producing levels of it. How might THAT be happening?
Look at Ben Stein. He was injected with only a small amount of COVID spike protein mRNA, but had disease like I did, when, in my case, the virus ran wild making BOTH spike protein AND more virus from it, in my cells.
The vaccine does NOT create any new virus. It does NOT have the full virus instructions. JUST the main one – the spike protein that provides a significant part of the viral shell.
Thus, the vaccine cannot create an EXPONENTIAL GROWTH of the spike protein, which the VIRUS does. The full virus creates more and more virus, meaning more and more spike protein, until something – immune response – shuts it all down.
The vaccine creates a few “fountains” of spike protein – basically “vaccine-infected” cells – but these get shut down as immunity builds. It never really gets out of control. Or at least, not normally.
So, for Ben Stein to have a powerful, disease-like experience, he needs cells that are cranking out far more spike protein than we would normally expect with the vaccine.
Well, if the INSTRUCTIONS for spike protein – in some people – got a bit upstream of just “slipping them into the print shop queue”, to where entire new print queues of spike protein and substantial, chimeric, problematic chunks thereof were being repeatedly ordered from DNA central operations, it would explain a whole lotta spike protein and associated chimeric junk being produced – more than anticipated.
And – I think I would be remiss if I didn’t consider the possibility that some of these bogus DNA instructions might be hard to shut down completely, thus providing an explanation of “long haulers” and “immunocompromised variant generators” beyond their known suffering of what can be rightly regarded as “simply” chronic damage from initial infection.
But let’s move on the to Pfizer nursing home case, and many other reported cases like it.
If we’re getting genetic incorporation of vaccine spike protein instructions at the DNA level by reverse transcription, like the Jaenish paper, perhaps in older individuals who are more susceptible to this problem, then it explains them testing positive later – and in some cases – if they can’t shut it off – DYING LATER.
Now – here is where KINETICS comes in. Kinetics is basically process flow rates. I talked about KINETICS in my LAST RANT on COVID-19, in which I began to put all this stuff together, but didn’t really put forth the totality of things until the comments section at the end of the post. I mentioned in the body of the post that the kinetics of viral interference didn’t seem to explain the nearly complete disappearance of flu while COVID was still significantly above herd immunity levels. It just felt to me that BOTH of these would shut down with greater similarity, if viral interference was the sole explanation. In that case, CDC lying to us about flu vaccine efficacy, understating the success to increase compliance, COMBINED with viral interference, provides a nicer (IMO) explanation of the observed kinetics.
Now, in the case of partial genetic incorporation, the kinetics of interest would be how fast the body shuts down spike protein production by cells without genetic incorporation, versus shutting down cells where there WAS genetic incorporation. If cells with significant production of spike protein due to genetic incorporation were not just sources of more spike protein and more symptoms, but also harder to shut down than “unincorporated” cells, and elderly people were increasingly subject to genetic incorporation with age, we might actually see the AGE-VACCINE DANGER relationship that is being seen in nursing homes, where the most elderly patients are at significantly greater and AGE-INCREASING risk from the mRNA vaccines – something we absolutely don’t want.
Are you starting to see why this explanation works for me?
Genetic incorporation of symptom-producing protein instructions by mRNA vaccines of the FULL SPIKE PROTEIN seems like a REAL WORKHORSE OF AN EXPLANATION.
And, if you’re following my reasoning, you can see that this can also explain the odd cases of thrombocytopenia in some younger patients getting the AstraZeneca vaccine.
In the AstraZeneca case, we would be seeing rare cases where spike protein production after genetic incorporation was just cranking away at levels reminiscent of hemotoxic envenomation by crotalids – or in English, snakebite, which is also (in certain snakes with certain proteins) characterized by thrombocytopenia.
I will tell you right now – there MAY be very similar cases in older patients – maybe not – but I suspect that such cases are less “systemically identifiable” in older patients where thrombosis is more “normal”, and will be more likely attributed to age and NOT the vaccine.
And here is the kicker. In all of these cases, because of the chimeric nature of the fragments noted in the Jaenisch paper, there is a certain RANDOMNESS which could be responsible for the random responses seen in different individuals and different vaccines, which by using significantly different mRNA vectors, may result in significantly different levels and exact circumstances of genetic incorporation in different individuals.
NOW – if it turns out that there IS genetic incorporation of vaccine-origin stabilized spike protein mRNA or DNA as genomic DNA, like the virus itself, then one of the first suspects for reverse transcriptase activity or induction thereof, would be the spike protein itself.
And THAT, my friends, opens up a REAL can of worms.
The Full Spike Protein Monty
Let me ask a really impertinent but really obvious question – something that Tucker Carlson is famous for.
Why are we vaccinating people with the WHOLE spike protein, or more precisely, stabilized analogs thereof?
OK – now I’m being a LAWYER here. I am asking questions to which I ALREADY know the answers, and in particular, the answers that Tony Fauci might give. Here is my argument on behalf of Fauci.
“We don’t really know EXACTLY where on the spike protein, might be the BEST place for antibodies to attack. Also, we don’t really have time to start guessing, when we can just use the whole thing. Most of the labs are modelling the whole molecule, and sharing data. It just makes sense that everybody sticks to the same model, so that any advances that one lab makes, can be quickly adopted by the other labs and researchers. If we begin using fragments of the spike protein, then results are going to be harder to interpret from lab to lab. There will be fragmentation of the science as well, and this will slow our response time tremendously. Comparison of results will be much more difficult. The timeline to a vaccine could be extended by months – even years. Maybe never……..”
See how that works? I would make a fantastic lying science bureaucrat – I know all the tricks already, because I used to negotiate compromises that result in the status quo in fake science in other ways.
Now – HERE is the superior counterargument that will LOSE because Tony Fauci is in control. For this argument, I’m a FRONT-LINE DOCTOR. Maybe I’m even Simone Gold, or one of the various doctors I followed back during the HCQ Wars.
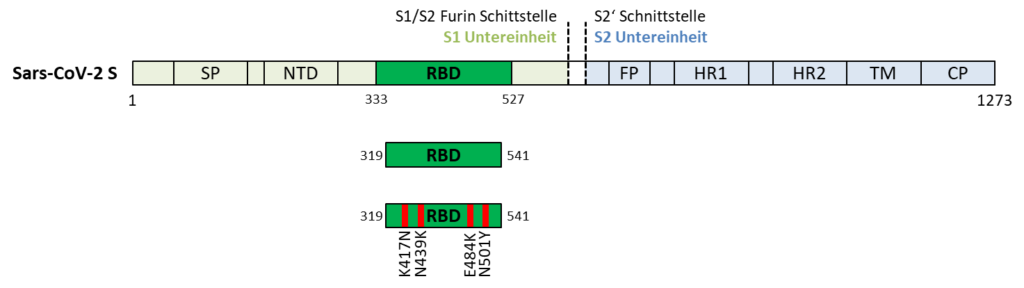
“Yes, that’s all fine and good. But we are doctors, administering a VACCINE to patients. Adverse effects are real, and we want to minimize them. The spike protein is almost certainly the cause of much of the endothelial damage by this virus. Anything we can do to avert that damage is smart, including NOT using the full spike protein or analogs thereof. If we know the primary sites that antibodies need to attack, which we actually do, we can just use shorter peptide sequences or protein fragments constituting those sites. Modeling can make sure these fragments present the same, active, pre-fusion conformation. We can stabilize as needed to prevent immune enhancement, just like in the full spike protein. This shorter peptide approach has been successful in hepatitis vaccines. These peptides can be created quickly and formulated as vaccines in roughly the same time as the full protein. In fact, vaccine expert Winfried Stoecker has already done this, using the receptor binding domain of the spike protein, and creating a short peptide based on it. Since this technology is well-known, we don’t have to take any of the risks of messenger RNA or DNA technology. Nor do we have to use adenoviral vectors or new lipid nanodroplet technologies. Likewise, all of the advances in stabilizing pre-fusion conformation in the full spike protein can be used for the RBD peptide, so the risks of immune enhancement will be just as low. So, unless you can give us a reason to stick with the toxic spike protein, I’d say this is a no brainer.”
At least, that’s the way it looks to me.
Now, here are some interesting facts.
First, EVERYBODY is doing the full spike protein. The ONLY party that made a vaccine using less, was Prof. Stoecker, and he got in trouble for it, with the German government, because he wasn’t properly authorized, even though – well – normally he just does vaccine work and that’s that.
Second, you should note that – IF the spike protein has any reverse transcriptase (RT) activity, that activity would likely have been LOST by switching to a small peptide dropping most of the molecule.
Third, you should note that – by switching to a small peptide, there is no mRNA or DNA corresponding TO that peptide, so there is no chance it will be genetically incorporated.
By now, it is VERY clear to me, that the industry picked the vaccine technologies that it did, precisely because they were modern and untested, and they needed an “emergency” to get these technologies into use, in preparation for their big goal – actual gene therapy. But – AND LOGIC here – that does not preclude there being even MORE motivation here. The more I see this “event”, the more I see everybody getting bought in by SOME new aspect of the scam.
Using a more conservative approach would have been SAFER, but it would not have advanced the technologies that were groomed to be advanced. Even the Novavax protein-based vaccine, fairly conservative, tests the novel use of nanoparticles to assemble the pseudo-spike proteins into cell-infective starburst patterns. It, too, is full spike protein.
But again, THIS. Everybody is ALL about the full spike protein.
Let’s ask WHY.
A Feature – Not a Bug
Now – if the Jaenisch work is good – and I think it is – and if genetic incorporation of vaccine mRNA into genomic DNA also occurs – and I strongly suspect it does – and if the spike protein itself is responsible to at least SOME degree in causing genetic incorporation – which I also think is very likely – then I am of the opinion that Fauci knew exactly what he was doing in pushing mRNA and DNA vaccines that code for the full spike protein, and that he did so as a sneaky way to get a reverse transcription promoter into the human genome.
Why? I don’t really know. Not yet. But this whole thing just seems intentional in its ELEGANCE.
This is easily expressed in logical hacking terms. Fauci uploaded a stealthy FTP uploading tool into humanity’s genetic account. FIRST as a problem, with China’s help. THAN as a solution, with the industry’s help.
The idea of “uploading an uploader surreptitiously” is just elegant. It’s HACKING. Any person who ever had to “learn to code” has to admire it. And it’s doubly elegant by doing it TWICE.
Stated in biological terms:
Create a genetic vaccine for a same-same disease, both containing the genetic sequence of a reverse-transcription promoter, such as a reverse transcriptase, as a way of creating a persistent or at least consistently available presence of a reverse transcription activator in humans.
And the beauty of this scam, is that it’s “WHOOPS” played TWICE. VIRUS, then VACCINE.
Let’s enjoy it! Scenic route…….
FIRST the disease – OH, NO, LOOK WHAT BAT SOUP DID!
The ChiComs are masters of psychology on Americans. First they whip up the cultural WTF.
THEN they whip up the OTHER side of Americans saying “don’t hate on Asian cultural differences!”
THEN they pull the whole offering back, with everybody left high and dry on CCP zoonotic transfer garbage narratives, minus “bat soup”, but including pangolin “look squirrels”, when the REALITY is that humanized animal models are almost all that is actually used for this kind of viral research any more (thanks to Mary Morse for this fantastic point).
Wuhan lab. Put ALL your chips on it.
MASTERFUL MANIPULATION, and many American academic scientists fell for it like soldiers on leave in a brothel district.
THEN the cure – the vaccine – which uses the SAME genetics to get MOAR of the uploader installed in MOAR people.
And if they get caught….”OMG, DID WE DO THAT? WE JUST FOLLOWED THE SCIENCE AND THE DISEASE! FULL SPIKE PROTEIN FOR THE WIN! IT’S *** SCIENCE *** !!!”
Introduction You have GOT to see the video I’m going to show you. It’s not just what they’re talking about. It’s WHERE IT LEADS. Most of the people who watch Rand Paul go after Fauci here, are concentrating on MASKS, because that is the TOP LAYER of the argument. But THAT is the small potatoes. …
Something is going on here, and it seems too purposeful to be mere incompetence.
SO – Does Wolf Take the Faucipox Vaccine?
Now – I’m gonna tell you – CRISPR-Cas9 vaccines are coming, and THOSE are straight-up genetic engineering. Save some ammunition for that fight. But right now, I think it’s worth bringing up some PRETTY TOUGH QUESTIONS about the current vaccines.
Simply stated – aren’t things with reverse transcription activity a RISK, like HIV, and why would we court that risk in a SOLUTION like a vaccine?
And what’s with all the LIES to keep people from noticing that the VACCINE causes positive tests in recipients, “because spike protein, sequences, PCR, and [COUGH] maybe a little incorporation”.
C’mon. This is so obvious now, it’s PAINFUL. CDC is not even looking foolish. They know this stuff isn’t the disease – it’s the vaccines. They’re LYING.
Sheesh. The whole thing is an outrage.
So. Am I going to take one of the current vaccines?
Not if I think there is a reverse transcription activator coded for in the mRNA or DNA, or even if it’s just in there as PROTEIN.
I’m quite good with my natural immunity, which sadly may ALREADY include some uploading of the uploader. I have no idea if I have any genetic incorporation from the virus already, but if I do, I know exactly where any future positive PCR test is coming from.
Anyway, thank you, Kary. You were right all along. They ABUSED your work.