“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
This is a great selfie video, done by a young lady with a glorious Southern accent, chronicling her week of COVID-19 and recovery, treated with ivermectin. It’s short – just under 7 minutes – but it captures a lot of information about symptoms and relief by the drug. I can’t embed the video here due …
I think it’s really helpful for people to see and hear the reality of an individual COVID case, to see what to expect. This kind of information can absolutely reduce unnecessary fears. It’s a real service, IMO.
Well, Omicron is here, and it got here VERY fast (more later). THANKFULLY, somebody who GOT IT took extremely good notes, and put them online.
Specifically, a medical doctor, Dr. Henry Smith, Jr., who has published on American Thinker, got the disease, treated it with hydroxychloroquine, and recovered VERY nicely.
His account of the disease is MUST READ material. It’s short – no excuses!
Plus, he’s a photographer, and has lots of nice pictures on his site.
No preview! Please visit his site. I left a comment there, letting him know about antihistamines, because this is something that can get past the “pharmacy gestapo” that Biden and CDC have created.
As Steve has noted here, the 2X dosage of modern, 2nd-gen antihistamines is quite safe, and his own doctor prescribed 4X dosages. This is completely analogous to doctor’s prescription of ibuprofen at 800 mg, which is 4X the OTC 1-pill dose.
I know that ivermectin is “all the rage”, but hydroxychloroquine is still an excellent drug to treat COVID, and I think it’s great to see it in use here. As I recently noted, I believe that none other than Bill Gates was behind the “take-down” of HCQ in the medical literature, via funding of studies designed to knee-cap it.
Dr. Smith comes to FIVE conclusions about Omicron, 3 being numbered, and 2 bonus thoughts after those, made post-illness, all of which I find excellent and agreeable. Please visit his post to see what they are.
OH – and his American Thinker article – a short but powerful post on the OBVIOUSNESS of the solution – natural immunity – entitled “Who Isn’t Getting Infected?”, is definitely worth reading as well.
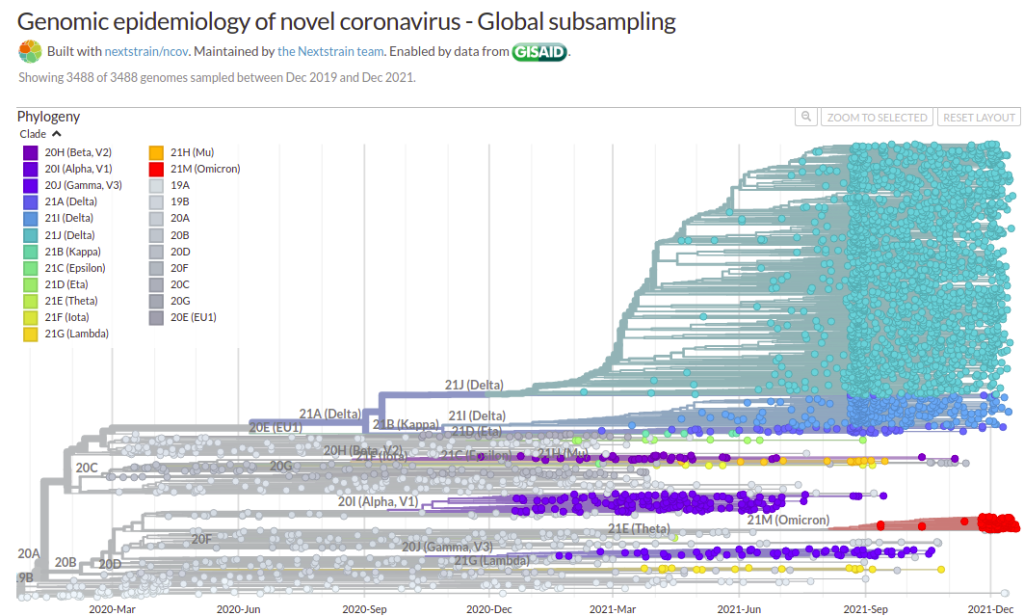
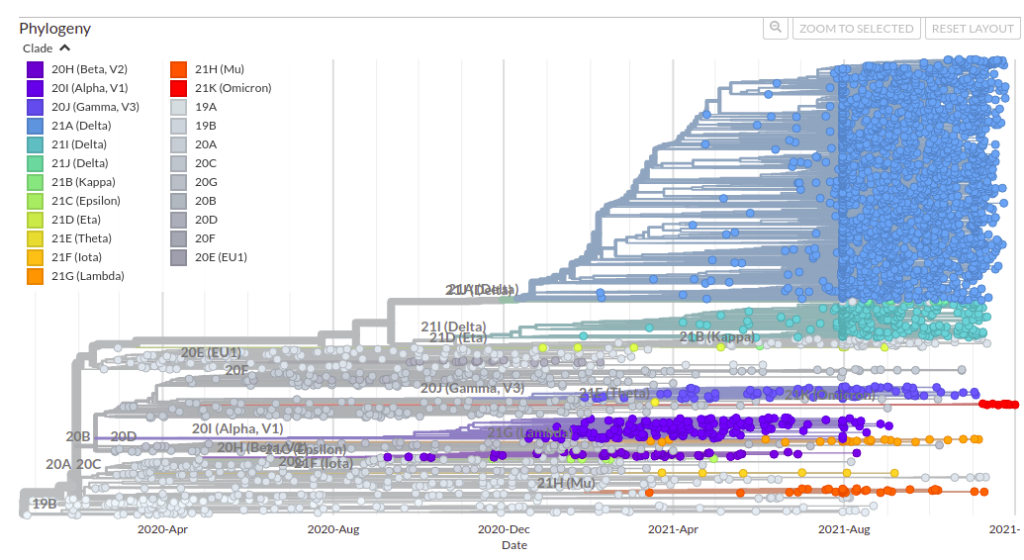
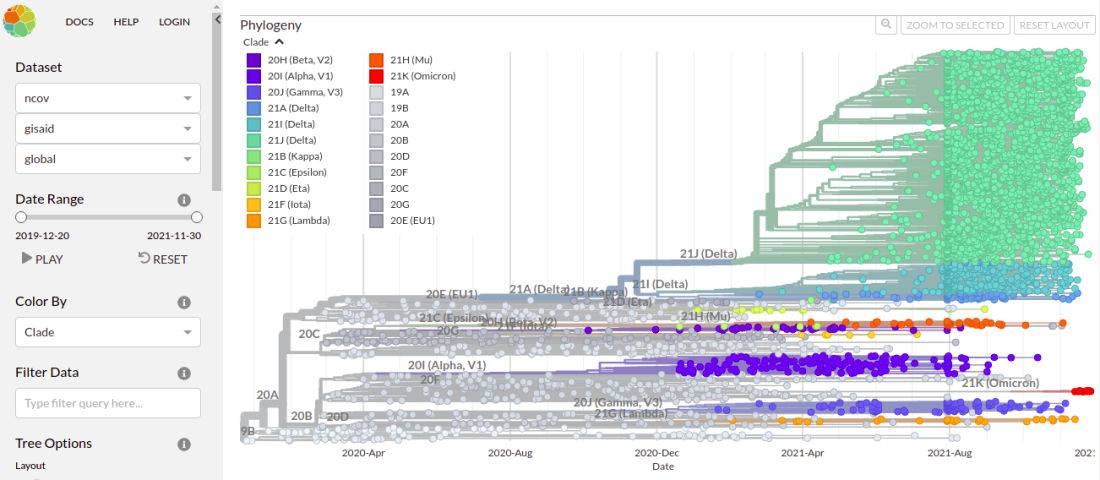
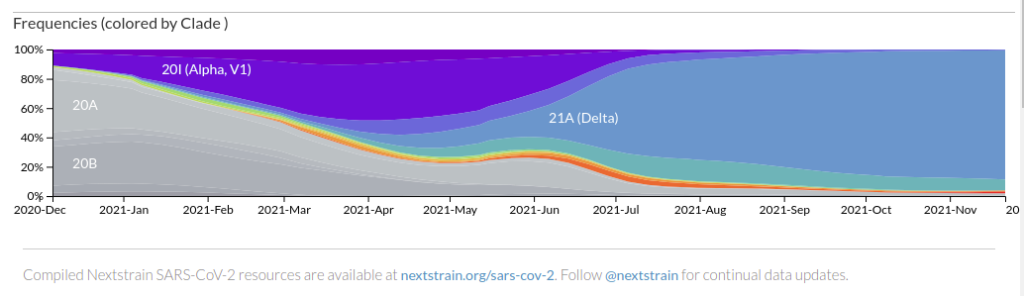
What this graph shows, is NOT “itty bitty” Omicron (red) sneaking up on “big old” Delta (turquoise).
It shows – at the extreme right edge – Omicron SQUASHING the Delta empire like a BUG. At the very edge, Delta basically STOPS – as Omicron keeps moving to the right.
Let’s look at an earlier screen capture from NextStrain. This one is GLOBAL, on December 4.
Here, you see the same thing I described above, but you see it earlier, because it took a while for the variant to travel to America, where it would displace Delta. The GLOBAL data is already showing Delta getting walloped.
From this, you can tell that I just missed Omicron. I had Delta with Day 0 (first symptoms) on November 26, and was likely infected on November 22 (yeah, not a good day). Everything in America was still DELTA at that time.
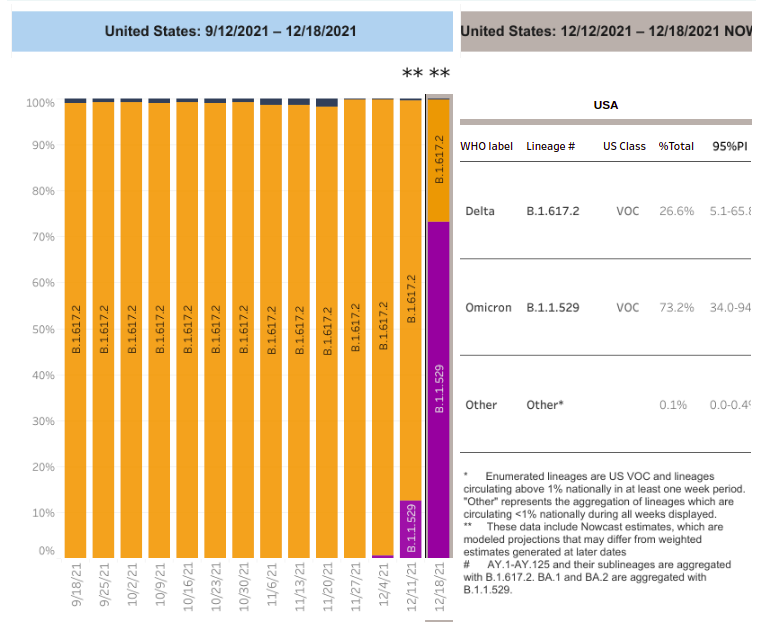
This is more easily seen in another graph. Source HERE at CDC.
Sadly, the current graphics will not archive properly.
As you can see, on 11/27/2021 in the United States, it was ALL DELTA. On 12/4, It was still almost all Delta. By 12/11, the United States was at over 10% Omicron, But ONE WEEK later, on 12/18, the USA was at
70% Omicron.
This is just INSTANT-FREAKIN’-TANEOUS.
Will it hit 100% Omicron?
Does it HAVE TO hit 100% Omicron to wipe out the nastier Delta?
Stay tuned….. for the next item.
3 – The Decline and Fall of the Omicron Variant
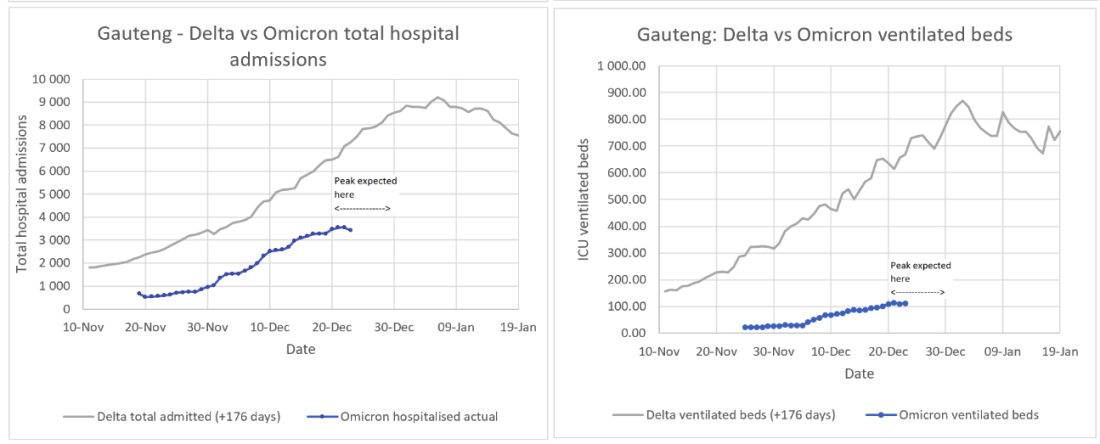
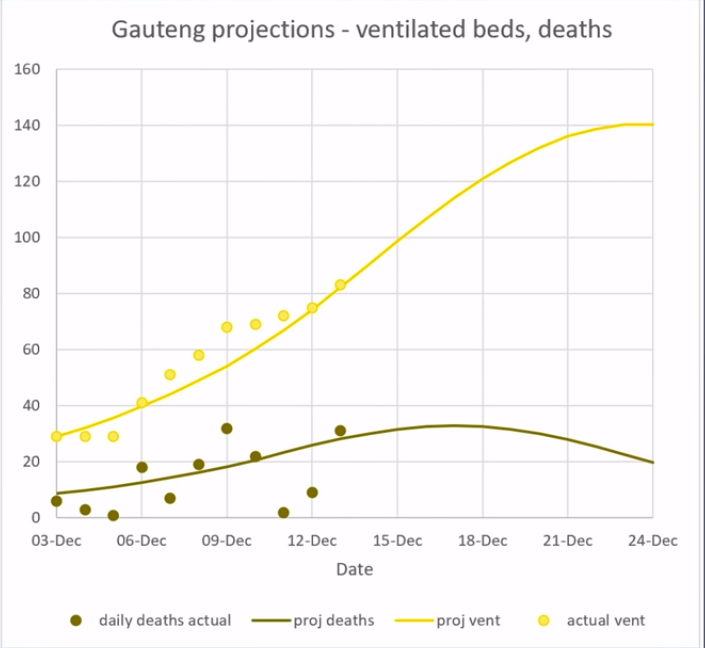
Hat tip to RF121 for this video, in which a South African engineering geek and university researcher, Pieter Streicher, who tracks and predicts COVID numbers, tells us what is going to happen to the Omicron variant, and is ALREADY happening in one of the “origin towns” in South Africa, where it is PAST THE PEAK.
I really recommend listening to this, because I am just grabbing a few things that caught my fancy. There is much, much more.
Streicher predicts that Omicron will PEAK and then DECLINE, leaving ultimately around 20% infected and recovered, maybe 30% tops.
It will NOT be a majority of the population.
Here is how Streicher’s predictions have been working so far:
Now – why would I trust this guy – and NOT the Imperial College guy who Bill Gates promoted?
YOU KNOW…..
THIS GUY.
Yeah, the guy who ignored his own lockdowns from dodgy overblown models, so he could do the old pokerino with another “damn near model”, Little Mrs. Rubylips, his married British intelligence handler mistress.
Well, Neil Ferguson’s predictions turned out to be WILDLY overblown.
Streicher, on the other hand, whose predicted curves and actual numbers you can see above, is predicting – at the PEAKS….
25-fold LOWER deaths for Omicron relative to Delta, and…..
6-fold LOWER ventilated hospital beds for Omicron vs. Delta.
SO – Untreated Omicron is NOT exactly free of risk, and we still need hydroxychloroquine or ivermectin to treat it.
AND – failing availability of those things, we need antihistamines and azithromycin – the Spanish protocol – implement widely, as I discussed earlier…..
Everybody underestimates Spain. The last letter in “PIGS” is far less of an insult than an error. Years ago, when I was at a conference, and Japanese industrial spies were getting me drunk (it was a great red wine), I decided that I had to give them SOMETHING for their time and effort, if only …
And if you doubt the utility of antihistamines against ALL variants of SARS-CoV-2, then you need the NEXT item to convince you otherwise.
4 – An Independent Discovery and Validation of Antihistamine Therapy for COVID-19 *and* for Both Long COVID and Genetic Vaccine Major Adverse Effects
THIS is worth getting the word out to doctors quickly. Hat tip to Gail Combs for bringing this critical video to my attention.
The antihistamine therapy for COVID-19 was independently discovered by a South African doctor, Dr. Shankara Chetty. Even more importantly, the doctor discovered the reasoning behind the therapy, and its applicability to both “long COVID” and vaccine side effects as well.
His REASONING is extremely convincing, and well-explained in the video.
This is a brilliant universal theory of severe COVID, long COVID, and vaccine side effects, which meshes quite perfectly with almost everything we know about SARS-CoV-2 and COVID-19.
Thus, we now have a universally available, over-the-counter treatment protocol for BOTH COVID and COVID vaccination side effects, the former of which was found to be 100% successful in TWO real-world studies, and which cannot be stopped by Fauci-controlled pharmacists or Gates-funded anti-studies.
This video is brilliant, because it really demonstrates how science is done, at the practicing level. A doctor and scientist, using observation and logic, figured out the antihistamine protocol BY REASONING FROM SYMPTOMS, rather than by observation of antihistamines as an accidentally useful therapy. Nevertheless, both independent discoveries confirm each other.
If, as it currently looks like from the South African experience, Omicron is less pathogenic, then this will help push Delta out, as it should decrease the likelihood that someone infected with Omicron will get re-infected with Delta.
Omicron has been shown to be highly transmissible and have extensive evasion of neutralizing antibody immunity elicited by vaccination and previous SARS-CoV-2 infection. Omicron infections are rapidly expanding worldwide often in the face of high levels of Delta infections. Here we characterized developing immunity to Omicron and investigated whether neutralizing immunity elicited by Omicron also enhances neutralizing immunity of the Delta variant. We enrolled both previously vaccinated and unvaccinated individuals who were infected with SARS-CoV-2 in the Omicron infection wave in South Africa soon after symptom onset. We then measured their ability to neutralize both Omicron and Delta virus at enrollment versus a median of 14 days after enrollment. Neutralization of Omicron increased 14-fold over this time, showing a developing antibody response to the variant. Importantly, there was an enhancement of Delta virus neutralization, which increased 4.4-fold. The increase in Delta variant neutralization in individuals infected with Omicron may result in decreased ability of Delta to re-infect those individuals. Along with emerging data indicating that Omicron, at this time in the pandemic, is less pathogenic than Delta, such an outcome may have positive implications in terms of decreasing the Covid-19 burden of severe disease.
Here are the critical points:
Importantly, there was an enhancement of Delta virus neutralization, which increased 4.4-fold.
The increase in Delta variant neutralization in individuals infected with Omicron may result in decreased ability of Delta to re-infect those individuals.
IMO, this is good news for people who are infected by Omicron. It is very likely that Omicron offers some real protection against Delta.
The degree of protection against Delta is roughly a THIRD of the degree of protection against Omicron itself which is afforded by infection with Omicron (4.4-fold vs. 14-fold). That’s still ballpark. Probably comparable to a Delta-specific vaccine.
Not bad at all, IMO. We’ll just have to see how real-world data pan out.
That’s all for now, but stay tuned.
Because YES – there’s MOAR.
W
John Fink, James Coburn, and Jennifer O’Neill having a meal in a scene from the film ‘The Carey Treatment’, 1972. (Photo by Metro-Goldwyn-Mayer/Getty Images)
Risks, Bets, Rewards and Losses – Why Vaccine-Conferred and Disease-Conferred Immunity are Both Proper Personal Gambles When Choice is Free and Enough Truth is Known or Unknown
Many of us were shocked that President Trump just showed his “pro-vax” hand in an interview with vaxx nutt Bill O’Reilly, but if you watch Trump long enough, you realize that he very often gets to the optimal perspective before anybody else – even with incomplete data.
It’s worth wondering why Trump said what he said, and said it when he said it.
Beyond the “credit” issue – which I can really see for many reasons, not the least of which is because Trump’s plan really messed up the Cabal plans on COVID – I think Trump knows people who are seeing the emerging data. And I think they are advising him correctly.
I’m going to try to show you some of that data, and what it means.
Rand Paul is a sharp guy, too. Trump respects Rand Paul. It pays to ask why. I think that part of it is because Rand is a doctor. Trump respects doctors, I am convinced. And Trump knows that doctors differ in their opinions, like everybody else, and that he (Trump) needs to listen to a number of them, to see where the best perspective resides.
Rand is not anti-vaxx. He’s pro-natural-immunity. There is a difference.
At the place where Trump’s viewpoint and Rand Paul’s viewpoint intersect, you will find much truth. I certainly did. And when I added in a few other doctors “on our side”, and looked carefully at where I was skeptical of some of their thinking, but also let them convince me to be skeptical of some of my own thinking, I hit the jackpot.
BOTH the vaccines AND the disease make sense as alternative, risky, immunity-conferring antigens. Neither one is obviously superior to the other for everybody, because the landscape of risk and benefit is too complex, and depends far too much on the needs, goals, and medical circumstances of the individual. Worse still, past choices – including accidental ones – affect future choices.
Rand Paul saw right into this – that the CRUX of the problem is that “natural immunity” is being ignored by a monetarily, scientifically, and institutionally compromised medical establishment. Natural, disease-conferred immunity is the BEST CHOICE for many people – particularly when combined with a “delay of onset” strategy, and TREATMENT, which alters the risk/benefit. We have known this all along, yet we have never truly internalized it, because the “Let’s You And Him Fight” strategy of the OBAMA MANDATES has widened and deepened the division between those who choose vaccines and those who don’t.
AND LOGIC.
Trump GETS THIS. And he said so. We ARE falling into their trap. BUT we can turn that around on a DIME.
It is critical for our side – the free and sane medicine side – to EXPOSE and BASH the performance of the vaccines, because the other side won’t do it. But it is also critical that we STAND UP for the freedom for others to take those risky vaccines voluntarily, and accept the truth that it can make sense, during a period where we don’t know everything, and MAYBE beyond that, after we know more.
Mandates are absolutely stupid, reckless, and anti-science. They interfere with medicine. The mandating commies need to BTFO. But letting fearful people take a risky vaccine – a personal gamble – is a part of freedom that we have to respect.
I want to show you data that makes this make sense.
Some of you may be surprised that I am defending the COVID vaccines AT ALL. At present I have ZERO intention of taking one. For me, and my wife, they are a BAD medical choice. For many others, too.
Well, what if I tell you that in doing so, I can defend disease-conferred immunity EVEN MORE?
What if I tell you that I can now see why, strategically, Trump waited until we “knee-capped” – but didn’t kill – the vaccines?
BOTH SIDES HAD TO SEE MORE CLEARLY.
Let me help you see more clearly.
Natural Immunity – More Risk With More Reward?
What I just said there is not always true.
For CHILDREN, it appears that the vaccines are MORE RISK, LESS REWARD.
Yeah, Trump was right about that.
It’s a NO-BRAINER to NOT, NOT, NEVER, EVER give this shit to kids, and I personally hope that God himself does whatever is needed to save children from the MONSTERS who are injecting them with these RELATIVELY dangerous vaccines.
Kids are being deprived of EXCELLENT natural immunity, for JUNK immunity that makes money for Big Pharma.
Just for starters, we may be condemning these kids to a lifetime of life-robbing spike boosters, just by virtue of a well-understood idea of “original antigenic sin”, or OAS. OAS is where one antigen leads to an inappropriate response to a later antigen, vaccine, or infection.
This means that if we give children a misleading FIRST ANTIGENIC STIMULUS, they may then be STUCK with sub-optimal antibody immunity, leaving them for an unknown time at GREATER RISK from the disease. It may very well be that the BEST FIRST ANTIGEN for SARS-CoV-2 is the DISEASE – not a spike protein vaccine.
We don’t KNOW what will happen long-term when we inject kids. Or, at least, most of us don’t. Maybe Fauci does.
OLYMPUS DIGITAL CAMERA
Is it a good idea? Should we bet ALL our kids on that idea?
NO FREAKING WAY.
And THAT is assuming that these vaccines do nothing to affect fertility. If they DO affect fertility, then this has to be made a KNOWN and ADMITTED risk, at the very least – not covered up, like it is right now.
A call for Nuremberg II, more likely, if this was knowingly advanced.
Who wants to risk their kids’ chance of having children?
This brings up the question of whether parents have the right to *knowingly* neuter their kids. Some parents already are, by “transing” kids. I think it’s pretty clear that’s where the Cabal is going – neutering and spaying humans. Interesting question. Should it be sent to SCOFFLAW SCOTUS? How is Amy Comey Barren going to vote on that one?
Asking for a FIEND.
I would even extend that thinking to teens and young adults. There is no reason that I can see to give them the vaccine. But should they have that choice, in consultation with their doctors? Interesting question. Very hard to reconcile a pro-life position with that, isn’t it?
But back to natural immunity.
Natural Immunity – More Rewards
Are there, in fact, more rewards?
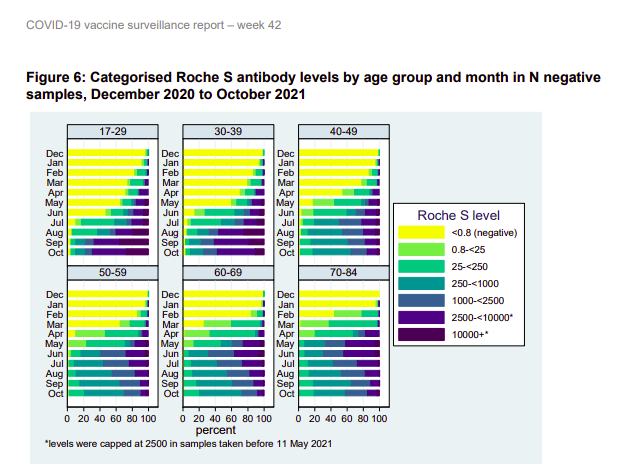
I think so. Look at these two figures from the UK Ministry of Health, showing spike protein antibodies in people in England in 2021.
The darker the color, the stronger the antibodies.
The first graphs are people who have no evidence of having caught the disease (N protein negative). They include the unvaccinated uninfected and the vaccinated uninfected.
The yellow is the unvaccinated people who have not caught the disease – mostly kids.
Green, blue and purple are various levels of vaccination success – the darker, the more spike antibodies.
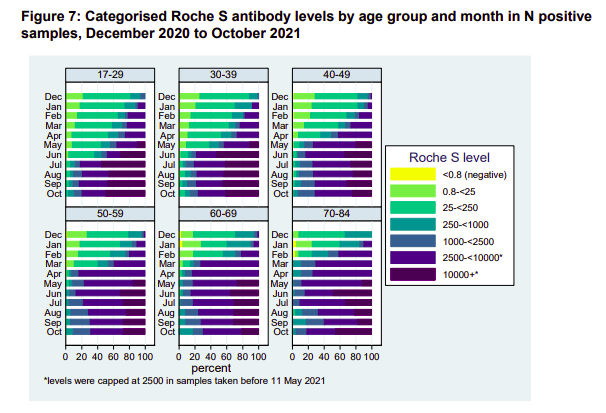
Now look at people who got some or all of their spike immunity by natural infection with the disease.
Assuming it’s a wash as far as the quality of the antibodies – which is not necessarily true – it’s obvious that these recoverees have a more robust spike antibody immunity – to say nothing of likely immunity to some or all of the other 20+ proteins in SARS-CoV-2.
Rand Paul, right here. The man is asking the right questions.
So why is Fauci ignoring this natural immunity stuff?
Notice that KIDS don’t mount a strong spike immunity, even though they beat down the disease in a hurry, with minimal symptoms. This is likely an EVOLVED RESPONSE – an EVOLVED STRATEGY – a form of EVOLVED INTELLIGENCE. What it says is that kids “know” by evolution – don’t build a lasting defense to the ever-changing spike protein. Meanwhile, the virus tries to “rope-a-dope” us slowly into concentrating on the spike as we age, misleading us with each attack. We lean on the crutch of spike antibodies that don’t work on the next strain, or actually make things worse.
Kinda funny that Fauci and the “follow the science” types don’t respect this signal from evolution, but whatever. That’s the basis of another post. But keep it in mind – it’s likely important.
So let us not digress.
The bottom line is that IF you’re going to make spike antibody immunity your standard of success, which Fauci and company clearly have, as part of Fauci’s “antibody hypnosis”, then by that standard, “natural immunity” from the disease gives MORE REWARD.
And again, I remind you, there are MANY other metrics of immunological success which are highly relevant, and which are ignored under Fauci spike antibody hypnosis. Always keep that in mind.
Natural Immunity – More Risks
SO – is the disease “more risk” to get that more reward?
My answer would be “maybe”.
It’s a complex calculation – particularly if you factor in “not getting the disease until you get it”. When you vaccinate, it’s a down payment in full, and with boosters, you’re even stuck with installments. You are “accepting that the risks happen” at 100%. Vaccination “collapses the probabilities”. But if you take your chances on the disease, by simply not vaccinating, you are delaying the (probably) higher risk, but the “risk over time” is substantially reduced.
Imagine the “payoff” of not vaccinating or getting the disease until Omicron. That would have been a GREAT gamble and winnings.
But let’s look at an ACTUAL COMPARATIVE RISK of vaccine vs. disease.
Now – let me be clear from the start – this article is a CLICK-BAIT CHERRY-PICKING of the highest order. The title numbers SEEM shocking – until you dig into it, and go to the source.
But still, they’re not “lying”. It’s just misguided. But that CHAFF led me to WHEAT.
Let me include the entire, short report, as it appeared in GWP.
On December 14th, 2021, Nature Medicine released a study based on a broad population data set analyzed by researchers at Oxford University. The researchers examined the risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination and infection.
The Oxford researchers reveal that 1 in 100 or 1% of all vaccinated individuals were admitted to the hospital or died with arrhythmia or irregular heartbeat.
Of the 38,615,491 vaccinated individuals included in our study, 385,508 (1.0%) were admitted to hospital with or died from cardiac arrhythmia at any time in the study period (either before or after vaccination); 86,754 (0.2%) of these occurred in the 1-28 days after any dose of vaccine. Of those who were admitted or died 39,897 (10.3%) had a SARS-CoV-2 positive test, with 29,694 (7.7%) having a positive test before vaccination. There were 7,795 deaths with cardiac arrhythmia recorded as the cause of death (1,108 had a SARS-CoV-2 positive test).
So 1 in 100 of the vaccinated individuals are going to the hospital with irregular heart beat and this isn’t international headlines?
This study appeared in the journal NATURE. That is the big leagues. We have to take this seriously. But let’s look at it closely. It REALLY helps to see that entire document, although SUSPICIOUS CAT should come out, just looking at the TITLE.
Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection
See? This isn’t just about the vaccines – it looks at infection, too. Is Gateway Pundit giving us the full story? Maybe not.
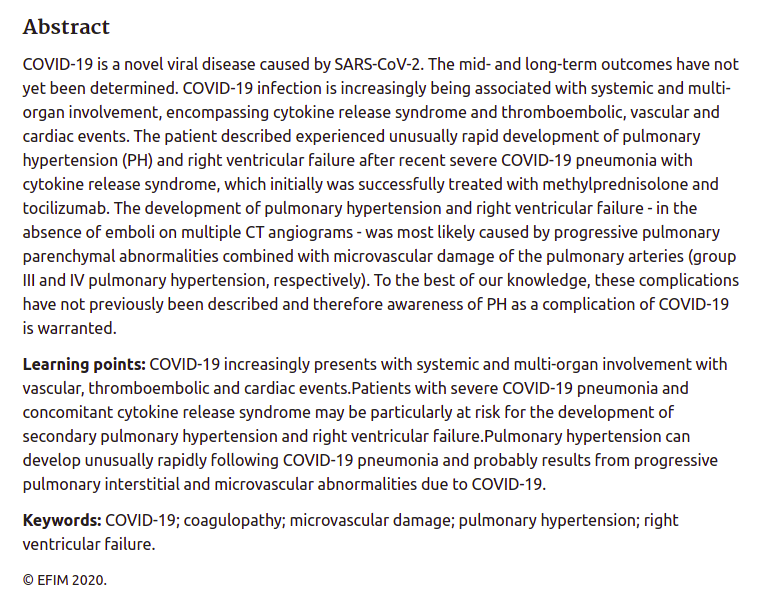
ABSTRACT:
Although myocarditis and pericarditis were not observed as adverse events in coronavirus disease 2019 (COVID-19) vaccine trials, there have been numerous reports of suspected cases following vaccination in the general population. We undertook a self-controlled case series study of people aged 16 or older vaccinated for COVID-19 in England between 1 December 2020 and 24 August 2021 to investigate hospital admission or death from myocarditis, pericarditis and cardiac arrhythmias in the 1–28 days following adenovirus (ChAdOx1, n = 20,615,911) or messenger RNA-based (BNT162b2, n = 16,993,389; mRNA-1273, n = 1,006,191) vaccines or a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positive test (n = 3,028,867). We found increased risks of myocarditis associated with the first dose of ChAdOx1 and BNT162b2 vaccines and the first and second doses of the mRNA-1273 vaccine over the 1–28 days postvaccination period, and after a SARS-CoV-2 positive test. We estimated an extra two (95% confidence interval (CI) 0, 3), one (95% CI 0, 2) and six (95% CI 2, 8) myocarditis events per 1 million people vaccinated with ChAdOx1, BNT162b2 and mRNA-1273, respectively, in the 28 days following a first dose and an extra ten (95% CI 7, 11) myocarditis events per 1 million vaccinated in the 28 days after a second dose of mRNA-1273. This compares with an extra 40 (95% CI 38, 41) myocarditis events per 1 million patients in the 28 days following a SARS-CoV-2 positive test. We also observed increased risks of pericarditis and cardiac arrhythmias following a positive SARS-CoV-2 test. Similar associations were not observed with any of the COVID-19 vaccines, apart from an increased risk of arrhythmia following a second dose of mRNA-1273. Subgroup analyses by age showed the increased risk of myocarditis associated with the two mRNA vaccines was present only in those younger than 40.
The TRUTH is right in there.
First, we have to remember that GWP was concentrating on 1% of vaccinated people during the study period, INCLUDING before they got vaccinated, going to the hospital for or dying from a cardiac arrhythmia. That “before they got vaccinated” point is a TIP, right there, that we really need to consider the risk for UNVACCINATED people, too – including these very same people – for comparison. And as an aside, what is the number for corresponding unvaccinated people? You can almost guess that for most old people, it’s gonna be – well – maybe 1%?
And indeed, when the researchers compared the risk of an “event” against the risks of these patients BEFORE vaccination, they got their answers.
The WORST CASE for the vaccines was myocarditis. So let’s look at that, first.
Here is the risk from the vaccines. Broken out with [notations] so it’s easy to understand.
We found increased risks of myocarditis …
associated with the first dose of ChAdOx1 [AstraZeneca] and BNT162b2 [Pfizer] vaccines
and the first and second doses of the mRNA-1273 [Moderna] vaccine
over the 1–28 days postvaccination period,
and after a SARS-CoV-2 positive test. [STRONGLY NOTE THIS!!!]
We estimated an extra two (95% confidence interval (CI) 0, 3),
one (95% CI 0, 2)
and six (95% CI 2, 8)
myocarditis events per 1 million people vaccinated with ChAdOx1, BNT162b2 and mRNA-1273, respectively,
in the 28 days following a first dose
and an extra ten (95% CI 7, 11) myocarditis events per 1 million
vaccinated in the 28 days after a second dose of mRNA-1273.
SO – this confirms what we know. The vaccines cause myocarditis. It’s a RISK. It’s a handful or two in a million, per injection.
But now, let’s look at the NEXT LINE.
This compares with an extra 40 (95% CI 38, 41)
myocarditis events per 1 million patients
in the 28 days following a SARS-CoV-2 positive test.
What this says TO ME is that the risk of this one heart problem, in a vaccine that gives less immunity, is a significant fraction of the same risk from the disease.
Obviously due to the SPIKE PROTEIN, and possibly with a simple correlation to exposure.
I will admit that it’s LESS RISK from the vaccines, but not all that much.
Look at MODERNA.
The compiled risk of myocarditis from the TWO SHOTS (6+10 = 16) is 40% of the disease risk (40).
And yet HERE is how the authors have to word things to get it past the referees and editors.
“In summary, this population-based study quantifies for the first time the risk of several rare cardiac adverse events associated with three COVID-19 vaccines as well as SARS-CoV-2 infection. Vaccination for SARS-CoV-2 in adults was associated with a small increase in the risk of myocarditis within a week of receiving the first dose of both adenovirus and mRNA vaccines, and after the second dose of both mRNA vaccines. By contrast, SARS-CoV-2 infection was associated with a substantial increase in the risk of hospitalization or death from myocarditis, pericarditis and cardiac arrhythmia.“
They played a lot of word games there – take it from a retired scientist. They are also STUDIOUSLY AVOIDING some big stories that would rub the industry wrong.
“Give the editors what they want.”
Now, before I examine that conclusion for further trickery on the “within a week” qualifier and several other points (not today), I just want to say that calling 16 “small” and 40 “substantial” is bullshit.
Author bias, implicit or imposed, as a virtue signal to Bill Gates’ “vaccine culture” in science.
I will bet MONEY that a third Moderna booster would come in at 14 or more, bringing the total myocarditis events from chronic spike protein exposure to 30 or more, AND at the 4th injection SURPASSING the risk of ONE untreated disease incidence.
Well, is it worth it?
I don’t want Dementia Joe telling ME that it’s worth it. I want to make that determination MYSELF.
And GUESS WHAT? I will also bet money that part of the reason that CDC wanted people to mix and match boosters was to get Moderna “recoverees” boosted with the less cardiotoxic Pfizer or J+J vaccines, while not admitting that…
….defects from each spike protein vaccine are cumulative.
See how that works? Science. It’s great when you’re HONEST.
And why IS Pfizer causing fewer cardiac problems? In my opinion, it is very likely because the vaccine is distributing more widely and slowly in the body, thanks to the extreme vaccine lipid nanoparticle longevity (hence shedding) and biodistribution – data that was hidden from us, but turned up in the Japanese freedom of information request.
To me, the fact that nobody sees or talks about this stuff, is just more evidence of “vaccine hypnosis” of academia, as noted by Peter McCullough.
The reality? PICK YOUR POISON. Disease or vaccine.
If we go back to the arrhythmia example, it turns out that the “shocking 1%” actually GOES AWAY when compared to the unvaccinated. This makes sense, when you recall the very common problem of “palpitation” sending people to the ER, long before “long COVID” was a thing.
Yeah, 1% is shocking, but it’s shocking for the unvaccinated, too. Gateway Pundit was just throwing unwarranted shade.
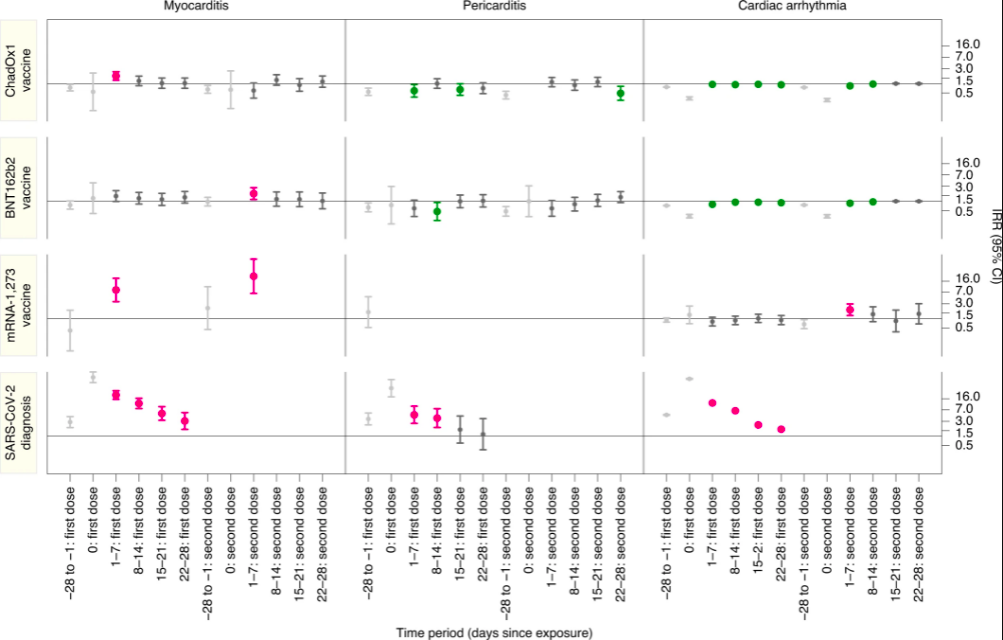
Now, let’s take a look at some GRAPHICS from the study. Pictures tell a thousand words – not all bad for the vaccines – not all bad for “natural immunity”.
On the left axis you have the three vaccines, AstraZeneca, Pfizer, and Moderna, followed by the disease.
On the bottom axis, time – repeated three times for the three diseases.
As you can see for cardiac arrhythmia (right side), the vaccines are basically fine, but the disease is problematic. This makes LOTS of sense, because the disease seems to cause many problems by nerve infiltration, secondary to vascular distribution, and those nervous system infections and inflammations are highly relevant for arrhythmias, whereas the vaccine is primarily a vascular villain, which does NOT reproduce and infiltrate.
The science makes sense here! Wonderful!
All of the vaccines have at least a little bit of myocarditis effect (left side), which is explained nicely by vascular distribution of the spike protein. Moderna, which is notorious for “disease-like symptoms” at the recipient experience level, is easily expected to have even more COVID-like spike protein effects that are not immediately obvious, such as myocarditis.
Big point – ONLY the disease (bottom side) kicks off all three diseases. THAT is what a virus can do, that a bare protein, or even a non-reproducing virus-like particle, cannot.
Everything is making sense here. Let’s look at ANOTHER view of the data.
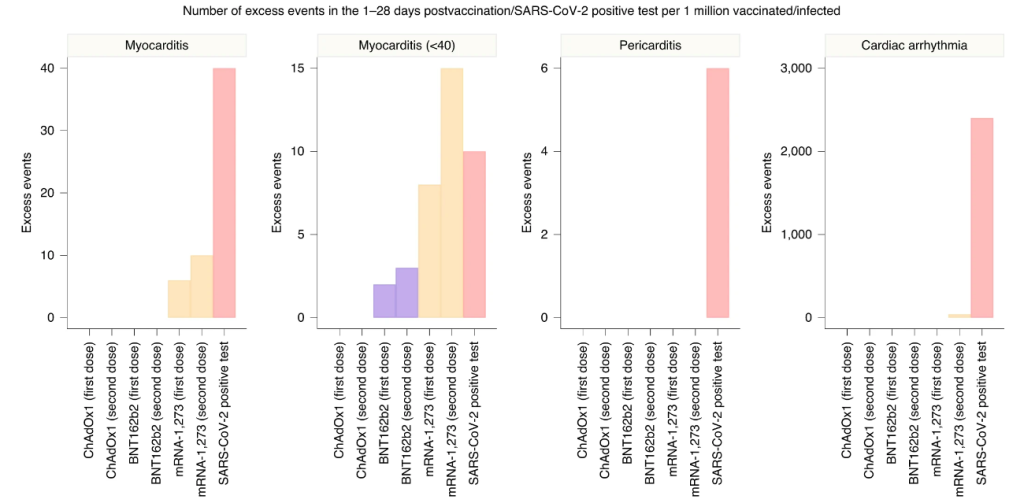
This graph has some GREAT STUFF. The myocarditis comparison described in detail above, is the graph on the LEFT. The numbers for the vaccines look substantially less, but you can see how Moderna boosters would quickly approximate the disease, and are already like a “mild case” in terms of risks. The authors of the paper avoid talking about the cumulative risks, but it’s clear that “boosterama” is PRECISELY Fauci’s game plan, and it has problems that got solved for Moderna by mix-and-match boosters.
Fauci and Walensky. Always taking care of their companies. Yeah, I kinda get it. But you gotta be HARD-ASS with them, like Director Wolf Moon would be.
The whole vaccine thing – including a lot of other adverse effects I’ve mentioned previously but not discussed here – looks to me like a trade-off. These are NOT good vaccines. They’re actually pretty marginal. BUT for people who really don’t think they can take the disease, it could be a reasonable gamble, IMO.
There are LOTS of people who take these vaccines, and no problem. I know – I talk to them all the time. I’m the most vaccine-supportive vaccine skeptic on Earth. These people just dump everything to me, because they know I don’t judge them, but respect their decisions. I’m interested in what happened to them, and they tell me.
NADA. ZIP. The most common reaction. For those people, the shot may make sense. But there are a good number of others who get laid up hard for a day in bed, and it sounds almost as bad as COVID. I worry about them. Some – A LOT.
Now look at the second graph – myocarditis in younger people. Clearly Moderna is WAY out of whack, and the others are comparable to the disease when boosted. Again – for these people – really BAD vaccines. This is why you saw action on the vaccines. Get values up close to the disease, in terms of numerical risks, and the problem becomes an elevator pitch that everybody understands.
Pericarditis and arrhythmia? Purely a disease problem. This looks very good for the vaccine. This is what you WANT with a vaccine – to AVOID some problem of the disease. BUT – can we trust those numbers?
I think so, and I think that Gateway Pundit got burned by looking at COMMENTS on a blog post explaining the Nature study.
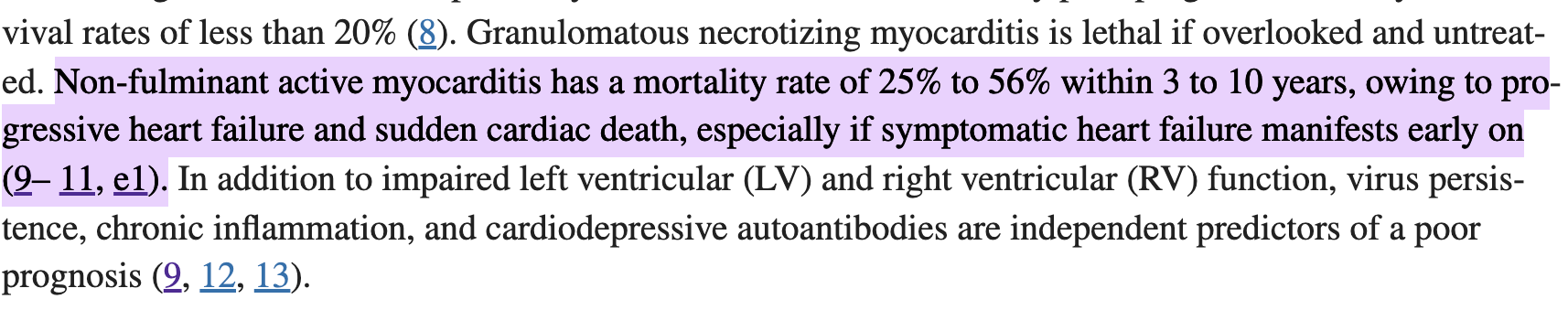
Public health policy in the USA and UK need to change fast. As a side note, if you listen to the mainstream media enough they’ll have you believing myocarditis is a mild symptom. Let me be clear, by definition, symptoms requiring hospitalization are defined as severe. What’s more, the average mortality rate of non-fulminant myocarditis is nearly 56% which is experienced within 3-10 years. Sadly, that is a consequence of the likely heart failure that develops after the acute phase of myocarditis has resolved. See picture below 👇🏻
All things considered, it is clear that individuals under 40 are at a high risk of experiencing vaccine induced myocarditis. The good news is, there are ways to deal with this. More specifically, increasing the time between the first and second dose, not giving boosters to all healthy individuals under 40, pausing Moderna for many under 30, and seeking the guidance of other countries. All of that makes for better public health policy and positive health outcomes. To finish, I will leave you with the words of a wise man, “Health care is vital to all of us some of the time, but public health is vital to all of us all of the time”. – C. Everett Koop
Wolf again.
Now – in the comments, somebody mentioned the “1% issue”, and I suspect this is where GWP picked it up. Sadly, the comment author deleted and restated their comment, probably after realizing it had spawned a widely read article.
Here is the replacement comment, with replies.
zuFpM5*M6 hr ago I erased my previous comment. The closer I look at this study, the more it freaks me out.
They compare vaxxed to vaxxed+covid and then declare covid is worse, but they measure rates of myocarditis/pericarditis in post covid with troponin levels and in post vaxx with hospitalization rates. Hmmmm
They don’t include any control group of unvaxxed. The vaxx+covid group should be compared to unvaxx+covid to determine the actual rate of post covid heart issues. This is not done that I can tell?
The vaccinated showed a 1% hospitalization rate for cardiac arrhythmia with ~385,000 in the period up to 28 days post vaccination. I tried to look up population rates of hospitalization and found some old news articles discussing ~350,000-500,000 hospitalizations annually for ‘atrial fibrillation’ for the entire US population. So a group of vaccinated in UK blew out the entire US annual budget of arrhythmia hospitalizations in a couple month period? And that isn’t a highlighted part of the research results but instead they compare only within the vaccinated group broken out by short temporal periods? Isn’t the most important thing the vaccinated versus background normal rate?
I begin to think this whole study was gamed to get vaccinated rates of these issues versus supposed covid rates so they could continue to say vaccines are safer, when the actual #s are showing a horrific rise in these issues. It is a preemptive narrative shaping attempt.
I am not a doctor, researcher or number cruncher, so if I am misunderstanding this, I would be interested to hear how.
br143 hr ago There’s no way to sugar coat the study.
Of the ~385,000 people with arrhythmia, 10.3% had a positive Covid-19 test, and 7.7% tested positive at some point prior to vaccination.
Even if you remove 18% of the total, that’s still an awful lot of people with arrhythmia. I suppose most of us have some form of arrhythmia at some time in our lives, but how many of us are treated in hospital?
zuFpM5*M3 hr ago Yes. I would not subtract them either. I feel that there would be a covid risk increase + vaccine risk increase + covid/vaccine interaction risk increase to account for. None of which can be done without estimating the covid risk increase by comparing with non-vaccinated covid patients.
This is where they lost me. They’re just tossing out “maybes”. Nothing jumps out at me as likely to change the result. I can even add my own experience with cardiovascular issues from the disease. They’re REAL. Very unlikely that the vaccines and disease would FLIP on the relative risks of arrhythmia.
Score 1 for the vaccines.
BACK TO THE TRUMP ISSUE.
Benefits of the Vaccine Admitted by Our Side
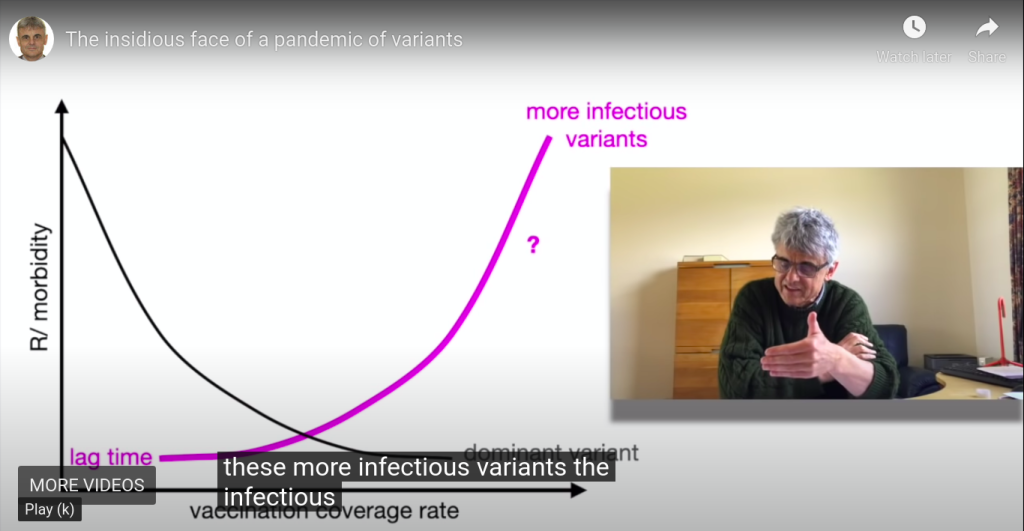
There is a GREAT video by Geert Vanden Bossche that I keep pushing, because it is one of the clearest explanations of why “leaky mass vaccination” is a bad idea. Note that this is from a pro-vaxxer who has indeed worked with vaccines for his whole career, and is a former member of GAVI.
He just demands good vaccines, and good public vaccination policy.
Now – if you jump to around 4:30 in the video, you can hear him list the positives of the clot shot. HOWEVER, it may be better to just invest some of your time in that 4 1/2 minutes where he warms up to that point, to understand that he’s putting the positives AND the negatives in context, and looking at the bigger picture to recommend that we NOT mass-vaccinate.
He is saying that we should NOT mass-vaccinate IN SPITE OF the benefits that he lists and explains.
a decrease of disease in many countries
decline of morbidity and mortality rates
less illness in people who got vaccinated
severe disease is resisted even when vaccinees are infected with variants
they will shed much less virus than the unvaccinated, even when infected with variants
seropositivity rates are increasing in the population thanks to vaccination
But THAT is where he begins to disagree with mass vaccination. He states that we will NOT reach herd immunity, due to variants, and he explains this fully.
Global Problems of Sub-Optimal Mass Vaccination
At 28:00 minutes, Geert explains what we need to do – which is NOT what public officials are doing.
The current mass vaccination program will make things worse, in the long term. Geert explains then the kinds of vaccines we really need – vaccines which can both generate sterilizing immunity, AND which prime the immune systems of their recipients toward cellular immunity.
Yeah, it’s a bit of a tough goal, but it’s realistic toward the challenges of the China virus, and honest about what we need to do.
So what does this mean about the benefits of the vaccine?
THEY ARE REAL, BUT THEY ARE SHORT-SIGHTED. And they are accompanied by risks. Not just to the vaccinees, but to ALL OF US ON THIS PLANET.
According to Geert, continued vaccination is going to HARM vaccinees, relative to the unvaccinated, who will need to avoid virus-shedding vaccinees. At that point, recoverees may be in the best position of all, but still – not great. ALL of us will be in trouble from the virus which will escape the vaccines.
Geert also explains how we can prove that he is correct – by looking at the mutations in the virus which is shed from vaccinees, which will show selection for more infectious variants, if he is correct.
Now – this is a GREAT interview of Geert by Dana Loesch, who looks more and more like Sandra Bullock for some reason, but what the heck – the shotgun shells on her microphone setup are EXCELLENT, very non-Bullock, and she gets a FANTASTIC explanation of the problem from Geert.
Geert actually talks about Omicron, and the DANGER of it potentially evolving to be MORE SEVERE.
Take a listen!
Does Trump know this stuff? I don’t know.
I personally believe that Geert is right. I am now of the opinion that most of what we are hearing from Robert Malone, Peter McCullough, and Geert Vanden Bossche is true, but that each one has to give a little toward the ultimate truth.
What does that look like to me?
Natural immunity is NOT permanent or complete toward other variants
Natural immunity is better than the vaccines, generally speaking, but not bulletproof
Untreated COVID is a loser relative to the vaccines, but treated COVID is a winner
McCullough’s natural immunity prediction based on SARS1 may be too confident
Malone’s whistleblower on more shedding by vaccinees may have been wrong or disinformation
Geert’s vax-brag of less shedding by vaccinees may have been too kind and not skeptical enough
We have to stop pushing the vaccines, for the good of humanity
We have to allow the vaccines to continue, at an acceptably lower rate, for research
We have to allow vaccines to change faster, to keep up with mutations, IF and only IF this will not PUSH the virus to mutate and select faster (immune pressure must be low enough)
We have to pursue the superior vaccines that Geert is specifying
We have to use infection, treatment, and recovery as a big gun to reach herd immunity
We have to let COVID burn out of epidemic status, to reach a treatable endemic status
We cannot do that with mass vaccination, so mandates must cease promptly and completely
Joe Biden and CDC must be stopped – by military power if need be – if they will not end the crazy mandates
Yeah, you heard me. We can’t let this demented bozo, backed by an evil Obama and China, make COVID worse by mass vaccination. Mandates are making things worse.
Freedom, Vaccines and Morality
Trump may not understand Geert Vanden Bossche’s warning, but if we set that aside as an unknown, you can understand where Trump is coming from.
If we want freedom, we have to let other people make stupid choices that affect them most of all. Vaccination is, in fact, one of those things. Indeed, it is by US seeing it that way, that I believe we will end this nightmare of division which PUMPS UP the vaxxies and the crazy mandates.
In the same way that there are vaxxies who now are defending OUR freedom to be unvaccinated, I believe we have to defend the right of people to stupidly (or smartly) take the vaccine. However, we MUST get the rate of vaccination DOWN below the level where immune pressure from the vaccine creates more and more infectious variants.
The FIRST thing is not to take the vaccine yourself, or give it to your children.
The SECOND thing is to fight for an end to mandates.
The THIRD thing is to fight for BETTER vaccines, and to expand belief that the current vaccines are NOT GOOD ENOUGH, and are of the WRONG TYPE. Make the vaxxies demand better, not defend bad vaxxes.
The FOURTH thing is to spread the message that the “socially responsible thing to do” is to support Vanden Bossche’s position, that NOT taking the vaccine NOW is what will ultimately “save grandma”.
The last one is a hard sell, with FAKE NEWS pumping vaccine stupidity, but hey – we’ve fought tougher battles already.
So what about Trump?
Well, he is not in the position to know or respond to the “Geert Vanden Bossche Question”. Not yet. It is only when that issue becomes BURNING HOT, that Trump will be able to smartly push FORWARD from the current stupid CLOT SHOTS.
We will have to RAISE VACCINE CONSCIOUSNESS to levels of understanding that SUBVERT FAKE NEWS. We can only do that by getting most of the vaxxies on our side – to demand BETTER vaccines.
If they want to be guinea pigs – GREAT. They can be heroes, and try the deadly experimental vaccines. But we should NOT be forcing all of humanity to be part of a BAD and MISGUIDED experiment.
And the JOKERS who are allegedly running our military need to understand this. Virtue signals which kill troops, even if slowly and quietly, where nobody can see them, are NOT ACTUALLY VIRTUOUS. I appreciate them kicking out the sane ones who understand that the current bad clot shots may cripple readiness at some point, rather than forcibly injecting them. We WILL have a reserve of trained people who are not destroyed by China and Biden, no matter what China’s coming chess moves. Thank you for that. But as for everything else – there could have been push-back against communism, instead of acquiescence.
Yes, we had to be shown. But I’m not sure showing us subservience to a COUP and CHINA and FAKE NEWS isn’t undoing half of the good stuff.
But this as well. If you guys delivered Omicron on purpose, thanks. It LOOKS like it may be working.
Merry Christmas!
W
Remember way back in July when I was banned by Twitter for saying that mandates were coming, vaccines weren’t working as promised and they’re gonna demand we all take boosters?
After a lost week of human self-experimentation to survive multiply mutated Fauci-Baric China Virus, Wolf has obtained answers to a thousand questions. Here are just a few of those answers.
Over the last week, overcoming my SECOND case of the China virus, I have been able to learn quite a bit about the enemy’s weaponry – AND our own.
I was READY this time. PREPARATION paid off, and big-league.
I tried to help others prepare, and ended up helping myself, too.
OK, people. It is time for THE WOLF to GET PATTON ON YOUR ASSES. As you may know, we now have many of our dear members actively fighting COVID-19, including one (gil00) in the hospital. Several have received Regeneron. Thus far, praise God, we have not lost anybody – and I intend to keep it …
I felt it was important to share what I have learned, and to answer people’s questions, but I wanted to have enough strength to actually do a post – not just a few quick answers lost in the middle of conversations.
I have answered a few questions already – I will try to link to some of those answers. Other answers I may copy here. But most of these questions are being answered here for the first time.
HERE WE GO!
1. Which version of COVID-19 did I have?
singingsoul1(@singingsoul1) Online Wolverine Reply to Wolf Moon December 3, 2021 19:46
Wolf is that [omicron] the strain you and your wife caught? I am wondering since you did not respond as well to Ivermectin?
Where did you catch the first virus covid and where do you think you caught the second virus? You caught two different strains?
What I had this time was almost certainly Delta.
What I had the first time was almost certainly a minor variant of the original Wuhan strain (COVID-19).
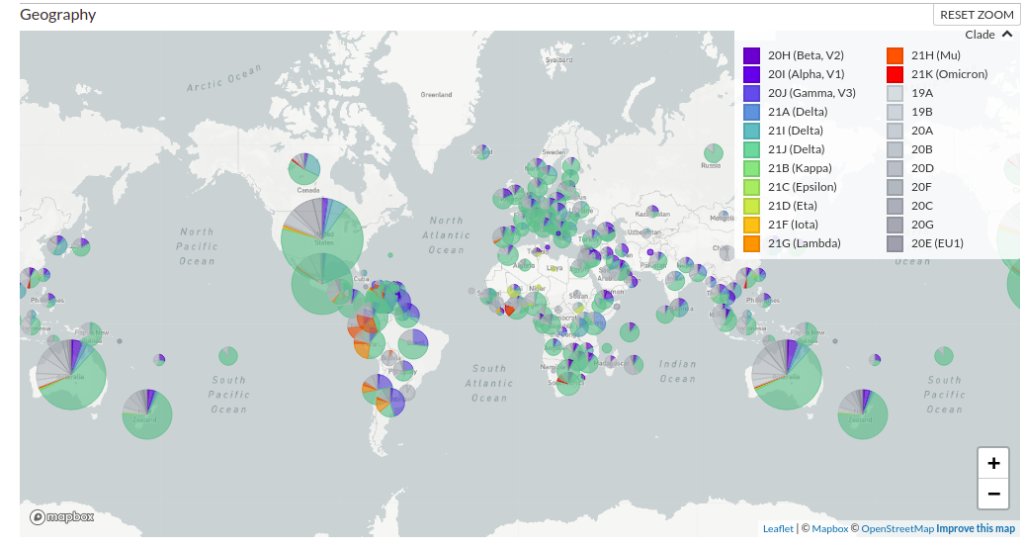
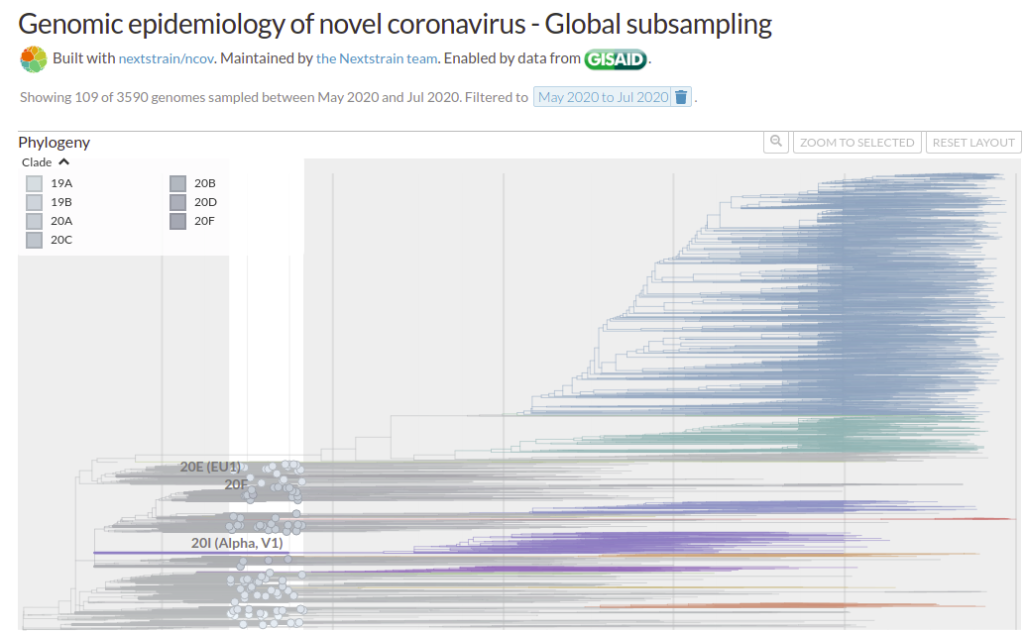
Here is the current worldwide geographic distribution according to NextStrain.
Note that the colors are not fixed – the same data may be shown with different colors from one day to the next.
The turquoise color which covers 2/3 to 3/4 of almost every pie chart across the planet is the Delta variant. You can see that it has rapidly become the predominant version.
The various grayish versions (1/4 to 1/3 of each pie) are basically the original Wuhan strains PLUS the gazillion minor morphs of THAT which formed immediately. You remember the “European strain” and the “Washington strain”, and the “New York”, “Italian”, etc. – those were all still basically Wuhan, and those are the variants that are still effectively treated by all the original vaccines and antibodies.
If things had stayed there, the vaccinated would largely not be having breakthrough cases right now. Similarly, I would not have had a “breakthrough case” on my natural immunity.
The purplish and orange versions are other minor variants of concern, some of which were once much bigger concerns, until delta began to predominate. The vaccines still held up fairly well against those, as did, apparently, my natural immunity.
Omicron (red) is barely on the map right now.
It is EXTREMELY unlikely that I had omicron. It is VERY likely that I had standard issue delta variant.
2. How do I know that I had COVID-19?
Within a 24 hour period, I was positive to three tests – TWO antigen tests (BinaxNOW and QuickVue), plus a PCR test run by my primary care physician’s group.
The same tests showed my wife to be negative on Day Zero and Day One of my infection.
However, LATER, on Day 4 of my case, another run of QuickVue showed my wife to be weakly positive.
In my opinion, and with as much experience as I have now, running them, these antigen tests are highly reliable and trustworthy.
But that’s just the beginning.
My new case was, in so many ways, almost identical to the case that I had in January 2020. That case predated the availability of tests. Also, because it predated antibody test availability, I never got an antibody test until 6 months later – which by then was negative.
But now I’m CERTAIN. I had COVID the first time. Same damn disease. THE SAME.
And it all makes sense. DELTA BREAKTHROUGH IS possible for Wuhan natural immunity, IMO. Maybe not for everybody, but it was for me.
3. Did ivermectin work for me?
I strongly suspect that ivermectin helped me avoid serious problems and recover quickly.
I cannot be sure that ivermectin actually helped, but it certainly didn’t hurt. I would be very tempted to use ivermectin again, if I got COVID again.
My wife also used ivermectin, and it seemed to “flatten the curve” of viral load for her, too.
I would be bullshitting to say that I know ivermectin helped, or that my case “proves that it works.” But I can easily say that I strongly suspect that it helped.
4. Did I have any side effects from ivermectin?
Yes, but the side effects were extremely minor, for as massively high of a dose as I was taking.
I decided to roughly follow the FLCCC “triple-dose” (0.6 mg/kg) recommendation for an active infection, because I had two of the conditions that cause FLCCC to recommend the highest dose – (1) likelihood of delta strain, and (2) multiple comorbidities.
I decided that the same applied to my wife.
To mitigate side effects, I did NOT take the daily amount in a single dose, but rather spread it out in 12-mg pill-pops during the day. But even with the spreading of the doses, and taking them with meals, I felt the following symptoms.
desire to sleep after meals
“lazy eye focus” for a few hours
stomach “not quite right”
None of this was bad enough to quit the drug, or even to reduce the dose, but after 5 days of it, I was absolutely done. I had ZERO desire to take ivermectin any more. I wanted my stomach to return to normal, even if that entailed a greater risk. Given that most of my other symptoms were gone, I didn’t feel like it was much of a risk.
Also, ivermectin has a pretty long half-life, so after 5 days of super-high-dosing it, I’m probably STILL flushing it out of my system.
My wife experienced the same stomach issues. She was ready to give it up after 6 days.
5. What about the Zelenko / Raoult protocols?
Yes. I credit azithromycin every bit as much as ivermectin, and I have more direct evidence that it helped me.
This is where the reasoning gets very complicated.
In early 2020, I was immediately impressed by the work of Didier Raoult (hydroxychloroquine + azithromycin) and later by the clinical real-world proof of Zev Zelenko (added zinc and moved treatment to outpatient prophylaxis). I was absolutely convinced that early azithromycin was key to stopping the killer pulmonary symptoms of the disease, and basically turned it into “just another weak, influenza-like coronavirus”.
Although it turns out that azithromycin has its own powerful antiviral activities, the main thing it did, in my opinion then and now, was to prevent any type of pneumonia from setting in. This is critical if you want to stay out of the hospital.
Thus, as soon as I started detecting what I considered scary lung issues (burning lungs, basically), which was almost immediately (end of day zero, middle of day one), I decided to begin TWO ADDITIONAL PROTOCOLS.
The first was a modified Zelenko protocol. I increased my zinc to my maximum levels ever taken, plus quercetin as natural capers (clearly the bad influence of Aubergine). My wife and I also began using elderberry syrup as an additional zinc ionophore.
However, the real key was adding azithromycin – 2 days at 500 mg, and 2 days at 250 mg. The very first dose resulted in an immediate improvement in my lungs.
There is simply no arguing against the clinical record of success of the Zelenko protocol. I trusted it in my scientific reasoning in 2020, and I trusted it to treat myself.
I get far more mileage out of real-world clinical studies like Raoult’s and Zelenko’s, than out of Fauci’s little “double-blind” – whoops – I mean “double-chump” scam studies that can be manipulated against both doctor and patient by lying, phony, deceptive, agenda-filled, biased, compromised, fake-neutral parties.
The whole idea of double-blind studies falls apart when the researchers and patients are innocent DUPES and CHUMPS, and the people who are supposed to be honest referees in charge of neutrality are in fact dishonest manipulators like NIH, CDC, CEPI, Gates, WHO, and all the rest.
In contrast, studies like Zelenko’s and Raoult’s are pretty much open source. No Fauci-type con-man is in charge of fake neutrality. This being a neutrality I have little care for anyway, because I don’t care what exactly saved the people – simply that they were saved.
Yeah – I’m biased in favor of MEDICINE ITSELF.
The protocol works, end of story.
Fauci’s “studied ignorance” of clinical success is exactly why the man should have been fired DECADES AGO. He’s not a doctor – not a patient-treating one – and he should not be in charge of doctors.
HOWEVER – I do have to admit – azithromycin was even harder on my gut than ivermectin. Four days was all I could take. My stomach was always double-queasy if I took AZM with my IVM. There was NO WAY I was going to do a fifth day.
But YES – the stuff worked, and IMO kept my lungs “infection-free”, knock on wood.
Thank you, Doctors Raoult and Zelenko!!!
6. What about antihistamines?
Absolutely. The same well-proven clinical success that Zelenko had with azithromycin, was also evident in the results from the Spanish nursing homes. It would have been negligent not to take an antihistamine, in my opinion.
That, plus some additional reasoning I will explain below.
Based on the recommendations of people here, I chose Claritin (loratadine), and quickly found that I tolerated it easily at the recommended double doses.
I experienced a very, very slight dryness of the mouth, but that’s it. Just to be careful, I tended to keep the dosing closer to 1.5 instead of double, but in the absence of all the other drugs I was taking, I would have been more rigorous about the double dose, without consequence.
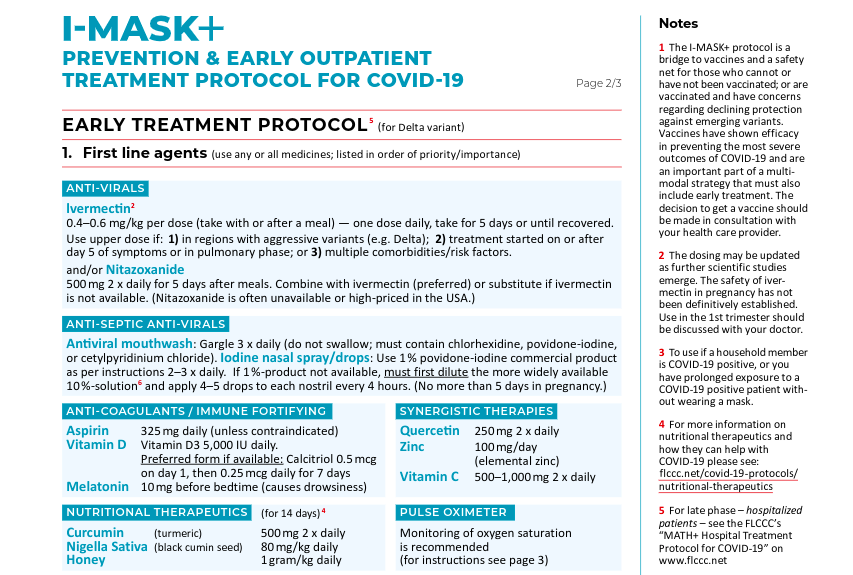
For those who need a refresher on the use of antihistamines against COVID…..
Everybody underestimates Spain. The last letter in “PIGS” is far less of an insult than an error. Years ago, when I was at a conference, and Japanese industrial spies were getting me drunk (it was a great red wine), I decided that I had to give them SOMETHING for their time and effort, if only …
Now – here is some important new reasoning I had.
In the FLCCC protocols, and the Zelenko protocols, there is very little if any “over-the-counter” patient control in terms of things which could possibly pre-address and prevent the “cytokine storm” problem – particularly any drug that is available on an outpatient, OTC basis.
In the FLCCC protocols, aspirin is the main anti-clotting drug with something approaching that function. In the original Raoult and Zelenko protocols, HCQ’s antirheumatic functions combined with azithromycin’s actions seemed to suppress pulmonary capillary clotting, although neither did so as well as steroids.
The fact is, however, that the Spanish nursing home study had extremely good success preventing cytokine storms by simply using antihistamines on ALL patients, both as treatment and as prophylaxis. The entire emphasis of the approach was not so much to prevent disease, as to simply limit the disease.
To me it was a no-brainer to add an antihistamine to prevent inflammatory clotting – something that I knew already I was susceptible to, because of my first case of COVID, after which I lost lung function.
Loratadine turned out to be a VERY high-bang-for-buck fix for me, because it also dried nasal and sinus secretions, helped my breathing, reduced lung congestion, and generally decreased symptoms.
Thus, I found that adding an antihistamine had both clearly observable short-term benefits, and very likely long-term benefits.
I highly recommend adding this protocol during COVID treatment. It’s completely OTC as well – the Medical Mafia in Washington simply can’t stop it.
Multiple studies have showed that aspirin, even at low doses, is both protective against getting COVID-19 and also protective against hospitalization and death. The numbers are substantial, too.
This is, again, part of the FLCCC protocol, and pretty much a no-brainer.
I started off using half a regular aspirin, but quickly found that it was just one more drug beating on my stomach.
Switching to low-dose aspirin worked nicely to make any stomach symptoms go away. I also found that I did not need more than 1 or 2 low-dose baby aspirins to control fever. I was able to routinely drop my fever back to near-normal with either 81 mg or 162 mg of aspirin.
Now, my doctor’s practice recommended acetominophen in case I had a high fever, but I never came close to needing it. As it was, I did not want to risk my liver in ANY WAY with all the other high drug doses, so there was NO WAY I was going to add dangerous acetominophen to the mix.
According to the literature studies, even a single baby aspirin per day was enough to show the protective effect. Thus, I made sure to always take 81-325 mg aspirin per day, and will continue with at least 81 mg/day for some time to be determined.
8. What about HCQ?
Not this time, but I would not rule it out in the future – particularly in the absence of ivermectin.
When I got my ivermectin, I had the opportunity to get hydroxychloroquine and azithromycin as well. I chose the latter, but decided not to bother with HCQ I would likely not use.
I let ivermectin be my “drug of choice” for fighting COVID, for many reasons, including the greater safety profile and better understanding by doctors’ groups, including FLCCC. I am satisfied that I made the right choice in ivermectin, but quite frankly, it would have been a good thing to have some HCQ on hand as well.
Anything that kills viruses, is better than their “stupidity of spike identity” vaccine.
9. Did I gargle?
Yes. I used FLCCC-recommended and study-backed Listerine “with essential oils”, and the benefits were obvious.
Actually, ALL the Listerine variations use the same “essential oils” – pick any of them. Some of the time, I used one that also packs zinc chloride, to really screw with the virus.
At first, I went with warm saturated sodium bicarbonate (baking soda) gargle, which was the gargle used by the Spanish nursing homes.
Warm bicarb is actually a really good solution, in terms of soothing the throat and decreasing viral load (as experienced through reduction of key symptoms), but it doesn’t really do a lot in terms of opening up breathing passages.
In contrast, Listerine gargle was EXCELLENT for helping to clear breathing passages, AND to decrease viral load in the throat and mouth. The beneficial effects even extended to the lungs. I only needed to do it 2 or 3 times a day, and the effects lasted for hours afterwards.
The Listerine gargle was also excellent before sleeping, to have a peaceful night’s rest, with clear breathing.
In my opinion, the gargling protocol is really key to helping end things quickly.
NOW – there is some difference between what I experienced and what FLCCC recommends. FLCCC only recommends (at the moment) Listerine for prevention – they DROP IT for early treatment, and recommend ONLY the other types of antiseptics (cetylpyridinium, povidone-iodine, chlorhexidine) once you get the disease. Yet, honestly, I was totally satisfied with the performance of Listerine for TREATMENT, and would not hesitate to use it again.
This may be an individual thing. As they say, your mileage may vary.
10. What about povidone-iodine gargle?
I didn’t use it this time, but I may very well try it next time!
I was not aware that you can just buy this stuff OTC, but yeah – it’s a product. In the studies I read, povidone-iodine was THE BEST in lowering viral load in patients. It did better than Listerine – not by a whole lot, but enough that it might be worth it.
So if you can’t stand Listerine of any kind, or Scope, or whatever – consider trying this one.
11. Did I get the monoclonal antibodies?
Yes. In “better late than never” fashion, I got the mAb infusion after the treatment with ivermectin and azithromycin was already finished, and my fever was gone.
I was fever-free when I got the antibodies, and fever free when I left the infusion center. Shortly after that, I became exhausted and had a fever again. In another 24 hours, my strength was back and the fever was gone yet again.
Basically, I was treating Delta with more Wuhan antibodies like my own, which had already only provided some protection.
I cannot really be sure if the antibodies helped. I personally found that they knocked me out, increased my fever, and made me suffer a “day of exhaustion” that I had otherwise MISSED thanks to ivermectin.
Were they beneficial? Possibly, but I can’t be certain.
My wife got the antibodies somewhat earlier in the progress of the disease, because she got them at the same time I did, but her case was tracking mine LATE by roughly four days.
The antibodies didn’t completely finish her case, but she really only had one more day of disease after the “antibody down day”.
I would say that antibody infusion was far more likely to have helped HER than it was to have helped ME.
If I had to choose between antibodies, aspirin, loratadine, azithromycin, and ivermectin, I’m not actually sure which one I would toss. I consider EACH of them, just one more tool to make sure the disease stays contained. Use as many as you can get.
12. So what happened to my “natural immunity”?
Try some “AND” logic.
It’s still there – waiting patiently for a disease that no longer exists.
This blurry snapshot from NextStrain is from a “play mode” view of the data, where you can watch the genetic data being added in accelerated time. I have focused the active band on early 2020. The “19” and “20” strains are pre-delta – they were well within the window of my natural immunity, which was probably generated by a strain within what they are now calling 19A.
Follow the evolution forward in time, and you can see the massive shift to delta versions, shown in turquoise and indigo below.
SO – what I have now is DOUBLE natural immunity to TWO HUGE CHUNKS of older/existing COVID-19/20/21/22, the now-rare “gray” stuff and the very common “blue-green” stuff.
You can see, though, where OMICRON in RED is now forming. Whether I have any, some, or no immunity to omicron is an open question. HOWEVER, I would much rather have combined natural immunity to TWO groups of COVID variants, than three, four, or even five vaccines.
We have to start being very scientific about immunity, including in particular natural immunity, which is IMO the BEST response to highly mutating diseases, just as it has ALWAYS been.
Fauci is gaslighting us. Ignore him.
Until the poisonous dwarf is removed from power, do your own science.
https://youtu.be/p_yOSM7ujM0
Start HERE:
This link in particular, to keep checking up on SARS-CoV-2 – an EVOLVING GROUP OF VIRUSES.
A Beautiful Demonstration of Real Science in Action, and How Political Correctness Prevents Obvious Correlations and Causations From Being Seen by Monetarily Dependent Scientists
Being “Sherlock Holmes” is easy, when everybody else in mainstream science has turned into a character from “The Muppets” or “Sesame Street”.
Except for Dr. Charles Hoffe, plus a bunch of other physicians and scientists who our media calls “The Dirty Dozen”, that “Count” guy is my only real competition now.
Of course, when he counts 57 genders, he will leave our little group of truth-tellers, but until then he can probably count protons and neutrons reliably.
Thankfully, I’m retired. I can speak the truth. “The Count” is still employed by the dirty establishment.
Consider a basic idea of vaccination known from literally centuries of science – from even BEFORE the first vaccination in the 1790s, when people used WEAKENED smallpox to gain immunity to NORMAL smallpox (a process called “inoculation” or “variolation”).
Here is that bedrock idea. A principle so simple, it borders on “an obvious trend in a collection of observations”.
“Immunity conferred by catching a disease naturally and recovering is strong, and any form of preventing the disease by inoculation (including variolation and vaccination) attempts to live up to that level of immunity. Some vaccines will give life-long immunity, if that is possible, or for as long as the disease itself gives immunity, if lucky, but in many if not most cases, the durability of immunity conferred by a vaccine is LESS than the durability of immunity conferred by the disease itself.”
So I repeat – this simple idea is something that “everybody knew” from roughly 1790 to 2019, and even before 1790, when vaccination wasn’t even called vaccination.
But then – suddenly – in 2020, the media talked us out of centuries of knowledge about how immunity works, by a kind of hand-waving authority – allegedly from “the experts” at CDC and NIH.
Fauci and Scarf Lady went along with the media hoax. They didn’t have to say a lot. It was mostly by leaving OPEN the question of natural immunity, when it should NOT have been left open, that damage to science and society was done.
Of course, after enough results poured in from laboratories around the world, noting how much stronger natural immunity to COVID-19 appeared to be, we were relieved to discover that – Yes, Virginia – immunity is still behaving just like it did before COVID-19.
(The feds will certainly have to do some “funding mechanics” to fix all those people reporting “incorrect science”, won’t they?)
And THAT is when Rand Paul began taking Anthony Fauci to the woodshed over natural immunity.
So why the heck did we ever suspect or believe otherwise?
No good reason, except the Fake News.
Think about it.
If this does not prove to you that the media controls science, and not the other way around, then wait for the next example.
I’m going to replay parts of a conversation some of us has on October 1 of this year.
It’s in images, but I will also provide a link and the text.
I now know two people personally who get the injection. One was my BIL who got covid anyway, but we made sure he got treated the right way and he got better immediately, and is back at full health despite diabetes.
The other is a friend who cannot breath well even with an oxygen tank turned to max. He has seen every type of doctor, and no one can figure out what the problem is.
He and I had a sharp but friendly argument over the injections a month or so ago. He is MAGA but a true “vax” believer (hard to imagine, but they exist).
I have spoken to him a couple times at length, but refrained from bringing up the injection as a possible cause of his present distress. His wife thinks he is not going to make it, but, again, I have not mentioned to her the injection as a consideration.
The doctors will not tell him, and at this point what difference could it make, other than making him feel more stress or more unhappiness?
I feel like this all the time. No one in my circles will listen. It’s pointless, and would end up splintering relationships that will be needed as these people all go down sick.
I actually feel this way about ALL vaccines to an extent, and I still think that my younger nephew is actually vaccine injured. No one will listen to me on that, either, given there is another diagnosis that fits. They didn’t listen to me about the one drug he was on, and I turned out to be right. I was the first one to call that the drug was the problem, and eventually it could not be ignored.
This is no different. All the research won’t change minds when all the people in family want to be able to do is travel, and that was the driver for the decision.
You are a real life Cassandra. The fact that you endure this psychological burden because you know at some point in the future those people will need you is admirable. You are demonstrating the true character of a disciple of the Lord. Your faith is obviously sustaining you.
He got the shots in March. I will ask him what type. The breathing problem was gradual and started about a month ago and has become severe.
We spoke again yesterday, and I suggested D3 and Zinc. Oddly enough, his own doctor told him to take those, and he has not taken them. Now he says he will.
He is going in for angiograms on Tuesday and used that as a polite excuse to defer on any further discussion.
But I would love to hear your perspective when I get you the info.
Great! Both D3 and zinc are necessary to fight off respiratory viruses, and they tend to be deficient as we get older. If he does have spike protein lung damage, every minor respiratory virus brings back the COVID lung problems.
Also magnesium helps me. It is a vasodilator and antihypertensive, and I suspect that it is a PULMONARY vasodilator, too.
I know that fear. Inability to breathe properly is extremely scary. And it scared a lot of people onto vents where they died.
One of the foulest tricks of both COVID and MASKS is that they mess up O2 / CO2 balance. One has to ADAPT to the new balance. THAT is hard. One reason I refuse to wear a mask is that it really messes with my oxygen balance. It messes me up for HOURS. And I’m IMMUNE, damn it! Pointless and CRUEL to make me wear a mask – these Stalinist bastards!
I am still trying to find out what “vax” he took. He is not doing well. He had two angiograms and the doctors are still uncertain what his problem is, and he has been fretful (so I am told).
It is a delicate situation.
But please keep this post in mind so when I find out we can discuss.
One way you might get him the proper help is to suggest that he may have HAD COVID AND DIDN’T KNOW IT. Both he and the Covidian doctors will believe that, before they will believe that the jab WAS the “Covid” that he got.
That will get the docs thinking that he has long-haul, and they may send him on to a “long-haul” specialist.
So far, that is the only sensible way. Truth is the best generally, but at the right time, otherwise it can be a bad choice if the truth creates more negativity.
Gail’s story of her long-term oxygen problem being cleared up by moxidectin (relative of ivermectin) may be useful, because it can be mentioned simply as fact – and it’s kind of funny because it was an accidental exposure (while dipping sheep in a skin-penetrating formulation).
I spoke to my friend. He took Moderna. When I asked he pre-emptively said “what I have has nothing to do with the voccine.”
He said the docs told him he had severe pulmonary hypertension, and there was nothing they could do except give him the generic form of Viagra.
The MDs might very well be telling him exactly the way it is, and who am I to say differently? Still, his case at least proves to me how deep my distrust is.
TY for engaging on this personal interest! As always, I highly respect your knowledge and judgment.
Wolf again…..
Now – if you follow through that conversation, you will see that Tona’s friend started off with vaccination, followed later by persistent shortness of breath. You can see that I suspected he might need magnesium as a pulmonary vasodilator – that his case might be similar to mine, which was from COVID itself, only his seems to be much WORSE.
Later, you see that he’s getting an angiogram – meaning, they’re going to look at his blood vessels. This is heading exactly where I thought it was going.
Finally, you see that it is verified that Tona’s friend took the Moderna vaccine, and has pulmonary hypertension.
This confirmed everything that I suspected.
Now – WHY did I suspect that this man had pulmonary hypertension?
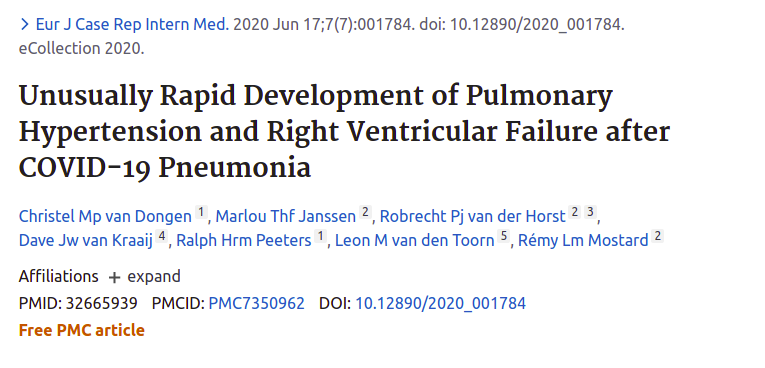
FIRST, because I have LONG been following the story of endothelial damage in the capillaries of the lungs by SARS-CoV-2 – more specifically by the spike protein – and resultant pulmonary symptomology (including shortness of breath), from all the way back in March and April of 2020, when Dr. Cameron Kyle-Sidell realized that the ARDS vent strategy “imported from China” was ALL WRONG. He started looking at high-altitude sickness as a better (though still flawed) model of the disease, and quickly understood the endothelial and pulmonary capillary thrombotic nature of SARS-COV-2 infections.
As you can see, by the middle of 2020, the DISEASE was already well understood in terms of being a provoker of coagulopathy and the sequelae of that.
It was this coagulopathy, that was causing shortness of breath.
And THAT leads to the SECOND reason I suspected pulmonary hypertension. Something I had seen HERE, actually, in various postings on our site. Thank you to all posters here, who brought this information.
But THIS information was not about the disease. This was about the VACCINE.
Please listen to the video below – it will not only explain what is happening – it will assure you of this good doctor’s credibility.
Canadian doctor warns the worst is ‘yet to come’ from blood clotting damage linked to COVID-19 shots
There is also a LARGER video which includes the above video – but it ALSO includes additional information – priceless information – about how Chinese crypto-kinetic warfare is used as part of “reality shaping” to support Chinese sociobiological warfare. See if you can arrive independently at the same understanding, and explain it to me in the comments. You will need to listen to the longer video to see it.
Everything Dr. Hoffe says is – sadly – bad news for “yours truly”, but it MASSIVELY confirms my “hunch” that COVID took at least a DECADE off my life.
This is just a gut-level assessment of the damage to my health, but everything that I’ve seen in my medical test data seems to confirm it. My respiratory, pulmonary, cardiac, vascular, and immune functions are all noticeably impaired after COVID. I do not know if I have pulmonary hypertension, but I suspect that if I do NOT have it, it is only because I have very successfully prevented systemic hypertension. My blood pressure is low, and I have kept it low, thanks to magnesium.
This is part of the reason I have been so adamantly opposed to vaccinating our troops, and regard that action as TREASONOUS. The only people who are helped by medical turnover of our military are the communists – both foreign and domestic.
But let’s not talk about me. Let’s not talk about the US Military.
Let’s talk about Tonawanda’s friend.
The fact that he had the Moderna vaccine is – in my opinion – very important.
Why?
This gets into the observed and known differences between the vaccines, which I have watched VERY CAREFULLY from the very beginning. I very CLOSELY watched the Phase One trials for both Pfizer and Moderna.
The Moderna vaccine was NOTORIOUS for causing symptoms VERY similar to the disease, including fever, exhaustion, headaches, muscular and kidney aches. Worse than that, the Moderna systemic effects were extremely common in the trial group.
If I had to describe my “non-taker” impression of the Moderna shot like a “gourmet” might, it would be like the Shingrix shingles vaccine first shot, only more systemic like the second shot.
The symptoms Ben describes are VERY MUCH like COVID-19 itself.
The Pfizer vaccine – surprisingly – did not have strong observable and immediate effects like Moderna. The incidence of anything more than a bit of local swelling was almost non-existent in the Phase One trial group.
The Pfizer vaccine moved up near the top of my “I might take this one” list.
Thus, it was very surprising that LATER, lots of problems with the Pfizer “clot shot” came into view, as the vaccine was being delivered to people. To some extent, I believe that the NUMBERS of many side effects simply don’t appear in trials, but THAT is not the whole story. I am now convinced that Pfizer is led by incredibly dishonest people, and that they very likely gamed the trials to hide problems.
And very ironically, there is some SCIENCE to back that up. The GAMING begins with the vaccine itself.
What’s interesting there, is that Pfizer’s data on biological distribution of their vaccine in test animals – which we had to get from the Japanese government – not only explained the nature and biodistribution of side effects seen in vaccine recipients – it explained the SHEDDING of VACCINE to others in close contact with the recipient.
This was, IMO, phenomenal detective work by the people who got that data. The Pfizer vaccine’s array of issues was due to the PERSISTENCE and SLOW RELEASE of the vaccine – as well as the obvious LIPID MOBILITY of the LIPID NANOPARTICLES. It took DAYS for the vaccine to release most of the mRNA into cells. The vaccine had plenty of time to move around in bodily lipids. It even had time to be EXCRETED in bodily lipids.
But NOW, I can ALSO use this same explanation for the difference between Pfizer and Moderna in the trials.
Pfizer basically created what is essentially a slow-release vaccine without telling people it was slow-release. VERY beneficial in trials – no?
Moderna’s vaccine also uses lipid nanoparticles, BUT their vaccine clearly deploys FASTER into cells. There is significant overlap, nonetheless, in cardiovascular deployment, as Dr. Hoffe notes. Moderna is likewise distributing throughout the body, and producing systemic vascular endothelium-centered effects much like COVID itself does, but Moderna produces symptoms FASTER than Pfizer. The vaccine effects of Moderna are thus much more noticeable – in some ways like the new shingles vaccine, which is a recombinant antigen vaccine, not an mRNA vaccine, and does NOT employ time-delaying lipid encapsulation technology.
Shingrix tends to produce rapid LOCAL symptoms on the first shot, and systemic symptoms on the booster, exactly as we might expect for two fundamentally different immune reactions (naive locally generated to injected antigen on shot 1, and immune secondary cytokine reaction to same on shot 2).
SO – back to Tona’s friend. He got MODERNA. Moderna SHOWS that it produces symptoms similar to COVID. Just ask Ben Stein. We have covered these “whole spike protein” vaccines.
Dr. Hoffe encountered his results using the MODERNA vaccine.
Dr. Hoffe – at the time of the video – had 9 out of roughly 900 Moderna-receiving patients who were significantly (medically) damaged by the vaccine – and that did not count the 62% of ALL patients (estimated from a smaller sample) who showed signs of microscopic clotting.
Of those 9 patients clinically damaged by the vaccine, SIX of them are described as having “reduced effort tolerance” indicative of pulmonary hypertension. That is exactly what I have from COVID itself. I’m just lucky that my prior health was SO GOOD – far better than most others my age, particularly with my set of comorbidities like “former smoker” – that I was simply “knocked back” to somewhat below normal levels of health for my age.
Others may choose not to believe that Tonawanda’s friend was a victim of side effects of the Moderna vaccine, but in my opinion it is IMPOSSIBLE to dismiss this possibility. In fact, I believe that this case is an exemplary fulfillment of Dr. Hoffe’s warning.
In my opinion, mRNA vaccines are a fundamentally flawed approach, relative to a carefully metered and controlled ANTIGEN vaccine. mRNA vaccines have a “sexy” mechanism, but the whole concept is SCIENCE-CENTERED – not PATIENT-CENTERED.
Science-centered vaccines are a perfect fit for BRUTAL Stalinist socialized medicine, which treats people coldly and unsympathetically.
And THAT is why the Faucist conspirators and Bidenazis are deploying it.
What would Obama do, if nobody could stop him?
THIS is Obamacare – the REALITY. Brutal, corrupt, industrialized medicine.
Ironically – so ironically – profit-centered and capitalist to the core – only the negotiation with the corrupt capitalists is run by Soviet-style bureaucrats. An interesting mix of communism and fascism.
Fauci and Pfizer have painted themselves into a bit of a corner.
I now believe that they “played a charade” on boosters – that boosters were their intent all along.
I think this WHOLE scam was very intentional.
But it gets far, far worse. I think I see that they have an agenda much bigger than the COVID scam.
And I think I see what that agenda is.
This is very hard to see, but I think that maybe some other people are going to be able to see it, so I’m throwing this out there in hope that those people MIGHT see this.
Let’s go progressively backwards in time.
The LATEST outrage is the Project Veritas revelation – in the words of Pfizer’s own scientists – which really shows you how utterly AMORAL or even IMMORAL the management of Pfizer really is.
Please watch this if you have not already.
H/T Sundance, Deplorable Patriot, and many others.
The big point that you need to get out of this, is that the management of Pfizer is NOT interested in doing the best thing for people. EVERYTHING that you have seen from them – the hiding of the vaccine migration data – the ripping off of countries – the manipulation of FDA against competitor J+J – it’s all confirmed by what Pfizer’s own scientists say.
And to top that all off, these scientists ADMIT what we all knew, and always knew – that natural disease-conferred immunity is SUPERIOR to vaccine immunity.
Likewise, if anybody around here has been as SHOCKED as I am, about how badly ISRAEL is now treating EVERYBODY – Jews, Arabs, whatever – with their draconian mandates and “Vaczi” passports – well, maybe it’s not so much of a surprise.
What a bunch of play-acting. THE DRAMA – IT BURNS.
The HYPOCRISY is meant to DISTRACT from the MESSAGE OF COMPLIANCE that SELLS PRODUCT.
Do you see how the propaganda works here? They think we’re stupid. No. We’re just as wise as the MAGA husband who comes home and finds the wife ISRAEL in bed with A DRUG REP.
OY VEY.
But it gets worse.
This earlier video, which has also been discussed both here and at CTH, has a VERY important point that takes a while to sink in.
Again, please watch this if you have not already.
Or maybe not.
[ NOTE – YouTube video REMOVED – old URL: https://youtu.be/ZwR7natWqLk ]
The biggest point is the final one, which the good doctor starts setting up at 10:00, and which he really gets down to at about 11:00 – that the COVID vaccines are actually SETTING UP BREAKTHROUGH INFECTIONS.
Yes.
I want you to read that again.
It appears that the jabs are making people MORE susceptible to the evolving virus.
This makes TONS of sense from an evolutionary perspective – which is why I have to laugh at all my liberal non-scientist friends who hate God, SWEAR that they believe in evolution, but would never believe what I’m about to tell you.
As you know from my prior discussion of viral evolution…..
OK – we’re going to have some fun here – but stick with me, and you could learn A LOT. Cue the music! Borrowed from Wheatie! Previous posts helped put both the SPIKE PROTEIN DISEASE and the SPIKE PROTEIN VACCINE into deep perspective. We were seeing that the SOLUTION was a significant part of the …
…..one of the best ways to look at a virus and one or more hosts, is to see how they all negotiate to a state of equilibrium, which then appears (because it IS) evidence of DESIGN. The design is just at a near-mathematical level – like a program that adapts and installs itself – rather than a cruder model that requires ridiculous microscopic interventions at every possible juncture.
Things work out for the benefit of LIFE, because we live in a PRO-LIFE universe. But the question is exactly HOW that works out. It may not be as SIMPLE in some ways as you think it might be – or conversely it may be SIMPLER.
We’re only humans, and we have a lot to learn.
And we could learn a LOT from space-time distributed, parallel-processed intelligence, a.k.a. LIFE.
Just like all our latest vaccine tech is bad mimicry of natural technology invented at least 70 million years ago (read the article – it’s fascinating), so our latest attempts to immunize ourselves are not even that.
These vaccines, which use our “next tech” but not our “best tech”, are corrupted by human GREED and DUPLICITY. Bluntly, Fauci, Pfizer and Moderna SCAMMED President Trump. They had a terrible motivation to push LITERAL “bleeding edge” vaccines, instead of more obvious and safer vaccines. That motivation was not to solve their phony crisis – it was to usher in gene therapies by using the same technology as a kind of false hero in a pandemic, riding on Trump’s coattails.
They needed “real science” to SHUT THE FUCK UP, while their FAKE SCIENCE cured their FAKE PANDEMIC with a FAKE HERO.
Dr. Nathan Thompson, in the video above, discovered that the vaccines are – at least in some fraction of people – LOWERING general immunity – and this appears from all data to be to everything EXCEPT a single VIRAL VARIANT which is about to SHIFT to a NEW VARIANT. And we now know that even THAT limited immunity wanes rather quickly.
But we knew that. We knew that ALL ALONG.
Go back in time, before Fauci LIED and said that everything we knew was wrong.
We KNEW that you don’t make vaccines to colds – and that you barely make them to the flu. We knew that coronaviruses were problematic. We knew that vaccines to them are plagued with failure, in some cases caused by phenomena like ENHANCEMENT, where the vaccines make catching the disease EASIER or WORSE.
We knew what these viruses are like. We knew what they were like DECADES AGO. And yet, the disgusting MEDIA played us into a state of credulity, where even expert scientists with the most basic and well-grounded knowledge from over a century of virology were not allowed to state the obvious, if it contradicted our rotten, lying CDC.
Something is VERY wrong there.
Stop and think about it.
They are pushing a vaccine that reduces immunity to everything EXCEPT the VERY specific thing they vaccinated you for – which disappears. So the net effect is to make things worse in all possible ways.
Reducing overall immunity is exactly what Trump WARNED US ABOUT.
The cure can’t be worse than the disease.
BUT IT IS.
And I am going to argue that they knew this ALL ALONG.
Take a look at these screen shots.
If you have ANY kind of modern primary care physician, then you get these reports at least once a year, from the lab tests that your doctor orders.
RIGHT? Am I right?
You can actually compare THESE EXACT NUMBERS – not the CD4 and CD8 cells, which are specialized, and you probably don’t get tested for, unless you have AIDS or another immunosuppressive disease – but everything else will show up on YOUR lab results. Sometimes they say “Granulocytes” and sometimes they say “Neutrophils”, etc., but you can look at the “normal” ranges and match things up very nicely.
You can compare YOUR immune results with the ones in the video. But that’s not my point.
YOU KNOW PFIZER WAS DOING – OR COULD EASILY HAVE DONE – BASIC LABS ON THEIR TEST SUBJECTS.
They had to do the basics – right? Maybe not the people in the trials that everybody was watching – maybe they “overlooked the basic tests” very “accidentally” or by some rule – but somewhere, somehow – there is no way that Pfizer didn’t run the most BASIC immune function tests – THAT WE ALL GET – on at least some test subjects – and discover exactly what we are discovering now.
They had to know what was happening, and what this meant.
$$$$$$$$$$$$$$$$$
If you have a virus, largely created by your friend in NIH, named Fauci, and his friends Baric and Daszak, and their friend Shi in China, and you have a vaccine for it that ONLY CREATES VERY SPECIFIC ANTIBODIES that your friend Fauci focuses on like a hypnotist, but otherwise the vaccines lower immunity and cause disease in general, and this virus changes itself quickly enough that boosters are continuously needed, or maybe only to the point where the vaccine harms immunity enough that the virus doesn’t HAVE to change……
Are you seeing what is happening here?
THE GENERAL LOWERING OF IMMUNITY IS KEY.
This is what counteracts ANY “good” that Fauci focuses on.
These vaccines are the ultimate damned heroin.
COVID vaccines are not heroic. They’re HEROIN.
Let me explain this again, in comparison to NATURAL IMMUNITY.
Natural immunity is the result of EVOLUTION – so it’s SMART. It knows from adaptive experience that a RIFLE SHOT at what just hit you will do no good – but a BLAST from a SHOTGUN will hit the bug the NEXT TIME IT COMES BACK DIFFERENT.
That is why the broad-based but complex immunity conferred by the DISEASE is BETTER than “just a few antibodies specific to yesterday’s villain.”
Nature KNOWS BETTER (by now) than to try to hit the shape-shifter where it was last standing.
Fauci doesn’t know better.
OR DOES HE?
I think he DOES know better.
And I think that Rand Paul, who is VERY SMART, is scaring Fauci because Fauci knows Rand is onto him.
I am no longer thinking these people are stupid.
I think they are very smart.
I think they are RINGERS.
I think they’re up to something.
Making money to continue their program is part of it, but not ALL of it.
They have a goal – the goal is NOT for our benefit.
I believe that these things are components of their agenda.
lower human immunity to disease AND to genetic modification
implement gene therapy as a gateway to genetic modification of humans
increase government’s power to complete medical control of humans
change humanity in a Fabian way – create some socialist human ideal
And THAT takes me back to something Cthulhu said, which has stuck with me.
Fauci was up to something VERY similar with AIDS. He wanted a vaccine desperately. He didn’t want to treat AIDS, but eventually he HAD TO – and when he finally did, it was remdesivir all over again.
And what I’ve come to realize, is that IF there had been a “working” vaccine for HIV / AIDS that worked anything like these terrible coronavirus vaccines, that vaccine would have LOWERED HUMAN IMMUNITY in the same dubious strategy – as the “prevention” for a disease that lowers immunity.
Do you see how WRONG and WEIRD that is?
You know – something is just “not right” with all this.
I’m not taking this vaccine. And I sure as hell hope YOU aren’t taking it either.