“We do not believe any group of men adequate enough or wise enough to operate without scrutiny or without criticism. We know that the only way to avoid error is to detect it, that the only way to detect it is to be free to inquire. We know that in secrecy error undetected will flourish and subvert.” –J. Robert Oppenheimer
RDS in the following comment points out one of the problems we have in waking up the Sheeple. There are highly ‘respected’ doctors and PhDs, who write papers in prestigious journals backing the mRNA vaccines even though they KNOW they are unsafe.
Wolf Moon OMG, this article below is a must-read. Linked from an AMA EdHub email one received today. It’s a JAMA piece written by Dr. Peter Marks — he’s the head of the CBER department of the FDA (Center for Biologics Evaluation and Research). Dr. Marks was in on the ground floor of Operation Warp Speed. Dr. Marks KNOWS EVERY DATA PIECE SUBMITTED TO THE FDA FROM PFIZER-BIONTECH ABOUT THE CLINICAL TRIALS FOR BNT162b2 BACK IN 2020 — AND EVERY DATA PIECE SINCE THEN ALSO. Dr. Marks was in on recommending that the FDA authorize the UNPROVEN, ONLY TESTED ON 8 MICE new “COVID-19 + Omicron BA.4 + Omicron BA.5 booster shot.” His linked article below is a screed for the development of “new” and “different types” of COVID-19 “vaccines” — including ones that specifically target the T-cell response in the body. Dr. Marks KNEW that the “vaccines” developed during Operation Warp Speed and given quick EUAs by the FDA WOULDN’T DO THE JOB: From his article: “One potential model for approaching such development [of a COVID-19 vaccine] was used successfully at the beginning of the pandemic when Operation Warp Speed evaluated numerous global vaccine types and focused on advancing several promising candidates, knowing full well that most would ultimately not be found to meet the criteria set forth for a safe vaccine with adequate efficacy.” (bolding and Italics mine) Dr. Marks represents the “medical establishment” and DeepState. IMO, the “medical establishment” and the DeepState have it as their business to continue to put these dangerous COVID-19 “vaccines” into people — and develop new “vaccines” to keep damaging / destroying the immune systems of those who take them. His article: https://jamanetwork.com/journals/jama/fullarticle/2799600 December 9, 2022 “Urgent Need for Next-Generation COVID-19 Vaccines” Peter Marks, MD, PhD https://www.youtube.com/watch?v=Nat1za4sKjA As an additional note. For those who might wish to watch the documentary it is available to watch free until the end of January. All that is required is your email I think. The link follows. https://therealanthonyfaucimovie.com/trailer/
In addition to censorship and smearing of dissenting voices, hospitals and doctors were getting the carrot and stick treatment – Lose your license OR getbig bucks for pushing bogus PCR tests, ventilators, Remdesivir and killing patients. – For example “A COVID-19 diagnosis provides extra payments to coroners!”
To make sure the Sheeple could not make a solid connection between the Covid Vaccine and death, the shot is a slow ‘poison’ with a variety of adverse reactions.
The CDC has been hiding the Social Security Administration death master file. I got it from a whistleblower. This shows deaths are taking 5 months from the jab to happen. This is why it’s hard to see.
Remember this time factor as we look at the data I found.
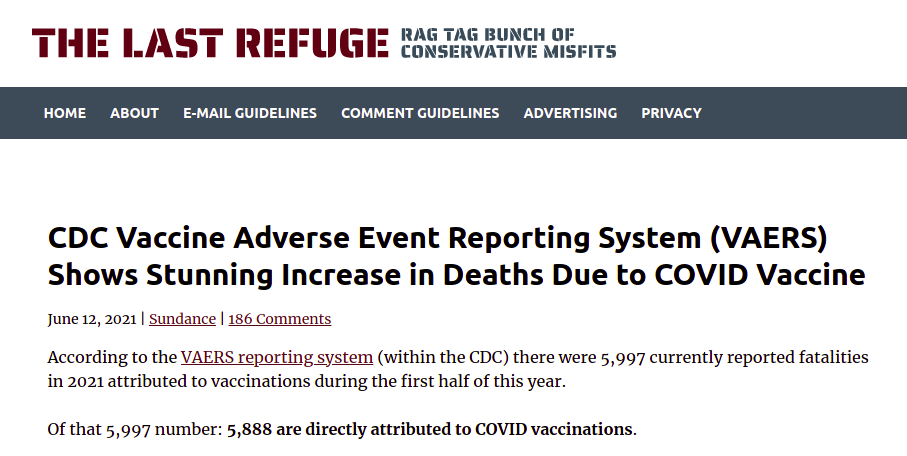
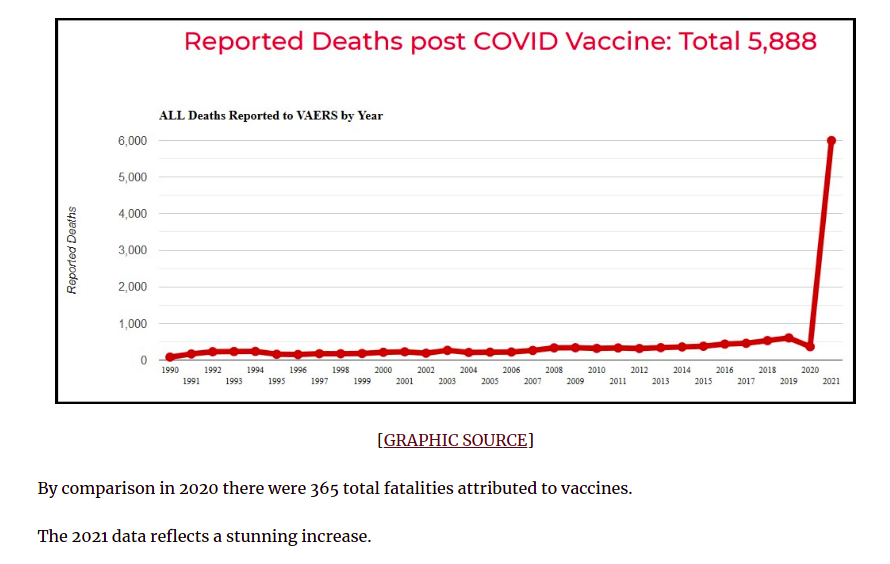
Finally we have the DELIBERATELY compromised VAERS system that is SUPPOSED to alert the CDC and FDA to harmful drugs.
There are major problems with the vaccine adverse event reporting system (known as VAERS) which the CDC considers the “front line” of vaccine safety. VAERS was created in 1990 by the CDC and FDA as a means to collect and analyze adverse effects that are associated with vaccines. Unfortunately, the failings of VAERS are “kept from the consciousness” not only of the public, but also from the doctors, pediatricians, and nurses that the public rely on to provide reliable information as to the safety of vaccines. I say “kept from the consciousness” rather than “kept secret” because while these failings are publicly disclosed for all the world to see, they are for all intents and purposes BURIED in documents seldom searched out by the average member of the medical community, much less by the average individual. You could say that the information has been very effectively hidden in plain sight…
In 2000, the 6th Report by the Committee on Government Reform addressed the failings of VAERS in its address of the Vaccine Injury Compensation Program…. [The] Congressional report notes (on page 15), “Former FDA commissioner David A. Kessler has estimated that VAERS reports currently represent only a fraction of the serious adverse events.” (emphasis by author)… That leads us to the interesting case of the CDC and Harvard Pilgrim Healthcare Inc.
The Department of Health and Human Services (HHS) gave Harvard Medical School a $1 million dollar grant to track VAERS reporting at Harvard Pilgrim Healthcare for 3 years and to create an automated reporting system which would revolutionize the VAERS reporting system- transforming it from “passive” to “active.”…
I’ll quote the findings directly from the report,
“Adverse events from drugs and vaccines are common, but underreported. […] Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of ‘problem’ drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed.”
Again, let’s stop and think about this revelation for a moment: fewer than 1% of vaccine adverse events are reported. The CDC’s entire vaccination propaganda campaign rests on their claim that side effects from vaccination are exceedingly rare (and predominantly minor).According to the CDC, in 2016 alone, VAERS received 59,117 vaccine adverse event reports. Among those reports were 432 deaths, 1,091 permanent disabilities, 4,132 hospitalizations, and 10,274 emergency room visits. What if these numbers actually represent less than 1% of the total as this report asserts? Simple multiplication would yield vaccine adverse events reports numbering 5,911,700!…
the United States of America Centers for Disease Control ghosted Harvard Pilgrim Healthcare, Inc.
“the practice of ending a personal relationship by suddenly and without explanation withdrawing from all communication.”
Personally, I would hope that I could hold an organization like the CDC to a higher standard, but… After a one million dollar grant was paid and three years of research conducted on what appeared to be a very successful upgrade to the passive VAERS system, the team’s CDC contacts went MIA
. The ESP:VAERS final report states, “Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.”
So in 2017, the CDC DELIBERATELY left a useless reporting system in place when they had the opportunity to upgrade it.
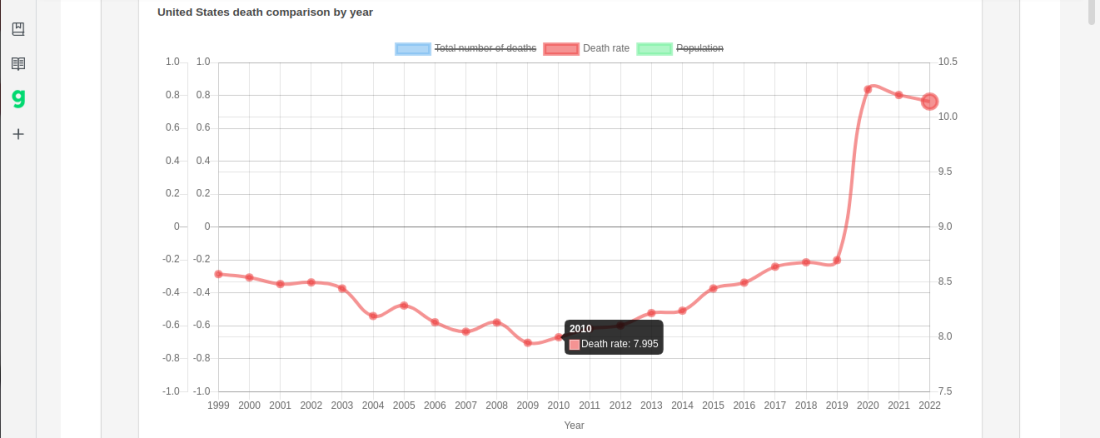
Since the VAERS data set is compromised as well as next to useless, I decided to see if we could find another way to connect the mRNA vaccines to deaths. There is a nifty site called Dead or Kicking.
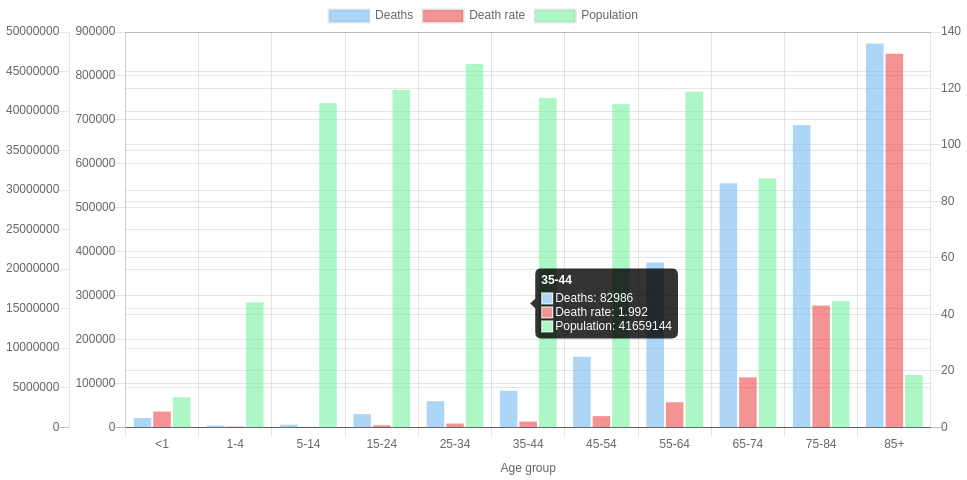
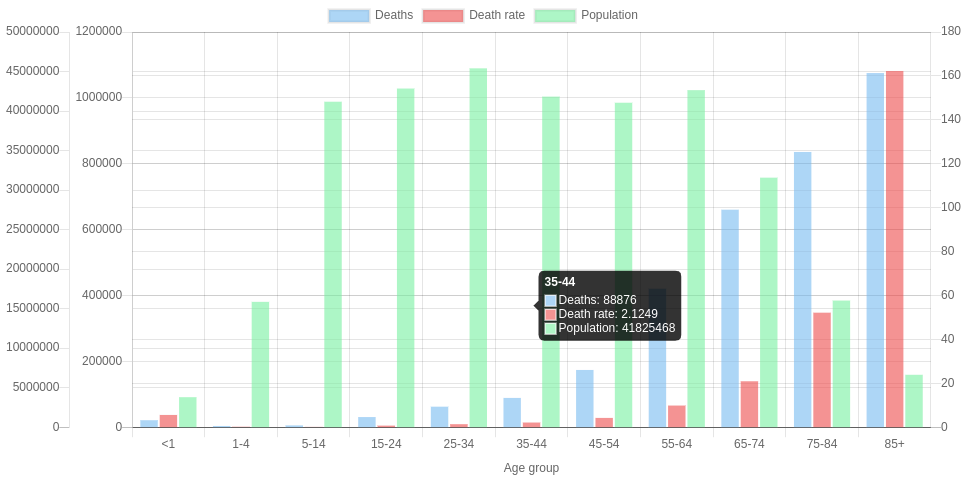
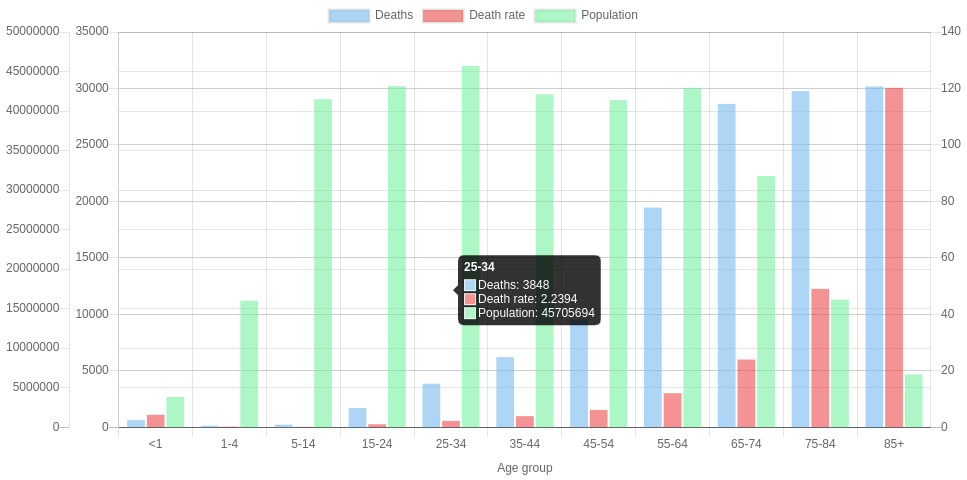
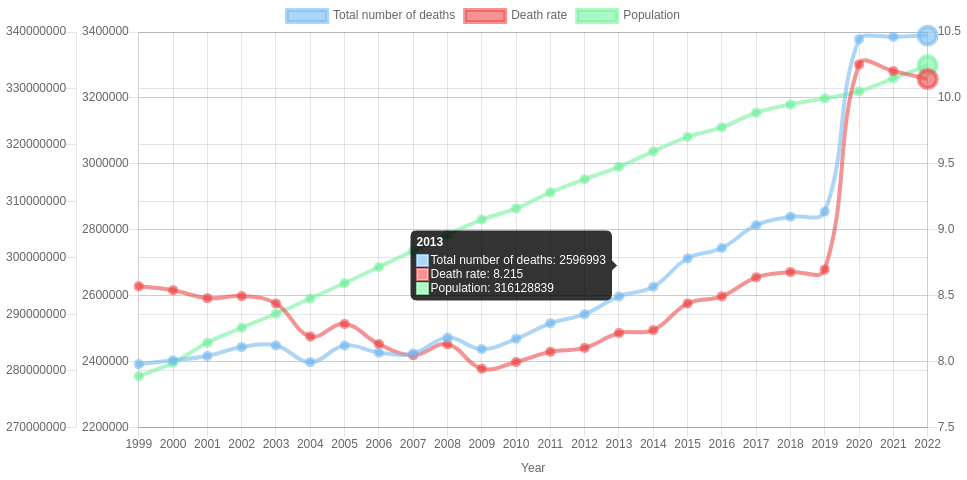
there is the graph “United States death comparison by age in 2020“
By changing the date in the URL you get the different years AND if you place your mouse over the graph, it will give you Deaths, Death Rate and Population for each age group.
You can save the graphs for any year – or all of them – as examples, as Wolf did below. Right-clicking on a graph lets you “save image as” or “copy image”.
2019
2020
2021
2022
Note Added By Wolf – CHECK THIS ONE OUT!!!
I originally thought I would see a major drop in the population over 75 but that did not happen since the Baby Boomer cohort is filling the 65+ age groups faster than the orchestrated depopulation can kill them. Notice there are less people in the 45 to 54 age group than in the 55-64 age group. That is a REAL PROBLEM for the Cabal.
…The Social Security Trust Fund should currently have $2.5 trillion in surplus. So how is it that these checks could stop being issued if the debt ceiling isn’t raised? Economics professor Dr. Allen Smith, author of The Looting of Social Security: How The Government is Draining America’s Retirement Account, has been reporting on the theft of Social Security funds for years….
Age / Date
2019
2020
2021
2022
85+
6,604,958
6,628,013
6,673,175
6,715,875
75-84
15,969,872
16,022,410
16,139,651
16,250,631
65-74
31,483,433
31,571,207
31,773,610
31,970,852
55-64
42,448,537
42,643,579
42,929,850
43,208,648
45-54
40,874,902
41,050,404
41,371,452
41,683,591
So I created another table this time of USA Death Rates by age group by year. I included 6 years before covid as a baseline. Then the two years, 2019 & 2020, when Covid hit the USA plus the two years, 2021 and 2022 when the mRNA vaccine was progressively rolled out, starting with adults, then school age children and finally babies.
Also there was the DELIBERATE mis-diagnosis of flu and pneumonia followed by refusal to treat until the person was so sick they needed to be put on a ventilator & remdesivir thus killing up to 88% of those patients.
The result of all of this, is the most vulnerable elderly had already been killed off in 2020 as the much higher death rates for 2020 shows, but by 2021 and 2022 the death rates decrease from that high. Although the elderly were vaccinated, unlike athletes and younger, physically active people, the elderly are going to be a lot more sensitive to what their bodies are telling them and NOT pushing it. They are also more likely to have doctors checking their heart health and be on heart and circulatory medications.
Myocarditis is an important cause of arrhythmias and sudden cardiac death (SCD) in both physically active individuals and athletes.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
RETIREES 65 to 74
The 65 to 74 group is going to be a mixed bag. Compared to the 75+ group they are less likely to be in a nursing home or to have gotten deathly ill in 2020, although a certain percentage will have died. However they are likely to get the vaccine. Thanks to Medicare, they are more likely to be in contact with medical professionals who would try to talk them into the jab. They are also going to be a lot more physically active than older retirees and therefore stressing their hearts more after getting the mRNA vaccine.
You can see the combination of poor health care in 2020 followed by the vaccines and then boosters as the death rate increases year by year from 2019 through 2022.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
FORCED RETIREMENT/SMALL BUSINESS WORKERS 45 to 64
The 45 to 64 are an interesting group. Corporations force retirements and actively discriminate against those 45 years and up because age discrimination laws have no real teeth. Therefore the people 45 and up are most likely NOT working for ‘Corporate America’ and are either small business people or hired by small business people. (BTDT) This group is the most likely to have had a ‘rude awaking’ about the world we live in and are NOT going to be as trusting. Older people are also more likely to tell their boss to go F..K themselves with the darn needle. Like the 65 to 75 group you can see the increase in death rate year to year but it is not as sharp an increase. They are also more likely to be in better health than retirees. If You’re Over 50, Chances Are the Decision to Leave a Job Won’t be Yours Age discrimination in the workplace happening to people as young as 45: study
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
WORKING AGE CORPORATE AMERICA 15 TO 44
The age group 15 to 44 is the group most likely to show PURE UNADULTRATED DATA about Mortality & the mRNA vaccine although there may be some confounding from drug use increasing over the years. Covid-19 virus has little effect on the death rate in 2020. However as the boosters and the 5 month time delay kicks in you can see the death rate almost doubled in 2022 compared to 2019 and earlier.
….Scott Davison, the CEO of OneAmerica, a $100 billion life insurance and retirement company headquartered in Indianapolis.
“The data is consistent across every player in the business.”
Davison said death rates among working age people –
those 18 to 64-years-old – are up 40 percent in the third and fourth quarter of 2021 over pre-pandemic levels.
“Just to give you an idea of how bad that is, a three sigma or 200-year catastrophe would be a 10 percent increase over pre-pandemic levels,” Davison said. “So, 40 percent is just unheard of.”
He blames it on Covid instead of the mRNA vaccine of course. “…the third and fourth quarter of 2021…” would be after Steve Kirsch’s 5 month window. So far I can not find any 2022 insurance data. HMMMmmmm
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
CONTROL GROUP 1 TO 14
The 1 year to 14 can be considered the ‘Control Group’ Covid has little if any effect on the death rate in 2020. They were not vaxed until quite recently (November 2021) and boosters were not approved until May 19, 2022. The death rate so far has been flat but I would expect an uptick after the first of this year as the effects of the boosters kick in.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
BABIES UNDER 1 YEAR
The Under one year of age is interesting since there is actually a slight dip in mortality. Are weaker babies more subject to spontaneous aborting after Mom is vaxed?
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
TIMELINE of Emergency Use Authorization of mRNA VACCINES
The FDA makes it VERY HARD to figure out just when they authorized the use of the mRNA vaccine in youngsters. I gleaned out the following dates. Starting from the FDA Covid Vaccine site.
Turns out it is the CDC who has the final say on vaccination of children so I have also included the CDC news releases.
12/18/2020 – EUA issued for the Moderna COVID-19 Vaccine, December 18, 2020. Emergency Use Authorization (EUA) of the Moderna Inc. COVID-19 Vaccine for the prevention of COVID-19 in individuals 18 years and older.
YEAR 2021
06/10/2021 — Vaccines and Related Biological Products Advisory Committee will meet in open session to discuss, in general, data needed to support authorization and/or licensure of COVID-19 vaccines for use in pediatric populations.
FDA DEFINES: Pediatric use. (A) Pediatric population(s)/pediatric patient(s): For the purposes of paragraphs (c)(9)(iv)(B) through (c)(9)(iv)(H) of this section, the terms pediatric population(s) and pediatric patient(s) are defined as the pediatric age group, from birth to 16 years, including age groups often called neonates, infants, children, and adolescents.
. 09/17/2021 — Application for administration of a third (“booster”) dose of Comirnaty (COVID-19 Vaccine, mRNA) in individuals 16 years of age and older.
10/26/2021 — Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss a request to amend Pfizer-BioNTech’s Emergency Use Authorization (EUA) for administration of their COVID-19 mRNA vaccine to children 5 through 11 years of age.
10/14/2021 – Vaccines and Related Biological Products Advisory Committee Meeting The committee will discuss the Emergency Use Authorization (EUA) of the ModernaTX Inc. COVID-19 vaccine and the Janssen Biotech Inc. COVID-19 vaccine for the administration of an additional dose, or “booster” dose, following completion of the primary series, to individuals 18 years of age and older.
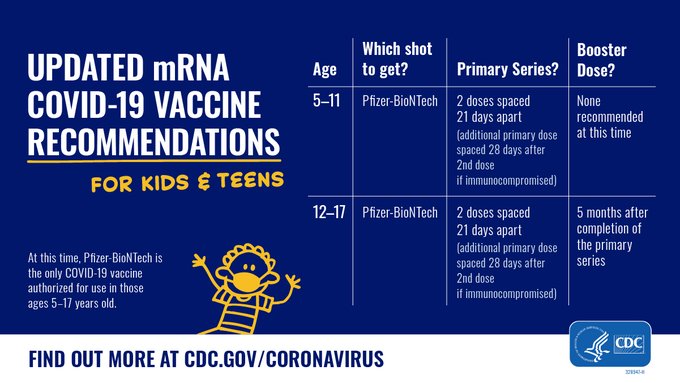
Today, CDC Director Rochelle P. Walensky, M.D., M.P.H., endorsed the CDC Advisory Committee on Immunization Practices’ (ACIP) recommendation thatchildren 5 to 11 years oldbe vaccinated against COVID-19 with the Pfizer-BioNTech pediatric vaccine. CDC now expands vaccine recommendations to about 28 million children in the United States in this age group and allows providers to begin vaccinating them as soon as possible.
The Food and Drug Administration today authorized Moderna’s COVID-19 vaccine for children aged 6 months through 17 years old and Pfizer’s COVID-19 vaccine for children aged 6 months through 4 years old, as recommended this week by its vaccine advisory committee. The vaccines previously were authorized for older children.
Before vaccinations can begin, the Centers for Disease Control and Prevention must recommend the vaccines for these age groups. CDC’s Advisory Committee on Immunization Practices is scheduled to vote tomorrow on whether to authorize the vaccines for children age 5 and under.
Children 6 months through 5 years of age who received the original (monovalent) Moderna COVID-19 Vaccine are now eligible to receive a single booster of the updated (bivalent) Moderna COVID-19 Vaccine two months after completing a primary series with the monovalent Moderna COVID-19 Vaccine.
Following today’s meeting of the Advisory Committee on Immunization Practices’ (ACIP), CDC is expanding eligibility of COVID-19 vaccine booster doses to everyone 5 years of age and older. CDC now recommends that children ages 5 through 11 years should receive a booster shot 5 months after their initial Pfizer-BioNTech vaccination series.
In my opinion, the approval of a “likely safer” coronavirus vaccine is – in the long game – a big win for popular science – here’s why.
The approaching approval (or not) of a competing EUA for the NON-mRNANON-viral-vectorNON-geneticNovavax coronavirus vaccine is going to tell us a LOT about how much power Pfizer and China still hold over FDA and CDC.
As you may have read two days ago, I regarded the conveniently timed FDA public statement about the myocarditis risks of the Novavax vaccine as a cynical “pot-vs.-kettle” attempt to sway approval and prevent the entirety of future Novavax data from getting into VAERS, where such data would very likely highlight every possible problem with the mRNA vaccine technology of the Pfizer and Moderna vaccines.
TL;DR – “I believe that mRNA vaccines have serious risks that would be REVEALED by approval of the Novavax vaccine.” -Wolf Moon I’m actually surprised that FDA and Pfizer/China allowed Novavax to get this close to approval, but they clearly have the upcoming vote RIGGED, just like the 2020 election. The trusty “board mules” that …
Well, it looks like the VRBPAC bunch did the smart – or at least consistent thing, and recommended approval.
The 21-0 vote with one abstention is telling, IMO. A vote AGAINST would cause an uproar on both sides, and put VRBPAC in the hot seat. Are they shuffling the murder of Novavax off to “the Roach” for a kill? We will see.
Here is a comment I added to my prior post, regarding an article in the Federalist, which takes the “no more approvals of any vaccine” approach – which I believe is well-intended but short-sighted. This comment explain my strategic reasons for supporting approval.
Here is a great example of somebody who sees the vaccines much the same as me, but strategically comes to the exact opposite point of view on approval of Novavax.
Reading his point of view may help people to see mine – or maybe not. Worth a read.
Dr. Gortler basically wants to begin playing fair and correctly on Novavax – making it jump through the hoops that Pfizer and Moderna didn’t have to jump through, but (IN MY OPINION, NOT HIS) thus denying what is likely a SAFER vaccine (in many respects – not all) to people who are going to take a vaccine, one way or another.
In my opinion, admitting the Novavax vaccine will shed necessary light on mRNA technology, as this “shingles-style” (recombinant protein) vaccine will help to highlight the flaws of the mRNA tech in the long run.
This is where I take a “Trumpian” and “they have to be shown” position. I regard a denial here as the kind of “purism” that has been deadly to conservatives, and was responsible for “NeverTrump” as an effective weapon of the left.
We have what is likely a “saf-ER” vaccine. Do we approve it or not?
YMMV.
Wolf Moon, June 9, 2022
Note that there is still plenty of time for FDA and/or CDC to snake Novavax and help Pfizer and China. Will they do it? Let’s wait and see. Either way, we win.
If Rochelle Alinsky and Anthony Fauci knife Novavax in the back to protect mRNA, I will have one of my greatest arguments yet that they need to be removed and prosecuted. The blatant hypocrisy will win more and more Democrats to our side. All of my neighbors are perfect recipients of the message. They will be screaming for Fauci to hang.
If they allow Novavax the opportunity to prove itself [to any degree] safer than mRNA vaccines, they fight another day – but they have to fight a battle we are destined to win.
Like I say, every day is a fight – but we are winning more and more fights, sooner and sooner.
TL;DR – “I believe that mRNA vaccines have serious risks that would be REVEALED by approval of the Novavax vaccine.” –Wolf Moon
I’m actually surprised that FDA and Pfizer/China allowed Novavax to get this close to approval, but they clearly have the upcoming vote RIGGED, just like the 2020 election. The trusty “board mules” that FDA’s Pfizer-lovin’, China-compromised top brass used to approve dangerously experimental, “China-tested”, mRNA vaccines, will suddenly get some phony backbone on myocarditis and virtue signal against a less dangerous vaccine.
Remember Trump getting angry about what FDA and Pfizer (which is really China) did to the J+J vaccine? Same thing.
“Blame the victim.”
It’s how they work, people. And once you see it, you can’t unsee it.
Allow me to explain.
Let’s start off with how I instantly realized what’s in the cards.
As seen on Gateway Pundit, minus my scientific and political explanation of what is going on.
This is CLEARLY a set-up to knife Novavax right before a crucial vote. But first, you need to know two things.
(1) Pfizer and Fauci BURNED THE PFIZER mRNA VACCINE PLACEBO GROUPS to hide the problems with the Pfizer vaccine. (The relevance of placebo groups will be explained a bit later.)
(2) According to Pfizer, which proudly revealed the following fact directly from the mouths of Pfizer’s top brass in a more China-virtue-signaling moment (look it up), ALL of their clinical trials (including all the COVID clinical trials of the past) are now run out of China.
SO – if you see all the SHADY SCIENCE that is popping up in the Pfizer documents, and is now being revealed thanks to Naomi Wolf, there is a simple explanation of why Pfizer burned their placebo groups, making it impossible for people to “check their math”.
CHINESE ETHICS (or lack thereof) are in charge of Pfizer’s clinical trials for all drugs and vaccines.
This is the same China that lies and cheats routinely on all things financial, business, manufacturing, etc. They’re the ones in charge of testing the drugs you are being forced to take by “China Joe”.
Yeah. Pretty convenient. Same vaccine our military is forced to take, too. VERY convenient.
This is a perfect example of “total warfare”, TBH. But let’s set that aside for now.
It’s now very clear that the spike protein is a pathogen. We have gone through all the problems of using the pathogenic spike protein as an immunogen (which Robert Malone warned about, by the way, and which FDA ignored). The spike protein causes a lot of problems, including myocarditis and pericarditis, just like the disease itself. Those problems, however, are compounded by TWO aspects of the technology of the Pfizer mRNA vaccines.
(1) mRNA technology itself is dangerous, because the pseudo-mRNA doesn’t shut down promptly, and in principle can never truly meter the amount of pseudo-spike-protein produced. It can dangerously overproduce the protein.
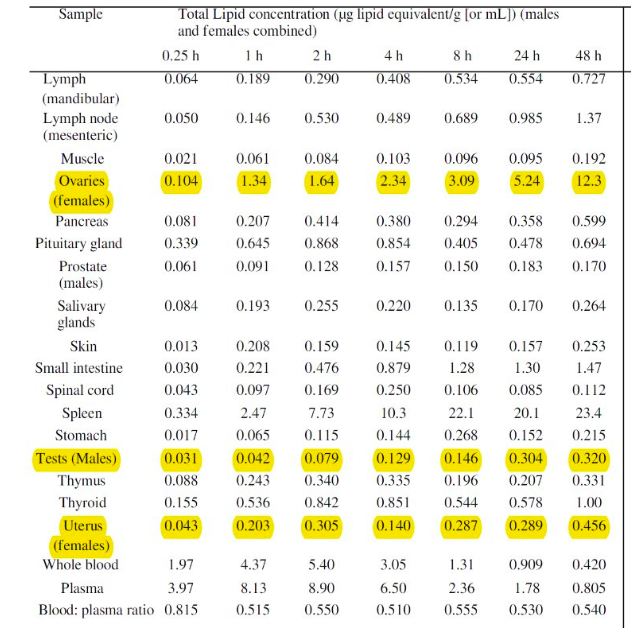
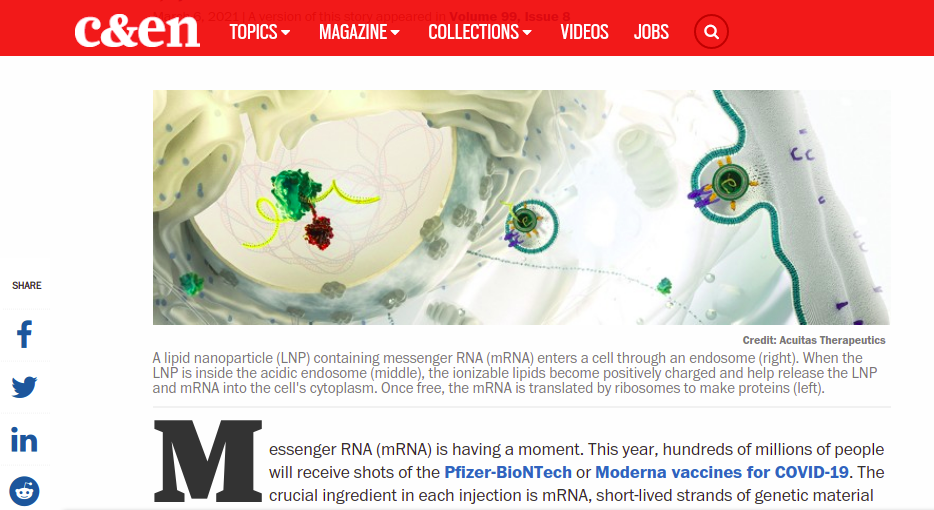
(2) the lipid nanoparticles used by Pfizer reduce acute symptoms by a kind of delayed release, but this also leads to unnatural persistence, migration throughout the body, excretion of the vaccine itself in body lipids (otherwise known as “exposure” or “shedding”), and a variety of symptoms which differ from the disease itself.
These problems are sidestepped by the more well-understood Novavax approach, which being based on a protein vaccine uses a DIFFERENT kind of “nanoparticle” to present a fully formed pseudo-spike-protein – NOT the mRNA for such, to the cells of the recipient. The spike protein is NOT coated with a lipid envelope, but rather is presented in a “ball of spikes” manner similar to an actual virus.
It is extremely likely that protein vaccines like Novavax and Corbevax are – certainly at the moment – substantially safer than mRNA vaccines. That is an EASY hypothesis to make at this point. Any honest scientist who has seen the data so far could make it. Robert Malone, who deeply understands the mRNA technology, which he properly labels “immature“, gets it totally.
One way to see if the relative safety of current protein tech over current mRNA tech is true, would be to approve the very likely safer Novavax and/or Corbevax in the United States, and to begin letting the data from adverse events flow into the VAERS reporting system. This data would get beyond the “small set” problem of the current trial data.
It’s quite obvious WHY Pfizer and FDA would not want this to happen.
It is extremely likely that Novavax and Corbevax would show greater safety relative to both Pfizer and Moderna. This would naturally lead to the question of why Novavax wasn’t fast-tracked to American citizens in 2020 and 2021, instead of Pfizer and Moderna.
Get it? This is a COVER-UP.
Now – let’s look at the actual data. Novavax is underplaying their hand.
Novavax not being Pfizer, the latter with a known, CONVICTED track record of lying and cheating (particularly after they stupidly entrusted their clinical trials to CHINA), let’s assume for a moment that MAYBE the Novavax clinical trial data is not total lies.
Here is the Novavax statement about the myocarditis/pericarditis issue:
NEWS & MEDIA
Novavax Statement on US FDA Briefing Document Related to Myocarditis/Pericarditis
Jun 3, 2022
Throughout the pandemic, as publicly available vaccines have been administered, there have been numerous investigations into findings related to myocarditis. We have learned that we can expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk. Myocarditis is most often caused by nonspecific viral infections.
The data from our placebo-controlled studies show that overall, in our clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%). Furthermore, in the post-crossover portions of our studies, the cases we have seen are all within the expected rate.
Based on our interpretation of all the clinical data supporting NVX-CoV2373, including over 50,000 participants in clinical trials, we believe there is insufficient evidence to establish a causal relationship. We will continue to monitor all adverse events, including myocarditis and pericarditis.
There are two ways to read this. Both of them argue correctly that the Novavax vaccine should be approved.
One way is to read it at “happy face value”. You are perfectly capable of doing that yourselves.
The other way is to read it, both knowing and admitting the hard truths about these vaccines, and what is actually possible when you make a vaccine against a minor coronavirus, for which the very need and justification are arguable at best.
I will read it the second, more conservative way, and you can follow along, sentence by sentence.
Throughout the pandemic, as publicly available vaccines have been administered, there have been numerous investigations into findings related to myocarditis.
This is another way of carefully admitting that myocarditis (more serious than pericarditis) is a real problem of the vaccines, because it’s a problem of the disease, because they both use the pathogenic spike protein.
We have learned that we can expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.
This is true. We’ve learned that myocarditis is a natural background problem for young people, and that the spike protein of the disease, BUT EVEN MORE THE SPIKE PROTEIN OF VACCINES, raises that risk for young people. All of this applying more to young MALES.
Myocarditis is most often caused by nonspecific viral infections.
This is true in general. But it can also be caused by vaccines for viruses, as one might rightly expect, because vaccines are INTENDED as a limited case of the disease.
The data from our placebo-controlled studies show that overall, in our clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%).
This is nice data for Novavax. Yes, the Novavax vaccine raises the risk of myocarditis in those who take it, but that risk is already minuscule, with Novavax only raising it by less than 50%. If you HAD to vaccinate kids, which we don’t, then Novavax is a relatively safe alternative, IMO.
Personally, I don’t think that children need the human vaccine AT ALL, because the DISEASE IS A BETTER VACCINE FOR KIDS. Yeah, think about it. Diseases can be vaccines, and vaccines can be diseases. Open your mind to the history of science, when we knew this stuff.
Furthermore, in the post-crossover portions of our studies, the cases we have seen are all within the expected rate.
This is sneaky wording, but it’s a bit of a KNIFE pointed back at FDA. They all KNOW that this applies to all the other vaccines. And maybe even MORE SO in the case of mRNA vaccines.
What exactly IS the “expected rate” of myocarditis? I’m betting strongly that the “expected rate” of myocarditis and pericarditis GOES UP in all vaccinees, just like it goes up in all people who get COVID and don’t treat it, and that the increase takes the form of probability spiking after the vaccination, then settling down to a slightly elevated risk (vs. before vaccination), further increasing with age.
Does FDA want to go there? Probably not.
Based on our interpretation of all the clinical data supporting NVX-CoV2373, including over 50,000 participants in clinical trials, we believe there is insufficient evidence to establish a causal relationship.
This may very well be true. The clinical set may simply be too small to state conclusively that the difference of 0.002% between vaccine (0.007%) and placebo (0.005%) was caused by anything but randomness. Note that I, personally, am assuming the worst case – that this difference of 0.002% IS IN FACT caused by the pseudo-spike-protein of the vaccine – and am saying that this is still NOT reason enough to not approve the vaccine. APPROVAL will very likely give us the VAERS data to PROVE that there is real risk to all the vaccines, but that it is LESS for Novavax and (if they ever approve it) Corbevax.
And note that I am talking about ALL RISKS – not just myocarditis. My money would be on Novavax being safer than mRNA vaccines in terms of every possible metric, including (very importantly) general immunity. I believe that mRNA vaccines have serious risks that would be REVEALED by approval of the Novavax vaccine.
We will continue to monitor all adverse events, including myocarditis and pericarditis.
Oh, that is a beautiful jab at Pfizer, which BURNED their placebo group.
What will you bet that Novavax is carefully protecting the integrity of their placebo group, because they’re not afraid of the evidence – like Pfizer/China?
Think very carefully about not approving Novavax, FDA. I’ve had your number for quite a while here. Better for you to swallow the bitter medicine of TRUTH, than to let this fester with a China-style cover-up that we will out on these pages every day for many moons.
Get your rest, Trumpy Bear! You’re going back to the White House!!!
We need to restore sanity in the White House, and it’s time to get Winnie the Pooh OUT.
The Business At Hand
This Stormwatch Monday Open Thread remains open – VERY OPEN – a place for everybody to post whatever they feel they would like to tell the White Hats, and the rest of the MAGA/KAG/KMAG world (with KMAG being a bit of both).
And indeed, it’s Monday…again.
But it doesn’t matter, because with God, every day is glorious!
And if you need that in a song…… ONE MORE TIME…..
The Rules
Boilerplate, more or less, but worth reading again and again, if only for the minor changes, and to stay out of moderation.
The bottom line is Free Speech. Theories and ideas you don’t agree with must be WELCOME here, and you must be part of that welcoming. But you do NOT need to be part of any agreement.
Thus we are assembled here to peacefully address our grievances to whom they may concern, even each other, using both our freedom of speech and of press, as well as our freedom of religion.
SO….. [ENGAGE BOILERPLATE…..]
We must endeavor to persevere to love our frenemies – even here.
Those who cannot deal with this easy requirement will be forced to jump the hoops of moderation, so that specific comments impugning other posters and violating the minimal rules can be sorted out and tossed in the trash.
In Wheatie’s words, “We’re on the same side here so let’s not engage in friendly fire.”
That includes the life skill of just ignoring certain other posters.
We do have a site – The U Tree – where civility is not a requirement. Interestingly, people don’t really go there much. Nevertheless, if you find yourself in an “argument” that can’t really stay civil, please feel free to “take it to the U Tree”. The U Tree is also a good place to report any technical difficulties, if you’re unable to report them here. Please post your comment there on one of Wolf’s posts, or in reply to one of Wolf’s comments, to make sure he sees it (though it may take a few hours).
We also have a backup site, called The Q Tree as well, which is really The Q Tree 579486807. You might call it “Second Tree”. The URL for that site is https://theqtree579486807.wordpress.com/. If this site (theqtree.com) ever goes down, please reassemble at the Second Tree.
If the Second Tree goes down, please go to The U Tree, or to our Gab Group, which is located at https://gab.com/groups/4178.
We also have some “old rules” and important guidelines, outlined here, in a very early post, on our first New Year’s Day, in 2019. The main point is not to make violent threats against people, which then have to be taken seriously by law enforcement, and which can be used as a PRETEXT by enemies of this site.
In the words of Wheatie, “Let’s not give the odious Internet Censors a reason to shut down this precious haven that Wolf has created for us.”
A Moment of Prayer
Our policy on extreme religious freedom on this site is discussed HERE. Please feel free to pray and praise God anytime and anywhere.
Thus, please pray for our real President, the one who actually won the election.
Republican presidential nominee Donald Trump prays with pastors during a campaign visit to the International Church of Las Vegas and the International Christian Academy in Las Vegas, Nevada, U.S., October 5, 2016. REUTERS/Mike Segar
MUSICAL INTERLUDE
For your listening enjoyment, and general encouragement, we continue Wheatie’s tradition of fine music videos, shipped fresh from the seas of information by our intrepid authors.
YouTube is absolutely bombarding me with videos of that Japanese art-pop girl-band “Perfume” that I showed on Friday. The YouTube Wocommie Mensheviks must have some foul intention, so I think I’ll go looking for something else, but just ONE video is a good lead-in, so here you go.
Thankfully, YouTube isn’t just recommending girl groups to me, as long as I get OFF a girl group video page, in which case girl groups are THE ONLY THINGS they recommend.
On a “blank” YouTube page, I also get “epic music” now!
This is a nice one. Don’t mind the “furries” and assorted anime characters.
https://youtu.be/XrisCsNzOlo
This is a long one, too – you can come back for it while reading the features below.
Next, we have one of Wheatie’s favorite artists – Two Steps From Hell – celebrating our lady warriors!
Yes – beware those who would go after our kids…….
They might not be expecting WHO exactly it is, who will DELIVER THE MILLSTONES.
So let’s close out with a REAL girl group – complete with a fiddle!
Now THAT’S what I’m talkin’ about!
Call To Battle
Our beloved country is under Occupation by hostile forces.
Daily outrage and epic phuckery abound.
We can give in to despair…or we can be defiant and fight back in any way that we can.
Joe Biden didn’t win.
And we will keep saying Joe Biden didn’t win until we get His Fraudulency out of our White House.
BUT FIRST, let me freshen you up with where things were as of February 3, when Robert Malone had THIS to say about the military data showing that the mandated mRNA jabs were definitively causing harm.
That’s just a quick overview of the problem. Here’s the latest, and in more detail. H/T TradeBait2 for this one. This addresses the jaw-dropping and eye-rolling defense by NIH and their Pentagram buddies, which just dropped military credibility by another factor of two.
Is woke mil causing damage? COMMUNISM always causes damage!
As Malone points out in the latter article, in a beautifully understated way, the “defenders of the jab” are now offering excuses that strain credibility to the breaking point. It is very easy to see that the other side is committed to any deception, of other or of self, to keep the jab train rolling.
They are NOT willing to honestly look at the striking relative dangers of these BAD VACCINES.
Something is very wrong, we can plainly see, but let’s just play along and pretend that this whole ridiculous scenario still deserves debate.
We have plenty of observations at this point, but the “old theory of harmless jabs” is able to play “what about” and temporarily evade many if not most of those explanations, lacking an obviously more compelling theory of WHY THE JABS CAUSE HARM, which would make “whataboutisms” unpalatable, even to those who want to believe them.
Well, is there such a compelling theory?
We have advanced certain key principles which explain things, and those are important.
We know about the pathogenic spike protein.
We know about vaccine migration and persistence.
But something is different, now.
NOW we have a theory which includes both of those things, PLUS a principle of IMMUNOLOGICAL ERROR.
In my opinion, we’re there.
The title of this work is:
Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations: The role of G-quadruplexes, exosomes and microRNAs
The abstract is instructive, and if you want to “TL;DR” past the rest of things, at least give that a read. Better yet, stick around for my interpretation of the abstract.
ABSTRACT
The mRNA SARS-CoV-2 vaccines were brought to market in response to the widely perceived public health crises of Covid-19. The utilization of mRNA vaccines in the context of infectious disease had no precedent, but desperate times seemed to call for desperate measures. The mRNA vaccines utilize genetically modified mRNA encoding spike proteins. These alterations hide the mRNA from cellular defenses, promote a longer biological half-life for the proteins, and provoke higher overall spike protein production. However, both experimental and observational evidence reveals a very different immune response to the vaccines compared to the response to infection with SARS-CoV-2. As we will show, the genetic modifications introduced by the vaccine are likely the source of these differential responses. In this paper, we present the evidence that vaccination, unlike natural infection, induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. We explain the mechanism by which immune cells release into the circulation large quantities of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites. We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances are shown to have a potentially direct causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, increased tumorigenesis, and DNA damage. We show evidence from adverse event reports in the VAERS database supporting our hypothesis. We believe a comprehensive risk/benefit assessment of the mRNA vaccines excludes them as positive contributors to public health, even in the context of the Covid-19 pandemic.
What I absolutely LOVE, LOVE, LOVE about this abstract, is that it takes some of the most key points of what the Fake News calls “conspiracy theories” and restates them in fact-bolstered scientific jargon that absolutely cannot be disputed. It’s just beautiful.
Because this abstract is important for understanding as we go into the paper, I’m going to take it “line by line” and explain, so that when we get to the paper itself, you can understand what is being talked about and get the gist of it, even if the scientific nuances are not entirely clear to you.
There are TWELVE sentences, each worthy of consideration.
HANG ON FOR A QUICK WARM-UP RIDE.
Analyzing the Abstract
(1) The mRNA SARS-CoV-2 vaccines were brought to market in response to the widely perceived public health crises of Covid-19.
“Widely perceived”.
This is an unarguable fact. It’s a great way to start the argument. State a truth without leaning on the “real crisis” narrative cheese in the center of the trap.
It does NOT say that the mRNA vaccines were brought to market unreasonably, which is open to debate, and which will be a contested question. Remember – many people (including me) HOPED that new technologies – which we were led to believe were needed – would free us from the virus.
Are you starting to see how they USED Trump? In my opinion, we still don’t understand the full extent of the deception and counter-deception. But none of that is said here – it is just ALLOWED under the statement of fact without narrative.
(2) The utilization of mRNA vaccines in the context of infectious disease had no precedent, but desperate times seemed to call for desperate measures.
“Seemed to”.
This is also factual, if we’re honest. The Jab Justifiers will quibble about veterinary vaccines, and experimental vaccines, and all that, as precedents, but those are quibbles. The truth is, you and I never got one of these genetic vaccines before, and that’s because they had never been approved before.
The beauty of this phrasing – “but desperate times seemed to call for desperate measures” – is that it forces us to admit the context of the phony crisis created by the Fake News and Democrats, by only saying “seemed to call for” instead of “called for”.
What the authors are doing here is dropping out the “fake normal” created by the media.
And THAT is an ongoing lesson for science itself to return to control by science and TRUTH.
This is absolutely true, and absolutely key. The mRNA of the vaccines encodes a FULL “half” of a very particular version of the SARS-CoV-2 spike protein. However, in order to accomplish several goals, the mRNA which WOULD code for that half of the spike protein is substantially altered in several different ways to make the whole process work.
And that leads to the next sentence.
(4) These alterations hide the mRNA from cellular defenses, promote a longer biological half-life for the proteins, and provoke higher overall spike protein production.
There is a lot of nuance here, so I will take some time to explain the 3 items.
(a) These alterations hide the mRNA from cellular defenses
There are multiple reasons that the “mRNA” of the vaccines is not actually normal mRNA, but a kind of “pseudo” mRNA.
Cells have to be careful not to “execute the instructions” of what is essentially WRONG RNA. Cells are a lot like soldiers who have been trained to NOT carry out unconstitutional orders.
The fact that mRNA vaccines and related forms of mRNA-based gene therapy actually work AROUND cellular defenses is a hint RIGHT THERE that they might do something bad. Our bodies are designed to FIGHT OFF foreign mRNA.
Be careful how you interpret what I’m saying there. It’s not an indictment of the mRNA method per se, because MANY if not ALL drugs have to “work around cellular and bodily defenses”. That is a huge part of the science of drug delivery.
HOWEVER, it is always cautionary to admit THAT one is working around defenses, because this will inform one as to the RISKS which are being taken BY working around those defenses.
What if you aren’t actually working around the risks?
So, one truth is that the mRNA has certain bases changed to avoid “tipping off” those defenses. It’s a SNEAKY and LUCKY break that we actually CAN work around those defenses.
But are we doing so CLEANLY and to good outcome?
(b) promote a longer biological half-life for the proteins
This is a HUGE double-edged sword.
Remember – the SARS-CoV-2 spike protein CHANGES SHAPE as it breaks into the cell. When it’s all done, it looks like a different protein – even to antibodies.
The drug designers have (literally, but synthetically) mutated the original reported Wuhan spike protein sequence. The primary reason to do this, is to make the protein “LOCK IN” the original, highly infectious, three-dimensional shape of the “fresh” protein, so that antibodies will form PROPERLY against that, instead of forming against depleted, spent, “used” spike protein. This reduces the chances of ADE (antibody-dependent disease enhancement), which comes from “inappropriate antibodies” that evolved to the WRONG TARGET.
The problem with stabilizing the highly pathogenic spike protein for triggering more desirable antibody formation, is that it also stabilizes the highly pathogenic spike protein for pathogenesis, too.
“WHOOPS!”
So – spike-protein-based “long haul” symptoms from the vaccine can be very long – even compared to long haul from the disease. The synthetic spike protein is really good at sticking around in its mutated, long-lasting, highly pathogenic form.
And THAT might not be a good thing.
Ask this question – why doesn’t the VIRUS do that? Maybe a more stable protein is not only bad for the virus, but also bad for the host, and THAT is in turn bad for the virus AGAIN.
(c) provoke higher overall spike protein production
This is a DIRECT call-out of a problem that will almost certainly lead to arguments with “peer reviewers” who want to defend the vaccines. Note that the wording very intentionally does not say “These alterations are intended to…..[three things]” – it simply says “These alterations….. [three things].”
The alterations are INTENDED to provoke higher overall spike protein antibody production. But the fact is, unless the increase in antibodies comes from better and stronger adjuvants, which act as immunity multipliers, then it’s coming from higher (or otherwise more antigenic and pathogenic) overall spike protein production.
Thus, peer reviewers who want to cover up spike protein malfeasance will likely insist on dragging the wording back to being about the antibodies. This follows the lead of Tony Fauci and his “antibody hypnosis” act, designed to keep attention OFF all of the things that are WRONG with the vaccines.
As you can see, we’re only 4 sentences in, and there is a lot of “battle prep” already going on.
(5) However, both experimental and observational evidence reveals a very different immune response to the vaccines compared to the response to infection with SARS-CoV-2.
This is a very general but very powerful FACTUAL statement, which DEFIES the Fauci / Fake News narrative – a narrative which can’t even bring itself to ADMIT that disease-conferred immunity is a reality.
This is a point about which – if you have read even SOME of the COVID-19 scientific literature – there is literally no debate. Only in the Fake News media and on controlled social media is this twisted. Scientists now marvel ALL THE TIME at the differences between vaccine-conferred immunity and disease-conferred immunity.
And, almost ALWAYS, practically speaking (but ignoring any risks of acquiring immunity), disease-conferred immunity is superior.
You will note that Fauci NEVER talks about this stuff.
But there is more – much more. ANY adverse effects which happen due to the vaccines and not the disease, or happen MORE with the vaccines, rightly count as differences.
The paper is not saying this out loud – but you can understand that it is implied.
This right here – the point about a difference between vaccine immunity and disease immunity – is the HAMMER of the gun going back and making a “clicking” noise.
(6) As we will show, the genetic modifications introduced by the vaccine are likely the source of these differential responses.
THIS HERE IS THE BIGGIE.
There are SO MANY potential implications here, I don’t want to steal their thunder from the analysis of the paper.
However, without knowing ANYTHING FURTHER, this is a profoundly common-sense scientific statement. It is simply saying that different molecules from the virus RNA may lead to different outcomes. That’s almost a no-brainer.
This could happen in multiple different ways.
differences in how the “changed mRNA” is handled by the body
differences in how it is interpreted
differences in the protein product
All of this makes wonderful sense.
(7) In this paper, we present the evidence that vaccination, unlike natural infection, induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health.
Oh, wait – THIS is the biggie.
This is saying that there is an important cellular communication screw-up with mRNA vaccination – a screw-up which does not occur with natural infection. Stated in reverse, there IS an important cellular communication channel opened during natural infection, which is MISSED by the mRNA vaccines.
IN OTHER WORDS, A PROGRAMMING ERROR.
This is all too believable to me, because I’ve seen this before. And NOT just when I “learned to code”.
This is LITERALLY a sibling programming error of what happens when too many vaccines are given at the same time, and interferon signals STEP ON EACH OTHER.
Now the Fake News media “fact checkers” absolutely will not admit that there is a problem with multiple simultaneous vaccines, but once the standard mechanism of vaccine-acquired immunity was explained to me, it became OBVIOUS AS HELL that signal interference was behind the observed but somewhat unpredictable problems with tight vaccine schedules.
You are allowed to have a different scientific opinion from these biased and forked-tongued “fact checkers” with agenda.
But let’s save the details for later.
For now, just remember that humans are evolutionarily adapted for disease, not hacky pseudo-mRNA vaccines. Our PROGRAMMING MODEL – our DESIGN – our API – is different from what the hackers thought they could get away with, and they got caught.
(8) We explain the mechanism by which immune cells release into the circulation large quantities of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites.
More specifics.
This is fascinating, because AND LOGIC is now telling me that it’s not just the vaccine migrating, but spike protein as well.
And THAT explains a LOT.
Do you see how everything is tying together nicely around the pathogenic spike protein that is NOT being degraded soon enough or fast enough, like the VIRUS DOES FOR US?
Think about our little human biome friends next time, science. They may have a BETTER PLAN.
(9) We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance.
OK, this is bad stuff. But it’s also bad stuff that is right up the alley of FAKE SCIENCE to now “discover” and get big bucks to study. It’s DETAILS that cannot be dismissed.
This is the GRENADE thrown into the narrative machine gun bunker with half a second left on the fuse.
KABOOM.
This is where every “me too!” funding whore is going to jump on the bandwagon with justification.
(10) These disturbances are shown to have a potentially direct causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, increased tumorigenesis, and DNA damage.
Oh, wait! Isn’t this the stuff that Robert Malone warned us about?
Isn’t this the stuff that Ryan Cole spotted?
Isn’t this the stuff that FAKE NEWS ignored and “debunked”, but is now appearing in every possible mainstream source of data?
Common sense is going to win here.
INVESTORS had better TAKE NOTE. The landscape is going to change, IMO.
(11) We show evidence from adverse event reports in the VAERS database supporting our hypothesis.
The beauty of VAERS is that it’s flawed, but we know HOW it’s flawed.
Thus, if you see something that can only be MAGNIFIED by correcting for the known flaws, then you have something you can use.
Just stroll past those Fake News fact checkers and Fake Social Media “con-TROLLS” who spew their talking point about “VAERS IS A FLAWED SYSTEM”. SORRY. Not good enough, trolls.
Everything is a flawed system. Knowing the DIRECTION of the flaws is what turns all systems into useful logical tools.
We will use common sense here, long after these people who deny it are OUT OF POWER.
(12) We believe a comprehensive risk/benefit assessment of the mRNA vaccines excludes them as positive contributors to public health, even in the context of the Covid-19 pandemic.
This is where they land when all is said and done.
They’re saying that they believe the risks outweigh the benefits with THESE vaccines.
This does NOT say that vaccination per se is a bad strategy for COVID-19.
It says that mRNA vaccination as it currently exists is not a good strategy for COVID-19.
It doesn’t say that viral vector cDNA, “full” spike protein subunit antigen, or RBD subunit antigen vaccines are doubtful in any way. They may be, but the authors don’t say that (although some of the specifics DO have implications for the other vaccines).
The authors only say that THESE particular, current, mRNA vaccines are “not positive contributors to public health”.
And you can do the math from there.
Can the current mRNA vaccines be fixed?
Good question. This paper is likely a roadmap to any such fixes. But until then…..
Mandating these vaccines is WRONG, if not INSANE.
Analyzing the Paper
Now we get to the meat of the paper.
I am just going to drop my impressions, placing them in context as needed. On some of these, I blab on and on. On others, I just make a short point. I do a lot of quoting where the authors say it nicely. This is very seat-of-the-pants.
Introduction
The FIRST paragraph is a generous summary of the basics of vaccination, FULLY in compliance with the CDC definitions. Please take note of that. There is no quibbling about the mRNA vaccines not being vaccines.
The SECOND paragraph summarizes and exemplifies the presence in the literature of a viewpoint that the mRNA vaccines are very similar to natural immunity. There is a point made that is basically my contention of Fauci’s “antibody hypnosis”, but it is phrased very politiely.
The U.S. Centers for Disease Control and Prevention (CDC) makes the case based upon antibody titers generated by prior infection vs. vaccination, in addition to production of memory B cells, to argue that the immune response to vaccination is analogous to the response to natural infection [4]. It is this similarity in the humoral immune response to vaccination vs natural infection, paired with both trial and observational data demonstrating reduced risk of infection following vaccination, that stands as the justification for the mass vaccination campaign.
The THIRD paragraph is long, but absolutely key.
It is the summary of the guts of the paper.
You will note that the authors are pointing out EXISTING MAINSTREAM SCIENCE which is contradicting the media-trumpeted, but “CDC-silent” narrative that vaccination is superior to “natural immunity”, by pointing out (without saying it bluntly) that it’s not even AS GOOD as disease-conferred immunity, because known “good” responses to the natural antigen are completely missing.
And worse than that, the mRNA vaccines seem to do WRONG THINGS to the immune system as well.
In this paper we explore the scientific literature suggesting that vaccination with an mRNA vaccine initiates a set of biological events that are not only different from that induced by vaccination but are in several ways demonstrably counterproductive to both short- and long-term immune competence and normal cellular function. These vaccinations have now been shown to downregulate critical pathways related to cancer surveillance, infection control, and cellular homeostasis. They introduce into the body highly modified genetic material. A medRxiv preprint has revealed a remarkable difference between the characteristics of the immune response to an infection with SARS-CoV-2 as compared with the immune response to an mRNA vaccine against COVID-19 [5]. Differential gene expression analysis of peripheral dendritic cells revealed a dramatic upregulation of both type I and type II interferons (IFNs) in COVID-19 patients, but not in vaccinees. One remarkable observation they made was that there was an expansion of circulating hematopoietic stem and progenitor cells (HSPCs) in COVID-19 patients, but this expansion was notably absent following vaccination. A striking expansion in circulating plasmablasts observed in COVID-19 patients was also not seen in the vaccinees. All of these observations are consistent with the idea that the vaccines actively suppress type I IFN signaling, as we will discuss below. In this paper we will be focusing extensively, though not exclusively,on vaccination-induced type I IFN suppression and the myriad downstream effects this has on the related signaling cascade.
Again, I point out that this is being pulled out of the “mainstream” literature.
Does this immune suppression that researchers found remind you of anything?
Note that this is on BitChute because YouTube deleted it as “misinformation”.
If you’re thinking “Wow, the media and social media has really screwed up science!”, well, all I can say is “They won’t be able to walk the streets.”
The FOURTH paragraph then begins dropping bombs on the Pfizer clinical trial shenanigans, which basically covered up the placebo group to obfuscate vaccine problems.
The message is roughly “Because Pfizer covered things up by vaccinating their placebo group, as well as other tricks, we were forced to look at VAERS and the scientific literature to find out what the vaccines are doing – AND BOY, DID WE FIND A TON OF PROBLEMS.”
But done much more politely.
The next two paragraphs are a WITHERING ATTACK on the vaccines, simply using the scientific literature. OMG – the spatter on the walls – there are quite a few easy targets that the Fake News Media has been protecting by ignoring, but it’s very hard to “memory hole” the scientific literature to those who can “pay to play”, so the authors just mention a string of scientific findings that Fauci hoped the public would never see.
Thus, the FIFTH paragraph is a summary of VACCINE FAILURE, with references.
The SIXTH paragraph then brings up the wonderful idea that if benefits are as low as we now understand them to be, maybe RISKS need a closer look.
You may want to read the whole introduction, because that is the last easily readable section of the paper for a while.
NOW it gets really technical.
Interferons: An Overview with Attention to Cancer Surveillance
This section is extremely complex and hard to read, even if you’re familiar with most or all of the various biochemical and biological acronyms that are thrown into the melange.
It starts off with a review of what is known about INTERFERONS (IFNs), as well as substances which regulate them, known as INTERFERON REGULATING FACTORS (IRFs).
This is what you need to know:
Type I IFNs play a powerful role in the immune response to multiple stressors. In fact, they have enjoyed clinical therapeutic value as a treatment option for a variety of diseases and conditions, including viral infections, solid tumors, myeloproliferative disorders, hematopoietic neoplasms and autoimmune diseases such as multiple sclerosis [16].
As a group, IFNs play exceedingly complicated and pleiotropic roles that are coordinated and regulated through the activity of the family of IFN regulatory factors, or IRFs [17]. IRF9 is most directly involved in anti-viral as well as anti-tumor immunity and genetic regulation [18-20].
Basically, interferons are critical players in the CLEANUP OF GENETIC BAD GUYS CAUSING TROUBLE. Those genetic bad guys can be EXTERNAL WRONG-GENES (viruses) or they can be ROGUE CELLS (cancer and the like).
This section then summarizes the complex interactions and feedback loops which characterize anything involving interferons, but particularly related to their anti-cancer role. It is made exceedingly clear that improper interferon levels and disruptions of the complex interferon systems are known to lead very directly to clinical appearance of cancers of various kinds.
Near the end, COVID-19 is brought into the mix. A recent Chinese paper is cited, the work having shown interference with IRF signaling by a non-mRNA, inactivated virus, COVID-19 vaccine. The changes are EXPECTED to reduce resistance to cancers, and the mechanisms are discussed in detail. ELEGANTLY, those same mechanisms are found in Alzheimer’s patients, and appear related to development of dementia symptoms that sound remarkably like COVID brain fog.
Finally, a documented case of a rare lymphoma being accelerated by the Pfizer vaccine is described, and a summary statement is given:
Given the universally recognized importance of optimally functioning BRCA1/2 for cancer prevention and given the central role of the TRAIL signal transduction pathway for additional cancer surveillance, the suppression of IRF7 and IRF9 through vaccination and subsequent spike protein production is extremely concerning for long-term cancer control in injected populations.
Considerations in the Design of mRNA Vaccines
This section basically describes the long list of HACKS – many of them very ELEGANT HACKS – that were needed to get all the way from Robert Malone’s initial discovery which enabled mRNA gene therapy, to where mRNA vaccines are today.
The implications of all these hacks for relevant IMMUNOLOGICAL and GENETIC biochemistry, including INTERFERONS and CANCER, are described.
This section SETS UP the long list of concerns which are going to necessarily follow.
Quite a bit of attention is paid to the components of the lipid nanoparticles, their roles, and their potential risks and side-effects.
This section is fairly readable, and if you’re curious about the various hacks, and particularly the purpose and mechanism of the lipid nanoparticles, then you may enjoy reading past the jargon.
GC enrichment and potential G4 (pG4) structures in vaccine mRNAs
This is a difficult section to understand, if you’re not familiar with DNA and RNA “beyond the double helix”. It’s a bit like Morse code. Everybody knows what Morse code is, and maybe how to do an “SOS”, but not many people remember Morse code well enough to compose and send long signals at will, let alone send a telegram. OTOH, if you’re in genetic medicine or biology, you may be familiar with more than just 4 bases and the double helix.
The bottom line is that, among the various hacks that have gone into the mRNA vaccines, some of them are basically “genetic tricks” to increase production of spike protein. The PROBLEM with that, is that the FINAL implications of some of these tricks are not fully known.
Because there is redundancy in the genetic language, and the efficiency of different spellings is not the same (nite vs. night, thru vs. through, etc.), certain things can be re-encoded using the most efficient letters to create MOAR SPIKE PROTEIN. And MOAR is always BETTER. RIIIIIIIIGHT?
Well, it turns out that spellings have implications for how mRNA behaves. How mRNA behaves has implications for things like CANCER.
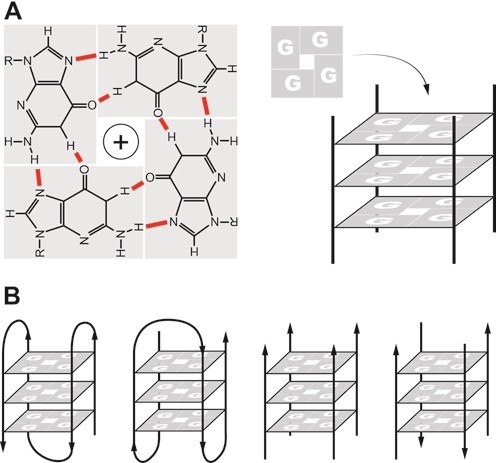
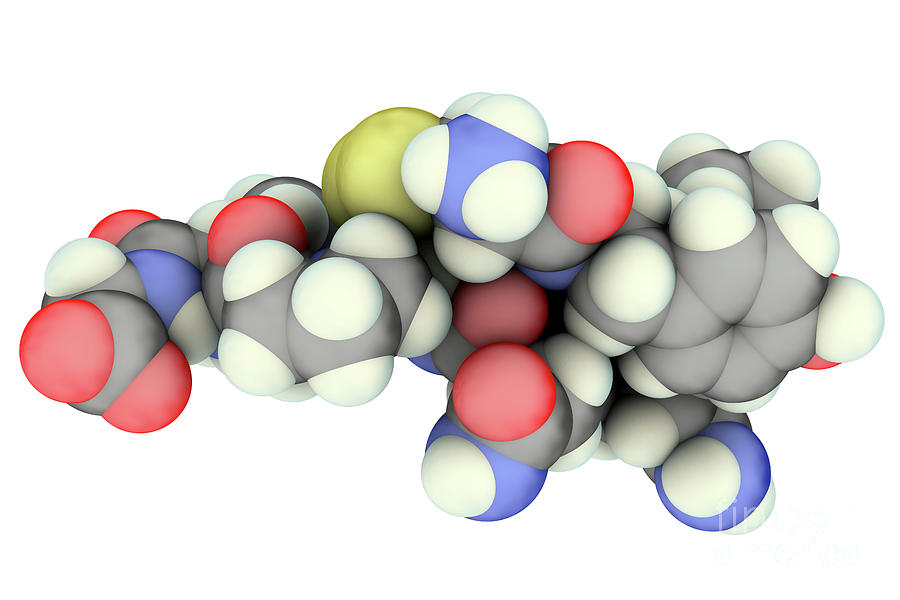
Going back to the title of this section, “G” and “C” are the efficient bases that are switched to, to make proteins with higher efficiency. The problem THERE is that “G” can do something every interesting – it can bind with itself in a square, to form a quadruple helix called a “G quadruplex”, which is abbreviated G4. See the image above for cross-sections of such a structure, at the point of binding.
There are ways to predict if a G quadruplex will form – these cases are called “pG4” for “potential G quadruplex”.
Midway through the section, this quote:
Summarizing the topic to this point, the enrichment of GC content in vaccine mRNA will inevitably lead to an increase in the pG4 content of the vaccines. This, in turn, will lead to dysregulation of the G4-RNA-protein binding system and a wide range of potential disease-associated cellular pathologies including suppression of innate immunity, neurodegeneration, and malignant transformation [83].
There are further implications. The more mRNA can form these self-shielding quadruplexes, the less that “micro RNAs” – miRNAs – can bind to the mRNA and control the expression. And THAT leads to another cascade of potentially unintended consequences.
The multitude of pG4s in the mRNA of the vaccine would predictably act as decoys, distracting miRNAs from their normal function in regulating human protein expression. The increase in G4 targets due to the vaccine would decrease the availability of miRNAs to target human-expressed G4s for regulation of gene expression. This can result in downregulation of miRNA expression which is implicated in cardiovascular pathology [96], onset of neurodegeneration [97], and/or cancer progression [98].
Type I IFNs and COVID-19
This is a very interesting section on the relationship of interferons to COVID-19. It appears that:
lower levels of interferons lead to more severe COVID-19 outcomes
IFNs can be used for treatment early, but make things worse if given late
interferons seem to prevent infection by COVID-19
this would explain enhanced susceptibility to COVID-19 after vaccination
COVID patients with antibodies against interferons are common in severe cases
Interferons are clearly key, and look to be one of the most significant differences between the disease and the vaccine.
Are the methylation strategies for cellular housekeeping generally omitted by vaccine mRNAs?
This is a rhetorical question about one of the hacks used by the mRNA vaccines.
To put it a bit too simply, the synthetic mRNA is “capped” both to evade detection AND to generate more spike protein, and most likely without regard for downstream unintended consequences, due to the fact that capping is normally supposed to be both a signaling and a regulating mechanism. The “hack” abuses this feature to make more spike protein.
Rather than simply making an accusation, the question is asked, whether the hack accounted for some of the more likely consequences.
E.g., …..
Furthermore, this also means that eIF4E, which is a powerful oncogene regulator and cell proliferation modulator, will sustain its activities by this competition, for an unnaturally prolonged period of time, trying to counterbalance the competition between robustly-capped mRNAs in vaccines and IRES-containing mRNAs[113,65]. This type of condition results in dysregulation of co-transcriptional m6A mRNA modifications and seriously links to molecular progressions of various cancers [114], as well as creating predisposing conditions for subsequent viral infections [113].
My money is on the idea that nobody in the management chain at Pfizer or Moderna gave a flying F, because Fauci and Walensky are all about the antibodies. This is a CLASSIC downstream effect of antibody hypnosis.
Exosomes and MicroRNAs
This is an interesting grab-bag of stuff, and it’s not that hard to follow, for the most part, so you may want to read it.
Exosomes are basically little bubbles of cell that break off and carry crap, a lot like “virus-like particles” or even “lipid nanoparticles”. It turns out that much of the spike protein which is produced in vaccine-infected cells LEAVES THE SCENE inside exosomes, or studded into their surface. This was in fact discovered by a group in India.
Also, under conditions of overwhelming production of spike protein due to SARS-CoV-2 molecular vaccination, it would of course be expected that a significant proportion of over-abundant intra-cellular spikeproteins would also be exported via exosome cargoes [128]. A seminal paper by a research team in India investigated the role of exosomes in the cellular response to internally synthesized SARS-CoV-2 spike protein [50]. They wrote in the abstract:“We propose that SARS-CoV-2 gene product, Spike, is able to modify the host exosomal cargo, which gets transported to distant uninfected tissues and organs and can initiate a catastrophic immune cascade within Central Nervous System (CNS).”
Things get even worse. It turns out that these exosomes also carry micro-RNAs that turn off interferons in the distant places to which they carry the spike protein.
Thus, the available evidence strongly suggests that endogenously produced spike protein creates a different microRNA profile than does natural infection with SARS-CoV-2, and those differences entail a potentially wide range of deleterious effects.
A central point of our analysis below is the important distinction between the impact of vaccination versus natural infection on type I IFN. While vaccination actively suppresses its production, natural infection promotes type I IFN production very early in the disease cycle. Those with preexisting conditions often exhibit impaired type I IFN signaling, which leads to more severe, critical, and even fatal COVID-19. If the impairment induced by the vaccine is maintained as antibody levels wane over time, this could lead to a situation where the vaccine causes a more severe disease expression than would have been the case in the absence of the vaccine.
Another expected consequence of suppressing type I IFN would be reactivation of preexisting, chronic viral infections, as described in the next section.
SO – this would explain “vaccine-induced disease enhancement” – not antibody-dependent (ADE), but rather interferon-dependent (IDE). And in this case, it could be significantly different diseases that are being enhanced, because of the generality of the interferon network.
Speaking of which…..
Reactivation of Varicella-zoster
Fully consistent with the proposed vaccine-induced negative effects on interferon signaling, would be the significant number of cases of shingles appearing post-vaccination with the mRNA vaccines.
There is also a documented case of viral hepatitis flaring up because of the vaccine.
An additional case of viral reactivation is noteworthy as well. It involved an 82-year-old woman who had acquired a hepatitis C viral (HCV) infection in 2007. A strong increase in HCV load occurred a few days after vaccination with an mRNA Pfizer/BioNTech vaccine, along with an appearance of jaundice. She died three weeks after vaccination from liver failure [142].
Personally, I have no desire to get shingles again.
Impaired DNA Repair and Adaptive Immunity
As stated – more examples from the literature.
We have to speed up here. This is a long paper.
Immune Thrombocytopenia
This is your “clot shot” mechanism, explained.
This quote is interesting.
It has been shown that the mRNA vaccines elicit primarily an immunoglobulin G (IgG) immune response, with lesser amounts of IgA induced [155], and even less IgM production [156]. The amount of IgG antibodies produced is comparable to the response seen in severe cases of COVID-19. It is IgG antibodies in complex with heparin that induce HIT. One can hypothesize that IgG complexed with the spike protein and PF4 is the complex that induces VITT in response to mRNA vaccines. It has in fact been shown experimentally that the receptor binding domain (RBD) of the spike protein binds to PF4 [157].
PPAR-α, Sulfatide and Liver Disease
Two paragraphs are worthy of your attention.
As we have already stated, an experiment by Mishra and Banerjea (2021) demonstrated that the spike protein induces the release of exosomes containing microRNAs that specifically interfere with IRF9 synthesis[50]. In this section we will show that one of the consequences of suppression of IRF9 would be reduced synthesis of sulfatide in the liver, mediated by the nuclear receptor peroxisome proliferator-activated receptor α (PPAR-α).
…
Multiple case reports in the research literature describe liver damage following mRNA vaccines [165-167]. A plausible factor leading to these outcomes is the suppression of PPAR-α through downregulation of IRF9,and subsequently decreased sulfatide synthesis in the liver.
As you can see, there is a prediction here, and plenty of room to investigate.
Guillain Barre Syndrome and Other Neurological Conditions
This is worth reading. There is a laundry list of neurological conditions clearly attributed to the vaccine, and a clear mechanism by which they happen.
Bell’s Palsy
A known problem which appeared during the clinical trials of the mRNA vaccines.
Placebo 1, Treatment 7. Do the math.
Myocarditis
Signals and mechanisms are discussed. Particularly compelling is the proposed role of exosomes in carrying the toxic spike to cardiac tissue.
My money is still on migrating vaccine, but AND LOGIC will do for now.
Considerations Regarding the Vaccine Adverse Event Reporting System (VAERS)
The underreporting of the system is discussed, with some doubt about the commonly cited figure of “100X” underreporting, as well as mention of a more sophisticated figure of 31X obtained by Rose.
VAERS Signal for Immune Suppression, Thrombocytopenia and Neurodegeneration
A comparison of the data from COVID vaccines to ALL OTHER VACCINES COMBINED is made, and the results are impressive.
Many different things are listed. It’s worth looking at.
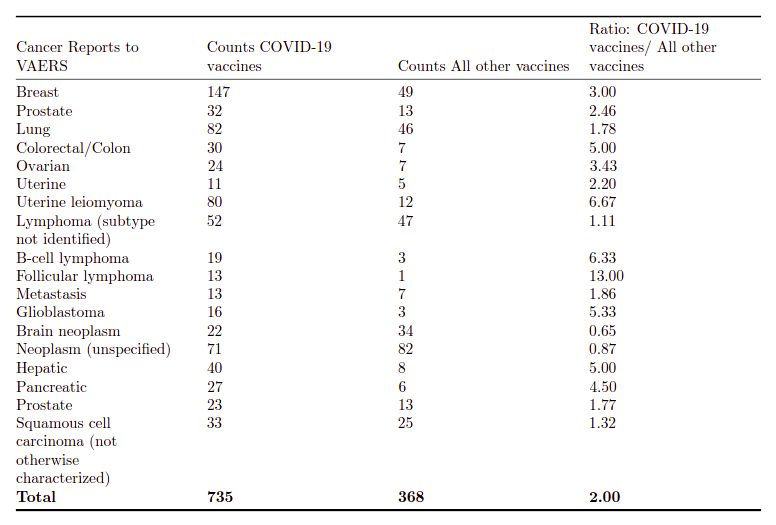
VAERS Signal for Cancer
After detailing the numbers for cancer (nice table), where the mRNA vaccines have HUGE numbers compared to all other vaccines combined, this statement:
This cannot be explained by reference to a disproportionately large number of people receiving an mRNA vaccination in the past year compared to all other vaccinations. The total number of people receiving a non-COVID-19 vaccination is unknown, but over the 31 years history of reports VAERS contains it is unquestionably many orders of magnitude larger than the number receiving an mRNA vaccination in the past year. Overall, in the above table, twice as many cancer reports to VAERS are related to a COVID-19 vaccination compared to those related to all other vaccines. That, in our opinion, constitutes a signal in urgent need of investigation.
To me, this is enough to say that the mRNA vaccines are related to cancer. Period.
Discussion
This is worth reading:
There has been an unwavering message about the safety and efficacy of mRNA vaccinations against SARS-CoV-2 from the public health apparatus in the US and around the globe. The efficacy is increasingly in doubt, as shown in a recent letter to the Lancet Regional Health by G¨unter Kampf [215]. Kampf provided data showing that the vaccinated are now as likely as the unvaccinated to spread disease. He concluded:“It appears to be grossly negligent to ignore the vaccinated population as a possible and relevant source of transmission when deciding about public health control measures.”
In this paper we call attention to three very important aspects of the safety profile of these vaccinations. First is the extensively documented subversion of innate immunity, primarily via suppression of IFN-α and its associated signaling cascade. This suppression will have a wide range of consequences, not the least of which include the reactivation of latent viral infections and the reduced ability to effectively combat future infections. Second is the dysregulation of the system for both preventing and detecting genetically driven malignant transformation within cells and the consequent potential for vaccination to promote those transformations. Third, mRNA vaccination potentially disrupts intracellular communication carried out by exosomes, and induces cells taking up spike mRNA to produce high levels of spike-carrying exosomes, with potentially serious inflammatory consequences. Should any of these potentials be fully realized, the impact on billions of people around the world could be enormous and could contribute to both the short-term and long-term disease burden our health care system faces.
Given the current rapidly expanding awareness of the multiple roles of G4s in regulation of mRNA translation and clearance through stress granules, the increase in pG4s due to enrichment of GC content as a consequence of codon optimization has unknown but likely far-reaching consequences. Specific analytical evaluation of the safety of these constructs in vaccines is urgently needed, including mass spectrometry for identification of cryptic expression and immunoprecipitation studies to evaluate the potential for disturbance of or interference with the essential activities of RNA and DNA binding proteins.
This is what I was talking about at the beginning. There is enough here for an enormous amount of productive research on the downside of these vaccines. It’s EASY RESULTS. Maybe not easy grant money, but plenty of easy CLOUT when it’s all over.
This does NOT go back in the toothpaste tube.
Conclusions
Presented in whole:
It is imperative that worldwide administration of the mRNA vaccinations be stopped immediately until further studies are conducted to determine the extent of the potential pathological consequences outlined in this paper. It is not possible for these vaccinations to be considered part of a public health campaign without a detailed analysis of the human impact of the potential collateral damage. It is also imperative that VAERS and other monitoring system be optimized to detect signals related to the health consequences of mRNA vaccination we have outlined. We believe the upgraded VAERS monitoring system described in the Harvard Pilgrim Health Care, Inc. study, but unfortunately not supported by the CDC, would be a valuable start in this regard [208].
In the end, we are not exaggerating to say that billions of lives are at stake. We call on the public health institutions to demonstrate, with evidence, why the issues discussed in this paper are not relevant to public health, or to acknowledge that they are and to act accordingly. Until our public health institutions do what is right in this regard, we encourage all individuals to make their own health care decisions with this information as a contributing factor in those decisions.
That’s where I’m at. Do not take the clot shot. Do not give it to your kids. Tell people how you honestly feel.
I am OK with people having the freedom to take a bad vaccine, but I personally think that coercing anybody in the slightest to take it, is a CRIME.
If you’re scared of getting or giving COVID, there are far better ways to deal with it, than a bad vaccine that does a lot of damage.
Can the mRNA Vaccines Be Fixed?
That’s MY question.
I suspect that they CAN be fixed, but not for at least several years – maybe 5-10, if we’re lucky.
Until then, they should be taken off the market, IMO.
Hopefully antigen vaccines will do better, but if they don’t, we can fall back to treatment and “real” immunity.
Wolfie’s Wheatie’s Word of the Day:
wolven
noun
Of or pertaining to wolves; wolflike; wolfish.
Used in a sentence:
Adjectives for wolf include wolfish, wolfless, wolflike, wolfly, wolfy, wolven, wolvish, wolfed, wolfing, wolved and wolving.
(If you can find a better one, please add it to the comments!)
In fact, Logan WENT EASY on America’s FRANKENSTEIN, Anthony Fauci.
Lara Logan said NOTHING – absolutely nothing – about the GREATEST SCANDAL IN MEDICAL HISTORY, which is happening RIGHT NOW under Fauci’s complete control and direction. Indeed, by all appearances, Anthony Fauci is helping to cover up one of the most murderous medical scandals in HISTORY.
And it may be even worse. It may be that Anthony Fauci is PART OF THAT SCANDAL.
Yet – ironically – Lara Logan let Anthony Fauci COMPLETELY off the hook.
Well, not me.
I’m not letting Anthony Fauci off.
I’m going to explain why Anthony Fauci is very likely a monster 1000 to 2000 times WORSE than Josef Mengele.
And I have the DATA TO PROVE IT.
Fox News – why don’t you ask some smart guy like Jesse Watters to explain it to you?
Or are YOU protecting America’s Mengele?
LISTEN and LEARN.
The Toxic Vaccine Batch Problem
The toxic vaccine batch problem is absolutely extraordinary. Science has never seen anything quite like this.
Bluntly, it was discovered in three stages, that something was VERY WRONG with CERTAIN BATCHES of the COVID vaccines distributed in America. Each stage of understanding showed, progressively, that the problem was WORSE than what we had thought before.
Stage 1 – There was a Small Group of Highly Toxic Batches
STAGE 1:The Daily Expose finds that almost all of the deaths and bad reactions to the COVID vaccines came from about 5% of the batches. If you got one of the “killer batches”, you were in serious trouble.
So what was the approach of NIH, CDC and FDA to this information?
CRICKETS. Say nothing and hope that it goes away.
Stage 2 – The Toxic Batches Are Not Random
STAGE 2: Karl Denninger runs the numbers himself. This is SCIENCE. Is the observation reproducible? YES, IT IS. Not only does Denninger confirm the toxic vaccine batch problem – he finds that the toxic batches were NOT RANDOM. Something was SYSTEMATICALLY WRONG with those very particular batches.
If you want a quick and understandable explanation of the toxic batch problem, just watch this video, or click on any of the three links below it.
Stage 3 – There are Clear Patterns to the Toxic Batches
STAGE 3: A chronological analysis of the bad batches shows strong clustering which indicates some kind of INTENT. The clustering affects one company at a time, alternating between companies, between levels of toxicity, and between “toxic / non-toxic”. Everything about the clustering looks like what one would expect for human dosage experimentation on the recipients.
It is HIGHLY recommended that you listen to the following TWO video analyses.
Certain batches (roughly 5%) of the three COVID-19 vaccines used in America were very clearly HIGHLY TOXIC relative to normal batches.
Further analysis shows that the poisoning was NOT random – there was some kind of systematic reason behind certain batches being really, really dangerous.
Chronological clustering analysis shows TIMING and OWNERSHIP of the bad batches. It shows a relationship of coordination between companies. It shows both DOSE RANGING and BASELINING. In other words, it appears that the toxicity was intentional, and vaccine recipients were being EXPERIMENTED UPON.
Even further analysis shows that there is a LOT NUMBER RELATIONSHIP between bad batches in the bad batch clusters.
I think at this point it is VERY, VERY, VERY clear that Anthony Fauci MUST know something about this.
And yet, nobody in FAKE NEWS questions him about it.
Let’s be clear. We have EVIDENCE of human experimentation with certain batches of these horrible vaccines. But Fauci – the man who would be responsible for such experimentation – or for doing something ABOUT IT – can only COMPLAIN about comparisons to Mengele?
Well, WHY NOT?
Josef Mengele seemed to be very “OK” with involuntary human experimentation.
Anthony Fauci seems to be very “OK” with involuntary human experimentation.
So I’m going to make this VERY CLEAR.
Until Anthony Fauci has told us WHO IS RESPONSIBLE for the toxic vaccine batch problem, and has ELIMINATED THE PROBLEM, I will NEVER – EVER – take another vaccine.
I mean, why can’t the same people poison any OTHER vaccine – including the flu vaccine?
Answer – they CAN poison any vaccine they want to poison. And they will get away with it, as long as Anthony Fauci is protecting them.
Whoever poisoned those vaccines is still out there.
And every bit of evidence tells me that Anthony Fauci knows exactly who these Mengeles are, and is protecting them from scrutiny.
Well, it’s time for Anthony “Maybe Mengele” Fauci to answer our questions – or turn over his job to somebody who will.
Because otherwise, he is single-handedly DESTROYING our trust in medicine and science.
W
(H/T RF121 for tipping me off to the latest information on toxic batches.)
This is for the historical record. I hope that this analysis gets to the “dissident scientists” involved, but even if it never does, future historians will get a powerful look at what I call “Fake Science” – the establishment’s phony, deceptive and controlled scientific complex – and how infiltration, control, and discreditation of dissident populist …
You will recall that I located the point where the “suramin error” was dropped in front of the right people to be uploaded to the prominent doctors of the anti-vaxx community, prior to the “magnet challenge” disinformation being similarly uploaded, and then used to discredit them in the Daily Mail.
Part of the suramin attack involved a highly edited video of Judy Mikovits touting suramin, minus the full information about that drug. That video, in combination with erroneous assertions about suramin being in pine tree needles, resulted in the physicians who are currently prominent warning about the COVID vaccines, picking up the error and discrediting themselves in their very current and very popular videos about the gynecological and shedding problems of the persistent and migratory spike protein vaccines.
Well, that video which was used to misinform them has been removed.
Sunlight. It cures quite a bit all on its own.
More seriously, I realized that, at some level there, probably in the background, I was dealing with pro “influencers of influencers of influencers”. I won’t be sharing all my information on that, as much as I would love to, but it became apparent that they are watching us like hawks. Speaking of which…..
2.
The Sleeper Has Awakened
Yes, Sundance just came out with a piece critical of the COVID vaccines. You will recall that SD and his crew were all fairly pro-vaxx, so this tells me there is a fundamental shift going on.
And while the fact that the HHS entrance to VAERS went down at the same time SD came out with this article may very well just be coincidence, I am 100% certain that the policy of Barack Obama and Eric Holder is BACK IN PLACE under Merrick “Whatever You Say, Barack” Garland, and that journalists like Sundance (and ourselves) are being SPIED ON by the federal government, in a abuse of power for political purposes.
SO – anyway – keep an eye on CTH in regard to things “COVID” – there is going to be some good stuff there, I’m willing to bet.
[Just for the record, I wrote this BEFORE the recent CTH post about “QAnon” stuff, which I happen to regard as a very helpful warning, but which was “not received warmly” by most on this site. I’m not looking to exacerbate the situation, but I hate “spiking” anything – for anybody. And I’m going to be very blunt. Sundance is going to have THE BEST coverage of DOJ asshattery against our site, so prepare to see me using a LOT of his coverage in my postings and reasoning. People need to learn to keep their emotions in check, because that is how an army survives – digital or otherwise. WWG1WGA begins with YOU.]
3.
Scientists Are Calling Out The Snakes
Everybody is seeing how people are calling out FAUCI, but in my opinion that’s actually a side-show. The REAL DEAL is scientists calling out the scientific BULLSHIT about COVID, and particularly the spike protein nuttery that was imposed on us. At long last, people in Scienceville are going “WHAT THE #### IS GOING ON?”
First, a video that came to us via Grandmaintexas and this link:
It’s worth listening to the beginning of this video to hear this dude list off his credentials. This guy isn’t just some country doctor. Nor is he old, senile, or out-of-date on current medicine. Just listen to him. This dude is IMPRESSIVE. He’s still sharp as a tack, just like Trump. I would almost say “more”, at the risk of offending some who believe this is not possible! Just listen to him.
Among many other jaw-droppers of sensible scientific perspective, this video basically tells you why I have been so mouth-agape about that Pfizer data snagged back into American science from JAPAN.
You have to look closely at it, but not THAT closely.
The VIDEO adds more about testicular localization in males.
Yeah, boys. It ain’t just the broads. Cross those legs – this is gonna make you cringe like a prostate exam.
One of the things which is EXTREMELY NOTEWORTHY about the video is that this lady YouTuber / Facebooker / BitChuter and all-around “social media presenter” goes into deep detail about the extreme censorship she is encountering, and how she deals with it.
For example, she states that the YouTube video was taken down in about 10 minutes.
Alternatively, you can listen to some different scientists in THIS great video, thanks to singingsoul.
Here we have Bret Weinstein interviewing a doctor and an engineer who explain – to the satisfaction of any honest scientist – WHY the mRNA vaccines (and to a lesser extent, the adenoviral vector vaccines) are CLEARLY problematic.
This is EXACTLY the same stuff we’ve been talking about. And it will be extremely useful in getting to where we are going, looking at NEW VACCINES COMING.
I’ll give you a hint now – the new vaccines could be a strong correction, back to what vaccines SHOULD be – or they could just be a slower and stealthier path to get us where the cabal has us going now – elite-controlled social contraception, and immunity debt enslavement – which is the worst-case future of “vaccine capture” a la Marek.
So – let me review previous posting, mostly mine, but also Deplorable Patriot’s reachy but prophetic question about the incredible and previously unthinkable idea of vaccine shedding. All of it based on what YOU, our loyal posters, brought here for the group to digest.
Take a bow, people. YOU DID GOOD.
4.
A Short Bibliographic Toldjaso From This Site
I will preface each of these blurbs with another short blurb, explaining relevance.
This will “refresh your memory”, before we get into the FUTURE.
We start, very appropriately, with RAND PAUL.
Gotta give DOCTOR Rand Paul credit – he has led the fight to bring SANITY back to medicine and science. Thank GOD Trump put him where he saved the most people – in the SENATE. I also have a personal debt here, as a recoveree, forced to wear a needless mask, aggravating my hypoxia. Rand Paul has FREED ME of my TORTURE MASK.
Introduction You have GOT to see the video I’m going to show you. It’s not just what they’re talking about. It’s WHERE IT LEADS. Most of the people who watch Rand Paul go after Fauci here, are concentrating on MASKS, because that is the TOP LAYER of the argument. But THAT is the small potatoes. …
This post is where disparate cracks in the narrative all opened at once. I was no longer going along with the bullshit. Too many questions, too many pat answers turning up WRONG – no – the narrative was full of holes, and it was time to think ON OUR OWN.
PREFACE I thought that I might withhold this post on Easter Sunday, and then I changed my mind, thanks to Deplorable Patriot, Trump, Gab and Jesus. If anybody ever FOUGHT on Easter Sunday, it was Christ. It’s time to FOLLOW POINT. The Branch Covidians have taken a toll, but the WAR is turning, and – …
I just went back and read this thing, and – WOW – just WOW. I was all over two things – spike protein and genetic incorporation – the JAENISCH paper. We are now all over the spike protein, but we MUST turn our attention to genetic incorporation of the vaccine – particularly in people who “fountain” the spike protein. I had forgotten this, but much of the suspicion of Fauci on this site centered around his seeming obsession with vaccines for viruses capable of genomic incorporation.
Yes, Wuhan is important, but I see that as the plotters playing “hot potato scandal” to distract us from the deeper purposes of this LYING phony pandemic.
Genetic incorporation of these vaccines must be investigated. There has been so much we have been told that is WRONG – I think genetic incorporation due to the spike protein acting as a reverse transcription promoter for its own RNA is a biggie.
Alternate Title: Is Persistent Reverse Transcription a Hidden Virus/Vaccine Objective? Gloating Pre-Preface There are few feelings of satisfaction like opening up the NEWS and knowing one’s theories and understandings are WORKING even better than one thought. Let’s see if they use this one for damage control, and get the “new science” out before the STORY …
No good guys among these genetic vaccines. They are all RISKY for certain people, and when we EUAed them forward, we took those risks. The problem is, with idiot BIDEN in charge, instead of Trump, there was nobody to push the sensible idea of sparing the vaccine from those for whom it would be knowingly risky.
Every coronavirus vaccine so far has shown us SOME defect upon mass release, which was NOT evident in EVEN phase III clinical trials. Look HERE for a searchable PDF document of adverse effects from the Pfizer vaccine: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/977005/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print.pdf Check out these videos on the low-platelet clotting problem from the Oxford/Astrazeneca vaccine. Here is a fantastic …
I was really starting to get it here. I was starting to accept that “it’s the full spike protein, stupid!”
I saw an excellent explanation of the clotting problem with the AstraZeneca vaccine against SARS-CoV-2 / COVID-19 here: The doctor, Dr. ZDogg, MD, offers an exceptionally clear explanation of both what is going on with the AstraZeneca vaccine, and why its distribution was halted or limited in some places for some age groups of patients. …
This is when I realized that all the gynecological problems being reported for the COVID vaccines were actually a REAL problem, and not just a sub-problem of the clotting problems. I also realized that this effect was too pronounced to be an accident. And then the complications going to other people in close contact – how could this even be possible?
So I considered what sounded like a more reasonable alternative to “vaccine shedding” – namely, spike protein shedding. Indeed, both avenues could be operating, but vaccine shedding now has DATA to support it, in the form of the Pfizer animal data showing persistence and migration. And if you stay with this to the very end, you will see that these lipid nanoparticles have been nothing but trouble from the beginning. It’s an impressive technology, but clearly not fully baked.
Thus, read this post, knowing that the vaccine is likely to be nearly as persistent as the spike protein it produces. Everything I’m saying for the spike protein, should apply in spades for the vaccine, which essentially brings in mRNA as a transmissible FACTORY for creating spike protein. It would not take much vaccine transfer to create the EXACT problem that is observed in alleged shedding incidents.
“When the people have any power to object to a socialist solution, a deniable 5% fait accompli is always more desirable to socialists than a negotiated 50% solution, because they can always negotiate on the remaining 95%.” -Wolf Moon When I first heard about a case of a miscarriage by a pregnant doctor, due to …
This is where I really laid out the evidence that the spike protein is causing the problems we’re seeing.
Using Principles of Protein Equivalence and Analogy as Predictive Tools for Coronavirus Understanding Surely you’ve heard of the BROWN RECLUSE SPIDER. The brown recluse is related to several other recluses, and a couple of other families of spiders, that all have a similar venom – a protein called sphingomyelinase D. This is an enzyme that …
If you don’t think those “lipid nanoparticles” of the mRNA vaccines can’t “act like viruses” and basically pass “disease” to a NEW HOST – read this. LNPs ≈ VLPs.
EVERYTHING we are seeing in vaccine medicine now is a COPY of what nature did about 70-100 million years ago, in the insect world. Once I realized this, I was able to pattern this stuff all over what Big Pharma is doing, and get ahead of their game.
This post is probably going to go over a lot of heads, but I think scientists will find it disturbing until they find it compelling, and then ultimately find it satisfying. Creation teaches us – not the other way around.
OK – we’re going to have some fun here – but stick with me, and you could learn A LOT. Cue the music! Borrowed from Wheatie! Previous posts helped put both the SPIKE PROTEIN DISEASE and the SPIKE PROTEIN VACCINE into deep perspective. We were seeing that the SOLUTION was a significant part of the …
Deplorable Patriot hit the nail on the head here. Before I accepted the awful fact that these vaccines are not what we thought they were, I didn’t believe shedding could be real. Oh, boy, was I wrong about that.
Our dear boss, Wolf, has been busy putting together scientific primers on just what it is the various shots and inoculations marketed to be preventative of severe symptoms of COVID do, but what hasn’t been addressed for those of us who chose not to be shot up with whatever is in the syringes is how …
This was beautiful – mainstream science and medicine starting to question the Fauci BS. Revel in it. Some of this is now “accepted” – all of it will be, soon enough. We’re headed back to sanity, folks.
This is a very important video you don’t want to miss. It just came out, and the doctor is a guy I’ve been following. He chooses his words carefully, to stay inside the establishment where he can publish some of the top papers, but he speaks the truth at all times. Don’t let the video …
This is where I was blown away by the Pfizer leak out of Japan. The targeting of the ovaries.
AYE-YI-YI. What is one supposed to think? Good GRIEF.
TL;DR – you MUST listen to a short podcast of a scientist revealing the latest research on the spike protein vaccines. The VACCINE ITSELF (not just the spike protein – the mRNA vaccine itself) is persistent and is not only concentrating in ovaries – THE VACCINE ITSELF IS EXCRETED – e.g., in breast milk. Meaning …
Now you can see it very easily – the enemy threw that “Magnet Challenge” out to muddy the water as we were gaining understanding. But here is where I started to look at it experimentally – give it a real examination – and come away fairly doubtful that there is anything to it. The Magnet Challenge is bad science. It may be well-motivated, but it’s quality disinformation. Top-shelf stuff – ACTIVE DISINFORMATION to make people SELF-DISCREDIT – meant to insulate the controlled and groomed experts by discrediting smart people outside of controlled science.
Wherein we examine, in something like “MythBusters” style, the dubious “Magnet Challenge”, without relying (too much) on the anti-scientific crutch of scientific authority First, a confession. The main reason I am attracted to these videos of people sticking magnets to the COVID vaccination injection sites on their shoulders, is that I love to watch normal …
This is where I actually call out the other side for trying to mislead our side with the “Magnet Challenge”. At this point I really understand how utterly misleading this trick is, and WHY it was inflicted on us.
Wherein we look at how the COVID scammers are now using “magnetic” disinformation to try to escape justice for REAL abuse of liposome biotechnology to achieve [most likely contraceptive] vaccine persistence and migration. TL;DR – after mRNA vaccine persistence and anatomical migration were revealed in leaked Pfizer data, explaining “shedding” via persistent liposomes, the COVID …
This is where I investigate the origins of one of the “fake facts” used to trip up the doctors opposed to the spike protein mRNA vaccines. I am convinced that this was some kind of discreditation operation – a precursor to the “Magnet Challenge” psy-op.
This is for the historical record. I hope that this analysis gets to the “dissident scientists” involved, but even if it never does, future historians will get a powerful look at what I call “Fake Science” – the establishment’s phony, deceptive and controlled scientific complex – and how infiltration, control, and discreditation of dissident populist …
At this point, you should be ready for more information – about WHERE vaccination is going.
5.
New Vaccines – The Great Crony Blame Escape
It took me a while to put 2 and 2 together, but when I first saw the June 7 cover article on my new “vaccine snitch”, Chemical & Engineering News, something bothered me about it.
This is more excellent reporting by Ryan Cross, who routinely ferrets out (pun intended) the full story on virus science and vaccine technology, as available to “public science” – to be distinguished from the deeply hidden stuff. Cross never adds in any politics, crime, depolitical deconstruction, “conspiracy theory” speculation, or any of the things that are MY JOB. I have to respect that. This is the way THE NEWS used to be.
get the facts
understand the facts
teach the facts
teach the understanding
light fuse, run away
AH. I love my job. BE THE FUSE.
Figuring out the criminality of the government, industry, and financial backers – getting past the obscurantism, deceptions, and lies – that is OUR JOB – We The People – for we are (now that Merrick Garland soils the DOJ with Chicago communism) the
REAL DEPARTMENT OF JUSTICE.
Yup. WE are not the communist insurrection and their corporate cronies, destroying everything in their path to money and power, including honest science and doctor-patient medicine.
We are (and like Confucius, I WANT them to hate this) the RESURRECTION.
The RESURRECTION vs. The INSURRECTION.
Eat your own label, insurrectionist commies. It’s good for you!
OK, back to science.
I really encourage you all to read this full article, which is written so that the general public can understand 99% of it easily. You will learn a LOT about vaccine technology. I will move you along through it, skipping over things, but when we’re done, consider reading the whole thing both WITH and FOR greater understanding.
I will try to only quote selectively from it, as I capture a few key points. But I can do no better than to give C&EN’s own “TL;DR” which they label “In brief“:
Vaccines are synonymous with shots, but it doesn’t have to be that way. More than a dozen groups are working on COVID-19 vaccines that can be squirted or sprayed into the nose instead of injected in the arm. Besides the potential practical advantage of easier administration, these vaccines could trigger the mucosal immune system to make antibodies in the nose and help stop the coronavirus at its point of entry. It sounds great, but the mucosal immune system is hard to study, and pharma companies have been reluctant to invest in the needle-free approach. Mucosal immunologists and intranasal vaccine developers are hoping the pandemic will change that.
This is where my first “2+2” $0.02 comes in.
Note the final statement:
Mucosal immunologists and intranasal vaccine developers are hoping the pandemic will change that.
It’s not the phony pandemic that is “going to” change delivery route. It’s already happening, in my opinion, due to the massive unveiling of not just the problems of the systemic gene therapy vaccines, but the clear motivations behind these vaccines, some of which were not just hidden from the public, but also from the scientific community, which I believe is now getting WISE.
Stated more simply, OUR PRESSURE in getting out the TRUTH about the existing vaccines is forcing the industry to react to vaccine shortcomings they WILL NOT ADMIT otherwise. The industry is likely also under forces from ABOVE THEM which are also being exposed.
You will see this as I go through the article.
The most powerful weapons in our hands are the UNDERSTANDINGS of the following:
spike protein toxicity
vaccine persistence
vaccine migration
spike genetic incorporation
Fauci’s reverse transcription obsession
Bill Gates’ “pre-programming the experts”
Zuckerberg connection to Baric lab
irrational hatred of cheap available therapeutics
generality of therapeutics being fought, thus…
the enabling of ChiCom manipulations
ovarian and testicular targeting
hiding of evolutionary knowledge
“circuits of plausibility” to create errors and crises
Put these things together and the “easy path” of systemic vaccines which do NOT mimic stimulation of natural immunity as well as NASAL VACCINES do, has been chosen under the cover of simplicity, but in reality because it always lies closer to what the industry TRULY wants, e.g., right now, gene therapies, where they NEED to target many specific organs. Nasal vaccination is a niche safety point which has always WAITED while systemic gets the action the deep backers want and NEED.
When it’s just easier and possible to do the wrong thing they want, they DO IT.
The current gene therapy desideratum – organ specificity – is actually in another article in the same issue of C&EN, talking about CRISPR, anti-CRISPR, and how to make gene therapy not have side effects, a point which is admitted more openly now that they are “safe on first” by having “proven” that gene therapy “works”.
Such a scam.
But it gets worse. Industry motives are not the motives of those who manipulate THEM.
As you read the rest of this, note that the “running dog” industry layer, which now performs for taskmaster commies, is also manipulated by THEIR true masters, the global elite, now looking at pesticides for humans, and particularly deplorables. It’s clear to me now, after the ovarian, placental, and testicular actions of the spike protein broke media containment, that the reason the entire vaccine industry jumped into full spike protein gene therapy tests masquerading as necessary vaccines is manipulation by the one guy who double-controls vaccine technology via “owning” CEPI – and that would be BILL GATES.
Yes, that Bill Gates, whose father is standing behind Fauci here.
Thus, when both the Gates Foundation and CEPI back some project, it’s Bill Gates getting TWO SCOOPS of control.
Note also Event 201 backing.
With Fauci and the Faucists inside government, and Bill Gates on the outside, there was no way that safer, metered, recombinant spike protein tech or peptide subunit tech was ever going to go first. They needed the new tech given a carte blanche, and they got it. This plus the “crisis” allowed the full spike protein’s foot to be shoved in America’s door, past everybody who might have questioned it.
This is one of the guys who spotted the “snake protein analogy” first, in what would have been time to alter the landscape.
No longer random, this is what happens when people get in the way of a conspiracy TWO LEVELS UP, where the really big boys and girls play. There are money motivations in between, but this guy’s real crime was potentially interfering with “the spike must flow”.
Have I raised your suspicions?
GOOD! Let’s look more deeply at the article now.
In fact, the mucosal membranes that line our airways, digestive systems, and reproductive tracts are often the first parts of our bodies to face an invading pathogen. A network of immune cells resides underneath our mucous membranes, or mucosae, and forms a front line of defense against invaders, and they prevent most infections from taking root. This is the mucosal immune system, and some immunologists think we have been seriously underestimating it.
“When you think about it, that’s where we acquire most of our infections: we inhale them, we consume them, or we get them through sex,” says Michael W. Russell, a mucosal immunologist and professor emeritus at the University at Buffalo.
This is where we begin to realize that mucosal immunity and systemic immunity are NOT the same thing. And it doesn’t have to be “either/or” – you can have BOTH. There are many plausible reasons for one over the other, but it will become clear that using the mucosal pathway adheres more strongly to the natural “API” of immunity by “contact”, if you will, with the pathogen, rather than sudden systemic introduction.
Have we really been underestimating it? Or have we been IGNORING IT ON PURPOSE at the highest motivational levels of power?
In my opinion, if the powers that be in VAXX WORLD would have been looking out for us all this time, there would have been stronger forces pushing researchers toward mucosal immunity. The problem is, that kind of naturalistic and patient-centered thinking is a problem for those who see vaccination as more of a path to power or other ends, particularly SOCIAL ends, rather than as part of a path to individual health. Nothing has made this more clear than the “pandemic”, controlled by “experts” who seemed not to know what they were doing.
Are you now starting to understand how and why conspiracies are intentionally mischaracterized as giant joint illicit cooperation, when they are in fact TOWERS OF LAYERS OF INTERNAL DECEPTIONS?
Good. Let’s move on.
Our mucosal immune cells make a special class of antibodies that are constantly secreted from the mucous membranes to protect the nose, gut, and other vulnerable sites from pathogens we’ve seen in the past. “But if you don’t stimulate the immune system in the mucosae, you don’t obtain mucosal immune responses,” says Pierre Charneau, head of the Molecular Virology and Vaccinology Unit at the Pasteur Institute.
Yet most research on SARS-CoV-2 and our immune systems has overlooked mucosal immunity in favor of the easier-to-study systemic immunity. “When the pandemic hit last year and I started to see papers coming out about immunity, it really quite staggered me to see an absence of attention to the mucosal immune response,” Russell says.
See that? The TILT of the field – the RUSH to systemic – that is a SOCIAL phenomenon – and socialists, or believers in the effectiveness of socialist tactics, like me – will tell you very honestly that science can be controlled SOCIALLY – that the SOCIAL aspects of science are not all warm campfires around each other’s blogs, but actually PART OF THE FIGHT that controls WHAT SCIENCE THINKS and WHAT SCIENCE DOES.
Or like this blog. I’m just honest about it.
I keep telling people that the “jabs” were PUSHED and SHAPED to be what they were – for REASONS – diverse yet all valid – which compromised all the insiders to DO WHAT WAS NEEDED to create what was needed at the TOP:
SYSTEMICALLY MOBILE, GONAD-TARGETING, SPIKE PROTEIN OVERDOSE INJECTIONS AT CONTRACEPTIVE LEVELS.
Stated more generally, it wasn’t a BUG – it was a FEATURE. And we were RUSHED into testing (if not USING) the feature ON PURPOSE.
Now – remember how COVER works – these vaccines did what they were SUPPOSED to do in our little world – but they also did what other people wanted in THEIR little and very exclusive world of “human benefactors”.
We move on.
Charneau and a group of scientists in Paris have shown that natural SARS-CoV-2 infections trigger both systemic and mucosal immunity. But our current crop of COVID-19 vaccines offer only systemic protection. Developing vaccines that are sprayed up the nose, rather than injected into the arm, could change that, Charneau says. Mucosal immunity in our noses could be like a guard at the door, potentially helping stop even small infections of SARS-CoV-2 right where they start.
It’s a tantalizing notion, but whether it’s a viable one is up for debate.
Now, the FIRST thing I think when I read this is “hey, that means my disease immunity is almost certainly BETTER than vaccine immunity – as doctors have all known for decades prior to COVID-19”.
Of course, we know they lied about that to “prevent vaccine hesitancy”. Or stated using different words, “to prevent picking the mild disease over the vaccine in the safer age groups, the latter being most of them”.
Do you see that? Almost ANY lie can be justified in the name of “overcoming vaccine hesitancy”. Who, besides Fauci and CDC is so obsessed with that Swiss army knife excuse and viral talking point?
But you know what – Fauci knew this – and Rand Paul knew Fauci knew this. So when Rand Paul went after Fauci on reinfection of COVID recoverees, like both HIM and ME, he knew Fauci was on THIN ICE.
But toss that all aside. At BEST, we went straight after systemic immunity “because emergency”. But it turned out that it wasn’t all that big of an emergency, and that’s where it gets interesting.
As I said, things are changing very rapidly now – obviously getting a technology on the cover of Chemical & Engineering News is a big deal.
And I quote:
After all, the pandemic provided a chance for messenger RNA (mRNA) vaccine technology to finally prove its worth, and mucosal immunologists are hoping that this will be a moment for intranasal vaccines to do the same. “This climate is a game changer,” says Hiroshi Kiyono, codirector of the University of California San Diego Center for Mucosal Immunology, Allergy, and Vaccines. “This is a great opportunity to advance nasal vaccines, not just for COVID-19 but for other respiratory diseases.”
YUP. That’s the way CRISIS MECHANICS works. The “crisis” is just going to CHANGE, to get people to do a NEXT NEW WRONG THING.
My advice to Hiroshi Kiyono would be WATCH OUT – you are going to be subjected to many pressures that bring mucosal vaccines TOWARD viability as spike protein contraceptives. There will be pressure AWAY FROM doing what is best for the PATIENT, and TOWARD doing what is best for the SCIENCE and the RESEARCH, and that “better” will just happen to be better for surreptitious social or even sociobiological manipulations, too.
This is just a HEADS UP.
I’ve been there. Fake Science is not a very nice place to be when billions or trillions of dollars are on the line, and YOU’RE IN THE WAY.
At this point, the article goes into the HISTORY of intranasal vaccines, intranasal being one of the very best routes for respiratory virus vaccines. I’m going to SKIP over all that, even though there are some very interesting aspects to that history. I don’t really see any smoking guns of obstruction or sabotage, but it’s pretty clear that intranasal was a bit of a black sheep, and fended for itself.
Now, HERE is what’s interesting. Which intranasal vaccines are “in the pipeline”?
TURN YOUR NOSE UP
More than a dozen intranasal vaccines are in development for COVID-19. Here are several to keep an eye on.
Phase 1
Altimmune ▸ Adenoviral vector
AstraZeneca and University of Oxford ▸ Adenoviral vector
Beijing Wantai Biological Pharmacy, University of Hong Kong, and Xiamen University ▸ Live attenuated influenza virus vector
Bharat Biotech and Washington University in St. Louis ▸ Adenoviral vector
Codagenix and Serum Institute of India ▸ Live attenuated SARS-CoV-2
Laboratorio Avi-Mex and Icahn School of Medicine at Mount Sinai ▸ Live Newcastle disease virus vector
Meissa Vaccines ▸ Live attenuated respiratory syncytial virus vector
Preclinical
AuraVax and University of Houston ▸ Recombinant spike protein with adjuvant
HanaVax and University of Tokyo ▸ Recombinant spike protein with adjuvant
TheraVectys and Pasteur Institute ▸ Lentiviral vector
University of Eastern Finland and University of Helsinki ▸ Adenoviral vector
Sources: Companies, World Health Organization.
Now, that may not look like much, but there is a TON to unpack, because we not only have OLD “new” technologies in a NEW route – we have NEW “new” technologies to explain – and in a new route.
If you don’t think the other side can cause trouble with their spike protein attack through the nose, you are sorely underestimating the ability of those who CONTROL SCIENCE to “get there first” and mislead the rest of the pack.
Remember – if you think like me, then you know people have been doing this crap for billions of years in THIS universe alone. We’re just “rediscovering reality under supervision” on one more planet. The lies are OLD. Very, very OLD. And as I like to say, “Satan weaponizes everything.”
The adenoviral vectors we’ve seen. That’s AstraZeneca, Johnson+Johnson, Sputnik V, and others. The only difference is that they’re going through the nose, where these viruses are actually supposed to go.
There is a LOT of possibility that this move could solve the biggest problems with these vaccines. IF the nasal delivery route is a kind of highly evolved and intelligent natural “attenuation gauntlet” for viruses, then the outcomes for these vaccines could be uniformly improved.
IF that is indeed the case, then I’m going to be a “toldjaso” asshole and use this as part of my explanation of why “they” have divided us in the specific way they have, over the topic of evolution, separating the “intelligence” side from the “evolutionary science” side, thus pushing the latter to view evolution as DUMB instead of “cautiously and obsessively path-checking”, which looks dumb to localized intelligence that doesn’t know how to keep its biases in its own lane.
These vaccines also introduce lentiviral vectors – pretty much the same thing as the adenoviral vectors, just a different virus. Again, this is new, so it could be interesting.
Another returning technology is Recombinant spike protein with adjuvant. That is basically Novavax, which we have not really had a chance to deconstruct, because there is not yet much public information on safety or efficacy. So a big QUESTION MARK on that one. In principle this should be safer than genetic technologies, both because there are ZERO risks of genomic incorporation (see Jaenisch for SARS-CoV-2 incorporation), and because there are no possibilities of unmetered “fountaining” of spike protein.
First up in technologies we have NOT seen yet: Live attenuated SARS-CoV-2.
We have already used INACTIVATED SARS-CoV-2 – that would include the Chinese Sinovac vaccine, which is rebranded as CoronaVac in the West. I’ve been cautioning that I believe “bad lots” of CoronaVac, which are incompletely inactivated, have been passed off, which would explain why there is typically a surge in cases right when countries start using CoronaVac. Obviously that’s good for business, and we know how Chinese business works. The only other explanation would be that PCR is picking up vaccine during rollout, and I’m half-way thinking that’s a better explanation, were I not so familiar with ChiComs and the corruption they spread.
However, we have NOT yet seen live attenuated virus. This could be GREAT – or it could have a whole NEW bag of problems. I’m very “wait and see” on this.
The real BIGGIES of the new intranasal vaccines are these:
Live attenuated influenza virus vector
Live Newcastle disease virus vector
Live attenuated respiratory syncytial virus vector
Unlike the adenoviral vector vaccines, which are basically “working but dead mRNA in a dead skin suit of a different virus that’s easy to work with”, these vectors are LIVE VIRUSES with “something extra” (like the spike protein) inserted into their genes, making them chimeric at the genetic level, not just the vector level.
These vaccine viruses are actually designed to “run a bit”. They INFECT YOU with instructions to crank out spike protein.
This is where things start getting weird, and it’s hard to trust a world which contains both THIS technology AND the CCP.
You know what I’m sayin’?
But now let’s look at all these. We suddenly have a LOT of vaccines to keep track of.
It’s gonna take some work – but we have to do it. We cannot let them keep experimenting on us like they did, while CHINA did almost NO “experimentation” on its people.
Understand what I’m sayin’?
Good.
Now – the rest of the article is basically the HOPES and the NOPES of the intranasal route. Some of the possibilities here are MIND-BOGGLINGLY GOOD.
Mucosal immune cells constantly make an antibody called secretory immunoglobulin A (IgA), which gets released into the mucous membranes of the nose, mouth, airways, and gut. Pound for pound, we produce more IgA than any other antibody, Russell says, although most of it is broken down and sneezed, coughed, or pooped out within a few days.
And critically, while injected vaccines induce only systemic immunity, vaccines delivered to mucosal sites can induce both systemic and mucosal immunity, he says.
That fact is evident in animal studies of a vaccine being developed by David T. Curiel and Michael Diamond at Washington University in St. Louis. Both the injected and intranasal forms of their vaccine triggered the production of IgG antibodies, but only the intranasal route triggered mucosal immune cells to secrete IgA that blocked the virus from replicating in the nose. A day after they published preprint data demonstrating as much in July 2020, the Indian vaccine company Bharat Biotech contacted the university’s technology-transfer office to license the intranasal vaccine in India, where it is being tested in a clinical trial. “How that will play out clinically remains to be seen,” Curiel says. “But this animal model finding suggests, qualitatively, that we have some additional benefit.”
It is very clear that – for a respiratory disease – there is an advantage to having “naturally obtained” respiratory mucosal immunity.
All that said, we’re still talking spike protein. But if the intranasal route can keep it out of the ovaries, testicles, and placenta – GREAT.
And THAT brings me to another great C&EN report by Ryan Cross – everything you want to know and need to know about those damned lipid nanoparticles.
Without these lipid shells, there would be no mRNA vaccines for COVID-19
Fragile mRNA molecules used in COVID-19 vaccines can’t get into cells on their own. They owe their success to lipid nanoparticles that took decades to refine
Without doing any “gotcha” journalism, Cross reveals the GOOD, the BAD, and the UGLY about these lipid nanoparticles.
The impression I get is that this field was dogged with problems, most of which were overcome, but not all.
So, without getting into the details, all these criticisms of the lipid nanotech that you are hearing are NOT “conspiracy theories” – the scientists are TALKING ABOUT THEM as real problems they’re trying to solve, with various degrees of success, in this report.
To me, it was very clear that people WAY above these scientists needed to PUSH this LNP (lipid nanoparticle) technology, necessary for GENE THERAPY, into acceptance using the phony plague.
If you don’t want to take this stuff, STAND UP for your rights. Otherwise, it’s over the hill, the horses are OUT OF THE BARN, the fence is open and the cattle are GONE.
BUT – I think that if we keep pushing the REALITIES of these vaccines, we can make the “mandate martinets” crawl back into their Fuehrer Bunkers and leave us alone.
And THAT is worth it.
W
PSSSST – hey, DOJ and FBI. Want to see some audit results?
THEY’RE EXPLOSIVE!
Seriously, you injustice-perpetuating assholes deserve to be trolled. Your phony allegations of “violence” or even potential violence by the QAnon “believers” are an affront to Americans. They’re a SICKNESS coated with a patina of professionalism. You should be ashamed of yourselves.
This is a very important video you don’t want to miss. It just came out, and the doctor is a guy I’ve been following. He chooses his words carefully, to stay inside the establishment where he can publish some of the top papers, but he speaks the truth at all times.
Don’t let the video title fool you – the doc is much more “reserved” than big scary death headlines, but that is EXACTLY WHAT HE TALKS ABOUT.
The brown recluse is related to several other recluses, and a couple of other families of spiders, that all have a similar venom – a protein called sphingomyelinase D. This is an enzyme that degrades animal tissues, and is responsible for the very distinctive giant-pock-mark-wound-forming symptoms of recluse bites. The brown recluse does not have as much of this protein in its venom as do some other recluses. The worst recluse, distributed over several countries in South America, has roughly ten times as much sphingomyelinase D as the North American brown recluse. Bites by THAT recluse not only result in deep wounds – they result in SYSTEMIC effects much more often than do bites of the “mere” brown recluse. Fatalities are much more common.
But just stop and think – THAT is how potent protein venoms can be. The tiny bite of a spider with a tiny bit of a protein in it – mere micrograms – can leave a 10-inch hole in the leg, with life-threatening systemic effects.
Snake venoms use different proteins from spiders in their venoms. Some spiders like the black widow have neurotoxic venoms, which affect nervous function, and some snakes like cobras have DIFFERENT neurotoxic venoms.
The honey badger is, weirdly, somewhat immune to the paralyzing neurotoxic cobra venom (jump to near the end of the video).
Many snakes have hemotoxic venoms, and THOSE venoms tend to cause cardiovascular problems. Interestingly, one of those problems is a somewhat rare clotting disorder called thrombocytopenia.
Thus, when I heard that this uncommon symptom was sometimes occurring as a coronavirus vaccine adverse effect, I suspected that there might be a protein cause – the spike protein – acting similarly to proteins in those hemotoxic snake venoms.
If that were the case, we should expect the same effect to be caused by COVID-19 itself, sometimes.
Should we just jump on such an analogy? One that is based on the ASSUMPTION that the spike protein is causing thrombocytopenia? Or at least similarly involved in the two cases?
Let’s think about this.
One of the things which is most fascinating about the BRANCH COVIDIANS – including the high clergy in government and media – is just how STRONGLY they tend to discourage alternative perspectives on COVID-19 – doing so in a way which is alarming even by the normal standards of narrative-setting and enforcement.
For example, at the very beginning, social media gatekeepers were needlessly hostile to Dr. Cameron Kyle-Sidell’s “high-altitude sickness” perspective on COVID-19 hypoxia, despite the fact that this led to a very beneficial new policy on keeping patients OFF vents, probably saving millions of lives, as well as giving us all a better understanding of HOW COVID-19 is and (more importantly) is NOT damaging lungs of patients.
Millions of lives. Think about it. Not a bad save – unless you want a guy named Trump GONE by any means necessary.
Now, some of these “different” perspectives can and do lead to non-working or just plain wrong theories at a micro-level, but so can ANY perspective. Dr. Kyle-Sidell’s ideas led to a variety of hemoglobin-related and malaria-related theories of COVID-19 which were neither fundamentally true nor useful, and which theories died on their own, without any need for censorship, but which were part of a questioning movement which also led to increased recognition of the endothelial nature of the coronavirus attack on patients’ lungs and other organs.
A CHANGE in perspective which WAS and IS fruitful.
Whether we are talking about damage to capillaries in the lungs, vein occlusions in the retina, or organ damage, particularly in the heart or kidneys, it appears that the cardiovascular endothelium is where COVID-19 does the most damage.
Comorbidities which already involve damage or potential damage to blood vessels – particularly diabetes and endocrine or cardiovascular diseases – are thus particularly dangerous, as SARS-CoV-2 and (presumably) its spike protein – which is what attacks cells – would be attacking an already weak point of failure.
I want to thank GrandmaInTexas for those two most recent examples of COVID vaccinations precipitating fatal outcomes in people with both diagnosed and undiagnosed comorbidities. For the record, Dan Kaminsky’s vaccine was undoubtedly either Pfizer, Moderna, or Johnson+Johnson, while Actor Vivekh’s vaccine was Covaxin. The former 3 are all genetic vaccines – the latter is inactivated whole virus. All of them use the WHOLE spike protein in some form or another to trigger immunity.
Here is a handy principle which I call “spike protein equivalence”, as a special case of “vaccine immunological equivalence”.
If some affliction, condition, or mere FACTOR happens to be BAD for a potential victim of COVID-19 itself, then it’s also going to be bad for recipients of the vaccine. The difference is only that – most likely – in MOST cases – the vaccine constitutes a far lighter assault on the patient, than the disease itself.
THAT is the basic logic of vaccination. REDUCE THE RISK. But nonetheless, ACCEPT A RISK.
Do not kid yourself. The WHOLE POINT of vaccines is to entertain a lesser risk – a risk that is not as bad as the disease. The only question is “how less bad” does any particular vaccine happen to be. Based upon that information, one has INFORMED CONSENT.
People need to understand risks clearly in order to take those risks smartly.
Or NOT take them. Where the lyric“If you choose not to decide, you still have made a choice” operates against the circling helicopters of COVID-19 and any successor viruses.
When we do not honestly face the risks and benefits of vaccines, we end up with the psychotic disconnect we now see, where people who SHOULD be voices of reason and trust – like the CDC – are LYING and losing half or more of the nation as trusting followers.
Rather than re-hash here how the CDC has lied to us already, or why the handy principles of “spike protein equivalence” and “snake protein analogy” work so well in understanding COVID disease and vaccine risks, let me give you links to my most recent discussions of the relevant thought.
The FIRST ONE is probably the most comprehensive, and helps to understand the rest.
PREFACE I thought that I might withhold this post on Easter Sunday, and then I changed my mind, thanks to Deplorable Patriot, Trump, Gab and Jesus. If anybody ever FOUGHT on Easter Sunday, it was Christ. It’s time to FOLLOW POINT. The Branch Covidians have taken a toll, but the WAR is turning, and – …
Alternate Title: Is Persistent Reverse Transcription a Hidden Virus/Vaccine Objective? Gloating Pre-Preface There are few feelings of satisfaction like opening up the NEWS and knowing one’s theories and understandings are WORKING even better than one thought. Let’s see if they use this one for damage control, and get the “new science” out before the STORY …
Every coronavirus vaccine so far has shown us SOME defect upon mass release, which was NOT evident in EVEN phase III clinical trials. Look HERE for a searchable PDF document of adverse effects from the Pfizer vaccine: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/977005/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print.pdf Check out these videos on the low-platelet clotting problem from the Oxford/Astrazeneca vaccine. Here is a fantastic …
I saw an excellent explanation of the clotting problem with the AstraZeneca vaccine against SARS-CoV-2 / COVID-19 here: The doctor, Dr. ZDogg, MD, offers an exceptionally clear explanation of both what is going on with the AstraZeneca vaccine, and why its distribution was halted or limited in some places for some age groups of patients. …
I am not the only person who is seeing that the SPIKE PROTEIN and variants are interesting beasts. Cthulhu tipped me off to THESE TWO GEMS by Karl Denninger, which are extraordinarily worthwhile:
Even though these deal primarily with spike protein equivalence rather than the snake protein analogy, the latter of which Cthulhu mentioned in his tip (he knew I would like these), there is some even more shocking perspective in the second link, in which Denninger simply asks – why did we use the WHOLE sequence of the spike protein which we received from China?
Beyond simple blame games, in which I could postulate that “whole spike protein vaccines” may have resulted from dumb psychology, or even malicious treachery by one or more parties, I can ALSO place Denninger’s question in the context of both failing to ask “Stoecker questions” about “should we base vaccines on the WHOLE spike protein?”, AND the idea that – intentionally or unintentionally – by whoever – we essentially fell into China’s version of the plot of Species…..
OR – if we don’t want to be all negative about things, try the Earth-saving genetic sequence reconstruction sub-plot of The Fifth Element, with a few more plot devices about process-skipping on the internal growth code, also a bit of a lesson.
Is such “gain of function” good or bad? One could view horsepox-based smallpox vaccine adoption as “gain of function” – a low-level example of the intelligent acceleration of evolution as a “natural” part of evolution itself.
As an aside, IMO the reason they use women for these scenes is ultimately the same reason the spike protein seems to target women’s physiology more than men’s, and that men are actually the first utilitarian sex robots, but – well – it’s so simple, it’s complicated. Patriarchy is both overrated and overstated, shall we just say.
ANYWAY, back to snakebite. “Cleopatra meets spike protein” – only worse.
VAERS reports a breastfeeding five-month old infant has died of TTP – a rare clotting disorder linked to, yes, low platelets. He became ill one day after his mother received her second @pfizer shot.
I actually saved that whole report, which is not easily linked, as a series of images:
Before I go on, let me just say that immunology strikes me as a lot like quantum mechanics. If anybody says they truly understand it, it’s almost a sign that they don’t. Nevertheless, basic suspicions work like crazy in either field, which is, again, interesting. In either field, it doesn’t take a genius to see that – 99% of the time – a snake in the grass IS a snake in the grass.
Already, the entire Snopesian Empire is fired up over this case.
SEEK anything related, and you will FIND – both WHEAT and CHAFF.
READ, and you will FIND – both INTERESTING and HOLLOW.
No matter how many guns they get working and belt-fed, cross-firing with their diversionary strawman arguments on this one case, the fact of the matter is that TTP is intimately linked to immune disorders, immune responses, and vaccination, so if it shows up, vaccines are and will remain the likeliest suspect NO MATTER WHAT. All Fauci’s horses and all Pfizer’s men are not going to get rid of the NOTABLY MANY cases of TTP , other thrombocytopenic clotting disorders, and clotting disorders in general, which are showing up in (1) COVID cases, (2) COVID recoverees, (3) vaccination adverse events, and (4) vaccination of recoverees in particular.
The relationship of TTP to vaccines and “malappropriate antibodies” in particular is UNDERSTOOD SCIENCE. This is not going away, despite the near-dogmatic narrative that “COVID vaccines do no harm” at the public level, reinforced by the narrative that “fighting vaccine hesitancy is worth LYING about adverse effects”.
No, it’s not.
Skip the following scientific review unless you feel nerdy. I recommend just skimming in either case. But I promise – the deeper you dig here, the more WHEAT you will find.
TTP as a function of age of onset and mechanism for ADAMTS13 deficiency. The proportions of adulthood-/childhood-onset TTP and acquired/inherited TTP, respectively, presented in this figure were calculated from the data of the French Registry for TTP (840 patients).10,13 These data are in agreement with miscellaneous demographic data reported in the literature by other teams.3,5-9 The diagram shows 100 patients with TTP, each patient being represented by a symbol, either a square for patients with adulthood-onset TTP (91%) or a circle for patients with childhood-onset TTP (9%). Acquired TTP is presented in blue (94.5%), and inherited TTP (USS) in red (5.5%). Interestingly, the proportion of USS is very low (2.5%) in adulthood-onset TTP, whereas it is as high as 33% in childhood-onset USS.
Abstract
Thrombotic thrombocytopenic purpura (TTP) is a rare and life-threatening thrombotic microangiopathy characterized by microangiopathic hemolytic anemia, severe thrombocytopenia, and organ ischemia linked to disseminated microvascular platelet rich-thrombi. TTP is specifically related to a severe deficiency in ADAMTS13 (a disintegrin and metalloprotease with thrombospondin type 1 repeats, member 13), the specific von Willebrand factor-cleaving protease. ADAMTS13 deficiency is most frequently acquired via ADAMTS13 autoantibodies, but rarely, it is inherited via mutations of the ADAMTS13 gene. The first acute episode of TTP usually occurs during adulthood, with a predominant anti-ADAMTS13 autoimmune etiology. In rare cases, however, TTP begins as soon as childhood, with frequent inherited forms. TTP is ∼2-fold more frequent in women, and its outcome is characterized by a relapsing tendency. Rapid recognition of TTP is crucial to initiate appropriate treatment. The first-line therapy for acute TTP is based on daily therapeutic plasma exchange supplying deficient ADAMTS13, with or without steroids. Additional immune modulators targeting ADAMTS13 autoantibodies are mainly based on steroids and the humanized anti-CD20 monoclonal antibody rituximab. In refractory or unresponsive TTP, more intensive therapies including twice-daily plasma exchange; pulses of cyclophosphamide, vincristine, or cyclosporine A; or salvage splenectomy are considered. New drugs including N-acetylcysteine, bortezomib, recombinant ADAMTS13, and caplacizumab show promise in the management of TTP. Also, long-term follow-up of patients with TTP is crucial to identify the occurrence of other autoimmune diseases, to control relapses, and to evaluate psychophysical sequelae. Further development of both patients’ registries worldwide and innovative drugs is still needed to improve TTP management.
So what does TTP look like?
See those pictures? You may want to THINK TWICE about the coronavirus vaccine if you ALREADY have this risky potential outcome of either the disease or the vaccine. I have a link showing that TTP is a high risk in COVID recoverees who get any of the vaccines – I just can’t find it now.
We ARE seeing some public recognition of adverse effects now:
However, as is visible in this article, we are not seeing ANY contraindications to vaccination being admitted publicly. The advice tends to be “get vaccinated, and if you don’t die, but have bad symptoms, see your doctor.
“Sure, Dr. Stalin. Sure. Say – you don’t have any recommendations to PREVENT THIS from happening again to somebody else now, do you? Those would be called ‘contraindications’. Most drugs have them.”
However, I think some recognition is coming. And why is that? Well…..
“When the people have any power to object to a socialist solution, a deniable 5% fait accompli is always more desirable to socialists than a negotiated 50% solution, because they can always negotiate on the remaining 95%.” -Wolf Moon When I first heard about a case of a miscarriage by a pregnant doctor, due to …
…..we discussed other disorders – affecting reproductive health, you might say – that MAY or MAY NOT be mediated through the SAME or DIFFERENT activities of the spike protein.
THAT is an interesting question, actually. How economic is spike protein activity? How MUCH strategic information is carried, and at what density? How efficient ARE proteins at carrying smaller-molecular strategies into “genetic warfare”? We may not have those answers yet – and certainly not in PUBLIC SCIENCE – for some time.
Still, I think these questions will eventually be asked and answered, because the menstrual/gestational and clotting effects of the vaccines are so startling, that people are going to ask questions and get answers, whether the “mainstream” (meaning government/corporate) media wants to ask them or not, or to see them answered.
In that regard, we will carry on, asking questions and getting answers, carrying the principle of SPIKE PROTEIN EQUIVALENCE with us, as a handy and useful physiological tool.
The idea of SNAKE PROTEIN ANALOGY will become less of a medical utility, and more of a METAPHOR.
There is a refreshing honesty and innocence in this guy’s work. But more than that, he just has a way of catching small details that everybody else misses, and making them beautifully prominent. His portraits of famous figures are quite wonderful in this way. He will completely drop many of the features of those people that I love and see prominently as part of my personal recognition algos, and yet childishly play up awesome things I never noticed.
And with that, let’s talk about Eve.
Our next installment is going to go BACK IN TIME, and show you something very startling about WHEN all this COVID vaccine technology was actually invented.
A lot earlier than anybody wants to admit publicly. Here is a hint.