“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
Joe Biden never won. This is our Real President – 45, 46, 47.
AND our beautiful REALFLOTUS.
This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both).
Our various sister sites, listed in the Blogroll in the sidebar
Our beloved country is under Occupation by hostile forces.
Daily outrage and epic phuckery abound.
We can give in to despair…or we can be defiant and fight back in any way that we can.
Joe Biden didn’t win.
And we will keep saying Joe Biden didn’t win until we get His Fraudulency out of our White House.
Wolfie’s Wheatie’s Word of the Week:
viricide
noun
alternate spelling of virucide
killing of viruses
killing of men or of husbands
substance or agent that inactivates viruses
substance that destroys or inactivates viruses
act of killing one’s husband
Used in a sentence
While hydroxychloroquine may be an atypical viricide, it has an excellent safety record and an acceptable therapeutic ratio.
Used conceptually in a meme
Underlying a bigger message which helps us understand where we are today
MUSIC!
On Inauguration Day, I am reminded of an old song we used to love on the radio. It’s been a while, but the song seems remarkably relevant now. Here is a version that’s easier to hear the lyrics.
Here’s a live version from 1986. Keep your eye on the flags.
THE STUFF
It’s time to recall Trump Gravity and “the roller coaster”!
Well, I don’t really have to do any holding together, now that I figured out what Trump is up to. He is shaking things out, but counting on Trump gravity to pull things back together as he moves along. He is moving “forward” at speeds Obama could not even dream of.
You and I will be anti-Trump trolls one day and MAGA heroes the next. Get used to it. Trump speed is the new normal. Some will call it flip-flopping, but that’s not what it is. Trump is dodging and weaving through reality faster than the reality can react to disrupt his plans.
I was explaining this to my wife. This is a roller-coaster now. Trump is no longer waiting for people to keep up. He is taking his bewildering art-of-the-deal campaign schtick into geopolitics, and for a lot of people who can’t keep up or hold on, it will be a rough ride.
Trump is no longer playing only with evil and cunning players who are still predictable, easily beatable dopes, like Hillary. He is playing against killers, with his own team of killers, and all the while he has scheming creeps like Hillary, BGI, SPLC, and the neocons gunning for him. Snake Ryan ready to bite when nobody is looking. “Warhead” McCain screaming for Russian blood. Psycho Kim and Samoa Obama plotting some kind of intrigue to take him down. And THOSE are the lightweights.
This is the majors now. Trump has to outwit world-class adversaries and “frenemies” by defining the deals that they will agree to. One minute they will think Trump is their friend – the next minute, a cunning, bitter foe. And he has to do this with evil cheerleaders like Warhead, Linderace, Dipsy Dowd, Maggie Haterman, and Fake Yapper trashing him or praising him alternately, no matter which way he goes. They can’t keep up, either.
Neither can many around him. I think that half of the problem with advisers crashing into each other is they don’t realize what Trump is doing.
And people will trash you, and they will trash me. Get used to it. I’ve already caught plenty of people mocking me. Well, just wait a week in Trump time. Look stupid and conned by Trump one minute, and you look like a sage three days later.
Trump will not find perfect solutions. He will find OPTIMAL solutions. We cannot ask for more. Trump has stood by and watched Perfect murder Good for 8 years – maybe longer. He’s not gonna do it. He’s going to deliver the best outcome possible, and he’s not waiting for us to feel relaxed about it.
Best presidency ever! Just hang on. More winning is coming, but a lot of people are going to scream that it’s all over at EVERY turn.
The best way through this is to define viewpoints, not people, because people will shift as they change position and velocity in Trump gravity. Bash the neocon, warmonger, and dopey globalist positions – not the people who are going to hold them one moment and come loose from them later. Trump is Jupiter moving through the asteroid belt. He is going to pull people into his orbit. A few will get slung off into space, but most will come along for the ride of their lives.
I am ON the Trump Train for good, even if I scream that I want off and can’t take it. In the end, I only want to scream “TOO MUCH WINNING!!!” 😀
Wolf’s 2024 Comment
If you are not seeing just how remarkably similar things are right now, to the way they were at the end of 2016 and beginning of 2017, then please re-read the above post ONE MORE TIME. While you do so, think about all that Trump is doing now – before he has even taken office.
Think of what he is preparing to do – that you know about. Think of what he is preparing to do that you DON’T know about. Ask yourself which part of that iceberg is bigger.
Think of how President Trump is going to Make America Great Again – and BEYOND. Far, far beyond.
Trump is literally bringing TITANS into his orbit. And I mean BIG titans.
Stars rapidly orbiting the giant black hole at the center of the Milky Way galaxy.
But Trump doesn’t just care about the physical realm. Consider how Trump is always aligning himself with the forces of good, of love, and of peace in this world.
It was a privilege to host Mrs. Akie Abe at Mar-a-Lago once again. We fondly remembered her late husband, former Prime Minister Abe, and honored his remarkable legacy.
213.7K Views
Watch how Trump is skillfully working around corrupted, broken, and ossified government processes. Watch how Trump is dealing with world problems already, despite all the forces, both at home and abroad, which are allied against him.
We are experiencing Trump Gravity in ways that I simply could not have predicted in 2017. Trump is beyond a mere TITAN at this point. He is GARGANTUAN. He is stretching, compressing, and shifting SPACE AND TIME THEMSELVES. And yet – it’s OK.
In God We Trust – as we enjoy this amazing ride in His loving universe.
Live your best life. All around the world the Communist Left and their insufferable foot soldiers are in retreat and crisis mode. Their world is shrinking. They are becoming irrelevant. We are everywhere. Nimble, snarky, fast and with the sunlight arguments that defeat them. Live your very best life. Ignore the dark imaginings they attempt to present in their last desperate effort to remain relevant.
NIH is sponsoring a new TRIAL of ivermectin to treat COVID-19.
The latest chess move by NIH may be a move toward truth, or it could be more smoke and mirrors. However, I am telling you now – WE THE PEOPLE can force the play to yield TRUTH, if we keep our eyes on the ball.
In my opinion, we are FORCING – by the threat of NUREMBERG 2 – various government agencies to turn away from the Faucist false narratives they KNOW will do them as much good as “We were only following orders” helped the lower-level Nazis.
For example, the recent FDA 16-3 vote AGAINST sketchy, unproven, and very likely USELESS or actually counterproductive boosters – which the Faucists had to REVERSE by diktat of CDC’s Rochelle Alinsky – tells me that people in government who KNOW THE SCORE are starting to REBEL against “top-down” medicine, if only to save their own skins.
Yes, YouTube is holding the line for Comrade Alinsky, but others are starting to move away from the pounding gavels of NUREMBERG 2, sounding from just over the horizon of time.
Notice how FAKE NEWS can’t help but go after ivermectin, even reporting that NIH is giving it a trial.
YOU’RE A JOKE, FAKE NEWS!
Now – trust me – there are a thousand ways that people inside NIH, CDC, NIAID, or FDA could game the results of this study. I may talk about some of the other methods, but there is ONE in particular that was already used against hydroxychloroquine.
Fool us once, shame on you. Fool us twice, shame on US.
The way to insure a FAIL of any trial of an antiviral against COVID-19 is to give it too late. That includes “standard” antivirals like acyclovir, remdesivir, etc., AND it includes non-standard antivirals like hydroxychloroquine or ivermectin.
To validly test an antiviral, you have to give it early enough that it makes a difference. For a safe but highly nonstandard (and likely WEAKER) antiviral, “early enough” means VERY EARLY.
Dr. Zelenko recognized this IMMEDIATELY. That is why he jumped on very early outpatient hydroxychloroquine PLUS azithromycin (Raoult’s therapy, moved up in time) PLUS zinc, knowing that all three have a very HIGH margin of safety, so there is no need to wait – thus better to GET THE JUMP on both SARS-CoV-2 AND bacterial pneumonia, as well as any possible zinc deficiency.
Zelenko moved Raoult’s therapy to ALMOST prophylaxis, and removed the concern of zinc deficiency, common in the elderly.
It was SIMPLE, but it was BRAVE and GENIUS.
Now – LATER – there were COWARDLY attack studies, where hydroxychloroquine was administered too late, too much, and to dying patients, long after both antiviral and antirheumatic activities would do absolutely no good.
The scientific community called these studies out, but still – SHAME.
Will it happen again here?
Not if we can help it.
WHAT WE HAVE A CHANCE TO DO HERE, IS TO MAKE SURE THAT THIS STUDY OF IVERMECTIN CAN’T BE PURPOSELY FAILED BY LATE ADMINISTRATION.
The beauty of this study is that WE THE PEOPLE are the ones who “call in” when we get COVID. The earlier that is done, the more likely that ivermectin will PROVE its awesome ability to stop COVID in its tracks.
Thus, it is imperative that truth-seeking Deplorables (or libtards who are red-pilled enough to believe me) who are at risk for COVID-19, be READY to get into this study the MOMENT they are diagnosed.
And the easiest way to do THAT is to simply do the following:
Be familiar with the study
have the site bookmarked
have its phone number saved to your contacts
Have a COVID test on hand at home
Abbott BinaxNOW test is $25 for two (2) tests
antigen test is highly accurate, is NOT a PCR test
test takes 15 minutes and is very simple to perform
Use ALL OPTIONS to accelerate delivery of the treatments
Working together to help people with COVID-19 feel better faster. Call 833-385-1880 today!
The ACTIV-6 Study
The ACTIV-6 research study is testing several medications that are already approved for other diseases to see if they can help people with mild to moderate COVID-19 feel better faster and stay out of the hospital.
If you are 30 years old or older, have tested positive for COVID-19 within the past 10 days and have at least 2 COVID-19 symptoms for 7 days or less, you can help make a difference by participating in ACTIV-6.
You can participate from anywhere in the U.S. Medications are shipped to you at no cost. You will keep track of your symptoms and how you feel over 90 days.
Medications in the ACTIV-6 Study
ACTIV-6 is evaluating repurposed medications for effective, safe treatments for mild-to-moderate COVID-19. Repurposed medications are already approved by the U.S. Food and Drug Administration for other indications. The study is now testing these medications:
Fluticasone
an inhaled steroid commonly prescribed for asthma and chronic obstructive pulmonary disease
Fluvoxamine
a selective serotonin reuptake inhibitor (SSRI), often prescribed for depression
Ivermectin
used to treat parasitic infections
These medications can be shipped anywhere in the United States at no cost to participants.
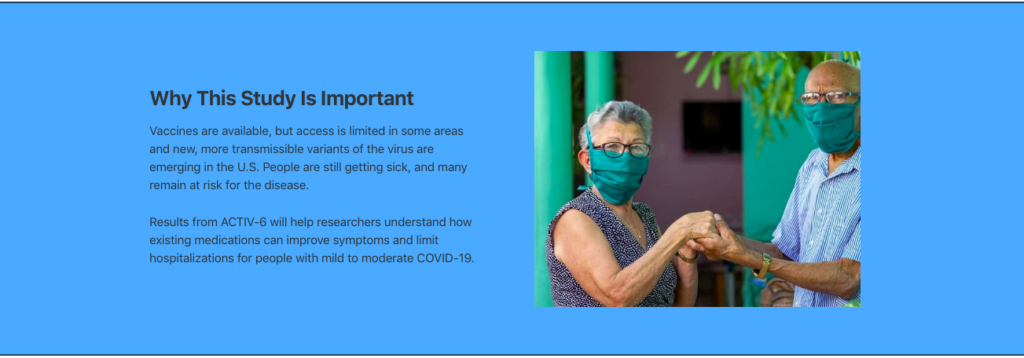
Why This Study Is Important
Vaccines are available, but access is limited in some areas and new, more transmissible variants of the virus are emerging in the U.S. People are still getting sick, and many remain at risk for the disease.
Results from ACTIV-6 will help researchers understand how existing medications can improve symptoms and limit hospitalizations for people with mild to moderate COVID-19.
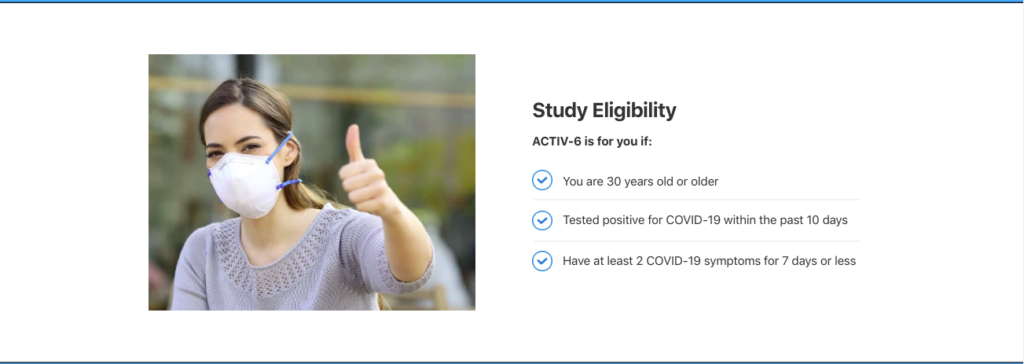
Study Eligibility
ACTIV-6 is for you if:
You are 30 years old or older
Tested positive for COVID-19 within the past 10 days
Have at least 2 COVID-19 symptoms for 7 days or less
Frequently Asked Questions
I am enrolled in ACTIV-6. How do I report a new health concern?
Click here to report a concern or medical event to our Call Center.
Does participation cost anything?
No, there is no cost to you to participate. All activities can be conducted on a private and secure website or over the phone.
Am I compensated for participating?
You may receive a gift card of up to $100 upon completion of the study.
Better treatments for COVID-19 are still needed, especially for patients with mild to moderate illness who are not hospitalized.
ACTIV-6 is part of a larger public-private partnership, Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV), announced in 2020 by the National Institutes of Health.
Enroll Today!
Fill out the screening form to have a study team member contact you, or call 833-385-1880 to speak with a study team member.
ACTIV-6 Study – Study Website – 29 – June – 2021 – English (Master) – V2.0
Now – I want to be absolutely clear about something – which is another way of saying that I want to rub FAKE SCIENCE’S NOSE in it’s own POOP.
We are not “gaming” this study by FORCING better science on establishment science. We are making sure that this is not a “gamed” study, by REMOVING the most likely (and proven) source of gaming the study to NOT SHOW A RESULT.
If the average starting time of therapy goes DOWN to where conclusive results are shown, that is GOOD DESIGN. That’s what we’re banking on here.
So – be sure to bookmark this sucker. If you get COVID, and this study (or a successor study) is running, you want to get into it.
Well, they can lock us out of The Q Tree, but they can’t stop the truth from getting out.
Enjoy a post first over on The U Tree and now HERE.
Here is a quickie in my WAR ON REMDESIVIR.
Fellow Treeper barkerjim dropped an interesting document today, from back in July, which showed the NIH mentioning black sheep IVERMECTIN on the same page as REMDESIVIR.
Such a beautiful misdirection. These guys are MAGICIANS.
This is a perfect example of my postulate that fighting FOR ivermectin will not yield results for restoring real science as fast as fighting AGAINST remdesivir.
In fact, I would go so far as to say that the enemy realized that getting us to fight FOR the saving drug would keep us from expending our energy fighting AGAINST the murdering drug that kills us off and gives them money for doing it.
You may recall my previous posts about remdesivir.
My next piece was going to be an expansion on Karl Denninger’s recent post which places remdesivir/ivermectin and remdesivir/hydroxychloroquine in the context of Anthony Fauci and the disturbingly similar case when he was “all about AIDS” – namely, AZT/bactrim.
YES. As Cthulhu has said before, “This is not Fauci’s first rodeo.”
Before there were hydroxychloroquine and ivermectin as innocent victims – good Samaritans accused falsely before the world – there was BACTRIM.
And there was FAUCI on all of them. AZT played the murderous part of remdesivir long before we forgot that “miracle drug”.
However, this new information from barkerjim’s drop right here needs to get out right away. The Q Tree site was brought down YET AGAIN as I started working on this, and again when I resumed, so I know it’s critical stuff. The ChiComs have a huge investment – both financial and military 4GW – in the American-killing drug remdesivir. They WILL protect it.
We know from doctors and scientists quoted in my first two articles, that remdesivir has a horrible track record – shocking, really – of renal toxicity. Studies of the drug against Ebola were TERMINATED because it was killing people in the hospital.
How déjà vu.
But here it comes again.
I read the same study results that the above celebratory announcement was made over. Those results were nothing to cheer about, with shot kidneys just the horrifying icing on the death cake. In my opinion, the results were far WORSE than any prior results for hydroxychloroquine. The results – to me – made HCQ look EXCELLENT in comparison.
Yes – by controlling what is acceptable science and what is not, Fauci was able to force the world to field a BAD, DANGEROUS DRUG that made money for Gilead, over a safe, mildly (but critically) effective drug, that made money only for the generics industry, and a French company.
And to top it off, Fauci USED Trump, who could do absolutely nothing about it, to take a KILLER drug into market as the ONLY way to treat his little pandemic.
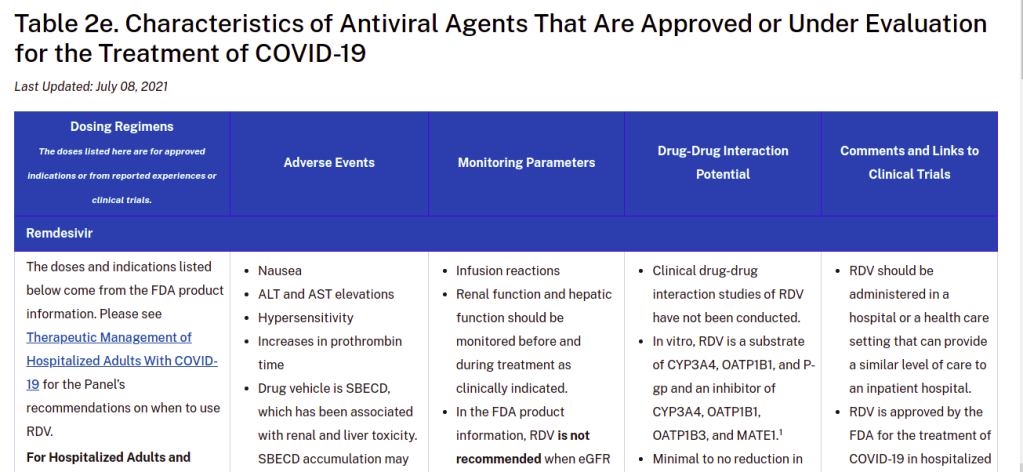
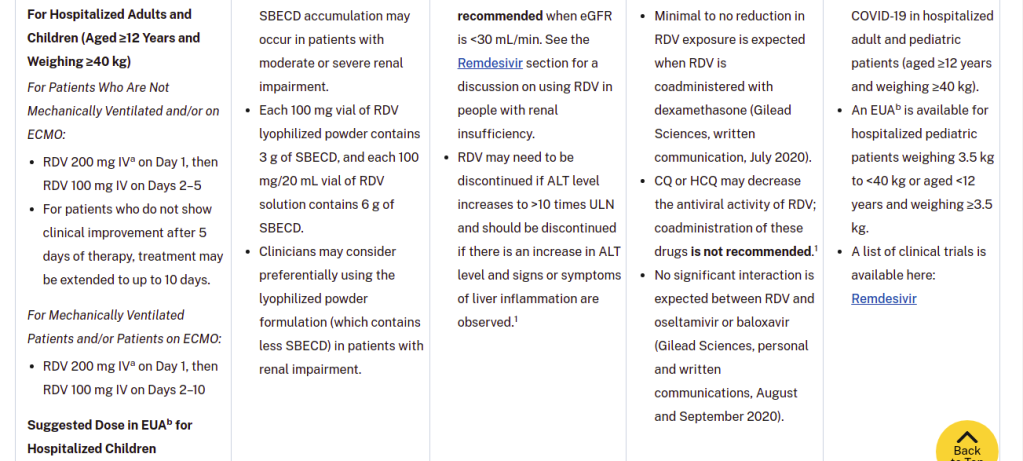
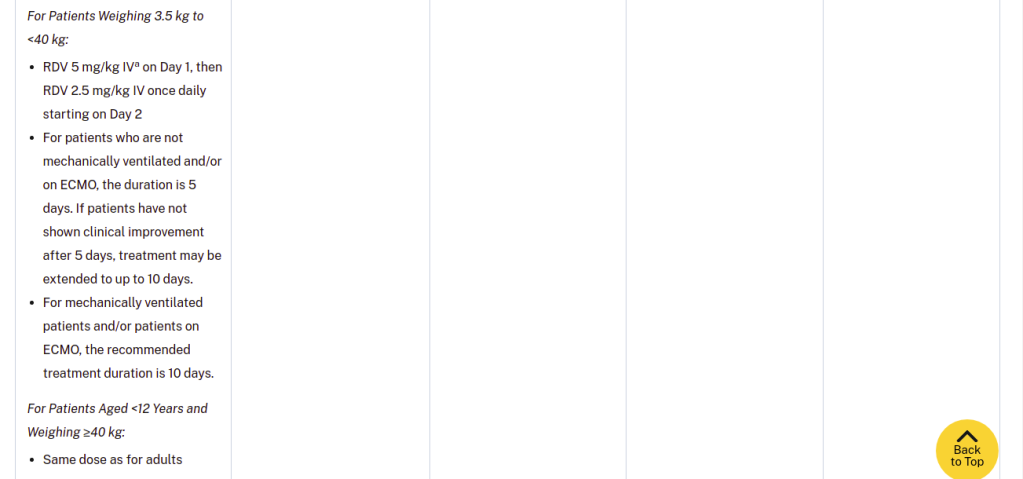
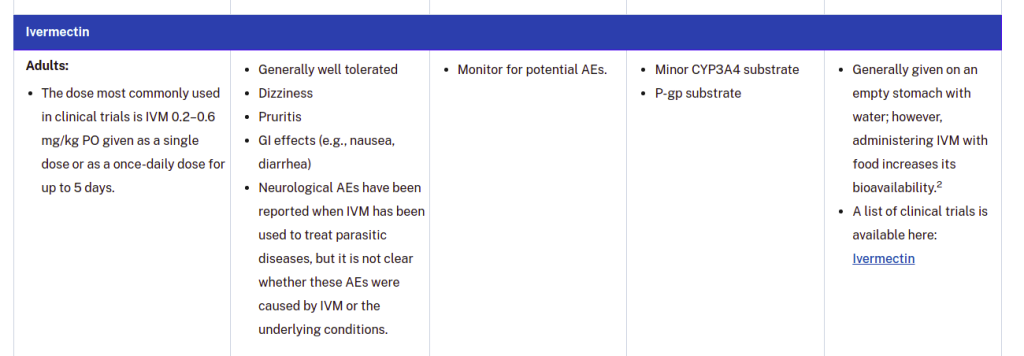
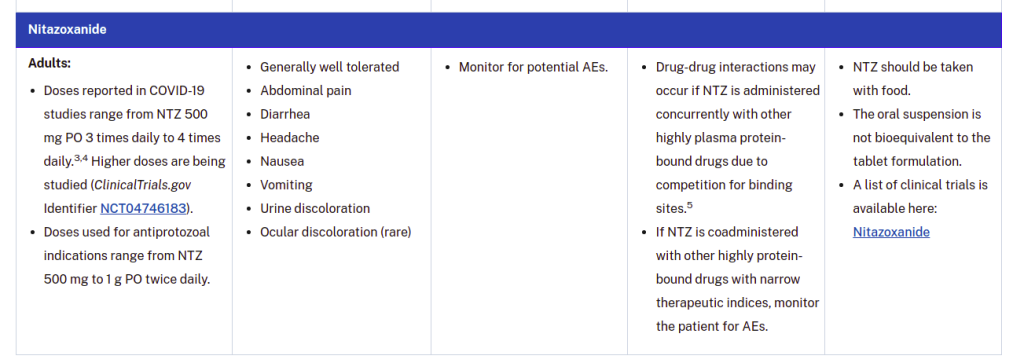
So let’s take a look at that page dropped by barkerjim. I have captured it as SIX IMAGES.
As you can see by our comments on The U Tree, most people will look at this table and think they are seeing positive and reasonable behavior by NIH. Adverse events are being discussed, and it appears that things are “even-handed” between different drugs.
And that is EXACTLY the style in which EVIL ABOUNDS IN WASHINGTON, DC (or Atlanta). Good and evil are forced into compromises where GOOD LOSES and EVIL WINS – but the result is called “meeting in the middle”.
CLOSER INSPECTION of the table gives you this, under Adverse Events for remdesivir.
Nausea
ALT and AST elevations
Hypersensitivity
Increases in prothrombin time
Drug vehicle is SBECD, which has been associated with renal and liver toxicity. SBECD accumulation may occur in patients with moderate or severe renal impairment.
Each 100 mg vial of RDV lyophilized powder contains 3 g of SBECD, and each 100 mg/20 mL vial of RDV solution contains 6 g of SBECD.
Clinicians may consider preferentially using the lyophilized powder formulation (which contains less SBECD) in patients with renal impairment.
This is some of the most remarkable “medical misinformation” I’ve ever seen. It’s truly a work of art.
NIH has HIDDEN – completely hidden – the pronounced renal toxicity of remdesivir. They have hidden it COMPLETELY. It’s GONE. What you are seeing there – the talk about renal and liver toxicity – is a BLAME-SHIFT to a substance that is used WIDELY in intravenous formulations, called sulfobutylether-β-cyclodextrin, or SBECD for short.
This substance is an EXCIPIENT.
An excipient is a substance that is used to MIX with a drug, and take that drug into a form where it can be ADMINISTERED easily. Thus, an excipient may DISSOLVE the drug, or help to dissolve it, into a liquid form. It may help POWDER the drug, so that it can be pressed into tablets or filled into capsules.
Excipients are often considered “inactive ingredients”, even though – YES – they very much can change the effective amount of a drug that the patient gets.
If I had to describe SBECD as something, it would be as a DETERGENT FOR DRUGS. It’s a kind of SOAP made from a cyclodextrin, instead of from some kind of fat or lipid.
Cyclodextrins are rings of sugar molecules that falls somewhere in between being a smaller chain sugar (like sucrose) and a starch. Cyclodextrins have lots of uses, because they form tubes that act like waffle cones for other molecules. Febreze uses cyclodextrins to trap molecules which have unpleasant odors, at the same time that they release more pleasant ones. A genius application, quite frankly.
Thus, if you make a SOAP that has a little waffle cone for drugs, you can EASILY get drugs to dissolve into a concentrated liquid form by using that soap.
See those sidechains hanging off the cyclodextrin ring? Those are the “SBE” part of SBECD. They are typical of DETERGENTS.
This SBECD stuff and things like it are VERY useful for delivery of drugs. AND they’re relatively safe, too. They are rapidly excreted through the kidneys. Yeah, you don’t want a SOAP piling up in your blood if your kidneys are not working, and THAT is the fact that is being TWISTED by NIH when they say:
Drug vehicle is SBECD, which has been associated with renal and liver toxicity. SBECD accumulation may occur in patients with moderate or severe renal impairment.
Did you catch that sleight of hand? I’m gonna show it to you.
What exactly is causing the renal problems in the FIRST PLACE that you MAY have to be careful about, so that you don’t build up the excipient FOR IT, which MAY constitute a FURTHER risk?
REMDESIVIR.
It’s a crafty little lie. If you have good kidneys, you don’t have anything to worry about with this SBECD crap. But if you have bad kidneys, the LEAST of your problems is SBECD buildup. It’s the remdesivir IN the SBECD that’s gonna kill you.
Weakened kidneys do NOT need to be hit with remdesivir.
Which doesn’t even work ANYWAY. Except to keep people LONGER in the hospital.
Now what you SHOULD be getting, when they administer remdesivir, at the point where the VIRUS is basically gone, and you’re dealing with spike protein damage, cytokine storm, and all that nasty crap, are antiinflammatory, antithrombotic, and immunomodulatory drugs. Even HCQ (a known antirheumatic) at reasonable doses had some antiinflammatory effect in late-stage hospitalized COVID cases, although steroids and other things work better.
When the virus is basically gone, and a bunch of its CRAP is left behind, there is no point administering a toxic antiviral like remdesivir, other than to send money to Gilead Pharmaceuticals and their Deep State friends.
Now, let me stop here and validate this stuff.
HERE is a link that explains how SBECD can be filtered out of blood ANYWAY if a patient has renal impairment.
Do you see what that means? SBECD is a nothingburger. It’s a DEFLECTION.
The renal problems of remdesivir are never mentioned, by quickly bringing up the risks of the excipient due to the unmentioned damage BY remdesivir.
What NIH did here was to quickly point their finger at THE OTHER GUY and said “HE DID IT!”
This is pure politicized science, where the politics is to defend the drugs and vaccines that enable the shared profits of both the Deep State and the companies that NIH, CDC, and NIAID are in bed with.
Let’s go back to that link I just gave you. THIS part of the conclusions comports very nicely with the reality of SBECD as a widely used excipient.
The finding that SBECD can be effectively removed by CVVH is clinically important, because some cyclodextrins have been associated with hepatotoxicity or nephrotoxicity due to vacuolation [3]. Although our study was small, no evidence to suggest SBECD as a cause of hepatotoxicity or nephrotoxicity was demonstrated in our study patients. This finding is consistent with other SBECD safety studies in humans [3,18]. Additionally, animal studies have only been able to demonstrate cyclodextrin toxicities when dosages more than 50-fold greater (3,000 mg/kg) than those used in humans were administered [3,19,20]. Unlike other cyclodextrins used in these animal studies, SBECD undergoes only minimal tubular reabsorption and limits concentrations within the intracellular tissues of the kidney, potentially reducing the risk of nephrotoxicity. Nevertheless, the FDA labeling for voriconazole recommends that IV therapy be avoided, if possible, in patients with a CrCl <50 ml/min [5]. Our data suggest that IV voriconazole can be safely administered in this population if the patient is concurrently undergoing CVVH.
Delafloxacin, a fluoroquinolone, has activity against Gram-positive organisms including methicillin-resistant S aureus and fluoroquinolone-susceptible and -resistant Gram-negative organisms. The intravenous formulation of delafloxacin contains the excipient sulfobutylether-β-cyclodextrin (SBECD), which is eliminated by renal filtration. This study examined the pharmacokinetics and safety of SBECD after single intravenous (IV) infusions in subjects with renal impairment. The study was an open-label, parallel-group, crossover study in subjects with normal renal function or mild, moderate, or severe renal impairment, and those with end-stage renal disease undergoing hemodialysis. Subjects received 300 mg delafloxacin IV or placebo IV, containing 2400 mg SBECD, in 2 periods separated by ≥14-day washouts. SBECD total clearance decreased with decreasing renal function, with a corresponding increase in area under the concentration-time curve (AUC0-∞ ). After IV delafloxacin 300 mg administration, SBECD mean total clearance was 6.28 and 1.24 L/h, mean AUC0-∞ was 387 and 2130 h·μg/mL, and mean renal clearance was 5.36 and 1.14 L/h in normal and severe renal subjects, respectively. Similar values were obtained after IV placebo administration. In subjects with end-stage renal disease, delafloxacin 300 mg IV produced mean SBECD AUC0-48 values of 2715 and 7861 h·μg/mL when dosed before and after hemodialysis, respectively. Total SBECD clearance exhibited linear relationships to estimated glomerular filtration rate and creatinine clearance. Single doses of IV delafloxacin 300 mg and IV placebo were well tolerated in all groups. In conclusion, decreasing renal function causes reduced SBECD clearance and increased exposures, but SBECD continues to exhibit a good safety and tolerability profile in IV formulations.
“In conclusion, decreasing renal function causes reduced SBECD clearance and increased exposures, but SBECD continues to exhibit a good safety and tolerability profile in IV formulations.“
Now, the above is not the only “New York Times” style trick that NIH plays here.
Let me list, without going into long-winded explanations, my additional favorites.
The table authors note that clinical drug-drug interaction studies have not been done, but nonetheless, they say “CQ or HCQ may decrease the antiviral activity of RDV; coadministration of these drugs is not recommended.1” – with a hanging reference.
For three OTHER potential drug interactions, communications from Gilead are cited as sufficiently exonerating. One is a non-competing generic steroid (dexamethasone) and the other two are patented big pharma antivirals from corporate “frenemy” Genentech. The interaction and “C-level mind-melding” between these two companies is very interesting. Look who just went from one to the other. Interesting times.
Some crafty shade is thrown at ivermectin by citing a possible adverse event risk and then retracting it, lawyer-style: “Neurological AEs have been reported when IVM has been used to treat parasitic diseases, but it is not clear whether these AEs were caused by IVM or the underlying conditions.” Meanwhile, the DEMONSTRATED risks of remdesivir are not even mentioned.
Bottom line – NIH is protecting Gilead on the toxicity of remdesivir, and they used FAKE NEWS tricks to do it. I keep telling people – science journalism is bad, and science governance is WORSE. It’s been CHINATIZED and OBAMATIZED.
This is for the historical record. I hope that this analysis gets to the “dissident scientists” involved, but even if it never does, future historians will get a powerful look at what I call “Fake Science” – the establishment’s phony, deceptive and controlled scientific complex – and how infiltration, control, and discreditation of dissident populist scientists was used in this era to keep them in check, protecting controlled science and the interests that keep it controlled – for money, power, and “say” in human destiny.
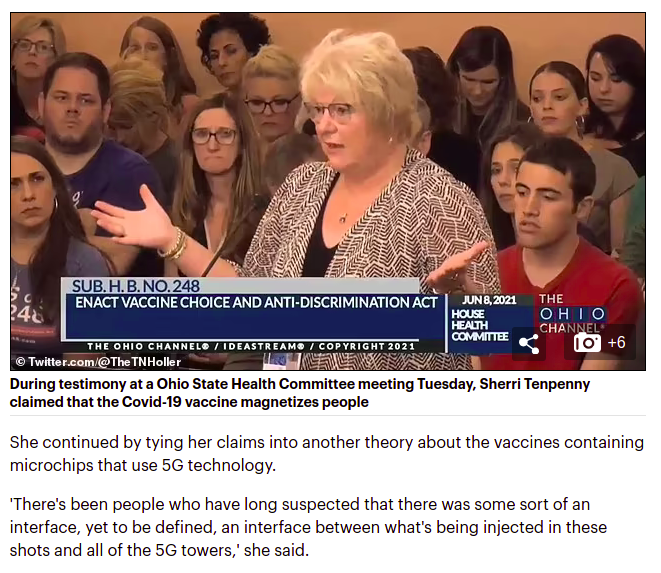
Even though this story has little or nothing to do with magnetism, I believe this was the beginning of strong discreditation of Judy Mikovits, Sherri Tenpenny, and other “COVID dissident doctors and scientists” who are pursuing the “spike protein and COVID vaccine gynecological problems”. Ultimately, the “coup de grace” was delivered via the phony vaccine magnetism psy-op.
The BIG HIT on this group was the discreditation of Dr. Tenpenny on “vaccine magnetism” – a CIA-constructed sandtrap which I could see coming a mile away, with great horror, as it was placed in front of these “insufficiently skeptical skeptics” – who are skeptical enough to doubt the controlling LIES marbled into mainstream science – but who are blithely unaware of just how evil the establishment really is, in making sure nobody listens to them.
That poor, poor woman. Sounds pretty crazy, doesn’t it? Well, here is the deal. The “establishment science skeptic community” is social, and because it’s a bit lonely in Skepticville, people become tolerant of the crazier stuff, very unlikely to be true, which can easily be fed into the community. Obviously an intelligence agency which knows psychology better than all our universities combined can have a field day with that stuff.
However, before THAT story – which we will get into later – there is THIS story – where I saw these doctors being set up for discreditation on a different topic.
Every time they used the word “suramin” I winced, and this is why.
I will follow this story in roughly chronological order, from my first awareness to today, when I saw the complete picture. However, I may “fast forward” to later knowledge, at times, to put things in context.
When I first saw THIS headline from the SGT Report posted in this site’s open thread (I think it was Duchess, so THANK YOU!), all I could think was “OMG, what a pile of unbelievability THIS is.”
Not only did I think that “vaccine shedding” was preposterous – the idea that it could be fended off somehow with pine needle tea just sounded NUTS.
That was May 10, 2021 – ironically exactly one month ago. I had NO CLUE that one month later – today – I would be convinced that not only is “vaccine shedding” real – Pfizer knew it was a “thing” all along – and long ago.
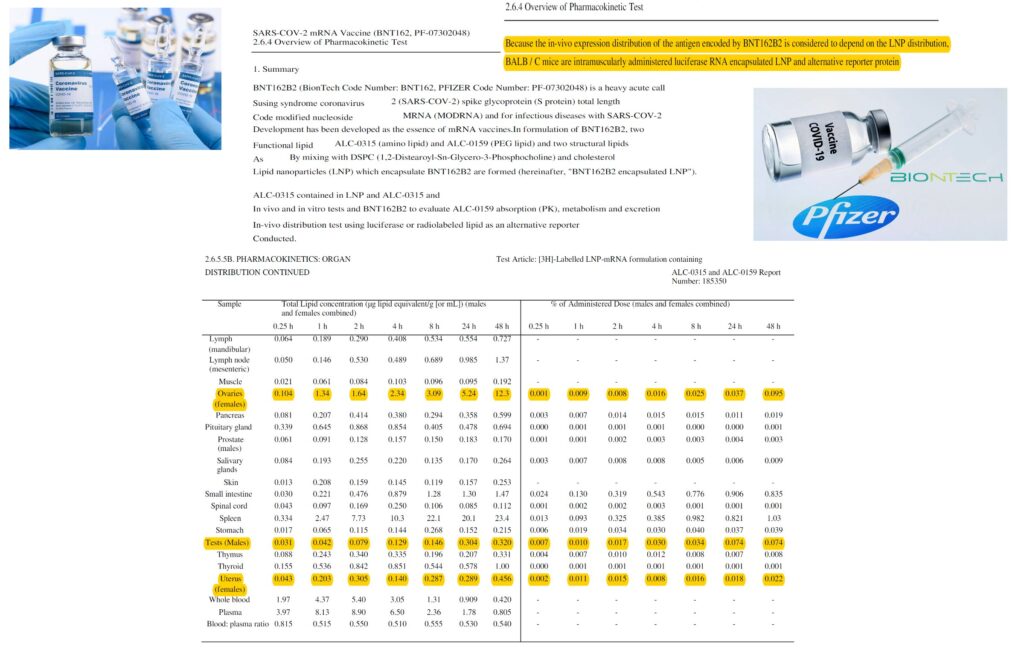
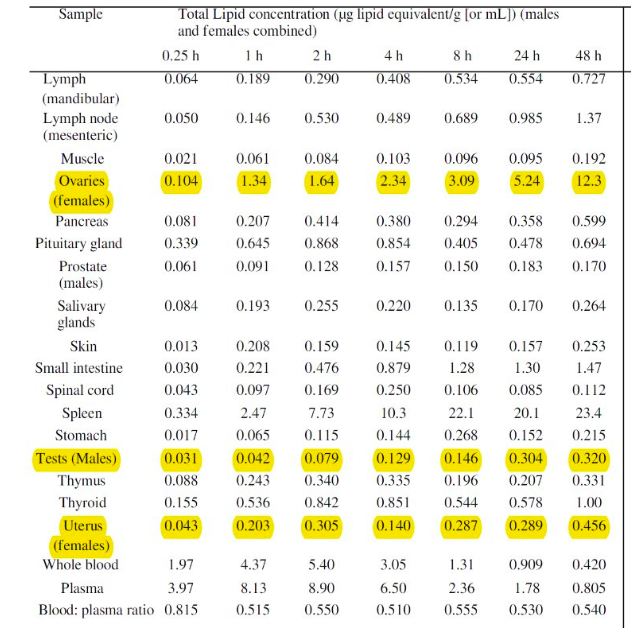
This is the Pfizer data obtained from the Japanese government.
This is the data up close.
The most important data is simple – the fact that the vaccine is relocating all over the bodies of the test animals – SHOCKINGLY to the ovaries as one of the primary destinations – and the amount of TIME it’s taking to do so. The reason is that the vaccine is encapsulated in lipids – fatty substances – which protect the mRNA, and give it time to get into cells.
Looking at this data, there is no reason to doubt that the vaccine could express in skin lipids, and given that it WAS INDEED expressed in breast milk (full of lipids), killing at least one baby, the EXCRETION of the vaccine at this point makes logical sense.
Thus, when this information got out, the CRITICS were in the catbird seat, and the INDUSTRY which oddly tolerated these results, was in trouble.
How does one flip that around? DISCREDIT THE CRITICS.
Now I did not realize at the time that THAT was what was going on with “pine needle tea”. I thought this was just the usual stuff that pops up routinely in the “natural health” world. However, a closer look at the article surprised me.
There appeared to be a chemical error, and it appeared to be Dr. Judy Mikovits making that error. But it’s not her making the error.
Here are two paragraphs of interest:
There is a potential antidote to the current spike protein contagion which is called Suramin. It’s found in many forests around the world, in Pine needles. Suramin has inhibitory effects against components of the coagulation cascade and against the inappropriate replication and modification of RNA and DNA. Excessive coagulation causes blood clots, mini-clots, strokes, and unusually heavy menstrual cycles.
Dr. Judy Mikovits asserts that globalists are well aware that pine needle tea is the answer to covid depopulation weapons, and they are secretly using pine needle tea to protect themselves from the very plague they have unleashed upon the world, Mikovitz explains.
I do disagree with a portion of Mikovits’ beliefs, but not everything. She really changed my whole view of “gain of function” – she sees very deeply into the problems of “Faucism”, shall we say. One thing she is NOT is stupid. So when I read that second paragraph, I simply didn’t believe it. It’s complete crap. “Pine Needle Tea vs. The Globalists”. Yeah, great movie! And kind of ironic that one would use a NATURAL ABORTIFACIENT to face off with “depopulationists”, but we’ll save that bit of “oy vey” for later analysis.
Well, deeper digging showed me where this came from. ANOTHER person who I usually trust, up to a point – Mike Adams of Natural News. From the day BEFORE – May 9.
Mike Adams is actually a pretty decent scientist, although he does allow guests on his show to wander off into clickbait generalities, far-fetched speculations, and utopian (or dystopian) characterizations. It’s just edgy stuff. Typical “natural remedies” world. I still buy the rational and reasoned parts of it – it’s just “old science”. And on the basic FACTS coming out of labs, Mike Adams doesn’t present “fake data”. He waits like a buzzard for REAL DATA that looks good for “naturalism” and then plays “AHA! LOOK AT THIS!” with mainstream medicine. It’s a “schtick”, but it’s a pretty good one.
Anyway, the wording is identical – SGT Report was just copying and mirroring Natural News, as they often do.
I saw at the time that Mike Adams had just picked this information up from some naturals blogger, and had copied it verbatim.
Now – beyond the nonsensical attribution to Mikovits, there are actually TWO big chemistry problems with this article that Mike is citing.
One is on the idea that shikimic acid – the desired ingredient in pine needles – IS Tamiflu.
Quoted in the story:
Researchers at the University of Maine at Orono say they’ve found a new and relatively easy way to extract shikimic acid — a key ingredient in the drug Tamiflu — from pine tree needles.
That’s not exactly true. Shikimic acid is NOT Tamiflu, nor is it an ingredient in Tamiflu. Now, a more accurate statement is also given:
Shikimic acid derivatives have also been shown to exhibit useful biological activity. Most notably, the well-known antiviral drug oseltamivir (Tamiflu), which acts as a viral neuraminidase inhibitor, is used to treat seasonal influenza and has been deployed during H1N1 influenza outbreaks.
YES. A derivative. Tamiflu is RELATED to shikimic acid, but it is a distinctly different molecule. Shikimic acid can be used to MAKE Tamiflu. But it is a building block – not the same thing.
All that said, shikimic acid, whether from star anise or from pine needles, is indeed antiviral in some contexts, and antiinflammatory in others. So, YES, pine needles are an actual curative thing. More than just containing an exotic natural acid, they were the equivalent of citrus fruit for North American Indians.
Indeed, pine needle tea can be used to treat scurvy, and it’s BETTER than just vitamin C (which it contains in vast amounts), because it also contains flavonoids which are curative for vascular symptoms of scurvy.
However, you have to pick the right pine needles – some are poisonous, and even the good ones can INDUCE ABORTION.
The part about inducing abortion is VERY critical. That would be very problematic for these doctor critics of the spike protein vaccines, if they were in fact advocating “a different abortifacient instead”.
See how that works?
That is – how do we say this? – ah, yes – discreditation.
Now, at the TIME, I just thought to myself “Wow – how unfortunate that these people who are going after the ‘abortion vaccine’ are advising people to take an abortifacient.”
And I’m not the only person who observed this. It turns out that the original blog article was edited a number of times, to ADD warning information about the potential abortifacient risks of pine needle teas. The information was not there originally. It looks to me like blog commenters (comments are invited but hidden) likely cautioned the author about the problem.
Yeah, let’s just give THAT the “jaundiced editorial eye” that Maria does so well.
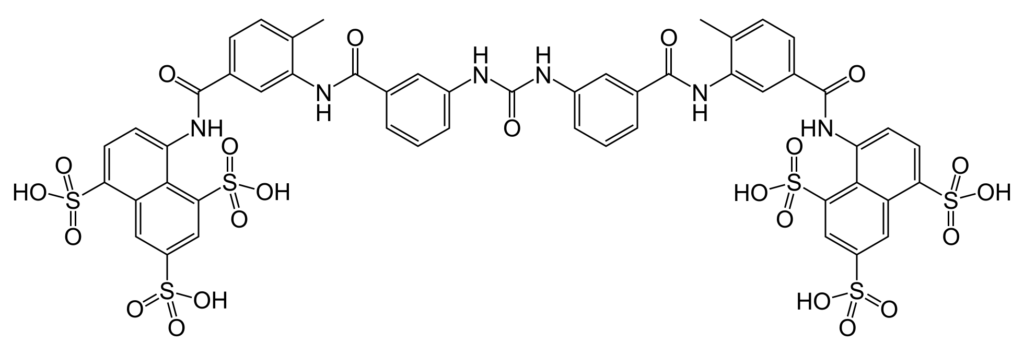
ANYWAY, on to the OTHER chemical mistake – SURAMIN.
This is actually rather cute, and the wicked industry that just savaged Dr. Tenpenny is going to get a little karma here.
As you will see, shortly, part of the “discred” here is also for suramin itself – because it’s a potential and very legitimate “HCQ” or “ivermectin” – a readily available treatment. I didn’t realize this at the time.
I will explain that more fully in a moment.
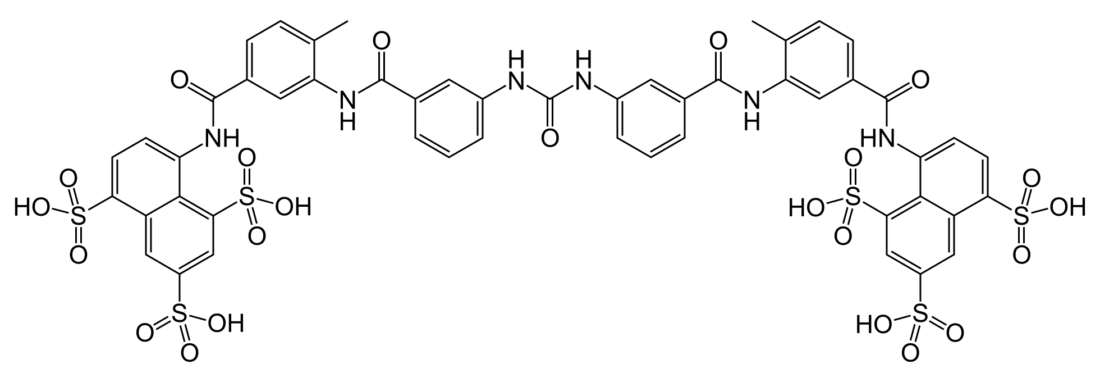
Suramin is a synthetic drug – it’s not a natural product. Many of us can tell just by looking at the structure.
And NO, this stuff is NOT in pine needles. Anybody who says this is INSTABLOCKED in SCIENCEVILLE.
Suramin is a killer of parasites – it’s used to cure sleeping sickness and river blindness in Africa. It’s actually a well-known, long-term, old drug. Indeed, it’s a lot like hydroxychloroquine, being on that WHO list of essential medicines.
Aubergine, our local naturals expert, quickly spotted that this was a synthetic drug and very unlikely to be in pine needles. I confirmed her suspicions, but I didn’t really dig into WHY this error had been made in the article – until today, when I saw it from a discreditation angle.
First of all – to my surprise – there is some real science behind suramin as a treatment for COVID-19.
The following is from a very solid source that monitors new medical developments in the scientific literature.
Here we report the discovery of suramin, a 100-year-old drug, as a potent inhibitor of the SARS-CoV-2 RNA dependent RNA polymerase (RdRp) through blocking the binding of RNA to the enzyme. In biochemical assays, suramin and its derivatives are at least 20-fold more potent than remdesivir, the currently approved nucleotide drug for COVID-19. The 2.6 Å cryo-EM structure of the viral RdRp bound to suramin reveals two binding sites of suramin, with one site directly blocking the binding of the RNA template strand and the other site clash with the RNA primer strand near the RdRp catalytic active site, therefore inhibiting the viral RNA replication. Furthermore, suramin potently inhibits SARS-CoV-2 duplication in Vero E6 cells.
Better than Remdesivir? AWWWWW. Where did we hear THAT before?
OH, I REMEMBER! It was some drug called “hydroxychloroquine”!
So what you are seeing here, is that ANOTHER old antiparasitic drug looked to be BETTER THAN REMDESIVIR as an antiviral. Why, that would almost be THREE FOR THREE. Were it not nipped in the bud.
So indeed, Dr. Judy Mikovits had spotted that suramin was a useful drug for COVID. She had prior knowledge that it has been trialed as a treatment for AUTISM, and that, also, with some surprising success.
Now – here is where it gets really interesting.
THIS video was cited in the “pine needle tea” blog post. It is HIGHLY edited. Just listen. The MUSIC is absolutely CRINGEVILLE.
https://youtu.be/JYHrmmmoX30
NOTE ADDED LATER (June 14, 2022)
You will note that the video is now just a link.
Here is an EARLIER screenshot from right after the video went down – which was basically a day after I published.
Note that it was NOT removed by YouTube – it was removed by the uploader at that time.
Here is a screenshot from the video when it was up.
This Academy of Divine Knowledge (June 14, 2022 discussion HERE) seems tied to many of the luminaries of the “discredited dirty dozen” – but IMO it may very well be part of the discreditation of them.
It’s too bad the video is down – you cannot see the skillful editing. Basically, an earlier video of Mikovits which was “good science” was recast by editing to create a point of division on falsehood, rather that a unification on truth.
As I was saying (before this note was added)……
This is a beautiful editing job which accomplishes two things:
(1) makes Mikovits look authoritative to people in the new age end of the natural remedies world ($$$$$)
(2) makes Mikovits look utterly discredited in the scientific world (?????)
One would not know, from this video, ANYTHING about the idea that suramin is turning out to be ANOTHER potential HCQ, safer and better than remdesivir.
But yet this video is “helping” her, and I seriously doubt she realizes just how undermining it is.
This is how discred works. Very often, the subject has NO IDEA. They may see the discrediting actions as not just neutral, but well-intended. But outside the understanding of the target, discred keeps things DIVIDED. Serious people are not going to take Mikovits seriously. Suramin will look like one more fish tank cleaner. Remdesivir (very likely on the cutting room floor for that video) won’t be threatened.
It’s so SLICK.
But THAT is not the best part. When suramin is FALSELY linked to pine needle tea, and the CHUMPS – the MARKS – are tricked into saying it – everything falls apart.
Mikovits’ advocacy of suramin as another potential HCQ / ivermectin looks loony
The Chinese chump scientists’ very legitimate work on suramin, but threatening remdesivir, gets memory-holed
Any doctors who pick up and repeat the error about suramin and pine needle tea are tainted by the error
The chump docs are now ready for the coup de grace – the phony magnetic vaccine psy-op
I hope you now see WHY these small errors matter – and why “opposition research” is a THING not only in politics, but in the highly politicized science, under which we now suffer.
I think these good doctors were SET UP.
I think that THIS:
…..was the DESIRED OUTCOME OF THIS:
“Dissident” doctors and scientists need to be more careful. We are up against very EVIL people.
This [Q-3]TH of AUGUST FRIDAY open thread is OPEN – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA / KAG! / KMAG world (KMAG being a bit of both MAGA and KAG!).
We're big over the target on this one!
PREDICTION: The #LancetGate effect of increases in both DEATHS and INFECTIONS upon banning of #HCQ will show up in all countries that reacted to the paper, including several which have not been publicly mentioned yet.
You can say what you want, comment on what other people said, and so on.
Free Speech is practiced here. ENJOY IT. Use it or lose it.
Keep it SOMEWHAT civil. They tried to FORCE fake Orwellian civility on us. In response, we CHOOSE true civility to defend our precious FREEDOM from THEM.
Our rules began with the civility of the Old Treehouse, later to become the Wolverinian Empire, and one might say that we have RESTORED THE OLD REPUBLIC – the early high-interaction model of the Treehouse – except of course that Q discussion is not only allowed but encouraged, and speech is considerably freer in other ways. Please feel free to argue and disagree with the board owner, as nicely as possible.
Please also consider the Important Guidelines, outlined here in the OLD January 1st , 2019 open thread. Let’s not give the odious Internet Censors a reason to shut down this precious haven.
SPEAK THE FIVE WORDS BOLDLY TO OUR PRESIDENT!
“I AM PRAYING FOR YOU!“
AND WHAT TIME IS IT?
TIME TO….
DRAIN THE SWAMP
Our movement
Is about replacing
A failed
And CORRUPT
Political establishment
With a new government controlled
By you, the American People.
Candidate Donald J. Trump
Also remember Wheatie’s Rules:
No food fights.
No running with scissors.
If you bring snacks, bring enough for everyone.
Little Boy, Fat Man & The Sundance Kid
OK – we have a problem. Sundance’s reveal, undoubtedly a NUKE of Eeyore proportions, is coming soon.
Many of us want to talk about “Sundance stuff”, which tends toward DOWNSIDE THINKING.
I will agree that SD does not do “mea culpa” well, or even “at all”!!!
I believe SD’s point about Mueller team control is not going to convince those who don’t see “control from below” as control. SD’s mind lives inside DOJ structure, and not everybody can or even wants to follow him there, but in a DOJ-centric problem, I gladly adopt his framework of seeing things, because it works like crazy for me, too.
Sundance’s warm-up revelation about Tash Gauhar is solving all sorts of problems for me, and is also enough of a reveal of the SERIOUSNESS of the long-term problems at DOJ, that I am on board with SD’s reveal JUST ON THAT ALONE. His big reveal (not the Durham deputy – the OTHER reveal) HAS TO BE in the space I’m computing, and that space is dangerous as hell to America, and must be revealed before the election, whether Barr is going after it or not. I’m not fully sure what it is, but just the SET OF POSSIBLES is enough that any sunlight becomes good sunlight, Barr or no Barr. IMO.
TheseTruths
I do see control from below as control. I would very much like to know more of your thoughts about your last paragraph. An article about that would be great (if I may be so bold!)!
"Durham" is the shiny thing to keep everyone distracted and looking in the wrong place. The real investigation has nothing Durham attached to it. You can debate the Barr strategy later on. I care not. https://t.co/vxmc9lUKqF
SD is also saying that he will reveal to selected journalists on FRIDAY, and will reveal to US on Saturday.
NOW – here is my problem.
Not everybody here wants to see Sundance stuff, which can be – WELL – for many people, especially Q people, demoralizing. I expect his reveal to be BEYOND controversial – I believe it will OFFEND and OUTRAGE, drawing mockery and derision, even if people claim it’s a nothingburger. It will stir the pot – as intended.
So I’m going to make three proposals about where I will discuss “Sundance stuff”.
keep it in the daily open – DEAL WITH IT – FIGHT OVER IT
separate posts, NOT in the daily open – KEEP IT AWAY
on The U Tree
I can live with any of these, but I currently believe “other posts here” is the best for all concerned. Let me know what you all think. It will happen before morning.
Thanks!
The LancetGateEffect
Repeating from last week, I continue to harp on the “LancetGate Effect”.
This is the article that brought it to my attention:
I alerted administration HCQ advocate Peter Navarro to this (having no idea if he saw my tweet – only TWITTER and the DNC and the CCP know), because I think there is a “knowledge crisis” here. Waiting too long for published data (by the same publications which were victimized by LancetGate, no less!) showing we’re killing people by letting the media badmouth a “best current early treatment”, is a RISK to many – science, the people, AND this administration – maybe even to its enemies, who will ultimately pay for an increasingly costly crime.
Peter – another "real time effect" exists for the FDA 6/15 decision. It's also a "LancetGate" effect, ironically started AFTER Swiss reinstatement of #HCQ on 6/11. Different delay – the shorter time from infection to viral test. Amazing proof. READ: https://t.co/lDV7XMyGzbpic.twitter.com/owqX6AMPUD
For those who are put off by the reciprocal graph, here is the data viewed more traditionally. Same point – a causally timed inflection point in cases when shadow is thrown on #HCQ by the out-of-date 6/15 (retracted) #LancetGate diss during rescinding of the EUA by FDA. pic.twitter.com/0FXd20tiMT
I really think we need to thoroughly explore this possible ‘TRAP’ (Damned if he does, damned if he doesn’t) so we understand it.
Gingersmom2009 earlier was saying that President Trump is ‘Weak’ because he did not use an E.O. to overrule the ANTI-HCQ SABOTEURS in the CDC, FDA….
… I and don’t want to be that floating turd — but someone was pretty strident here in a reply to me yesterday AM about the Stanton Act and how POTUS can’t go against Fauci/Birx or he’ll be removed from office. The EUA is exactly what needs to happen….
That was me.
DP, Ginger, and others.
Causualties in nursing homes was done PRECISELY to get the reaction you have. These people have spent over 100 years perfecting the methods of ‘herding you’ into the direction they want you to go
AND THEY ARE PURE EVIL….. [start of a long comment]
[MUCH REMOVED]
I can understand why DP, Ginger, and others are furious and want POTUS to DO SOMETHING! I am livid too. I am so angry that if a Karen demonrat gets in my face about masks I would probably punch them…
HOWEVER, I can step back and I THINK I SEE A TRAP.
So what say you?
Is POTUS sidestepping a trap? Or is he ‘weak’ in not using an E.O. to address the HCQ issue?
THIS is a beautiful demonstration of how politics and science are interacting BADLY, and why we need to keep both politics and corporate money OUT of influencing science judgments.
We will deal with part of this below, in something I call “therapeutic agnosticism”.
For now, I think it’s very legitimate to ask about Trump’s relationship with both the health bureaucracy – much of which OPPOSES HIM and SUPPORTED HILLARY CLINTON – and with the corporate and NGO behemoths – much of that world controlled by Bill Gates – and most of which is also politically opposed to Trump.
I think that the other side will weaponize ANYTHING, and yes – I think they may well have been trying to trap Trump on HCQ.
In my opinion President Trump has done enough. He has been honest about his belief in HCQ, but he is letting the medical pros make decisions, and they will answer for any mistakes.
If FDA scientists don’t reverse course on HCQ due to the LancetGateEffect, and the evidence keeps rolling in, then I believe Azar and Hahn will have all they need to clean the place out very soon.
There are constructive paths forward – I’ve suggested one already, but there are others. Any EUA or other action which broad-brushes early use of more antivirals and explicitly includes HCQ is fairly absolving without spotlighting, and serves the interests of both “big pharma” and “people’s pharma”.
Note that remdesivir has been approved for more widespread use. If that use can be moved forward in time, such as allowing an early bolus injection “somewhat off label” or EUAed under doctor’s supervision, early in HCQ COVID treatment, and it gives improved results (I would almost bet on it), then patients, doctors, and researchers all benefit. Likewise, EIDD-2801 and RLF-100 need to be tried earlier, IMO.
Yes, to some extent this is expensive “boutique medicine”, adding big costs for small percentages of better outcomes, but honestly, THAT is exactly why people have private insurance and THEIR OWN preferred providers and drugs. Research is expensive, well-heeled customers who will spare no expense WANT that extra edge, so it’s a match made in capitalism.
If the MONEY can get these new fresh drugs WHEN THEY NEED THEM, and those who want cheap and reliable HCQ can get THAT when they need it, then hopefully we can all benefit – most of all insuring that patients are not dying of this minor but annoying flu which – I have to say on now-sketchy lungs – is not exactly as minor as the usual coughs and colds, even if it is, for most, more minor than regular flu.
So let’s talk about therapeutics in general, but FIRST just one of them.
Ivermectin & COVID-19
Thanks to bakocarl for turning me on to this article, which has proven very enlightening as I’ve dealt with the PROCESS of understanding it at a general level.
I had promised that I would do an explainer on this, and to some extent I already did, in comments, but I want to get some deeper thoughts out there. Also, this topic brings up the issue of “therapeutic agnosticism”. This is about not just STATING conflicts of interest in backing or not backing particular therapeutics, but DEALING with those conflicts – ADDRESSING THEM – very openly. Thus, I explain this idea more fully below.
If you search through the whole article, you will NOT find zinc mentioned AT ALL, and any time zinc is not controlled, an HCQ or HCQ+AZT study is operating with a loose wheel, in my opinion.
This becomes even more important because of the way the CONTROL for the ivermecting (IVM) add-on was done.
The control study for IVM+HCQ+AZT was done by RETROSPECTIVE ANALYSIS of earlier hospital treatment using HCQ+AZT alone. The authors understand fully the limitations of doing this, and I agree with them fully – it is better to do a potentially flawed study here than none at all. There is a strong ETHICAL argument for comparing PAST BEST to NEW BEST – and one doesn’t have to invoke Melania to know it’s right – DOING BEST is BEING BEST!
Using dice to send some patients to WORSE TREATMENT is not a braggable thing. Better to take some lumps on uncertainty, IMO.
What are the risks of comparing two hospital studies NOT done at the same time – where one of them is designated a “control”?
“Control” assumes that you’ve changed exactly what you know you changed – it means that you have a reliable reference, preferably MINIMIZING differences that have to be explained away.
Yes, it’s the same hospital, the same doctors, the same staff, but we all know that treatment for COVID has changed MASSIVELY over time. Here are important changes:
less vents
more steroids
better diet including vitamins and minerals to resolve deficiencies
more oxygen earlier
better testing, all kinds
As you can see, there are reasons for outcomes to be better now, completely independent of the study object, ivermectin. NEVERTHELESS, the authors DO see better results – significantly better – if they give patients a big dose of IVM at the beginning of HCQ-AZT treatment. They do as much correcting for differences as they can, in comparing individual outcomes, and I believe they tried to do a good job.
Skipping past how I got there, my reading of this is that IVM is very likely acting a LOT like AZT (azithromycin, Z-pak, AZM, whatever). It is providing a SHOTGUN for unicellular and multicellular organisms, weighted toward PARASITES. It has a different SPECTRUM from AZT, and will complement it. This will affect both pre-existing and new infections.
It is EXTREMELY LIKELY that this should work, even if IVM has NO ANTIVIRAL ACTIVITY.
It’s beautiful science – and also explains why the “pro-crisis” camp would oppose use of ivermectin.
The argument isn’t whether ivermectin is an antiviral, or any worse or better than anything else. The argument is whether is can be used to save lives, and how well it does that, versus something else – including simply NOT USING IT.
If these results hold, or are even partially confirmed, then I think ivermectin needs an EUA along with HCQ and several other new antivirals, for doctors to begin solving things EARLY with antivirals and “therapeutic adjuvants”, when they work best, as I mentioned LAST WEEK.
Now, let’s talk about therapeutic agnosticism.
On Staying Therapeutically Agnostic
Now – we have seen incredible bias against hydroxychloroquine – nicely summarized HERE:
Dr. Harvey Risch, MD/PhD from the department of epidemiology at Yale responds to the senseless attack and attempt to discredit him for his research on hydroxychloroquine.
If you get into that article, you will see where “the powers that be” try to KNEECAP hydroxychloroquine into “hospital use only” – which absolutely does not make sense, until you realize that one of the more unique problems of the new and just recently approved antiviral drug remdesivir (which Fauci labeled the “new standard” despite unimpressive performance in late-stage COVID), is that the drug needs to not only be administered by IV, but it also has to be observed closely for nasty side effects, and thus being up until recently stuck in a late stage, hospital patient track, which is NOT a good place for antiviral success.
SO – rather than getting remdesivir into earlier settings, what did they do? What the CHICOMS routinely do – KNEECAP THE COMPETITION in some way that nobody sees.
Honestly, if you’ve been in science and been halfway observant, you’ve seen how the corrupt ChiComs operate – MAFIA techniques – frequently SABOTAGING the other guy, although perhaps not until AFTER stealing the technology – so they seem to be quite comfy with the general lack of morality of the growing “medical mafia” in the US.
A match made in HELL.
Anyway – here is the deal.
We do NOT want to be like them THE OTHER WAY.
don’t cheer the failure of ANY drug – figure it out and fix it
every drug is different – help them ALL find their perfect niche to help us
never ever conduct a sabotage study like LancetGate
don’t reject studies “going the other way” – UNDERSTAND AND EXPLAIN THEM
call out sabotage, bias and error, no matter who is committing it
if you know why “the other guy’s drug” is FAILING, you are morally obligated to help fix it
if you know why “the other guy’s drug” is WORKING, you are morally obligated to explain and even recommend it
pharmacology is not a zero sum game, even though patients are a zero sum market – every new drug adds to the arsenal of salvation
In short, I wish for people who are fighting the suppression of HCQ to not become deniers, defamers, and “opponents” of other drugs and vaccines, because doctors need those too, for patients who want or need those specific drugs or treatments.
LIVE AND LET LIVE.
Even if the other team doesn’t play that way.
By this attitude, we will DEMONSTRATE the superiority of our approach, which I sometimes call POPULAR MEDICINE.
Masks OFF
The fly in the ointment that mocks the smooth, lying MASK SOCIALISTS is SWEDEN.
“With numbers diminishing very quickly in Sweden, we see no point in wearing a face mask in Sweden, not even on public transport.” -Swedish State Epidemiologist Anders Tegnell, 7/28/20
This wonderful meme comes from Aubergine. I also used it HERE:
Wake up! I can MEASURE my oxygen hurt by all 3 of my masks, using my pulse oximeter. It's mild, but it's persistent and long. 97 (sleepy) is not 98 (calm) is not 99 (alert), and 93 is where they take you to the hospital.
We need to start thinking about measuring things, because I am CERTAIN that masks are hurting us – nickeling and diming us to death.
I am having success understanding oxygen deprivation using my cheap oximeter, but I need perhaps a more expensive model to take finer cumulative readings and record them.
Gail Combs suggests that we can capture mask CO2 as well.
Let us think about this problem, because I am certain that CHINA is behind it.
I will add details later of why I believe normal mask wear leads to cognitive deficits for 30-60 minutes AFTER shopping with a mask.
This [(10*Q) + 7]TH of AUGUST FRIDAY where Q = 0 open thread is OPEN – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA / KAG! / KMAG world (KMAG being a bit of both MAGA and KAG!).
We're big over the target on this one!
PREDICTION: The #LancetGate effect of increases in both DEATHS and INFECTIONS upon banning of #HCQ will show up in all countries that reacted to the paper, including several which have not been publicly mentioned yet.
You can say what you want, comment on what other people said, and so on.
Free Speech is practiced here. ENJOY IT. Use it or lose it.
Keep it SOMEWHAT civil. They tried to FORCE fake Orwellian civility on us. In response, we CHOOSE true civility to defend our precious FREEDOM from THEM.
Our rules began with the civility of the Old Treehouse, later to become the Wolverinian Empire, and one might say that we have RESTORED THE OLD REPUBLIC – the early high-interaction model of the Treehouse – except of course that Q discussion is not only allowed but encouraged, and speech is considerably freer in other ways. Please feel free to argue and disagree with the board owner, as nicely as possible.
Please also consider the Important Guidelines, outlined here in the OLD January 1st , 2019 open thread. Let’s not give the odious Internet Censors a reason to shut down this precious haven.
The following is an excerpt from the brief being filed today in Maryland state court in Attkisson v. Rosenstein and others for the government computer intrusions.
Plaintiff Sharyl Attkisson, an award-winning journalist—along with her husband and child—have tried for years to pursue their significant and credible claims of illegal government surveillance, but the U.S. Government has stonewalled them at every turn. Yet, despite the Government’s repeated efforts to obfuscate and delay, the Attkissons detailed in their Complaint:
Expert forensic computer analysis of the Attkissons’ computers, revealing that an unauthorized entity or entities gained remote access to the Attkissons’ computers for a prolonged period, and that one of the pathways by which the intrusions occurred were IP addresses controlled by the U.S. Government.
Confirmation, via testimony, that the U.S. Government controlled the IP addresses identified in the Attkissions’ computers.
The degree to which senior figures in the Department of Justice were concerned about, and took steps to block, Sharyl Attkisson’s reporting, as well as her use of confidential governmental sources;
Many documented instances of abnormal, otherwise unexplained behavior of the Attkissons’ computer systems and devices.
But then it gets interesting…..
Plaintiffs’ investigator has interviewed Ryan White, a Government whistleblower (and named Defendant). During this interview, White made the following significant assertions:
White worked with defendants Sean Bridges (who was then a Secret Service agent) and the FBI’s Shawn Henry in Baltimore and reported directly to defendant Rod Rosenstein.
White and Agent Bridges were ordered to conduct various clandestine operations involving hacking computer systems, servers, emails, and phones.
White and Agent Bridges were directly involved in the illegal surveillance of the Attkissons’ computers and the exfiltration of data.
The rogue order to target the Attkissons came directly from Agent Henry and Rosenstein.
Later, Agent Bridges and another federal agent were convicted of corrupt acts for their involvement in the Government’s notorious Silk Road Task Force, also based in Baltimore, in which corruption by federal agents was uncovered, resulting in the convictions of Bridges and another federal agent.
As far as I can tell, the surveillance of journalists at that point (2009-2012) was coming from Obama and ERIC HOLDER. So if Rosey was working Holder’s game under Obama, this fits in perfectly with everything I know about DOJ intentions and actions during the first 2 years of the Trump White House, when Rosey and Holder’s lieutenant Tashina Gauhar were running the show.
Rosey sure looks like a black hat to me. But I’m listening. If Rosey was an informant, then WHO was he informing under Obama and Mueller, as Mueller was clearly allowing spying on Attkisson, and planting of incriminating documents on her laptop?
But let’s move on, since Rosey’s guilt or innocence may be reflected in any upcoming indictments…..
Trump’s tweet on the getaway is wonderful. Sundance clearly SAVED it, lest it disappear. Or DID IT ALREADY? I cannot find it.
ANYWHO – indictments are very likely coming SOON.
This is worth a listen (in thread). I take it as a tip that there will be some predictable turbulence when indictments hit, and security has already prepared for it. Seatbelts. https://t.co/pUx0Xui5K3pic.twitter.com/0B2ZAGrCBw
Scientifically, this is exactly where I was when Didier Raoult (or Raoult Didier – whatever his name is) published his first “pay dirt” data with demonstrable dose-related antiviral activity in ALL test subjects. His numbers can be off by a factor of 50%, and it’s still huge and can’t be explained away as anything but SOME kind of real effect.
Numbers like these are either massive fraud or pay dirt. And they could be real nuggets. With a solid, known antiviral explanation, it’s almost certainly REAL.
Now – let’s take a look at a country a bit off the commonly argued map. You don’t hear a lot about COVID-19 in Turkey. Here’s why.
The situation isn’t done in Turkey – they are teetering very close to lockdowns. Turkey is trying the same thing as Trump – avoiding lockdowns. A lot of information on how hard that has been, in this article.
Scott Adams found Turkey’s claimed near-100% effectiveness of contact tracing a bit unbelievable, and I have to agree – it’s not easy to either prove or disprove such a claim, but in a country like Turkey, it should be nearly impossible to contact everybody catching the disease.
Who believes Turkey has an extensive testing/tracing network that is making a difference? https://t.co/HMvMWsSekb
NEVERTHELESS, those people who DO get caught by contact tracing ARE very likely to live, if they are getting HCQ as early as possible. See how that works? The more the tracers catch, the more contacts they find, the more contacted contacts are WAITING FOR SYMPTOMS with their HCQ in hand, and the more likely the HCQ is going to work. Clearly, [HCQ + contact tracing] makes sense. BUT here is the deal. People have to TRUST the government behind it.
Not exactly easy in New York.
Moving on, HERE is the biggie. I call it the “LancetGate Effect”.
Yes, that would be THE Steven Hatfill, falsely accused by Mueller in the 2001 anthrax attacks.
BUT WAIT – THERE’S MOAR.
Peter Navarro – THE KILLER – tweeted the article.
Dr. Steven Hatfill's clutch hit. Best take down of anti-Trump Hydroxy Hysteria media this side of @ScottAdamsSays CNN might be killing tens of thousands. https://t.co/b4ThfIaQvG
And then I introduced HIM to something even more shocking.
There was a LancetGate Effect in The United States.
Peter – another "real time effect" exists for the FDA 6/15 decision. It's also a "LancetGate" effect, ironically started AFTER Swiss reinstatement of #HCQ on 6/11. Different delay – the shorter time from infection to viral test. Amazing proof. READ: https://t.co/lDV7XMyGzbpic.twitter.com/owqX6AMPUD
For those who are put off by the reciprocal graph, here is the data viewed more traditionally. Same point – a causally timed inflection point in cases when shadow is thrown on #HCQ by the out-of-date 6/15 (retracted) #LancetGate diss during rescinding of the EUA by FDA. pic.twitter.com/0FXd20tiMT
Now – I’m not going to show you this – you have to dig to find – but in the wake of my comments, Daughn came in for an assist, and we were then both engaged by HCQ opponents. One kept emphasizing that FDA head Hahn, who was in charge when the EUA was rescinded, is a Trump appointee – like this was going to bother me somehow.
NO. TRUTH IS TRUTH.
I thought this was clearly an attempt to generate “Alinsky fears” – specifically POLITICS BEFORE SCIENCE, because it might hurt Trump or Hahn, as a way of shutting me up.
NONSENSE!
Hahn, as I tried to explain, has his own mind. I LIKE THAT. It’s like the way things used to be. I believe that Trump hired him because Hahn is a strong believer in FAST TRACKING new drugs, like Trump is. A believer in TRUMP TIME. Hahn’s opinion on HCQ, wrong as it turns out to be, is secondary. This is WAR, people make mistakes, people die. Generals and Colonels live with this horrible responsibility, and WE SOLDIERS SUPPORT THEM.
BUCK UP, WORLD. We do our best, we trust in God, but we do NOT lie and cover up when we understand error. People have been all over the place on HCQ, but when the chips come in STRONGLY that it works, and even more so that banning it is a PROVABLE mistake, we have to consider CHANGING COURSE.
One way to do that would be to listen to Dr. Zelenko and have a NEW EUA (Emergency Use Authorization) for HCQ – this time without Rick Bright’s toxic “hospitals only” poison pill attached.
YES! We can RECOVER from the LancetGate blunder by doing what Zelenko suggests.
BUT WAIT – THERE’S MOAR.
HCQ Insights
One way to make Zelenko’s new EUA actually happen would be to INCLUDE NEW DRUGS – albeit handled DIFFERENTLY from HCQ, as part of the EUA.
I call this the “EUA EUA“.
“Early Use of Antivirals Emergency Use Authorization”
The way this would work is to grant flexibility to doctors WORKING WITH pharmaceutical companies and state governments to try new antivirals early in the disease process upon confirmed diagnosis. HCQ is well-tested, and as the “standard of this EUA”, it becomes the GOLD STANDARD of safety and efficacy for other newer drugs to beat, using whatever delivery tricks and codrugs make these other drugs work best. Those drugs need every advantage we can find for them, just like South Korea (zinc), Didier Rauout (azithromycin), and Zelenko (zinc + azithromycin, very early) found for HCQ.
One of my rationales here is that we can reduce or even remove toxicity from the equation by low-dosing a lot of these drugs, since EARLY use can mean less drug needed for the more toxic ones. In some ways, what I am doing here is learning from sabotage studies of HCQ, which used massive and toxic doses LATE. We are doing the opposite – trying to “help” alternatives to HCQ by giving THEM access to patients at the same time when HCQ works best. Some – maybe even most patients may still opt for HCQ, but others may welcome new drugs like EIDD-2801 and RLF-100, the latter of which may prove to be effective not just late, but early as well.
The point is, get EVERYBODY early, so we remove the incentive to let patients deteriorate, which is now “imposed” on drugs which need desperate patients for “right to try”. The EUA, in essence, would EXPAND right to try to early or even asymptomatic patients – not just patients at death’s door.
The EUA EUA *removes* any incentive to delay treatment, or to bash HCQ, but at the same time, it doesn’t blockade new drugs from access to patients at the time when THEY might be very effective, too, which our current system, weirdly, does.
WIN, WIN, WIN.
#LancetGate had a terrible price! #HCQ bans and discouragements KILL.
I think a new EUA that included both #HCQ *and* other drugs in the pipeline having antiviral actions, FOR EARLY USE (badly needed for antivirals) is the big life-saver, that would get buy-in from Big Pharma. pic.twitter.com/Dt3Fb5NXUZ
This will not only help absolve @US_FDA on the #LancetGate-effect downside of rescinding the prior EUA (by compensating quickly) – it will provide HCQ as an automatic standard to beat with new agents in compassionate horse-races EARLY. Basically moves up "right to try".
The fundamental problem we're ALL facing is what @zev_dr saw first – antivirals need to be early, but we perpetually move risks LATE in treatment (for good reasons). But I believe super-early and *LOW DOSE* may be KEY to next-gen agents AND antiviral therapies, avoiding tox.
I'm very excited about EIDD-2801 and RLF-100, with the latter now in use LATE. Opening up early treatment and letting HCQ be the punching bag old coach standard will breed champions. pic.twitter.com/MWGHYWG8eh
NOW – about HCQ alleged toxicity. Here is an AR-15 of logic to take down trolls.
It’s important to address the cardiac toxicity issue head on, because that “problem” is really a deflection by people who “pretend not to know” how minor the problem really is, ESPECIALLY compared to LIVES SAVED.
This is JUST AS TRUE as it was with MALARIA.
Yup. MAMET PRINCIPLE. And behind that – AUBERGINE’S RAZOR.
Systematic review of cardiac complications attributed to routine hydroxychloroquine use…
From the years 1963-2017:
– Only 50 events of cardiac toxicity (since 1963!) – Total of 12 deaths – Median patient had been taking HCQ daily for 8 YEARShttps://t.co/5hgnw6qccH
Now – here is one reason I think that NON-VACCINATION AND TREATMENT is an important option.
One of the primary reasons to use HCQ instead of a vaccine, is the likelihood that coronavirus vaccines will cause immune overreaction TO infection by the disease, instead of actual protection FROM infection.
This is a nice article which introduces you to Dr. Peter Hotez, vaccine maker, vaccine advocate, but also vaccine truth-teller on immune enhancement. Hotez is somebody very difficult for the MSM to downplay and crush. At least, SO FAR.
Scientists were close to a coronavirus vaccine years ago. Then the money dried up.
“We just could not generate much interest,” a researcher said of the difficulty in getting funding to test the vaccine in humans.
March 5, 2020, 4:30 AM EST / Updated March 8, 2020, 4:23 PM EDT
There will be more talk about immune enhancement later. Be prepared. It’s a very “sciencey” argument AGAINST mandatory vaccination. It is a much more EFFECTIVE argument than “I don’t trust Bill Gates” – even though the latter is a HUGE motivator for most people.
And now THIS.
Time To Go To WAR Over Hydroxychloroquine
What are we up against?
Something that runs us over if we DON’T put it down.
This FRIDAY THE JUNETEENTH open thread is OPEN – VERY OPEN – as in LET’S OPEN UP ALREADY – but don’t open up on a looter unless the LAW is on your side – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA / KAG! / KMAG world (KMAG being a bit of both MAGA and KAG!).
You can say what you want, comment on what other people said, and so on.
Free Speech is practiced here. ENJOY IT. Use it or lose it.
Keep it SOMEWHAT civil. They tried to FORCE fake Orwellian civility on us. In response, we CHOOSE true civility to defend our precious FREEDOM from THEM.
Our rules began with the civility of the Old Treehouse, later to become the Wolverinian Empire, and one might say that we have RESTORED THE OLD REPUBLIC – the early high-interaction model of the Treehouse – except of course that Q discussion is not only allowed but encouraged, and speech is considerably freer in other ways. Please feel free to argue and disagree with the board owner, as nicely as possible.
Please also consider the Important Guidelines, outlined here in the OLD January 1st , 2019 open thread. Let’s not give the odious Internet Censors a reason to shut down this precious haven.
SPEAK THE FIVE WORDS BOLDLY TO OUR PRESIDENT!
“I AM PRAYING FOR YOU!“
AND WHAT TIME IS IT?
TIME TO….
DRAIN THE SWAMP
Our movement
Is about replacing
A failed
And CORRUPT
Political establishment
With a new government controlled
By you, the American People.
Candidate Donald J. Trump
Also remember Wheatie’s Rules:
No food fights.
No running with scissors.
If you bring snacks, bring enough for everyone.
Seriously – FRANCE just banned use of HCQ for treating COVID-19.
DUMB!
Looks like there is going to be a SCIENCE and MEDICINE FIGHT in the middle of RIOTS and DECLAS.