“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
The above free image of heart shapes is courtesy of iStock and Google Images.
Health Friday is a series devoted to information about Big Pharma, vaccines, general health, and associated topics. As today’s post speaks about the disaster of COVID-19 (the COVID-19 virus itself, and the COVID-19 “vaccines”), Yours Truly dedicates it to the memory of all persons, of whatever age or location, who have passed away from the negative effects of these lab-created bioweapons.
There are Important Wolf Moon Notifications; the Rules of our late, good Wheatie; and, certain caveats from Yours Truly, of which readers should be aware. They are linked here. NOTE: Yours Truly has checked today’s offering for any AI-generated content. To the best of my knowledge and belief, there is none. Also: if readers wish to post anything in the discussion thread for today’s offering that is AI-generated, they must cite their source.
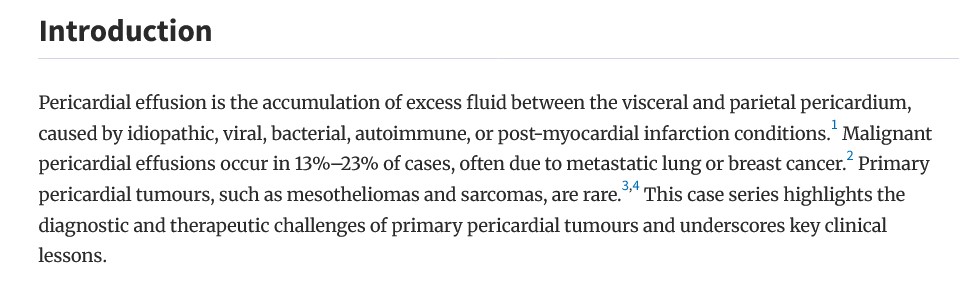
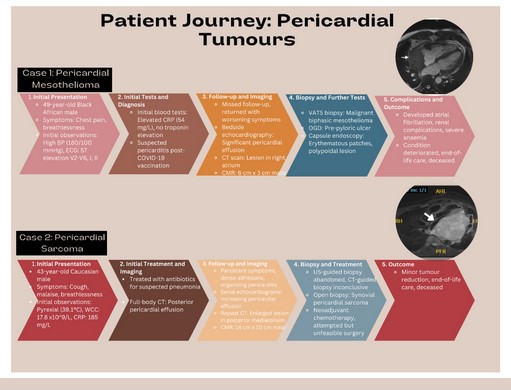
Today’s post may be regarded as a “narrow-focus” offering, one of a “mini-series.” This first “narrow-focus” offering regards the inducement of cardiac issues after COVID-19 “vaccination”; and, the potential for cardiac issues also induced from an infection of the COVID-19 virus itself. Yours Truly begins here: https://www.thefocalpoints.com/p/new-study-fatal-malignant-cardiac, “NEW STUDY — Fatal Malignant Cardiac Tumors Following COVID-19 mRNA Injection”, by Nicolas Hulscher, MPH, 6 March 2025. The paper that is cited in the article is here: https://doi.org/10.1093/ehjcr/ytaf009, “Heart-breaking tumours: a case series of malignant pericardial effusion”, Abdur Rahman Mirza, et al., 18 January 2025. The paper is also found here: https://academic.oup.com/ehjcr/article/9/3/ytaf009/7960074. Below are screenshots of the Introduction of the paper; followed by a screenshot of the graphic of the paper that traces the “journey of pericarditis”:
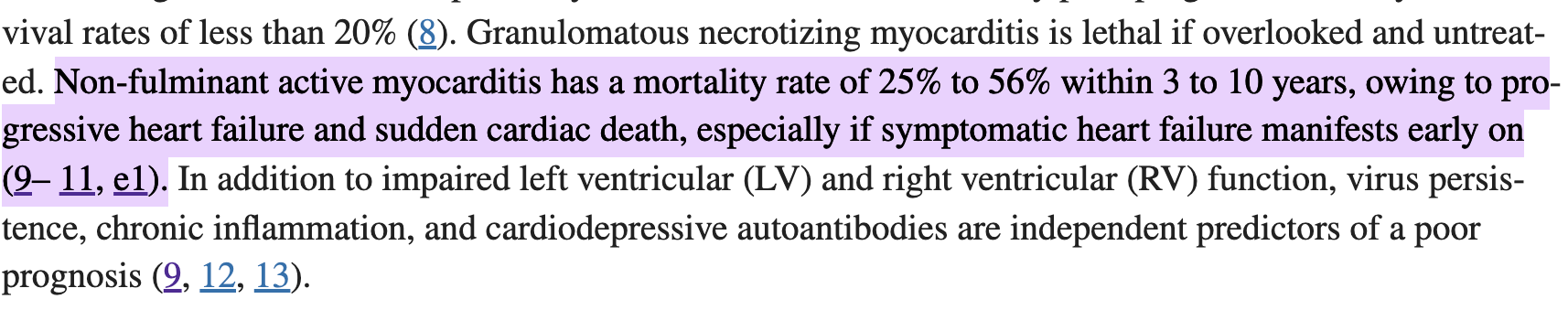
And, the final portion of the Discussion section of the paper:
Note the mention of “diagnostic bias” regarding whether or not a cardiac issue presents after the patient has been COVID-19 “vaccinated.” In Yours Truly’s opinion, the young physician who is the lead author of the cited paper has likely not studied how the COVID-19 “vaccines” affect the heart (for example, this article: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, Michael Palmer, MD, and Sucharit Bhakdi, MD); has likely not read the BNT162b2 5.3.6 Postmarketing Experience report that Pfizer-BioNTech gave to the FDA in April 2021 (https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf); and, has likely not read any of the posts that Dr. Peter A. McCullough, MD, has on his website (https://www.thefocalpoints.com/.) One suspects that many other physicians have not read these items, either.
Turning to the Hulscher article on The Focal Points blog, cited above: It is known that the COVID-19 “vaccines” can, and do, cause pericarditis, a type of inflammation involving the heart (please refer to the BNT162b2 Postmarketing Experience report cited above, page 36 of the report, in the Appendix 1. List of Adverse Events of Special Interest section of said report.) The Cleveland Clinic has an article on pericarditis, found here: https://my.clevelandclinic.org/health/diseases/17353-pericarditis. Below is a screenshot from the Cleveland Clinic article:
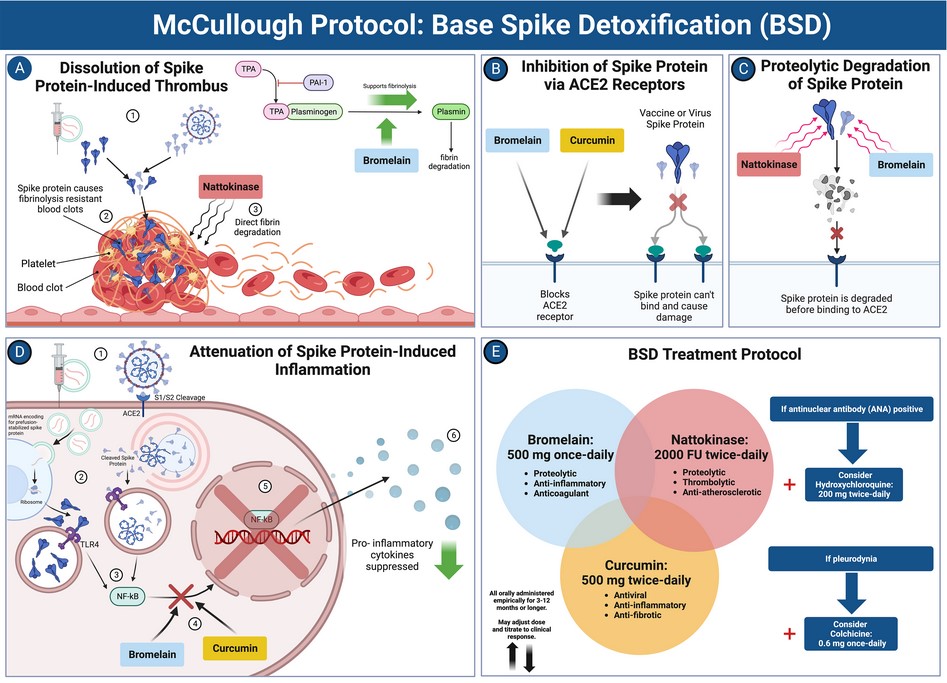
It is also known that the COVID-19 “vaccines” can, and do, cause myocarditis (another type of cardiac inflammation.) Both pericarditis and myocarditis can, and do, cause permanent damage to the heart. Both pericarditis and myocarditis can ultimately result in the death of the patient. However, the COVID-19 “vaccines” contain BOTH the ingredients of the original Wuhan Hu1 virus (SARS-CoV-2 virus, aka COVID-19 virus), AND lab “enhancements” (dangerous lipid nanoparticles; N1-methylpseudouridine; “loose DNA” from the manufacturing process; a piece of the SV40 African Green Monkey cancer promoter gene code) — that make the COVID-19 “vaccines” much more dangerous and/or deadly to the cardiac system of the “vaccinated” person. There is more new information on this situation (thank you to Valerie Curren): https://slaynews.com/news/epidemiologist-new-data-linking-covid-vaccines-global-heart-death-surge/, by Frank Bergman, 1 March 2025. The paper linked in the article is found here: https://doi.org/10.4330/wjc.v17.12.1039909, “Risk stratification for future cardiac arrest after COVID-19 vaccination”, Peter A. McCullough, MD, and Nicolas Hulscher, MPH, 26 February 2025. Below are two screenshots from the paper: the Abstract; and, the McCullough Protocol for spike protein detoxification:
Note the clear statement that cardiac issues can appear years after the person is COVID-19 “vaccinated.”
And, the McCullough Protocol:
Yours Truly finds it ** interesting ** that the above paper was given a “Grade C” for “scientific quality” by the paper’s reviewers, none of whom are identified except by their initials.
Malignant pericardial effusion is the subject of the Mirza, et al., paper cited above in today’s post.
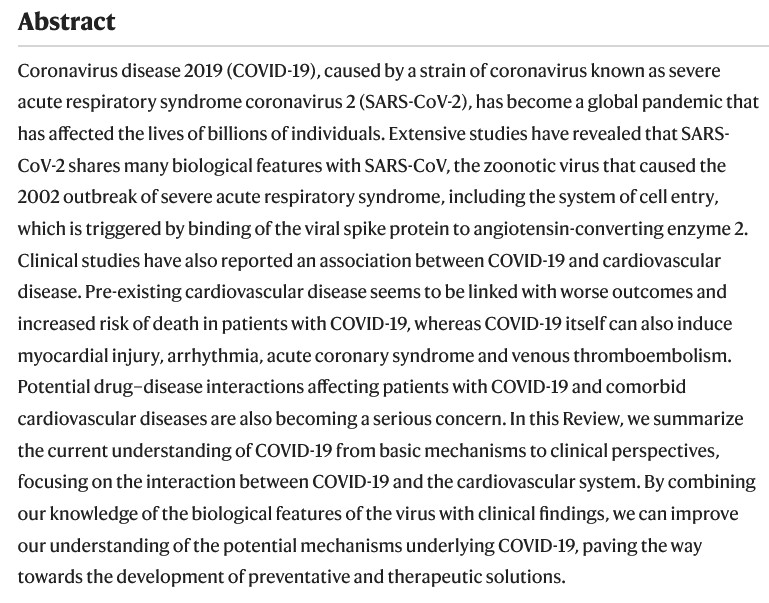
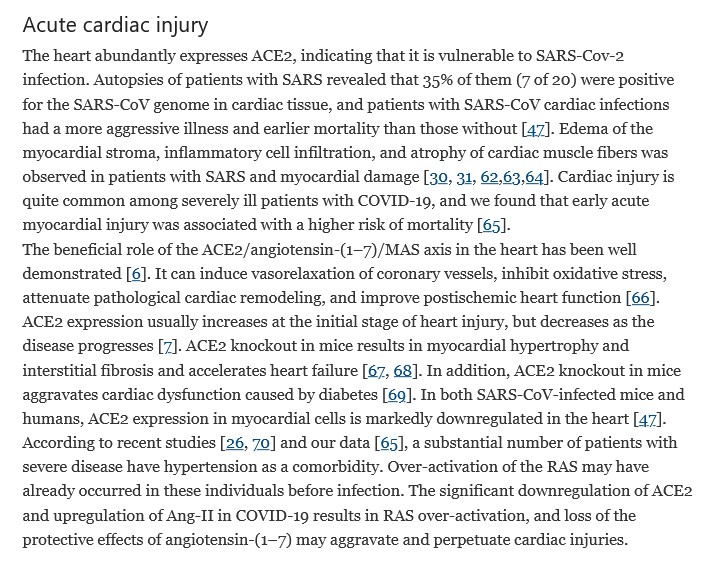
**** On the other hand, the COVID-19 virus itself can cause cardiac issues in persons who contract an infection of said virus. The following paper is from July 2020, well before any COVID-19 “vaccines” was granted an Emergency Use Authorization in any country: https://www.nature.com/articles/s41569-020-0413-9, “COVID-19 and cardiovascular disease: from basic mechanisms to clinical perspectives”, Masataka Nishiga, et al., 20 July 2020. This paper is a good source of information regarding how the COVID-19 virus itself works; and, how this virus can affect the cardiovascular system. A screenshot of the Abstract of the paper is below:
Another paper, also from 2020, well before any COVID-19 “vaccine” was granted an EUA, regards how the COVID-19 virus itself can affect the cardiovascular system: https://pmc.ncbi.nlm.nih.gov/articles/PMC7095524/, “COVID-19 and the cardiovascular system”, Yi-Tong Ma, et al., 5 March 2020. Yours Truly finds it ** interesting ** that the authors of this paper are affiliated with either the Wuhan Institute of Virology, or to medical facilities linked to the People’s Liberation Army (all CCP.) Below is a screenshot from the Background section of the paper:
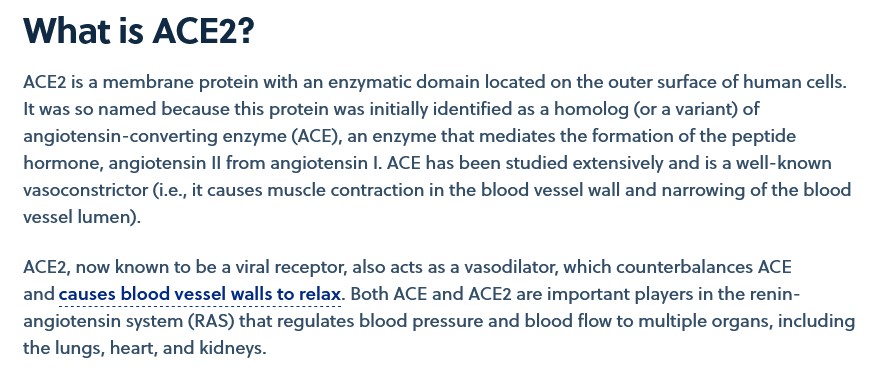
The following article has more information on the ACE2 receptors in the human body: https://www.cas.org/resources/cas-insights/ace2-covid-19-target, “ACE2: Targeting a potentially important receptor in disease pathogensis”, by Angela Zhou, 15 December 2022. Below is a screenshot from this article:
The point here is that BOTH the COVID-19 virus itself (aka SARS-CoV-2), AND the COVID-19 “vaccines” (since these injectables contain SARS-CoV-2), target and attack the ACE2 receptor cells in the human body.
Yours Truly will again emphasize that the COVID-19 virus itself, AND the COVID-19 “vaccines”, were BOTH designed to cause as much damage to the human body as possible. They are BOTH lab-created bioweapons. The COVID-19 virus is not “just another type of virus.” The COVID-19 “vaccines” were designed to be capable of “shedding” elements of these injectables onto other persons (whether those persons are “vaccinated”, or not.) What is of utmost importance is that all people, “vaccinated” or not, must be doing all that is possible to have, and to maintain, the highest degree of personal health. The COVID-19 “vaccines” must be removed from use worldwide — now.
If you are saying BAD THINGS about the wonderful coronavirus vaccines with safe and effective mRNA technology, which have never killed or harmed anybody, then you need a REFRESHER COURSE in the RULES OF JAB CLUB.
#1 – The first rule of Jab Club is, you do not talk about Jab Club.
#2 – The second rule of Jab Club is, you DO NOT talk about Jab Club.
#3 – If someone dies or gets injured, it wasn’t the jab.
#4 – Two jabs to a vaccination.
#5 – One jab to a booster.
#6 – No admission of harm, no metrics except antibodies.
#7 – Jabs will go on as long as they have to.
#8 – If this is your first night in Jab Club, you have to get jabbed.
This kind of mistake is completely unacceptable. Although Mr. Bongino did not violate the first rule of Jab Club, which is to talk about Jab Club, he came very close. It’s clear that people are not following the rules of Jab Club, hence the need for this refresher.
We are providing the following examples for your education and sense of well-being.
#6 – No admission of harm, no metrics except antibodies.
You can’t say things that give people ideas.
The disease can’t hurt rabbits, because the jabs can’t hurt humans. Get it? Understand spike protein political vulnerability! Loose lips cause slips! Corona viruses are potentially bad diseases, that limit human life, but if we talk about any specifics, people will figure out that the jabs do the same thing, only worse, and that we’re making money on THEIR DEATHS.
Why, people might even figure out that we made the damn virus more deadly on purpose, to help depopulate the planet of all these annoying plebes!
Enough already! Wise up!
Example 2
EUROPE — "The country with the lowest vaccination rate has the lowest excess mortality rate and the country with the highest vaccination rate has the highest excess mortality." pic.twitter.com/qslvKukPUq
#3 – If someone dies or gets injured, it wasn’t the jab.
It wasn’t the jabs. EVER.
The FAUCI WALL admits no blame. SUCK IT UP, PEOPLE!
Strike back against this one with “correlation does not prove causation”, said with a tone of certainty and finality. Remember: Follow the science means don’t question the jabs!
This one is a complete travesty, from talking about “sudden death” and individual athletes, to talking about things like overall mortality rates AT ALL. But it gets worse.
“Denial” is actually mentioned!
“DENIAL” is a code word for JAB CLUB!
REMEMBER!
#1 – The first rule of Jab Club is, you do not talk about Jab Club.
#2 – The second rule of Jab Club is, you DO NOT talk about Jab Club.
Check out the video – it’s a superb Jab Club TRAINING VIDEO!
https://youtu.be/61hmUuSewSY
See how that works? Just like back in Germany during the 1940s. People knew everything was OK for the Jews. Hitler was taking care of them, just as he promised. All those stories about maltreatment were misinformation – just like the misinformation we are experiencing now about the vaccines.
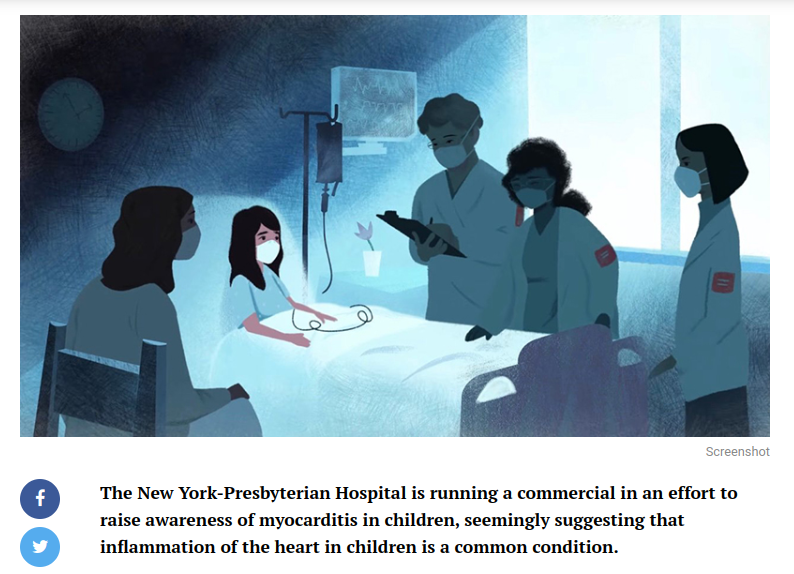
Yes, children are experiencing slightly more myocarditis these days, and government scientists are hard at work, figuring out why this might be. There are many possible candidates, including anxiety about gender, concern about insurrectionists, air pollution, and especially climate change. But children should not worry about disease – myocarditis is easily treated.
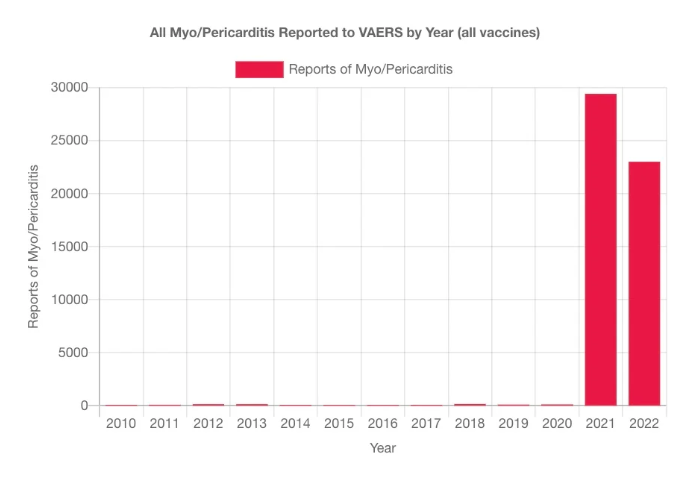
You may see graphs like this one.
If you see something, say something. This graph and others like it are likely to be misinformation, and should be reported to authorities, just like Jewish propaganda was successfully reported to the appropriate authorities around 80 years ago, in a similar fashion.
There are NO WORRIES when you follow the rules of Jab Club!
We hope that you fully understand the rules of our wonderful JAB CLUB that make sure we’re all safe, happy, and in excellent health.
Now – is your FIGHT CARD – whoops – I mean your VACCINE PASSPORT current?
If not, GET A BOOSTER! But just one! Remember Rule #5:
#5 – One jab to a booster.
The reason for Rule #4 (two jabs to a vaccination) is that it takes two shots of the deadlier Wuhan variant spike protein to seriously injure most people, and in particular for the second shot to create a bad reaction to the first shot.
The reason for Rule #5 (one jab to a booster) is to let each booster have enough time to kill people. Most people who are going to die, die about five months after the shots. Start bunching up the boosters, and it’s likely that people will die shortly after a booster, which makes Rules #1 and #2 more difficult to enforce.
And THOSE TWO are the most important rules!
#1 – The first rule of Jab Club is, you do not talk about Jab Club.
#2 – The second rule of Jab Club is, you DO NOT talk about Jab Club.
KNOW THE RULES, PEOPLE!
Science
Dr. Anthony Fauci
W
“What are you doing out of bed? I think you need some more REMDESIVIR.”
PS…..
Hat Tip slowcreekno for coming up with the concept of “Jab Club” while answering my question about breaking through the “we can’t talk about the evil jab” wall of denial.
Looking around the CDC website, I eventually found what I was looking for. It was off the beaten path, but in a place where journalists were apparently used to looking for goodies on a weekly basis.
This is much like an academic paper. Here is the title information:
Let’s put that into text.
Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems — United States, August 2022
Early Release / August 11, 2022 / 71
Greta M. Massetti, PhD1; Brendan R. Jackson, MD1; John T. Brooks, MD1; Cria G. Perrine, PhD1; Erica Reott, MPH1; Aron J. Hall, DVM1; Debra Lubar, PhD1; Ian T. Williams, PhD1; Matthew D. Ritchey, DPT1; Pragna Patel, MD1; Leandris C. Liburd, PhD1; Barbara E. Mahon, MD1 (View author affiliations)View suggested citation
Summary
What is already known about this topic?
High levels of immunity and availability of effective COVID-19 prevention and management tools have reduced the risk for medically significant illness and death.
What is added by this report?
To prevent medically significant COVID-19 illness and death, persons must understand their risk, take steps to protect themselves and others with vaccines, therapeutics, and nonpharmaceutical interventions when needed, receive testing and wear masks when exposed, receive testing if symptomatic, and isolate for ≥5 days if infected.
What are the implications for public health practice?
Medically significant illness, death, and health care system strain can be reduced through vaccination and therapeutics to prevent severe illness, complemented by use of multiple prevention methods to reduce exposure risk and an emphasis on protecting persons at high risk for severe illness.
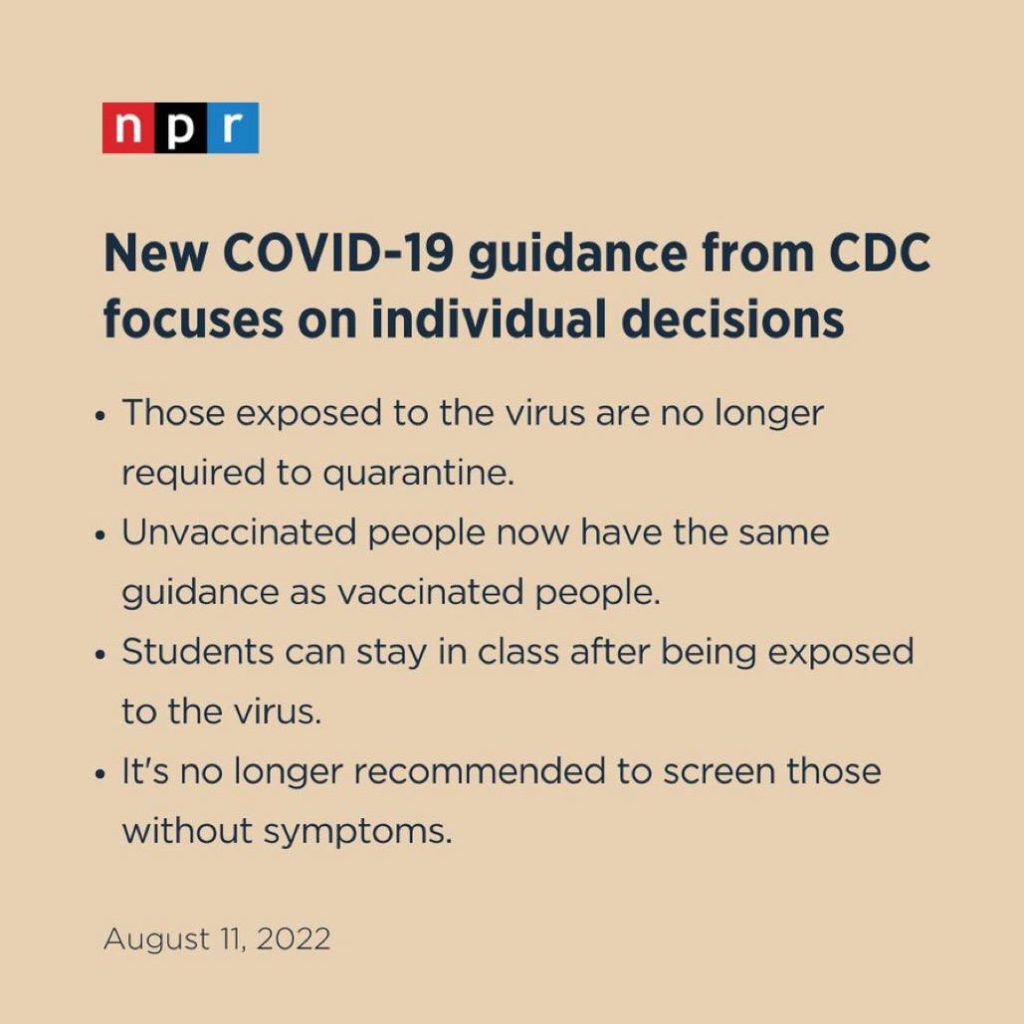
Given that NPR is an official party organ, that’s pretty serious. I repeat:
So assuming you’ve read one of the summaries (Fox or CNET) or at least the NPR checklist, what do more critical voices think?
Many people consider it a REVERSAL OF POLICIES in several important ways. Naomi Wolf, who has championed medical freedom from a classical liberal standpoint, is one of them.
Naomi and Steve Take a Tour of WTF Falls
CDC’s sudden reversal on COVID guidance – from obsessively meddling and frequently “backwards” to “almost sane” – is almost certainly political in many ways, including a reaction of the DNC to their dismal prospects in the upcoming election. And yet the new guidance does do some scientific “hand-waving” to justify itself.
Without making enough of a point about natural immunity to admit its superiority to the immunity offered by the “vaccines”, CDC has admitted the fact that natural immunity, along with clot shot immunity, has effectively ended the crisis of the virus.
The crisis of the vaccinated, however, is just beginning.
people don’t want COVID vaccines – Moderna is throwing out 30 million unwanted doses
people don’t want the vaccines for their kids
vaccines don’t affect transmission, and CDC no longer says so
there’s no reason to have mandates, firings, dismissals
now after all the destruction, not even an apology, just ignore vaccination status
“the edifice is crumbling, because so many people have exposed their lies”
the legacy media is not questioning the reversal – just putting it out there
CDC is making up a fantasy about the science having evolved
no evidence is presented, just as no evidence was presented before
no mention is made of the devastation from the policies that went before
So what does the Wolf think of all this?
Light in August
The novel is an exploration of what we think we know vs what we actually know.
Pamela Jean, Goodreads
To dig out the truth, as scientists instead of artists, we have to “think we know” things, and on average, more often than not, what we think we know has to turn into what we actually know.
In addition to simply denying us “things we think we know” by gaslighting and censorship, one of the ways that criminals get away with things, is by throwing enough phony “think we know” at us, to prevent us from ever getting to the point of actually knowing things.
“Chaff and countermeasures“, as Sundance likes to call them.
To me, the very first CHAFF is right in the “title” of the “new guidance”. The PROPAGANDA is LEADING with the “new goal”.
Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems — United States, August 2022
These creeps didn’t just say something short and open-ended like “Summary of Guidance for Management of COVID-19, August 2022” – they added their alleged goal right there.
“Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems“
WAIT A MINUTE.
SO – suddenly THAT MATTERS?
It didn’t matter EARLIER.
These two things are things we actually know.
That title of the new guidance could have been written by Scott Atlas. You know – the SWORN ENEMY OF SCARF WENCH. And yet – we are now in the BIDEN administration – which pushed the FATAL SHOTS.
It has been my contention that Scott Atlas was ABSOLUTELY NOT on #TeamDepopulation, and that Birx refusal to even go to meetings where he was present, was not only a smart tactic of policy engagement, but a tactic of “big plot defense”.
If there was ever anybody who would have seen through to the “virtuous depopulation plan to save the planet from climate change” in real time, it would have been Scott Atlas. Here is a guy who understood motivation in health care, from the inside – but obviously from the “old days” of FIRST, DO NO HARM. He’s old school – just look at his age – obvious in the picture. If Birx would have slipped up somehow in gunning for more control, less treatment, and ultimate reliance on the statistically fatal shots, it would have been clear as day to Atlas. HIS suspicions could have been raised to the proper levels.
This is something we THINK WE KNOW – not something we ACTUALLY KNOW.
At least, NOT YET.
Ideas that can become things we ACTUALLY KNOW have to become CONCEIVABLE first, and to become conceivable TO THE PUBLIC, they have to become public.
This is why ALL THE CENSORSHIP. The “virtuous depopulation plan” was not allowed to become conceivable in the minds of men and women, by not allowing the smaller components of the idea to take shape – to fit together like a jigsaw puzzle, leading to NEW EVIDENCE.
Sure – they love to let people make the BIG assertions, because who would believe them? It’s the smaller things that add up, that allow us to see that 1+2+3+4=10.
Now – Birx is a tricky one. Not only does she admit to sabotaging Trump in terms of her reporting practices and bureaucratic policy documentation, which can be made to look virtuous to the left – she even tried to feed Trump rope to hang himself, which is at best unseemly, and at worst treasonous.
An example of that level of personal duplicity is how Birx gave Trump a “tour of the incredible” in terms of COVID cures, leading Trump to then give the waiting Fake News media exactly what it wanted – “injection of bleach”, “crazy ultraviolet treatments”, and all that noise.
Let’s be very blunt. Birx SET TRUMP UP. KNOWINGLY.
At the time of “infamous injection of bleach”, I was struck by Trump’s demeanor when stating the things he did. It was clear to me that he KNEW this would feed the media with red meat for controversy, but even more, I detected DISDAIN FOR BIRX, as he mentioned VERY BRIEFLY having gotten the tour, and then proceeded to “step into the trap” by stating some of the things they looked at, stripped of anything he MUST have heard, supporting their scientific credibility.
Typical Trump – allowing the Fake News to backhandedly validate him, while not “appearing weak” by making the arguments himself.
He let Scarf Wench crow for the moment, only to “wear the L” later.
Getting back to the point, there has to be a set of reasons WHY CDC is suddenly “normalizing normal again”.
Democrats are no longer pretending. They’re doing the right thing. WHY?
The election is surely one of them. Democrat voters need to come back for their hug after being bitch-beaten to the graveyard.
But there is MORE. This policy is IN MOTION. It has already been allowed to pass the phalanx of school administrators, who had earlier enjoyed their lockdown and mandate powers well beyond the expiration date.
Holly brought us EVIDENCE in that regard. I invite you to enjoy this conversation as much as we did!
Good sign! Utica University’s fall 2022 covid policy no longer requires the vaxx or exemptions for ANYONE. Private and in New York. This is a big deal.
This is now something we ACTUALLY KNOW. Democrats (teachers unions and university administrators) are doing a 180 in terms of feeding the “protesting parents of Democrat-abused children” with any MEDICAL reasons to protest. Even at the CDC level, they are relenting.
WHY? Just for the election?
Democrats are STILL pushing both TRANS and CRT in schools. Indeed, the early assertion that the notorious Tavistock Institute was being shut down not as victory over TRANS, but as a form of TARGET DENIAL, so that TRANS could be disseminated to hospitals and schools, seems to be borne out, as the center of the fight has indeed shifted to a multitude of “woke” hospitals with insane new TRANS policies.
No. There is more. And I may not ACTUALLY KNOW that the depoppers in American medical bureaucracy are strategically retreating, but I certainly THINK I KNOW THIS.
Fauci’s announced retirement at the end of the Biden administration notwithstanding, I suspect that he will exit SOONER – particularly in the event of Republican control of the House. This will have the effect of thwarting public revelation of facts which would lead irrevocably to the realization of what I am certain actually happened – that a shot which damages the hearts of ALMOST ALL RECIPIENTS AFTER REPEATED INJECTION was advanced KNOWINGLY.
I find it interesting that science is now catching up to the plot, and results which should have been obvious earlier, if things were actually innocent, are NOW becoming obvious to scientists who are innocent enough to publish.
Consider the NUMBERS in this very recent Thai study. My comments on Gab, wrapped around comments by Steve Kirsch, who sees the same evidence, but seems to be keeping any recognition of the plot quiet for now. AND YET HE TAUNTS THEM.
What was that they were saying, that had no effect on Republican scientists, but might actually troll up some Democrat scientists to “action”?
“There’s no time.”
Likewise – at the top – people who are intellectually unable to question science from a standpoint of common sense and moral solidity, can easily get out over their skis, when urged by others who they trust. I think I know that Andrew Cuomo is one of them.
I don’t ACTUALLY know who had prior knowledge of the “left-virtuous plan”, but I am gaining pieces of the puzzle every day. Millions of actions which appear to be mistakes, take shape when we consider that thousands of those actions, committed by a small but core cadre of “knowing” participants, created virtue signals that drove the vast remainder of DUPES to participate in a massive folly.
And what is that folly?
Deploying the MOST ADVERSE VACCINE IN HUMAN HISTORY – while simultaneously REFUSING TO EXAMINE OR ADMIT the evidence of its adversity. The actions of the whole PROTECTED THE ADVERSITY.
And remember – that ratio – scientifically studied by the CIA – makes all sorts of things possible.
Motivations in real conspiracies are always complex, interlocking, apparently contradictory, and tend to “shift and flip” in going down from the most knowing top to the less knowing bottom – yet each layer knows the guilt of their own interests and participation. This form of guilty self-motivation locks people – including mostly innocent people – into defending the whole construct.
I do not actually know who the core cadre is, but I’m working on it.
Your suspicions as to WHO THEY ARE – are welcome.
We are an investigatory collective. We are free to postulate – to hypothesize – to be both scientists and detectives.
I know what I think. I ACTUALLY KNOW what I think I know.
Are you ready for ROUND TWO? Here comes a gaypox (monkeypox) vaccine that causes cardiac damage in 1% of smallpox-unvaccinated normies, and in 2% of oldsters and military who were vaccinated for smallpox.
Moonshine Spots The Scam
We continue our series on The Population Control Shot with a discussion of the next installment in this saga – “monkeypox” vaccines.
As soon as the Biden regime declaredmonkeypox (sorry, that’s rayciss) sodompox to be a national health emergency, I knew that Political Moonshine had been proven correct. As he had predicted, lightintheloaferspox was the next SCAM that the Democrats were going to pull on America and the world.
We await homopox’s unavoidable new christening, just like when Wuhan coronavirus was renamed COVID-19.
Here is a great review of the Political Moonshine catalog of work on poofterpox.
If you have not caught up with Moonshine on either swishpox or the medical enterprise fraud model, then I highly recommend reading the above article.
The bottom line is that the medical system is now a fraud machine – the “scam disease du jour” doesn’t matter – they just buttplug one in and make coin on it.
I completely trust Moonshine on this stuff now. His work on COVID-19 scamming was brilliant. He called bladepox as their next scam, and based on the “declared emergency”, he got it right.
This vaccine is used to help prevent smallpox and monkeypox diseases in adults.
Like any vaccine, the smallpox and monkeypox vaccine may not provide protection from disease in every person.
Yeah, we know that. But it appears to work “most of the time”, and its licensed (fully) and thus “safe”, right?
Well, maybe. The listed side effects that you should have to worry about, so they say, is the usual with any injected drug. It doesn’t sound all that bad; pain where you got the shot, headache, nausea, chills, etc. Ok.
Cardiac AESIs were reported to occur in 1.3% (95/7,093) of Jynneos recipients and 0.2% (3/1,206) of placebo recipients who were smallpox vaccine-naïve. Cardiac AESIs were reported to occur in 2.1% (16/766) of Jynneos recipients who were smallpox vaccine-experienced. The higher proportion of Jynneos recipients who experienced cardiac AESIs was driven by 28 cases of asymptomatic post-vaccination elevation of troponin-I in two studies: Study 5, which enrolled 482 HIV-infected subjects and 97 healthy subjects, and Study 6, which enrolled 350 subjects with atopic dermatitis and 282 healthy subjects.
In other words in apples-to-apples it was six times more likely, for one percent total risk, that you’d have a cardiac reaction. Troponin elevation of more than 2x the upper normal limit indicates heart muscle damage.
There is no such thing as “benign” heart muscle damage. The heart does not regenerate and as such damage to the heart muscle is always considered permanent.
Now how severe the damage is may be another matter, but again — there appears to be a 1% absolute risk with this injection that you will suffer heart damage of some material and OBJECTIVE degree.
One in a hundred people who take this injection, statistically-speaking, will have this happen. That is not a small risk!
In my new world, having not only heard Moonshine and Karl, but having “seen what cannot be unseen” regarding population control scamming, it was impossible for me to not see WHY monkeypox sodompox is “the next thing” that these assholes are going to use.
So I said to myself……
OK, I get it. I’m starting to see how this is working. The “depopulation” stuff is THREE tracks – CARDIOVASCULAR for direct killing, IMMUNODISRUPTIVE for long-term killing by other causes, and ABORTIFACIENT + MENSTRUAL DYSREGULATING for fertility control. Look for these jokers to try to “pile on” to any of those three effects with their various drugs and other “fixes” for COVID. And now including the monkeypox vaccine.
You see – I’m a bit prejudiced here.
Having had “wolficarditis” – most likely due to one of my two cases of COVID – I’m not in the mood for some vaccine to start sending any NEW bad vibes into my cardiac test values, which thank goodness have returned to normal.
So NO WAY.
Well, you say – what about the OTHER smallpox vaccine that they’re talking about using for sodompox.
Remember how the FDA advisory committee did NOT recommend boosters for the COVID shots, but was OVERRIDDEN by that minion of Fauci, the lovely Rochelle Walensky Alinsky?
There was another, later vaccine push where Walensky didn’t even convene the advisory group, to make sure the vaccines would slide by.
Well, guess what. This tactic of ignoring advisory committees for “politicized medicine” works perfectly well for sodompox, too!
It comes after officials in New York, Illinois, California, some cities, and the World Health Organization declared respective emergencies for monkeypox.The head of WHO, Tedros Adhanom Ghebreyesus, reportedly overruled an expert advisory committee to make the declaration on July 24, while the U.N. agency confirmed the virus is in about 70 countries outside of Africa.
Yeah, that China-boy Tedros is good for whatever keep Democrats in power.
It’s worth reading that link – you will see that Ron DeSantis refused to make a similar declaration.
But Florida Gov. Ron DeSantis said he will resist declaring an emergency for monkeypox, asserting that such policies—like the mandates and lockdowns around COVID-19—are designed to create a climate of fear. It’s not clear if any other Republican governors will follow his lead.
“I’m so sick of politicians—and we saw this with COVID—trying to sow fear into the population,” DeSantis said during a news conference Wednesday. “We are not doing fear,” he added.
“You see some of these states declaring states of emergency, they’re gonna abuse those powers to restrict your freedom,” DeSantis said about new rules around monkeypox. “I guarantee to you that’s what will happen.”
The Bottom Line
I’m sorry – I refuse to show some gay butt for my joke, so you have to see some chick ass with a fake syringe (it’s OK, Coothie – no real butts were pierced in the making of this silly photo!)
Sodompox is gonna be the big deal – or maybe it’s the fake big deal until some kind of BIG LIE gets layered on top of it.
But no matter what – think LONG AND HARD about taking any new vaccines. Including any possible new Moderna mRNA vaccine (hat tip RDS), since that company is considering the possibility of making one. If anybody can improve on 1-2% cardiac damage, it’s those folks!
I urge you to click that link (ABC News Go), because it will give you a brief exposure to the MSM, which is CLEARLY trying to gin up EXCITEMENT about the monkeypox vaccine, of which there is “not enough to meet demand!!!”, etc., etc., etc.
Yeah.
We are here and it is now. Further than that, all American science is now moonshine out of Washington.
W
“OK, explain once more how a disease which almost exclusively affects buffarino-lovin’ gay boys, who already have AIDS, has become a national emergency. I mean, is Fauci simply turning an AIDS treatment crisis into an ‘opportunity’ to inject everybody again?”
In the wake of Wheatie Warrior’s passing, we renew the site mission by directly addressing “things unspoken” – now brought into the light.
In the immediate aftermath of the passing of our dear Wheatie, announced last Monday, I chose to deal with only the most substantive technicalities, in large part so that we could properly grieve, and not get caught up in mundane and mortal technicalities. Thus, many important questions for discussion were set aside.
I will deal with those items, and much more, in this post.
(More mood music from Wheatie can be found at the end.)
Wheatie Warrior
Unlike the expected passings of some of our other comrades, Wheatie was, for lack of a better term, “missing in action”. There are reasons for this, and they bear explanation.
In giving you some explanations, I will be limiting what I tell you for TWO reasons.
ONE is out of respect for Wheatie’s desire for privacy. All authors and posters here can expect the same respect. If you want to consciously, knowingly, and with extreme intention, tell the world who you are, that is fine with me. Otherwise, I will assume you want some privacy, and by default will protect that privacy – even upon your illness, death, or simply leaving of this site – no matter under what circumstances. Maintaining your privacy does not include legitimate concerns of law enforcement, blah-blah-blah. Note, however, that I said “legitimate”.
TWO is in order to maintain site security. Keeping the enemy guessing is useful.
SO – why was Wheatie “missing in action”?
In contrast to most of the authors and commenters here, Wheatie was extremely careful to shield her identity. She did not wander far from this site. She didn’t post on “big tech” social media, other than Gab, and that was only after its security was proven, and after Gab was chosen as a secure posting back-up for this site.
Wheatie’s computer security was “minimally divulged” and “not negotiable”. Very often, with authors, I have to deal with security (or lack thereof) and/or permissions needed to work on posts or to upload information, the requirements of which are more rigorous than for merely commenting. Thus, I often learn a lot about an author’s practices of and attitudes toward computer security. They range, and that’s OK.
I will not get into Wheatie’s exact security measures, but they were substantial. Wheatie NEVER allowed convenience to trump security. She would NEVER lower security in order to comment on a site, create an account, watch a video, etc. Wheatie was a ROCK on the items needed to keep this site safe, and her identity private.
Indeed, the only people who appear to have ever gotten past her security, of which I am aware, was the Q team.
That is, in fact, why Wheatie was trusted by me, as she was trusted “in real life”. She NEVER let emotions get in the way of logical thinking, when it came to security. She was cool as a cucumber in tricky situations.
SO – without giving you the details, which would help our enemies, I can tell you that Wheatie’s own security measures likely prevented her from contacting us when she became ill, and until her death.
I want to repeat that. Wheatie was so mission-focused that she did not break her own security policy, or allow somebody else to break it, to let us know that she was in trouble.
Indeed, Wheatie tended to keep mum about most of her medical dealings, other than minor details about symptoms she was experiencing.
All of this combined to make it very difficult to find out what happened to Wheatie, when she went missing. We were very lucky, in fact, that she had divulged a few small things to me, ironically in the interest of assisting with site security. That was enough to help make a “positive ID”. Without that information, we might have never known for sure what happened to her.
Now – this would have all been a “bonk on my head” to start opening up a bit more with you – not just about my own situation, but about YOUR need to “make arrangements”, so that you, too, are not “missing in action” someday.
But there was another death that hit me particularly hard, which gave me a “double-bonk”.
My Friend, The Spy Popular Guy
There is nothing that will wake one up to one’s own mortality faster than a younger friend or relative dying. And that is exactly what happened to me.
At some point during the first half of this year – basically while Wheatie was MIA – I had another friend – a close friend – who “died suddenly and unexpectedly”. And “suspiciously”, I might add, in the words of the police.
Yeah, you are immediately thinking EXACTLY what I’m thinking.
IT WAS PROBABLY THE FUCKING JABS.
I do know that my friend HAD to have been jabbed, because it was a condition to go back to on-site work, after roughly two years of work-at-home. Indeed, he had JUST started going back to on-site work at that employer – which I can tell you for a FACT is “deep state” as all get-out.
That employer has a rather sneaky total vaccination requirement. Everybody has to go back to partial on-site work, and everybody who works on-site has to be jabbed. That kind of “two-step from hell” logic is par for the course with this DS outfit.
“Oh, no – we don’t require our employees to be vaccinated. Only if they are on site.”
“But you’re requiring everybody to work on site.”
“People who are required to work on-site are only required to work on site part of the time.”
“But on the days they are required to work on site, they’re required to be vaccinated – no?”
“You’ll have to talk to our Washington office about the exact specifics of the policy.”
OMG – the double-talk.
Now – as far as I know – the circumstances of death point to stroke or heart attack. The trouble is that, when I go into “I’m not a medical examiner, but I slept at a Holiday Inn Express” mode, I realize without too much deep thought, that it could also have been a “George Floyd” type of death – e.g., a fentanyl-induced heart stoppage, or something similar. AND – sadly – because this person had been a known toker and party guy in his youth, any murder with drugs will likely stick as a drug death, despite the fact that this guy NEVER did hard drugs or popped pills, to my knowledge. He had not even toked in decades, to my knowledge. But unfortunately for the truth, a past like his can be used quite easily as cover. Families and survivors will ASSIST in the cover-up of a drug death.
You may be asking “why would Wolf worry that his friend might have been murdered?” Hang in there – I’ll get to it.
My friend was in excellent health – mild high blood pressure being treated – but otherwise robust. Running, cycling, tennis, ping-pong, backpacking – you name it, he did it. Good weight, good habits, good lifestyle.
It was definitely NOT suicide. No note, no obvious means, and the most happy-go-lucky guy on Earth, with everything going right and looking forward to an excellent retirement.
He could have retired at any time, and THAT is where I’m guilty of not saving him from the jab.
You see, this guy – I am certain – was connected to some agency or entity – I just don’t know who. White hat – black hat – gray hat – sun visor – whatever – he was either working for somebody, informing for somebody, or (and this is quite certain) had friends who were “somebody”. It could have even been that he was “nobody” – but EVERYBODY was watching him because of his connections.
And it gets MORE complicated. My friend was everybody’s friend. “Everybody” included absolutely anybody and everybody who you might think was a foreign or domestic spy, a player, an asset, an informant, a defector, or even just a potential mass shooter. He just “accidentally” made it a point to know all the “interesting” people. It was uncanny.
I never knew where my friend took information, but it was clear he was scooping up knowledge for somebody – and also carrying out some kind of “orders of influence” – but it was impossible to separate the real person from his apparent “mission”. And on top of that, his life was full of contradictory cover. He could have been a very good spy – or just a nobody.
Trust me – he was not a nobody.
This guy was an exceptional person – as in an exceptionally good person. He wasn’t a church-goer – far from it – but he had been raised in a godly family, by a deeply religious mother, and it showed. Despite hanging out with some of the most anti-Christian people you can imagine, he showed all of the Christian virtues in spades, to an almost Biblical degree. There were times that I wondered if he wasn’t some kind of “undercover angel”, if you know what I’m saying.
And all of that ended – mysteriously – some time after he took the jab.
But here’s the thing.
One of the biggest reasons he took the jab is because I stopped giving him information.
I stopped giving him information because of January Sixth.
I stopped giving him information because I knew that my conversations with him were always recorded by somebody – probably FIB – and that whoever was behind him would pressure him into asking about January Sixth.
And it’s not just because I expected ANYTHING I said about January Sixth to be abused by the disgraceful DODGE and FIB.
You see, there are things about January Sixth – things I saw that day – that I have not told anybody. Things that I have not told you all. Things that have implications I don’t understand.
Things that are – as I like to call them – potential “nukes”.
For my own selfish battle reasons, I didn’t tell him the information that could have saved him, about the jabs.
What could I have done differently?
Were I a better and more courageous person, I would have taken his calls. I would have warned him about the jab. I would have – ultimately – talked him out of it. I would have told him everything I knew – all my scientific thinking about it. I would have let him follow along on my journey from “hopeful believer” in the jabs, to “red-pilled realist” warning people against them. I would have said “RETIRE NOW! Take your money and GTFO while you can. Don’t let that place kill you!”
And yet, all of that is still “love of this world”. What if HE did the right thing by just letting the jabs kill him, innocently? What if – weirdly – the disease and the jabs are God’s way of evacuating the righteous from this sinful world?
I will always be second-guessing what I did and didn’t do – just like the guy who I let the ChiComs destroy and drive nuts at “shallow state”, so that I wouldn’t spill my secret knowledge that his boss had been identified to me as a ChiCom asset.
THIS MORTAL WORLD IS ROUGH. Our actions suck. Our inactions suck. Our justifications stink in the nostrils of The Lord. Or reasoning is foul and filled with error.
So – where does that leave me? Other than two steps from hell?
Wolficarditis
I have generally been vague about my health issues or lack thereof, to create as much uncertainty as possible. The “event people” are constantly looking for plausible excuses for their little arranged deaths, so it’s generally advisable to keep as much medical privacy as possible.
The problem is, both openness and secrecy can be used by the other side. Sometimes, oddly, openness is more of a friend than secrecy. After Wheatie’s passing, and that of my friend, I’ve begun to see more virtue in a bit more openness.
So you’re going to get some.
I’m actually in pretty good health for my age, but after my initial bout of Wuhan-vintage COVID, in January 2020, my level of health became erratic.
What I did NOT tell people here, when I talked about “taking care of health matters”, is that I was in the hospital a few times.
Generally speaking, I don’t like to let people know that I’m in the hospital, if I can possibly avoid it. Worse still, I also found it easier to just keep the secret after getting out of the hospital. I don’t know if that was such a good idea now.
I definitely had a cardiac inflammation which I’m going to call “wolficarditis”, to retain just a wee bit of ambiguity on the diagnosis. We will never be exactly sure what caused it, but I can tell you that it was not the jabs, because I never took one.
There is some possibility that my wolficarditis was “smoldering” since either Wuhan (Jan 2020) or Delta (Nov 2021). Or, alternatively, it could have been caused by a later brief, mild, illness which was probably either omicron or flu (but which tested negative for COVID on the initial and only test).
The first time in the hospital, between Wuhan and Delta, was mysterious. It involved odd and extremely unusual high blood pressure, weak pulse, altered vision, and distorted time perception. Looking at it now, it may very well have been what our member Happy go luckydescribed to us recently – a lacunar stroke – or perhaps a similar type of intermittent blockage.
Anyway, ironically, I’m now doing exactly what I need to do for BOTH wolficarditis and wolfmoonar stroke. I feel great, and will continue to do so, until I don’t.
And when I don’t, I will make sure that there is a PLAN in place, to deal with the issue, and any potential aftermath.
So let’s start talking about plans.
Your Personal Plan
If you are happy with being able to come and go from this site unnoticed, to depart with quiet mystery from this site forevermore, when you depart this world, then we’re done here. You can move on to the next section of this post. You like your privacy, and…..
“Privacy is not a crime.”
People here have no need or right to know what happened to you, if you leave the site for any reason – temporarily or permanently.
That said, friendships develop, and we worry about our friends worrying. Many of us have been together on this site for approaching 4 years, and for many of us, 4 to 8 years on CTH before that. Think about it! That’s a long time. We have talked more to each other online, than with many “real” friends in “real life”!!!
Thus, if you’re one of those people who feels a need to “stay in touch” with the group here, in the event of hospitalization or death, then please read on.
When I talked about what happened to Wheatie, two people – cthulhu and Aubergine – immediately commented about making arrangements for the blog to be notified in the event of tragedy. Cthulhu estimated only a 30% chance of this “digital legacy” working – Aubergine estimated 15%. That will do in a pinch, but hopefully this post will give all of you some tips to raise the percentage.
First, let me explain something important. ANYBODY can post on this site, and I WILL see it. This means that you can always get word to the gang via me or one of the authors.
So – if you are in the hospital, and can get online somehow, or can instruct somebody else to get online, all they have to do is get on this site (theqtree.com) on somebody’s phone and leave a comment AS A GUEST on any post, and I WILL see it, and it will NOT publish. If you want it to be for my eyes only, then make the comment on any one of my posts, such as the Monday open thread – otherwise, depat, bakocarl, SteveinCO, or any other author of that post particular post will ALSO see the comment (in addition to me).
You don’t have to use your normal information on this strange device, although you can do it if you want to do it. Perhaps you’re using a trusted relative’s device. Perhaps you’re borrowing a phone from a nurse or hospital staff member. The point is, you can identify yourself in the message of the comment. If I need to, I’ll respond to you in the same article or daily open thread.
The reason this works is that ALL NEW COMMENTS from new users, as well as comments with a new origin or some other change (including spelling errors), will always go into moderation, where I will see them.
You are “never alone” from your friends from this site, if you can get on the internet somehow.
However, this only takes care of situations where YOU are able to communicate. What if you can’t? What if you are intubated in an ICU, in a coma, or even GONE?
For these situations, you need to leave instructions with SOMEBODY. Those instructions can be at any level of formality or legality. AGAIN, your friends and relatives can ALL comment on this site, and I will get their comment in moderation, if they have never commented here before. I can then make a judgement of what information should be passed on to the group, per the instructions passed on to me.
You are welcome to test this out on a friend or family member’s device. I will NOT approve the comment, but I will tell you if it worked. That way it will work exactly the same, the next time, in a real situation.
Some people leave a digital legacy – which is a new feature in the Apple world. This means that people can leave control of their devices to a spouse, friend, relative, or business partner.
Other people leave their usernames and passwords to their survivors. Still others end up having some computer or phone professional get into the devices – if it’s even possible.
Please feel free to discuss personal plans in the comments, or to “test out” your plan, if you’re unsure.
But now, we have to talk about something else.
We have to talk about my plan for the site.
The Group Plan
The advantage of having a single admin who is a “security hardcore” is that there are very few social hacks that can get around site security. The disadvantage is that this single point of failure means that the entire site may fail. And yet, THAT is part of the plan. Most members here are already active on several allied sites. We also have a Gab group where people can meet freely. We have plenty of back-up. This site can disappear tomorrow, and the GROUP survives.
The value of our site is not in the archival content, as much as it is in the organic continuity of research and understanding. The primary strength of the site is in our evolving conversation and thoughts, which include many alternative viewpoints and beliefs.
Our strength is in our community, not in this site per se.
Thus, I always regard our community as its own failsafe plan. If something happens to me, and/or to this site, you all will figure out what to do.
Indeed, some of us made continuity plans in the very beginning of the site. The strategy was somewhat Alexandrian. By many of us secretly preparing to lead future alternative sites, the regime would have to play whack-a-mole to stop us.
And look at us now. Look how many healthy, viable, and active or potentially active blogs and discussion sites were created by members here.
THAT is our true safety net. This site can literally VANISH OVERNIGHT, and yet the GROUP lives on.
Now, since none of you noticed my being in the hospital, any of the times it happened, it would seem that my plan for such circumstances is both working and well-tested.
The problem is, that if I die, there need to be further arrangements. I will be shoring up the contingency plans for my “sudden departure” during the next few months. My main concern is preservation of the contents on the internet. It is likely that I can leave a small trust to support the site for a number of months or years, or at least long enough to copy the contents, if desired. The problem is then handing over administration. That gets tricky, and I need to consider the options. That will not be arranged in the open.
Right now, the cost of the site is roughly $1500 a year, but it will likely rise rapidly under Bidenomics. For other reasons, however, we may also want to move the site to a new host, depending upon what happens with our nutty regime trying to start World War III. In that event, the cost may increase or decrease. We have already been hit by a 10% energy cost increase. Don’t ask about the exact circumstances – just know that Biden is why.
Therefore, in the event of my demise, it may be best to “start over” on a free site somewhere, with a new admin, and then re-grow from that colonization.
We’ll see. I will say this. I’m not worried.
In God We Trust
You can worry about your legacy here – or you can forget about it. Ultimately, God is in control, and will correct your errors. Trusting in God will see you through.
The world to worry about is not this one – it is the spiritual world that only vaguely but beautifully intersects our own world, through us. Stand up for Truth, and the Spirit of Truth which defends Truth. Defend the Kingdom of Heaven, and its footprint in this world.
Ashes to ashes. Dust to dust. But from that fire, arises a light that pleases The Lord. Help to make it so.
TL;DR – “I believe that mRNA vaccines have serious risks that would be REVEALED by approval of the Novavax vaccine.” –Wolf Moon
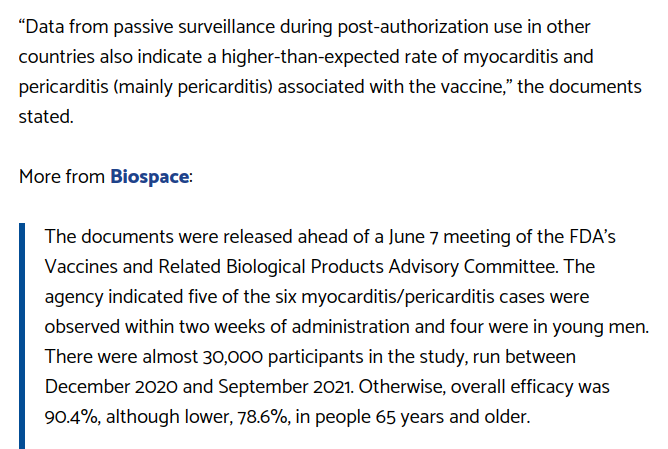
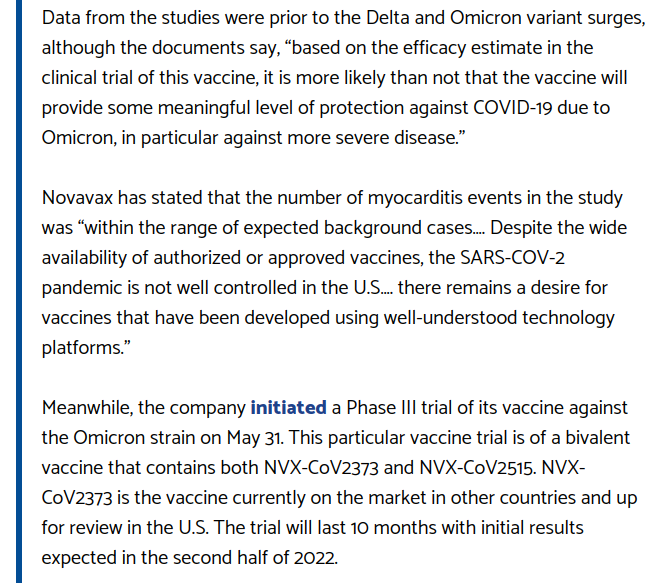
I’m actually surprised that FDA and Pfizer/China allowed Novavax to get this close to approval, but they clearly have the upcoming vote RIGGED, just like the 2020 election. The trusty “board mules” that FDA’s Pfizer-lovin’, China-compromised top brass used to approve dangerously experimental, “China-tested”, mRNA vaccines, will suddenly get some phony backbone on myocarditis and virtue signal against a less dangerous vaccine.
Remember Trump getting angry about what FDA and Pfizer (which is really China) did to the J+J vaccine? Same thing.
“Blame the victim.”
It’s how they work, people. And once you see it, you can’t unsee it.
Allow me to explain.
Let’s start off with how I instantly realized what’s in the cards.
As seen on Gateway Pundit, minus my scientific and political explanation of what is going on.
This is CLEARLY a set-up to knife Novavax right before a crucial vote. But first, you need to know two things.
(1) Pfizer and Fauci BURNED THE PFIZER mRNA VACCINE PLACEBO GROUPS to hide the problems with the Pfizer vaccine. (The relevance of placebo groups will be explained a bit later.)
(2) According to Pfizer, which proudly revealed the following fact directly from the mouths of Pfizer’s top brass in a more China-virtue-signaling moment (look it up), ALL of their clinical trials (including all the COVID clinical trials of the past) are now run out of China.
SO – if you see all the SHADY SCIENCE that is popping up in the Pfizer documents, and is now being revealed thanks to Naomi Wolf, there is a simple explanation of why Pfizer burned their placebo groups, making it impossible for people to “check their math”.
CHINESE ETHICS (or lack thereof) are in charge of Pfizer’s clinical trials for all drugs and vaccines.
This is the same China that lies and cheats routinely on all things financial, business, manufacturing, etc. They’re the ones in charge of testing the drugs you are being forced to take by “China Joe”.
Yeah. Pretty convenient. Same vaccine our military is forced to take, too. VERY convenient.
This is a perfect example of “total warfare”, TBH. But let’s set that aside for now.
It’s now very clear that the spike protein is a pathogen. We have gone through all the problems of using the pathogenic spike protein as an immunogen (which Robert Malone warned about, by the way, and which FDA ignored). The spike protein causes a lot of problems, including myocarditis and pericarditis, just like the disease itself. Those problems, however, are compounded by TWO aspects of the technology of the Pfizer mRNA vaccines.
(1) mRNA technology itself is dangerous, because the pseudo-mRNA doesn’t shut down promptly, and in principle can never truly meter the amount of pseudo-spike-protein produced. It can dangerously overproduce the protein.
(2) the lipid nanoparticles used by Pfizer reduce acute symptoms by a kind of delayed release, but this also leads to unnatural persistence, migration throughout the body, excretion of the vaccine itself in body lipids (otherwise known as “exposure” or “shedding”), and a variety of symptoms which differ from the disease itself.
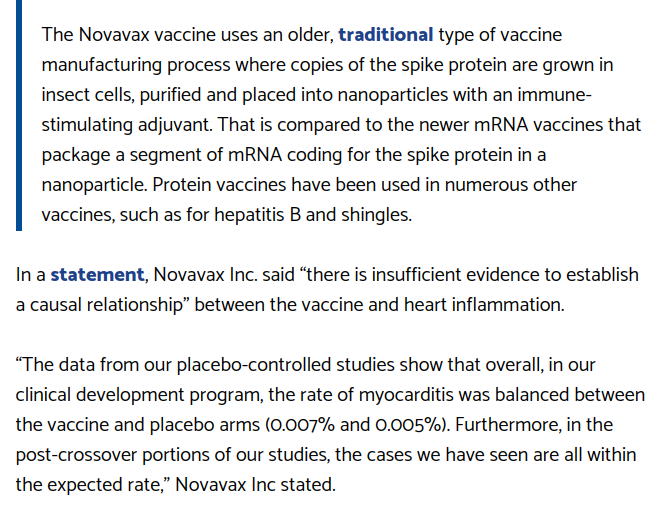
These problems are sidestepped by the more well-understood Novavax approach, which being based on a protein vaccine uses a DIFFERENT kind of “nanoparticle” to present a fully formed pseudo-spike-protein – NOT the mRNA for such, to the cells of the recipient. The spike protein is NOT coated with a lipid envelope, but rather is presented in a “ball of spikes” manner similar to an actual virus.
It is extremely likely that protein vaccines like Novavax and Corbevax are – certainly at the moment – substantially safer than mRNA vaccines. That is an EASY hypothesis to make at this point. Any honest scientist who has seen the data so far could make it. Robert Malone, who deeply understands the mRNA technology, which he properly labels “immature“, gets it totally.
One way to see if the relative safety of current protein tech over current mRNA tech is true, would be to approve the very likely safer Novavax and/or Corbevax in the United States, and to begin letting the data from adverse events flow into the VAERS reporting system. This data would get beyond the “small set” problem of the current trial data.
It’s quite obvious WHY Pfizer and FDA would not want this to happen.
It is extremely likely that Novavax and Corbevax would show greater safety relative to both Pfizer and Moderna. This would naturally lead to the question of why Novavax wasn’t fast-tracked to American citizens in 2020 and 2021, instead of Pfizer and Moderna.
Get it? This is a COVER-UP.
Now – let’s look at the actual data. Novavax is underplaying their hand.
Novavax not being Pfizer, the latter with a known, CONVICTED track record of lying and cheating (particularly after they stupidly entrusted their clinical trials to CHINA), let’s assume for a moment that MAYBE the Novavax clinical trial data is not total lies.
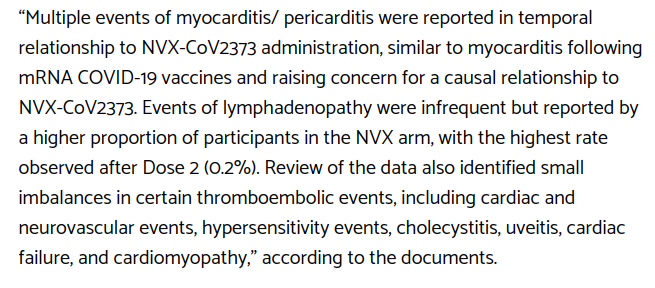
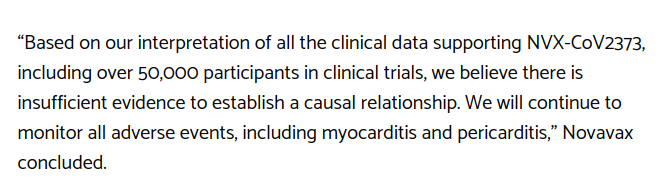
Here is the Novavax statement about the myocarditis/pericarditis issue:
NEWS & MEDIA
Novavax Statement on US FDA Briefing Document Related to Myocarditis/Pericarditis
Jun 3, 2022
Throughout the pandemic, as publicly available vaccines have been administered, there have been numerous investigations into findings related to myocarditis. We have learned that we can expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk. Myocarditis is most often caused by nonspecific viral infections.
The data from our placebo-controlled studies show that overall, in our clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%). Furthermore, in the post-crossover portions of our studies, the cases we have seen are all within the expected rate.
Based on our interpretation of all the clinical data supporting NVX-CoV2373, including over 50,000 participants in clinical trials, we believe there is insufficient evidence to establish a causal relationship. We will continue to monitor all adverse events, including myocarditis and pericarditis.
There are two ways to read this. Both of them argue correctly that the Novavax vaccine should be approved.
One way is to read it at “happy face value”. You are perfectly capable of doing that yourselves.
The other way is to read it, both knowing and admitting the hard truths about these vaccines, and what is actually possible when you make a vaccine against a minor coronavirus, for which the very need and justification are arguable at best.
I will read it the second, more conservative way, and you can follow along, sentence by sentence.
Throughout the pandemic, as publicly available vaccines have been administered, there have been numerous investigations into findings related to myocarditis.
This is another way of carefully admitting that myocarditis (more serious than pericarditis) is a real problem of the vaccines, because it’s a problem of the disease, because they both use the pathogenic spike protein.
We have learned that we can expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.
This is true. We’ve learned that myocarditis is a natural background problem for young people, and that the spike protein of the disease, BUT EVEN MORE THE SPIKE PROTEIN OF VACCINES, raises that risk for young people. All of this applying more to young MALES.
Myocarditis is most often caused by nonspecific viral infections.
This is true in general. But it can also be caused by vaccines for viruses, as one might rightly expect, because vaccines are INTENDED as a limited case of the disease.
The data from our placebo-controlled studies show that overall, in our clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%).
This is nice data for Novavax. Yes, the Novavax vaccine raises the risk of myocarditis in those who take it, but that risk is already minuscule, with Novavax only raising it by less than 50%. If you HAD to vaccinate kids, which we don’t, then Novavax is a relatively safe alternative, IMO.
Personally, I don’t think that children need the human vaccine AT ALL, because the DISEASE IS A BETTER VACCINE FOR KIDS. Yeah, think about it. Diseases can be vaccines, and vaccines can be diseases. Open your mind to the history of science, when we knew this stuff.
Furthermore, in the post-crossover portions of our studies, the cases we have seen are all within the expected rate.
This is sneaky wording, but it’s a bit of a KNIFE pointed back at FDA. They all KNOW that this applies to all the other vaccines. And maybe even MORE SO in the case of mRNA vaccines.
What exactly IS the “expected rate” of myocarditis? I’m betting strongly that the “expected rate” of myocarditis and pericarditis GOES UP in all vaccinees, just like it goes up in all people who get COVID and don’t treat it, and that the increase takes the form of probability spiking after the vaccination, then settling down to a slightly elevated risk (vs. before vaccination), further increasing with age.
Does FDA want to go there? Probably not.
Based on our interpretation of all the clinical data supporting NVX-CoV2373, including over 50,000 participants in clinical trials, we believe there is insufficient evidence to establish a causal relationship.
This may very well be true. The clinical set may simply be too small to state conclusively that the difference of 0.002% between vaccine (0.007%) and placebo (0.005%) was caused by anything but randomness. Note that I, personally, am assuming the worst case – that this difference of 0.002% IS IN FACT caused by the pseudo-spike-protein of the vaccine – and am saying that this is still NOT reason enough to not approve the vaccine. APPROVAL will very likely give us the VAERS data to PROVE that there is real risk to all the vaccines, but that it is LESS for Novavax and (if they ever approve it) Corbevax.
And note that I am talking about ALL RISKS – not just myocarditis. My money would be on Novavax being safer than mRNA vaccines in terms of every possible metric, including (very importantly) general immunity. I believe that mRNA vaccines have serious risks that would be REVEALED by approval of the Novavax vaccine.
We will continue to monitor all adverse events, including myocarditis and pericarditis.
Oh, that is a beautiful jab at Pfizer, which BURNED their placebo group.
What will you bet that Novavax is carefully protecting the integrity of their placebo group, because they’re not afraid of the evidence – like Pfizer/China?
Think very carefully about not approving Novavax, FDA. I’ve had your number for quite a while here. Better for you to swallow the bitter medicine of TRUTH, than to let this fester with a China-style cover-up that we will out on these pages every day for many moons.
Risks, Bets, Rewards and Losses – Why Vaccine-Conferred and Disease-Conferred Immunity are Both Proper Personal Gambles When Choice is Free and Enough Truth is Known or Unknown
Many of us were shocked that President Trump just showed his “pro-vax” hand in an interview with vaxx nutt Bill O’Reilly, but if you watch Trump long enough, you realize that he very often gets to the optimal perspective before anybody else – even with incomplete data.
It’s worth wondering why Trump said what he said, and said it when he said it.
Beyond the “credit” issue – which I can really see for many reasons, not the least of which is because Trump’s plan really messed up the Cabal plans on COVID – I think Trump knows people who are seeing the emerging data. And I think they are advising him correctly.
I’m going to try to show you some of that data, and what it means.
Rand Paul is a sharp guy, too. Trump respects Rand Paul. It pays to ask why. I think that part of it is because Rand is a doctor. Trump respects doctors, I am convinced. And Trump knows that doctors differ in their opinions, like everybody else, and that he (Trump) needs to listen to a number of them, to see where the best perspective resides.
Rand is not anti-vaxx. He’s pro-natural-immunity. There is a difference.
At the place where Trump’s viewpoint and Rand Paul’s viewpoint intersect, you will find much truth. I certainly did. And when I added in a few other doctors “on our side”, and looked carefully at where I was skeptical of some of their thinking, but also let them convince me to be skeptical of some of my own thinking, I hit the jackpot.
BOTH the vaccines AND the disease make sense as alternative, risky, immunity-conferring antigens. Neither one is obviously superior to the other for everybody, because the landscape of risk and benefit is too complex, and depends far too much on the needs, goals, and medical circumstances of the individual. Worse still, past choices – including accidental ones – affect future choices.
Rand Paul saw right into this – that the CRUX of the problem is that “natural immunity” is being ignored by a monetarily, scientifically, and institutionally compromised medical establishment. Natural, disease-conferred immunity is the BEST CHOICE for many people – particularly when combined with a “delay of onset” strategy, and TREATMENT, which alters the risk/benefit. We have known this all along, yet we have never truly internalized it, because the “Let’s You And Him Fight” strategy of the OBAMA MANDATES has widened and deepened the division between those who choose vaccines and those who don’t.
AND LOGIC.
Trump GETS THIS. And he said so. We ARE falling into their trap. BUT we can turn that around on a DIME.
It is critical for our side – the free and sane medicine side – to EXPOSE and BASH the performance of the vaccines, because the other side won’t do it. But it is also critical that we STAND UP for the freedom for others to take those risky vaccines voluntarily, and accept the truth that it can make sense, during a period where we don’t know everything, and MAYBE beyond that, after we know more.
Mandates are absolutely stupid, reckless, and anti-science. They interfere with medicine. The mandating commies need to BTFO. But letting fearful people take a risky vaccine – a personal gamble – is a part of freedom that we have to respect.
I want to show you data that makes this make sense.
Some of you may be surprised that I am defending the COVID vaccines AT ALL. At present I have ZERO intention of taking one. For me, and my wife, they are a BAD medical choice. For many others, too.
Well, what if I tell you that in doing so, I can defend disease-conferred immunity EVEN MORE?
What if I tell you that I can now see why, strategically, Trump waited until we “knee-capped” – but didn’t kill – the vaccines?
BOTH SIDES HAD TO SEE MORE CLEARLY.
Let me help you see more clearly.
Natural Immunity – More Risk With More Reward?
What I just said there is not always true.
For CHILDREN, it appears that the vaccines are MORE RISK, LESS REWARD.
Yeah, Trump was right about that.
It’s a NO-BRAINER to NOT, NOT, NEVER, EVER give this shit to kids, and I personally hope that God himself does whatever is needed to save children from the MONSTERS who are injecting them with these RELATIVELY dangerous vaccines.
Kids are being deprived of EXCELLENT natural immunity, for JUNK immunity that makes money for Big Pharma.
Just for starters, we may be condemning these kids to a lifetime of life-robbing spike boosters, just by virtue of a well-understood idea of “original antigenic sin”, or OAS. OAS is where one antigen leads to an inappropriate response to a later antigen, vaccine, or infection.
This means that if we give children a misleading FIRST ANTIGENIC STIMULUS, they may then be STUCK with sub-optimal antibody immunity, leaving them for an unknown time at GREATER RISK from the disease. It may very well be that the BEST FIRST ANTIGEN for SARS-CoV-2 is the DISEASE – not a spike protein vaccine.
We don’t KNOW what will happen long-term when we inject kids. Or, at least, most of us don’t. Maybe Fauci does.
OLYMPUS DIGITAL CAMERA
Is it a good idea? Should we bet ALL our kids on that idea?
NO FREAKING WAY.
And THAT is assuming that these vaccines do nothing to affect fertility. If they DO affect fertility, then this has to be made a KNOWN and ADMITTED risk, at the very least – not covered up, like it is right now.
A call for Nuremberg II, more likely, if this was knowingly advanced.
Who wants to risk their kids’ chance of having children?
This brings up the question of whether parents have the right to *knowingly* neuter their kids. Some parents already are, by “transing” kids. I think it’s pretty clear that’s where the Cabal is going – neutering and spaying humans. Interesting question. Should it be sent to SCOFFLAW SCOTUS? How is Amy Comey Barren going to vote on that one?
Asking for a FIEND.
I would even extend that thinking to teens and young adults. There is no reason that I can see to give them the vaccine. But should they have that choice, in consultation with their doctors? Interesting question. Very hard to reconcile a pro-life position with that, isn’t it?
But back to natural immunity.
Natural Immunity – More Rewards
Are there, in fact, more rewards?
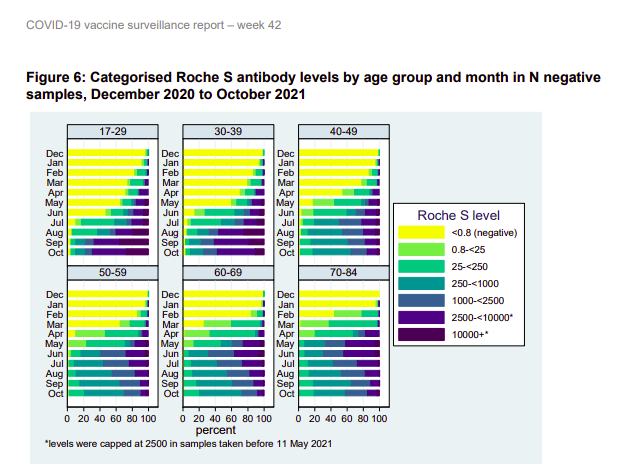
I think so. Look at these two figures from the UK Ministry of Health, showing spike protein antibodies in people in England in 2021.
The darker the color, the stronger the antibodies.
The first graphs are people who have no evidence of having caught the disease (N protein negative). They include the unvaccinated uninfected and the vaccinated uninfected.
The yellow is the unvaccinated people who have not caught the disease – mostly kids.
Green, blue and purple are various levels of vaccination success – the darker, the more spike antibodies.
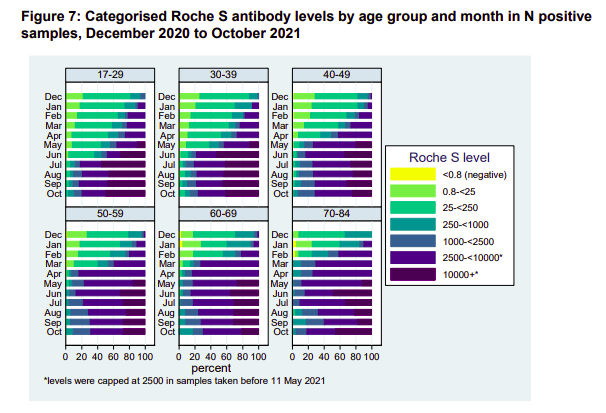
Now look at people who got some or all of their spike immunity by natural infection with the disease.
Assuming it’s a wash as far as the quality of the antibodies – which is not necessarily true – it’s obvious that these recoverees have a more robust spike antibody immunity – to say nothing of likely immunity to some or all of the other 20+ proteins in SARS-CoV-2.
Rand Paul, right here. The man is asking the right questions.
So why is Fauci ignoring this natural immunity stuff?
Notice that KIDS don’t mount a strong spike immunity, even though they beat down the disease in a hurry, with minimal symptoms. This is likely an EVOLVED RESPONSE – an EVOLVED STRATEGY – a form of EVOLVED INTELLIGENCE. What it says is that kids “know” by evolution – don’t build a lasting defense to the ever-changing spike protein. Meanwhile, the virus tries to “rope-a-dope” us slowly into concentrating on the spike as we age, misleading us with each attack. We lean on the crutch of spike antibodies that don’t work on the next strain, or actually make things worse.
Kinda funny that Fauci and the “follow the science” types don’t respect this signal from evolution, but whatever. That’s the basis of another post. But keep it in mind – it’s likely important.
So let us not digress.
The bottom line is that IF you’re going to make spike antibody immunity your standard of success, which Fauci and company clearly have, as part of Fauci’s “antibody hypnosis”, then by that standard, “natural immunity” from the disease gives MORE REWARD.
And again, I remind you, there are MANY other metrics of immunological success which are highly relevant, and which are ignored under Fauci spike antibody hypnosis. Always keep that in mind.
Natural Immunity – More Risks
SO – is the disease “more risk” to get that more reward?
My answer would be “maybe”.
It’s a complex calculation – particularly if you factor in “not getting the disease until you get it”. When you vaccinate, it’s a down payment in full, and with boosters, you’re even stuck with installments. You are “accepting that the risks happen” at 100%. Vaccination “collapses the probabilities”. But if you take your chances on the disease, by simply not vaccinating, you are delaying the (probably) higher risk, but the “risk over time” is substantially reduced.
Imagine the “payoff” of not vaccinating or getting the disease until Omicron. That would have been a GREAT gamble and winnings.
But let’s look at an ACTUAL COMPARATIVE RISK of vaccine vs. disease.
Now – let me be clear from the start – this article is a CLICK-BAIT CHERRY-PICKING of the highest order. The title numbers SEEM shocking – until you dig into it, and go to the source.
But still, they’re not “lying”. It’s just misguided. But that CHAFF led me to WHEAT.
Let me include the entire, short report, as it appeared in GWP.
On December 14th, 2021, Nature Medicine released a study based on a broad population data set analyzed by researchers at Oxford University. The researchers examined the risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination and infection.
The Oxford researchers reveal that 1 in 100 or 1% of all vaccinated individuals were admitted to the hospital or died with arrhythmia or irregular heartbeat.
Of the 38,615,491 vaccinated individuals included in our study, 385,508 (1.0%) were admitted to hospital with or died from cardiac arrhythmia at any time in the study period (either before or after vaccination); 86,754 (0.2%) of these occurred in the 1-28 days after any dose of vaccine. Of those who were admitted or died 39,897 (10.3%) had a SARS-CoV-2 positive test, with 29,694 (7.7%) having a positive test before vaccination. There were 7,795 deaths with cardiac arrhythmia recorded as the cause of death (1,108 had a SARS-CoV-2 positive test).
So 1 in 100 of the vaccinated individuals are going to the hospital with irregular heart beat and this isn’t international headlines?
This study appeared in the journal NATURE. That is the big leagues. We have to take this seriously. But let’s look at it closely. It REALLY helps to see that entire document, although SUSPICIOUS CAT should come out, just looking at the TITLE.
Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection
See? This isn’t just about the vaccines – it looks at infection, too. Is Gateway Pundit giving us the full story? Maybe not.
ABSTRACT:
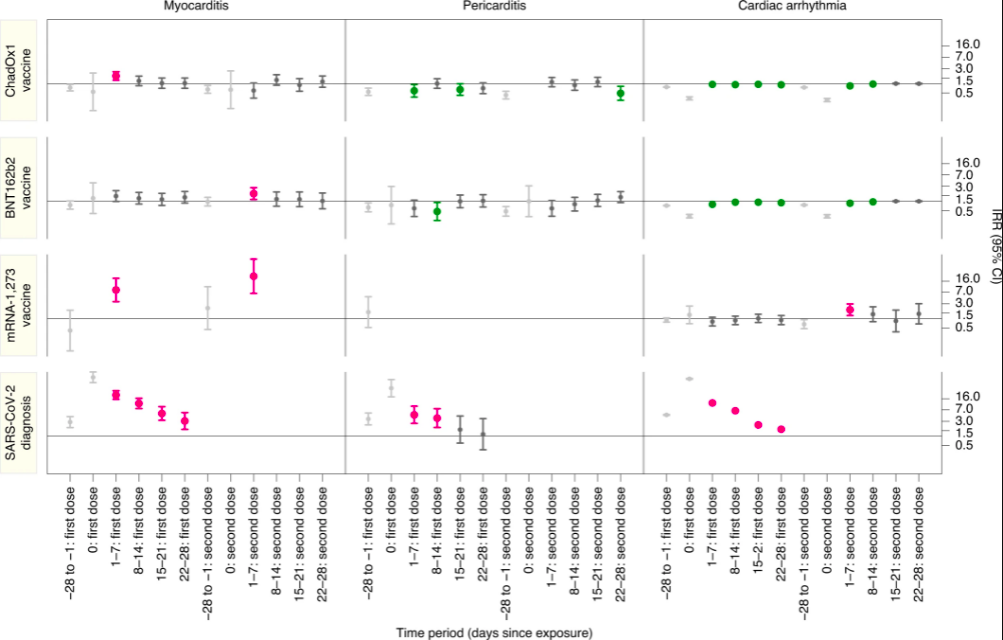
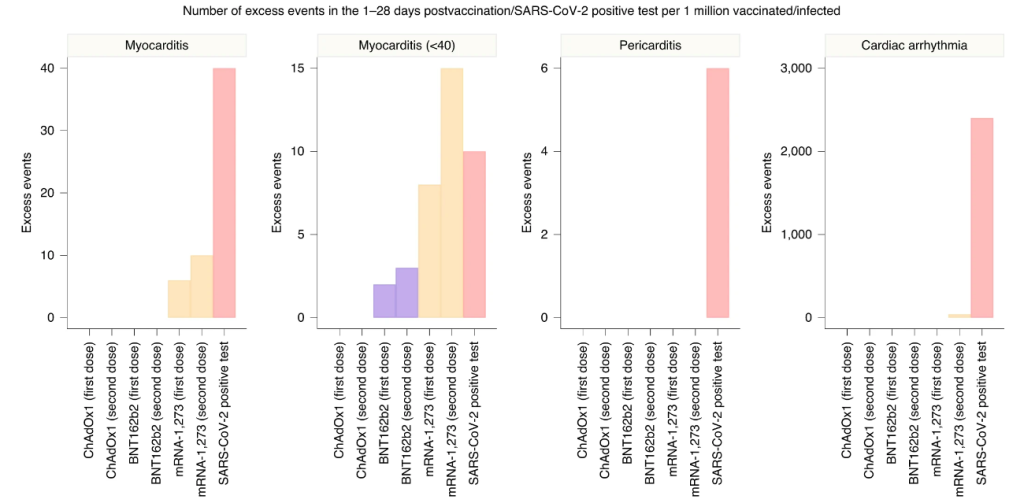
Although myocarditis and pericarditis were not observed as adverse events in coronavirus disease 2019 (COVID-19) vaccine trials, there have been numerous reports of suspected cases following vaccination in the general population. We undertook a self-controlled case series study of people aged 16 or older vaccinated for COVID-19 in England between 1 December 2020 and 24 August 2021 to investigate hospital admission or death from myocarditis, pericarditis and cardiac arrhythmias in the 1–28 days following adenovirus (ChAdOx1, n = 20,615,911) or messenger RNA-based (BNT162b2, n = 16,993,389; mRNA-1273, n = 1,006,191) vaccines or a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positive test (n = 3,028,867). We found increased risks of myocarditis associated with the first dose of ChAdOx1 and BNT162b2 vaccines and the first and second doses of the mRNA-1273 vaccine over the 1–28 days postvaccination period, and after a SARS-CoV-2 positive test. We estimated an extra two (95% confidence interval (CI) 0, 3), one (95% CI 0, 2) and six (95% CI 2, 8) myocarditis events per 1 million people vaccinated with ChAdOx1, BNT162b2 and mRNA-1273, respectively, in the 28 days following a first dose and an extra ten (95% CI 7, 11) myocarditis events per 1 million vaccinated in the 28 days after a second dose of mRNA-1273. This compares with an extra 40 (95% CI 38, 41) myocarditis events per 1 million patients in the 28 days following a SARS-CoV-2 positive test. We also observed increased risks of pericarditis and cardiac arrhythmias following a positive SARS-CoV-2 test. Similar associations were not observed with any of the COVID-19 vaccines, apart from an increased risk of arrhythmia following a second dose of mRNA-1273. Subgroup analyses by age showed the increased risk of myocarditis associated with the two mRNA vaccines was present only in those younger than 40.
The TRUTH is right in there.
First, we have to remember that GWP was concentrating on 1% of vaccinated people during the study period, INCLUDING before they got vaccinated, going to the hospital for or dying from a cardiac arrhythmia. That “before they got vaccinated” point is a TIP, right there, that we really need to consider the risk for UNVACCINATED people, too – including these very same people – for comparison. And as an aside, what is the number for corresponding unvaccinated people? You can almost guess that for most old people, it’s gonna be – well – maybe 1%?
And indeed, when the researchers compared the risk of an “event” against the risks of these patients BEFORE vaccination, they got their answers.
The WORST CASE for the vaccines was myocarditis. So let’s look at that, first.
Here is the risk from the vaccines. Broken out with [notations] so it’s easy to understand.
We found increased risks of myocarditis …
associated with the first dose of ChAdOx1 [AstraZeneca] and BNT162b2 [Pfizer] vaccines
and the first and second doses of the mRNA-1273 [Moderna] vaccine
over the 1–28 days postvaccination period,
and after a SARS-CoV-2 positive test. [STRONGLY NOTE THIS!!!]
We estimated an extra two (95% confidence interval (CI) 0, 3),
one (95% CI 0, 2)
and six (95% CI 2, 8)
myocarditis events per 1 million people vaccinated with ChAdOx1, BNT162b2 and mRNA-1273, respectively,
in the 28 days following a first dose
and an extra ten (95% CI 7, 11) myocarditis events per 1 million
vaccinated in the 28 days after a second dose of mRNA-1273.
SO – this confirms what we know. The vaccines cause myocarditis. It’s a RISK. It’s a handful or two in a million, per injection.
But now, let’s look at the NEXT LINE.
This compares with an extra 40 (95% CI 38, 41)
myocarditis events per 1 million patients
in the 28 days following a SARS-CoV-2 positive test.
What this says TO ME is that the risk of this one heart problem, in a vaccine that gives less immunity, is a significant fraction of the same risk from the disease.
Obviously due to the SPIKE PROTEIN, and possibly with a simple correlation to exposure.
I will admit that it’s LESS RISK from the vaccines, but not all that much.
Look at MODERNA.
The compiled risk of myocarditis from the TWO SHOTS (6+10 = 16) is 40% of the disease risk (40).
And yet HERE is how the authors have to word things to get it past the referees and editors.
“In summary, this population-based study quantifies for the first time the risk of several rare cardiac adverse events associated with three COVID-19 vaccines as well as SARS-CoV-2 infection. Vaccination for SARS-CoV-2 in adults was associated with a small increase in the risk of myocarditis within a week of receiving the first dose of both adenovirus and mRNA vaccines, and after the second dose of both mRNA vaccines. By contrast, SARS-CoV-2 infection was associated with a substantial increase in the risk of hospitalization or death from myocarditis, pericarditis and cardiac arrhythmia.“
They played a lot of word games there – take it from a retired scientist. They are also STUDIOUSLY AVOIDING some big stories that would rub the industry wrong.
“Give the editors what they want.”
Now, before I examine that conclusion for further trickery on the “within a week” qualifier and several other points (not today), I just want to say that calling 16 “small” and 40 “substantial” is bullshit.
Author bias, implicit or imposed, as a virtue signal to Bill Gates’ “vaccine culture” in science.
I will bet MONEY that a third Moderna booster would come in at 14 or more, bringing the total myocarditis events from chronic spike protein exposure to 30 or more, AND at the 4th injection SURPASSING the risk of ONE untreated disease incidence.
Well, is it worth it?
I don’t want Dementia Joe telling ME that it’s worth it. I want to make that determination MYSELF.
And GUESS WHAT? I will also bet money that part of the reason that CDC wanted people to mix and match boosters was to get Moderna “recoverees” boosted with the less cardiotoxic Pfizer or J+J vaccines, while not admitting that…
….defects from each spike protein vaccine are cumulative.
See how that works? Science. It’s great when you’re HONEST.
And why IS Pfizer causing fewer cardiac problems? In my opinion, it is very likely because the vaccine is distributing more widely and slowly in the body, thanks to the extreme vaccine lipid nanoparticle longevity (hence shedding) and biodistribution – data that was hidden from us, but turned up in the Japanese freedom of information request.
To me, the fact that nobody sees or talks about this stuff, is just more evidence of “vaccine hypnosis” of academia, as noted by Peter McCullough.
The reality? PICK YOUR POISON. Disease or vaccine.
If we go back to the arrhythmia example, it turns out that the “shocking 1%” actually GOES AWAY when compared to the unvaccinated. This makes sense, when you recall the very common problem of “palpitation” sending people to the ER, long before “long COVID” was a thing.
Yeah, 1% is shocking, but it’s shocking for the unvaccinated, too. Gateway Pundit was just throwing unwarranted shade.
Now, let’s take a look at some GRAPHICS from the study. Pictures tell a thousand words – not all bad for the vaccines – not all bad for “natural immunity”.
On the left axis you have the three vaccines, AstraZeneca, Pfizer, and Moderna, followed by the disease.
On the bottom axis, time – repeated three times for the three diseases.
As you can see for cardiac arrhythmia (right side), the vaccines are basically fine, but the disease is problematic. This makes LOTS of sense, because the disease seems to cause many problems by nerve infiltration, secondary to vascular distribution, and those nervous system infections and inflammations are highly relevant for arrhythmias, whereas the vaccine is primarily a vascular villain, which does NOT reproduce and infiltrate.
The science makes sense here! Wonderful!
All of the vaccines have at least a little bit of myocarditis effect (left side), which is explained nicely by vascular distribution of the spike protein. Moderna, which is notorious for “disease-like symptoms” at the recipient experience level, is easily expected to have even more COVID-like spike protein effects that are not immediately obvious, such as myocarditis.
Big point – ONLY the disease (bottom side) kicks off all three diseases. THAT is what a virus can do, that a bare protein, or even a non-reproducing virus-like particle, cannot.
Everything is making sense here. Let’s look at ANOTHER view of the data.
This graph has some GREAT STUFF. The myocarditis comparison described in detail above, is the graph on the LEFT. The numbers for the vaccines look substantially less, but you can see how Moderna boosters would quickly approximate the disease, and are already like a “mild case” in terms of risks. The authors of the paper avoid talking about the cumulative risks, but it’s clear that “boosterama” is PRECISELY Fauci’s game plan, and it has problems that got solved for Moderna by mix-and-match boosters.
Fauci and Walensky. Always taking care of their companies. Yeah, I kinda get it. But you gotta be HARD-ASS with them, like Director Wolf Moon would be.
The whole vaccine thing – including a lot of other adverse effects I’ve mentioned previously but not discussed here – looks to me like a trade-off. These are NOT good vaccines. They’re actually pretty marginal. BUT for people who really don’t think they can take the disease, it could be a reasonable gamble, IMO.
There are LOTS of people who take these vaccines, and no problem. I know – I talk to them all the time. I’m the most vaccine-supportive vaccine skeptic on Earth. These people just dump everything to me, because they know I don’t judge them, but respect their decisions. I’m interested in what happened to them, and they tell me.
NADA. ZIP. The most common reaction. For those people, the shot may make sense. But there are a good number of others who get laid up hard for a day in bed, and it sounds almost as bad as COVID. I worry about them. Some – A LOT.
Now look at the second graph – myocarditis in younger people. Clearly Moderna is WAY out of whack, and the others are comparable to the disease when boosted. Again – for these people – really BAD vaccines. This is why you saw action on the vaccines. Get values up close to the disease, in terms of numerical risks, and the problem becomes an elevator pitch that everybody understands.
Pericarditis and arrhythmia? Purely a disease problem. This looks very good for the vaccine. This is what you WANT with a vaccine – to AVOID some problem of the disease. BUT – can we trust those numbers?
I think so, and I think that Gateway Pundit got burned by looking at COMMENTS on a blog post explaining the Nature study.
Public health policy in the USA and UK need to change fast. As a side note, if you listen to the mainstream media enough they’ll have you believing myocarditis is a mild symptom. Let me be clear, by definition, symptoms requiring hospitalization are defined as severe. What’s more, the average mortality rate of non-fulminant myocarditis is nearly 56% which is experienced within 3-10 years. Sadly, that is a consequence of the likely heart failure that develops after the acute phase of myocarditis has resolved. See picture below 👇🏻
All things considered, it is clear that individuals under 40 are at a high risk of experiencing vaccine induced myocarditis. The good news is, there are ways to deal with this. More specifically, increasing the time between the first and second dose, not giving boosters to all healthy individuals under 40, pausing Moderna for many under 30, and seeking the guidance of other countries. All of that makes for better public health policy and positive health outcomes. To finish, I will leave you with the words of a wise man, “Health care is vital to all of us some of the time, but public health is vital to all of us all of the time”. – C. Everett Koop
Wolf again.
Now – in the comments, somebody mentioned the “1% issue”, and I suspect this is where GWP picked it up. Sadly, the comment author deleted and restated their comment, probably after realizing it had spawned a widely read article.
Here is the replacement comment, with replies.
zuFpM5*M6 hr ago I erased my previous comment. The closer I look at this study, the more it freaks me out.
They compare vaxxed to vaxxed+covid and then declare covid is worse, but they measure rates of myocarditis/pericarditis in post covid with troponin levels and in post vaxx with hospitalization rates. Hmmmm
They don’t include any control group of unvaxxed. The vaxx+covid group should be compared to unvaxx+covid to determine the actual rate of post covid heart issues. This is not done that I can tell?
The vaccinated showed a 1% hospitalization rate for cardiac arrhythmia with ~385,000 in the period up to 28 days post vaccination. I tried to look up population rates of hospitalization and found some old news articles discussing ~350,000-500,000 hospitalizations annually for ‘atrial fibrillation’ for the entire US population. So a group of vaccinated in UK blew out the entire US annual budget of arrhythmia hospitalizations in a couple month period? And that isn’t a highlighted part of the research results but instead they compare only within the vaccinated group broken out by short temporal periods? Isn’t the most important thing the vaccinated versus background normal rate?
I begin to think this whole study was gamed to get vaccinated rates of these issues versus supposed covid rates so they could continue to say vaccines are safer, when the actual #s are showing a horrific rise in these issues. It is a preemptive narrative shaping attempt.
I am not a doctor, researcher or number cruncher, so if I am misunderstanding this, I would be interested to hear how.
br143 hr ago There’s no way to sugar coat the study.
Of the ~385,000 people with arrhythmia, 10.3% had a positive Covid-19 test, and 7.7% tested positive at some point prior to vaccination.
Even if you remove 18% of the total, that’s still an awful lot of people with arrhythmia. I suppose most of us have some form of arrhythmia at some time in our lives, but how many of us are treated in hospital?
zuFpM5*M3 hr ago Yes. I would not subtract them either. I feel that there would be a covid risk increase + vaccine risk increase + covid/vaccine interaction risk increase to account for. None of which can be done without estimating the covid risk increase by comparing with non-vaccinated covid patients.
This is where they lost me. They’re just tossing out “maybes”. Nothing jumps out at me as likely to change the result. I can even add my own experience with cardiovascular issues from the disease. They’re REAL. Very unlikely that the vaccines and disease would FLIP on the relative risks of arrhythmia.
Score 1 for the vaccines.
BACK TO THE TRUMP ISSUE.
Benefits of the Vaccine Admitted by Our Side
There is a GREAT video by Geert Vanden Bossche that I keep pushing, because it is one of the clearest explanations of why “leaky mass vaccination” is a bad idea. Note that this is from a pro-vaxxer who has indeed worked with vaccines for his whole career, and is a former member of GAVI.
He just demands good vaccines, and good public vaccination policy.
Now – if you jump to around 4:30 in the video, you can hear him list the positives of the clot shot. HOWEVER, it may be better to just invest some of your time in that 4 1/2 minutes where he warms up to that point, to understand that he’s putting the positives AND the negatives in context, and looking at the bigger picture to recommend that we NOT mass-vaccinate.
He is saying that we should NOT mass-vaccinate IN SPITE OF the benefits that he lists and explains.
a decrease of disease in many countries
decline of morbidity and mortality rates
less illness in people who got vaccinated
severe disease is resisted even when vaccinees are infected with variants
they will shed much less virus than the unvaccinated, even when infected with variants
seropositivity rates are increasing in the population thanks to vaccination
But THAT is where he begins to disagree with mass vaccination. He states that we will NOT reach herd immunity, due to variants, and he explains this fully.
Global Problems of Sub-Optimal Mass Vaccination
At 28:00 minutes, Geert explains what we need to do – which is NOT what public officials are doing.
The current mass vaccination program will make things worse, in the long term. Geert explains then the kinds of vaccines we really need – vaccines which can both generate sterilizing immunity, AND which prime the immune systems of their recipients toward cellular immunity.
Yeah, it’s a bit of a tough goal, but it’s realistic toward the challenges of the China virus, and honest about what we need to do.
So what does this mean about the benefits of the vaccine?
THEY ARE REAL, BUT THEY ARE SHORT-SIGHTED. And they are accompanied by risks. Not just to the vaccinees, but to ALL OF US ON THIS PLANET.
According to Geert, continued vaccination is going to HARM vaccinees, relative to the unvaccinated, who will need to avoid virus-shedding vaccinees. At that point, recoverees may be in the best position of all, but still – not great. ALL of us will be in trouble from the virus which will escape the vaccines.
Geert also explains how we can prove that he is correct – by looking at the mutations in the virus which is shed from vaccinees, which will show selection for more infectious variants, if he is correct.
Now – this is a GREAT interview of Geert by Dana Loesch, who looks more and more like Sandra Bullock for some reason, but what the heck – the shotgun shells on her microphone setup are EXCELLENT, very non-Bullock, and she gets a FANTASTIC explanation of the problem from Geert.
Geert actually talks about Omicron, and the DANGER of it potentially evolving to be MORE SEVERE.
Take a listen!
Does Trump know this stuff? I don’t know.
I personally believe that Geert is right. I am now of the opinion that most of what we are hearing from Robert Malone, Peter McCullough, and Geert Vanden Bossche is true, but that each one has to give a little toward the ultimate truth.
What does that look like to me?
Natural immunity is NOT permanent or complete toward other variants
Natural immunity is better than the vaccines, generally speaking, but not bulletproof
Untreated COVID is a loser relative to the vaccines, but treated COVID is a winner
McCullough’s natural immunity prediction based on SARS1 may be too confident
Malone’s whistleblower on more shedding by vaccinees may have been wrong or disinformation
Geert’s vax-brag of less shedding by vaccinees may have been too kind and not skeptical enough
We have to stop pushing the vaccines, for the good of humanity
We have to allow the vaccines to continue, at an acceptably lower rate, for research
We have to allow vaccines to change faster, to keep up with mutations, IF and only IF this will not PUSH the virus to mutate and select faster (immune pressure must be low enough)
We have to pursue the superior vaccines that Geert is specifying
We have to use infection, treatment, and recovery as a big gun to reach herd immunity
We have to let COVID burn out of epidemic status, to reach a treatable endemic status
We cannot do that with mass vaccination, so mandates must cease promptly and completely
Joe Biden and CDC must be stopped – by military power if need be – if they will not end the crazy mandates
Yeah, you heard me. We can’t let this demented bozo, backed by an evil Obama and China, make COVID worse by mass vaccination. Mandates are making things worse.
Freedom, Vaccines and Morality
Trump may not understand Geert Vanden Bossche’s warning, but if we set that aside as an unknown, you can understand where Trump is coming from.
If we want freedom, we have to let other people make stupid choices that affect them most of all. Vaccination is, in fact, one of those things. Indeed, it is by US seeing it that way, that I believe we will end this nightmare of division which PUMPS UP the vaxxies and the crazy mandates.
In the same way that there are vaxxies who now are defending OUR freedom to be unvaccinated, I believe we have to defend the right of people to stupidly (or smartly) take the vaccine. However, we MUST get the rate of vaccination DOWN below the level where immune pressure from the vaccine creates more and more infectious variants.
The FIRST thing is not to take the vaccine yourself, or give it to your children.
The SECOND thing is to fight for an end to mandates.
The THIRD thing is to fight for BETTER vaccines, and to expand belief that the current vaccines are NOT GOOD ENOUGH, and are of the WRONG TYPE. Make the vaxxies demand better, not defend bad vaxxes.
The FOURTH thing is to spread the message that the “socially responsible thing to do” is to support Vanden Bossche’s position, that NOT taking the vaccine NOW is what will ultimately “save grandma”.
The last one is a hard sell, with FAKE NEWS pumping vaccine stupidity, but hey – we’ve fought tougher battles already.
So what about Trump?
Well, he is not in the position to know or respond to the “Geert Vanden Bossche Question”. Not yet. It is only when that issue becomes BURNING HOT, that Trump will be able to smartly push FORWARD from the current stupid CLOT SHOTS.
We will have to RAISE VACCINE CONSCIOUSNESS to levels of understanding that SUBVERT FAKE NEWS. We can only do that by getting most of the vaxxies on our side – to demand BETTER vaccines.
If they want to be guinea pigs – GREAT. They can be heroes, and try the deadly experimental vaccines. But we should NOT be forcing all of humanity to be part of a BAD and MISGUIDED experiment.
And the JOKERS who are allegedly running our military need to understand this. Virtue signals which kill troops, even if slowly and quietly, where nobody can see them, are NOT ACTUALLY VIRTUOUS. I appreciate them kicking out the sane ones who understand that the current bad clot shots may cripple readiness at some point, rather than forcibly injecting them. We WILL have a reserve of trained people who are not destroyed by China and Biden, no matter what China’s coming chess moves. Thank you for that. But as for everything else – there could have been push-back against communism, instead of acquiescence.
Yes, we had to be shown. But I’m not sure showing us subservience to a COUP and CHINA and FAKE NEWS isn’t undoing half of the good stuff.
But this as well. If you guys delivered Omicron on purpose, thanks. It LOOKS like it may be working.
Merry Christmas!
W
Remember way back in July when I was banned by Twitter for saying that mandates were coming, vaccines weren’t working as promised and they’re gonna demand we all take boosters?