The Pub is OPEN again!
With a blend of humor and seriousness, like any good bar, we celebrate this grand re-opening of WOLF’S PUB on Christmas Eve, December 24, 2021, by actually opening near closing time on Christmas Eve Eve, but what the heck.
IT’S ALMOST CHRISTMAS.
While our beloved bartender takes a needed break of unknown duration, we will ENDEAVOR TO PERSEVERE.

I will admit right off the cricket bat that this here substitute bartender doesn’t know jack shit about alcohol compared to our regular one, so he’s going to have to substitute some rather wild and crazy concoctions for the drinks, seeing as he does have some experience with ALCOHOLS OF THE WRONG KIND.
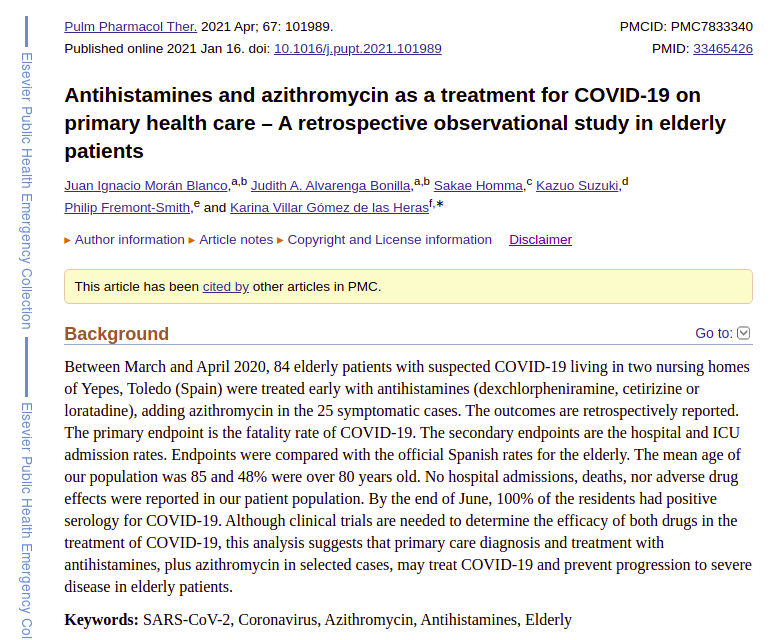
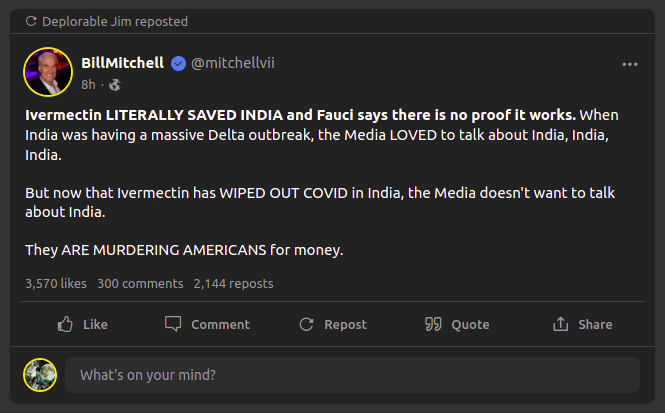
And while we’re at it, THANK GOD FOR INDIA, and another alcohol with medicinal applications!!!


Truthfully, some of the best ideas in science are to be found at local pubs, when the research groups go out and have enough beer and wine to begin saying what they REALLY think about this or that.
So WHO KNOWS what fascinating things might be said in Wolf’s Pub on a Thursday or Friday night?
But first, let’s get the RED TAPE out of the way.
VERBATIM, from the regular bartender.
HOUSE RULES

God bless us, every one! Tiny Tim had such a beautiful soul. He hadn’t a mean bone in his body…unlike most of us. But in keeping with Christmas, we promise to honor Wolf’s rules and keep Scrooge at bay. The Utree is where the Ghost of Christmas Present will conduct you should you need to rattle some chains. Another option, should all hell break loose is here.
Now, back to business.
AMEN!
And TGIF!
And thus a moment of thanks to ALL our contributors, current, past, and future!
H/T DP for this one!

Current Art On The Wall

Every bar needs some art on the wall, and seeing that we’re a virtual bar with access to millions of digital counterfeit prints, you may find more than just “Dogs Playing Poker”. That said…..

A Late Nod To Hanukkah

I totally missed Hanukkah this year. I was planning on doing a post, but this year, Hanukkah fell PRECISELY during my bout with Delta, and my quarantine period afterwards, and I just blew it off.
Well, better late than never.
Indeed, I think it’s pretty cool that I was “counting the days” during my illness – with Hanukkah falling on “Day 2” – the height of my illness – and finishing on “Day 9” – completely recovered and feeling great.
I love these pictures of President Trump and FLOTUS Melania – she really looked happy at this White House Hanukkah celebration.

Nothing can take away the FOUR GREAT YEARS of the Trump Presidency. Nothing. They will live forever. And for some weird reason, the story of Hanukkah reminds me of the story of the Trump Presidency.
And THAT story is not over yet!
Vaccine Stuff

If you have not seen the video of President Trump with Candace Owens, then give SUNDANCE a click (below) and watch the video over there. Hat Tip to WSB for alerting me to this great video. She also has a comment over there, and HERE, too. Be sure to watch to the end! You won’t regret it.
REAL NEWS
This week has seen quite a bit of WTF, one might say, with “Dear Leader” “Chidin’ Biden” wagging his Bill Clinton FINGER OF NO SLEEPY NO CREEPY at the unwashed unvaxxed, but we’ve got better things to do, than to listen to that lying old coot.
Go sniff somebody else’s hair, Fake President! #FJB!!!
How about, instead, I drink a bit too much ginger ale, and tell you all how I believe Bill Gates sabotaged hydroxychloroquine? With the aid of some people who we all know VERY well? Have a seat! It’s quite a story.
How (IMO) Bill Gates Sabotaged HCQ
You all are the first to hear this story.
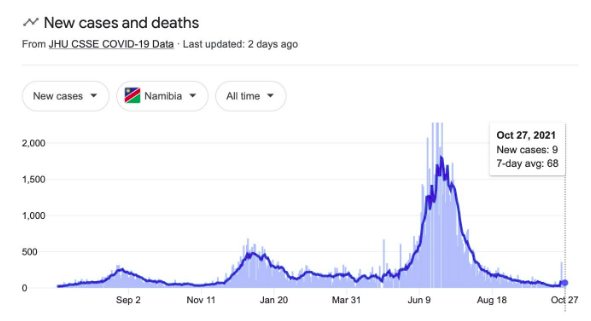
Let’s start off by listening to two Steves – Bannon and Hatfill – talking REALITY about OMICRON.
The “traveling vaccine”, as Dr. Hatfill calls it. This is short – 4 minutes.
Now Dr. Hatfill is an interesting guy. And MORE than just how he got SET UP as a PATSY on anthrax, by THEM.
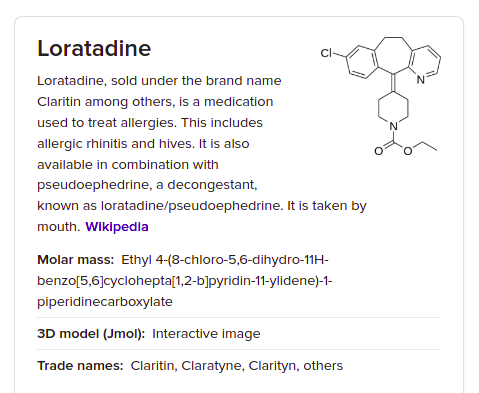
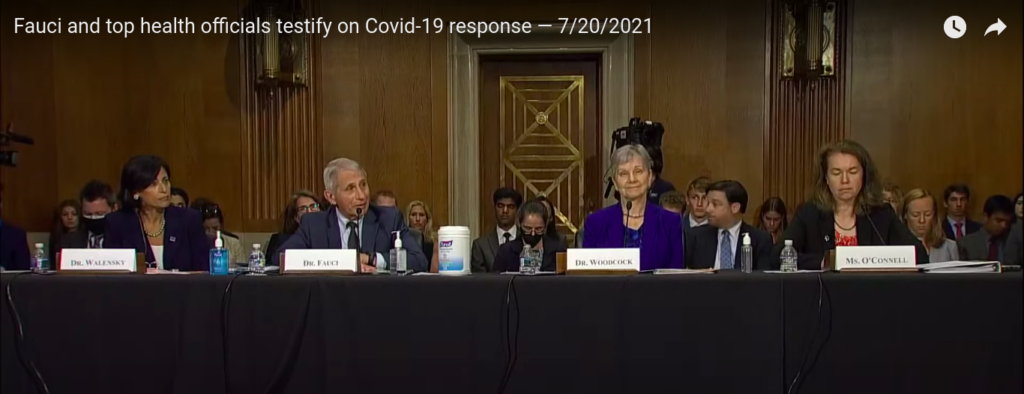
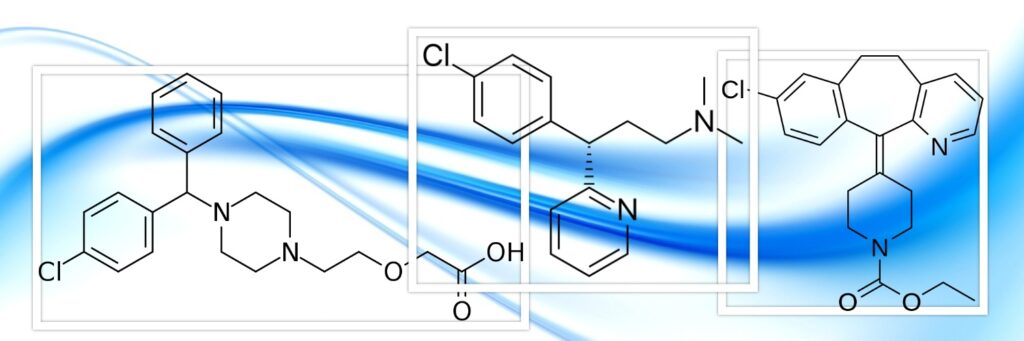
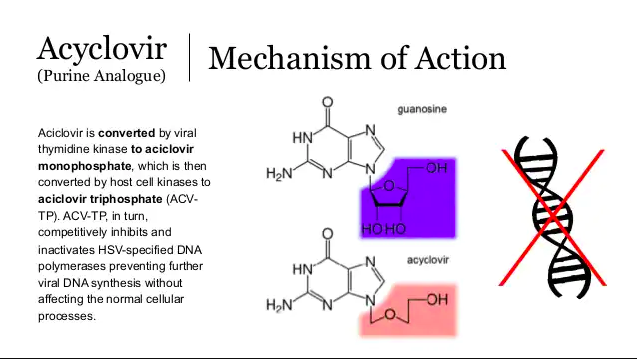
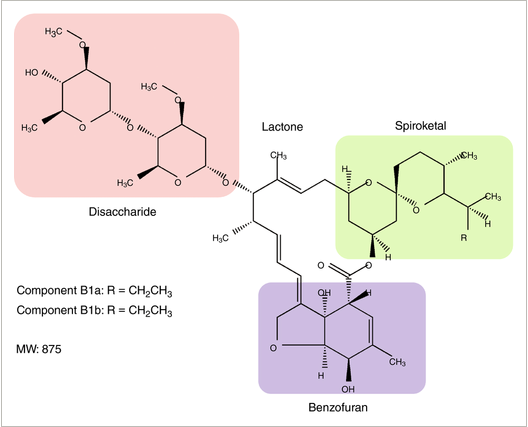
He actually knows how an alcohol called hydroxychloroquine …..
…..was deep-sixed by Rick Bright, Janet Woodcock, and Tony Fauci. Details here:
LINK: https://drstevenhatfill.com/how-a-single-point-failure-destroyed-the-national-pandemic-plan/

So this guy understands the DUPLICITY – the SABOTAGE – the DECEIT – that actually goes on in science.
That duplicity is well-represented by the recent guilty verdicts against the former Chairman of the Harvard chemistry department, Dr. Charles Lieber. You know – that guy who was helping the ChiComs with their “Thousand Talents [OF SILVER] Program”, and hiding his take from the feds.
So wait – where was I? [….looks for beer glass….]
The thing is, I discovered even MORE about how HYDROXYCHLOROQUINE was knifed in the back by the enemies of truth.
Do you all remember that GREAT video on Vitamin D in preventing COVID-19?
Well, this Doc, Roger Seheult, has ANOTHER video that I was looking at, where he talks about the vaccines. And you have to be wondering “GREAT! Is he PRO or ANTI vaccine?”
I would say that he’s definitely PRO-VAX, but not BLINDLY so. More like – the vaccine is a tool, and he’s gonna use it. He treats patients – they’re young and dying – he’s very emotional – he wants to save them – and he believes the vaccine helps. So he tells people – get the vaccine.
He’s also marginally supportive of research on ivermectin, but he’s NOT gonna buck the system by advocating current use. He does NOT seem to have very much discernment about DECEIT and CORRUPTION in science, IMO. He’s a bit of an innocent, or even a chump, just like most people in science, who think the whole thing is a zone of trust, relatively free of deception and trickery.
Here is the video.
This is actually really good stuff, but if you’re looking for ammo against vaccines, this is not it. This is more like a “good doctor” trying to convince you – with mostly good data – but in some places weak data – to take the vaccine.
I can almost see it. ALMOST. But not quite. Not for me, certainly. My “medical advisor” who says “what in the HELL happened to contraindications and the VERBOTEN status of vaccination during pregnancy?” says “NO”.
HOWEVER, if you’re looking for where the pro-vax side is WEAK and DEFENSIVE, this is also a great video. You can see where they’re in trouble, and where they’re avoiding things, and where they’re grasping at straws. It’s very edgy scientific detective work, but I read these people pretty well.
More on THAT stuff in a full post to come.
This dude doesn’t want to lose his channel. Bottom line. But you can read past some of what is said.
So first, BEFORE we get to the BIG CRIME, a small sidebar.
Sidebar: Dr. Geert is Right Again
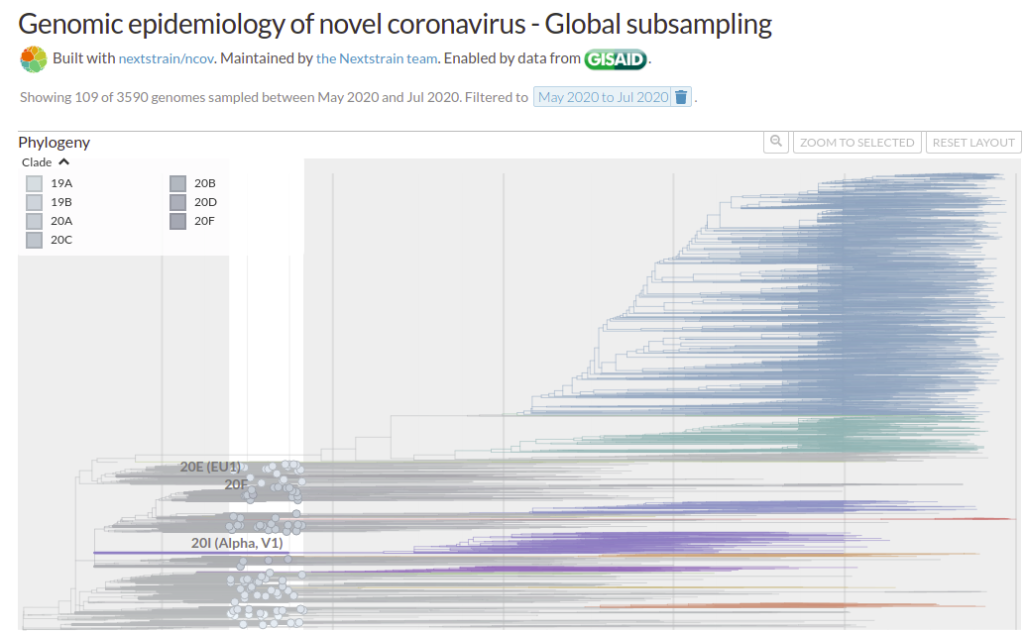
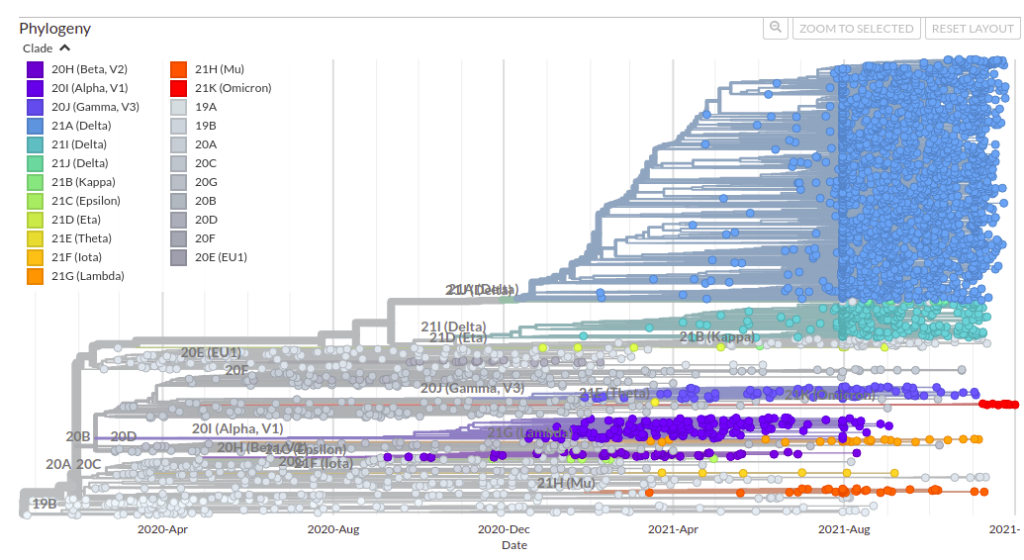
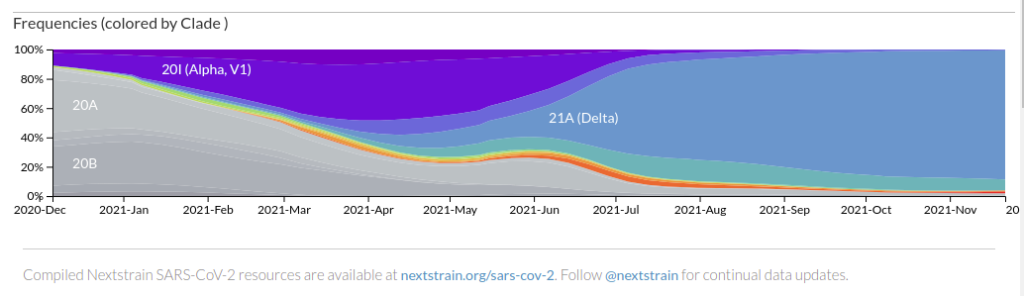
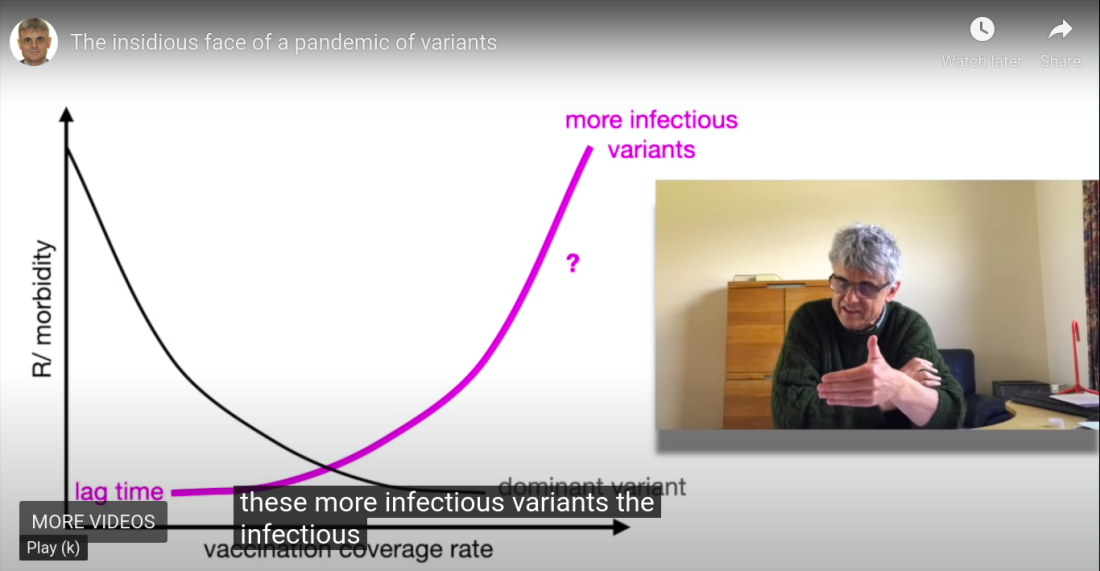
There is a slide in Doc Rogers’ video that PROVES ONE MORE TIME that Dr. Geert Vanden Bossche is TOTALLY RIGHT.
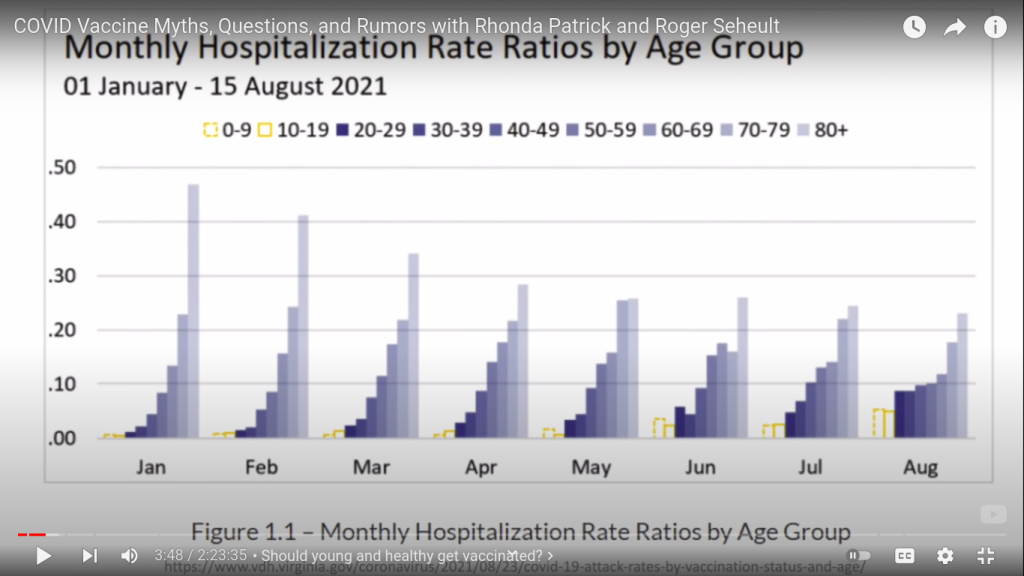
Dr. Roger is showing this to us, to emphasize that younger and younger people are being hospitalized with COVID now – that pediatric cases are increasing, as Delta is taking over. This is part of why the DOCTORS are pushing to vaccinate kids. They’re getting more and more young adult, teen and pediatric cases in the hospitals. It’s an emotional strain on them to watch young people die.
But there is a problem.
MASS VACCINATION ITSELF IS CAUSING THIS PHENOMENON.
This is EXACTLY what Dr. Geert Vanden Bossche has been warning about. EXACTLY.
People have got to start listening to this dude.
Bill Gates’ CEO, who is advising Joe Biden, was an adjunct professor of epidemiology. Surely she can understand Geert. But she’s also on Pfizer’s board. That’s a problem. A real conflict of interest. Geert is an epidemiologist, and he is predicting all this stuff like clockwork. Maybe she should take a listen.
BUT – back to the story…..
Of the ASSHOLES who are pushing vaccination…..
By INTERFERING with science…..
By UNDERMINING science at the most basic levels.
So you see by that example – the slide of hospital age groups – what is so great about these sorts of videos is that these docs and experts will pop out the convincer graphs and references, and you can either screen capture like above, or GO TO THE SOURCE.
OR go somewhere ELSE they don’t want you to look.
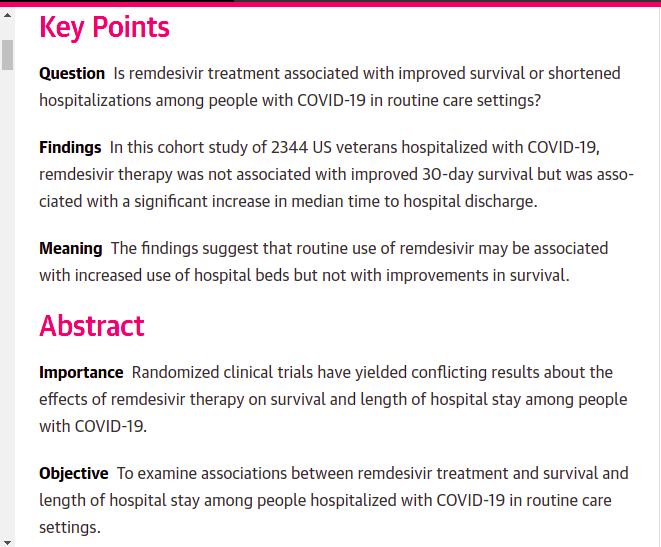
So LATER in this Dr. Roger video, immediately after a rather prog-chauvinistic, hand-waving excuse why certain positive foreign studies of ivermectin should be dismissed (pure Fauci shade-throwing – go to 1:22:30), he mentions some American study – which was NOT LancetGate – that he says disproved hydroxychloroquine.
He just throws that in as an aside – but that’s BULLSHIT.
HCQ isn’t GREAT, but it works when given very early, it has saved MANY lives, and there is simply no doubt about it, at this point. So the good doctor is LOSING credibility with me right there. He’s following close, but he’s not following close enough, because he’s clearly trusting NIH, CDC, and Fauci.
He’s a chump – and he can be fooled by flowing along with the similarly chumped mainstream of science. He’s inside the big deceit – he has no reference frame.
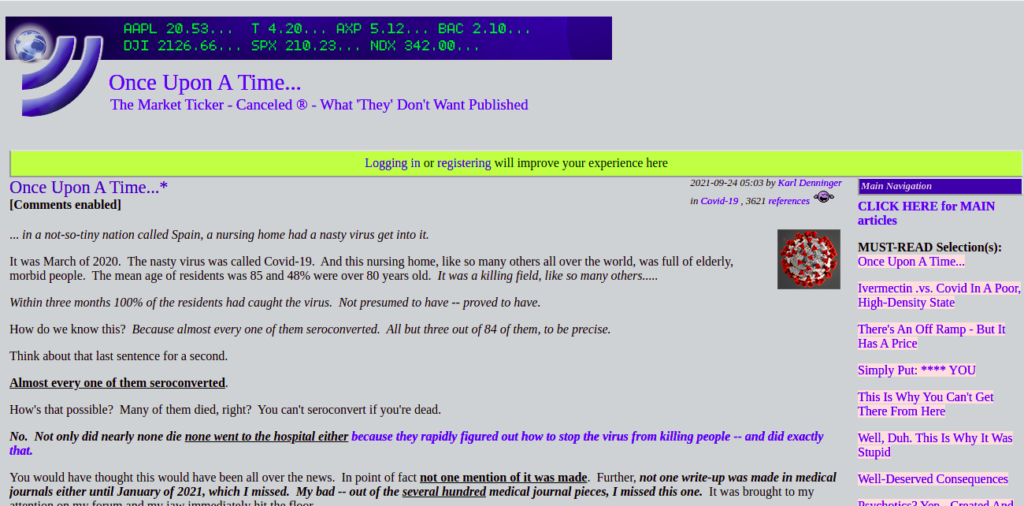
So what IS this study that “disproved” HCQ? Screenshot:
This thing was called the “Together COVID Trial”. And it’s still out there.
LINK: https://www.togethertrial.com/
These ad hoc COVID trials have been taking place in CANADA and BRAZIL – both of which make Suspicious Cat *immediately* purr “serious communist problems in both places” – and if you recall that French communist, Agnes Buzyn, who very stealthily took HCQ out of OTC status in France, you understand that this is significant.
Union communists and other embeds make GREAT footsoldiers. They’ve infiltrated medicine – they’ve infiltrated science – they’ve infiltrated universities, and hospitals – and they do the dirty jobs, where a spy would otherwise be required. My first exposure was in a university scandal, and that was just the beginning. I’ve had to deal with top-shelf university science commies on this very site. They tried to pull a really fast one on us, back at the beginning of COVID. They are dead serious in this big attempt to install WORLD COMMUNISM.
ANYWAY – back to the story.
At THAT point, I remembered something Bill Gates said on TV – the ONLY time he mentioned hydroxychloroquine. He said that “WE” would have to do studies on it.
As soon as I heard that, I rolled my eyes. Oh, yeah. FOX in the freakin’ hen-house.
“We have to STUDY the chickens.”
What a joke.
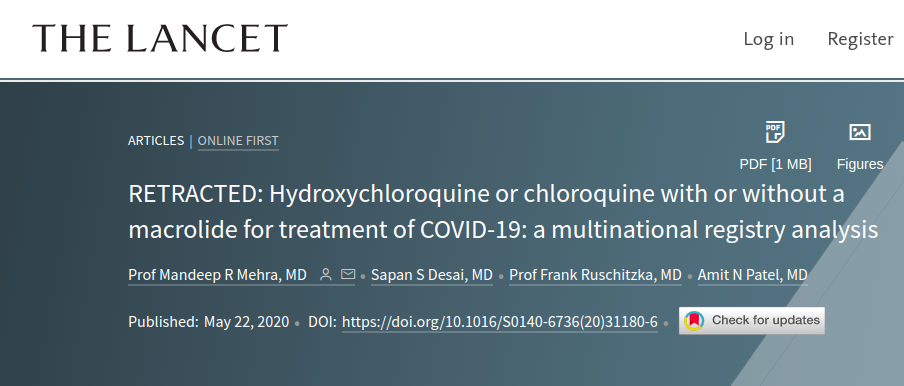
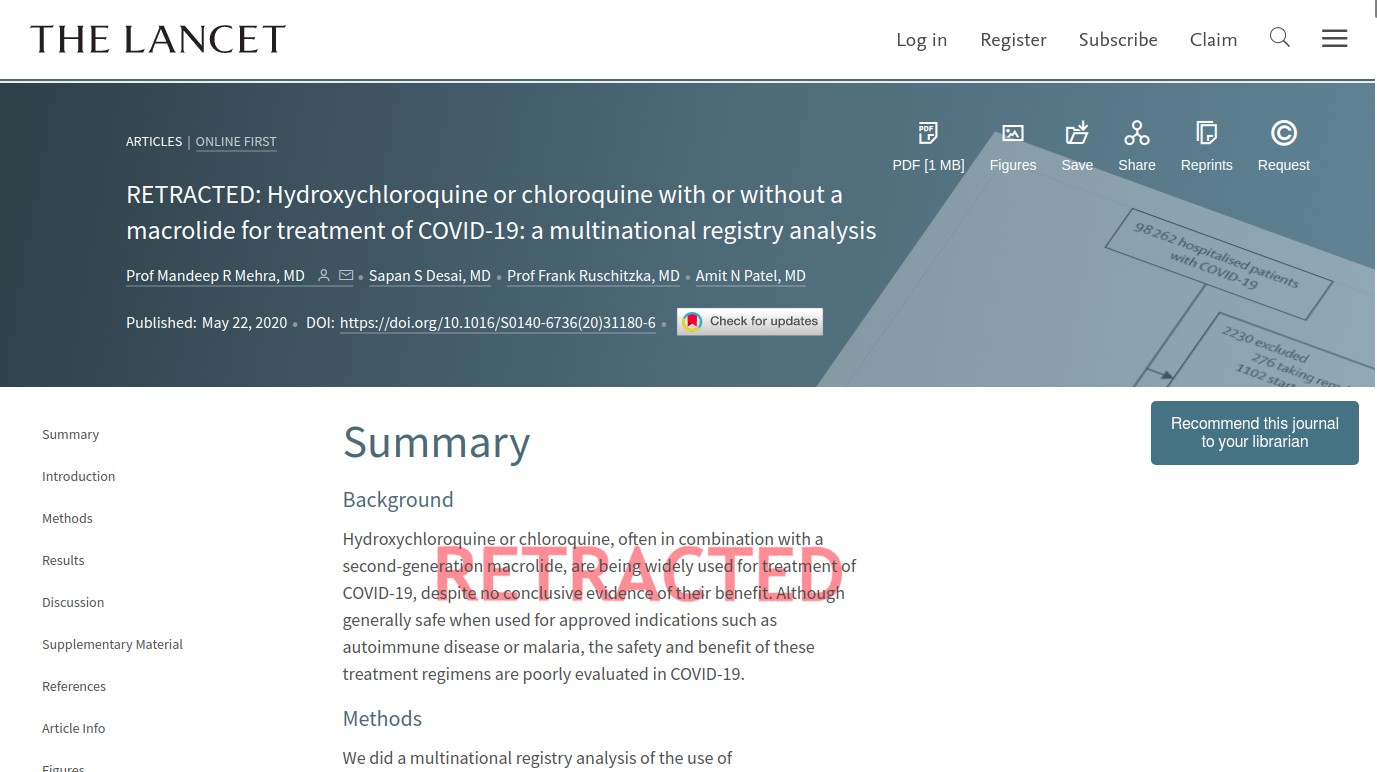
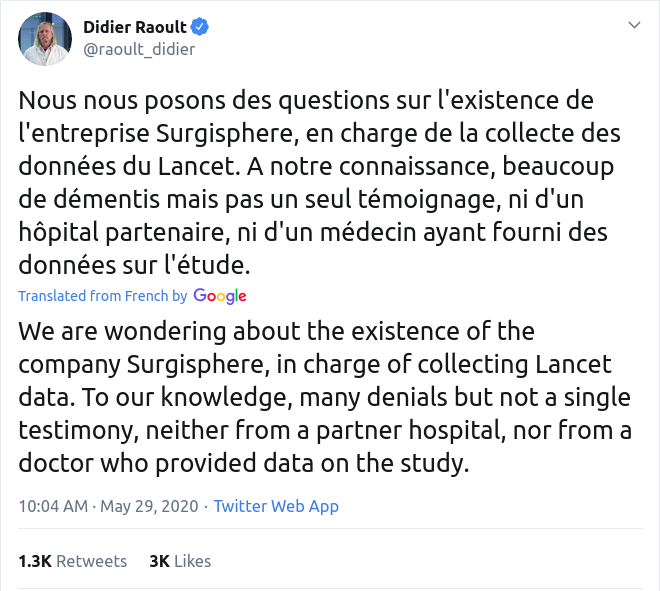
I have always felt that Gates was behind Surgisphere and LancetGate, the biggest hit job EVER on hydroxychloroquine, which was retracted, but I have yet to find evidence of his involvement – and I have looked several times.
HOWEVER, it turns out that Gates WAS behind the studies of hydroxychloroquine that killed people by overdoses, while giving it too late to save them.
Yeah. That’s convenient. That combination of two crucial errors is diagnostic for a very professional scientific kill job, BTW. When you REALLY want it dead, wooden cross and silver bullet. A scientific double-tap.
See? You learn something every day.
So I’m thinking – well, maybe GATES is behind THESE STUDIES.
So then I go looking to see who is behind them, and this is what I see.

AH! So who’s that?
I went after “Rainwater” first, because I was thinking “Oh, yeah, baby – this sounds like the Tides Foundation” – that being the “charity” by which John Kerry and his rich wife send all kinds of seed money to left-wing operations.
But I check it out, and it’s just some Texan good old boy named Rainwater who left his fortune as a foundation, and at worst, the money got pointed to help Gates by some lefty kid or nephew. More likely an alumnus story or something like that.
NOPE. Not that one.
So what about “Fast Grants”?
GOLD MINE.
LINK: https://fastgrants.org/
ARCHIVE: https://archive.fo/YQI2N
The way this org is set up, the people who choose the grant proposals get a gazillion begs, from which the operation can pick and choose. And there is nothing that can prevent a secret reach-around where the choosers or their puppets can SEND THEIR OWN PUPPET PROPOSALS INTO THE SCAM.
See how that works? Very slick.
So who funds the begs?
The grants are currently supported by: Arnold Ventures, The Audacious Project, The Chan Zuckerberg Initiative, John Collison, Patrick Collison, Crankstart, Jack Dorsey, Kim and Scott Farquhar, Paul Graham, Reid Hoffman, Fiona McKean and Tobias Lütke, Yuri and Julia Milner, Elon Musk, Chris and Crystal Sacca, Schmidt Futures, and others. AWS has contributed compute credits.
OK. This is so easy, I’m gonna leave some of these names for everybody else. But this thing is so full of “usual suspects”, it should be a movie.
The Chan Zuckerberg Initiative is Facebook, which incidentally had – until right after COVID was released – a BOARD MEMBER and DIRECTOR who happened to be the CEO of the Bill & Melinda Gates Foundation – a lady named Dr. Susan Desmond-Hellman – who recently joined the board of Pfizer – and is also now one of Joe Biden’s presidential science advisers. I mentioned her above.

Hellman was appointed to the social media platform’s board in March 2013 and served as it Lead Independent Director from June 2015 until October 30th 2019, shortly before the first reported case of COVID-19.
https://thenationalpulse.com/exclusive/pfizer-board-member-is-former-facebook-director/
Yeah, that’s cozy.
Covered here previously.
The Vaccine-Powered Rona-Coaster
Is the Directed Evolution of Variants – Something Deeply Understandable to Joe Biden’s Science Advisors – Being Abused by the Corporate-Government-Academic Axis? Yeah, you remember that one! Several hat tips to Sundance on this one, too. It’s now becoming very clear that the mercenary Bill Gates getting involved with healthcare was one of the LAST …
So we have BILL GATES linked to, and MARK ZUCKERBERG and his CHICOM WIFEY funding, a study that tried to take down HCQ, and certainly seems to have influenced a lot of doctors against it.
SMART. Influence the docs, but do it quietly and behind the scenes – so there’s not so much outrage stirred up like LancetGate, which outraged the scientific community, and caused those two journal editors to squawk excuses in the “leaked” telephone conversation.
Less visibility, but more long-term effect. I really think this is why a lot of doctors “gave up” on hydroxy.
BUT WAIT – THERE’S MOAR.
Who else is behind Fast Grants?
CHOOMER RASPUTIN – a.k.a. Jack Dorsey, of Twitter.
It’s a small world at the top of the COUP, ain’t it?
BUT WAIT – THERE’S MOAR.

Who’s the last person on that list? It’s not who you think.
“AWS has contributed compute credits.”
AWS is Amazon Web Services. That’s the CIA. So THEY’RE handling the computers in some way. They likely had INSIGHT into all the trials.
Does this all make sense now?
Good.
Now – I have not looked at this paper yet, which knifed HCQ in the back – nor have I looked at one of the Together Trial studies of ivermectin which they also did, which found no utility.
I’m sure I will look at these papers at some point, but I’m lazy, and it’s late, and my wife wants me to go to bed.
But with these tips, I’m certain that some intrepid HONEST scientists out there will now find obvious problems with the studies. Because they’re gonna be there, trust me.
This is the state of science. It is extraordinarily manipulable. And one of the BEST ways to manipulate it, is to FUND IT, and then have access and control that is hidden from the public.
That’s life in the big city.
Bottom line – I think this is one piece of the puzzle of how hydroxychloroquine was taken down. MULTIPLE HITS by Bill Gates. The man was NOT taking any chances.
Christmas Eve
I could let this post end with a story of science corruption, but that’s not how things end. That’s never how things end.

You see – there was this guy named Jesus, and he was all about bringing GOD (or G_D, if you prefer) to the low-lifes. The tax collectors. The prostitutes. The immigrants. The wise guys. People like me. People like the people I understand. People like us. People like all of us.
There are a lot of things I could talk about, relating to the Kingdom of Heaven, and how it’s a lot closer than people realize, but what’s funny about THAT, is that it’s a lot like some of the things we run into here, in our efforts to shine the light of Truth on things.
The small stuff is easy to write off, and the big stuff is protected by unbelievability.
But nevertheless, I won’t give up, trying to get others to see the beauty of it all.
That the big party really is there.
That we’re all invited.
And that it really is ALL THAT AND A BAG OF CHIPS.
I don’t approach Christianity like most people. I use the Bible to try to understand the nature of reality. I try to understand what Christ was telling us at a weird and deep level, because I’ve found that his “thought experiments”, if you will, were always consistent on many levels of interpretation, and they help me to see – with more beauty and less words – what he meant.
I trust now for different reasons than I trusted before, but I still trust.

Anyway, Christmas is a time to reflect on Christ. And interestingly, this year, it’s really working for me.
I hope I can help you to do the same!
Merry Christmas, friends and neighbors. Posters and lurkers. Believers and skeptics. Allies and enemies.
There’s room for you all at a certain place in this town. Or very close by.
W