I. The Clot Shot
First things first.
Nobody would be calling ALL of the various full-length stabilized SARS-CoV-2 S1 subunit spike protein vaccines “the clot shot” if there weren’t some clear and obvious problems with the full-length stabilized SARS-CoV-2 S1 subunit spike protein ITSELF.
We already know that clotting dysfunction is key to COVID-19 pathogenicity. SO – it’s not exactly a surprise that the spike protein itself, and likewise the S1 subunit of that protein – a.k.a. THE BUSINESS END – are themselves pathogenic.
EXAMPLE:
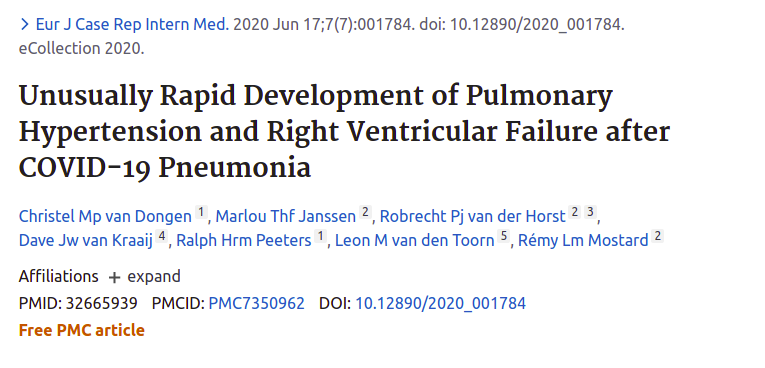
Spike Protein S1 Subunit as Direct Lung Pathogen

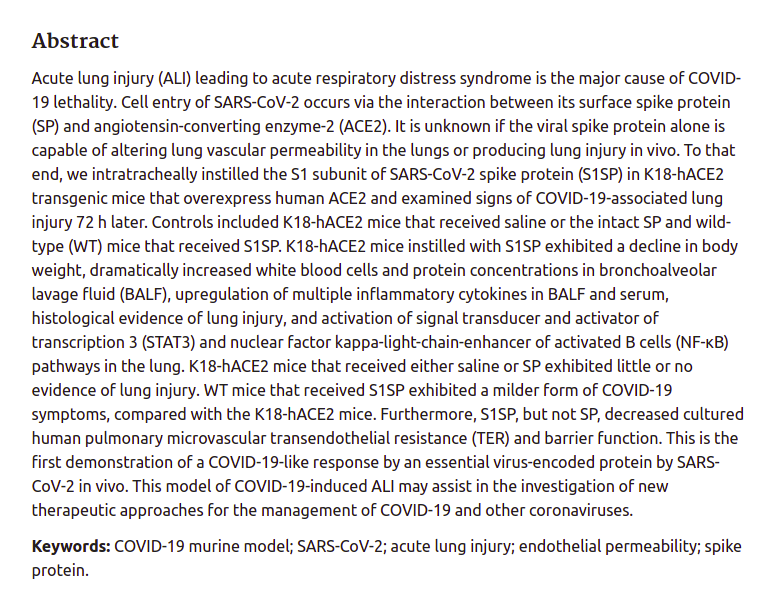
LINK 1: https://pubmed.ncbi.nlm.nih.gov/34156871/
LINK 2: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8384477/
In the above example, the S1 subunit of the spike protein was basically 100% lethal to humanized mice when applied to their lungs.
And when they looked at the mice, the damage was basically the same as the damage from COVID-19.
Just sayin’.
So let me now TEST you, and see if you’re more of a scientist than Fauci’s protege Rochelle Alinsky – WHOOPS – I mean Rochelle Walensky – who heads the CDC for Fauci to maintain control of it.

If you give a SPIKE PROTEIN VACCINE to somebody, and they have symptoms of COVID-19 during the next few days, or even during the next two weeks, which scenario is more likely?
(A) – The person just happened to get real COVID-19, and THAT spike protein did BAD THINGS.
(B) – The spike protein you put inside the person did BAD THINGS.
Do you see how science works?
It’s a lot like common sense, only it’s applied to fancy stuff.
I want you to meet some great scientists here. These are people with very little scientific authority, but they simply practiced science, instead of repeating what authorities told them.
(1) – The CNA who would not accept “super-spreader” myths
This guy was one of the first people to administer the Pfizer vaccine to nursing home residents.
He was shocked that his nursing home residents would die shortly after being vaccinated – after having survived for months BEFORE the vaccine – in a way that was clearly related to their being vaccinated with the Pfizer vaccine.
Nursing home management would NOT admit to the obvious connection – and created a mythical “super-spreader” to explain the deaths.
This man is a HERO.
The first 10 minutes of the video is this man working up the courage of conscience – to SPEAK THE TRUTH. If you just want to hear what he needed to say, you can jump to 10 minutes and you will hear the SCIENCE.
LINK 2: https://www.bitchute.com/video/cpQ7dnqu0Sos/
(2) – From Physician’s Assistant to VAERS Whistleblower
This lady, a hospital physician’s assistant, started out as a “COVID training true believer”, but she began observing what the shots were doing in her hospital. From there, she began encountering resistance to “doing the right thing”.
Now, in retrospect, you can see everybody in the system avoiding responsibility – not just for the problem, but for even reporting it.
A fantastic interview by Del Bigtree’s Highwire show.
LINK 1: https://thehighwire.com/videos/these-patients-deserve-to-be-heard-vaers-whistleblower/
(3) – Doctor Discovers Disseminated Clotting in Most Vaccinated Patients
We covered this just recently, HERE.
This doctor discovered not only that “the jab” was leading to loss of wind (reduced effort tolerance) in too many of his patients – a whopping 62% of all his patients were showing signs of microscopic clotting – similar to COVID-19 – after vaccination.
LINK: https(colon)//www.bitchute(dot)com/video/A6GbcUl6blpJ/
Bibliography of our own Spike Protein Suspicions
Now – this site has also not been negligent in reporting on the problems of the “clot shot”, as you can see from the following bibliography.
Thus, you will see that we were READY when a good explanation of the clot shot arose.
II. The Explanation
I want to start by thanking barkerjim for posting a comment with a link that leads to a very recent paper (pre-peer-review, of course) that explains the clot shot. He found the link HERE on Denninger’s Market Ticker site.
The order of the finding:
Denninger Comment: https://market-ticker.org/akcs-www?singlepost=3724148
Q Tree Comment: https://www.theqtree.com/2021/10/18/dear-kmag-20211018-joe-biden-didnt-win-%e2%9d%80-open-topic/comment-page-2/#comment-816737
Ecosophia Comment: https://ecosophia.dreamwidth.org/152821.html?thread=20225013#cmt20225013
Preprint Paper: https://www.biorxiv.org/content/10.1101/2021.10.12.464152v1.full.pdf
I will include the entirety of the anonymous comment on the Ecosophy blog.
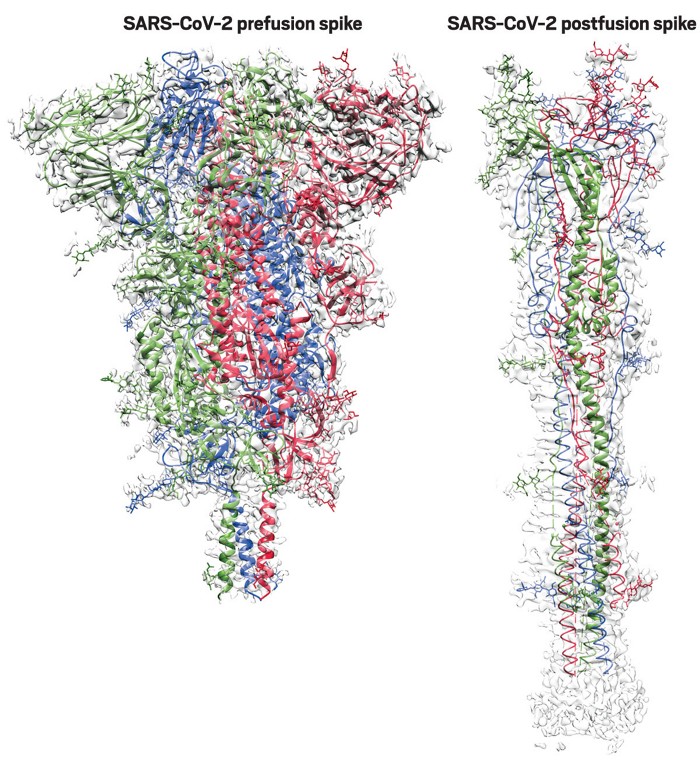
Spike Protein Clotting Mechanism
Date: 2021-10-14 06:10 am (UTC)
From: (Anonymous)
Preprint posted today. This is potentially a bombshell paper.
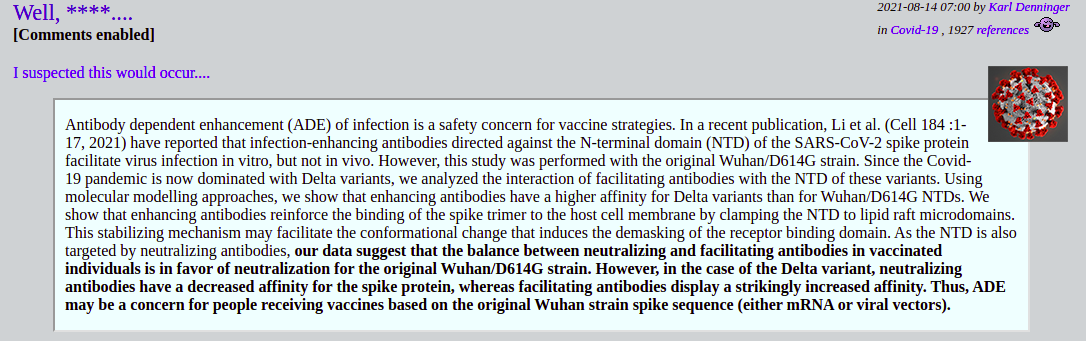
SARS-CoV-2 spike protein induces abnormal inflammatory blood clots neutralized by fibrin immunotherapy
https://www.biorxiv.org/content/10.1101/2021.10.12.464152v1.full.pdf
“Here we report that the Spike protein from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) binds to the blood coagulation factor fibrinogen and induces structurally abnormal blood clots with heightened proinflammatory activity. SARS-CoV-2 Spike virions enhanced fibrin-mediated microglia activation and induced fibrinogen-dependent lung pathology. COVID-19 patients had fibrin autoantibodies that persisted long after acute infection.”
“The central structural component of blood clots, and a key regulator of inflammation in disease, is insoluble fibrin, which is derived from the blood coagulation factor fibrinogen and is deposited in tissues at sites of vascular damage (10, 11). Hypercoagulability in COVID-19 is associated with inflammation and the formation of fibrin clots resistant to degradation despite adequate anticoagulation (3-5). Extensive fibrin deposits are detected locally in inflamed lung and brain tissues from COVID-19 patients, sometimes without evidence of direct viral infection at autopsy (1, 8, 12-14). The high prevalence of thrombotic events with these unique hypercoagulability features suggests an as yet unknown mechanism of abnormal blood clot formation in COVID-19. We set out to determine how blood clots form in COVID-19 and to identify therapies to combat the deleterious effects of abnormal coagulation occurring in acute and convalescent stages of disease.”
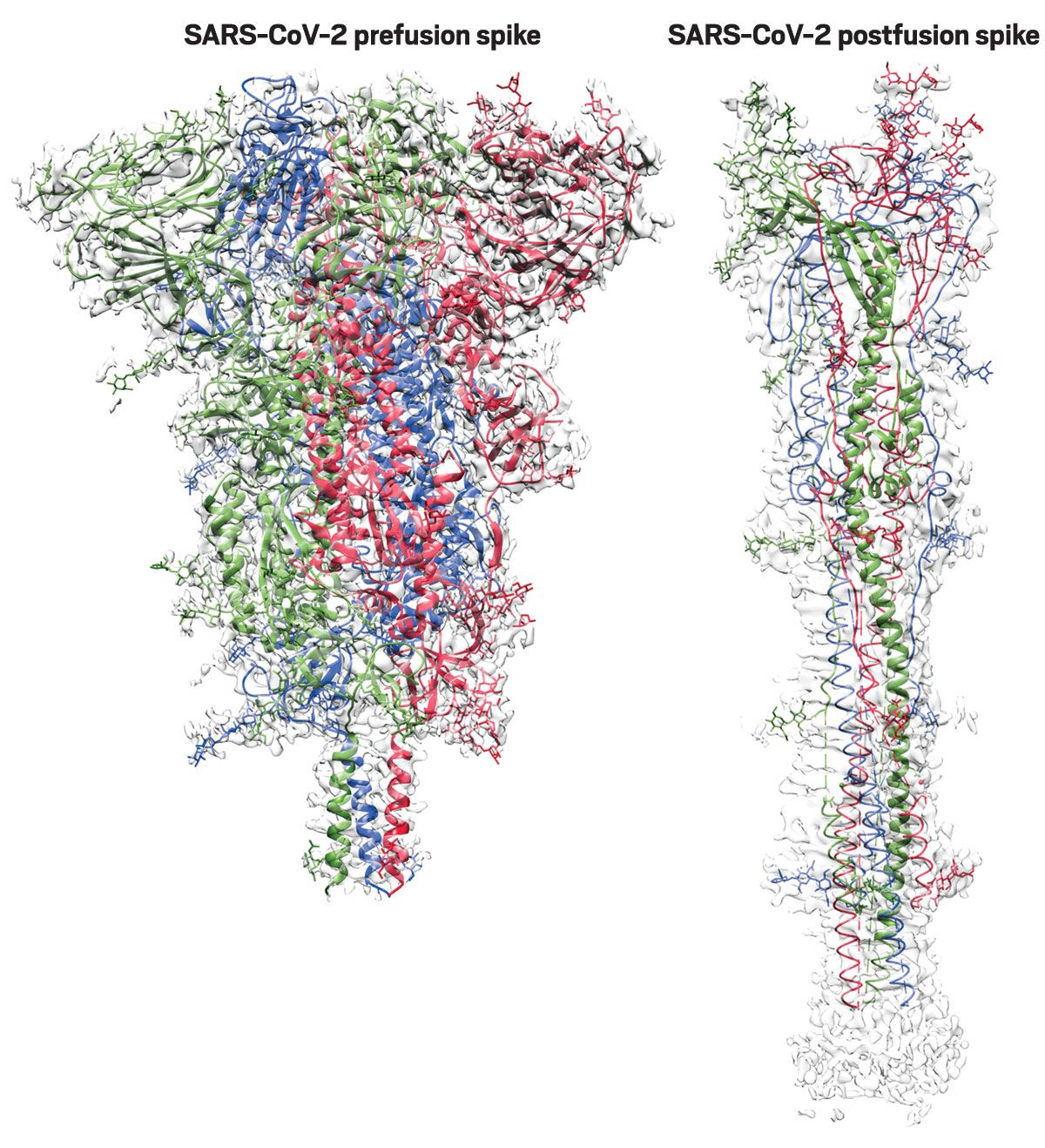
“Since hypercoagulability in COVID-19 patients has features distinct from those of other inflammatory diseases, we hypothesized that SARS-CoV-2 directly affects the structural and functional properties of blood clots. Incubation of SARS-CoV-2 recombinant trimeric spike protein (Spike) with healthy donor plasma increased fibrin polymerization (Fig. 1A). Spike strikingly altered the fibrin clot structure resulting in thinner fibers with a rough appearance and increased clot density as shown by scanning electron microscopy (SEM) (Fig. 1B, fig. S1), identifying direct effects of SARS-CoV-2 Spike on fibrin clot architecture. Consistent with these structural changes, a solid-phase binding assay revealed binding of Spike to both fibrinogen and fibrin (Kd 5.3 μM and 0.4 μM, respectively) (Fig. 1C). Fibrinogen immunoprecipitated with full-length recombinant trimeric Spike, and studies with deletion mutants identified an interaction with the S2 domain of Spike (Fig. 1D, fig. S2).”
“Intravenous administration of Spike PVs in wild-type (WT) mice induced extensive fibrin deposition in the lung (Fig. 2A). (…) Fibrin deposition was associated with activated endothelium in the lung, and gene expression analysis revealed increased expression of endothelial and inflammatory markers in Spike PV-injected mice (…) consistent with findings of SARS-CoV-2 toxicity to endothelial cells (19). (…) Mice genetically-deficient in fibrinogen (Fgα–/– mice), which express all other blood proteins except fibrinogen and are protected from autoimmune and inflammatory conditions (11), did not exhibit lung pathology following Spike PV challenge (Fig. 2E, fig. S5).”
“Fibrinogen is causally linked to the activation of macrophages and microglia in autoimmune and inflammatory diseases in the brain and periphery (11, 21). Fibrin is a driver of microglia-induced cognitive dysfunction (22) and is associated with perivascular-activated microglia and macrophages in brains of COVID-19 patients even without signs of infection (12).”
“A surge of autoantibody production against diverse immune targets have been detected in COVID-19 patients (25). To determine whether COVID-19 patients develop autoantibodies
against abnormal blood clots, we tested autoantibody responses to fibrin. (…) We tested longitudinally collected serum samples ranging from acute to convalescent disease stages from 54 COVID-19 asymptomatic, mild, and severe disease patients requiring
admission to the intensive care units (table S3). Fibrin autoantibodies were abundant in all three groups of COVID-19 patients and persisted during the convalescent stage, but were scarce in healthy donor controls or in subjects with non-COVID respiratory illnesses (Fig. 4A, B).”
“In summary, we find that SARS-CoV-2 Spike protein enhances the formation of highly
inflammatory clots that are neutralized by a fibrin-targeting monoclonal antibody. Our data shed
new light on the enigmatic coagulopathy found in COVID-19 revealing a causal role for fibrinogen
in thromboinflammation – even independent of active viral replication. The high incidence of clotting complications in COVID-19 has been attributed to systemic inflammation (3), vascular damage including abnormal levels of circulating coagulation proteins (1, 26), genetic susceptibility to tissue factor and complement genes (27), and prothrombotic autoantibodies (28). Our findings now show that coagulopathy is not merely a consequence of inflammation. Rather, the interaction of SARS-CoV-2 Spike with fibrinogen and fibrin results in abnormal blood clot formation that in turn drives inflammation.”
[ THIS HERE IS THE PART TO READ ]
Assuming the results are correct – and I can see little reason to doubt them though replication is always important – this really starts to put the puzzle pieces together. I’m frankly amazed that it took so long to figure this out.
In less-scientific language:
1. The spike protein binds directly to fibrinogen, the protein precursor of fibrin which forms blood clots.
2. This binding causes the fibrinogen to polymerize to form fibrin strands, thus forming clots.
3. Spike binding to fibrin in clots also changes the clot structure and renders it resistant to degradation.
4. Fibrin induces immune inflammation. This is usually adaptive because clotting occurs at sites of injury. It is dangerous when it occurs in response to diffuse and extensive spike-mediated micro-clotting. This helps to explain the runaway immune-mediated inflammatory response characteristic of severe Covid-19.
5. Spike *alone* (in the absence of an infectious virus) induces fibrin deposition and inflammation in the lungs of mice. However, mice lacking the gene for fibrinogen exhibited no pathology upon spike exposure, demonstrating that the fibrinogen-spike interaction is necessary and sufficient for spike-induced pathology.
6. Fibrin induces cognitive dysfunction via immune inflammation in the brain.
7. Many recovered Covid-19 patients have abundant autoantibodies against fibrin – independent of disease severity – while these autoantibodies are rare in unexposed people. This indicates both that spike-mediated fibrin formation is occurring in the course of actual human infection, and that autoreactive antibodies are formed which may play a role in chronic/long-haul symptoms or prolonged clotting problems.
8. A fibrin-targeting monoclonal antibody greatly reduced inflammation, suggesting a potential new route for disease treatment.
The paper never uses the word “vaccine” – a glaring and clearly intentional omission – but it should be obvious based on these findings that instructing the body to produce large amounts of spike protein on multiple occasions is a dangerous prospect, and it also explains those autopsy revelations of bodies full of clots.
One caveat: The coordinating author is working with a start-up company to develop treatments based on reducing fibrin-mediated inflammation, so there is clearly some commercial interest here that could be influencing objectivity. On the other hand, it is often the entrepreneurial think-outside-the-box types who end up making groundbreaking discoveries.
Mark L
[ BOOM!!! ]
This is AMAZING and powerful work.
Remember that scientific paper that we started this article with?
NOW we know exactly how that happens. See how the SCIENCE is all connecting together?
The commenter on Ecosophia makes TWO critical points.
POINT ONE is that vaccines are never mentioned. That is how this work will eventually be published. The Rochelle Alinsky CDC could STOP the paper as potentially causing “vaccine hesitancy” if the authors mentioned vaccines, but by throwing no stones, none bounce back.
The CDC will still likely DELAY this from being published for as long as they can. But by avoiding mention of vaccines, the paper cannot be scuttled on the grounds that it “might cause vaccine hesitancy”, which is the FALSE IMPERATIVE that the CDC socialists use to control science and force vaccines on us as a social sabotage. Instead, the READER can make the connections and understand the implications for vaccines.
Do you see why PREPUBLICATION COMMUNICATIONS (like this one) are now so important?
POINT TWO is that it’s JUST THE SPIKE PROTEIN – NOT THE VIRUS AS A WHOLE – that causes the problems. And it’s been PROVEN. And it’s been PROVEN that THIS is the mechanism of the problems induced by the spike protein.
The moniker of “CLOT SHOT” is literally proven to be correct.
This is a BOMBSHELL because it indicts the entire concept of full-length spike protein vaccines as fundamentally flawed. It indicts mRNA vaccines as even more flawed than antigen, because the amount of toxic spike protein is unregulated. (Notice that I’ve been saying this all along.) It doesn’t necessarily say that other types of vaccines (like RBD subunit antigen vaccines) are any safer than spike protein antigen vaccines, but they MIGHT BE.
Something even BETTER here, than just the fibrinogen mechanism, is the way that this EXPLAINS (point 4 above) what one nurse practitioner observed – that COVID strikes PRE-EXISTING INFLAMMATION. Both the WHY of some people having severe COVID and others not, and the LOCATION of those issues, is explained by fibrin’s ties to pre-existing inflammation. We now have a mechanism which we already know follows that rule, because that’s how fibrin works.
This also explains why antihistamines work to save people from severe COVID. Antihistamines are generally useful against severe inflammation by pathogenic substances which cause inflammatory reactions. It’s why they administer benadryl as a general emergency antiinflammatory for purposes like anaphylaxis prevention.
The Zyrtec Rebellion
Everybody underestimates Spain. The last letter in “PIGS” is far less of an insult than an error. Years ago, when I was at a conference, and Japanese industrial spies were getting me drunk (it was a great red wine), I decided that I had to give them SOMETHING for their time and effort, if only …
And yet the CDC has WARNED people against taking antihistamines with the vaccine – when this work LITERALLY PROVES WHY THAT IS A GOOD STRATEGY – just as it is a good strategy to take antihistamines to protect against severe COVID.
Like I said, this study proves THAT we were right, and WHY we were right.
And why is CDC so WRONG – time and time again?
This is a breaker of logjams. The insistence on the use of a fundamentally flawed vaccine is CRIMINAL.
Mandates are bad enough, but over a vaccine, the very principle of which is scientifically proven as DANGEROUS?
If mandates continue, these people need to be in JAIL. If they RESIST, they need to be OVERTHROWN.
In short, THIS.
Mandating this fundamentally dangerous vaccine is so wrong on so many levels.
This is a EUGENIC VACCINE if there ever was one. It’s almost DESIGNED to finish off people who are not 100% healthy.
How can this be right? Seriously. How can this be right?
We can no longer tolerate these people who pretend not to know.
III. The Faucist-Lysenkoist CDC That Pretends Not To Understand
I start this section by thanking three people – Sundance, Aubergine, and Trumpismine – who helped me to see what is going on here.
SUNDANCE informed me of the “Mamet Principle” – that liberals pretend not to know things
AUBERGINE formulated her wonderful Razor – that it is dangerous to dismiss such pretense as mere stupidity, when it might be the product of malice or guile.
TRUMPISMINE turned me on to the Wikipedia definition of Lysenkoism, which contained enough detail that I was able to connect the goals of old Lysenkoism to the actions of the left today.
The so-called Mamet Principle is a paraphrase of a repeated point by David Mamet, which Sundance encapsulated as a principle. This has been discussed and exemplified many times, both here and on CTH.
In asking WHY liberals “pretend not to know things”, we now understand that Hanlon’s Razor is an EXCUSE – that it’s COVER – and that it’s NOT because they’re STUPID, but rather because they’re smart and evil.
The best and most concise description is a reworking of Hanlon’s Razor by our own Aubergine.
So what if we apply this to Saint Fauci of Antibodies?
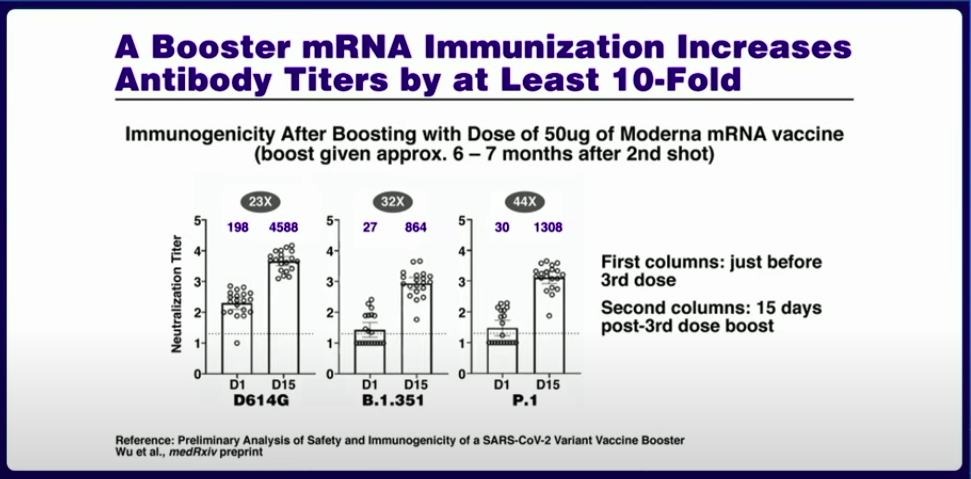
Anthony Fauci has a literal MAGICIAN’S POWER to make people focus on the WRONG THING. His skills of EVASION are absolutely outstanding. I love to call it “antibody hypnosis”, because that is exactly what it seems like.
“YOU WILL LOOK AT THE ANTIBODIES. THE ANTIBODIES WILL SAVE YOU. LOOK ONLY AT THE ANTIBODIES. YOU ARE FEELING WARM. YOU ARE FEELING SAFE. YOU ARE HAPPY ABOUT THE ANTIBODIES. THE MORE ANTIBODIES YOU SEE, THE WARMER YOU FEEL – LIKE THE SUN ON YOUR FACE ON A BEACH.”
You even hear his voice when you read that – don’t you? That gravelly, reassuring voice.

It’s VERY intentional.
Focusing on ONE WRONG THING – or even ONE RIGHT THING – is a technique of misdirection, but it is one of the BEST ways of pretending not to know things.
“Let’s only talk about this.”
Rand Paul knows all about it. He has gone many rounds with the Fauci critter.

But it’s not just Fauci.
His protege in CDC, who gives Fauci effective control of medical science, is every bit as bad.

It even includes Rand Paul’s colleagues in Congress.
The man behind the launch of censorship. Is this guy even AMERICAN?
What a PUTZ.
ANYWAY, this is where I started to figure things out.
This WEIRD LOVE of the radical left for brutal, aggressive, stupid, uncaring science – where does it come from?
I did not expect the answer that I found, with the help of Trumpismine and Wikipedia.
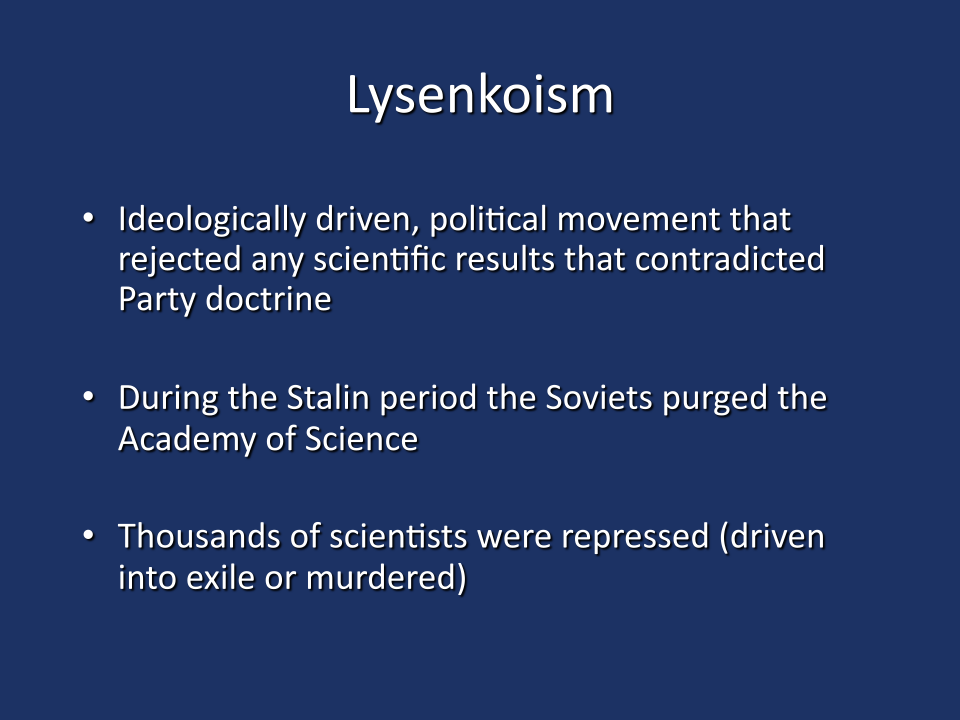
Lysenkoism

LINK: https://en.wikipedia.org/wiki/Lysenkoism
It’s very helpful to read this, including this part:
Marxism–Leninism postulated “universal and immutable laws of history” (historical materialism and dialectical materialism), which assumed unavoidable large-scale change at the collective level of societies.[5]Collectivism was a key feature of Marxism; Darwin’s concept of a random mutation in an individual being able to propagate and transform subsequent generations was at odds with the ideology, and was perceived as having a strong liberal inclination.[6] Marxist–Leninist theorists presented Lysenkoism as a new branch of biology, arguing that “dialectic method shows that development is carried out in a dual form: evolutionary and revolutionary.” Darwin was attributed with discovering “only the evolutionary” path, while Michurin and Lysenko were presented as making a “great step forward” toward the discovery of a “revolutionary” path of biologic development.[7]
Most people brought up in mainstream, establishment, Western science use the term Lysenkoism without really understanding the political angle of it. We understand it merely as “politics being imposed on scientists in the Soviet Union, which set back Soviet biological science by decades.”
Yes, that’s true, but it’s not ALL of the truth. The more you know about it, the more it looks EXACTLY like “Woke Science”.
As an aside, clearly it makes sense WHY China (and to a lesser extent Russia) would want to promote Lysenkoism in the United States, as part of their own interests. “China First” and “Russia First” by socialist and ex-socialist means are unlikely to be pretty. “Fuck the other guy up so he can’t win” is a valid technique in a corrupt world.
But it goes deeper.
Lysenkoism is far less about being STUPID, than about being REVOLUTIONARY. That is a critical idea. That quality of being revolutionary makes mistakes, and when it does, it’s generally STUPID. But when it does NOT make mistakes, it’s generally EVIL.
Let me repeat what I said, earlier about Lysenkoism.
[QUOTE]

Wolf Moon Online Admin Coyote Reply to trumpismine October 18, 2021 02:36
This is EXCELLENT READING!!!
You know what? This is actually really interesting reading.
In a WEIRD WAY – Lysenko was “right”, in that he maniacally predicted EXACTLY what the communists are doing NOW with gene therapy. His assertion of a “genetic dialectic” – of the “evolutionary” in conflict with the “revolutionary” – is actually what we’re seeing RIGHT NOW with the “natural evolution” crowd (US) versus the commie-forced gene therapy crowd (THEM).
Marxist–Leninist theorists presented Lysenkoism as a new branch of biology, arguing that “dialectic method shows that development is carried out in a dual form: evolutionary and revolutionary.” Darwin was attributed with discovering “only the evolutionary” path, while Michurin and Lysenko were presented as making a “great step forward” toward the discovery of a “revolutionary” path of biologic development.[7]
It was just total hubris and pathological commie science – a lot like what we see from Fauci, Gates and Walensky – but it “anticipated” what WOULD come eventually through science – that someday WE would have the power to do the things – and make the mistakes – that we are making now.
So in many ways these people ARE the intellectual inheritors of Lysenkoism!!!
Lysenko’s mistake was claiming that things WERE what they merely COULD BE through greater understanding.
Imagine some person coming BEFORE Galileo and trying to FORCE heliocentrism in their country – killing, jailing, ousting, and attacking the geocentrists.
In a sense, that was Lysenko, who attacked natural evolution.
Natural processes are “evolution”.
Genetic modification is “revolution”.
The dude was a NUT, trying to assert that the NATURAL was both, when it’s almost all ONE. But if he would have simply said “We must become revolutionary in genetics, which is merely evolutionary now”, then he would have been like the Lenin of biology, and he would likely be admired today by all these crazy leftists and depoppers, instead of an old Soviet embarrassment.
But ALL OF THAT comes back and tells me that these people are the modern recapitulation of Lysenkoist THOUGHT, but using the GAINS of actual evolutionary understanding.
The nutbaggery we see NOW with the communist jab-maniacs, is just like Lysenko’s assertions, only MORE REAL because they have MORE TECH.
[END QUOTE]
Soviet science, and Lysenko in particular, were characterized by a kind of VIRTUE SIGNALING, and that is what we are seeing now on universities, only it tends to be about peripheral things, like race, diversity, gender – whatever is in leftist vogue.
But NOW, in our phony socialist “pandemic”, we are seeing the virtue signals rise to levels that affect the practice of science itself. It’s starting at GOALS, but very soon, it will get a bit like CLIMATE LYSENKOISM, where people CHANGE DATA, HIDE DATA, DROP EVIDENCE, and basically act like MAINSTREAM MEDIA JOURNALISTS, who are in a continuous state of covering things up by omission, distraction, and promotion of contradicting narratives.
That is NOT GOOD.
I think that we are now seeing with publications like the one featured in this article, is some PUSH-BACK by scientists who realize where things are headed – a VERY BAD place. They are GETTING THE TRUTH OUT.
We need to help promote awareness of science that CDC and the communist infiltration are going to hide.
W
On August 7, 1948, at the end of a week-long session organised by Lysenko and approved by Stalin,[14] the V.I. Lenin Academy of Agricultural Sciences announced that from that point on Lysenkoism would be taught as “the only correct theory.” Soviet scientists were forced to denounce any work that contradicted Lysenko.[19] Criticism of Lysenko was denounced as “bourgeois” or “fascist,” and analogous “non-bourgeois” theories also flourished in other fields such as linguistics and art in the Soviet academy at this time. Perhaps the only opponents of Lysenkoism during Stalin’s lifetime to escape liquidation were from the small community of Soviet nuclear physicists: as Tony Judt has observed, “It is significant that Stalin left his nuclear physicists alone and never presumed to second guess their calculations. Stalin may well have been mad but he was not stupid.”[20]