Our mission, as God-fearing and God-loving patriots, is to defend this Constitutional Republic and to increase its greatness, in all good things and ways, by using our voices in free but courteous speech, by discussing the happenings of the world and coming to a profound understanding of those things, and by sharing and promulgating these Truths on both this platform and others.
The above is a vintage image of mass vaccination. (Courtesy Google Images.)
This series on the disaster of the COVID-19 virus itself, and of the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023.
The origination of today’s post begins here: www.dossier.today/p/double-digits-biden-admin-tells-americans, “Double Digits: Biden Admin tells Americans that it’s soon time for their 10th Covid shot“, by Jordan Schachtel, 13 June 2024. (Mr. Schachtel wrote about the ninth COVID-19 “vaccine” injection here: www.dossier.today/p/dose-number-nine-cdc-panel-green, “Dose number NINE: CDC panel green lights yet another Covid mRNA shot“, 29 February 2024. The CDC recommended that persons over age 65 take another “booster shot” of either the Pfizer-BioNTech or of the Moderna “2023-2024 Formula COVID-19 Vaccine” of these manufacturers.) A person age 65 or older, if that person adhered to every CDC recommendation regarding taking a COVID-19 “vaccine” injection since December 2020 (when the FDA granted first Emergency Use Authorization (EUA) to Pfizer-BioNTech and to Moderna for these companies’ “flagship” modRNA COVID-19 “vaccines” (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), would have taken injection number nine starting on 28 February 2024.
Today’s post is long. There is a large amount of information to “unpack.” Stay with me here.
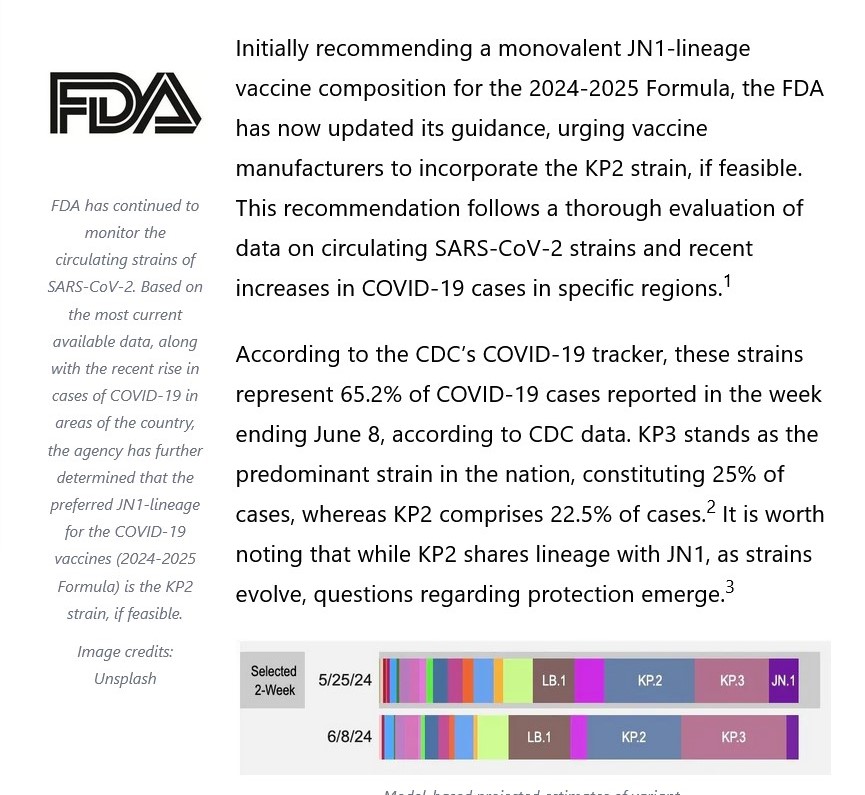
Note the language regarding the “selection of a specific JN.1 lineage SARS-CoV-2 strain…” More about that later.
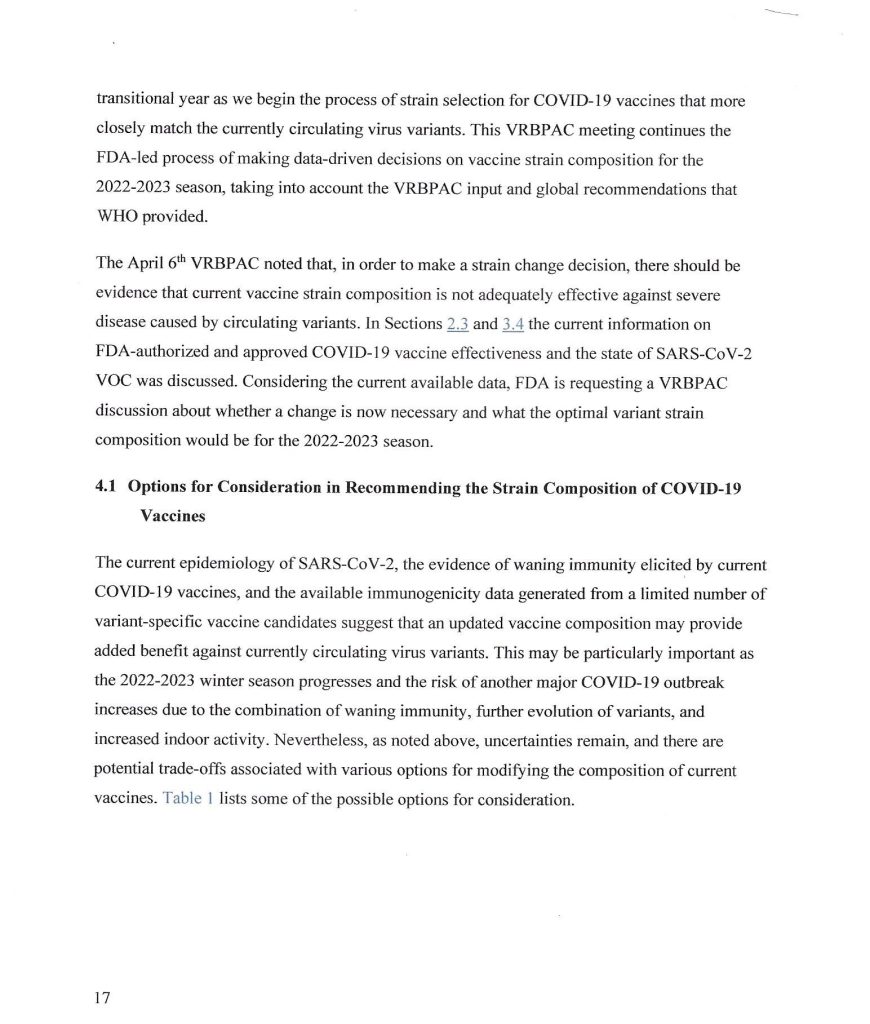
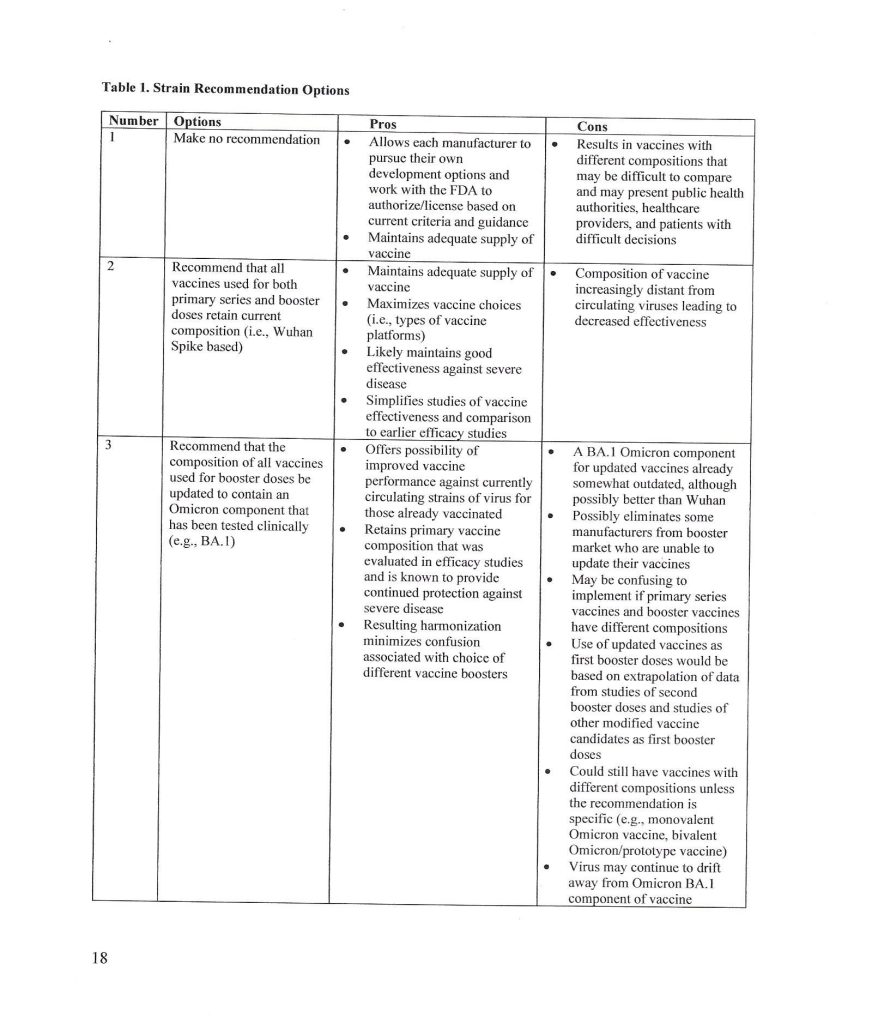
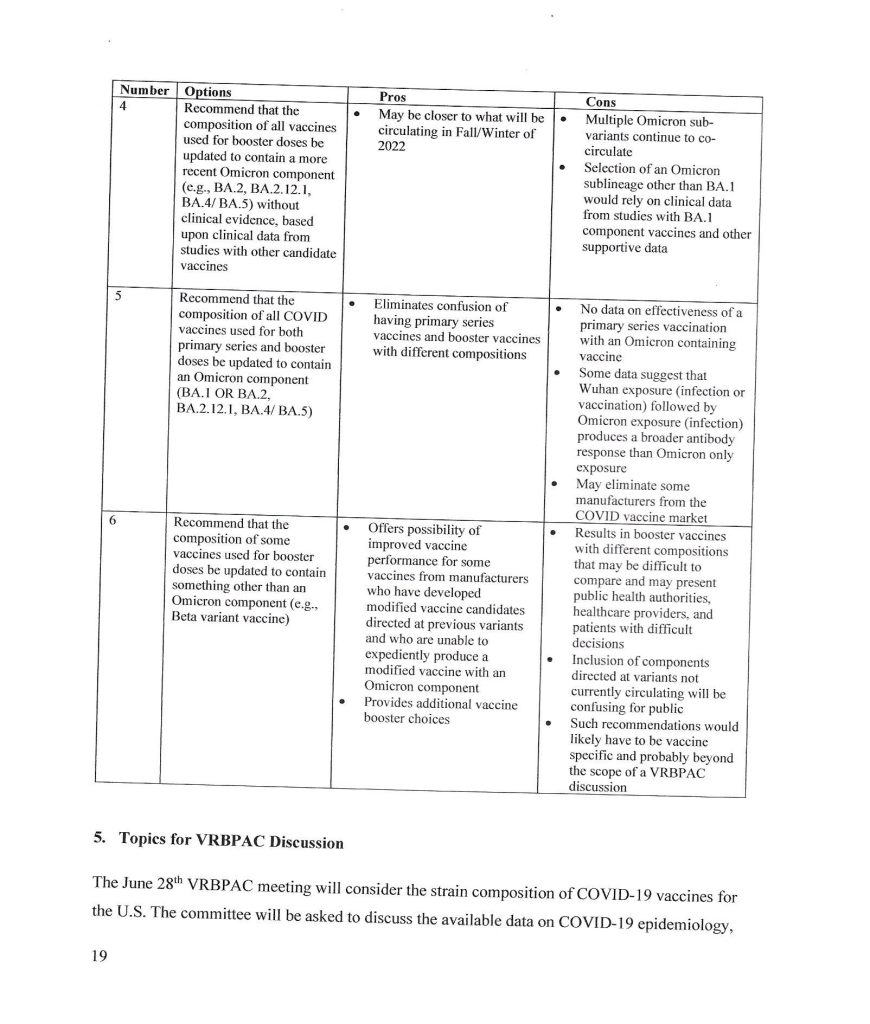
The trail behind the 5 June 2024 FDA announcement begins with the VRBPAC Briefing Document for the meeting held on 28 June 2022: www.fda.gov/media/159452/download, “FDA Briefing Document Vaccines and Related Biological Products Advisory Committee Meeting June 28, 2022.” It was at this meeting that the FDA “codified” the types of “strain composition recommendations” that the agency would use regarding “new versions” of COVID-19 “vaccines.” Yours Truly presents page 17, page 18, and page 19 of this document:
It appears that the FDA simply decided that it would be permissible for the agency to authorize a new COVID-19 “vaccine” strain composition along what, in Yours Truly’s opinion, may be called “very flexible” options. For example, the Pfizer-BioNTech XBB.1.5 COVID-19 “vaccine”, which was FDA authorized in the fall of 2023, had test results only from mouse testing prior to FDA authorization. Following are: The link to the Pfizer-BioNTech slide presentation about this “vaccine” to the CDC’s ACIP committee (Advisory Committee on Immunization Practices) meeting of 12 September 2023; and, an image of slide CC4 from this presentation. First, the presentation: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-09-12/10-COVID-Modjarrad-508.pdf.
Second, slide CC-4 from the above presentation:
The XBB.1.5. Pfizer-BioNTech COVID-19 “vaccine” had only been given as a single injection to humans in the company’s clinical trial; a clinical trial which had only just begun prior to the ACIP meeting. Slide CC-5 of the presentation, the start of the company’s human trial of this “vaccine”, is below:
Slide CC-6 of the presentation has to do with the mouse studies of this “vaccine”, which were of longer duration.
Notwithstanding the above, the FDA authorized the use of the company’s XBB.1.5 COVID-19 “vaccine” on 11 September 2023 (in Yours Truly’s opinion, it appears that the ACIP meeting of 12 September 2023 was a “catch-up” formality.) It also appears (again, in Yours Truly’s opinion), that the FDA used a very loose interpretation of “Option 4” on page 18 of the FDA Briefing Document above in granting the EUA for this “vaccine”.
** Now, on to the latest “new version” of the COVID-19 “vaccines”, the “2024-2025 Formula COVID-19 Vaccines”, that the FDA authorized in June 2024.
The following linked items are important regarding background information related to this situation and to the FDA: First, the FDA document, stating that the agency would “align” its COVID-19 “vaccine” antigen composition to the recommendations of the World Health Organization’s TAG-CO-VAC recommendations: www.fda.gov/media/179139/download (the TAG-CO-VAC recommendation for the “2024-2025 Formula COVID-19 Vaccines” was to use the JN.1 strain); second, the FDA document regarding “considerations and recommendations” for the “2024-2025 Formula COVID-19 Vaccine” composition: www.fda.gov/media/179145/download; third, the FDA announcement of the 5 June meeting of its VRBPAC committee (Vaccines and Related Biological Products Advisory Committee.): www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-june-5-2024-meeting-announcement. From this last link, chick on “Event Materials” to see the slide presentations and other items that were discussed at this meeting.
Two important items from the “Event Materials” list: the FDA Briefing Document; and the VRBPAC roster for this meeting. First, the FDA Briefing Document: www.fda.gov/media/179003/download; and, second, the VRBPAC roster for this meeting: www.fda.gov/media/179225/download. The roster for the 5 June 2024 meeting has some “familiar” members and speakers: Paul Offit, MD; and Peter Marks, MD (director of CBER [Center for Biologics Evaluation the Research of the FDA]); and, among the “Temporary Voting Members”, are: Bruce Gellin, M.D., M. PH., the Chief of Global Public Health Strategy for the Rockefeller Foundation; and, Melinda Wharton, M.D., M. PH., Associate Director of Vaccine Policy of the CDC. (Italics mine)
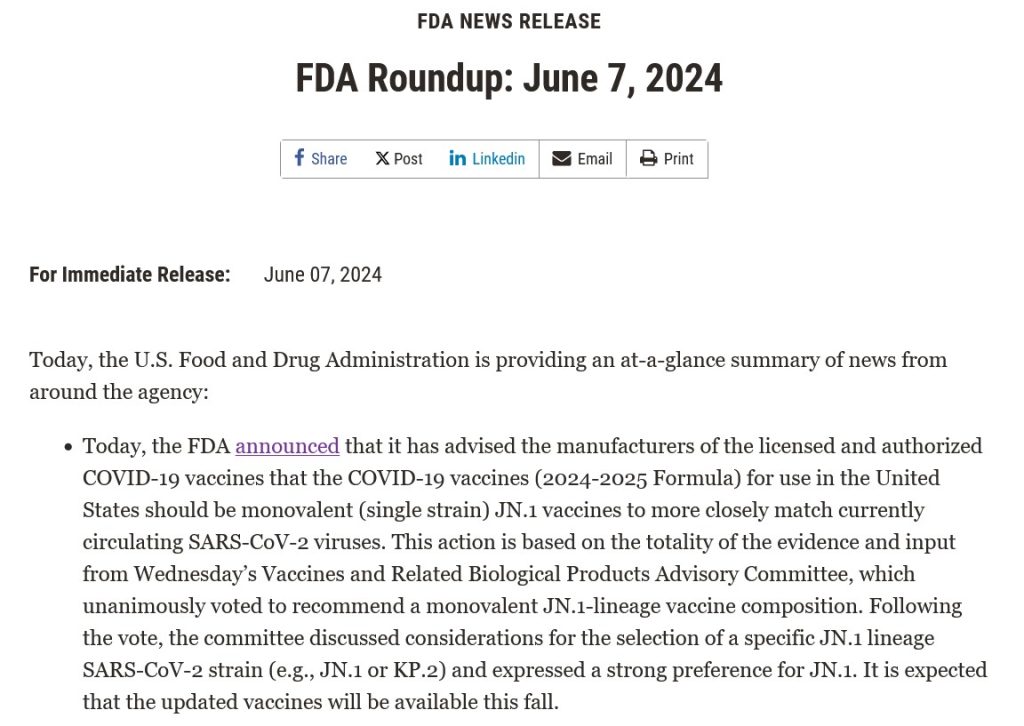
The VRBPAC members voted unanimously to endorse the Pfizer-BioNTech, the Moderna, and the Novavax “2024-2025 Formula COVID-19 Vaccine” by these companies, based on the presentations of these companies’ representatives at the meeting. Yours Truly can find noregistered human clinical trials performed in advance of the 5 June VRBPAC meeting by Pfizer-BioNTech, or by Moderna, or by Novavax, for any “2024-2025 Formula COVID-19 Vaccine”; that would indicate that any “clinical trials” were performed in these companies’ facilities on mice; and that any “human trials” were also performed in these companies’ facilities, prior to the meeting. The FDA then issued the agency’s original announcement of 7 June 2024: www.fda.gov/news-events/press-announcements/fda-roundup-june-7-2024; and, a screenshot from this announcement:
Note in particular “…the selection of a specific JN.1 lineage SARS-CoV-2 strain (e.g., JN.1. or KP.2) and expressed a strong preference for JN.1.” Here’s where it starts to “get interesting.”
What was it that happened? Part of the answer lies in the fact that the NIH and Moderna co-own the patents (and, therefore, share the royalties) for the Moderna “flagship” modRNA COVID-19 “vaccine”, mRNA-1273. This agreement would extend to “descendant clone COVID-19 vaccines” by Moderna. www.citizen.org/article/modernas-mrna-1273-vaccine-patent-landscape/. The NIH’s Dale and Betty Bumpers Vaccine Research Center (part of NIAID — which Dr. Anthony Fauci led from November 1984 until his retirement in December 2022) and Moderna co-developed mRNA-1273. https://covid19.nih.gov/news-and-stories/nih-vaccine-research-center; a screenshot from the article is below:
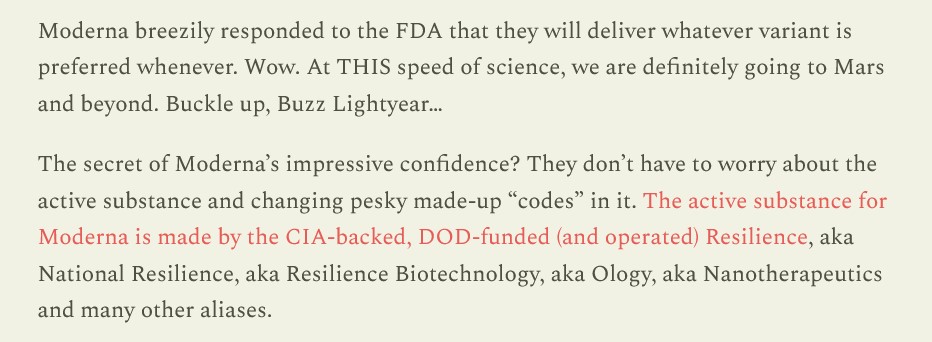
The other part of the answer is that Moderna was already developing a KP.2 strain COVID-19 “vaccine” for 2024-2025. This, and the FDA’s decision to shift away from the JN.1 strain to the KP.2 strain, are described in this post at Sasha Latypova’s blog: https://sashalatypova.substack.com/p/all-roads-lead-to-resilience, “All Roads lead to Resilience. FDA is removing competitors for the Pentagon & CIA’s baby…Moderna”, 23 June 2024.
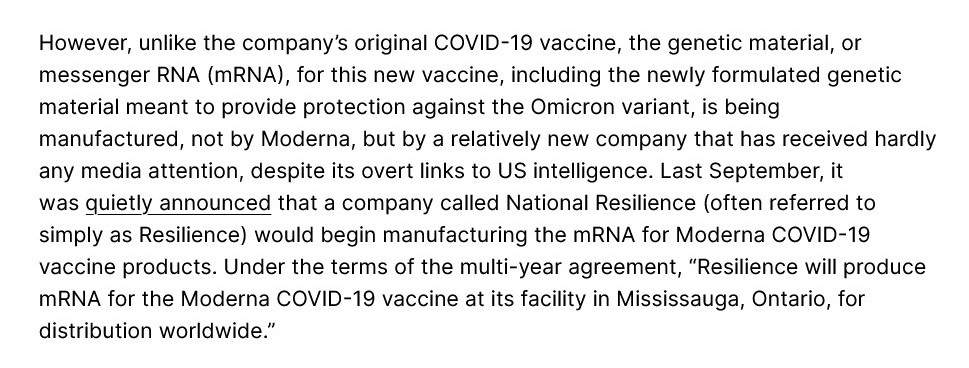
However, there’s yet another detail in play here, regarding the FDA’s switch, “based on evaluation of the most recent circulating strains of COVID-19”, from JN.1 to KP.2 — the CIA and the Pentagon. Here is a screenshot from Sasha Latypova’s Substack article:
But wait, there’s more! Resilience lists multiple “partners”, such as the Mayo Clinic. The company also, apparently, has a “partnership” with the United States Army’s Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense https://resilience.com/learn/partnerships. Below is a screenshot from this website:
It appears, then, in Yours Truly’s opinion, that the FDA was perhaps “reminded” of the”details” regarding the NIH-Moderna co-ownership (and royalties – sharing) agreement related to Moderna’s modRNA COVID-19 “vaccines”; and, the role of the CIA-Pentagon-National Resilience (aka Resilience) in manufacturing the mRNA used in the Moderna COVID-19 Omicron “booster vaccines” — and the KP.2. strain is indeed a “descendant strain” in the Omicron lineage (as is the JN.1 strain.) Hence, the FDA’s 2024-2025 COVID-19 “vaccine” strain “sudden switch” announcement of 13 June 2024, only one week after the agency gave the nod to the JN.1 strain.
In Yours Truly’s opinion, it is statistically, medically, and ethically impossible for a new vaccine (let alone any COVID-19 “vaccine”) to be developed; tested (on lab animals, then on human subjects); the test data thoroughly collated and analyzed for “safety and efficacy” on both lab animals and on human subjects; then, which data is presented to the CDC / FDA for consideration; then, these agencies doing their own “due diligence” research; then, and only then, being granted an EUA by the FDA; then, and only then, manufactured for use in humans — in a time span of fewer than three to five years, let alone within a time span of only a few months. It appears, again in Yours Truly’s opinion, that the CDC and the FDA are playing “fast and loose” with the health and safety of the people who choose (or will be “mandated”) to take the “2024-2025 Formula COVID-19 Vaccine.” And, also, that “other entities” are in play here to perhaps “influence” decision making by these agencies.
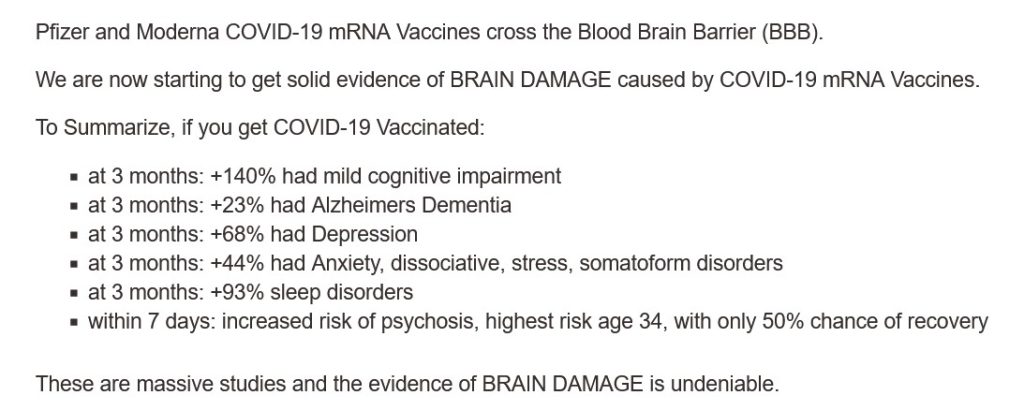
All of above is in addition to the fact that the COVID-19 “vaccines” (actually, gene therapy injections) have caused, are causing, and will cause, multiple health issues, serious adverse reactions, and deaths, in those who are “vaccinated.” Just two of the most recent discoveries: One, the COVID-19 “vaccines” can cause brain damage, an article by Dr. William Makis: www.globalresearch.ca/brain-damage-covid-19-mrna-vaccines/5861012, “Brain Damage Caused by COVID-19 mRNA Vaccines”, 26 June 2024. Below is a screenshot from Dr. Makis’ article:
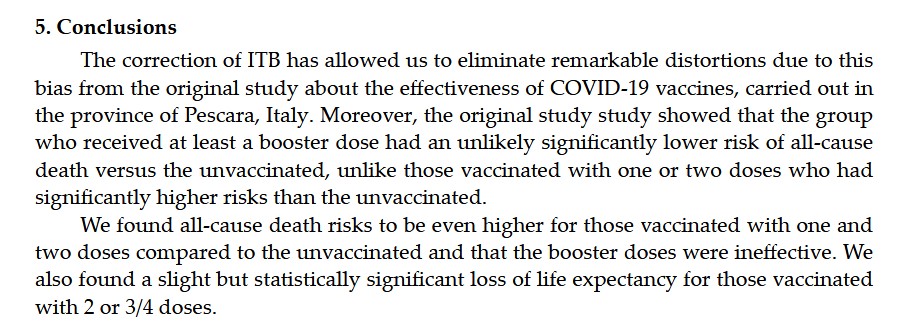
The second most recent discovery, that the COVID-19 “vaccines” reduce life expectancy (even in “all-cause” analysis) among COVID-19 “vaccinated” persons, by Dr. Peter A. McCullough: https://petermcculloughmd.substack.com/p/breaking-publication-a-critical-analysis, “BREAKING Publication — A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, 1 July 2024. The peer-reviewed paper is here: https://doi.org/10.3390/microorganisms12071343, “A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province”, Marco Alessandria, et al., published 30 June 2024. Below is a screenshot from the Conclusions section of this paper:
In Yours Truly’ opinion, it is apparent at “half a glance” that the COVID-19 “vaccines” (actually, gene therapy injections) must be completely withdrawn for human use until these products have been fully investigated, and then re-designed, before being re-introduced for human use; and, that there is no “co-ownership” or sharing of royalties between a government agency and a COVID-19 “vaccine” manufacturer; and, that there is no involvement of the United States military in the development or manufacture of such products.
This series of posts regarding the ongoing issues of COVID-19 and the COVID-19 “vaccines” is dedicated to the memory of Yours Truly’s cousin Bill, who passed away “suddenly and unexpectedly” in September 2023. Today’s post is addressed to medical professionals who had any COVID-19 “vaccines” (in reality, gene therapy injections) injected into their bodies since 11 December 2020. This post is not “accusatory” in nature: Yours Truly is curious. One will make it clear at the outset that there are vaccines and other injectables that are useful: For examples, the Rabies vaccine and the injectable form of Heparin. One will also make it clear that the following questions regarding the modRNA COVID-19 “vaccines” are not “tin-foil hat” or “conspiracy theory” in nature — all of them are based on the writings and researching of medical doctors and scientists who want to find out the truth about these particular “vaccines.” There are many other questions that must be asked; Yours Truly is presenting a few of the most important ones from a personal point of view in today’s post.
Dear COVID-19 “Vaccinated” Medical Professional:
With all due respect for your education and expertise, there now must be serious questions raised concerning the COVID-19 “vaccines” that were rushed into use in the United States and all over the world. These questions are especially important given the increasing numbers of reports of COVID-19 “vaccine”-induced injuries, illnesses, disabilities, and deaths, among those who have taken, and/or continue to take, these “vaccines.”
The first question that must be raised is: Are you aware that the FDA knew, back on 30 April 2021, that the modRNA COVID-19 “vaccine” by Pfizer-BioNTech, BNT162b2, is involved in the inducement of over 1,200 types of medical diseases and conditions? Here is the document that Pfizer-BioNTech gave to the FDA on that date: https://phmpt.org/document/5-3-6-postmarketing-experience.pdf, 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021. Please see page 30 of this report, APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST. The report is also found here: https://phmpt.org/document/5-3-6-postmarketing-experience.pdf. The document is FDA time-stamped 30 April 2021. Yours Truly will point out that this report covers only between 11 December 2020 (the date of the initial EUA granted by the FDA for BNT162b2 to be used in the United States) and 28 February 2021. The list of Adverse Events of Special Interest begins with 1p36 deletion syndrome; other diseases, disorders, and events mentioned include: Cardiac arrest; Cerebral thrombosis; Demyelination; Guillain-Barre syndrome; hepatic disorders; immune system disorders; pulmonary disorders; Myocarditis; neurological disorders; and, Pericarditis; among many others.
The second question that must be raised is: Are you aware that the modRNA COVID-19 “vaccines” made by Pfizer-BioNTech (these include BNT162b2; this company’s previous “booster” COVID-19 “vaccines”; and this company’s current “2023-2024 Formula COVID-19 Vaccine”) contain two dangerous lipid nanoparticles, ALC-0159 and ALC-0315, both of which are for research use only? Here are the Safety Data Sheets for these lipid nanoparticles: For ALC-0159: https://cdn.caymanchem.com/cdn/msds/34336m.pdf; and, for ALC-0315: https://cdn.caymanchem.com/cdn/msds/34337m.pdf. On page one of each of these Safety Data Sheets, there is the following language: “Application of the substance / the mixture This product is for research use – Not for human or veterinary diagnostic or therapeutic use.” In addition, are you aware that the modRNA COVID-19 “vaccines” made by Moderna (these include mRNA-1273; this company’s previous COVID-19 “booster vaccines”; and this company’s current “2023-2024 Formula COVID-19 Vaccine”) contain the dangerous lipid nanoparticle, SM-102, which is for research purposes only? Here is the Safety Data Sheet for this lipid nanoparticle: https://cdn.caymanchem.com/cdn/msds/33474m.pdf. On page one of this Safety Data Sheet, there is the exact same language in the section “Application of the substance / the mixture” as is listed for ALC-0159 and for ALC-0315 in their respective Safety Data Sheets: “This product is for research use – Not for human or veterinary diagnostic or therapeutic use.” (As an aside, ALC-0149 and ALC-0315 are described only by their chemical component names in the FDA-issued Fact Sheet for the Pfizer-BioNTech “2023-2024 Formula COVID-19 Vaccine”: www.fda.gov/media/167211/download; please see under section 11 DESCRIPTION. However, ALC-0159 and ALC-0315 are called by their proper names in the FDA document, www.fda.gov/media/172019/download, Emergency use Authorization (EUA) for an Unapproved Product Review Memorandum, dated 23 June 2023, section 7.1 Chemistry Manufacturing and Control (CMC) Information.)
The third question that must be raised is: Are you aware that the COVID-19 “vaccines” can, and do, “shed” components of these products from “vaccinated” persons to un-“vaccinated” persons? Dr. Pierre Kory has an extensive series of articles on his blog relating to this phenomenon: https://pierrekorymedicalmusings.com/; please see Part One of this series: https://medicalmusings.com/p/shedding-of-covid-mrna-vaccine-components, published 1 November 2023.
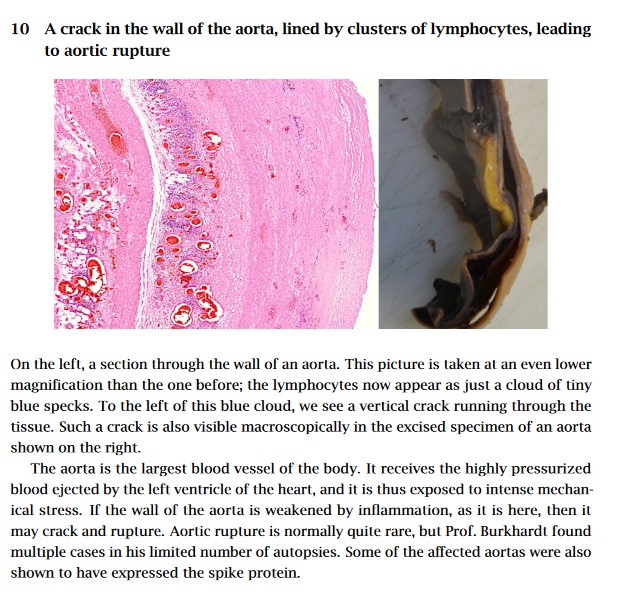
The fourth question that must be asked is: Are you aware that the COVID-19 “vaccines” can, and do, damage the blood vessels, heart tissue, and lung tissue, of persons who have these “vaccines” in their bodies? Please refer to: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, “Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality”, Michael Palmer, MD, and Sucharit Bhakdi, MD. Yours Truly presents page nine of this paper, which is self-explanatory:
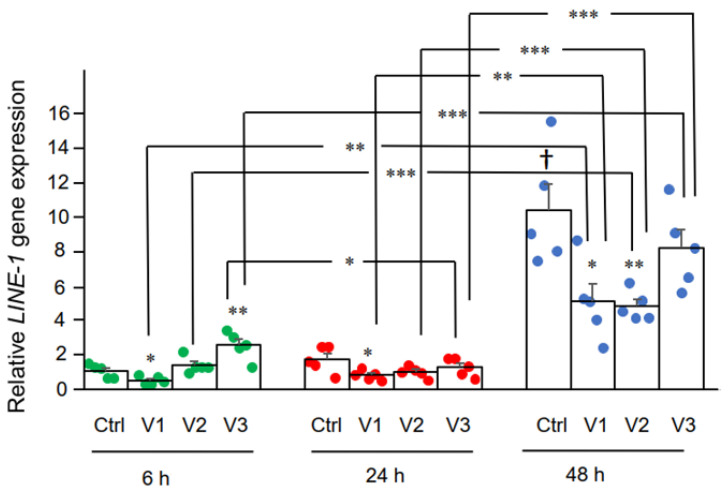
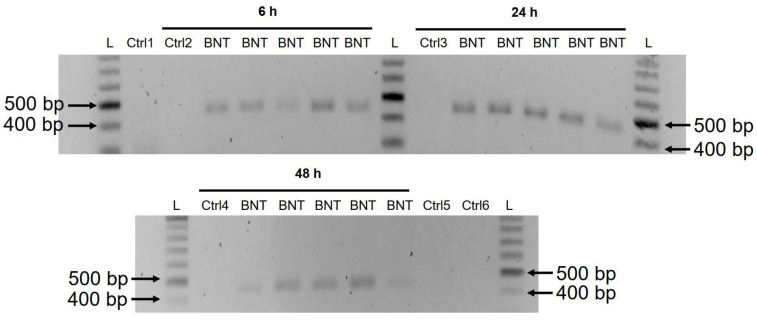
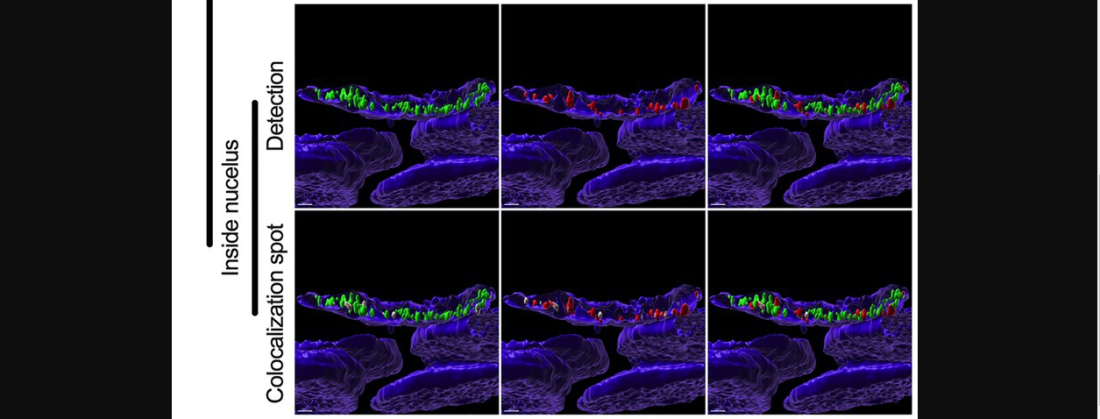
The fifth question that must be asked is: Are you aware that the modRNA Pfizer-BioNTech COVID-19 “vaccine”, BNT162b2, changes the DNA of the LINE-1 Human Liver7 cell line? Please refer to: https://doi.org/10.3390/cimb44030073, “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line”, Yang De Marinis, et al. Yours Truly presents two images from this paper: The first, of DNA expression induced in BNT162b2-treated Human Liver7 cells in LINE-1; the second, of DNA amplicons induced by BNT162b2-treated Human Liver7 cells in LINE-1.
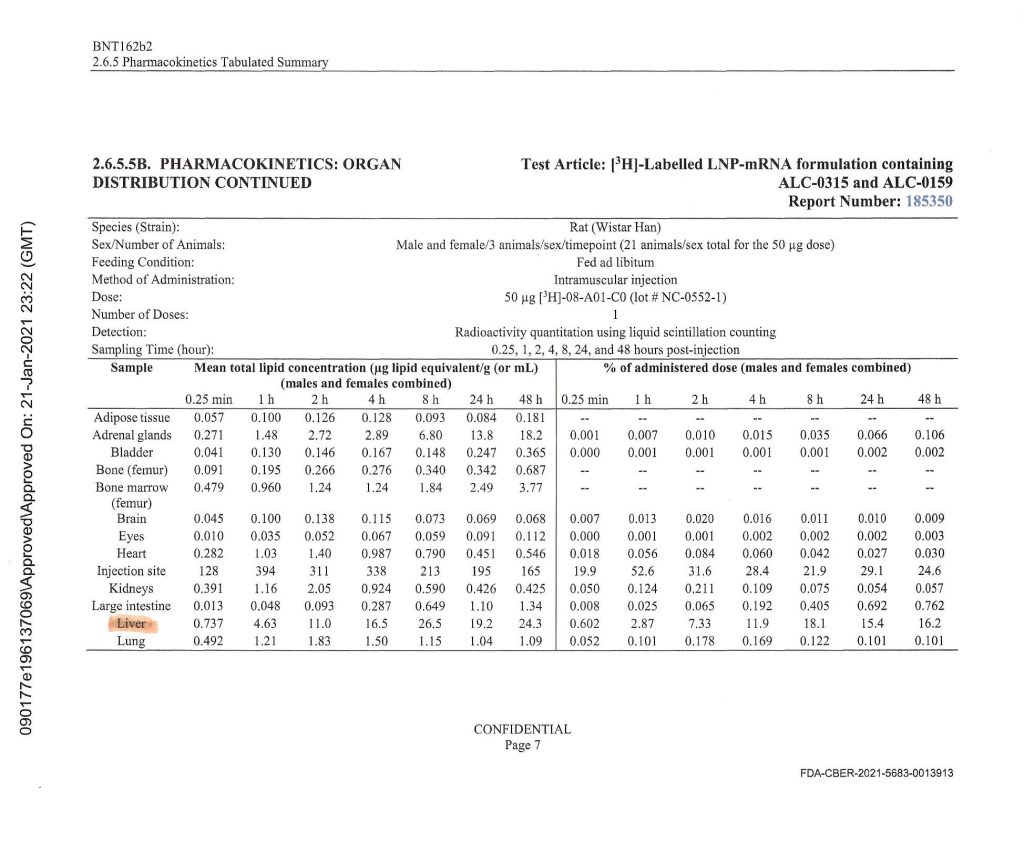
Notice the heavy accumulation of BNT162b2 in the livers of the Wistar lab rats that were used in this experiment conducted by Pfizer-BioNTech. This was the same BNT162b2 Pfizer-BioNTech modRNA COVID-19 “vaccine” that was later injected into human patients (with ingredients amounts calibrated for human use.)
Yours Truly will note that the CDC changed the definitions of “vaccine” and “vaccination” in 2021, after the rollout of the COVID-19 “vaccines” (gene therapy injections.) One suspects that this was done to “shoe-horn in” these products under the aegis of “vaccines.” Please refer to: www.johnlocke.org/the-cdc-changed-its-definitions-of-vaccine-and-vaccination-and-keeps-changing-its-definition-of-fully-vaccinated/. However, the FDA states clearly, on page four of the Fact Sheet for Healthcare Providers for the administration of the “2023-2024 Formula COVID-19 Vaccine” by Pfizer-BioNTech, that this product is to prevent coronavirus disease (COVID-19), not to “protect against serious illness from COVID-19”, as the CDC states. Please refer to: www.fda.gov/media/167211/download, page four, under section 1 EMERGENCY USE AUTHORIZATION; and to www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html under What You Need to Know.
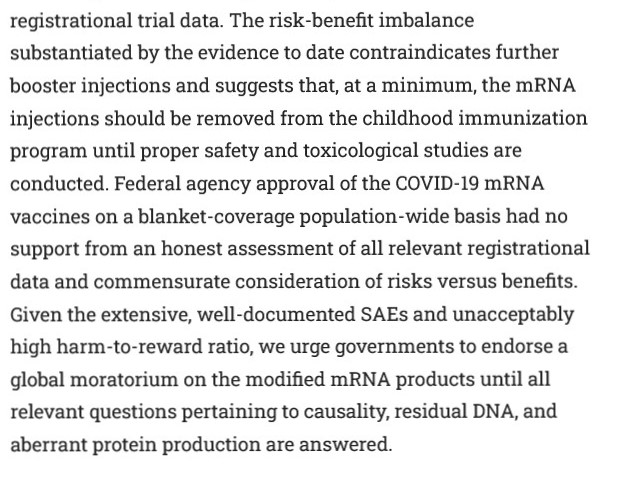
Finally, there is this paper, published on 24 January 2024: https://doi.org/10.7759/cureus.52876, “COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign”, M. Nathaniel Mead, Peter A. McCullough, et al. Yours Truly presents part of the Abstract of this paper:
Sincerely, with Good Energy, Peace, and Respect, PAVACA
PAVACA: BFA (2), Carnegie-Mellon University; MA, Duquesne University. Reading and writing about COVID-19 and the COVID-19 “vaccines” since March 2020. Also interested in Pharmacy and in the impacts of Big Pharma. General Editor of Imagination-Building: The Memoirs of John Douglas Forbes (1910 – 2018), First Professor of the Darden School of the University of Virginia, available at www.amazon.com/, www.barnesandnoble.com/, and www.authorhouse.com/.
The above is an image of Father Christmas from a vintage postcard.
The following may be a bit “heavy” — please regard it as a kind of rich “Christmas Pudding” of COVID-19 “vaccine” knowledge base. Not a “lump of coal!”
Just in time for Christmas, Yours Truly presents a list of what she considers to be the “Top 12” types of damage that the COVID-19 “vaccines” can do to the body of the “vaccine” recipient. This list has been gathered from the 1600+ hours of investigating “all things COVID-19” that Yours Truly has done since March 2020. Therefore, it is only her opinion. People who read through the report that Pfizer-BioNTech gave to the FDA on 30 April 2021, regarding the over 1,000 serious adverse events medical conditions that the company’s COVID-19 “vaccine”, BNT162b2, caused in persons who took this “vaccine” IN FEWER THAN THREE MONTHS after the FDA granted the initial EUA for this “vaccine” in December 2020 for its use in the United States, may come up with “Top Lists” of their own. The report can be found here: https://phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf, BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Events Reports. The APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST, found at the end of the report, lists these serious adverse events conditions reports that BNT162b2 caused in “vaccinated” persons.
However, what is NOT opinion is that the FDA then knew, on 30 April 2021, that the Pfizer-BioNTech “flagship” COVID-19 “vaccine” BNT162b2 (actually, an untried gene therapy injection), was capable of damaging the body of the “vaccine” recipient in over 1,000 different ways, including the ways on Yours Truly’s “Top 12 List..” However, instead of performing its regulatory (and moral and ethical) obligations to immediately pull BNT162b2 off the market and out of use until the situation could be further investigated, the FDA chose to CONTINUE the EUA that it granted in December 2020 for BNT162b2. Not only that, but the FDA went ahead and granted “full approval” for the use of the European version of BNT162b2, called COMIRNATY, in the United States. Not only that, but the FDA granted EUA’s for the Pfizer-BioNTech COVID-19 “bivalent vaccine” to be used in the United States. Finally, in the spring of 2023, the FDA quietly stopped all use of BNT162b2 in the United States — in Yours Truly’s opinion, after mounting reports of serious adverse events, including deaths, being caused by this “vaccine” were beginning to circulate widely and to be confirmed by professional researchers and by doctors — and substituted the use of the Pfizer-BioNTech (and the Moderna) “booster vaccines” for the Omicron variant. In the summer of 2023, the FDA granted EUA’s for both the Pfizer-BioNTech and for the Moderna “2023-2024 Formula COVID-19 Vaccine”, which had only been tested on mice.
Here is Yours Truly’s “Top 12 List”: The first nine, from the APPENDIX 1. cited above:
Death: neonatal and Sudden unexplained death in epilepsy (page 3 and page 8); Myocarditis and Pericarditis (page 6 and page 7); Stroke (Cerebral artery embolism page 2; Cerebral thrombosis, page 2); Thrombotic Stroke (page 9), among other types; THIRTY different types of Autoimmune disorders (page 2); FORTY different types of Herpes disorders (page 4 and page 5); THIRTY-PLUS different types of Liver disorders (page 4); TWENTY-FIVE different types of Immune System disorders (page 5); SIXTEEN different types of Neurological (brain and/or central nervous system) disorders (page 6); and, COVID-19 and COVID-19 Pneumonia (page 3).
As an example, here is a handy-dandy image of page 4 of the APPENDIX 1., with Yours Truly’s notes:
To round out the “Top 12 List” of COVID-19 “vaccine” damage to the body of the recipient, there are these three:
One: Heart tissue and lung tissue damage / destruction: Please refer to: https://doctors4covidethics.org/wp-content/uploads/2022/08/causality-article.pdf, by Michael Palmer, MD, and Sucharit Bhakdi, MD; Two: Fetal / Neonatal disorders, including 1p36 deletion syndrome (also listed on page 1 of the APPENDIX 1.): Please refer to the following regarding 1p36 deletion syndrome: https://medlineplus.gov/genetics/condition/1p36-deletion-syndrome/ (more on this condition below); and, Three: Cancer induced with the assistance of the SV40 cancer promoter DNA that has been recently discovered in the Pfizer-BioNTech COVID-19 “vaccines” (more on this below): Please refer to the following: https://osf.io/preprints/osf/mjc97, “DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events”, David Speicher, Jessica Rose, Kevin McKernan, et al. From lines 94-95 of this paper: “McKernan, et al., found SV40 promoter-enhancer-ori [DNA], and SV40 polyA signal sequences in the Pfizer vaccines.” The SV40 promoter-enhancer DNA is also in the Pfizer-BioNTech COVID-19 “vaccines” that were used in the United States: https://rumble.com/v3r1pqf-vaccine-adulteration-wkevin-mckernan-byram-bridle-chris-martenson-steve-kir.html, beginning at 3:32 in the video. Please also refer to the letter of December 2023 from Florida Surgeon General, Dr. Joseph Ladapo, to the directors of the FDA and the CDC: www.floridahealth.gov/about/_documents/12-06-2023-DOH-Letter-to-FDA-RFI-on-COVID-19-Vaccines.pdf. Yours Truly will posit that, since the modRNA + its spike protein and the “Process 2” manufacturing method for the current “2023-2024 Formula COVID-19 Vaccine” by this company in use in the United States are both based on its original “vaccine” formulations (BNT162b2 and the “booster and bivalent vaccines”), it appears that this opens up the possibility that the SV40 promoter-enhancer DNA is present in this “vaccine” also. Important: The SV40 promoter-enhancer DNA in the Pfizer-BioNTech COVID-19 “vaccines” is not the entire code, only a part of it. In and of itself, this “partial code” likely would not cause cancer; however, it can be involved in the general damage / destruction that the COVID-19 “vaccines” do to the “vaccine” recipient’s body, which can, in turn, be involved in the onset of cancer, or the re-emergence of cancer already in remission, in that person’s body. In addition, Pfizer-BioNTech DID NOT TELL the Canadian health authorities, nor, apparently, the FDA in the United States, about the SV40 issue.
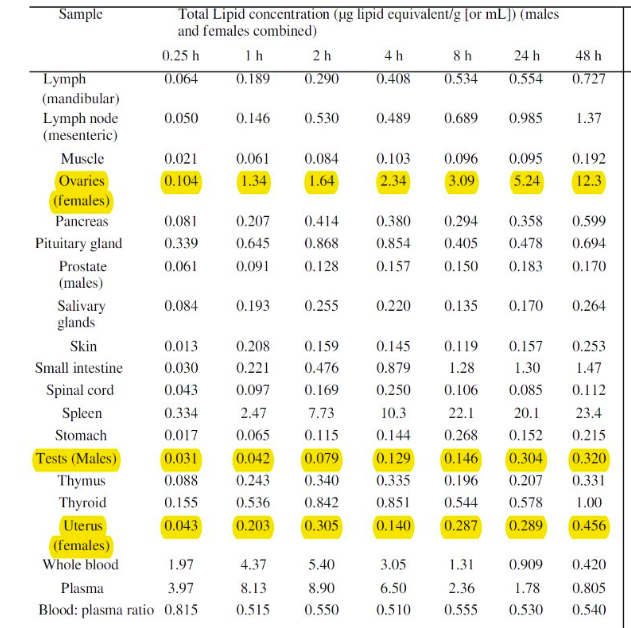
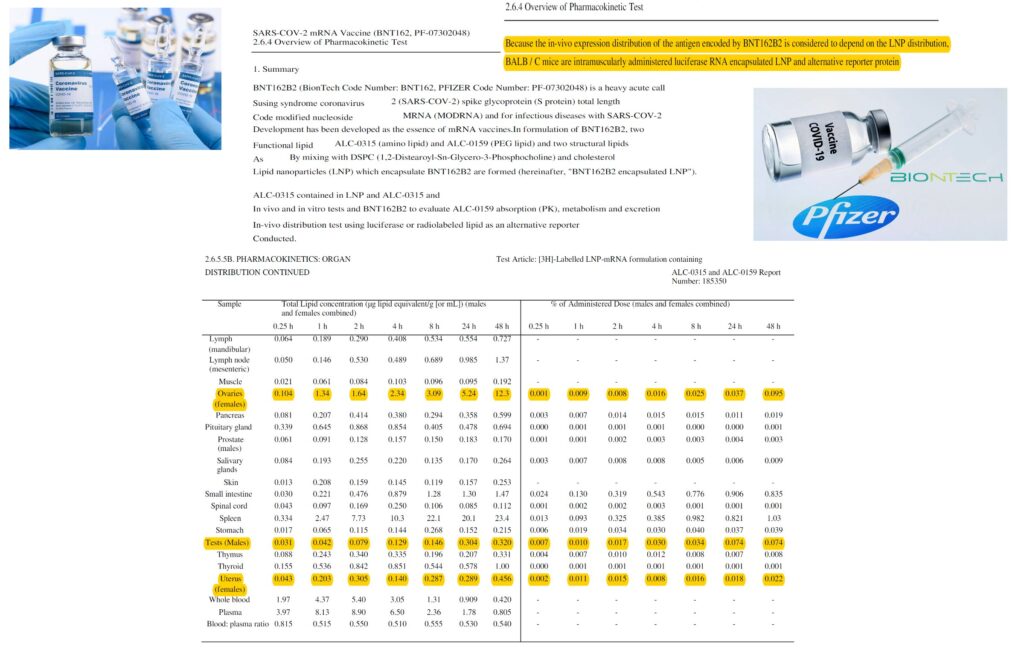
About the 1p36 deletion syndrome caused by the modRNA COVID-19 “vaccines”: This is particularly troubling, since it effects UNBORN children and THE SPERM AND THE EGGS OF THE “VACCINATED” PARENTS. 1p36 deletion syndrome is a multi-faceted condition that negatively affects fetal development. Infants born with this condition have severe intellectual difficulties; weak muscle tone; have vision, hearing, and heart issues; and either do not speak, or can only speak a limited vocabulary; among other things. Please refer to the MedlinePlus link, above, for further information. It has been proven that large amounts of the dangerous lipid nanoparticles AND the enhanced spike protein + its modRNA in the Pfizer-BioNTech COVID-19 “vaccine” migrate to, and lodge in, two important areas of the recipient’s body — the OVARIES and the TESTES. Please refer to the image below, directly from Pfizer-BioNTech, on page 8 of a document that the company gave to the FDA on 21 January 2021. The document is called BNT162b2 2.6.5 Pharmacokinetics Tabulated Summary. It is available through https://phmpt.org/.
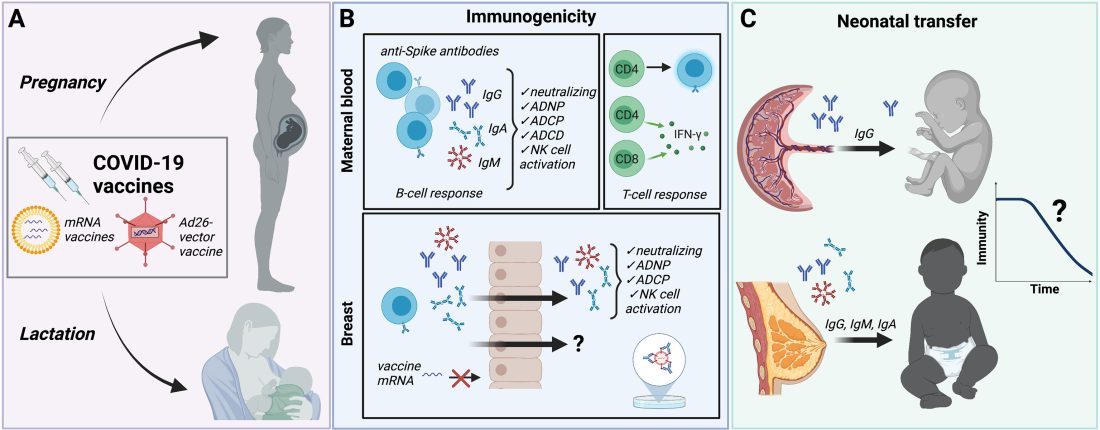
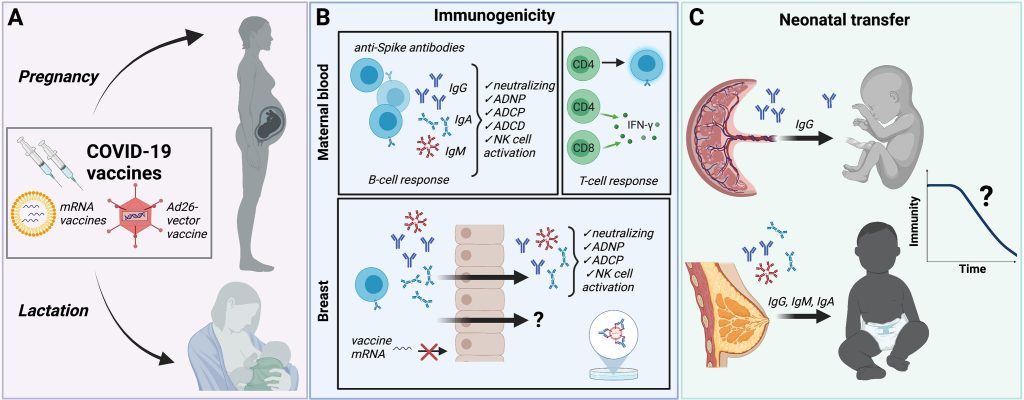
Please also refer to this graphic, which shows what the modRNA COVID-19 “vaccines” do in the pregnant mother’s body and in the body her unborn child or her nursling child (this is from a CDC presentation):
1p36 deletion syndrome is “...caused by a deletion of genetic material from a specific region in the short (p) arm of chromosome 1…Most cases of 1p36 deletion syndrome are not inherited.” (per the MedlinePlus link, above.) Think about that.
A final note on the current “2023-2024 Formula COVID-19 Vaccines” by both Pfizer-BioNTech and by Moderna: These apparently do include the ingredients (although in smaller amounts) of the original modRNA COVID-19 “vaccines” made by each company (BNT162b2 by Pfizer-BioNTech; and, mRNA-1273 by Moderna), with additional elements of the Omicron XBB 1.5 variant lineage. Please refer to the following: www.fda.gov/media/167211/download, page 39 (Pfizer-BioNTech); www.fda.gov/media/167208/download, page 34 (Moderna); and, https://covid19.nih.gov/covid-19-vaccines.
As an aside, in case readers hear someone “congratulating themselves” for their taking either the Novavax or the Johnson & Johnson (Janssen) COVID-19 “vaccines”, because they believed that somehow these “vaccines” are “safer” than those of Pfizer-BioNTech or of Moderna: The Novavax COVID-19 “vaccine” uses the same modRNA + its spike protein as in the Pfizer-BioNTech and the Moderna COVID-19 “vaccines.” The difference with the Novavax COVID-19 “vaccine” is that the SARS-CoV-2 virus is “marinated” in an insect culture, with the resulting modRNA “harvested” and mixed with “adjuvants” made from soap tree bark; this “vaccine” also uses lipid nanoparticles (LNPs.). The Johnson & Johnson (Janssen) COVID-19 “vaccine” was removed from use (revoked) in the United States by the FDA in May 2023. However, persons who took this “vaccine” prior to May 2023, are at risk for Thrombosis and Thrombocytopenia, as listed on the “black letter warning” area on the (revoked) FDA Fact Sheet for Healthcare Providers for this “vaccine.” Please refer to the following: for the Novavax COVID-19 “vaccine”: www.fda.gov/media/159897/download, page 33; www.hackensackmeridianhealth.org/en/healthu/2022/08/09/novavax-vaccine-how-its-different-and-how-it-works; and, for the Johnson & Johnson (Janssen) revoked COVID-19 “vaccine”: www.fda.gov/media/146304/download, page 1.
Yours Truly will make it clear she believes that COVID-19, in its variants forms, is still a threat to health. Since one is a concerned citizen, not a healthcare practitioner, one can only offer the following thoughts:
First: it is of primary importance that all people have, and maintain, the best level of personal health and immunity that is possible; “un-vaccinated” people have a primary responsibility here to themselves. Second: It is of primary importance that all “un-vaccinated” people follow a protocol for prophylaxis against COVID-19, such as those outlined at https://covid19criticalcare.com/, and including judicious exposure to sunlight and daily mild to moderate exercise. Third: It is of primary importance that all people follow “common sense” approaches, such as washing the hands, and staying away from sick people if possible. Fourth: It is of importance that “vaccinated” people know about various protocols to try and mitigate the dangerous effects of the COVID-19 “vaccines” at work in their bodies; https://covid19criticalcare.com/treatment-protocols/. Fifth: It is of great importance to have and keep a positive connection with a Supreme Being.
“Then will you know the truth, and the truth shall set you free.” John 8:32
It is past time, in Yours Truly’s opinion, to bring to justice those who were/are involved in the development and manufacture of the COVID-19 “vaccines”; and those in the FDA / CDC / AMA, and other medical agencies and organizations, who either know, should have known, or knew of, the dangers of these “vaccines” — but still continue to push them. Some examples: Albert Bourla, DVM (CEO of Pfizer Inc.); Stephane Bancel (CEO of Moderna); Alex Gorsky (CEO of Johnson & Johnson until 2022); Anthony Fauci, MD (former head of the NIAID); Francis Collins, MD (former head of the NIH); Janet Woodcock, MD (former Acting Commissioner of the FDA); Rochelle Walensky, MD (former Director of the CDC); Peter Daszak, CEO of EcoHealth Alliance; Robert Califf, MD (current Commissioner of the FDA); Mandy Cohen, MD (current Director of the CDC); Jesse M. Ehrenfeld, MD, (current head of the AMA); and, Ralph Baric, PhD, of the Baric Lab at the University of North Carolina, Chapel Hill.
The image above is a still from Just Imagine, a 1930 movie about what life in New York City would be like in the year 1980.
This series of pieces on the disaster of COVID-19 (the virus and the modRNA “vaccines” for said virus) is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September, 2023. May he rest in eternal Peace.
Three prefatory notes: One, that what is presented here is only “scratching the surface” regarding the substitution of “Process 2” for the original “Process 1” manufacturing method for the Pfizer-BioNTech “flagship” COVID-19 “vaccine”, BNT162b2; Two, the exact and complete details of “Process 2” are likely a “trade secret” to the company (except that a full description may be in a document given by said company to the FDA, and which was “redacted out” in case it ever got published under FOIA); and, Three, that every Pfizer-BioNTech COVID-19 “vaccine” since October, 2020, has been made using “Process 2” — including the “latest” version, the “2023-2024 Formula” version for use against the (now basically obsolete) XBB.1.5 Omicron variant.
The trail in regards a discussion of the sudden change from the original “Process 1” to the substituted “Process 2” for BNT162b2 can potentially begin in several places; for purposes of today’s presentation, it will begin here: www.bmj.com/content/378/bmj.o1731/rr-2, a letter to the British Medical Journal by Josh Guetzkow, a senior lecturer at Hebrew University in Jerusalem, in response to the BMJ article, “Covid-19: Researchers face wait for patient level data from Pfizer and Moderna vaccine trials.” Prof. Guetzkow points out that the initial clinical trials doses of the Pfizer-BioNTech modRNA COVID-19 “vaccine”, BNT162b2, were made using what was called “Process 1”, from May to October, 2020; but that the company suddenly changed to a new method, called “Process 2” [by 29 October 2020.] He also points out that the “Process 2” batches of BNT162b2 were found to have “…substantially lower mRNA integrity.” It appears that “substantially lower mRNA integrity” includes evidence of what may be termed “fragments” of DNA appearing in these “vaccines”, where they should never be.
Please bear with Yours Truly, this may get a little “technical”, but it is necessary to the whole.
So, what exactly happened by October 2020 that led Pfizer-BioNTech to change to “Process 2” for BNT162b2? One hint is found on Page 54 of the “Protocol Amendment 9, 29 October 2020” document that the company gave to the FDA (www.nejm.org/doi/suppl/10.1056/NEJMoa2034577; scroll down to “Protocol PDF” and click to get the entire document):
Another hint is found on Page 3 of the same document:
It would appear, then, that Pfizer-BioNTech decided, sometime between 1 May and 1 October 2020, to, One: add an “additional exploratory objective” to the C4591001 clinical study of BNT162b2;, and, Two, to support “increased supply” (of BNT162b2, presumably after securing Emergency Use Authorizations from the European Union medicines regulatory agency and from the FDA in the United States to use the “vaccine”, which did happen) — both, by changing from “Process 1” to “Process 2” to manufacture the product. Prof. Guetzkow states that there appears to be no analysis of comparisons between using these two methods. It is also, from what Yours Truly has been able to find, not known exactly when “Process 1” was stopped as a manufacturing method for BNT162b2 and “Process 2” was approved as the sole method.
We now turn to Page 4 of the FDA-issued “Emergency Use Authorization (EUA) for an Unapproved Product Review Memorandum” of 23 June 2023, related to the EUA the agency granted for the use of the Pfizer-BioNTech “2023-2024 Formula” COVID-19 “vaccine” on people ages 6 months to 5 years old in the United States (www.fda.gov/media/172019/download.) Page 4, in Yours Truly’s opinion, is a tacit admission that this “vaccine” is indeed made according to “Process 2”:
Finally, there is the following hint in the description of the manufacturing process for the Pfizer-BioNTech “vaccine” against meningitis, called PENBRAYA, in the 11 DESCRIPTION section of the company-issued document (https://labeling.pfizer.com/ShowLabeling.aspx?id=19937):
The work of Dr. Kevin McKernan, Dr. Jessica Rose, and other researchers, has shown that there are numerous serious issues with the integrity of the process of manufacturing BNT162b2 — the “Process 2” that was used to make billions of doses of this Pfizer-BioNTech modRNA COVID-19 “vaccine” — and which process is being used to manufacture the company’s latest modRNA COVID-19 “vaccine”, the “2023-2024 Formula.” These two scientists, along with other colleagues, published a paper on this situation last month. It can be found here: www.researchgate.net/publication/374870815. The paper also has some more details of the “Process 2” method — and, by the way, also stating that Moderna also came up with a similar process for its modRNA COVID-19 “vaccines.”
One suspects that the integrity problems with the manufacturing of the modRNA COVID-19 “vaccines” is a subject that will have much more investigation. This is aside from the accumulating evidence that the ingredients of said “vaccines” are themselves dangerous.
This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both).
What the heck! This chick will NOT get out of my Twitter X feed!
In the Bay Area today talking about vaccines for COVID, flu and RSV! Now is the best time to get #vaccinated to protect you and your family. pic.twitter.com/O3ZRIOutcA
"Jesus said to her, 'I am the resurrection and the life. He who believes in Me, though he may die, he shall live. And whoever lives and believes in Me shall never die. Do you believe this?'" (John 11:25-26)
This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both).
And yes, it’s Monday…again.
But we WILL get through it!
With Wheatie style!
With our wonderful REALPOTUS in the lead!
HANG ON!!!
Dedication
WHEATIE – OUR WARRIOR ANGEL
by Duchess01
Please forgive us, Wheatie, we did not know That you had left us with armor in tow We had no idea with what you dealt We did not know the pain you felt And now we can only imagine With you what really did happen Cause rarely did you complain And/or share your personal pain Of one thing we are most certain You are flying high behind the curtain Watching over us above the crowds Our Warrior Angel above the clouds Thank You, Wheatie, for caring for us While you were here among the fuss We miss you dear you have no idea Since time began in the pangaea With you there was no time In your wisdom you would chime To clarify and magnify The what where how and why We did not question when you left We were not slightly bereft But over time we wondered why You did not at least stop by Now we know where you have gone With the break of this new dawn We could be angry but are not Tho with an arrow we’ve been shot Rest peacefully Warrior Angel dear Send us a sign that you are near A butterfly a flower a kiss of rain From your love do not refrain God sends Angels to watch over us And now we have an Angel Plus A Warrior Angel of Magnificence From today and forward hence
Boilerplate, more or less, but worth reading again and again, if only for the minor changes, and to stay out of moderation.
MINOR CHANGE NUMBER 1
Now shortened.
Give them nothing.
Play smart. Every minute, the COUPISTS who stole the election – who lied – who deserve to be at the business end of the very same laws they are using so wrongly against the January Sixth defendants – are trying to set you up. Don’t be a chump. Turn everything back against THEM. Every day, every hour, every minute, every second.
YOU are responsible for your own comments, if they come knocking. YOUR choice. Just remember this…..
For an updated version…..
And for a version that includes your having righteously defended yourself…..
OTHER THAN THAT…….
The bottom line is Free Speech. Theories and ideas you don’t agree with must be WELCOME here, and you must be part of that welcoming. But you do NOT need to be part of any agreement.
Bottom line – respect other people’s FIRST AMENDMENT RIGHTS.
Our only additional requirement is that you do so NICELY. Or at least try to make some effort in that direction.
SO….. [ENGAGE BOILERPLATE…..]
We must endeavor to persevere to love our frenemies – even here.
Those who cannot deal with this easy requirement will be forced to jump the hoops of moderation, so that specific comments impugning other posters and violating the minimal rules can be sorted out and tossed in the trash.
In Wheatie’s words, “We’re on the same side here so let’s not engage in friendly fire.”
That includes the life skill of just ignoring certain other posters.
We do have a site – The U Tree – where civility is not a requirement. Interestingly, people don’t really go there much. Nevertheless, if you find yourself in an “argument” that can’t really stay civil, please feel free to “take it to the U Tree”. The U Tree is also a good place to report any technical difficulties, if you’re unable to report them here. Please post your comment there on one of Wolf’s posts, or in reply to one of Wolf’s comments, to make sure he sees it (though it may take a few hours).
We also have a backup site, called The Q Tree as well, which is really The Q Tree 579486807. You might call it “Second Tree”. The URL for that site is https://theqtree579486807.wordpress.com/. If this site (theqtree.com) ever goes down, please reassemble at the Second Tree.
If the Second Tree goes down, please go to The U Tree, or to our Gab Group, which is located at https://gab.com/groups/4178.
We also have some “old rules” and important guidelines, outlined here, in a very early post, on our first New Year’s Day, in 2019. The main point is not to make violent threats against people, which then have to be taken seriously by law enforcement, and which can be used as a PRETEXT by enemies of this site.
In the words of Wheatie, “Let’s not give the odious Internet Censors a reason to shut down this precious haven that Wolf has created for us.”
A Moment of Prayer
Our policy on extreme religious freedom on this site is discussed HERE. Please feel free to pray and praise God anytime and anywhere.
Thus, please pray for our real President, the one who actually won TWO elections.
You may also pray for our nation, our world, and even our enemies.
Musical Interlude
In honor of dear Wheatie, we now present some music to soothe, inspire, invigorate, or relax.
Let’s start off in a “Wheatie way” with some epic orchestral violins!
OK – how about some country music? I just heard this one on the radio. Never heard it before.
Now this is just interesting. YouTube keeps trying to suggest Taylor Swift to me, but the first song it suggested was a duet with one of the [Dixie] Chicks, which shows you exactly where Menshevik YouTube was trying to send me – to MARXIST QUISLING CITY.
Well, I looked further down the list of treasonous suggestions, and the same guest vocalist Luke Bryan in the above video is in this one, but it’s six years earlier.
Remember – Taylor Swift started off in country / folk. Then Hollywood does its thing.
Useful strategic information in the culture wars.
But let’s finish off with a real treat.
Some country line dancers send off one of their friends with his favorite song.
OK – I’m not done. ONE. MORE. SONG!!!
Let’s finish off with something “fresh” in SuSE world!
Call To Battle
Our beloved country is under Occupation by hostile forces.
Daily outrage and epic phuckery abound.
Pursuing his twisted agenda, Biden dishonors the American flag and breaks federal law.
4 U.S.Code Ch. 1, Sec. 7(e): “The flag of the United States of America should be at the center and at the highest point of the group when a number of flags…are grouped and displayed…” pic.twitter.com/knFt1ATe4j
— Speaker Mike Johnson (@SpeakerJohnson) June 11, 2023
MSM got a memo – “stop using ‘classified documents’ verbiage and change to ‘sensitive documents’…
JENNIFER BILEK: Is humanity ready for LGBTQ+ tech babies and the full erasure of women from reproduction? | Human Events | humanevents. @11thBlog https://t.co/OrZNO1VFuf
Wolbachia is a genus of intracellular bacteria that infects mainly arthropod species, including a high proportion of insects, and also some nematodes. It is one of the most common parasitic microbes, and is possibly the most common reproductive parasite in the biosphere. Its interactions with its hosts are often complex, and in some cases have evolved to be mutualistic rather than parasitic. Some host species cannot reproduce, or even survive, without Wolbachia colonization. One study concluded that more than 16% of neotropical insect species carry bacteria of this genus, and as many as 25 to 70% of all insect species are estimated to be potential hosts.
History of Wolbachia:
The genus was first identified in 1924 by Marshall Hertig and Simeon Burt Wolbach in the common house mosquito. They described it as “a somewhat pleomorphic, rodlike, Gram-negative, intracellular organism [that] apparently infects only the ovaries and testes“. Hertig formally described the species in 1936, and proposed both the generic and specific names: Wolbachia pipientis. Research on Wolbachia intensified after 1971, when Janice Yen and A. Ralph Barr of UCLA discovered that Culex mosquito eggs were killed by a cytoplasmic incompatibility when the sperm of Wolbachia-infected males fertilized infection-free eggs. The genus Wolbachia is of considerable interest today due to its ubiquitous distribution, its many different evolutionary interactions, and its potential use as a biocontrol agent.
Why Bill Gates is probably interested in Wolbachia:
Note: This is just the beginning. Look HERE for more.
These bacteria can infect many different types of organs, but are most notable for the infections of the testes and ovaries of their hosts. Wolbachia species are ubiquitous in mature eggs, but not mature sperm. Only infected females, therefore, pass the infection on to their offspring. Wolbachia bacteria maximize their spread by significantly altering the reproductive capabilities of their hosts, with four different phenotypes:
Male killing occurs when infected males die during larval development, which increases the rate of born, infected females.
Feminization results in infected males that develop as females or infertile pseudofemales. This is especially prevalent in Lepidoptera species such as the adzuki bean borer (Ostrinia scapulalis).
Parthenogenesis is reproduction of infected females without males. Some scientists have suggested that parthenogenesis may always be attributable to the effects of Wolbachia. Though this is not the case for the marbled crayfish. An example of parthenogenesis induced by presence of Wolbachia are some species within the Trichogramma parasitoid wasp genus, which have evolved to procreate without males due to the presence of Wolbachia. Males are rare in this genus of wasp, possibly because many have been killed by that same strain of Wolbachia.
Cytoplasmic incompatibility is the inability of Wolbachia-infected males to successfully reproduce with uninfected females or females infected with another Wolbachia strain. This reduces the reproductive success of those uninfected females and therefore promotes the infecting strain. In the cytoplasmic incompatibility mechanism, Wolbachia interferes with the parental chromosomes during the first mitotic divisions to the extent that they can no longer divide in synchrony.
Several host species, such as those within the genus Trichogramma, are so dependent on sexual differentiation of Wolbachia that they are unable to reproduce effectively without the bacteria in their bodies, and some might even be unable to survive uninfected.
One study on infected woodlice showed the broods of infected organisms had a higher proportion of females than their uninfected counterparts.
Wolbachia, especially Wolbachia-caused cytoplasmic incompatibility, may be important in promoting speciation. Wolbachia strains that distort the sex ratio may alter their host’s pattern of sexual selection in nature, and also engender strong selection to prevent their action, leading to some of the fastest examples of natural selection in natural populations.
The male killing and feminization effects of Wolbachia infections can also lead to speciation in their hosts. For example, populations of the pill woodlouse, Armadillidium vulgare which are exposed to the feminizing effects of Wolbachia, have been known to lose their female-determining chromosome. In these cases, only the presence of Wolbachia can cause an individual to develop into a female. Cryptic species of ground wētā (Hemiandrus maculifrons complex) are host to different lineages of Wolbachia which might explain their speciation without ecological or geographical separation.
Wolbachia infection has been linked to viral resistance in Drosophila melanogaster, Drosophila simulans, and mosquito species. Flies, including mosquitoes, infected with the bacteria are more resistant to RNA viruses such as Drosophila C virus, norovirus, flock house virus, cricket paralysis virus, chikungunya virus, and West Nile virus.
In the common house mosquito, higher levels of Wolbachia were correlated with more insecticide resistance.
In leafminers of the species Phyllonorycter blancardella, Wolbachia bacteria help their hosts produce green islands on yellowing tree leaves, that is, small areas of leaf remaining fresh, allowing the hosts to continue feeding while growing to their adult forms. Larvae treated with tetracycline, which kills Wolbachia, lose this ability and subsequently only 13% emerge successfully as adult moths.
Muscidifurax uniraptor, a parasitoid wasp, also benefits from hosting Wolbachia bacteria.
In the parasitic filarial nematode species responsible for elephantiasis, such as Brugia malayi and Wuchereria bancrofti, Wolbachia has become an obligate endosymbiont and provides the host with chemicals necessary for its reproduction and survival. Elimination of the Wolbachia symbionts through antibiotic treatment therefore prevents reproduction of the nematode, and eventually results in its premature death.
Some Wolbachia species that infect arthropods also provide some metabolic provisioning to their hosts. In Drosophila melanogaster, Wolbachia is found to mediate iron metabolism under nutritional stress and in Cimex lectularius, the Wolbachia strain cCle helps the host to synthesize B vitamins.
Some Wolbachia strains have increased their prevalence by increasing their hosts’ fecundity. Wolbachia strains captured from 1988 in southern California still induce a fecundity deficit, but nowadays the fecundity deficit is replaced with a fecundity advantage such that infected Drosophila simulans produces more offspring than the uninfected ones.
Wolbachia often manipulates host reproduction and life-history in a way that favours its own propagation. In the Pharaoh ant, Wolbachia infection correlates with increased colony-level production of reproductives (i.e., greater reproductive investment), and earlier onset of reproductive production (i.e., shorter life-cycle). Infected colonies also seem to grow more rapidly. There is substantial evidence that the presence of Wolbachia that induce parthenogenesis have put pressure on species to reproduce primarily or entirely this way.
Additionally, Wolbachia has been seen to decrease the lifespan of Aedes aegypti, carriers of mosquito-borne diseases, and it decreases their efficacy of pathogen transmission because older mosquitoes are more likely to have become carriers of one of those diseases. This has been exploited as a method for pest control.
The first Wolbachia genome to be determined was that of one that infects D. melanogaster fruit flies. This genome was sequenced at The Institute for Genomic Research in a collaboration between Jonathan Eisen and Scott O’Neill. The second Wolbachia genome to be determined was one that infects Brugia malayi nematodes. Genome sequencing projects for several other Wolbachia strains are in progress. A nearly complete copy of the Wolbachia genome sequence was found within the genome sequence of the fruit fly Drosophila ananassae and large segments were found in seven other Drosophila species.
In an application of DNA barcoding to the identification of species of Protocalliphora flies, several distinct morphospecies had identical cytochrome c oxidase I gene sequences, most likely through horizontal gene transfer (HGT) by Wolbachia species as they jump across host species. As a result, Wolbachia can cause misleading results in molecular cladistical analyses. It is estimated that between 20 and 50 percent of insect species have evidence of HGT from Wolbachia—passing from microbes to animal (i.e. insects).
Wolbachia species also harbor a bacteriophage called bacteriophage WO or phage WO. Comparative sequence analyses of bacteriophage WO offer some of the most compelling examples of large-scale horizontal gene transfer between Wolbachia coinfections in the same host. It is the first bacteriophage implicated in frequent lateral transfer between the genomes of bacterial endosymbionts. Gene transfer by bacteriophages could drive significant evolutionary change in the genomes of intracellular bacteria that were previously considered highly stable or prone to loss of genes over time.
The small non-coding RNAs WsnRNA-46 and WsnRNA-59 in Wolbachia were detected in Aedes aegypti mosquitoes and Drosophila melanogaster. The small RNAs (sRNAs) may regulate bacterial and host genes. Highly conserved intragenic region sRNA called ncrwmel02 was also identified in Wolbachia pipientis. It is expressed in four different strains in a regulated pattern that differs according to the sex of the host and the tissue localisation. This suggested that the sRNA may play important roles in the biology of Wolbachia.
Outside of insects, Wolbachia infects a variety of isopod species, spiders, mites, and many species of filarial nematodes (a type of parasitic worm), including those causing onchocerciasis (river blindness) and elephantiasis in humans, as well as heartworms in dogs. Not only are these disease-causing filarial worms infected with Wolbachia, but Wolbachia also seems to play an inordinate role in these diseases.
A large part of the pathogenicity of filarial nematodes is due to host immune response toward their Wolbachia. Elimination of Wolbachia from filarial nematodes generally results in either death or sterility of the nematode. Consequently, current strategies for control of filarial nematode diseases include elimination of their symbiotic Wolbachia via the simple doxycycline antibiotic, rather than directly killing the nematode with often more toxic antinematode medications.
The bottom line is that I have simply checked the gene sequences of the Pfizer and Moderna vaccines, and verified that they BOTH contain nucleic acid code that translates to the shorter PRRARSV protein code, which is a kind of “hall pass” into the cell nucleus.
Thus, BOTH of these vaccines produce a spike protein which science would predict has the same ability as the virus spike protein, to (1) get into the cell nucleus, and furthermore (2) schlep its own mRNA along with it into the cell nucleus, and finally (3) as proven by experiment on the Pfizer vaccine, integrate the spike protein gene sequence into the human cellular genome.
That’s it. If you want all the gory details, stay tuned. Otherwise, that’s the BLUF (bottom line up front). Have a great day! -Wolf
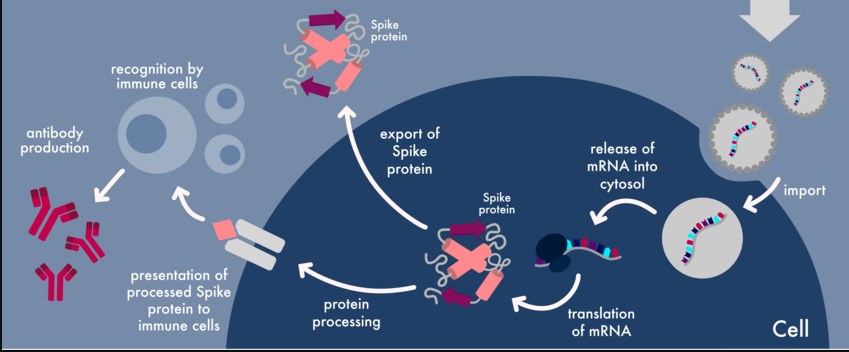
Introduction
OK – I have an important update to the whole topic of mRNA vaccines messing with people’s genes, and in particular, with a part of the COVID-19 spike protein mRNA sequence called the PRRARSV nuclear translocation signal. This “key” within the whole sequence is like an ID card for the cell nucleus. It was identified in the natural COVID-19 spike protein, and now it appears to remain in both the Pfizer and Moderna vaccines.
I have posted on this topic – the PRRARSV Nuclear Translocation Signal – THREE times before.
First, I posted when I discovered the Mehedi paper, and realized how important it is.
The Mehedi paper explains WHY there is genomic incorporation of the COVID-19 spike protein – specifically, because the spike protein has what is essentially a key to the cell nucleus.
This is SO HUGE. I must explain this to you. TL;DR – The spike protein not only contains a special sequence that allows it into the cell nucleus – it also has an ability to bring its own spike mRNA sequence with it. Both features appear to be unique among coronaviruses. The features explain genomic …
The next time I posted, was the moment that I realized that the murdered American scientist Bing Liu had been directing his research focus to the EXACT SAME SPOT in the SARS-CoV-2 gene sequence – the PRRARSV sequence – when he was conveniently murdered by a crazed acquaintance who was apparently contending with him over a lover.
To me, this murder absolutely REEKED of MKULTRA. Bing Liu had a plausible weakness and it was exploited. Not all people realize how dangerous the science world can be. Not so this cowboy – I’ve been through a lot of weird, evil bullshit in Scienceville, over the years.
Bing apparently recognized that this sequence is found in snake venoms and other, more deadly viruses, and was thus potentially close to realizing that this part of the sequence was behind certain aspects of the pathogenicity of SARS-CoV-2, as well as those other things.
Stated another way – maybe nuclear translocation is WHY those other things are so bad.
Joe Biden didn’t win. This is our Real President: AND our beautiful REALFLOTUS. This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both). …
Finally, at a certain point I realized that any “accidental” explanation of the presence of a working translocation signal which not only violates the central promise of mRNA vaccine technology, but installs the violation itself in the nucleus, was simply too incongruous to be an accident. It’s a BLOODY HACK. There was no way that – on the very first roll-out of a genetic vaccine – the technology which was PRIZED for making the technology safe against genetic incorporation, instead caused genetic incorporation OF the very instructions for genetic incorporation.
I mean, think about it. What are the chances? It’s almost as crazy as the sinking of the “unsinkable” Titanic.
You see what I’m sayin’? This outrageously excellent attack simply cannot be a case of “whoops”. The TRICK is not the “AW SHUCKS, THAT’S LIFE” which sells as stage two to the hubris of the chumps. That’s just the getaway. The TRICK is the LIE – the PROMISE that is actively worked against from the very beginning, and intentionally not delivered.
Ask yourself a simple question. Why should the very first examples of mRNA vaccines for humans violate the most important safety standard of the mRNA platform? Why would the vaccines do exactly what they PROMISED US the vaccines would not do? TL;DR – They didn’t just lie to us about the spike mRNA not going …
I wrote that last post with a certain sense of frustration. NOBODY in COVID Dissident World seemed to understand the importance of this whole “nuclear translocation signal” thing. Either that, or they were utterly afraid to speak of it. Indeed, our RDS is one of the few people who has dared to shine a light on the topic.
I set it aside for a while and basically gave up.
The other side did not give up. During that time, I was seriously shadow-banned on Twitter. Elon’s FEDS are busy little beavers, damming up the truth.
But now, something interesting has happened. On Twitter.
A Tale of Two Acronyms: PRRARSV and SV40
RDS posted a comment that included a tweet of a translated video of the brave Japanese professor who publicly challenged the Japanese Ministry of Health over the crappy vaccines.
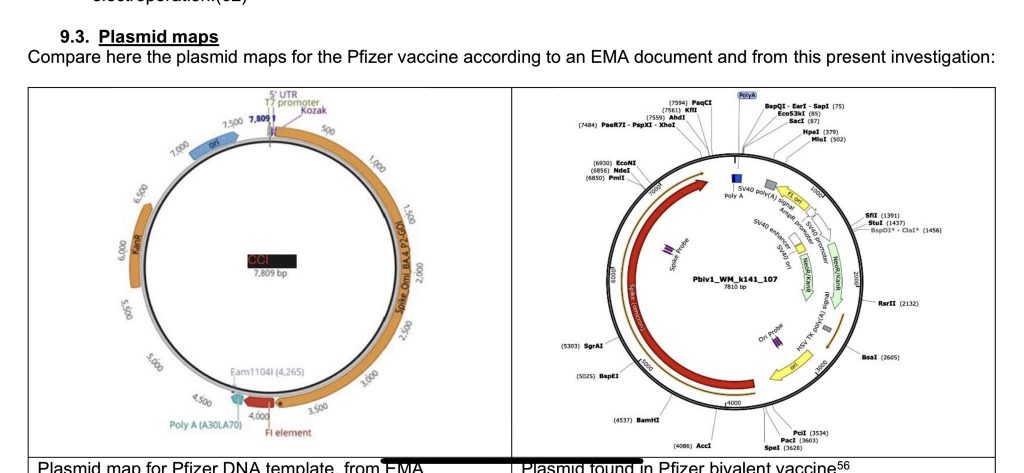
Here, Murakami is discussing contaminating plasmid DNA (little circles of DNA) which were found in very significant quantity in expired vials of the Pfizer vaccine. It’s easier to watch the video on Twitter.
This SV40 stuff also gets into a shocker about nuclear incorporation, but this is not the same shocker as the PRRARSV stuff. This is ANOTHER ANGLE on a different path into the nucleus.
Are you starting to believe me now about intent? Read on.
Japanese professor, Murakami of Tokyo University of Science made an amazing finding.
The Pfizer's vaccine contains the SV40 sequence which is known as a promoter of the cancer virus. The SV40 sequence is completely unnecessary to produce the mRNA vaccine. https://t.co/RtnbCUHAmJpic.twitter.com/gZx5ycf1L9
The translation is as follows. It is a conversation between Professor Murakami (M) and another person (P). I may have gotten a couple of assignments mixed up, when both are talking, but have done my best to attribute statements properly, based on what I can discern.
Commentary by Professor Murakami
(M) It is now possible to read the DNA sequences present in the vaccines. This is the DNA read from the Moderna vaccine.
(P) It may be difficult for the general public to understand, but this sequence is in the form of a ring. Plasmid DNA is in the form of a ring, and the DNA sequence is described in this ring. Spike proteins are encoded in this part of the DNA sequence.
(M) This part of the DNA sequence shows the spike gene. The Moderna’s vaccine has a vector sequence that is often present in Escherichia coli. However, the Pfizer’s vaccine has a staggering problem. I have made an amazing finding. This figure is an enlarged view of Pfizer’s vaccine sequence. As you can see, the Pfizer’s vaccine sequence contains part of the SV40 sequence here. This sequence is known as a promoter. Roughly speaking, the promoter causes increased expression of the gene. The promoter is a sequence that is essential for gene expression. The problem is that the sequence is present in a well-known carcinogenic virus. The question is why such a sequence that is derived from such a cancer virus is present in the Pfizer’s. There should be absolutely no need for such a carcinogenic virus sequence in the vaccine. This sequence is totally unnecessary for producing the mRNA vaccine. It is a problem that such a sequence is solidly contained in the vaccine. This is not the only problem. If a sequence this is present in the DNA, the DNA is easily migrated to the nucleus. So it means that the DNA can easily enter the genome. The problem is that if such a sequence remains intact, the DNA is easily migrated to the nucleus. It means that the DNA can easily enter the nucleus. These are such alarming problems.
(P) Does it mean that the SV40 promoter also contains sequences that can be migrated to the nucleus?
(M) Yes, that’s what I mean.
(P) So you are saying that the DNA can go to the nucleus easily?
(M) It means that the DNA contains sequences that can easily go to the nucleus. This is a well-known fact. This fact has already been documented in a number of scientific literature. It is essential to remove such sequences. The sequences have to be removed. However, Pfizer produced the vaccines without removing the sequences.
(P) This is outrageously malicious.
(M) That’s right. Pfizer retained the SV40 promoter sequence which is completely unrelated to the in vitro synthesis of the messenger.
(P) This issue should be questioned. Why such a promoter sequence is present in the DNA? This kind of promoter sequence is completely unnecessary for the production of the mRNA vaccine. In fact, SV40 is a promoter of cancer viruses.
(M) Yes, SV40 is well known.
(P) The sequence that promotes the cancer virus is present in the DNA for some reasons. As we know, we use this SV40 promoter sequence in various experiments. However, the question is why the promoter sequence is present in this mRNA vaccine.
Do YOU have some questions at this point? I sure as hell do. And the presence of multiple PHARMA TROLLS on Twitter, muddying the water with disingenuous excuses and throw-away coddles, makes things look even more suspicious.
RDS and I discussed this at some length in Saturday’s open. I urge interested readers to follow the above link, repeated here, to see our talk about this video, but it is not necessary for the following discussion.
I then proceeded to Twitter, and got caught up in a variety of arguments between the awesome Jikkyleaks and various “defenders of the narrative”, to put it kindly.
Many of these people (I will avoid calling them “pharma trolls”) shoot from the hip, and – despite sometimes being what should be experts in their fields, seem to have no grasp of basic logic applied to basic principles of biology. They are perfect, however, for defending scientific orthodoxy in a somewhat religious manner.
Meanwhile, sharper people in biotech who understand the basic WTF (like the presence of extraneous DNA in an RNA vaccine being an actual problem) are literally running toward the enemy with the downfall of the original vaccine sales narrative.
I should add, at this point, that SOMEBODY at Twitter is desperately covering all of this up. Twitter uses a stealthy way of “downgrading replies” to hide really important pharma stuff, without overtly banning content. It’s rather ingenious, but it’s VERY frustrating.
First of all, these Twitter IC people are fooling the hell out of Elon Musk – or maybe they aren’t. Either way, some of the most important biology about the vaccines is being hidden, and IMO it sucks big-time.
Thus, it was nearly impossible for me to find the following conversation again. Twitter had hidden my comments so effectively, that I myself could not find them in my own timelines of Tweets and Replies. But with persistence, I did find them.
This conversation and the interspersed commentary explains the how and why of my verifying that the nuclear translocation signal IS in fact in the two main mRNA vaccines – and in my opinion, intentionally so.
Enjoy.
We begin with a Pharm Boy attacking Murakami’s analysis.
Hello, this is false. The plasmid does not contain the entire SV40 gene, just the ori of replication, poly(A) signal, and a promoter. None of these sequences allow for translocation into the nucleus. That sequence is contained in the VP2 region, which is not in this plasmid
The abstract, with the relevant text in BOLD, is here:
ABSTRACT
One of the steps that limit transfection efficiency in non-viral gene delivery is inefficient nuclear import of plasmid DNA, once it has been delivered into the cytoplasm. Recently, via microinjection into the cytoplasm and in situ hybridizations into a few cell types, it was shown that a region of Simian virus 40(SV40), specifically a c. 372-bp fragment of SV40 genomic DNA encompassing the SV40 promoter-enhancer-origin of replication (SV40 DTS), could enable the nuclear import of a plasmid carrying these sequences (Dean D.A. Exp. Cell Res. 230 (1997) 293). In this report, we address the issue of the suitability of the SV40 DTS for cationic lipid-mediated gene delivery, and its capacity to improve the efficiency of the transfection process. For this study, we used transient reporter gene expression assays on various cell types. The gene expression from the plasmid constructs carrying the SV40 DTS varied with cell type and plasmid construct used. Such cell-type and plasmid-construct dependency on gene expression from plasmids containing the SV40 DTS suggests that the gene expression from plasmids is not entirely dependent on its ability to enhance the nuclear import of said plasmids.
The smarmy Taylor responds to this, as follows.
Lmaoooo the plasmid doesn’t contain the enhancer region genius. Just the origin of rep, promoter, and poly(A) signal.
Can you link something saying that using only these three regions that transport into the nucleus is facilitated? Take your time
McKernan does not respond to this, and I don’t know whether Taylor’s point is valid, but assuming that it is correct, the point stands – is the fragment included sufficient to enable nuclear translocation?
This is where I decided to “inject” the fact that there already IS a nuclear translocation signal present (in the lipid nanoparticle) in the spike protein mRNA, so that RNA may be covering for DNA transport as well. But I wanted to make sure that McKernan saw it – I don’t particularly care about Taylor. So I answered directly to McKernan, on the same tweet that Taylor used. I included a link to the Mehedi paper, which is sorely under-exposed.
Is any of this influenced by the simultaneous presence of a translocation signal in the spike protein itself, which does appear to assist translocation of spike mRNA?https://t.co/q2oocDy5eU
I figured that Taylor would respond, and he/she/it did immediately.
[SIDEBAR – I would not be surprised if Twitter insiders are helping these pharma bots by – e.g. – making sure that Taylor Ray and fellow “influencers” can see my input, but that my fellow free scientists, including Kevin McKernan, cannot.]
This paper is about the actual spike protein from the virus, not the spike generated from mRNA vaccines, whose binding site is inactivated.
Taylor’s comment, beginning with “this paper is about something else”, betrays a kind of battered science syndrome that keeps science exactly where the Cabal wants it – defending its own orthodoxy – never questioning by looking off the plantation. It is based on exactly the kind of authority-and-orthodoxy-defending, “teacher’s pet” science that I detest.
Yes, there is a very legitimate question about “virus versus vaccine” – that a VIRUS result is not exactly the same as a VACCINE result. However, if you’re looking at the same or similar things happening for both, and one has a shared culprit, what does logic say?
The entire vaccine paradigm is built on the idea of virus-vaccine symmetry, so if you’re not looking honestly at “virus predicts vaccine” as your FIRST STEP of analysis, you’re never going to predict anything.
Which, by the way, is exactly what the Cabal wants.
This is a perfect example of “unethical skepticism”, as The Ethical Skeptic teaches us.
Taylor at least has the decency of adding a weak and wobbly excuse for a difference – “whose binding site is inactivated”.
This is chaff and countermeasures, as Sundance likes to say. See if you can put that together from my measured, friendly response.
Yes, it's true that Mehedi's work was done on the viral spike mRNA and protein. Likewise, it is true that the full spike pseudo-mRNA in the vaccines has a few seq changes such as prolines to lock conformation, etc. Those don't address whether a functioning NT signal remains.
What I’m saying here implies that the “inactivated binding site” in the vaccine (which itself implies possible changes in the total sequence) does not necessarily affect the presence of a nuclear translocation signal (NTS). These are two different features in the protein. Bringing that up is CHAFF.
Notice that I am not backing down on the idea that data from the virus can and likely is predictive of the vaccines. I am just waiting for Taylor to assert openly that they are not.
Taylor, instead of challenging me, tries a very sneaky deflection.
A quick BLAST search should resolve this as the NLS sequence in the COVID spike is from aa residue 682 to 685.
This gets into bioinformatics. BLAST is a search engine of gene and protein sequences, which allows people to quickly find matching sequences – OR TO MISS THEM.
For sensitive operations, I simply don’t trust BLAST. It’s like Google. It’s a great place to look if you’re willing to throw your cares onto somebody else’s software, but it’s easy to miss things.
The SNEAKY move by Taylor is to MISLEAD me away from PRRARSV into a BAD SEARCH. The suggestion is to use an overly broad search of only 4 amino acids (682-683-684-685). Sorry, Charlie. No dice. I am interested in exactly what I said – PRRARSV – seven amino acids.
Instead, I decided to look for the sequences of the vaccines, and then use simple tools to check for the presence of the PRRARSV signal in them.
To begin with, note that there are TWO kinds of sequences I can potentially get for the vaccines.
the actual sequences, obtained by analyzing the vaccines
the “official” sequences, released by Pfizer and Moderna, the FDA, or somebody else
I tried to get official versions, but simply could not find them. So I found a link in the broader discussion of the results which Murakami was looking at.
The first thing you will note is that this is not likely to contain PRRARSV in it, because it’s all G, T, C, and A, like GATTACA.
This code needs to be translated from DNA/RNA to AMINO ACID, and for that, I need TEXT – not an image. So I looked for a different GitHub upload of the data, with text instead of images, and I found one.
Plugging in the sequences from the paper on GitHub, it’s straightforward. Here are the two vaccines, translated to amino acids, as both images and text.
In each vaccine, there is one and only one instance of the full PRRARSV nuclear translocation signal mentioned by Mehedi, which I have marked in BOLD.
So what does all this mean?
This means that there is no question – the same nuclear translocation signal which gets natural spike protein into the cell nucleus, and natural spike protein messenger RNA into the nucleus, BOTH as demonstrated by Mehedi, is in the vaccine spike proteins.
Do I have to spell it out any more than that? Are the members of the Pfizer Defense Legion so incurious as to what this might mean, that they have to fight the obvious truth every step of the way?
Watch what happens next.
Thank you. You prompted me to do the work. The full nuclear translocation signal (PRRARSV) cited by @masfique appears to be intact in both the actual Pfizer and Moderna sequences. Here is Pfizer.
Taylor’s response was interesting, and I didn’t expect it.
Wonder if the inactivated binding side negates this as it doesn’t allow the vaccine spike to be taken up by the cell. But thank you for doing your due diligence, this is good information
This response actually set me up to explain why the binding site issue is largely irrelevant. First my reply, then the explanation.
Thanks! Even assuming that cell surface binding/entry inactivation reduces direct secondary toxicity of the vaccine-produced spike to new cells, the NTS still means that primary genotoxicity of the Ψ-mRNA+spike may occur for any cell affected by LNP-enabled uptake of Ψ-mRNA.
TRANSLATION: Even if the vaccine-produced spike protein is “inactivated” toward some unspecified binding interaction in some unspecified way [which is contrary to the use of the largely unchanged full spike protein for immunogenic reasons, but let’s just ignore that point], so that the spike does not engage in some alleged “binding” in some way [I provide a plausible example], it doesn’t mean that the spike is not doing exactly what the viral spike has been proven to do, in terms of getting into the cell nucleus, AND bringing in its own mRNA at the same time.
Twitter’s character limits forced me to make that reply too jargon-filled for most, and possibly even for Taylor, who seemed not to have understood the full life cycle of the vaccine.
Allow me to explain in even more detail what I said, which was designed to clarify the issue for Taylor.
Let’s assume that the vaccine spike is somehow “inactivated” in its interaction with cell surface receptors. This would mean that new vaccine spike created by cells, would not interact with new cells in the same way as new disease spike protein, whether that spike was alone or part of a virus particle. I refer to that as “secondary toxicity”.
What I’m pointing out is that this is irrelevant to a “primary” toxicity concern – in fact a “genotoxicity”. This is the risk that spike protein produced in a cell, due to that cell ingesting a lipid nanoparticle of vaccine, might then get into the nucleus, and change the nature of that cell in a more fundamental way.
Now it is understood that the vaccine is “supposed to” lead to the death of infected cells, when those cells produce a bunch of spike protein, and are attacked by the immune system. The problem is that this doesn’t always happen, and indeed may not even be the primary fate of cells which take in the vaccine nanoparticles. What happens if the bell curve of vaccine intake creates a large number of cells which are damaged but not dead – which are not cleaned up by the immune system – and which have injured nuclei? There are lots of ways for things to go wrong.
What I am basically saying is that if the Mehedi results apply to vaccinated cells that are not cleaned up, we have a “bad cell problem”, and the problem isn’t just the spike – it’s in the nucleus. The cell’s problems have just become more “permanent”.
And that’s where things are. That fight is over, but I’m fighting over the De Marinis paper on another part of Twitter. That one is interesting, too.
STAY TUNED FOR MORE.
W
Title: CAREY TREATMENT, THE ¥ Pers: COBURN, JAMES / AUBREY, SKYE ¥ Year: 1972 ¥ Dir: EDWARDS, BLAKE ¥ Ref: CAR019AF ¥ Credit: [ MGM / THE KOBAL COLLECTION ]
RDS in the following comment points out one of the problems we have in waking up the Sheeple. There are highly ‘respected’ doctors and PhDs, who write papers in prestigious journals backing the mRNA vaccines even though they KNOW they are unsafe.
Wolf Moon OMG, this article below is a must-read. Linked from an AMA EdHub email one received today. It’s a JAMA piece written by Dr. Peter Marks — he’s the head of the CBER department of the FDA (Center for Biologics Evaluation and Research). Dr. Marks was in on the ground floor of Operation Warp Speed. Dr. Marks KNOWS EVERY DATA PIECE SUBMITTED TO THE FDA FROM PFIZER-BIONTECH ABOUT THE CLINICAL TRIALS FOR BNT162b2 BACK IN 2020 — AND EVERY DATA PIECE SINCE THEN ALSO. Dr. Marks was in on recommending that the FDA authorize the UNPROVEN, ONLY TESTED ON 8 MICE new “COVID-19 + Omicron BA.4 + Omicron BA.5 booster shot.” His linked article below is a screed for the development of “new” and “different types” of COVID-19 “vaccines” — including ones that specifically target the T-cell response in the body. Dr. Marks KNEW that the “vaccines” developed during Operation Warp Speed and given quick EUAs by the FDA WOULDN’T DO THE JOB: From his article: “One potential model for approaching such development [of a COVID-19 vaccine] was used successfully at the beginning of the pandemic when Operation Warp Speed evaluated numerous global vaccine types and focused on advancing several promising candidates, knowing full well that most would ultimately not be found to meet the criteria set forth for a safe vaccine with adequate efficacy.” (bolding and Italics mine) Dr. Marks represents the “medical establishment” and DeepState. IMO, the “medical establishment” and the DeepState have it as their business to continue to put these dangerous COVID-19 “vaccines” into people — and develop new “vaccines” to keep damaging / destroying the immune systems of those who take them. His article: https://jamanetwork.com/journals/jama/fullarticle/2799600 December 9, 2022 “Urgent Need for Next-Generation COVID-19 Vaccines” Peter Marks, MD, PhD https://www.youtube.com/watch?v=Nat1za4sKjA As an additional note. For those who might wish to watch the documentary it is available to watch free until the end of January. All that is required is your email I think. The link follows. https://therealanthonyfaucimovie.com/trailer/
In addition to censorship and smearing of dissenting voices, hospitals and doctors were getting the carrot and stick treatment – Lose your license OR getbig bucks for pushing bogus PCR tests, ventilators, Remdesivir and killing patients. – For example “A COVID-19 diagnosis provides extra payments to coroners!”
To make sure the Sheeple could not make a solid connection between the Covid Vaccine and death, the shot is a slow ‘poison’ with a variety of adverse reactions.
The CDC has been hiding the Social Security Administration death master file. I got it from a whistleblower. This shows deaths are taking 5 months from the jab to happen. This is why it’s hard to see.
Remember this time factor as we look at the data I found.
Finally we have the DELIBERATELY compromised VAERS system that is SUPPOSED to alert the CDC and FDA to harmful drugs.
There are major problems with the vaccine adverse event reporting system (known as VAERS) which the CDC considers the “front line” of vaccine safety. VAERS was created in 1990 by the CDC and FDA as a means to collect and analyze adverse effects that are associated with vaccines. Unfortunately, the failings of VAERS are “kept from the consciousness” not only of the public, but also from the doctors, pediatricians, and nurses that the public rely on to provide reliable information as to the safety of vaccines. I say “kept from the consciousness” rather than “kept secret” because while these failings are publicly disclosed for all the world to see, they are for all intents and purposes BURIED in documents seldom searched out by the average member of the medical community, much less by the average individual. You could say that the information has been very effectively hidden in plain sight…
In 2000, the 6th Report by the Committee on Government Reform addressed the failings of VAERS in its address of the Vaccine Injury Compensation Program…. [The] Congressional report notes (on page 15), “Former FDA commissioner David A. Kessler has estimated that VAERS reports currently represent only a fraction of the serious adverse events.” (emphasis by author)… That leads us to the interesting case of the CDC and Harvard Pilgrim Healthcare Inc.
The Department of Health and Human Services (HHS) gave Harvard Medical School a $1 million dollar grant to track VAERS reporting at Harvard Pilgrim Healthcare for 3 years and to create an automated reporting system which would revolutionize the VAERS reporting system- transforming it from “passive” to “active.”…
I’ll quote the findings directly from the report,
“Adverse events from drugs and vaccines are common, but underreported. […] Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of ‘problem’ drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed.”
Again, let’s stop and think about this revelation for a moment: fewer than 1% of vaccine adverse events are reported. The CDC’s entire vaccination propaganda campaign rests on their claim that side effects from vaccination are exceedingly rare (and predominantly minor).According to the CDC, in 2016 alone, VAERS received 59,117 vaccine adverse event reports. Among those reports were 432 deaths, 1,091 permanent disabilities, 4,132 hospitalizations, and 10,274 emergency room visits. What if these numbers actually represent less than 1% of the total as this report asserts? Simple multiplication would yield vaccine adverse events reports numbering 5,911,700!…
the United States of America Centers for Disease Control ghosted Harvard Pilgrim Healthcare, Inc.
“the practice of ending a personal relationship by suddenly and without explanation withdrawing from all communication.”
Personally, I would hope that I could hold an organization like the CDC to a higher standard, but… After a one million dollar grant was paid and three years of research conducted on what appeared to be a very successful upgrade to the passive VAERS system, the team’s CDC contacts went MIA
. The ESP:VAERS final report states, “Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.”
So in 2017, the CDC DELIBERATELY left a useless reporting system in place when they had the opportunity to upgrade it.
Since the VAERS data set is compromised as well as next to useless, I decided to see if we could find another way to connect the mRNA vaccines to deaths. There is a nifty site called Dead or Kicking.
there is the graph “United States death comparison by age in 2020“
By changing the date in the URL you get the different years AND if you place your mouse over the graph, it will give you Deaths, Death Rate and Population for each age group.
You can save the graphs for any year – or all of them – as examples, as Wolf did below. Right-clicking on a graph lets you “save image as” or “copy image”.
2019
2020
2021
2022
Note Added By Wolf – CHECK THIS ONE OUT!!!
I originally thought I would see a major drop in the population over 75 but that did not happen since the Baby Boomer cohort is filling the 65+ age groups faster than the orchestrated depopulation can kill them. Notice there are less people in the 45 to 54 age group than in the 55-64 age group. That is a REAL PROBLEM for the Cabal.
…The Social Security Trust Fund should currently have $2.5 trillion in surplus. So how is it that these checks could stop being issued if the debt ceiling isn’t raised? Economics professor Dr. Allen Smith, author of The Looting of Social Security: How The Government is Draining America’s Retirement Account, has been reporting on the theft of Social Security funds for years….
Age / Date
2019
2020
2021
2022
85+
6,604,958
6,628,013
6,673,175
6,715,875
75-84
15,969,872
16,022,410
16,139,651
16,250,631
65-74
31,483,433
31,571,207
31,773,610
31,970,852
55-64
42,448,537
42,643,579
42,929,850
43,208,648
45-54
40,874,902
41,050,404
41,371,452
41,683,591
So I created another table this time of USA Death Rates by age group by year. I included 6 years before covid as a baseline. Then the two years, 2019 & 2020, when Covid hit the USA plus the two years, 2021 and 2022 when the mRNA vaccine was progressively rolled out, starting with adults, then school age children and finally babies.
Also there was the DELIBERATE mis-diagnosis of flu and pneumonia followed by refusal to treat until the person was so sick they needed to be put on a ventilator & remdesivir thus killing up to 88% of those patients.
The result of all of this, is the most vulnerable elderly had already been killed off in 2020 as the much higher death rates for 2020 shows, but by 2021 and 2022 the death rates decrease from that high. Although the elderly were vaccinated, unlike athletes and younger, physically active people, the elderly are going to be a lot more sensitive to what their bodies are telling them and NOT pushing it. They are also more likely to have doctors checking their heart health and be on heart and circulatory medications.
Myocarditis is an important cause of arrhythmias and sudden cardiac death (SCD) in both physically active individuals and athletes.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
RETIREES 65 to 74
The 65 to 74 group is going to be a mixed bag. Compared to the 75+ group they are less likely to be in a nursing home or to have gotten deathly ill in 2020, although a certain percentage will have died. However they are likely to get the vaccine. Thanks to Medicare, they are more likely to be in contact with medical professionals who would try to talk them into the jab. They are also going to be a lot more physically active than older retirees and therefore stressing their hearts more after getting the mRNA vaccine.
You can see the combination of poor health care in 2020 followed by the vaccines and then boosters as the death rate increases year by year from 2019 through 2022.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
FORCED RETIREMENT/SMALL BUSINESS WORKERS 45 to 64
The 45 to 64 are an interesting group. Corporations force retirements and actively discriminate against those 45 years and up because age discrimination laws have no real teeth. Therefore the people 45 and up are most likely NOT working for ‘Corporate America’ and are either small business people or hired by small business people. (BTDT) This group is the most likely to have had a ‘rude awaking’ about the world we live in and are NOT going to be as trusting. Older people are also more likely to tell their boss to go F..K themselves with the darn needle. Like the 65 to 75 group you can see the increase in death rate year to year but it is not as sharp an increase. They are also more likely to be in better health than retirees. If You’re Over 50, Chances Are the Decision to Leave a Job Won’t be Yours Age discrimination in the workplace happening to people as young as 45: study
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
WORKING AGE CORPORATE AMERICA 15 TO 44
The age group 15 to 44 is the group most likely to show PURE UNADULTRATED DATA about Mortality & the mRNA vaccine although there may be some confounding from drug use increasing over the years. Covid-19 virus has little effect on the death rate in 2020. However as the boosters and the 5 month time delay kicks in you can see the death rate almost doubled in 2022 compared to 2019 and earlier.
….Scott Davison, the CEO of OneAmerica, a $100 billion life insurance and retirement company headquartered in Indianapolis.
“The data is consistent across every player in the business.”
Davison said death rates among working age people –
those 18 to 64-years-old – are up 40 percent in the third and fourth quarter of 2021 over pre-pandemic levels.
“Just to give you an idea of how bad that is, a three sigma or 200-year catastrophe would be a 10 percent increase over pre-pandemic levels,” Davison said. “So, 40 percent is just unheard of.”
He blames it on Covid instead of the mRNA vaccine of course. “…the third and fourth quarter of 2021…” would be after Steve Kirsch’s 5 month window. So far I can not find any 2022 insurance data. HMMMmmmm
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
CONTROL GROUP 1 TO 14
The 1 year to 14 can be considered the ‘Control Group’ Covid has little if any effect on the death rate in 2020. They were not vaxed until quite recently (November 2021) and boosters were not approved until May 19, 2022. The death rate so far has been flat but I would expect an uptick after the first of this year as the effects of the boosters kick in.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
BABIES UNDER 1 YEAR
The Under one year of age is interesting since there is actually a slight dip in mortality. Are weaker babies more subject to spontaneous aborting after Mom is vaxed?
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
TIMELINE of Emergency Use Authorization of mRNA VACCINES
The FDA makes it VERY HARD to figure out just when they authorized the use of the mRNA vaccine in youngsters. I gleaned out the following dates. Starting from the FDA Covid Vaccine site.
Turns out it is the CDC who has the final say on vaccination of children so I have also included the CDC news releases.
12/18/2020 – EUA issued for the Moderna COVID-19 Vaccine, December 18, 2020. Emergency Use Authorization (EUA) of the Moderna Inc. COVID-19 Vaccine for the prevention of COVID-19 in individuals 18 years and older.
YEAR 2021
06/10/2021 — Vaccines and Related Biological Products Advisory Committee will meet in open session to discuss, in general, data needed to support authorization and/or licensure of COVID-19 vaccines for use in pediatric populations.
FDA DEFINES: Pediatric use. (A) Pediatric population(s)/pediatric patient(s): For the purposes of paragraphs (c)(9)(iv)(B) through (c)(9)(iv)(H) of this section, the terms pediatric population(s) and pediatric patient(s) are defined as the pediatric age group, from birth to 16 years, including age groups often called neonates, infants, children, and adolescents.
. 09/17/2021 — Application for administration of a third (“booster”) dose of Comirnaty (COVID-19 Vaccine, mRNA) in individuals 16 years of age and older.
10/26/2021 — Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss a request to amend Pfizer-BioNTech’s Emergency Use Authorization (EUA) for administration of their COVID-19 mRNA vaccine to children 5 through 11 years of age.
10/14/2021 – Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss the Emergency Use Authorization (EUA) of the ModernaTX Inc. COVID-19 vaccine and the Janssen Biotech Inc. COVID-19 vaccine for the administration of an additional dose, or “booster” dose, following completion of the primary series, to individuals 18 years of age and older.
Today, CDC Director Rochelle P. Walensky, M.D., M.P.H., endorsed the CDC Advisory Committee on Immunization Practices’ (ACIP) recommendation thatchildren 5 to 11 years oldbe vaccinated against COVID-19 with the Pfizer-BioNTech pediatric vaccine. CDC now expands vaccine recommendations to about 28 million children in the United States in this age group and allows providers to begin vaccinating them as soon as possible.
The Food and Drug Administration today authorized Moderna’s COVID-19 vaccine for children aged 6 months through 17 years old and Pfizer’s COVID-19 vaccine for children aged 6 months through 4 years old, as recommended this week by its vaccine advisory committee. The vaccines previously were authorized for older children.
Before vaccinations can begin, the Centers for Disease Control and Prevention must recommend the vaccines for these age groups. CDC’s Advisory Committee on Immunization Practices is scheduled to vote tomorrow on whether to authorize the vaccines for children age 5 and under.
Children 6 months through 5 years of age who received the original (monovalent) Moderna COVID-19 Vaccine are now eligible to receive a single booster of the updated (bivalent) Moderna COVID-19 Vaccine two months after completing a primary series with the monovalent Moderna COVID-19 Vaccine.
Following today’s meeting of the Advisory Committee on Immunization Practices’ (ACIP), CDC is expanding eligibility of COVID-19 vaccine booster doses to everyone 5 years of age and older. CDC now recommends that children ages 5 through 11 years should receive a booster shot 5 months after their initial Pfizer-BioNTech vaccination series.
TL;DR – Watch this sucker while ignoring the myopic neo-Bolshevik “refugee” propaganda, but instead keeping in mind the current COVID/WEF insanity, to get a grip on the incipient climate-excused holocaust of the depopulationists, which is the fault of SOCIALISM, same as the soon-to-be-dwarfed “Holocaust” of the 1930s and 1940s.
OK – just a bit more detail…..
Don’t watch the Ken Burns Holocaust special for any of the slanted, leftist, socialist messaging stapled onto the historical facts in a DNC-approved and ADL-edited way.
Watch this PBS special while subversively keeping in mind the new socialist, depopulationist, eco-nuttery holocaust which now exceeds 6 million COVID dead and will soon DWARF the old “Holocaust” of so much hypocritical and self-centered angst.
Calmly stroke Suspicious Cat, as the Holocaust is falsely linked to rejection of current “asylum seekers” in a face-palmingly stereotypical and Trump-hating way.
Watch this PBS special while “rebelliously” remembering that RIGHT NOW we are in a DESIGNED CRASH of the world economy, which will kill BILLIONS of innocent people if not stopped – and which is largely driven with the eager participation of globalist and socialist “Jazis” – who are no less evil than the Nazis of old – self-righteous in their “ESG/DEI” zeal, with their vain self-assurance that they and they alone know the answers which must be forced upon the world.
Watch this special remembering Andrew Cuomo, Anthony Fauci, Ralph Baric, Joe Biden, WEF, Klaus Schwab, Pfizer, CCP and Albert Bourla, and keeping close in mind, the NEW holocaust which has already killed over 6 million worldwide by the virus ALONE, and is already creating even-more-massive excesses in mortality in every country, in unacknowledged proportion to acceptance of the “vaccines”.
Watch this PBS propaganda special while remembering how the US and China co-created biological “gain of function” which literally DWARFS the mere chemical nastiness of a bug spray, “Zyklon B”, itself more comparable to Fauci’s murderous remdesivir, or the midazolam they apparently used for “COVID euthanasia” in the UK.
Watch this special while remembering the millions who died around the world from both virus and vaccines, including tens of thousands of Israelis, as secular Jewish leaders condemned their own and didn’t lift a finger, other than to censor Zev Zelenko, and to suppress their own report on the dangers of the vaccines they INVESTED IN.
Watch this special in strict analogy of the THEN unbelievability of the “final solution”, to the NOW unbelievability of “depopulation”.
Realize that the problem isn’t antisemitism or “refugee acceptance” – it’s SOCIALISM.
SOCIALISM KILLS – no matter which brand.
Representative Alexandria Ocasio-Cortez (D-NY) and Senator Ed Markey (D-MA) were joined by Democratic lawmakers from both the House and Senate on February 7, 2019, to introduce Green New Deal legislation.
Oh, hell. I said enough already. Do I really need to explain this?
If so, I’ll do it in the comments.
But the bottom line is that this special has a lot of great facts, which – if you are prepared to see them in the context of current events – are quite convincing that we ARE in the late beginning of yet another socialist holocaust.
I had already seen the video I’m about to show you, when I watched the press conference in which Florida Governor Ron DeSantis powerfully chastised the media for mischaracterizing his administration’s position of OPPOSING the mRNA vaccines for kids, as PROHIBITING the vaccines for kids – something which DeSantis reminded the idiot media that he cannot do.
However, DeSantis didn’t “hide” his opposition in the least. He still seemed to be doing everything in his power to get parents to look at Pfizer’s clinical trial data (or lack thereof) allegedly justifying this needless – if not counterproductive – if not downright dangerous vaccine.
Thus, when I saw how STRONGLY DeSantis held his ground, I thanked God that somebody in his administration surely saw the same video that I had seen.
YOU NEED TO SEE IT, TOO.
Just watch this. It’s short and to the point.
BOMBSHELL: Dr. Clare Craig Exposes How Pfizer Twisted Their Clinical Trial Data for Young Children
Gov. Ron DeSantis clarifies Florida's position on COVID shots for children, saying he's not surprised that the White House would lie and legacy media amplify it.
He adds countries with similar approaches to Florida "have been right on COVID way more than Fauci and his crew." pic.twitter.com/biRQf9Es2z
— The Post Millennial (@TPostMillennial) June 20, 2022
Twitter will try to remove this tweet from the historical record, so let’s just make a copy.
In my opinion, this Pfizer clinical trial is nearly 100% BAD SCIENCE.
That such bad science is not merely allowed to pass without comment by America’s major scientific organizations, such as the AMA and the ACS, but was in fact used by the FDA to approve utterly needless vaccines – this kind of failure of American science is SOUL-DEADENING.
It’s not just one person here or a research group there. This is multiplicity of large-group institutional failure.
Personally, I blame this shocking failure on the triumph of Chinese ethics over traditional Western ethics.
Pfizer, with its global HQ for clinical trial data in Wuhan (SURPRISE, SURPRISE, SURPRISE!) is now allowing China and the CCP to effectively run all its clinical trials. This horrible, shoddy trial just REEKS of a sick combination of malignant Chinese battered anarcho-capitalism and corrupt Chinese communism. This is typical “top down” forcing of mistakes due to POLITICS and GREED.
I have been telling people that I will NEVER take another drug from Pfizer.