
A continuation of Dear DePat’s Tuesday Open Thread
A call for weekly open-thread authors on Tuesday and Thursday
A discussion of various pathological possibilities, including some new ones, and an explanation of why I lean toward particular theories
First of all, the boilerplate.
By reference, I call to incorporate the rules spoken of in any of Deplorable Patriot’s recent posts, such as her final one.
With that settled, I jump to the second item on the agenda.
A call for weekly open-thread authors on Tuesday and Thursday.
I know this seems abrupt, but DePat’s obituary has already published, and I’m already going to talk about even more sensitive topics now – by request – so I don’t feel too much guilt in making sure that DePat’s MISSION of keeping this site running is fully taken care of.
The best thing that we can do, in my opinion, to maintain Susie’s legacy in the MAGA world, is to keep all of her posts here (just under 1000 of them) online and searchable. SO – we need new authors for Tuesday and Thursday, to keep this site running.
Gudthots is thinking about taking over Thursday.
Do we have anybody else, who would like to do Tuesday? Which means that the post goes up Monday night, scheduled for one minute after midnight (I can help with this).
Just to be clear to potential authors, these daily threads are YOUR BABIES – meaning they don’t have to be anything like the way that DePat did them. In fact, it’s probably better not to. I invite new authors to come up with their own new styles.
We do have a very thin guideline post of basics in the sidebar, shown here:
We were actually more rigorous about format then, but it does help that daily open posts publish on the day listed in the title, and that the titles have a searchable format.
Anyway, if you are interested, just leave a comment.
If you are shy about saying something, you can always do “PMTW” (see “Contact”), commenting on this post, and then I can respond anonymously in public, although I recommend just being open.
Looking forward to somebody picking up DePat’s second sword.

And now for the big item.
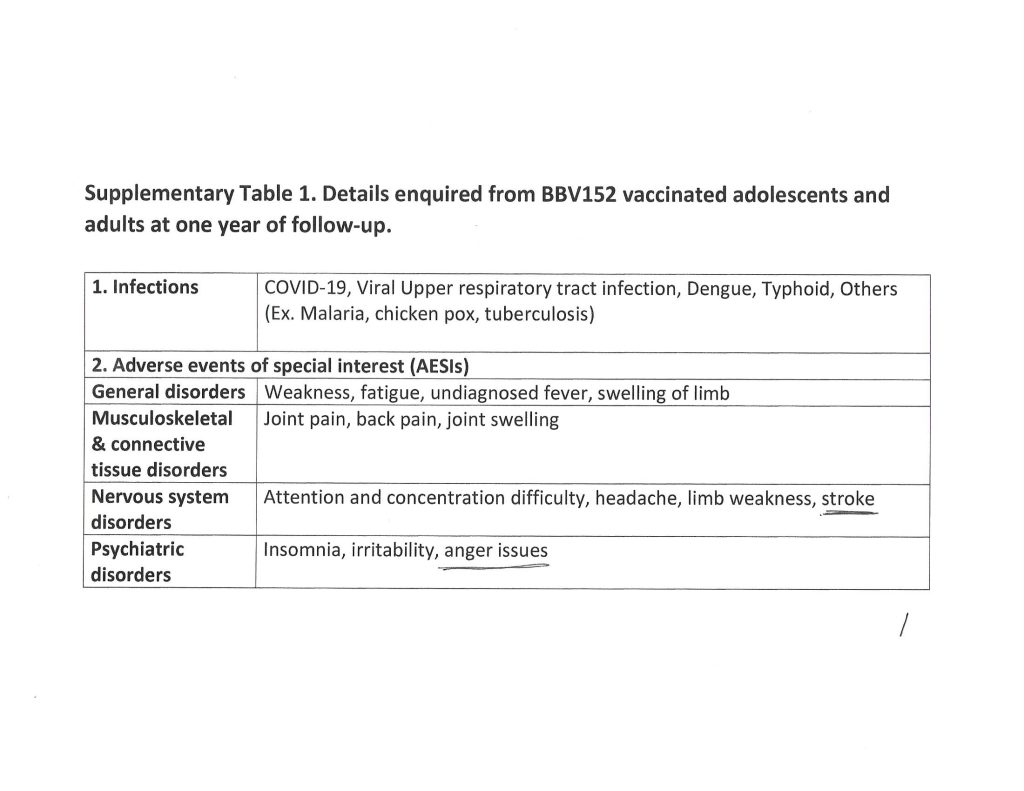
A discussion of various pathological possibilities, including some new ones, and an explanation of why I lean toward particular theories.
I begin by citing relevant portions of FG&C’s report on the “sudden and unexpected” passing of Susie, which he communicated to me privately.
7-8 weeks ago Susie attended a choir rehearsal, during which she had stood right next to a fellow choir member who she learned afterwards had been Covid vax-boosted for the 4th time that day. Perhaps she mentioned at some point in these pages that in the time since that night she believed she had contracted “long Covid”, experiencing physical weakness, insomnia, a persistent cough, and low appetite. She believed she had inhaled “spike proteins” shedding from the woman she stood next to that night at rehearsal, stating that had she known the woman had been so recently vaxxed she would never have gotten so close to her.
Recently, she had stated she was feeling better, the cough all but gone, and in the past week felt she had gotten over the insomnia hump and was getting good rest. I was optimistic. However, on Monday AM….inauguration day….her brother discovered her in her bedroom, unresponsive, after becoming concerned he had not heard her moving about and she had not come downstairs. Paramedics were subsequently unable to resuscitate her, and it is currently believed she suffered a heart attack and passed away in her sleep. After many attempts to reach her (we texted daily), her brother called me this afternoon with the news. I knew you would want to know as well.
I am going to tease this apart very gently, so that you can see all the possibilities that we’re actually dealing with.
Point 1 – “Shedding”
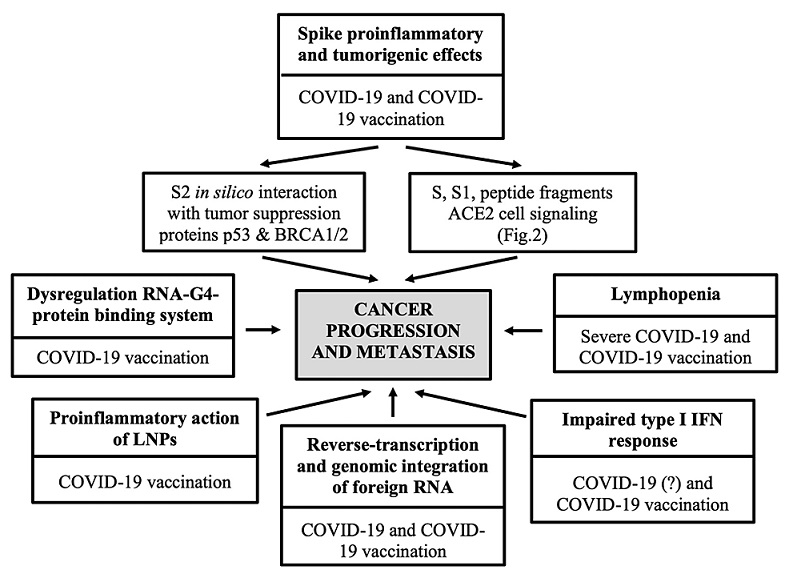
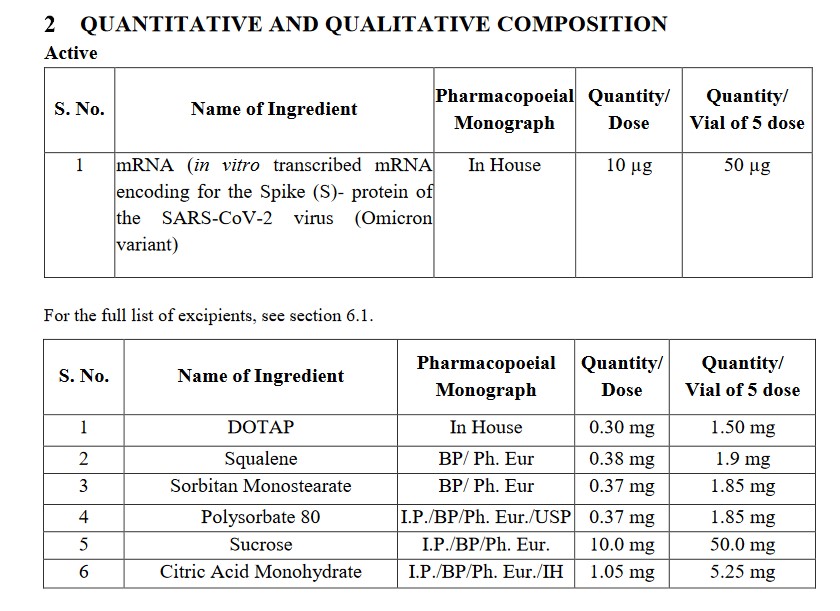
Now, if you were following along with DePat’s posts in recent weeks, then you realize that she was very convinced that she had been subject to shedding of [COVID-19 vaccine-created] spike protein.
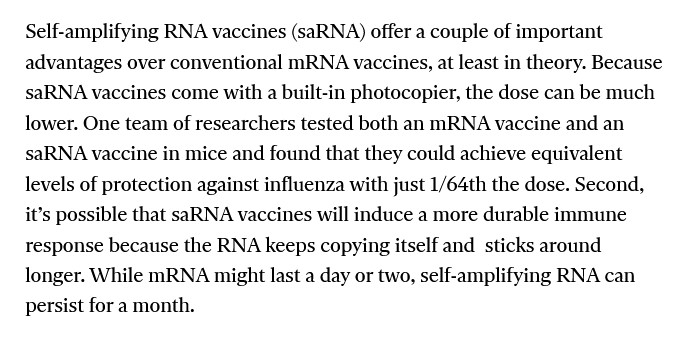
The first problem there, is that very near the end, DePat realized that the vaccine-originated shedding would more likely have been the spike mRNA, not the spike protein.
Here is her comment, which was in fact her third-to-last, made on January 17, 2025.
https://www.midwesterndoctor.com/p/covid-19-vaccine-shedding-experiences “What We’ve Learned from Over a Thousand Vaccine Shedding Reports”, by A Midwestern Doctor, 7 January 2024 (detailing the phenomenon of COVID-19 “vaccine” shedding, and how such shedding affects people);
This one is particularly scary as it claims the shedding is due to mRNA and not the spike protein. Drat.
Does anyone have further evidence on this or a rebuttal? I always thought it was just the spike protein. So far, no heart issues or unexplained pain, true brain fog (I’m sleepy today as the insomnia is FINALLY subsiding. I slept a LOT in the last 24 hours.), or any of the other hard core stuff. A LOT of stiffness keeping warm, and the return of some relatively normal complaints for me in winter.
Fortunately, we haven’t given away the bulk of my mother’s tools she used for the last so many years of her life after the hip replacement, and subsequent ailments. They’ve come in handy. I have another friend who is helping me out in a lot of ways. The next week will be a challenge temperature wise and then I can at least sit in the front door and soak up radiant heat as the sun comes out. Less than a half hour is recommended.
I’ve decided to use this experience as part of writing about an elderly or disabled person. There’s too much challenge at this point to really articulate it, but this is for the birds even if the worst of it is fatigue.
And, yes, stay away from crowds and people you know who get boosters.
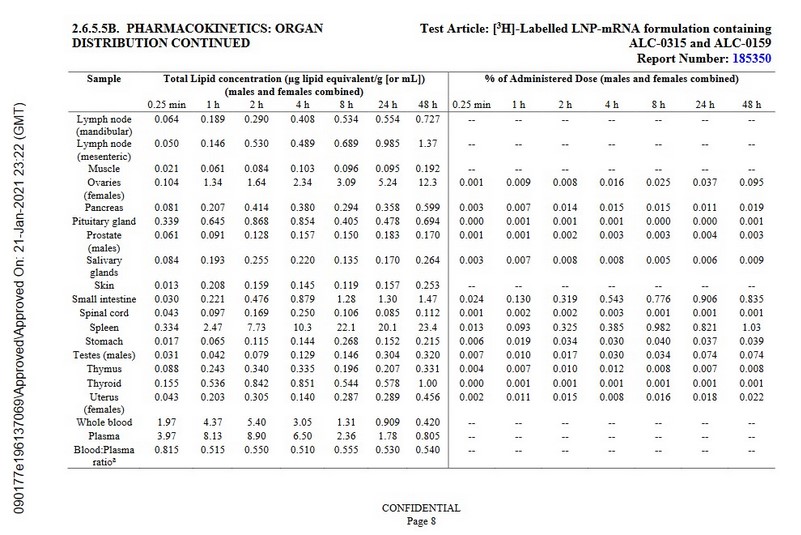
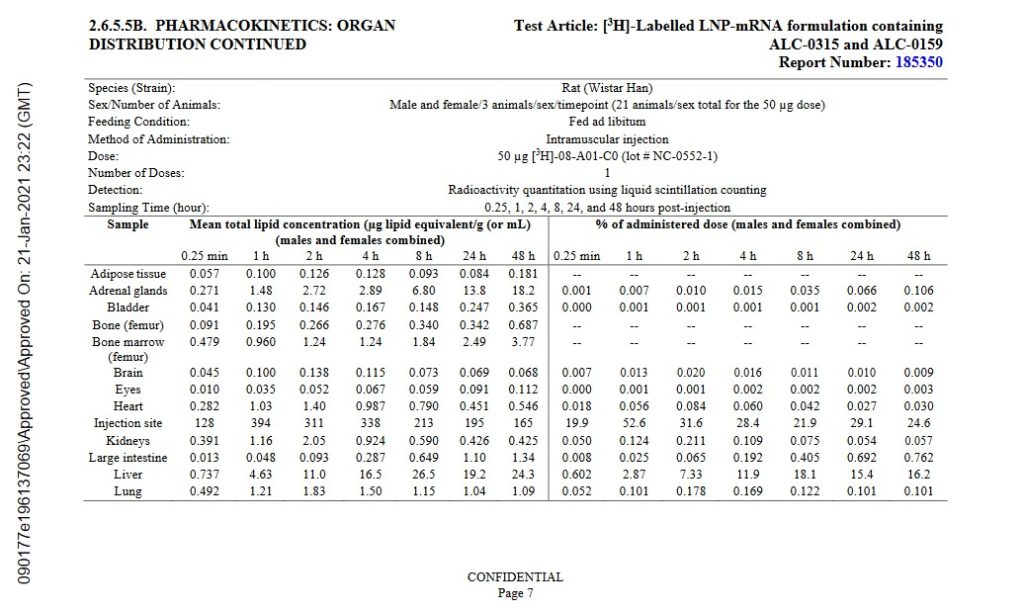
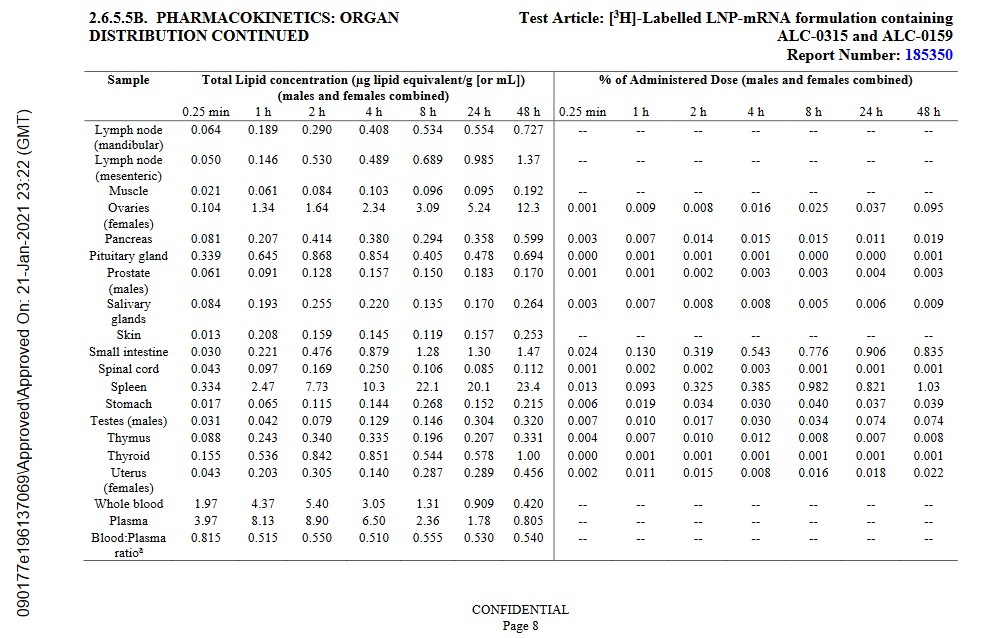
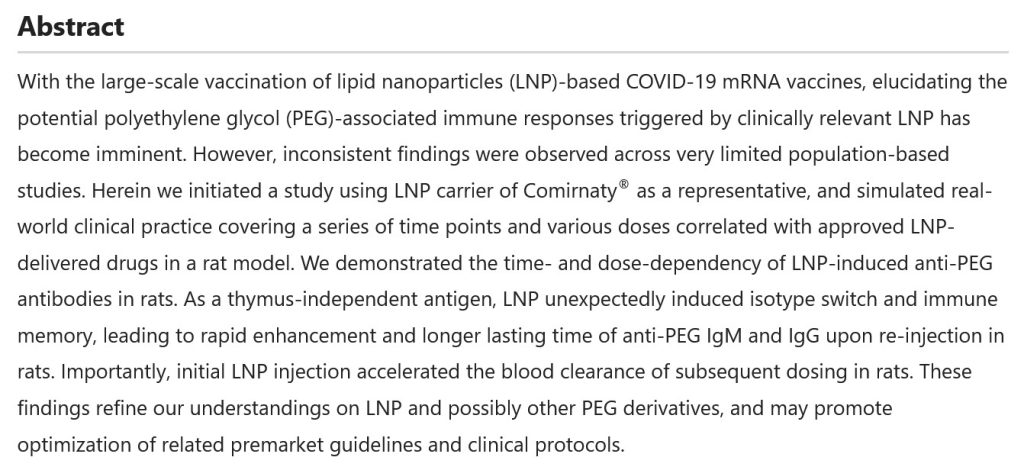
So – let me just spell this out. DePat realized that vaccine shedding could be the spike protein, but that it’s more likely (and more dangerously) to be the spike protein mRNA enclosed in lipid nanoparticles that can get into cells. It is by this mechanism that much more spike protein could be created in the body of the shedding recipient.
Not a pleasant thought.
Now – just a side note. DePat and I had discussed all this, many times, WAY BACK in late spring of 2021, so she knew this stuff years ago. Thus, I really believe that she had some brain fog recently. And we know from her comments – DePat understood that she had brain fog, too, despite the fact that it was interfering with her memory.
Years ago, she and I had speculated on the shedding of spike protein, to explain things which were being observed in people close to vaccine recipients. Unlike DePat, I was not a believer in “shedding”, but when Naomi Wolf started reporting observations consistent with some kind of shedding phenomenon, I came up with a scientifically solid explanation of how shed spike protein could actually cause such symptoms, if the spike protein had highly potent, oxytoxin-like pharmacological activities.
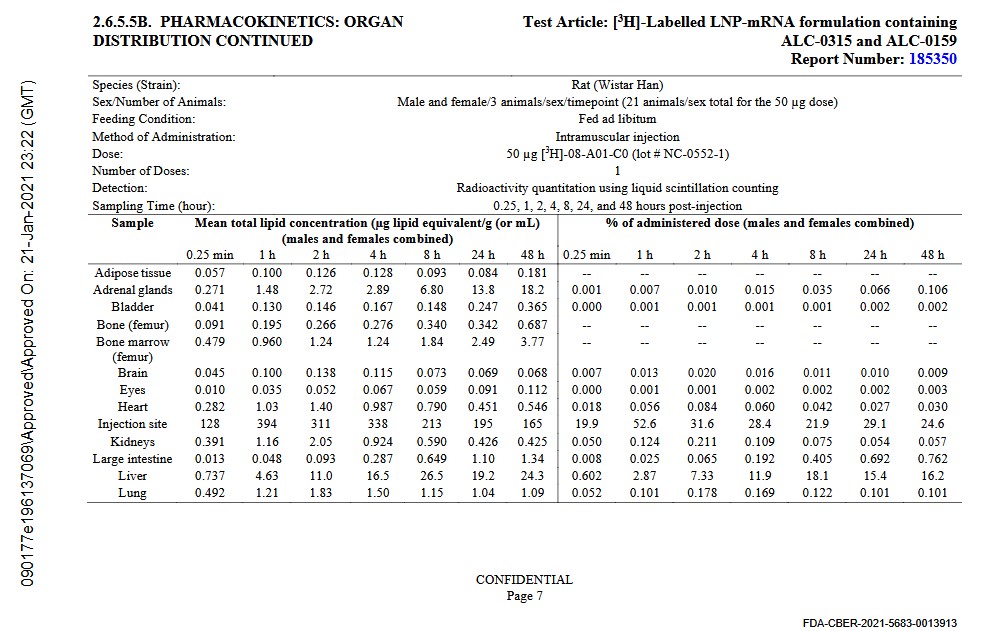
The idea of spike protein shedding seemed plausible AS IS, but when Pfizer’s own data, released to vaccine skeptics by the Japanese government, showed the vaccine itself persisting and migrating in test animals, it became clear that shedding of the VACCINE would be an even better explanation.
Which I posted about.
The point about snake venoms and spike protein is an ANALOGY – it’s not direct – but it’s very useful in understanding both potencies and pharmacological and pathological actions.
I want people to understand this. EVEN if it was just the spike protein being shed, if that protein is even slightly like snake venom in pathogenicity, then it behooves us to look at how snake venoms are dealt with in real life.
Specifically, when cages of venomous snakes are being cleaned, those present have to actually wear respirators. Not just masks – respirators. That is because the dust from dried snake venom in venomous snake cages can literally cause dangerous symptoms in people cleaning the cages.
SO – I want people to understand that DePat had a good theory here – namely, the theory that she got many lung-fulls of either spike protein, or (more dangerously) vaccine nanoparticles, from that vaccine-injected choirmate of hers.
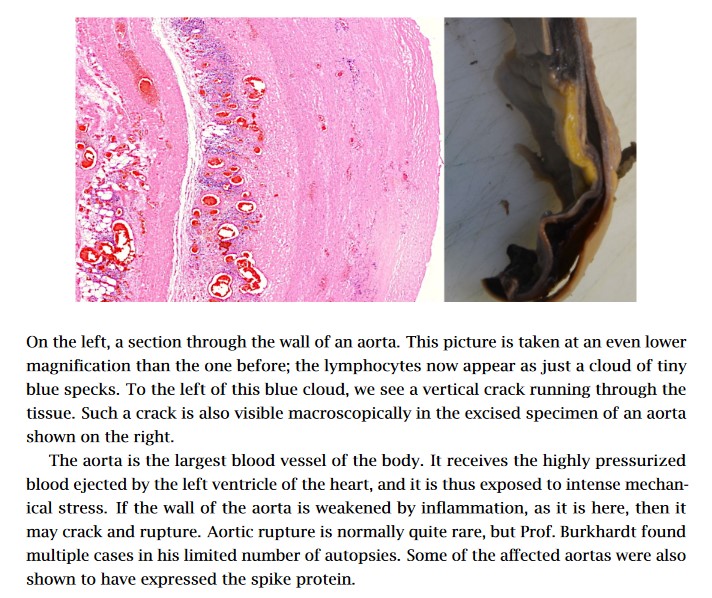
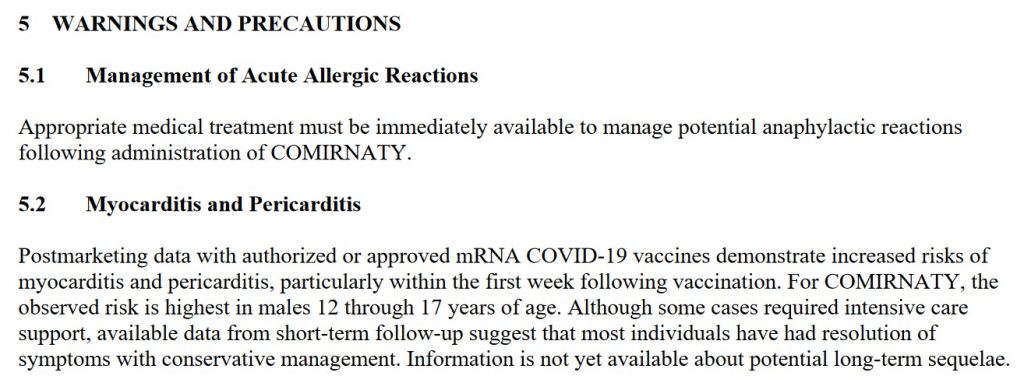
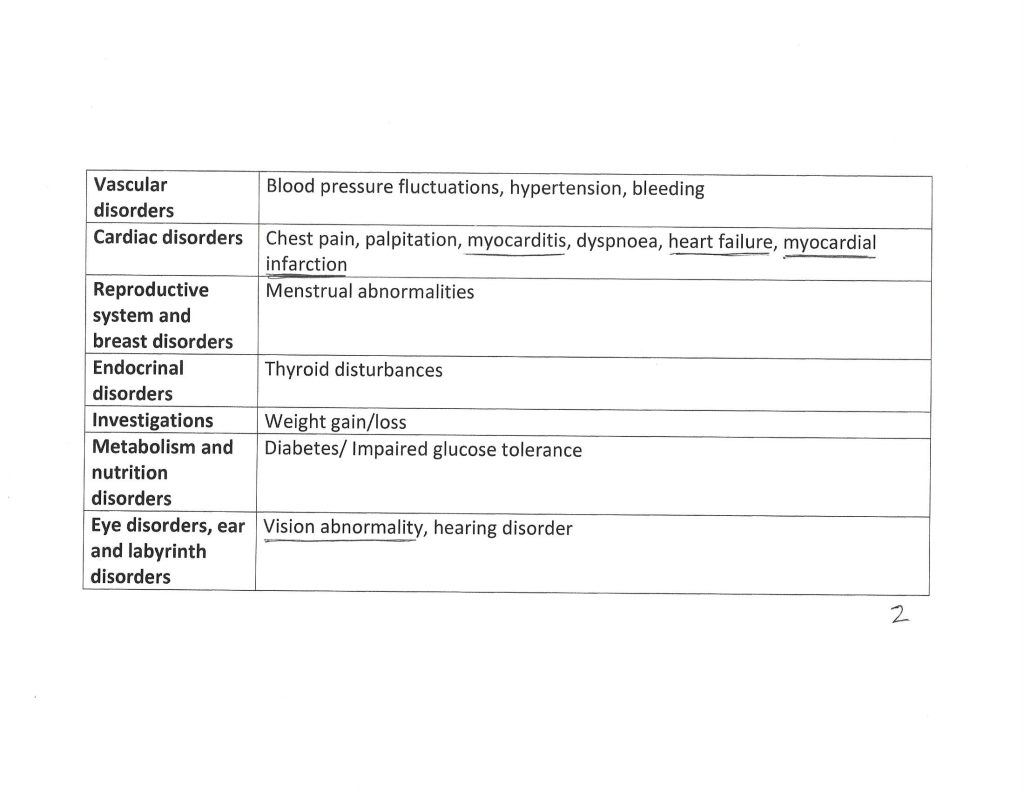
According to this theory, not only did the “shed” vaccine cause typical vaccine-related symptoms – it potentially caused myocarditis, aortal embolism, blood clots, or any one of the many serious cardiovascular events that the vaccines are capable of causing.
This is actually a really reasonable theory.
However, it’s not the only one.
Point 2 – Nicotine
DePat’s last post indicates that she was continuing to use nicotine patches as an off-label way to “inhibit spike protein”. Here is that post.
I’m trying, be sure of that.
Others in my family aren’t. They think this will all go away just with ivermectin. I’m not done with the nicotine protocol yet.
OK – so what is this “nicotine protocol”?
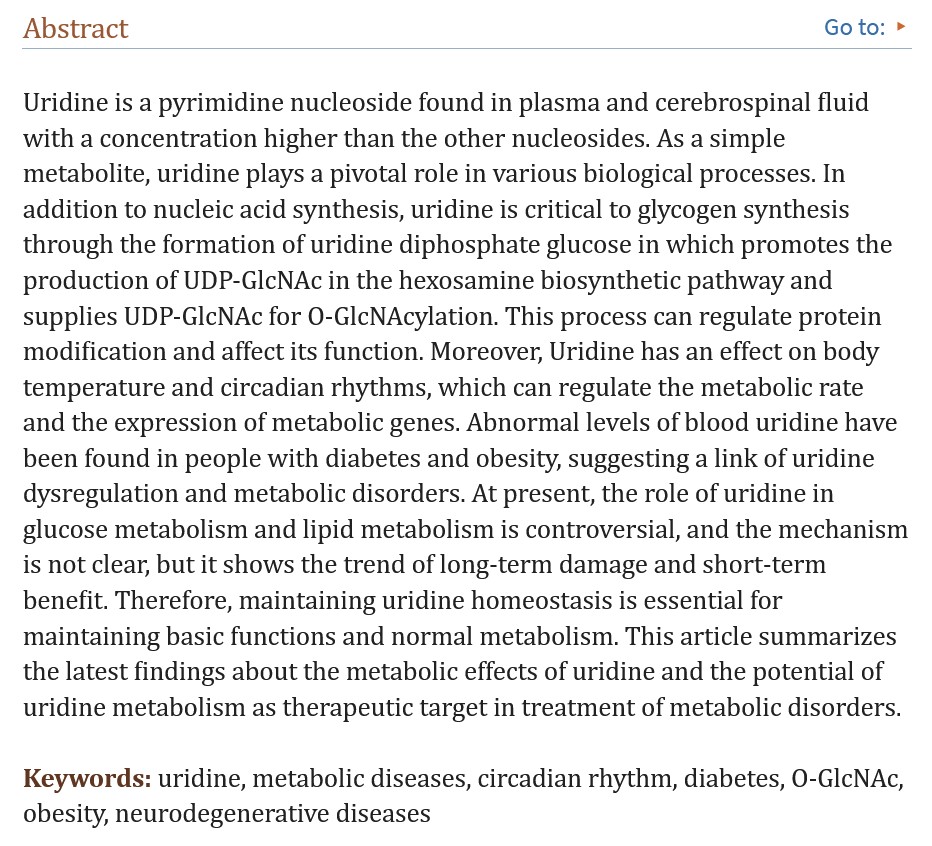
The TL;DR is that one of the alternative medical treatments for “spike protein” / “long COVID” – and particularly “brain fog” – is medicinal nicotine, either as chewing gum, patches, or sublingual.
But before I get into this treatment, it’s helpful to see when and where DePat began investigating nicotine as a solution to her ailment. The entire conversation is very instructive, and begins here, where DePat began asking all of us for suggestions about treatment of her condition.
Okay, I need to pick a few brains.
After talking over symptoms with a friend who is in the same boat as many of us are with the COVID shots – she didn’t take them, but her husband did and she’s now suffering with the side effects despite all sorts of alternative treatment – I think whatever this is that I have is related to a choir member getting a booster last month and exposing me. The fatigue symptoms pretty much match what she had. Just unloading and loading the dishwasher is a challenge. Forget actual housework which desperately needs to be done. (When the kids get here on Saturday, I’m using them to deck the halls.) This crap is for real.
Other than making a run for Tennessee, which really isn’t that bad of a drive from here, for Ivermectin, any ideas? My friend ordered me a nebulizer and is willing to help me use it to break up biofilm, etc., but is there anything in anyone’s arsenal of natural remedies that may help? I had a talk with our Lord and Savior at Eucharistic Adoration today, and I’m hoping my Novena for wellness is doing some good, but, really, I have a lot to do and no energy to do it. Just about every old injury has flared up – especially in my torso which are pretty much all from singing – and some other things.
I just want and need this to go away.
Any ideas?
Thanks.
P.S. please pray for a cousin, A, and her husband, K, who are suddenly expecting identical twins over the summer. it’s a CLASSIC case of you make plans, God laughs. They are in their late thirties, and their toddler was born via c-section due to pre-eclampsia. Fortunately, her OB services are through a Vanderbilt extension, so we’re all hoping for the best.
P.P.S. Next week, we are going to have a house full of people, so the posts will be placeholders of a sort. I’m going to resurrect an old one and draft something new for the day after Christmas. Just a head’s up.
Now, at that time, all of us came in with a wide variety of suggestions, but one late response came from a hitherto lurking account, I Hate Acronyms, now registered as Sigma.
Very long time lurker here from the great Q purge OT. Please consider nicotine patches. The highest strength, cut into fourths. Apply one of the fourths to your skin, replacing with a fresh one daily. Do a search on Rumble for “nicotine and spike proteins”. “Nicotine vs nanotech”
If they are going to work, you should see results within days, if not hours. Non-addictive.
As I felt this was earnest and helpful advice, and that the nicotine method had solid science behind it, I approved the comment immediately, hoping it might help DePat.
I am sure that DePat thoroughly investigated this, and found all the same information that I did. If you dig deep enough and far enough on this, you will find all of the following.
- there are valid scientific reasons to think nicotine might work as a treatment for “long COVID” / “long vax” / “spike protein”
- there is a wide range of voices supporting treatment with nicotine
- those voices include more “controversial” ones like Dr. Bryan Ardis and Dr. Tau Braun
- they also include more widely respected ones like Dr. Peter McCullough
- there are also discrediting connections to “nanomachines” and the like, which I ignore
- for some people with long COVID, nicotine has helped when nothing else has worked
I advise just doing the recommended Rumble searches, to learn more.
For example, this video shows a variety of scientific papers which not only explain why nicotine affects spike protein-based symptoms, but also show demonstrated clinical benefit in actual patients.
LINK: https://rumble.com/v5wubbq-nicotine-protects-you-from-shedding.html
But now addressing a bigger question.
I do NOT suspect that nicotine poisoning was involved in DePat’s death. Toxic levels of nicotine result in very obvious symptoms (nausea, vomiting, tremors, vertigo, flushing, palpitations, etc.) that quickly make people back off on whatever means by which they were ingesting nicotine. I know, because the first cigar I ever smoked sent me into nicotine poisoning. People learn very quickly how to dose nicotine correctly.
DePat was actually getting some positive results with this method. More specifically, it was making her feel better. I personally think her efforts would have been more successful under a doctor’s supervision (preferably one connected to FLCCC or the like), but when I suggested “doctors and tests” to DePat, she was not a fan.
LINK: https://www.theqtree.com/2025/01/14/dear-kag-20250114-open-thread/#comment-1395665
DEPAT: I’m wondering if some of this fatigue is coming from trying to stay warm in a drafty house.
Hmmm….
ME: That sounds very likely to me.
Your body basically sends your periphery into overdrive to stay warm. Long johns / thick leggings and a sweater indoors can be very helpful. Feeling warm indoors can stabilize you.
Also wondering if your doctor is running a yearly thyroid check (TSH) If the numbers are odd or marginal, you may have something going on there.
DEPAT: Doctor? I learned my lesson with conventional medicine a long time ago.
It just seems the bad days are colder.
ME: Sounds a lot like COVID. Have you tested yourself at any point?
DEPAT: No. But I was exposed to two people who had their boosters over a month ago. The coughing fits started on the 17th last month. True weakness and needing to sit down for tasks the three days before Thanksgiving. I think I’m just about at the end.
In my opinion, DePat really needed a complete physical checkup, if only because it might have picked up any underlying conditions. But even more than that, there was a need for better diagnosis of what was ailing her. Simply assuming that it was vaccine shedding was risky, IMO.
Point 3 – COVID-19
Notice that I had asked DePat about COVID. The symptoms of being a “shedding recipient” should be almost the same as “long vax” – which should be very similar to the disease itself. Even more to the point, it is extremely easy to pick up COVID in a place like a choir. In fact, it only takes a much smaller dose of an infectious organism, than it does of a “shed vaccine”, to cause the exact same kind of problems that DePat was having.
DePat seemed very resistant to the idea that she might have had COVID or a similar ILI (influenza-like illness). However, to rule out an actual disease takes some effort. And to PREVENT disease takes even more.
Was she taking her temperature daily or twice daily? As far as I know, NO.
Was she taking ivermectin AT ALL, much less regularly? NO.
Was she taking vitamin D? Had she ever tested her levels of vitamin D? NO.
Was she taking enough zinc? I don’t think she was taking ANY zinc.
DePat’s situation was a lot like Wheatie’s. She KNEW – more or less – what sorts of things might be useful if she ever got COVID, but she had NOT prepared by having those things purchased, fully understood, and on hand, ready for trouble. Even more, she was not ready to DIAGNOSE COVID.
I KNOW that I have had COVID three times, because I’ve done the testing and clinical work to make absolutely firm diagnosis. I know that what I have right now is most certainly influenza, and NOT COVID.
And that brings me to my next point.
Point 4 – Influenza
I think it is VERY likely that DePat had the very nasty influenza that is going around right now, which singingsoul1 suffered from greatly, at almost the same time as DePat, and which I am suffering from at this very moment. As is my wife – so I am studying TWO cases, almost identical.
- “feel bad”
- aches and pains
- persistent cough
- no appetite
- insomnia
- chills
- fatigue
- sense of smell OK
- stuffy sinuses and phlegm – mostly upper respiratory
- “forget doing housework”
- need a nebulizer (I use saline spray, myself)
Everything DePat was saying about what she was suffering, sounds like what I’m suffering right now. And, in fact, what MANY people are suffering right now.
And here’s the kicker. Influenza is a PRIME candidate for setting up a heart attack afterwards.
https://health.clevelandclinic.org/can-the-flu-trigger-a-heart-attack
I know that many of you (like me) might suspect that this angle is pure post-clot-shot “explain away the vaccine heart attacks” bullshit, BUT the fact is, influenza has ALWAYS been notorious for killing old people, and heart attacks is one of the ways that it does it. Viral diseases – colds and flu – are also notorious as initiators of pericarditis and myocarditis. They didn’t have to make this shit up, to use it to deflect from their horrible vaccines.
As I love to say, there’s no cover like the truth.
Now – one might think DePat would have known if she had the flu, but this thing my wife and I have, has proven to be surprisingly low-fever – especially for my wife. Even after the fever has subsided, we still feel very ill. Were I not monitoring our temperatures every day, getting actual numbers, and signal over noise, it would have been easy to dismiss this thing as something other than influenza.
At numerous times during the last week, I have thought that maybe this was something other than influenza. But the reality keeps coming back, as I read more and more solid information about influenza and its treatment. What I have – what my wife has – what singingsoul had – and what DePat likely had – was a long, slow case of influenza, with a long recovery time.
Bear in mind that viral diseases often leave patients stuffy and suffering many symptoms for 60 days (2 months), long after the virus is gone. That fits perfectly with the timescale that DePat reported.
I think it is very critical to make a correct diagnosis, and to beware of reflexive “it’s the vaccine” thinking, when DISEASE never went away as a significant threat. Maybe even a MORE significant threat.
It’s entirely possible that DePat was exposed to “shed vaccine” – but I would argue that it’s more possible she was exposed to a nasty flu, didn’t have the right tools to diagnose or treat it, and damage by this flu ultimately led to a heart attack or stroke.
Either way, I now urge everybody – investigate treatments ahead of time. Don’t wait for being sick, because you won’t make it to the store – you won’t make that long trip to Tennessee – you won’t figure out which drug, where to get it, and how to take it.
Do all that ahead of time, if you want to live.
With that, I invite people to give me THEIR opinions. Feel free to disagree with me! After all, we have free speech back. THANK GOD!!!
Finally, this. Say a prayer for DePat and her family – grieve as you need, and you WILL need – but trust that God knows what God is doing, and seek comfort in that knowledge.
Trust in God. He is with us, and DePat is with Him.
All the best,
W